Embed Size (px)
Citation preview

EFFECT OF CARBOHYDRATE SOURCE ON POSTPRANDIAL
BLOOD GLUCOSE IN SUBJECTS WlTH TYPE 1 DIABETES USlNG
INSULIN LISPRO
Nadia H.J. Mohammed
A thesis submitteâ in confomity with the mquimments for the ûegme of Master of Science,
Griduate Department of NutrStionaI Sciences Univemity of Toronto
@ Copyright by Nadie ~ o h a ~ h e d 2001

National Cibrary û i b i i i u e nationale du Canada
Acquisitions and Acquisitions et ôibiiüg i-aphic Services services bibiiographiques 395 Weliingtolr Street 395. rue Wdington OnawaON KlAOW O(tawaON K 1 A W Canada CaMda
The author has granted a non- L'auteur a accordé une licence non exclusive licence allowing the exclusive permettant à la National Libraxy of Canada to Bibliothèque nationale du Canada de reproduce, 10- distrtiute or seil reproduire, prêter, distribuer ou copies of this thesis in microfom, vendre des copies de cette thèse sous paper or electronic formats. la forme de microfiche/nlm, de
reproduction sur papier ou sur fomat électronique.
The author retains ownersbïp of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protège cette thèse. thesis nor substantial exûacts fiom it Ni la thèse ni des extraits substantiels may be printed or otherwise de celle-ci ne doivent être imprimés reproduced without the authw's ou autrement reproduits sans son permission. autorisation.

To my parents

TABLEi OF CONTENTS page
ACKNOWLEDGEMENT ..........i....................................... iu
.......................................................... LIST OF TABLES
LIST OF FIGURES .........................................................
LIST OF APPENDICES ...................................................
ABSTRACT .................................................................. vïii
CHAPTER 1 INTRODUCTION AND LITERATURE REVIEW 1.1 Introduction .....................................................
................................................. 1.2 Literature Review 1.2.1 De~tionofDiabetesMe~tus .................... ... 1.2.2 Prevalence ................................................ 1.2.3 Classification ......................................*...... 1.2.4 Diagnosis ................................................. 1.2.5 Type 1 Diabetes Mellitus ................................
............................... 1.2.6 Type2DiabetesMelliais 1.2.7 Complications ............................................
.................. 1 -2.8 Monitoring Blood Glucose Control ..................... 1 -2.9 Intensive Blood Glucose Control
1.2.10 Treatment ................................................. ........ . 1.2.1 O 1 Non-f harmacological Therapy
.................... 1.2.10.1.1 Exercise 1 .2.10. 1.2 Nutritional Management ..
.......................... 1.2.10.2 Insulin'ïherapy 1.2.10.3 Lispro Insulin ......W.........-...........
.......... 1 -2.10.4 Lispro and Meal composition ................................ 1.2.11 TheGlycemicIndex ............................. 1 -3 Study Objectives and Hypothesis
.................................... 1.3.1 Study objectives .................................... 1.3.2 Study Hpthesis
CHAPTER 2

MATERIALS AND METHODS Subjects ............................................................
............................................. 2.1..1 Screening ..................................... Study Design and Protoc01
............................................. 2.2.1 Rationale ............................................... 2.2.2 Protocol
............................ 2.2.2.1 Hypogiycemia Test Meal Preparation ...........................................
............................... 2.3.1 Instant Mashed Potato .......................................... 2.3.2 White Bread
2.3.3 Spaghetti .............................................. ....................................... 2.3.4 Pearled Barley
............. ................... 2.3.5 . Pineapple Juice ... ........................................ Blood Glucose Analysis
............................................... S t a î i s t i c a l ~ s i s
CHAPTER 3 RESULTS 3.1 Subjects ........................................................... 36 3 -2 Glycemic Response Data ...............................-.....Le 38 3.3 Hypogiycemic Outcomes ....................................... 46
....................................... 3.3.1 Hypoglycemia 50 ................................. 3.3.2 Low B l d Glucose 50
3.3.3 GI and Pg in Relation to Hypoglycemic ............................................. Outcomes
CHAPTER 4. DISCUSSION AND CONCLUSIONS 4.1 Discussion ......................................................... 58 4.2 Potentid Practical Implications ................................ 64 4.3 Future Research ........-........................................... 66 4.4 Conchsions ...................................................... 66
REFERENCES ClTED 68
~Pl?ENDKEs 76

In the name of Allah, the most mercz~l, the most graciour
Fkst and forernost, I would like to thmk my hwband and e v q
member in my family. Without their unconditio~u~l love, patience and
support, I would not have been able tu accornplsh this work
I'm gratefùl d thanml tu my supervisor Dr. Wolèver, for his
continuous encouragement and i m a l ~ ~ ~ b l e guihnce throughout the
program- 1 would also like to thank Dr. Jenkns and Dr. Rao for their valued
input. Bank you fo Dr. Singer for appraising the thesis and Dr. El-Sohemy
for chairing my defense.
1 am irrdebted to al2 my subjects who volunteered to participate in my
stuc&- ïlbanks to everybody in my Zab group, d special t h k to Janet Vogt
for her heIpfu2 advice. Inmks to CZaudio in the Glycemic Index Testing
Offce for hm technical support. Also greati'y appreciated is thefiiendsh* of
everyone ut the Clinical Nuhition and Risk Factor Modzifiation Centre at
St. Miehael's Hospital. A special thmrAyou tu Zènith Xu for her kind heb.
1 would like to extend my thanh to the Faculty of Medicine in Kuwait
University, for ofering thk scholmship.
mis thesis was made possible by a grantfiom Eli Lil& company.

Table 2.1
Table 3.1
Table 3.2
Table 3.3
Table 3.4
Table 3.5
Table 3.6
Table 3.7
LIST OF TABLES
GI, Weigbt and Composition of Test Foods
M- Demographic and Biochemical Profile of the Sample at srreening
Two-Way AnalysiP of Variana ofLncremental Bkxxi Glucose Responses Mer Difllerent Types ofFood
Mean Bbod Ghicose Increments for Food Types vs. Time
Two-Way A d y s k of Variance of Area Under Giy- Curve (AUC) Mer Werent Types of Food
Mean Area Under the Curve (AU0 of the Glycedc Response Curve for Food Types
Number of Hypogiycemk and Low Blood Glucose Episodes per subject

Figure 2-1
Figure 3-1
Figure 3.2
Figure 3.3
Figure 3-4
Figure 3.5
Figure 3 -6
Figure 3.7
LIST OF FIGURES
Tes te Day Protocol
Correlation between Ghicometer a d YS1 Blood Glucose co~~centrations
Mean B W Ghicose Increments (by YSI) For Food Types vs. Time
Mean Blood Ghicose Concentrations (by YSI) For Dïfkent Test Foods
Correhtion Between Mean AUC of Test Foods and Their Glycemic Iodices
No. of Hypoglycemic and Low Bbod Ghrose Episodes per Food Types
Correlation of No. of Hypoglycemic Episodes (by Glucometer a d Y SI) with GI a d Pg
Correlation of No. of Low Bbod Glucose Episodes @y Glucometer and YSI) with GI and Pg

LIST OF APPENDICES
AppendixA Consent Fomi
Appendix C Weight and Nuîrient Content of Standard DBmr Meal
Appendix D Data Fonn
Appendk E Demograpbic and Biocbemical Pro& of the Subjects at s-
Appendk F TllSUlBl Types and Mean Doses Used By Subjects

.................. AD A ANOVA ..........-.. M T .................. AUC ................. BMI .................. CS11 ................. DCCT ....O..........- DM ................... FBG .................
IFG ................... .................... IGT
L ....................... LDL
SBGM ............O.-.. SEM ....................
...................... U YS1 ...................
The Americaa Diabetes Association Analysis of Variance AhnmeTransarninase Area Undet Giycemic Response Curve BodyMassIndex Coiitinuous Subcutaneous IrisulEnmn Diabetes Control and Complication Trial Diabetes Mellitus Fasting Blood G b s e Granis GestatiodDiabetes Giycemic Index Hours Hemogiobh Alc ImpairedFastmgGhicose Ingiiired Ghicose Tokrance -gram Litre hw-Densii Lipopmtem Mü1snole per Litre Propoen of carbohydnie absorbed as ghmse Correlationcoefficient SelfBbod Glucose Monitoring Standard Error of the Mean units Yellow Spring Instruments Adyzer

Effect of Carbohydrate Source on Postprandial Glycemia in Type 1 Diabetic Subjects Treated with
Lispro Insulin.
Master of Science, 2001 Nadia HJ. Mohammed
Graduate Department of Nutritional Sciences University of Toronto
ABSTRACT
Treatment o f type 1 diabetes (TID) with iispro h s u h reduces postprsndial
hyperglycemia, but because of its rapid onset of action, postprandial hypoglycemia may
occur. To see ifgiycemic index (GI) and proportion of carbohyârate absorbed as *se
(Pg) affecteci g iym-c responses and occurrence of hypogiycemia, 8 T1D subjects on
lispro were studied for 4 h on 5 &ys af€er o v ~ g h t fàsts. Subjects took their usual
insulin dose and ate 50g carbohydrate tiom a starchy food (Pg=I; instant potato G1=83,
white bread GI=71, spaghetti G P U , barley GI=ZS) or pineapple juice (Pg=0.5; 01-46).
Glycemic responses differed significantiy for the diffèrent foods and were close&
rehted to GI ( d . 9 8 , p<O.Ol). Hypogiycemia was more muent 0 . 0 5 ) for foods with
low Pg, while time to hypoglycernia was shortet with Iower GI.
In conclusion, GI predids glycemic responses of foods in T l D subjects ushg
lispro. Pg affects the occurrence of hypoglycerrria whüe GI afkcts its timing.

1. INTRODUCTION AND LITERATURE REViEW
1.1 INTRODUCTION
The therapeutic importance of tight blood glucose control is well
established in both type 1 (1) and type 2 (2) diabetes. G d blood glucose
control for people with type 1 diabetes depends on coordination of insulin
doses, quantity and timing of food intake, and physical activity.
The Arnerican Diabetes ASSOC-iation (ADA) recommends considering
total carbohydrate consumed rather than type of carbohydrae, thus \
traditionally ins& dose has been adjusted based on the amount of
carbohydrate in the mealS. However, meals may differ not only in the
amount of carbohydrate they contain, but also in the source. The Glycemic
Index (GI) is a classification of foods based on their relative blood glucose
raising potential(3), which in tum depends on the rate at which carbohydrate
is digested and absorbed (4). Oiir lab.has demonstrated that the GI of foods
is the same for people regardes oftheir glucose tderance (5). We have also
shown that lowering the GI of the diet improves b l d glucose control in
both type l(6) and type 2 (7) diabetes. More recently we have demonstrated
that day-to-day variation in both the amount of carbohydrate and the GI of
the diet of subjects with type 1 diabetes influences the glycemic control(8).
1

This suggests that to achieve optimal diabetic controi, adjwtment of insulin
dose should be based on both the amount and source of carbohydrate in the
meal to be consumed.
Recently, an analog of human insulin, lispro, is increashgly used
because of its more rapid and physiologie response. This results in reduced
postprandial blood glucose compared to reguiar bulin (9) and the potentid
for improved blood glucose control(10). However there is the potentiai for
postprandial hypoglycemia especially when a low carbohydrate meal is
consumed (11). This Mcates that the dose of lispro needed depends on the
amount of carbohydrate present in the meal. However, the= are no studies
yet on how to adjust lispro for dzerent types of carbohydrate foods.
The general purpose of the present study is to determine the pattein of
blood glucose response produced by an equivalent amount of different
carbohydrate f d s in type 1 diabetic subjects ushg insulin lispro, and to
determine the influence of carbohydrate source on lispro-induced
postprandial hypoglycemia The overall aim is to be able to advise diabetic
people whether to adjust lispro dose for different types of carbohydrate for
optimal glycernic control

1.2 LITRATURE REVIEW
1.2.1 Definition of Diabetes Mefitus
Diabetes Mellitus is defhed as a heterogeneous group of metabolic
diseases characterized by the presence of hyperglycemia due to defective
iasulin secretion, insulin action, or both.
1.2.2 Prevalence
Currently, diabetes has been diagnosed in 5% of Canadians or 1.5
million people (12). This number was expected to reach 2.2 million by the
year 2000 and 3 million by 2010 (13). Moreover, because U.S statistics
demonstrated that for every person with diabetes there is someone with
undiagnosed diabetes, these numbers most likely underestimate the
prevalence of the disease. Assumùig that the same situation is tme in
Canada, up to 10% of Canadian adults may currently have diabetes.
1 -2.3 classincation
Diabetes is recently reclassified into five distinct types based on the
pathogenesis rather than treatment (14). The vast majority of cases f d into
two broad categories, which are type 1 a d type 2 DM (discussed later).

Gestational diabetes (GDM) is any degree of glucose intolerance that is
recognized during pregnancy.
A variety of relatively uncornmon conditions are listed under "other
specifïc îypes". These consist mainly of specifïc genetically defïned fonns of
diabetes (e.g. abnormalities of insulin or its teceptor) or diabetes associated
with other diseases or drug use.
Impaired glucose tolerance (IGT) and mipaired fasting glucose (IFG)
are metabolic stages interniediate between
established diabetes. They are mt clinical
are risk factors for Miire development
disease.
nomal glucose homeostasis and
entities in their own rather they
of diabetes and cardiovascular
1.2.4 Diagnosis
The Diagnosis (14) of diabetes is established by a fasting plasma
glucose (FPG) value equal to or greater than 7.0 mmol L, a random plasma
glucose greater than 11.0 m V L with symptom, or plasma glucose value
in the 2-h sample of the oral glucose test (75g - glucose load) greater than
11 .O mmoVL.
Diagnosis of IGT depends on a plasma glucose value in the 2-h sample
of the oral glucose test (75g - glucose load) between 7.8-1 1.0.

Impaired fasting glucose (WG) has been established to iden* another
intermediate stage of abnomal glucose homeostasis analogous to IGT. IFG
is diagnosed by a fasthg plasma glucose value between 6.169.
1.2.5 Type 1 Diabetes MeIlitus
Type 1 DM commonly occurs in childhood and adolescence, thus is
also known as Iwenile-onset diabetes. It represents about 5-10% of all cases
of diabetes. It results fiom absolute deficiency of insulin secretion due to
destruction of the B-cells of the pancreas, the etiology of which is either an
autoimmune cell mediated or idiopathic.
1.2.6 Type 2 Diabetes Mefitus
Type 2 DM is the cornmonest type of diabetes. Approximately 3% to
5% of the general adult population has unrecognized type 2 diabetes. It may
range ftom predominant insulin resistance with relative insulin deficiency to
a predominant secretory defect with insuliÙ resistaiace. Studies have
identified increased risk associated with older age, central obesity, certain
ethnic back grounâ, physical inactivity, hïstory of GDM, overt
cardiovascular disease, high fasting insulin levets, and IGT (1 5,16,17).

1.2.7 Complications
Diabetes is a serious M.th problem associated with acute and chronic
complications. It often disables people in their middle years and as a group,
people with diabetes die younger than those not affited by it (18).
Major acute complications are hpglycemia and hyperglycemic crises
including ketoacidosis and hyperglycemic-hypemsmolar states.
The chronic hyperglycemia of diabetes is associated with long term
macro and microvascualr disease causiag damage, dysfunction, and
ultimately failure of various vital or- especially the kidney, eye, nerves,
heart and biood vessels,
Diabetes (both type 1 & type 2) is a major cause of coro- artery
disease, which is the leading cause of death in Canada. Morbidity and
mortaliîy rates are 2-to4fold higher than in age-and sex-matched groups in
the non-diabetic population (19,20,21,22,23) it is &O a leading cause ofnew
cases of blindness and kidney disease in adults.
1.2.8 Monitoring Blood Glucose Control
Daily Self Blood Glucose Monitoring (SBGM) has markedly improved
the ability to acutely control blood glucose levels. It permits recognition of
low levels of blood glucose before hypoglycernia occurs (24,25) and allows

people to assess the effècts of diet, exercise and changes in treatment
regimens.
People with type 1 diabetes often use pre-meal and bed time tests, as
well as intermittent ps t meal testing to adjust insulin doses. Testing for
glycated hemoglobin, as it refleck average blood glucose levels of
approximately the previous three months, should be pe150-d penodically
to assess long-term glucose control (26). A specific type of glycated
hemoglobin, HbAlc, is a tool for assessrnent of the preceding 6 8 weeks
(27)-
1.2.9 Intensive Blood Glucose Control
Epidemiological studies and studies done in animal models of diabetes
implicate hyperglycemia in the pathogenesis of long-terni complications of
diabetes. Consequently the aim of diabetes management is to maintain the
glycernic status as close to the no& range as safey possible.
Intensive insulin therapy was applied in the Diabetes Control and
Complication Triai @CCT) by multiple daily insulin injections administered
as basal insulin with short-acting bolus insulin (basal-bolus) adjusted
according to SBGM, meal composition and level of physical activity.
Continuous subcutaneous insuiin infusion (CSII) using a pump is an
alternative to multiple daily injections. DCCT achieved inipmved b l d

glucose control, which in turn effectvely delayed the omet and slowed the
progression of diabetic complications (1).
1 -2. 1 O Treatment
The primaty goal of therapy is to avoid acute & long-terrn
complications. In addition, the person's quality of life & overd sense of
weU-being should be considered. Depending on the type of diabetes and the
therapy required, this objective may be more or less dSicult to achieve
without acute adverse effkcts. Thus treatment must be tailored individilally
based on medical & social factors. If medication is required to achieve
diabetic controI, it should be optimized with regular physical activity and
healthy eating.
Since my thesis is about people with type 1 diabetes, I'Il d y focus
on them in my discussion.
1.2.1 O. 1 ~ o n - ~ h ~ c 0 1 0 g i c a l Therapy
While insulin therapy is essentid for M e in people with type 1
diabetes, it should be optimized with regular physical activity and
nutritionally adequate food intake.

An active He style pmmotes cardiovascular fitness and well being
(28). However the net effect of exercise on glycemic control is unpredictable *
and varies among individu& with type 1 diabetes because many variables
innuence glucose supply and utilkation. These include the state of nutrition
and metabolic control before and at the onset of the exercise, duration and
intensity of exercise, fitness of the patient, type, dose and site of insulin
inj ec tion (29).
In general, low to moderate intensity exercise lowers glucose levels
both during and d e r the activity, inc~iea~ing the risk of hypoglycemic
episode. Conversely, intense exercise raises glucose levels and can lead to
progressive hypergIycemia and even ketosis. Accordingly, physical activity
may require the adjustment of insulin and carbohydrate intake both before
and after the activity to prevent exercise-induced hypoglycemia In addition,
fiequent blood glucose monitoring should aid any adjetment. Obviously,
intensive diabetes management plus SBGM provide flexibility in
appropriately modi@ing insulin for exercise (343 1).
The advantages of increased activity levels must be balanced against
the risks due to diabetic complications or other medical conditions; thus,
plans for physical activity should be individuaiized.

1 -2.1 0. 1 -2 Nutritional Management
As fàr as nutrition is concerned, it should contribute through dietary
recommendations to irnprove glycemic control and avoid short-term
symptoms fkom hypoglycemia and hypergiycemia.
In Canada, dietary recommendations for people with diabetes are the
same as those for the gewral population, k d follow the principles of
Canada's guideliws for healthy eating (32). ControUed fat intake for the
prevention of cardiovascuiar diseases is the underlyhg principle of the
recommendations. For adults with normal lipid levels and reasonable weight,
the guidelines reconimend daily fat intake not to exceed 30% of total da@
energy requirements, where sahirated and poly-msaturated fats each not
exceeding IO%, with the remainder coming h m mono-unsahirated fat (33).
Protein intake, preferably fiom vegetable sources, should range fiom 10-
20% of total energy with daily intake of about 0.86glKg, which is similar to
that of the general population. The remainder 50-60% of the individual's
energy requirements should corne fiom dietary carbohydrates, especiaiiy
those . unrefined, slowly absorbed, and rich in soluble fibers (33).
On the other band, the ADA nutrition recommendations stress
individualkation of diet based on the patient Westyle, and the results of
clhical monitoring. It is recontmended that proteins, saturated ht, a d poly-

unsaturated fat contribute a total of 30=4û% of daiiy ewrgy intake, and the
remainllig 60-70% to come h m a combination of carbohydrates and mono-
unsahuated fats (34). Daily fiber intake of at least 25-35gld is reconmiended.
Soluble fiber intake has been associated with reduced blood glucose
responses, and improved blood glucose control(35)
Several health agencies recornmend an h a s e of low-GI foods in the
diets of individuals with diabetes (36,37,38). However, the ADA has
questioned the clinical utility of the GI and recommends tbat priority should
be given to the amount rather than the source of carbohydrate (39). ,
On the contrary, Jenkins focused on the concept of 'spreading the
nutrient load'. He suggested 4 factors that prolong the time of nutrient
absorption fiom the gut, understanding of which is helpful in the dietary
management of both diabetes and hyperlipidemïa. These are increased food
fiequency (nibbling), viscous soluble fibers, low GI foods, and enzyme
~ ï i t o r s of absorption (34). He added that m y higbfiber f d s that lower
LDL cholesterol also have low glycemic indices, such as bkley, beans, etc.
Therefore, exp1oration of low-GI f d s might be used to expand, rather than
limit, the carbohydrate food choices of people with diabetes.

1.2.10.2 Insulùi Therapy
Classically insuJin pfeparations can be classified according to theii
time of omet and duration. In ascending order, these include short acting
(Regular), intermediate acting W H , Lente) and long acting (Ultralente).
Intermediate and long acting insuiin injecti011~ provide appropriate basal
circulating insulin concentrations overnight and between meals. Pre-meal
bolus injections of short acting are given to prevent an excessive rise in
postprandial blood glucose immediately after meals (40).
Combinations of these insulins can be given in a variety of protocols.
In the split-mixed protocol, mixture of short and longer acting msulni is
administered twice a day, before breakEast and dirmer. Altematively, in the
basal-bolus protocol, also known as multiple daily injections, short-acting
insulin is given before each m e 4 while N'PH or Ultralente injections
provide basai requirements (4 1).
The available short acting insulin preparations have vatious
shortcomhgs. The most evident is a delayed omet of action and
uiappropriately long duration of action. Studies indicate that the peak effect
of Regular insulin occurs h m 2 to 6 heurs d e r injection, and its effect may
last as long as 16 hours (42). In addition, it was f o d diat Reguiar insulin

should be given fiom 30 to 60 minides before d s to achieve optimal
control of postpraadial glucose (43).
This is fàr tlom normal physiology where endogenous, pancreatic
insului secretion is stimulated irnmediately after blood glucose concentration
begins to rise following food ingestion, so that insulin concentration peaks
fat around 60 minutes postprandial, then declines over 3 hours to reach a
basefine level.
This departine in the pharmacokinetics of Regular insulin ftom normai
pancreatic insului springs fiom the fact that injecteci human insulin must be
in a mommeric fom before it c m be absorbed through the capillary
membrane into circulation. However, the himian insulin molecule has a high
tendency for seKassociation (44). When Regular insuiin solution is stored in
vials or cartridges, insulin molecules are in a polymeric, mostly hexameric
form to maintain stability. The dissociation rate into monomeric molecules is
low at the injection site, hence the delay in peak insulin concentration and
activity after subcutaneous injection (45). The end of the insulin B chain
(specifically Proline at position B28) is the site responsible for the self-
association of insului molecules.
Recently, bul in analogues have been developed which overcome
many of these problems. They are very rapiidly absorbed so that their onset

and peak action are closer to the injection time, which matches more closely
the postprandial glucose excursion (46).
1.2.10.3 Lispro Insulin
[LYS (B28), Pro (B29)I-h~man msulin (Lyspro or Lispro (Humalog)) is
an insulin analog in which the natucal amino acid sequence of the Bchain at
position 28 and 29 is inverted. These changes result in reduced capacity for
self-association (47), and account for the monomeric behaviour of Lispro in
solution (48), and for the faster phannacodynarnic action than Regular
insulin when injected subcutaneously (49).
Lispro insulin beguis to work within 15 minutes after subcutaneous
injection, peaks in about one hour, and has duration of 2 to 4 hours.
Compared to Reguiar insulin, Lispro insulin has a %ter absorption and a
more rapid elimination, effectively produchg a shorter duration of action,
which may offer an advantage over Reguiar insulin in the control of blood
glucose after meals (49).
Studies addressing mealtime glycemic control using Lispro iniifody
indicate that the postprandial rise in blood glucose is signiscantly lower,
approximately 1 to 4 ~ l l t l ~ V L , than with human Regular insulin (50,5 1) .The
best postprandial contml was obtained with an injection immediately before

the meal. Even if Lispro is injected shortly after the meal, the postprandial
glycemia is still well controlied (52,53).
The long-tem dycemic control as reflected by an improvement in the
HbAlc level is better with insulin Lispro than with human Regular insulin
(54), provided tbat an appropriate basal insuiin regimen is used to take into
account its shorter diwtion of action (55).
In type 1 diabetic patients, the hypoglycemia rate was found to be 12%
iower (particularly at night tirne) during treatment with Lispro compared to
Regular insulin (56). In addition, rate of severe hypoglycemia (defïned as
coma or requiruig glucagons or IV glucose), can be reduced by 30% with
insulin Lispro (57).
1.2.10.4 Lispro and Meal Composition
M. BU& (58) demonstrated the importance of meal composition in
relation to lispro-induced Post-prandial hypoglycemia. He used isocaloric
meals with different carbohydrate content. His expriment revealed that pre-
prandial lispro has tendency for Post-prandial hypogiycemia in the setting of
reduced carbohydrate iotake. This is consistent with other studies showing
that amount of carbhydraate in individual f d s inauences postprandial

blood glucose response (59). The author concluded that lispro dose need to
be adjusted depending on meal composition to avoid hypoglycemia
On the other han& M. Strachan (11) examined the effect of meal
composition on postprandial glycemia to establish optimal time for lispro
administration. He assumed that because meal composition affects rate of
gastric emptying (60,61) which in tum affects timing of post-prandial blood
glucose rise (62), meal composition has to be considered when timing of
lispro administration is adjusted. So he concluded that for meals with high
carbohydrate content, the optimal time for lispro administration is pre-
prandial. However, for meals with hi& fàt content, pst-prandial
administration is preferred to minsnize risk of pst-prandial hypogiycemia.
A group of patients with type 1 diabetes on Lispro insulin mêet
regularly at the Clinical Nutrition Center at St. Mchael's Hospital, Toronto,
Ontario. They have reported that a h consuming some foods but not others
(e.g. spaghetti, beans) thei. blood glucose &op initially, followed by 'a late
rise (Wolever TMS, personai communication). Both beans and spaghetti are
low-glycemic index f d s that are digested and absorbed slowly resulting in
delayed pst-prandial blood glucose rise. So probably in case of low-GI
carbohydrates, the blood glucose lowering action of iispro precedes the
absorption of carbohydrate resulthg in ~vch desirable pattern of blood

glucose response. Numerous studies have shown that pst-prandial blood
glucose and insulin responses are intluenced by both the amount of
carbohydrate consumed and its source (Brand et al. 1985, Jenkins et al.
1985, Wolever et al. 1996 and others). SO, ifcarbohydrate f d s differing in
terms of GI, nature, proportion of carbohydrate absorbed as glucose (Pg),
etc. produce significantly different blood glucose responses, then alteration
in either the dose andor timing of lispro administration may allow people
with type 1 diabetes to achieve more acceptable pattern of blood glucose and
reduce the risk of pst prandial hpglycemia.
1.2.1 1 The Glycemic Index
Systematic classification of f d s according to their glycemic
responses was first undertaken by Otto and Nüdas (3) in an attempt to
incorporate foods into diabetic diets in amounts inversely proportional to
their glycemic responses. The glycemic Index (GI) was developed
independently as ranking of foods based on theu postprandial blood glucose
responses compared with a reference food. More precisely, it is deîined as
the incremental area under the glucose ciirve of a 50g carbohydrate portion
of a test food divided by the incremental area under the glucose c w e of a
50g carbohydrate portion of a standard reference food (white bread) and
17

multiplied by 100 (3). Several methods have been used to calculate the area
under the glycemic-response cunre (63) and resuit in markedly different
areas and GI values (3). Woiever and Jenkllis use the incremental area for
calculations, where the area below the b a s e k glucose value is not inchded
in the calculation (64). Area d e r the cuve (AUC) is calculated by using
what has corne to be known as the 'the trapezoidal de ' . This calculation for
AUC is well described in the literature (3). In 1981 Jenkms et al (65)
published the fht lid of GI vahies for 62 f d s .
Studies have shown that both the amount and source of carbohydrate
innuence the acute blood glucose response to meah in normal (59), type
2(66) and type 1(67,68) diabetic subjects. Furthemore, Wolever et al have
shown that in type I diabetes, coasistency in both the amount and GI of
dietary carbohydrate is associated with ùnproved blood glucose control
indicated by H b ~ l c (8). This supports adherence to a consistent diabetic diet
plan. However, people with diabetes regard following a strict diet a burden.
Liberalization of the diet is an alternatik that is suggested to relieve tbis
bwden without adverse effects on glycemic control. To achieve optimal
glycemic control with a Ii'beralized diet, education about adjusting insulin for
both the amount and the GI of dietary carbohydrate is needed. This is
consistent with a study showing that unlike in type 2 diabetes, blood glucose

control in subjects with type 1 diabetes was not related to the composition of
the diet in te- of diet GI and amount of Carbohydrate and fiber intake (69).
This suggest that as long as insulin dose is adjusted to reflect food intake, the
composition of the diet may not be important for optimizing glycemic
control. This fact mostly applies to diabetics on intensive insulin treatment.
Although it is generally agreed that different carbohydrate f d s have
different glycemic effects, controversy exist about the therapeutic
implications of this information for diabetes. High carbohydrate diets are
recommended for individuais with diabetes and hyperlipidemia but the type
of carbohydrate is likely to be important in determinùlg the metabolic
response to such diets. Increasing carbohydrate intake with high GI f d s
may increase blood glucose, insulin, and triglycerides concentrati0~1~ (70).
However, increasing carbohydrate intake with low GI starchy f d s may
allow carbohydrate intake to be increased witbut these unwanted effects. In
long-term trials, low GI diets with no change in dietary fiber content result
in modest but signincatlt improvements in overall blood glucose control in
patients with type 1 diabetes as measured by glycated hemoglobin (6).
Perhaps of greater therapeutic importance is the abiüty of low GI diets to
reduce insului secretion and lower blood lipid concentration in patients with

hypertriglyceridemia (3). h o , low GI starchy foods improved glycemic
control and lowered sennn cholestero1 m type 1 diabetic children (71).
1.3 STUDY OBJECTIVES AND HYPOTHESIS
1.3.1 Study Objectives
1.3.1.1 To detemine the pattern of b l d glucose response for equivalent
a m t of carbohydrate foods with different Glycemic Index values d e r a
standard dose of lispro in type 1 diabetic subjects.
1.3.1.2 To determine how equivalent amount of carbohydrate f d s with
different Glycemic Index values idluence the pst-prandial hypoglycemia
induced by Lispro.
1 -3 -2 Study Hypothesis
1.3.2.1 Significantly different blood glucose responses will be elicited by
equivalent amounts of carbohydrate fiom different sources with different
Glycemic Index values in subjects taking a standard dose of lispro.
1.3.2.2 Postprandiai hypoglycemia will be elicited by lispro in subjects
taking equivalent mmunts of carbohydrate h m different sources more
fiequently with foods baving lower Glycemic Index a d lower Proportion of
carbohybte absorbed as glucose.

2. MATERIALS AND METBODS
2.1 SrnJECTS
Volunteers were recniited by study invitation posters distributecl in
Endocrinology clinics in 6 major hospitals in Greater Toronto area and in
Clinical Nutrition Centre at St. Michael's hospital, and by 3-day newspaper
advertisement on three occasions.
Recruiûnent period lasted 10 months between Feb 2000-Nov 2000,
during which subjects were tespondhg sporadically and not in groups.
A lecture was given to nurses and dietitians working in Clinical
Nutrition Centre explainhg the purpose and procedures of the study and
subject criteria to heQ in recruitment process.
A totd of 17 people were screened, 14 were eligible according to our
study criteria, and 11 of these were recniited. They were 8 femaie and 3
male subjects. Three female subjects withdrew d e r 1-2 test sessions for
personal reasons. So a total of 8 subjects each successfully completed the
whole 5 tests. Each subject needed a period of 5-8 weeks to complete the
study.

2.1.1 Screening
Subjects were interviewed pria to study commencement in the
screening session to assess suitability for participation. EligibIe subjects
were male or non-pregnant females, 14-75 years of age, with type 1 diabetes
who intensively seKmanaged their diabetes using lispro insulin for at least 3
months, the dose of which was adjusted based on the amount of
carbohydrate in the meal. Usual fasthg blood glucose had to be between 4
and 16.7 mmoVL, and HbAlc lower than or equal9.1%. Other inclusion and
exclusion criteria are listed below:
Inclusion criteria:
14-75yrswithtype 1DM
On insulin lispro for at l e s t 3 months
Male or non-pregnant females
Moderate to good glycemic control WAlc 1 9.1%; normal 4.5- 5.8%).
Usual fasting blood glucose between 4 and 16.7 mmoYL
Willllig and able to coiriply with shdy protoc01 and give U i f o d consent.

Exclusion criteria:
a History of severe hypogiycaemia (needs assisame of amther person)
more than once withh the last 3 monthS.
a Use of dnigs other than insulin that affect carbohydnte metabohm
(e.g. oral hypoglycemic agents, steroids). Use of stable doses of beta-
blockers or thiazide diuretics for the treatment of hypertension is
dowed.
Symptomatic gastroparesis or other gastrointeshl condition
affecthg digestion or absorption of nutrients.
a Use of drugs afEecting gastrointestinal motility or nutrient digestion or
absorption.
a Surgery, infection or signincant cardiovascular event within the last 3
months.
a Liver disease; severe rend failure or r d dialysis.
History of HIV infection or hepatitis.
Substance abuse.
Females already ptegnant or intendhg to become pregtiant driring the
study, or sexuaily active with childbearbg potential not ushg birth
control methods.

+ Lactating females less than 6 months after delïvery.
4 Participation in another medical, surjgical or pharmaceutical
investigation.
Any other physical, mental or behavioral condition that may make
participation of the subject dangerous to the subject's health or that of
others, or affect the results obtained.
In the screening session subjects came fasting to Clinical Nutrition
Centre at St. Mchael's Hospital. The study protocol was described and
queries of the subjects were answered. Also they were given instructions
about the standard dimer and snack for the night of the test. Then subjects
who were willing to participate signed on a consent fonn (Appendix A) and
were asked to give a fasthg bblood sample for biochemical analysis of blood
glucose, iipids, HbAlc, AST, creatinine and ma. A snack was given after
blood collection.
Mernards they answered a questionnaire about their medical history
and home blood test results (Appendix B), their height and weight were
measured and before they leave they were provided with the standard d i r
for the f h t test.

2.2 STUDY DESIGN AND PROTOCOL
SLMichael's Hospital Research Ethics Board approved the shidy
protocol. The study had a randombed, cross-over design.
Eligible subjects came to Glycemic Index Testing Office (55 Queen
St. East, 2d floor) on five occasions at weekly intends in the moming
between 8:O and 8 3 0 am after 10 to 12 buis ovemight h t for a 4%hom
test (testing day protocol, Figure. 2.1). In each test day they were studied
with one of the following 5 test foods: instant mashed potato, white bread,
spaghetti, pearled barely and pineapple juice, each containing 50g glycemic
carbohydrate.
2.2.1 Rationale
The rationale for choosing the above test f d s was to study 4 starchy
carbohydrates with a 3-fold Merence in terms of their GIS to elicit blood
glucose responses over a-wïde range. Pineapple juice was included because
the carbohydrate it contaùis consist of sugars (sucrose, glucose, and
hctose) that overall elicit a dwerent glycemic profile. These foods also
m e r in the proportion of carbohydrate absorbed as glucose (Pg). Starchy
foods have a Pg = 1 because they are totally absorbed as giucose, while

& =-s-ri. FBG = Fasting Blood Glucose
Figure 2.1 Testing Day Protocol

pineapple juice bas a Pg = 0.5 because sucrose is absorbed as half glucose
and half hctose (72).
2.2.2 Protocol
For dinner and snack (if n o d y coasumed) on the evening before
each test day, they consumed a standard meal that was provided, and nothing
else except for water. This meai consisted of a number of Choice Bars
(Mead Johnson) and a- c m of Ensure F o d a (Ross, Abbott Laboratones),
which is similar in ewrgy and carbohydrate content to their normal dinner
(Appendix C: Weight and nutrient content of standard dinner). If the subject
had to break his overnight fbt due to hypoglycemia, the test was cancelled
and rescheduled for amther day.
Upon arriva1 on the moming of the test, the subject was weighed and a
fasthg hger-prick capiiIary blood sample was obtained with Autolet
lancets. If blood glucose was less than 4 or more than 16.7, then the test was
cancelled for that day, and was rescheduled for another day. If blood glucose
was in the above range, the test was carried out and the subject took the dose
of insulin lispro that he or she would normally take before eating 50g of
carbohydrates.-For each subject, the same dose of lispro was repeated at the
same tirne (before the start of the test meal) on each of the test days.

Within few (2-7) minutes d e r lispro administration, the subject started
to eat a test meal containhg 50g available carbohydtate h m a standard
portion of instant potato, white bread, spaghetti, pineapple juice or pearled
bdey (GI, weight, and composition of test meals shown on Table 2.1). Test
meals were fed to subjects in random order.
Test meals were served with 250 ml water or tea (up to 50ml2% d k
and 2 bags of non-nutrient sweetener are allowed if desired). The drink
chosen remained the same for each subject for all subsequent tests. Test
me& had to be consumed withh 10 min. Additional finger-prick samples
were obtained haKhourly for 4 ho= after the start of the test meal
(Appendix D: Data Form). Each capillary blood sample was split into 2
aliquots; 3 drops of blood was saved in fluorocitrate tubes for subsequent
glucose analysis using a YS1 glucose analyzer. Results of which used for
study analysis. An additional drop was used for immediate analysis by
glucorneter (Precision TM, Abbott Laboratories, Columbus, -OH). The
glucorneter resdts were used to cietennine eligi'bility of f&hg blood
glucose, for subject safety, and for analysis of hypogiycemic outcornes.
During the test, subjects were expected to remain seated and they were
not pennitted to smoke. M e r the test was over, a snack or lunch meal was
provided if desired.

Table 2.1
GI, Weight and Composition of Test Foods
Weight
Moisture
Total Fat
Total carbohydrate
Available carbohYdrateB
Instant White Pineapple spaghettir P emled potato' 13readt ~uice # ~ a r l e y ~
83 71 46 41 25
67.3 67** 373 72.3 79.6
6.1 9.1 1.5 11.1 8.4
4.5 NIA N/A 7.2 7.6
0.6 0.4 0.4 1.6 1.5
1.9 NIA NIA 0.5 1 .O
4.2 2.1 O 2.0 11.2
Weight and composition in grams.
Portion size and nutrient composition baçed on a d y s k (TMS Wolever). * Portion size and nutrient composition based on food tables. * GI values nom literature (Foster-Powell K et al 1995) ** Weight of fiou.. * Available carbohydrate = total carbohydrate (by difference) -total dietsry nkr.

To minnnize withh- subject variation, data were only included for
tests when the subject's fastmg plasma glucose on the study days varied by
no more than 6 mmoVL. Tests outside this range were repeated.
2.2 -2.1 Hypoglycemia
According to our protocol, hpglycemia was recorded if blood
glucose dropped below 3.0 mmoi/L at the time of blood s a m p b based on
the glucometer or the YS1 analyzer retrospectively, or if at any time the
subject experienced imtohbIe symptoms of hypoglycexnia. At this point the
test was terminated and depending on the severity of hmycaemia, subject
was treated with oral dextrose, *ose Tablets or simp1y H cup of juice and
something to eat if required. Then blood glucose was monitored until it was
recovered-
Time to hypoglycemia was recorded exactly as minutes at which
hypoglycemia (based on glucorneter-or symptoms) occurred nom the start of
the test food or retrogradely as discovered by YS1 blood d y z e r .
The occurrence of 'low'blood glucose was defined as a reaâing less
than 4.0 mmoVL by glucometer or YS1 anaiyzer.

2.3 TEST MEAL PREPARATION
Portion sizes of white bread, potato, spaghetti, and barley were
determined based on d y s i s of moisture, ash, protein, fat and total dietary
fiber with available carbohydrate calculated by diffe~ence (Wolever TMS).
Portion size of pineapple juice was determined based on food Tables.
2.3.1 Instant Mashed Potato:
2 5 W boilùig water and '/z tbs salt was added to 67.3g of potato,
stirred mtil unifody hydrated. It was pqared just before servïng.
2.3 -2 White Bread
White bread was baked in 525g loaves containhg 250g carbohydrates.
250g of warm water was mixed with 334g of d-purpose flour (Robin hood),
7g sucrose, 6.5g Quick Rise Instant Yeast, and 4g of salt. The ingredients
were placed into an automatic bread d e r (BlackBcDecker) according to
instructions and mixed, kneaded and baked over a 2-hour p e n d Loaves
were cooled at room temperature for 1 hr and weighed. C ~ s t ends were
sliced off and discarded. The remainder of the loaf was cut into 105g
portions contalliing 50g carbohydrate, packed into plastic freezer bags and
fiozen. Prior to consumption, bread was thawed in microwave oven.

2.3.3 Spaghetti
72.30 of plain spaghetti (No Name Spaghetti) was boiled in a covered
pot in about 175ml-salted water for 15 min mtil all water was absorbed. It
was prepared the nigM before the test, kept in ikidge and micro waved before
consumption.
2 -3 -4 Pearled Barley
79.6 g of pearled barley m. Goudas) wai boiled in a covered pot in
about 250ml-sdted water for about 2(hnin until aU water was absorbed. It
was prepared the night before the test, kept io fiidge and micro waved before
c onsumption.
2.3.5 Pineapple Juice
373 g of unsweetened pineapple juice (Dole), (approximately 1%
cups), was served after reiiigeration.
2.4 BLOOD GLUCOSE ANALYSIS
Blood giucose measurements were obtained ushg an automatic
glucose analyzer (Yellow Springs Instruments YS1 Myzer) , which &es
the glucose oxidase technique (73). A standard glucose solution (10mmoVL)
was used to calibrate the equipment. Ali the saniples were andyzed ody
after the reading of the standard solution gave values in the range of 9.8-10.2

mmoVL. This standard was run before each set of samples belonging to a
single test meal of each subject.
When D-glucose in blood sample makes contact wÏth the immobilized
enzyme glucose oxidase, it is rapidly oxidized pduciog hydrogen peroxide
(H202). The H G is, in turn, oxidized at the platinum d e , producing
electrons. Thus, a dynamic equilibrium is achieved when the rate of H202
production and the rate at which it leaves the immobiîized emyme layer are
equivalent and is indicated by a steady state tesponse. The electron flow is
linearIy proportional to the to the steady state of H202 concentration and
therefore, also to the concentration of glucose (74).
As with direct oxygen measurement, whole blood or hemolysed blood
interferes with methods rneasuritlg H202 directly. This problem is
circumvented with the YS1 analyzer by enclosing the enzyme in a semi
permeable polycarbonate envelope. This allows measurement in whole
blood, senmi or plasma

2.5 STATXSTICAL ANALYSIS
Lotus 123 97-dtion database software was used. Results were
expressed as means +/- SEM. Mean incremental areas mder the glucose
curves, ignoring any areas below the fast& level were calculated (3).
The GI for each test food was calculated for each subject using the
incrementd area under glycemic response cinve for 50 g of carbohydrate
fiom that test food and expressed as a percentage of the response to 50 g of
carbohydrate f?om white bread. Calculated GI values were divided by 1.4 to
be expressed by glucose scale (GI of glucose = 100). AUC of white bread
for one of the subjects was zero, and therefore food GIS pertaining to his
tests could not be calculated. As a result, these were omitted fkom the
calculation of mean GIS of foods, and n was considered to be 7 rather than 8.
Mean blood glucose increments and mean areas mder the glucose
response curve for food types were compared ushg two-way analysis of
variance. The Newman-Keuls method was used to adjust for multiple
~~mparisons.
Hypoglycemia and low blood glucose happened kquently based on
both glucorneter and YS1 ivralyzer. Least squares linear regression analysis
was perfonned to evaluate how hypoglycemia, low blood glucose, and time
to hypoglycemia correlate with several independent fktors such as

fkequency at which subject went hypogLycemic/low, kting blood glucose
concentration, food GI, and food Pg. Multiple regression d y s i s was a h
perfiormed to evaluate the correlation between hyjmglycemic outcomes; time
to hpgiycemia; and low blood giucose, aed the abve fàctom when
combined. Differences were considered statistically significant when p
<0.05.

3. RESULTS
3.1 SUBJECTS
8 subjects, 3 males and 5 females, each completed 5 test sessions.
Their age ranged between 14 and 74, with a mean of 36.75 years. Mean
duration of diabetes was 13 years, with a range of 2-32 yem. They were on
insulin Lispro for at least 3 months, with HbAlc raaging between 0.05 and
0.087. Main subject description is summarized in Table 3.1 (fully detarled in
appendix E).
All 8 subjects were using lispro and human insulin in a multiple
injection (basal-bolus) regimen. Seven subjects were treated with
intermediate acting insulin to provide basal needs. Two of these were on
Lente Uisuiin and five were on NPH insulin (3 taking it twice daily, 2 ody in
the evening). The remahhg 1 subject was on continuous subcutaneous
insulin infusion (CSII by pump releasing lispro at a basal rate of 1.2 Uh).
The mean of their total evening insulin dose was 15.9 f 4.5 U (range 6 to 44
U). The mean of their total monhg dose was 8.6 f 2.7 U (range 6 to 44 U).
The mean of their total lispro bolus intake was 8.3 f 2.5 U (range 2.6 to 24)
for the evening and 6.6 f 2.7 U (range 2 to 25) for the moniing. Appendix F
describes the insulin treatment of the subjects.

Table 3.1
Main Demographic and Biochemical Profile of the Sample at Screening
BMI
FPG (mrnoUL)
- Values (where applicable) are means f SEM * Indicates gJycated hemoglobin (Normal range 0.035 - 0.065)

The subjects completed a total of 40 tests. An additional 5 tests were
perfonned, as repetitions to those where the subject's fhsting blood glucose
varied by more than 6 mmoYL on the study days according to our study
protocol. One test couldn't be repeated because the subject could not attend.
3.2 GLYCEMIC RESPONSE DATA
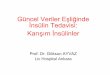
Blood glucose concentrations were measured by glucometer as well as
by YS1 anaIyzer. Linear correlation showed that readings obtained fiom
these two methods are siificantly correlateci, where the slope eqiials 1.05 f
0.01 and the correlation coefficient (r) = 0.97 at p<O.OOl (Figure.3.1). Tbere
was a percentage Merence between the slopes of correlation line and line
of identity. Analysis of the glycemic respoose data was based on YS1
readings.
Patterns of mean postprandial blood glucose increments and mean
blood glucose concentrations plotted against t h e for different test foods are
demonstrated in Figure. 3.2 and Figure 3.3; respectiveiy. Barley and
spaghetti had relatively d y negative b l d glucose incremeats, thereafter
maintaining a relatively steady state. Instant potato and white bread, on the
other hand, had relatively higher incrementai levels, which were m t l y
maintaked above the baseiine level before it undershot Iate in the cuwe.

- S m
25- --- Line of Identity
0 /
0
I I
8 a 2 2 0 - 0
8 % g 8 g w E 15- 8 , 1 s > 10-
m u & 5-
O " I I I I 1 O 5 10 15 20 25
Bbod Gkrocse Concentration by Glucometer (mroYL)
Figure 3.1
Correlation between Glucometer and YS1 Blood Glucose Concentrations

+PdatQ +Wb Bread +- Pineapple Juice *Spaghe(G -0- Bariey
Figure 3.2 Mean Blood Glucose Increments @y YSI) for Food
Types vs. Time

Figure 3.3
Mean Blood Glucose Concentrations (by YSI) For Different Test Foods

Pineapple juice shows a high early blood glucose increment peak followed
by rapid decline.
Two-way ANOVA of blood glucose increments vs. tirne for food types
(Table 3.2) shows a significant effect of food type (P4).05) h m 30 to 180
minutes, and a highly si@cant effect of subject (P<0.001) throughout the
test.
Cornparison of mean blood glucose increments for food types vs. time
is shown in Table 3.3. Sisnificant difEerences were noted only between 30
and 180 minutes postprandial. Throughout the test, the glycemic responses
of instant potato and white bread were not significantly different. Lïkewise,
the responses of spaghetti and barley were not significantly dinerent
throughout the test. The glycemic responses of spaghetti and barley were
signincantly difkerent fiom instant potato between 30 and 150 minutes, and
nom white bread between 60 and 120 minutes. As for pineapple juice, the
blood glucose increment was signincantly greater than all other f d types at
30 W e s , but only h m spaghetti and barley at 60 minutes. At 90 minutes,
it was signiscantly different h m only instant potato, and at 120 to 150
minutes, fiom both potato and white bread- At 180 minutes, the oniy
significant merence was noted between pineapple juice and potato.

Table 3.2
Two-Way Analysis of Variance of Incremental Blood Glucose Responses After Different Types of Food
30min
Source SS MS F P- Val Foods 234.9 4 58.7 11.2 <0.001
Source SS MS F P- Val Foods 86.7 4 21.7 16.0 <01001 Subject 50.0 7 7.1 5.3 <0.001 Error 38.0 28 1.4 Total 174-7
60min F d s 179-9 4 45.0 12-6 <0.001 Subject 206.6 7 29.5 8.3 <0.001 Error 99.6 28 3.6 Total 486.1
1 Foods 185.7 4 46-44 8.8 <0.001
90 min Subject 351.6 7 50.2 9.6 xO.001 Error 146.4 28 5.2 Total 732.9
120 min Subject 339.8 7 48.5 9.2 c0.001 Emr 147.4 28 5.3 Total 672.9

C0nt' d: Two-Way A d p i s of Va- of focrementa1 B h d Ghmse Respo- After Different Types of Food
Source SS Q F P-Val Foods 147-6 4 36.9 6.6 <OB01 Subject 319.7 7 45.7 8.1 <0.001 Error 157.2 28 5.6 Total 624.5
Source SS df F P-Val Foods 79.8 4 20.0 3.6 0.0176
180 min Subject 309.7 7 44.2 7.9 <O.ûûl Error 155.9 28 5.6 Toîal 545.4
I Source SIS df MY F P-Val
~~~~~ - -
I Source SS df MS F P-Val
210 min Subject 264.5 7 37.8 8.5 (0.001 Error 124.8 28 4.5 Total 434.4
240 min Foods 25 -3 4 6.3 1.4 0.2523 Subject 280.5 7 40.1 9.0 e0.001 Error 124.7 28 4.5 Total 430.6

Table 3.3
Mean Blood Glucose Increments for Food Types vs. Time
Pearled Barky Spgkttr* Pineapple White Bread Illstant Potuto J i e
- VaIues are means f SEM expressed as nmiol/L. - Cornparison of al1 means: means sharing same letter superscript are not sign%cantiy Fiifferent. Means with differenî superscripts are s igdbdy Merent at f l .05.

The mean mas under glucose response curve (Am) for food types
were examined. Two-way ANOVA of AUC (Table 3.4) shows that the
variation in AUC for food types can be explained by the signincant effects
of both food type @ < 0 .05) and subject (P<0.001). Table 3.5 lists mean
AUCs + SEM for food types. Mean AUC for barley and spaghetti did not
m e r signincantly, but were significantly Mirent h m that of instant
potato. Mean AUC fot barley was significantly different fiom that of white
bread. Mean AUC for pineapple juice was not diffemnt fiom all other test
foods. The AUCs of test f d s were significantly related to their respective
GIS (r = 0.984; p<O.Ol; Figure 3.4). There was no signincant correlation
between Pg and mean AUC.
The mean t SEM GI for each test food was calcdated and was found
to be 22 + 8.4 for barley, 65 f 15.2 for pineapple juice, 172 + 65.4 for
potato, 27 f 8 for spaghetti, and 71 for white bread (GI for @ose = 100).
Calculated GI values of test foods were significantly related to thei. GI
values obtained fiom the Merature (r = 0.88 at p < 0.05).
3.3 HYPOGLYCEMIC OUTCOMES
Blood glucose concenûations baseâ on both glucorneter and YS1 were
used for analysis of hypoglycemic outcornes, namely hpglycemia (Le.

Table 3.4
Two-Way Analysis of Variance of Area Under Glycemic Curve (AUC) Mer DifEerent Types of Food
Source
Foods
Subject
Error
Total
p p p p p
1214845.8 4 30371 1.45 5.5976174 <0.001
2768793 7 395541.86 7.290117 <0.001
1519203.6 28 54257.272
5502842.5

Table 3.5
Mean Area Under the Glycemic Response Curve (AUC) for Food Types
Food Tpes AUC
-
Pearled Barley
Spaghetti
Pineapple Juice
White Bread
Instant Potato
- Vahies are means * SEM expssed as mmolmia/l 0 - - Cornparison of d means: means shering same letter superscript are not q @ b n t f y
different. M~eans with différent mpema@ts are signiscantiy different at @.OS.

Glycemc Index
Figure 3.4
Correlation Between Mean AUC of Test Foods and Their Glycemic Indices

blood glucose G . 0 m V L ) , time to hypoglycemia, and low blood glucose
(Le. < 4.0 mmoYL).
Based on YSI, all 8 subjects experienced hypoglyrcemia compared to
ody 5 subjects based on the glucometer. Out of the 40 tests, hypoglycemia
occurred more fkequently based on the YS1 (17/40, Le. 42.5%) than the
glucometer (12/40, Le. 3W). This is consistent with our observation that
YS1 readings were on average lower than glucometer readings for the same
blood samples. The fhquency at which each subject had hypoglycemia
ranged fiom 0.2 to 0.8 (i.e. 1 of 5 to 4 of 5 tests) with both methods of
measurement. Hypoglycemia occurred with aU food types at times ranghg
fkom as early as 87 minutes, up to the end of the 4-hour test period (240
minutes).
3-3-2 LOW BLOOD GLUCOSE
AU subjects at some point had low blood glucose based on glucometer
and YSI. Similar to hypoglycemia, episodes of low *ose occurred more
fkequently based on YS1 (22140) than glucometer (20/40). The fhquency at

which each subject had low blood glucose ranged nom 0.2 to 1 (le. once to
aIl5 tests) on both YS1 and glucorneter.
Table 3.6 summarizes number of hypoglycemic and low glucose
episodes per subject based on glucometer a d YSI. The number of
hypoglycemic and low glucose episodes based on food type is illustrated in
Figure. 3.5 as detected by YS1 and glucometer. Episodes of hypoglycemia
and low glucose occmed most hquently with pkapple juice.
3.3.3 GI AND Pg IN RELATION TO HYPOGLYCEMIC OUTCOMES
The number of hypogiycemic and low glucose episodes was plotted
agakt food GI and Pg in Figure 3.6 and Figure 3.7, respectively. Resuits
fiom linear regression showed that food GL was not significantly related to
number of hypogiycemic or low blood glucose crpisodes. However, Pg was
inversely related to number of hypoglycemic (YS0 and low blood glucose
(glucometer) episodes @ < 0.05). Nevertheless, the number of points (types
of test meals) is small to draw conclusions.
Simple correlation was perfo~ned to obtain the relationship between
the occurrence of hypoglycemia, low blood glucose and GI and Pg of the
foods. There was no signincant correlation between food GI and
hypoglycemia or between food GI and low blood glucose by YS1 or

Table 3.6
Number of Hypoglycemic and Low Blood Glucose Episodes per subject
Numbers represent No. of episodes occurring in 5 tests.
Hypoglycemia
LowBlood Glucose
Subjects
Glucorneter YS1 Glucorneter YS1 -
2
3
1 2 O
1
4
4
3 O
2
4 O
3 1 2 1 4 1 4 1 3
3 1 3 4 4 1 5 1
5 6 1
1
7 4
5
1
1
% T o t a l 12 17 20 22

O Barley Pineapple Juice Potato Z Spaghetti White Bread
Test Foods
ü P - Low Blood Glucose
O Barley Pineapple Juiœ Potato Ir' Spaghetti White Bread
Test Foads
Figure 3.5 No. of Hypoglycemic and Low Blood Glucose
Episodes per Food Types

Figure 3.6
Correlation of No. of Hpglycemic Episodes (by Glucorneter and YSI) with GI and Pg.

"Law" (meter) vs. GI
"Low" (meter) vs. Pg a 1
Figure 3.7
"Law" (Ys9 vs. GI 8 1
Correlation of No. of Low Blood Glucose Episodes (by Glucorneter and YSI) with GI and Pg.

glucometer. However, Pg was significantly related to YSL-based
hypoglycemia (r = 0.46, slope = - 1-13, P<0.005) and to low blood glucose
based on YS1 (r = 0.33, slope = - 0.8 1, P< 0.05) and glucometer (r = 0.38,
slope = - 0.94, p<O.OS). The above relationships between Pg and occurrence
of both hypoglycemia and low blood glucose remained sipnincant after
including subject, fasting blood glucose, and GI in a multiple regression
mode1 (Table 3.7). Multiple regression didn't show any sigoificant
relationship between GI and hypoglycemia nor between GI and low glucose.
Simple correlation did not show any significant relationships between
time to hypoglycemia and GI, Pg or fasting blood glucose (FBG). However,
multiple regression analysis revealed that tirne to hypogiycemia based on
YS1 was signifïcantly related to GI (r = 0.82, pKO.05) and to FBG (r = 0.82,
p<o.o 1).

Table 3.7
Multiple Regression Analysis
Dependent 1 Variables Fas ting
r Subject BIood GI pg G k o s e
- -
Occurrence of Hypogiycemia §*
Glucometer
Occurrence of Low Glucose $*
Glucometer
YS1
Time to Hypoglycemia *
YSI*"
* ~efined as blood glucose < 3 nmoYL or symptoms of hypogiYCenga ~enned as blood ghrose < 4 inmVL.
* Number of observations = 40 ** Numbet of observations = 12 *** Number of observations =16
3
Values are X coefkients
r
-
(slope) fobwed ôy p vahies. NS = not signiscant.

4. DISCUSSION AND CONCLUSIONS
4.1 DISCUSSION
The purpose of this study was primarily to compare the pattern of
blood glucose response for carbohydrate f d s with Merent GI values in
type 1 diabetics on Lispro insulin. This was examined in two ways. The h t
method was plotting the measuced blood glucose increme~~ts vs. time for
each food to obtain the correspondhg curves. Another method was
cornparhg mean AUCs for Metent f d s .
The results obtained h m both methods indicate that the source of
carbohydrate significantly Muences blood glucose responses in type 1
diabetic subjects using insulin lispro. We believe that our study design was
strong enough to detect real differences, which were not due to error or
chance. These foods dEered in their glucose response because their GI
values dfler over a wide range, i .e. their carbohydrates are digested and
absorbed at different rates depending on thek nature (starch vs. sugar) and
chernical structure (amylose: amylopectin ratio). Among starchy test foods,
barley and spaghetti, which have relatively low GI values (25 and 41
respectively) produced significantly lower glucose increments compared to
bread and potato which have relatively high GI values (71 and 83

respectively) between 60 and 120 minutes, as shown in Table 3.3.
Furthemore, the mean AUC for potato was significautly greater than that
for spaghetti and barley (Table 3.5). The mean AUCs for test f d s were
signifïcantly related to the respective GI values (Figure 3.4) obtained h m
the lïterature (these GI values were determined in normal and type 2 diabetic
subjects). This incücates that the GI is valid in this group of subjects with
type 1 diabetes using lispro.
In the case of pineapple juice, GI done caowt explain its blood
glucose response pattern. Pineapple juice contains sugars that dser fiom
starchy f d s in 2 ways. Sugars are absorbed more rapiâly compared to
unprocessed starchy carbohydrate. Therefore, although it has a GI lower (GI
= 46) than 2 of the starchy f d s , the initial (30 minutes) mean blood
glucose increment for pineapple juice was greater than al1 the starchy foods
(Table 3.3). However, shortly after that, its incremental blood glucose fêUs
rapidly and, by 90 minutes, it becomes no longer different fiom that of
barley (Gr = 25). This is probably because sucrose, the main coristituent of
pineapple juice is half glucose and half hctose. Fmctose, in him, has a very
small effect in raising blood glucose, which lends pineapple juice its Pg
value of 0.5, and exp1abs the rapid deche in blood glucose incremental
curve.

Despite having different Pg, mean AUC for pineapple juice retained its
median location among other test foods (Table 3.5) because AUC is rehted
to GI rather than Pg.
Our finding regardhg the signifïcance of source of carbohydrate on
glycemic response contradicts with current ADA Recommendations (1994)
on dietary cahhydrates, which state: "From a cfinical perspective, fbt
priority should be given to the total amount rather than the source of
carbohydrate consumed". One reason for the disagreement maybe that, for
this study, we selected carbohydrate sources with a wide range of GI, which
we expected to produce a wide range of glucose responses. However, in
practice, cornmon foods nom difEerent sources may not have large
Herences in GI and, thus, would not be expected to affect giucose
responses (Wolever et al. 1994). Thus, source of carbohydrate will affect
postpmdial glucose responses only if the GI values of the different f d s
differ by a sutnciently large amount. In addition, other factors such as
number of subjects king tested and variation between and within-subjects
may all affect the ability to detect difEerences in blood glucose responses to
different f d s .
Another aspect, which may infiuence the validity of our conclusions, is
the use of individual foods rather tban mixed meah in our experiment. Some

studies showed that diBeremes in source of carbohyclrates make no
merences to glycemic responses in the context of mixed me& because of
the potential effects of fat and protein on glucose response. However, faulty
methods were used in a numbet of the studies cited to support this position
(Wolever and lenkùis. 1986). In addition, there are other studies showkg
that GI retains its predictive ability in the mixed d setting (Collier et
d.1986). Furthemore, alterhg diet GI was fomd to improve overall blood
glucose control in diabetes (Wolever et al. 1992a).
Apart fiom GI and Pg, methodological factors may also înfiuence
profoundly the interpretation of glycemic response data (3). Factors that
might innuence blood glucose value obtained include: method of blood
sampiing subject characteristics (e.g. body fatness, glucose tolerance status,
insulin resistance); dose and timing of lispro and long-acting insulin; degree
of diabetic control and particularly the fasting blood glucose value on the
day of the test.
Om results indicate that subject factors had a significant effect on
blood glucose increments throughout the test (Table 3.2) and on the area
under the glycemic response curve (Table 3.4). This is because subjects
m e r fiom each other. In addition, variability could arise fkom within-
subject variation. That is, when a group of subjects test a food once, the

glycemic response obtained in each subject may Vary considerably (3) which
doesn't necessarily mean real dif fe~e~:es between the subjects.
Our measurement of glucose response was based on capillary whole
blood, because it is simple, non-invasive a d f d a r to our patients. In
addition, it was suggested that the use of capillary compared to venous blood
is more precise, as the glycemic responses are gceater in capillary biood.
That is, greater absolute differences between f d s and greater heterogeneity
between means d o w detedion of small differences in glycemic responses to
diflierent foods, and thus more experimental power is obtained (61).
Both glucorneter and YS1 d y z e r were used to masure capillq
glucose concentration. The former measures it in plasma; the latter in whole
blood. Glucose concentration is lower in red blood cells compared to
plasma; therefore, our hding that glucose concentration measurements
using glucorneter were greater was not unexpected.
The second objective of the study was to determine if the source of
carbohydrate expressecl as GI and Pg c m predïct the occurrence and timing
of hypoglycemia induced by iispro.
Results h m simple and multiple tegression d y s i s showed that the
tendency of haviag hypoglycemia postprandially was inversely mlated to Pg
(O* in YSI-based hypoglycemia). Similarly, the occurrence of low glucose

was sigdicantly related to Pg (YS1 and giucorneter). GI did not contribute
signincantly to the aforementioned correlations.
Om explanation for the finding that Pg predicts occurrence of
postprandial hypoglyceniia and low glucose is that Pg detemiines the
amount of carbohydrate absorbed as glucose, which in tum directly
influences its avdability in blood. The results of blood response studies
(Lee and Wolever) indicate that the less glucose consumed, the quicker the
blood glucose drops to baselb. Accordingiy, the occurrence of
hypoglycemia and low glucose is more likely expected with carbohydrate
foods having lower Pg (Le. more sucrose) regardless of their GI values.
GI did not predict occurrence of hypoglycemia and low glucose. Low
GI carbohydrates produce relatively lower glucose increments and smaller
AUCs, yet because they are absorbed slowly their glucose increments are
sustained for a longer tïme than the high GI carbohydrates. This may be why
we found no significant tendency for low GI to be related to hypoglycemia.
On the other hand, other fkctors could be responsible for missing a
signincant correlation between GI and hpglycemia such as the high
variability of giucose responses in type 1 diabetes. More power may be
needed to obtain a signifiant result.

When time to hpgiycemia was assessed, it was not found to be
signiscantly related to Pg. However, it was directly related to GI and FBG
(YS1 only; in multiple regression only, F0.05). Therefore, should
hypoglycemia happen, it wiU occm eariier with foods hahg lower GI
values and in subjects baving lower basehe glucose.
4.2 POTENTUU, PRACTICAL IMPLICATIONS
The current fïnding regardiig the signincant effect of the source of
carbohydrate (GI and Pg) on postprandai glycemia is relevant to every day
life of type 1 diabetics, especially those who are intensively treated with
lispro. One possible practical miplication of this shdy is that education
about insulin adjustment for the GI and Pg of dietary carbohydrate may be
needed to achieve optimal glycemic control. This is especially important
with diabetics following libersrlized diet. We have shown that high GI
starchy carbohydrates producecl on average greater glycemic responses up to
3 hours *postpratldidy compared to those with low GI. So, it may be
beneficial to advise diabetics to arlminrstei 0 a relatively larger dose of lispro
for higher GI carbohydrates Furthemore, spaghetti, which is low GI, slowly
digested carbohydrate showed unfavorable siycemic response after lispro in
the sense that blood glucose dmpped early for a while before it became

sustained for the rest of the c w e . So there is a potential for early
postprandial hypoBlyda, although we could not demonstrate it. So,
alteration in either the dose or timing of lispro by admiiiistering a smaller
dose or admmiste~g the dose a& eatiog may aliow patients to achieve a
more acceptable pattern of blood glucose.
One of the fkdhgs was thet f i t juices are more readily absorbeci
caused an initial greater and fater rise in postprandial glucose than starchy
carbohydrate. Furthemore, they are more Iürely to predispose to
hypoglycemia than starchy carbohydrates. Thmefore, if juices are to be
taken, then tighter contro1 of blood glucose may be achieved if a larger dose
of lispro taken preprandially. If this is the case it may be necessary to take a
snack to prevent late postprandial hpglycemia

4.3 FUTURE RESEARCH
One area for fiÙtrae research is to examine the effect of carbohydtate
source on postprandial glycemia in the context of mixed rneals rather than
individual carbohydrates (as m our study) to look at the possible
confounding variable effects of fat and protein. This way, the validity of our
conclusions in normal meal conditions can be d e t e e ,
A M e r step would be to examine the glycemic response to dif5erent
GI meals with different doses of lispro. Variation in timing of lispro
injection can also be tried. These procedures would be helpful in
detemiinùig how best to adjust the dose of lispro for diffierent carbohydrate
sources.
4.4 CONCLUSIONS
There were 2 objectives outlined in this thesis. The primary objective
was to compare postprandial glycemic response profile for equivalent
arnounts of carbohydrate foods k m different sources with different
glycemic index (GI) values aAet a standard dose of lispro in type 1 diabetic
subjects. The data supported my first hypothesis that signiscantly different
blood glucose responses will be elicited by quivalent amounts of
carbohydrate fkom dierent sources having different GI vaiues.

M y second objective was to determine how equivalent amounts of
carbohydrate foods with Merent GI values influence the postprandial
hypoglycemia induced by lispro. W e hpthesized that postprandial
hypoglycemia will be elicited by lispro in type 1 diabetic subjects taking
equivalent arnounts of carbohydrate firom different sources more fkequently
with foods having lower GI d lower proportion of carbohydrate aôsorbed
as glucose (Pg). The resuhs supported the hypothesis for tbe Pg but not for
the GI. However, GI innuencecl the timing of postprandial hypoglycemia

REFERENCES
The Diabetic Control and Complication Trial research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in - insulindependent diabetes mellitus. New Eng j Med 1993;329:977-86.
UK Prospective Diabetes Study Group. Intensive blood glucose control with SUlphonyIureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53.
Wolever TMS, Jenkins DJA, Jenkins AL, Josse RG. The glycemic Index: Methodology and clinical implications. Am J Clin Nutr 1991 ;54:84654.
Jenkins DJA, Ghafari H, Wolever TMS, Taylor RH, Barker HM, Fielden 6 Jenkins AL, Bowling AC. Relationship between the rate of digestion of f d s and postpcandial glycemia. Diabetelogica l982;22:450-55.
Wolever TMS, Jenkins DJA, Josse RG, Wong GS, Lee R. The glycemic index: Similarity of values derived in insulindependent and non insului-dependent diabetic patients. J Am Coll Nutr 1987;6:295-305.
Collier GR, Giudici S, Kalmusky J, Wolever TMS, Helman G, Wesson V, Ebrlich RM, Jenlùns DJA. Low glycemic index starchy foods improve glucose control and lower senmi cholesterol in diabetic children. Diab Nuh Metab 1988; 1 : 1 1-1 9.
Wolever TMS, Jenkins DJA, Vuksan V, Jeakias AL, Wong GS, Josse RG. Betieficial eff i t of low-gh/emic index diet in overweight NIDDM subjects. Diabetes Care 1992; 1 5:S6266.
Wolever TMS, H . S, Chiasson JL, Josse RG, Leiter LA, Rodger NW, Ross SA, Ryan EA. Day-to-day consistency in amount and source of carbohyârate intake associated with improved b l d

glucose control in type 1 diabetes. J Am Coll Nutr L999;18(?):242- 47.
Burge MR Castille KR, Schade DS. Meal composition is determinant of lispro-induced hypoglycemia in IDDM. Diabetes Care l997;ZO: 152-55.
Ebeling P, Jaasson PA, Smioth U, Lalli C, Bolli GB, Koivisto VA. Strategies toward improved contr01 during insulin lispro therapy in IDDM: Importance of basai insulùl Diabetes Care lWT2O: 1287-89.
Strachan MWJ, Frier BM. Optimal time of administration of insulin lispro: Importance of meal composition. Diabetes Care 1998;2126- 31.
Tan H, Maclean DR. Epidemiology of diabetes meIlitus in Canach C h Invest Med 1995; l8:24O6.
Tan a Daneman D, Lan DCW, et al. Diabetes in Canada: Strategies towards 2000. Toronto: Canadian Diabetes Advisory Board; 19979.3.
Report of the Expert Cornmittee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care l997;2O: 1-1 5.
Charles MA, Fontbonne A, Thibult N, et al. Risk factors for NIDDM in white population. Paris Prospective Study. Diabetes 1991; 40:796-9.
Eastman RC, Cowie CC, Harris MI. Undiagnoseci diabetes or i m p d -ose tolerance and cardiovasc& risk Diabetes Care l997;2O: 127-8.
Tuomilehto J, Knowler WC, Zimmet P. Rimary prevention of non- insului-dependent diabetes meilitus. Diabetes Matab Rev 1992;8:339-53.
Diabetes in America 2d ed. Washington= National Diabetes Data b u p , National Iastaute of Diabetes and Digestive and Kïdney Diseases, National htiitute of He* 1995.

19. Fuller JEE, Elford J, Goldblatt P, et al. Diabetes mortality: new lïght on an underestimated public health problem. Diabeteloica l983;24:3364l.
20. Garcia W, McNamara PM, Gordon T, et al. Morbidity and mortality in diabetics in the Fmmhgham population. Sixteen year foilow-up study. Diabetes l974;23: 105-1 1.
21. Jarrett J. Mortality in diabetes. Q J Med l99O;75:4 13-4.
22. Stamler J, Vaccaro O, Neaton JD, et al. Diabetes, other risk Iactors, and 12-year wdiovascular moaality for men screened in the Multiple Risk Factor Intervention TM. Diabetes Care 1993;16:434- 44.
23. Krolewski AS, Kosiski El, Warram JH, et al. Magnitude and determinanis of comnary artery disease in juvenileonset, iusuiim dependent diabetes mellitus. Am J Cardio 1987;59:750-5.
24. Cox DI, Kovatcheu BP, Juüan DM, et al. Frequency of severe hypogiycemia in insulin-riependent diabetes mellihis can be predictednom self-monitoring blood glucose data J Clin Endocrino1 Metab 1994;79: 165962.
25. SchifFRn A, Suissa S. Predicting nocturnal hypoglycemia in patients with type 1 diabetes treated with continuous subcutaneous insulin infusion. Am I Med 1987;82:1127-32.
26. Inada M, Oishi M, Nishikawa M, Kurata S, Imura- H. Chical evaluation of measiuing glycosylated hemoglobin levels for assessing the long-tenn blood glucose control in diabetics. Endocrino1 Jpn. l980;27:4 1 1-5.
27. Kilpatrick ES, Maylor PW, Keevil BG. Biological cariation of glycated hemoglobm: Ins>lications for diabetes screening and monitoring. Diabetes Care l998;2 1 261-4.
28. Pate RR, Pmtt M, Blair SN, et al. Phrysical activity and public healtk A recommendation h m the for Disease Control and

Prevention d the American College of Sport Medicine. $.MA 1995;273:402-7.
Ha Lean MEJ. Technical Review: Recommendations for the nutritional management of patients with diabetes mellitus. Eumpian Journal of CLinical Nutrition l997;52:467-8 1.
American Diabetes Association. Diabetes meIlitus and exercise. Diabetes Care 1998;21(Suppl1):540-4.
Wasserman DH, Zinman B. Exercise in individuals with IDDM. Diabetes Care 1994; 17:924-37.
Health and W e l f h Canada. Action Towards ... Canadian Guidelines for Healthy Eating and ~ e c o k n d e d Strategies for Implementation. The Report of the CommUnicatio~plementatiom Conmittee. Ottawa: W s t e r of Supply and Services Canada; 1990.
Health and WeKare Canada- Nutrition reconmendations. The Report of the Scientific review Cornmittee. Ottawa: Canadian Govenunent Publications Centre; 1990:Cat No. H49-42/lg!JO E.
American Diabetes Association Position statement. Nutrition recommendations and principles for people with diabetes mellitus. Diabetes care 1994; 175 19-22.
CRC Handbook of Dietary Fiber in Humui Nutrition 2& ed. Baca raton, FL: CRC Press; 1 993:lll-52.
Diabetes and Nutrition Study Group of the Europian ~ssociation* for Study of Diabetes: recomrnendations for nutritional -nt of patients with diabetes meIlitus. Diab Nutr Metab l995;8: 186-9.
World health Organization: Diet, Nutrition, and the prevention of chronic diseases. Technical Report Series. l99O;797: 1-204.
Canadian Diabetes Association: Guidelines for nutritional management of diabetes m e b in the 1990's (Positive Statement). Beta Release 1989; 13%-17.

39. American Diabetes Association: Nutritional Recommendations and principles for people with diabetes meIlitus (Positive Statement). Diabetic Care 1995; 18(Suppll): 16-9.
40. 1998 Clinical practice guidelines for the management of diabetes in Canada. CMAJ 1998;159(Suppl8),5 16.
41. Reeves ML, Seigler DE, Ryan EA, Skyler JS. Glycemic control in insulùi dependent diabetes mellitus: comparison of outpatient intensined conventional therapy with continuous subcutaneous insulùi infusion. Am J Med 1982;72:673-80.
42. Bhasker R, Ghon MCY, Field JB: Tirne-action charecteristics of regular and NPH insulin-treated diabetics. J Clin Endocrin Metab 1980;50:475-80.
43. Lean MJE, Ng LL, Tennison BR Intemal between insulin injection and eathg ni relation to blood glucose control in adult diabetics. Br Med J 1985;29O: 105-8.
44. Brange J, Owens DR, Kang S, Volund A. Monomeric insulin and their experimental and clinical implications. Diabetes Care 1990; 1 3:923-54.
45. Ter Brack EW, Woodworth JR, Biamhi R, et al. Injection site effects on the pharmacokinetics and glucodynamics of insuiin lispro and regular insulin. Diabetes care 19%; 19: 1437-40.
46. Kang S, Brange J, Burch A, Volund A, Owens D. Subcutaaeous mSuim absorption cxp1aMed by insulin's physicochemical properties: Evidence fiom absorption studies of soluble human insulin and insulin analogues in humans. Diabetes Care 1991;14:942-8.
47. DiMarchi RD, Mayer JP, Fan L, Brems DN, Frank BH, Green LK, Hofnnan JA, Howey DC, Long HB, Shaw WN, Shields JE, Slieker LJ, Su KSE, S d e U KL, Chance RE. Synthesis of a kt-acting insulin based on structural homology with msulin-lilre p w t h -or 1 in peptides Symposium. ESCOM 1992:26-8.

48. Brems DN, Alter LA, Beckage MJ, Chance RE, DiMarchi RD, Green LK, Long HB, Pekor Shields JE, Frank BH. Altering the association properties of insulin by amino acid replacement. Protein Eng 1992;5:527-33.
49. ~ o w e ~ DC, Bowsher RR, Brunelle RL, Woodworth JR. ~ys(B28),Pro(B29)]-Human Insulin= A rapidly absorbed analogue of human insuün. Diabetes 1994;43:369-40.
50. Anderson JHJr, B ~ l l ~ ~ l l e R, Koinsto VA, Trautmann ME, Vignati S, DiMarchi R. The Multicenter Insulùi Lispro Study Group. Improved meai time treatment of diabetes meIlitus using insulin analogue. Clin nier 1997; 19:62-72.
51. Anderson JIZ Brunelle RI,, DiMarchi R, Koivisto VA, Pfiibner A, Trautmm ME, Viguati L. The Multicentre Insulin Lispro Study Group: Reduction of p o s t p d a l hypogly~emia and fiquency of hypoglycernia in IDDM patients on insulin analogue treatment. Diabetes 1997;46:265-70.
52. Schemthaner G, Wein W, Sandholzer K, Equiluz-Bruck S, Bates P, Birkett MA. Postprandial insulin lispro: a new therapeutic option for type 1 diabetic patients. Diabetes Care 1998;21:570-3.
53. Schernthaner G, Wein W, Sandholzer K, equiuz-Bmck S, Birkett M. Postprandial use of insulin lispro: A new therapeutic option in the treatment of type 1 diabetic patients? 9Abstract). Diabetologica 1996;39:A24.
54. Ebeling P, Jansson P-A, Smith ULF, Lalli C, Belli GB, Koivisto VA. Strategies towards improved control uring insuiin lispro therapy in IDDM: Importance of basal insuiin, Diabetes Care l997;20(8): 1287-9.
55. Koivisto VA. The human insulin analogue insulin lispro. Am Med 1998;30260-6.
56. Anderson JH Jr., Brunelle RL, Koivisto VA, PiÙtzner A, T r a m ME, Vigoati L, DiMarchi R Reduction of postprandial

hypoglycemia and ~~y of hypoglycemia in IDDM patients on insuiin-analogue treatment: Multicentre InsuIin Lispro Shidy Group. Diabetes 1997;46:265-7O.
57. Brunelle RL, Llewlyn J, Anderson JH Jr., Gale EAM, Koivisto VA. Meta-analysis of the effect of insulin lispro on severe hypoglycemia in patients with type 1 diabetes. Diabetes Care 1998;21(10).
58. Burge Castillo KR, Schade DS. Meal composition is a determinant of lispro-induced hypoglycemia in IDDM. Diabetes care l997;20(2).
59. WoIever TMS and Bolognesi C. Source and amornt of carbohydrate affect postprandial glucose and insulin in normal subjectsJ Nutr 1996; 126-2798-806.
60. Kong M-F S-C, Macdodd IA, Tattersall RV. Gastric emptying in diabetes. Diabet Med 1996; 13: 1 12-9.
61. Macdonald IA. Physiological regdation of gastrying emptying and glucose absorption. Diabet Med 19%; 13(SupplS):S 1 1-5.
62. Horowitz M, Edelbtoek MAL, Wishart JM, Straathof JW. Relationship between oral glucose tolerance and gastric emptying in nomal healthy subjects. Diabetologia 1993;36:857-62.
63. Wolever TMS. How important is prediction of glycemic response? Diabetes Care 1989; l2:59l-3.
64. Wolever TMS, Jenkins DJA. The use of glycemic index in predicting the blood glucose response to mixed me&. Am J C h Niitr l986;43: 167-72.
65. Jenkins DJA, Wolever TMS, Taylor RH, et al. Glycemic Index of f d s : a physiological b i s for cahhydrate exchange. Am J C h Nutr 198 1 ;34:362-6.
66. Wolever TMS, Jenkins DJA, V - V, icAtm\en L, Jeakias AL, Josse RG. Variation in d fat does not affect the relative blood

glucose response of spaghetti in subjects with type 2 diabetes. Diab Nutr Metab 1992;5:191-7.
67. Rasmussen O. Dose-dependency of the glycemic response to starch- rich meals in insulùi dependent diabetic subjects: Studies at constant insulinemia. Metabolism 199334237 10- 1 3.
68. Hennanser K, Rasmussen O, A d k d J, Winter E, Schmitz O. Glycemic effects of spghettï and potato wnsumed as part of mmed meal on TDDM patients. Diabetes care 1987; IO:4Ol6.
69. Wolever TMSy Nguyen P-M, Chiasson J-L, H a t JA, Josse RG, Pairnason C, Rodger NW, Ross SA, Ryan EA, Tan MH- Relatiomhip between habitual diet and blood glucose and lipids in nominsulin dependent diabetes. Nutt Res 1995; lS:843-57.
70. Reeves GM. Dietary therapy for non-insulin-dependent diaetes rnellitus. N Eng J Med l988;3 l9:862-4?.
71. Collier GR, Giudici S, Kalmusky J, Wolever TMS, H e h G, Wesson V, Ehrlich RM, Jenkms DJA. Low glycemic index starchy foods improve *ose control and lower senmi cholesterol in diabetic children. Diab Nibr Metab 1988; 1 : 1 1-9.
72. Wolever TMS, Vuksan V, Katzmm-relle L, Je* AL, Josse RG, Wong GS, Jenkins DJA. Glycemic index of f i t s and nuit products in patients with diabetes. International J Food Sci Nutr 1993;43:205- 12,
73. Bumin JM, Alberti KGMM. What is blood glucose: can it be measured? Diabetes Medicine 199O;7: 199-206.
74. Shimizu S, Yasai K, Tani Y, Yamada H- Acyi-CoA oxidase with an alternative oxygen accepter. An C h Biochem 1980; 13: 1 5 1.

Appendix A
CONSENT FORM
Effect of Carbohydrate Source on Postprandial Blood Glucose in Subjects with Type 1 Diabetes using Insulin Lispro
Investigators: Thomas Wolever MD, PhD, Tel: (416) 978-5556 Dept. of Nutritional sciences, University of Tonwto MSS 3E2 St- Michaei's Hospital, 30 Bond St, Toronto MSB 1 W8
Loren Grossman, MD, Tel: (416) 699-7294 Eli Liiy Canada, 3650 D a n f i Ave., Toronto MIN 2E8 St. Michael's Huspital, 30 Baad St., Toroato MSB 1 W8
Nadia Mohammed, MD, Tel: (41 6) 978-0548 Dept of Nutriti-onal sciences, University of Toronto MSS 3E2
Study Sponsor: Eli Lily Canada, 3650 Danforth Ave., Toronto MIN 2E8
BACKGROUND Good blood glucose (sugar) control for people with type 1 diabetes depends on
achieving a balance between insulin, diet and physical activity. Insulin Iispro m s i m k to r e m human insulin but acts Wer and may a b w for better blood glucose contml. Studies have shown that the amount of msulin lispro d e d depends on the amount of carbohydrate present in the meal about to be consumed, However, there are no studies on how much insulin iispro needed for different types of Catboirydrate foods- Some people on insuijn iispro have reported large swings of blood sugar after eating some f d s but not others. This may be because carbohydrate foods are digested and absorbed at different rates and produce different blood giucose responses. The Wer the carbohydrate in a food is digested d absorbed the highR the blood ghtçose response. We ex* tbat different foods will produce diBiirent patterns of Mood sugax tesponse m people Usmg bsdin lispro, however, we don't Iniow exactiy how big the diffkences will be. If large ciiffierences ex&, it may be possible to contrd these by adjusting the dose or timing f insulin lispro. The purpose of this study is to determine the pattern of blood glucose response produced by di&nmt catbohydrate foods in people ushg irrmlin lispro.
PROCEDURES The study m v o h 6 visits to the Clinical Nutrition Centre of St. Michael's
Hospïtaf, 61 Queen Street eest, 6* floor between 7:30 and 8:ûû A M d e r 10-12 hour overnight fàsts over a 6 8 week penod The first visit is tbe screamig visa and will Iast about 30 minutes- The other 5 visits are fbr tests that wïil ïast about 4% hours.
To detemiiw eiigibiüty for the shdy, you wül à asked questions about yoia medical history and home b M test nsuhs. a d be asked to give a fiistiqg bkmd sample and have height and weight m e . . Ifeîigiile you wili be d e d to record a 3 day diet history to determine the nature of the meals which wili be provided duriqg the study.

For dinner and snack (if noma& consumed) on the evening before each test &y you wiIl be asked to eat standard meals which will be provided, and mthing else except for water. If need to eat something to tceat an Uwilni reaction, the test Win be cancekd and rescheduled for another day. Upon arriva1 at the Nutrition centre, you will be weighed and a fhsthg Wer-prick blood sample obtaïned- If b h d sugar is les than 4.0 mmoYL or more than 16.7 rmiloYL, the test win not be done, and will be reschedled fbr another day. If the test is camed out, you will take the dose of insuii~ lispro mmdy used for a standard breakfgst and eat a test meal mnsisting of a standard portion of either mashed potato, bread, barley or pineapple juice. Thp test d wili be given with a drink of water, wfke or tea (the same drinlr chosem on the ht day will be &en to you on every other test). The same dose of iasulin kpro wiU be taken et the yime time Gefore the start of the test meal on each of the 5 test days. Finger-prick Mood samples w-ill be taken every 30 minutes afta startmg to eat for 4 hours; 2-3 drops of bbod wiil be taken into a tube for of bbod ghxose in the bratory. An additional drop of blood will be used to determine blood giucose by meter- If you k l symptoms of low blood sugar, it wiU be measured immed&eiy. If at any time your biood giumse Qops below 3.0 k Y L , then the test Win be stopped, and you will be given 10 g oral glucose and sometbiag to eat ifrequired and blood glucose monitored untiï it bas recovered.
During the test, you will not be permitted to smoke and wili remain seated (except to vis3 the washroom). Mer the 4-hour blood simple, you will be fke to ieave. A snack or lunch of your choice will be provideci if desired.
RISKS There are virtually no risks iwolved in this study- Each test will involve 9 fhger-
stick blood samples, which may be more than usually done m one day. Rowever, we have done several thousand similar tests in subjects with diabetes with no problems more serious than occasional sore fingers. The test meals have been selected to khide foods with hi& low and intermediate blood giucose responses- Thus, blood ghicose vahies higher or lower than those norxœUy seen niay occur. Blood glucose monitoring every 30 minutes wïil allow detection and treatment of bw blood sugar ifit occurs.
BENEFITS You wiü learn how your blood glucose respoads to di&ent fbds. This niay heîp
you and others know how to ad* msulin Iispro dose for difkent types of carbohydraîe foods-
EXPENSE REIMBURSEMENT As compensation for the thœ required to participate, you wiü receive $40 for each
test conipleted (total of $ZOO for 5 tests). Parking or public transit costs wiil a b be reimbursed for each visa you bave to male for the study (including visits if a test camiot be done because of bigh or bw biood giuwse). The resdts wili be most useful if you complete d the tests.

Your records will remain codidential The results of this research study may be presented at meetings or in publications. However, your identity win not be disclosed in those presentations-
STOPPING THE STUDY Your participation in the study is voluntary, and you may withdraw at any time
without penalty and without dfixthg your fUturP medical care. The mvestigators may also stop your part ic i in in the study without your consent if your continued participation in considered dangerous to you or others, the results are not useful or for any other reason,
RESEARCH ETHICS BOARD CONTACT If you have my questions as a research sub- you may contact Dr. Julie Spence,
Chair of the Research Ethics Board at (416) 8646060 Ext 2557,
CONSENT I am at least 14 years old, am not pregnant and am willing to comply with the shdy
protocol. I have read and understand this consent form I am h l y volunteering to take part m these tests. I understand I may stop at any time doe any reawn without prejudice.
NON-WAIVER CLAUSE You do not waiver any of your legal rights by si& this consent,
Date

Appendix B
Effect of Carbohydrate Source on Postprandial Blood Glucose in Subjects with Type 1 Diabetes usmg Insulin Lispro
MEDICAL HISTORY QUESTIONNAIRE
Today's date (d/m/y): Name: Date of Blrth ( M y ) : Address: -- - City: - Province: --- Postal Code: - Telephone (Home): - (Work): G e d e r M-F-
(If fernale Are you pregnaiit, p h h g jmgnancy or breast feedmg? Yes - No --) Are you participating in another medIcal study? Yes - No - Do you have any a.liergy/reaction to potato, wheat, barley or pïneapple? Yes -- No - MEDICAL HISTORY Have you had any of the followïng (write on back if more space needed)?
Yes No If yes, what and/or w k n
QUESTIONS ABOUT DIABETES How long have you bad diabetes? - How was it found? -- H O ~ long have ~ O U been taking i n a h Iispro? --- InsulinDo~imRip: - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
Usual blood giucose (sugar) reading m the morniag before bmakû~: H o w mmy tÏmes m the iast 3 montbp bave you had the help of someone e k because of an insulin reaction (iow blood sugar)?

Appendix C
Weight and Nutrient Content of Standard Dinner Meal
[l] Choice dm? Bar (Mead Johnson Nutritionals)
Weight ber bar) Energy Protein Fat
Saturated Fat Linoleic Acid Leiolenic Acid
Carbohydrates Sorbitol
[2] Ensurem Formula (Abbott Lahratories)
#O g 150 Kcal
7 g 5.4 g 2.7 g 0.7 g 0.16 g 21 g
Volume ber cm) Energy Protein Fat Polyunsaturates Linoleic Acid Linolenic Acid Momu~lsaturates Saturates Cholesterol
235 mL 250 Kcal
9.4 g 6.7 g 1.4 g 1.3 g
0.21 g 2.8 g 0.5 g 1.7 g 38 g

Appendix D
Effect of Carbohydrate Source on Postprrndial Blood Glucose in Subjects with Type 1 Diabetes asing insulin Lispro
Data Form m: - - - - ID No.: - - Date (d/m/y): ---------- Weight : Did subject CODSUIIL~ standard dinner meal last nïghî? Yes - No -
Time of cünner meak Type: THne of snacks (iiany): -- Type: -II-
Insu lin: Night before Type(s): ----- mse: -------- T&: - - - - - - - - - - -
--HI---- --------- ----------------------
MornÙig of test: ----., -- -II-----
*-- --- - - Site of injection: LI- T'hm taken (minutes before startzhg to eat): ---
Endpoint Glucose * Fastmg = time of &hg blood sample. ** Tick if sample on time, write in time if sample not on tirne. 5 Test is mot to be done if fasting Glucose by meta is 4 .0 or N7.6 rnmoüL.
T h started to eat: ------ Time to eat meai (miautes): -------- Exercise in previus 24 hrs. (type and dination): -------- -- Any u n d concerns on day befire test? Yes:- ;No: - (ifyes exphin) --- Was hypoglycemia or other adverse event(s) e- during the test? Yes: -; No: (if"yest), piease explaia and use this sppce to record treatmpnt:

Appendix E
Demographic and Biochemical Profile of the Subjects at Screening
Age Duration of Diabetes Duration of Being On Lispro Height Weight SM1 FPG HbAlc Triglycerides Cholesterol HDL LDL Creatinine Urea Na K Cl .
Total CO2 Albinnin Protein AST
* "Acceptable" ranges are pre-requisite for enrollment in the study. They are NOT necessarily "normal" ranges.

Appendix F
Insulin Types and Mean Doses Used By Subjects
No. of Memi dose (y) I subjects SEM
PM INSULIN DOSE Lispro Bolus mers *
* Other types of insulin in P M doses are NPH (5 subjects), lente (2 subjects), and Lispro pump [CSII at rate 1.2 Um] (1 subject).
AM INSULIN DOSE Lispro Bolus Others *
* Qthertypes of insulin in AM doses are NPH (3 subjects), lente (2 subjects), and Lispro pump [CSII at rate 1.2 U h ] (1 subject).
8 6.6 t 2.7 6 8.6 t 2.7