Embed Size (px)
Citation preview

Effectiveness of TheophyllineProphylaxis of Renal Impairment AfterCoronary Angiography in Patients With
Chronic Renal InsufficiencyWolfgang Huber, MD, Chrysantha Schipek, Kathrin Ilgmann, MD, Michael Page, PhD,
Michael Hennig, PhD, Annette Wacker, MD, Ursula Schweigart, MD,Leopoldo Lutilsky, MD, Christian Valina, MD, Melchior Seyfarth, MD,
Albert Schomig, MD, and Meinhard Classen, MD
Contrast media can lead to renal impairment that resultsin longer hospitalization and increased mortality. Aden-osine is a crucial mediator of contrast-induced nephrop-athy (CIN; an increase in serum creatinine of >0.5mg/dl within 48 hours). Therefore, it was the purpose ofour study to investigate whether the adenosine antago-nist theophylline reduces the incidence of CIN after cor-onary angiography. We also characterized risk factorsfor CIN after coronary angiography. One hundred pa-tients with serum creatinine concentrations of >1.3mg/dl randomly received 200 mg IV theophylline orplacebo 30 minutes before coronary angiography(amount of contrast medium >100 ml). Patients whoreceived theophylline and the controls were comparablewith regard to baseline creatinine levels (means � SD)(1.65 � 0.41 vs 1.72 � 0.69 mg/dl) and the amount ofcontrast medium received (235 � 89 vs 261 � 139 ml).Theophylline significantly reduced the incidence of CIN(4% vs 20%, p � 0.0138). With placebo, creatininesignificantly increased at 12 (1.82 � 0.79 mg/dl, p �
0.0057), 24 (1.90 � 0.86 mg/dl, p � 0.0001), and 48hours (1.90 � 0.89 mg/dl, p � 0.0007) after adminis-tration of contrast medium. With pretreatment with theo-phylline, mean creatinine only increased 24 hours aftercontrast medium administration (1.70 � 0.40 mg/dl,p � 0.029), but was stable 12 hours (1.65 � 0.43mg/dl, p � 0.99) and 48 hours after contrast mediumadministration (1.65 � 0.41 mg/dl, p � 0.99). Thefollowing parameters were significantly associated withcontrast-induced renal impairment: Cigarroa quotient>5 (contrast medium [milliters] � serum creatinine/bodyweight [kg]), elevated troponin T, >300 ml of contrastmedium, and emergency angiography. In conclusion, the-ophylline reduces the incidence of CIN in patients withchronic renal insufficiency undergoing coronary angiogra-phy. It should be used especially in patients receiving largeamounts of contrast medium, and in patients with aCigarroa quotient of >5 and/or elevated troponin Tlevels. �2003 by Excerpta Medica, Inc.
(Am J Cardiol 2003;91:1157–1162)
The frequency of contrast-induced nephropathy(CIN) (Table 1) strongly depends on a number of
risk factors (Table 2). In the worst case, CIN occurs in�50% of patients.1–9 CIN, according to Barrett’s def-inition (increase of serum creatinine of�0.5 mg/dlwithin 48 hours after contrast medium1), results inlonger hospitalization2 and increased mortality.3,4 Thein-hospital mortality of patients with CIN requiringdialysis can be as high as 36%.4 A large number ofprophylactic procedures have been investigated. Re-cently, the antioxidant acetylcysteine has been shownto be prophylactic in patients who receive smallamounts of contrast medium (75 ml) intravenously.5
Data in patients who underwent coronary angiographyare contradictory.11–13Adenosine is a key mediator ofCIN and functions further upstream than oxygen-free
radicals (OFRs) and antioxidants.14–16Several clinicalstudies have investigated the competitive adenosine-antagonist theophylline as a prophylaxis.2,17–21Thesestudies either involved relatively small numbers ofpatients2,21 or the benefit was only detectable usingvery sensitive methods. Another recent study included100 high-risk patients22; it demonstrated a significantreduction in the incidence of CIN according to Bar-rett’s definition using a theophylline prophylaxis. Thisstudy was not restricted to patients who underwentcoronary angiography. We also investigated 100 pa-tients who underwent coronary angiography withlarger amounts of contrast medium (�100 ml). Inaddition to the evaluation of theophylline prophylaxis,the time course of 5 proteinuria markers and thepredictive value of several cardiac parameters and riskfactors of CIN were studied.
METHODSStudy design: Our institutional ethics review board
approved this study. Informed consent was obtainedfrom all patients. One hundred patients with stableserum creatinine of�1.3 mg/dl (114.4 mmol/L) wereprospectively randomized to receive either placebo
From the II. Medizinische Klinik, Institut fur Klinische Chemie, Institut furMedizinische Statistik und Epidemiologie and I. Medizinische Klinik,Klinikum Rechts der Isar, Technische Universitat Munchen, Munich,Germany. Manuscript received September 16, 2002; revised manu-script received and accepted January 29, 2003.
Address for reprints: Wolfgang Huber, MD, Klinikum Rechts derIsar, Intensivstation 2/11, Ismaningerstr. 22, D-81675 Munchen,Germany. E-mail: [email protected].
1157©2003 by Excerpta Medica, Inc. All rights reserved. 0002-9149/03/$–see front matterThe American Journal of Cardiology Vol. 91 May 15, 2003 doi:10.1016/S0002-9149(03)00259-5

(saline 0.9%; n � 50) or 200 mg theophylline (n �50). Placebo or theophylline were applied intrave-nously as a short infusion (100-ml saline, 0.9%) 30minutes before coronary angiography with �100 mlof the low osmolarity contrast medium iomeprol(Imeron 350, Byk-Gulden, Germany; osmolarity 618mosmol/kgH2O).
The stability of serum creatinine was verified bythe comparison of baseline values immediately beforecontrast medium with �1 “screening” value of thepreceding 2 days. Patients with a difference of �0.3mg/dl were excluded.
Further exclusion criteria were pregnancy or con-traindications to theophylline (history of seizures, ar-rhythmia resulting in circulatory instability, and/orLown classification of IVa or higher within 24 hours
before administration of contrast me-dium). Additional medications in-cluding diuretics or acetylsalicylicacid were not restricted. A fluid sup-ply of �2 L/day was advised. Addi-tional hydration was performed ac-cording to clinical examination, x-ray, and central venous pressures, ifavailable.
Evaluation criteria: Serum creati-nine and blood urea nitrogen weredetermined once between 48 and 12hours before (screening), immedi-ately before (baseline), and at 12,24, and 48 hours after administrationof contrast medium. Urinary excre-tion of N-acetyl-�-glucosaminidase(�-NAG), creatinine, total protein,
albumin, and �-1-microglobulin were determined 0, 4,12, and 24 hours after administration of contrast me-dium. The primary end point was the incidence of CIN(increase in serum creatinine of �0.5 mg/dl within 48hours after contrast medium).
Statistical analysis: Sample size (n � 100) wasestimated assuming a CIN incidence of 2% in thetheophylline group and of 24% in the placebo group,with a 2-sided 5% significance level and a power of80%. Dichotomous parameters were compared by chi-square test. The Wilcoxon test for unpaired sampleswas used to compare continuous parameters betweenthe treatment groups. The Wilcoxon test for pairedsamples was used to compare the follow-up values ofserum creatinine and the 5 proteinuria markers withthe respective baseline values before contrast medium.
The predictive value of risk factors according toTable 2 was evaluated by (1) comparison of the inci-dences (dichotomous parameters) and mean � SD(continuous parameters) among patients with andwithout CIN; and (2) multiple regression analysis(backward selection) with Y � maximum increase ofserum creatinine compared with baseline within 48hours; the continuous variables of age, weight, creat-inine, blood urea nitrogen, and Cigarroa quotient atbaseline; amount of contrast medium; and the dichot-omous (“yes/no” ) parameters of theophylline, diabe-tes, hypertension, nephrotoxic medication, protein-uria, impaired cardiac function, elevation of creatinekinase, elevation of troponin T, emergency angiogra-phy, acetylsalicylic acid, and diuretics. All statisticalanalysis was performed using SAS software (version6.12, SAS Institute, Cary, North Carolina).
RESULTSDemographic data and risk factors of the patients:
All patients were Caucasian and a mean age of 68.8 �11.1 years. The most frequent reasons for renal im-pairment were hypertensive (62%) or diabetic ne-phropathy (28%). Two patients had drug-induced re-nal impairment, and 8 patients had chronic renal fail-ure of unknown origin. Patients receiving theophyllineand the controls were comparable with regard to riskfactors for CIN, such as screening creatinine (1.67 �
TABLE 1 Incidence of Contrast-induced Nephropathy (CIN), Depending onAdditional Risk Factors (patients without medical prophylaxis)
Previously unimpaired renal function and no risk factors �1%Age �70 yrs9 21/183 11%Serum creatinine 1.5/mg/dl12* 10/91 11%Diabetes and serum creatinine 1.3/mg/dl4* 88/452 20%Serum creatinine �1.2, 75 ml of contrast medium5 9/42 21%Patients with Cigarroa quotient �56*† 6/21 21%Serum creatinine 2.8 mg/dl13* 15/61 25%Serum creatinine �1.5 mg/dl2* 6/20 30%Serum creatinine 2.55 mg/dl8* 17/55 31%Serum creatinine 1.56 mg/dl11* 13/29 45%Diabetes and mean serum creatinine of 5.9 mg/dl7* 1/42 50%
Data are presented as numbers and percentages.*These studies included only patients who underwent coronary angiography.†See Table 2.To convert from milligrams per deciliter to millimoles per liter, multiply by 88.4.
TABLE 2 Risk Factors for Contrast-induced Nephropathy(CIN)
Impaired renal function (serum creatinine �1.2 mg/dl*)Diabetes mellitus*Dehydration*High dose of contrast medium*
�2 ml contrast-medium/kg BWCigarroa quotient �5
Contrast medium (ml) � creatinine (mg/dl)/kg BW �5 (21% vs2% increase of creatinine �1 mg/dl; p �0.001)
Old age*Hypertonus*Intra-arterial contrast medium application*Heart insufficiency: NYHA class �III; EF �50%*Nephrotoxic medication*
NSAID*Diuretics*AminoglycosideVancomycinAmphotericin B
Repeated exposition to contrast medium*ProteinuriaPlasmocytoma/paraproteinuria
HyponatriemiaHypomagnesemia10
*Risk factors frequently found in patients who underwent coronaryangiography.
BW � body weight; EF � ejection fraction; NSAID � nonsteroidal anti-inflammatory drug; NYHA � New York Heart Association.
1158 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 MAY 15, 2003

0.42 vs 1.75 � 0.71 mg/dl, p � 0.41), baseline cre-atinine (1.65 � 0.41 vs 1.72 � 0.69 mg/dl, p � 0.41),baseline blood urea nitrogen (27.1 � 13.5 vs 27.1 �11.2 mg/dl, p � 0.46), amount of contrast medium(235 � 89 vs 261 � 139 ml, p � 0.45), and preva-lence of diabetes (28% vs 34%, p � 0.51) (Table 3).Mean baseline creatinine and screening creatinine lev-els were not significantly different for all patients(1.71 � 0.58 vs 1.68 � 0.57 mg/dl, p � 0.13) or forthe subgroups who received placebo (p � 0.29) ortheophylline (p � 0.32).
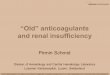
Primary end point: The incidence of CIN, accordingto Barrett’s definition, was significantly reduced from10 patients (20%) who received placebo to 2 patients(4%) who received theophylline prophylaxis (p �0.0138; Figure 1). Only 2 of the 12 patients with CINwere discharged with a serum creatinine as low orlower than before receiving the contrast medium (Fig-ure 2). Compared with baseline, mean serum creati-nine of the 12 patients with CIN was significantlyelevated at discharge (2.44 � 1.1 vs 2.13 � 1.3 mg/dl,p � 0.0207). Therefore, contrast-induced renal im-pairment for a prolonged period must be assumed.
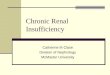
Secondary end points: Compared with baseline(1.72 � 0.69 mg/dl), mean creatinine significantlyincreased after using placebo at 12 hours (1.82 � 0.79mg/dl, p � 0.0057) (Figure 3), 24 hours (1.90 � 0.86mg/dl, p �0.0001), and 48 hours after administrationof contrast medium (1.90 � 0.89 mg/dl, p � 0.0007).With theophylline, mean creatinine levels were stable12 hours (1.65 � 0.43 mg/dl, p � 0.99) and 48 hoursafter receiving contrast medium (1.65 � 0.41 mg/dl, p� 0.99) compared with baseline (1.65 � 0.41 mg/dl).Mean serum creatinine levels were significantlyhigher (1.70 � 0.40 mg/dl, p � 0.029) only at 24hours after administration of contrast medium.
Complete proteinuria diagnosticswere performed in 66 patients (31 ontheophylline, 35 on placebo). Over-all, the time course was not differentwithin the 2 subgroups. The only dif-ference was a marginally significant(p � 0.046) increase in �-NAG ex-cretion after 4 hours in the patientswho received theophylline, whichwas not observed in the placebogroup. These 66 patients had a sig-nificant increase in �-NAG excretion4 (p � 0.022) and 24 hours (p �0.033) after administration of con-trast medium compared with base-line. Urinary creatinine levels signif-icantly decreased at 4 (p �0.0001 forall groups) and 12 hours after receiptof contrast medium. The total urinaryprotein and albumin excretions werestable at 4, 12, and 24 hours aftercontrast medium within all groups.Alpha-1-microglobulin excretionsignificantly increased 24 hours aftercontrast medium in all groups (p �0.004 placebo group; p � 0.018 theo-
phylline group; p � 0.00023 for all patients). Theexcretion of albumin and total protein did not signif-icantly change in either group.
Evaluation of predictive parameters: Of the 12 pa-tients with CIN, there were significantly more patientswho underwent emergency angiography (33% vs 5%,p � 0.0006), who had baseline elevations of troponinT (38% vs 6%, p � 0.0041) and creatine kinase (38%vs 8%, p � 0.01), who received contrast medium of�300 ml (50% vs 17%, p � 0.009), and who had aCigarroa quotient of �5 (83% vs 32%, p � 0.0006).Furthermore, the patients with CIN received signifi-cantly higher amounts of contrast medium (338 � 233vs 236 � 86 ml, p � 0.0474) and had a higher meanCigarroa quotient (9.9 � 8.0 vs 4.4 � 2.0, p � 0.002).Multiple regression analysis of the maximal increaseof serum creatinine after administration of contrastmedium demonstrated that receiving placebo insteadof theophylline was a significant risk factor (p �0.0055), providing additional evidence for the effec-tiveness of theophylline. Further significant predictorswere the Cigarroa quotient (p �0.0001) and increasedbaseline levels of troponin T (p � 0.018).
DISCUSSIONIn our study we demonstrated the prophylactic
effect of a single infusion of 200 mg theophylline 30minutes before administration of contrast medium by3 methods (reduced incidence of CIN, prevention ofan increase in mean serum creatinine levels after 12hours and 48 hours, and prophylactic effect in theregression analysis). The nephro-protective effect oftheophylline is due mainly to its glomerular adenosineantagonism. Contrast media osmotically irritate tubu-lus cells. This results in an increased adenosinetriphosphate turnover and the subsequent release of
TABLE 3 Demographic Data and Main Risk factors of the Patients
Placebo(n � 50)
Theophylline(n � 50) p Value
Age (yrs) 68.9 � 10.4 68.8 � 12.0 0.76Women/Men 11/39 (22/78%) 6/44 (12/88%) 0.06Body weight (kg) 80.3 � 14.8 80.2 � 12.8 0.92Baseline creatinine (mg/dl) 1.72 � 0.69 1.65 � 0.41 0.41Baseline blood urea nitrogen (mg/dl) 27.1 � 11.2 27.1 � 13.5 0.23Contrast medium (ml) 216.6 � 95.0 196.5 � 84.1 0.24
Range 100–530 100–500Diuretics 32 (64%) 40 (80%) 0.07Proteinuria (�150 mg/g creatinine) 28/46 (61%) 23/47 (49%) 0.25Systemic hypertension 47 (94%) 48 (96%) 0.56Diabetes mellitus 17 (34%) 14 (28%) 0.51Left ventricular ejection fraction
�55% 13 (26%) 13 (26%)35%–55% 23 (46%) 28 (56%)�35% 9 (18%) 7 (14%) 0.72
Calcium antagonists 9 (18%) 7 (14%) 0.59Creatine kinase elevated 6 (12%) 3 (6%) 0.29Troponin T elevated 4 (8%) 3 (6%) 0.70Glycohemoglobin elevated 14 (28%) 11 (22%) 0.16Emergency angiography 5 (10%) 3 (6%) 0.48Acetylcysteine �1,200 mg/d 0 0Acetylcysteine 600–900 mg/d 2 (4%) 2 4%)
Data are presented as mean � SD, numbers, or percentages.
CORONARY ARTERY DISEASE/EFFECTIVENESS OF THEOPHYLLINE PROPHYLAXIS 1159

adenosine.14,19 In contrast to other tissues in whichadenosine results in hyperemia, in the kidney, adeno-sine induces marked vasoconstriction of the vas affe-
rens via the adenosine-1-recep-tor.15,16,23–26 With an increase in re-nal impairment, the adenosine-mediated vasoconstriction alsoincreases.15,27 This may explain thelower preventive effect of theo-phylline in patients without severerenal impairment. The importance ofadenosine among other mediators ofCIN, such as OFRs,5,10–13,28,29 pros-taglandins, and angiotensin-convert-ing enzymes is further emphasizedby the finding that the inhibition ofadenosine re-uptake by dipyridamolesignificantly increases renal impair-ment by contrast media19 and leadsto a 70% depression of total renalperfusion.26 Our 200 mg dose oftheophylline is greater than theminimum dose required to block
renal vascular adenosine receptors.14,19,23–25 There-fore, we did not administer the dosage using a weight-based strategy. In previous studies, theophylline waseffective in dosages of 2.1 mg/kg IV,20 2.6 mg/kg IV22
and 2.88 mg/kg once daily.19 Assuming 90% gastro-intestinal absorption, the 2.88 mg/kg dosage is nearlyequivalent to our dosage of approximately 2.5 mg/kg.Nevertheless, considering the weight range of the pa-tients included in our study (50 to 130 kg), a weight-based dosing schedule should be applied in futurestudies. The plasma half-life of theophylline is about 7hours, which is longer than the half-life of contrastmedia in patients with normal or modestly impairedrenal function. However, in patients with severelyimpaired renal function, the half-life of contrast me-dium might be longer than that of theophylline. Inthese patients, a second dose of once daily or IVtheophylline might be beneficial.
In addition to the direct glomerular vasoconstric-tion caused by adenosine, adenosine metabolism toxanthin and hypoxanthin increases the generation ofOFRs.30 Thus, OFRs may act as “second messenger”of adenosine in the pathogenesis of CIN. An importantrole of OFRs in the pathogenesis of CIN has beenshown by several experimental studies28,29 and by theprophylactic effect of the antioxidant acetylcys-teine.5,11,13 Acetylcysteine was effective in patientswho received smaller amounts of contrast medium(between 75 and 117 ml)5,13 or in patients with mod-estly impaired renal function12 (mean serum creatinineof 1.61 mg/dl). The mean Cigarroa quotients in thesestudies were 2.9, 4.1, and 3.9, respectively. However,in a recent study that included 183 patients who re-ceived higher amounts of contrast medium (meanamount of 197 ml; mean Cigarroa quotient of 4),Briguori et al12 did not find any significant effect onthe occurrence of CIN with acetylcysteine treatment.In our study, theophylline prophylaxis reduced theincidence of CIN in patients with a mean Cigarroaquotient of 5.1 and who received a mean amount ofcontrast medium of 207 ml. However, the number ofpatients included in these studies and in our study are
FIGURE 1. Significant reduction in the incidence of CIN with theophylline prophylaxiscompared with placebo (4% vs 20%). p � 0.0138.
FIGURE 2. Time course of serum creatinine for the 12 patientswith CIN. *Compared with baseline, mean serum creatinine lev-els in these 12 patients were significantly elevated at discharge(2.44 � 1.1 vs 2.13 � 1.3 mg/dl; p � 0.0207). To convert val-ues for serum creatinine to micromoles per liter, multiply by88.4.
1160 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 MAY 15, 2003

too small to compare the prophylactic efficacy ofacetylcysteine and theophylline. Whether a prophy-laxis with acetylcysteine or a combination with the-ophylline is superior to theophylline alone, should bethe subject of further studies.
Proteinuria: In contrast to Barrett’s definition,changes in proteinuria were not strongly correlatedwith the clinical outcome of patients. Similarly toprevious studies,18,22 we found an increase in �-NAGrelease 4 and 24 hours after administration of contrastmedium. Due to the lower number of patients includedin the proteinuria part of our study, the 24-hour in-crease was only significant when examining all of thepatients. The increase of �-NAG excretion 4 hoursafter receipt of contrast medium was observed amongthe patients who received theophylline (p � 0.046)but not among the controls. This is in contrast to 2studies reporting that—in addition to the predomi-nantly glomerular protective effect of theophylline—
tubular protection also tookplace.18,22 One of these studies dem-onstrated a prevention of an increasein �-NAG release 48 and 72 hoursafter administration of contrast me-dium by theophylline.18 However,we did not examine proteinuria laterthan 24 hours after contrast mediumadministration. Furthermore, an in-crease in �-1-microglobulin excre-tion in both study groups demon-strated a tubular impairment, whichwas not affected by theophylline.The decrease in urinary creatinineexcretion can be explained mainlyby the osmo-diuretic effect of thecontrast medium itself. Additionally,a reduced glomerular filtration ratemight contribute to the decreasedurinary creatinine levels. However,additional markers of glomerulardamage, such as albumin and totalprotein excretion, did not change inany group.
Characterization of risk factors ofCIN: In addition to medical prophy-laxis and hydration, the character-ization of patients at risk and theminimization of risk factors mightbe crucial for the prevention of CIN.Among the most predictive parame-ters in our study were well-knownrisk factors, such as a high amountof contrast medium with a criticalthreshold of 300 ml and high Cigar-roa quotients. We found the samethreshold of Cigarroa quotient �5 tobe predictive as Cigarroa et al.6 Addi-tionally, elevated levels of troponin Twere predictive for both the maximalincrease in creatinine and the inci-dence of CIN according to Barrett’sdefinition. Elevated levels of troponin
T are not only found after myocardial impairment, butalso in patients with impaired renal function. To ourknowledge, these are the first data confirming a predic-tive value of this clinical chemical parameter, which isoften routinely determined in patients undergoing coro-nary angiography. Elevated levels of creatine kinasewere predictive only for the incidence of CIN, but not forthe maximal increase in creatinine.
In conclusion, theophylline is an effective and safeprophylaxis of CIN in high-risk patients with impairedrenal function undergoing coronary angiography. Itshould be used especially in patients receiving �300ml of contrast medium, in patients with an elevatedCigarroa quotient, and/or in patients with elevatedtroponin T concentrations.
1. Barrett BJ, Parfrey PS. Prevention of nephrotoxicity induced by radiocontrastagents. N Engl J Med 1994;331:1449–1450.
FIGURE 3. Time course of serum creatinine at different times after administration ofcontrast medium. p Values <0.05 indicate a significant difference compared withbaseline serum creatinine levles. To convert values for serum creatinine to micromolesper liter, multiply by 88.4.
CORONARY ARTERY DISEASE/EFFECTIVENESS OF THEOPHYLLINE PROPHYLAXIS 1161

2. Abizaid AS, Clark CE, Mintz GS, Dosa S, Popma JJ, Pichard AD, Satler LF,Harvey M, Kent KM, Leon MB. Effects of dopamine and aminophylline oncontrast-induced acute renal failure after coronary angioplasty in patients withpreexisting renal insufficiency. Am J Cardiol 1999;83:260–263.3. Levy EM, Viscoli CM, Horwitz RI. High mortality in contrast-associated renalfailure is not explained by comorbidity. J Am Soc Nephrol 1996;5:400.4. McCullough PA, Wolyn R, Rocher LL, Levin RN, O’Neill WW. Acute renalfailure after coronary intervention: incidence, risk factors, and relationship tomortality. Am J Med 1997;103:368–375.5. Tepel M, van der Giet M, Schwarzfeld C, Laufer U, Liermann D, Zidek W.Prevention of radiographic-contrast-agent-induced reductions in renal function byacetylcysteine. N Engl J Med 2000;343:180–184.6. Cigarroa RG, Lange RA, Williams Hillis LD. Dosing of contrast material toprevent contrast nephropathy in patients with renal disease. Am J Med 1989;86:649–652.7. Manske CL, Sprafka JM, Strony JT, Wang Y. Contrast nephropathy inazotemic diabetic patients undergoing coronary angiography. Am J Med 1990;89:615–620.8. Stevens MA, McCullough PA, Tobin KJ, Speck JP, Westveer DC, Guido-Allen DA, Timmis GC, O’Neill WW. A prospective trial of prevention measuresin patients at high risk for contrast nephropathy. J Am Coll Cardiol 1999;33:403–411.9. Rich MW, Crecelius CA. Incidence, risk factors and clinical course of acuterenal insufficiency after cardiac catheterization in patients 70 years and older.Arch Intern Med 1990;150:1237–1242.10. Katholi RE, Woods WT, Taylor GJ, Deitrick CL, Womack KA, Katholi CR,McCann WP. Oxygen free radicals and contrast nephropathy. Am J Kidney Dis1998;32:64–71.11. Diaz-Sandoval LJ, Kosowsky BD, Losordo DW. Acetylcysteine to PreventAngiography-Related Renal Tissue Injury (The APART Trial). Am J Cardiol2002;89:356–358.12. Briguori C, Manganelli F, Scarpato P, Elia PP, Golia B, Riviezzo G, LeporeS, Librera M, Villari B, Colombo A, Ricciardelli B. Acetylcysteine and contrastagent-associated nephrotoxicity. J Am Coll Cardiol 2002;40:298–303.13. Shyu K-G, Cheng J-J, Kuan P. Acetylcysteine protects against acute renaldamage in patients with abnormal renal function undergoing a coronary proce-dure. J Am Coll Cardiol 2002;40:1383–1388.14. Osswald H, Gleiter C. Renal effects of adenosine: possible consquences forkidney transplantation. Zentralbl Chir 1993;118:90–102.15. Arakawa K, Suzuki H, Naith M, Matsumoto A, Hayashi K, Matsuda H,Ichihara A, Kubota E, Saruta T. Role of adenosine in the renal responses tocontrast medium. Kidney Int 1996;49:1199–1206.16. Oldroyd SD, Fang L, Haylor JL, Yates MS, El Nahas AM, Morcos SK.Effects of adenosine receptor antagonists on the responses to contrast media in theisolated rat kidney. Clin Sci 2000;98:303–311.
17. Erley CM, Duda SH, Schlepckow S, Koehler J, Huppert PE, Strohmaier WL,Bohle A, Risler T, Osswald H. Adenosine antagonist theophylline prevents thereduction of glomerular filtration rate after contrast media application. Kidney Int1994;45:1425–1431.18. Erley CM, Duda SH, Rehfuss D, Scholtes B, Bock J, Muller C, Osswald H,Risler T. Prevention of radiocontrast-media-induced nephropathy in patients withpre-existing renal insuffiziency by hydration in combination with the adenosineantagonist theophylline. Nephrol Dial Transplant 1999;14:1146–1149.19. Katholi R, Taylor GJ, McCann WP, Woods WT, Womack KA, McCoy CD,Katholi CR, Moses HW, Mishkel GJ, Lucore CL, et al. Nephrotoxicity fromcontrast media: attenuation with theophylline. Radiology 1995;195:17–22.20. Kolonko A, Wiecek A, Kokot F. The nonselective adenosine antagonisttheophylline does prevent renal dysfunction induced by radiographic contrastagents. Journal of Nephrology 1998;11:151–156.21. Shammas NW, Kapalis MJ, Harris M, McKinney D, Coyne EP. Aminoph-ylline does not protect against radioconterast nephropathy in patients undergoingpercutaneous angiographic procedures. J Invasive Cardiol 2001;13:738–740.22. Huber W, Ilgmann K, Page M, Hennig M, Schweigart U, Jeschke B, LutilskyL, Weiss W, Salmhofer H, Classen M. The effect of theophylline on contrastmaterial-induced nephropathy in patients with chronic renal insufficiency: con-trolled, randomized, double-blinded study. Radiology 2002;223:772–779.23. Deray G, Martinez F, Cacoub P, Baumelou B, Baumelou A, Jacobs C. A rolefor adenosine, calcium and ischemia in radiocontrast-induced intrarenal vasocon-striction. Am J Nephrol 1990;10:316–322.24. Spielman WS. Antagonistic effect of theophylline on the adenosine-induceddecrease in renin-release. Am J Physiol 1984;247:F246–F251.25. Spielman WS, Arend LJ. Adenosine receptors and signaling in the kidney.Hypertension 1991;17:117–130.26. Tello R, Hartnell GG, Hill T, Volpe J, Finn JP, Cohen M. MR perfusionimaging of the kidney pre- and post-dipyridamole stress. J Magn Reson Imaging1996;6:460–464.27. Pflueger AC, Schenk F, Osswald H. Increased sensitivity of the renalvasculature to adenosine in streptozotocin-induced diabetes mellitus in rats. Am JPhysiol 1995;269:F529–F535.28. Bakris GL, Lass N, Gaber AO, Jones JD, Burnett JC. Radiocontrast medium-induced declines in renal function: a role for oxygen free radicals. Am J Physiol1990;258:F115–F120.29. Yoshioka T, Fogo A, Beckman JK. Reduced activity of antioxidant enzymesunderlies contrast-media-induced renal injury in volume depletion. Kidney Int1992;41:1008–1015.30. Xia Y, Khatchikian G, Zweier JL. Adenosine deaminase inhibition preventsfree radical-mediated injury in the postischemic heart. J Biol Chem 1996;271:10096–10102.
1162 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 91 MAY 15, 2003