Embed Size (px)
Citation preview
Dustin M. Ellinger BSN, MHA, RN
Rolf Consulting LLC
Emergency Preparedness: New CMS Rules for ICFs/IID
OHCA / OCID
August 24, 2017
So What’s New?
2012 Life Safety Code • Published: May 4, 2016 (S&C 16-22-LSC)
• Effective: July 5, 2016
• Implementation: November 1, 2016
Emergency Preparedness Rule• Published: September 16, 2016
• Effective: November 15, 2016
• Implementation: November 15, 2017
2012 LSC – References
2012 LSC – Key References
NFPA 101 (2012 ed.)• Life Safety Code Handbook
• Core Chapters (18/19 Health Care)
• Other chapters address means of egress, fire protection, etc.
NFPA 99 (2012 ed.) • Health Care Facilities Code Handbook (for Health Care Occupancies)
• Key Areas Addressed – Gas and Vacuum Systems, Electrical System, HVAC, Medical Gases, Fire Protection
• New Requirement for Risk Assessment
**Other References NFPA 10, NFPA 13, NFPA 25, NFPA 70,
NFPA 72, NFPA 80, NFPA 96, NFPA 110, NFPA 220
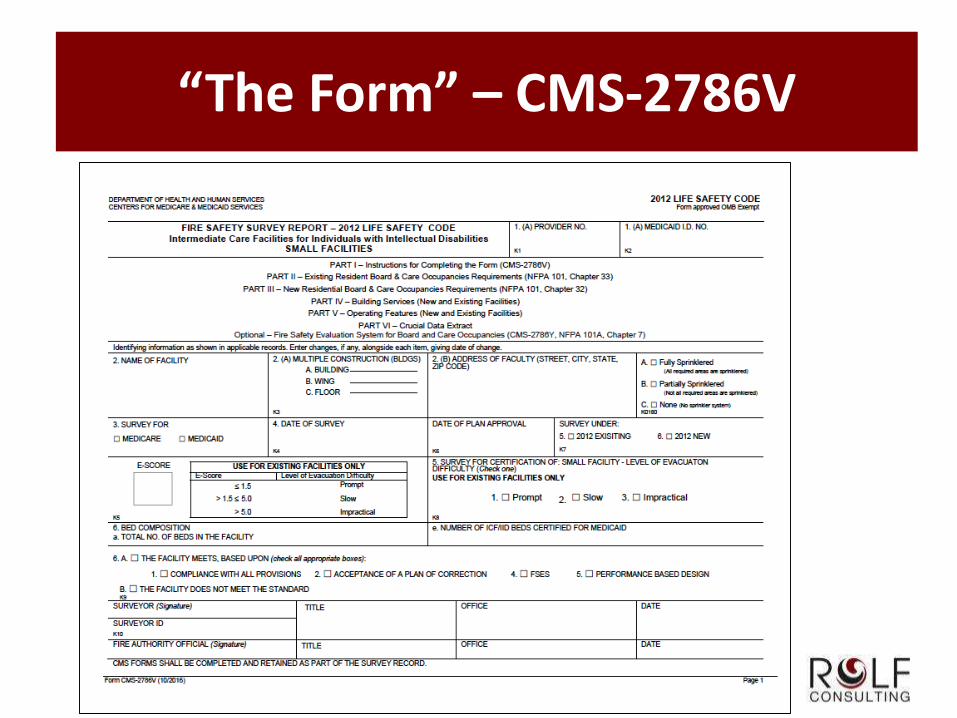
“The Form” – CMS-2786V
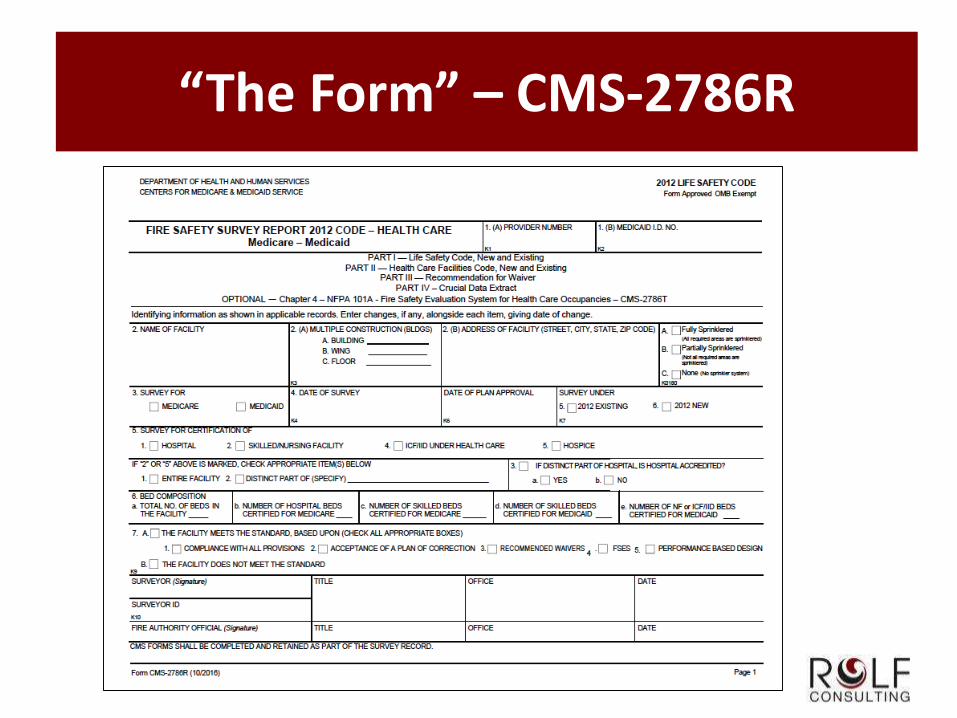
“The Form” – CMS-2786R
Procedural Changes
Fire Safety Evaluation System (FSES)
• Equivalency concept used in lieu of waivers
• “Grandfathered” buildings no-longer performed by ODH
• Approximately 40-50 buildings affected
• FSES required with annual LSC survey (qualified consultant)
The “Short Form”
• Used for Health Care Occupancy
• Not used as of September 1, 2016
• New process under consideration
Emergency Preparedness
Existing Health Requirements
• W438 – W439(CFR 483.70[h]) Standard: Emergency Plan
and Procedures
(1) The facility must develop and implement detailed written
plans and procedures to meet all potential emergencies and
disasters such as fire, severe weather, and missing clients.
(2) Must communicate, periodically review, make the plan
available, and provide training to the staff
Emergency Preparedness
Existing Health Requirements
• W440 – W451(CFR 483.70[i]) Standard: Evacuation Drills
(1) The facility must hold evacuation drills
• at least quarterly for each shift of personnel
• and under varied conditions
• to ensure all personnel on all shifts are trained to perform assigned tasks
• and ensure that all personnel on all shifts are familiar with the use of the
facility’s fire protection features
• and evaluate the effectiveness of emergency and disaster plans and
procedures
Emergency Preparedness
Existing Health Requirements (CFR 483.70[i], continued)
(2) The facility must
• actually evacuate clients during at least one drill each year on each shift
• make special provisions for the evacuation of clients with physical
disabilities
• file a report and evaluation of each evacuation drill
• investigate all problems with evacuation drills, including accidents
• and take corrective action
• during fire drills, clients may be evacuated to a safe area in facilities
certifed under health care occupancy chapter (18/19) of the Life Safety
Code.
(3) Live-in relief staff must meet quarterly drill requirement
Emergency Preparedness
Existing Health Requirements
• W451 - 439(CFR 483.70[j]) Standard: Fire Protection
(1) The facility must meet Life Safety Code (NFPA 101) health
care occupancy (18/19) or Residential Board and Care
(32/33)
(2) The survey agency may apply one or both occupancy
chapters
(3) Board and Care occupancies must have evacuation
capability evaluated
(4) applicability of state fire code
(5) Must comply with battery lighting (90 min) *
New Preparedness Rules
Emergency Preparedness Rule
Published in Federal Register on September 8, 2016
Effective November 15, 2016
Compliance Expected by November 15, 2017
Advanced Guidelines Published by CMS on June 2, 2017
CFR 483.475 – Condition of Participation: Emergency
Preparedness
• (a)Emergency Plan – based on risk assessment, all-hazards approach
• (b)Policies and Procedures – based on plan and risk assessment
• (c)Communication Plan – coordination of patient care internally and
externally, and communications with emergency officials
• (d)Training and Testing – initial and annual training, drills and exercises
and/or participate in actual incident that tests plan
Advanced Guidance (App. Z)
S&C 17-29-ALL
Published June 2, 2017
Interpretive Guidelines will be incorporated into the State
Operations Manual under Appendix Z
All 17 provider types listed in App. Z
Citations will be cited as “E” Tags (e.g., E0001 to E0044)
State agencies will decide whether evaluated by Health
or Life Safety Code surveyors
Questions about Emergency Preparedness Rule can be
sent to [email protected]
(a) Emergency Plan
Reviewed and Updated Annually
Community-based, all-hazards approach, including missing
residents
Based on risk assessment (slides to follow)
Population-specific
*Includes:
• continuity of operations
• delegations of authority
• succession plans
• cooperation with state & local leaders
*Templates available online
(b) Policies and Procedures
Subsistence needs for staff and clients, whether evacuating or
shelter
• food, water, medical, and pharmaceutical needs
Alternate sources of energy to
• maintain safe temperature, emergency lighting, fire suppression,
sewage/waste
System to track location of staff and residents
Evacuation (not just locations but “how to”) & transfer
agreements
Means to shelter in place for those remaining
Medical records documentation
Use of volunteers
1135 Waiver
(c) Communication Plan
Names and contact information for:
• Staff
• Entities providing services under arrangement
• Clients’ physicians
• Other ICFs/IID
• Volunteers Federal, state, regional emergency preparedness staff
• Licensing and certification agencies
• State protection and advocacy agencies
Primary and alternate means to contact staff / EMA entities
Method for sharing info with other care providers for continuity
Means to release information
Means of providing general condition and location info
Means of communicating with incident command center
Sharing info with residents / families
(d) Training & Testing
Initial and Annual Training (with documentation)
Unannounced staff drills
Full-scale community-based exercise (unless actual event activates
plan)
Second full-scale exercise or tabletop exercise, with after action
review
Integrated healthcare systems
• May participate in integrated program
• However, each certified facility must participate in development
• Must take into account each facility’s unique circumstances, population,
services
Training and Testing Memo
CMS S&C 17-21 ALL, published March 24, 2017
Training and Testing requirements expected to be fully
met by November 15, 2017
Includes both full-scale, community-based exercise and
tabletop exercise.
Note: CMS says they “understand that a full-scale
community-based exercise may not always be possible
for some providers and suppliers” and outlines provisions
for completing an individual facility-based eoercise with
documentation of why the community-based exercise
couldn’t be completed.
Follow “CMS S&C Policy and Memos to States”
Emergency Rule – FAQ
Continuity of Operations, Delegation of Authority, Succession
Planning
• No specific format or order required but plan must include these elements
• Resource provided below
• http://www.phe.gov/Preparedness/planning/hpp/reports/Documents/hc-
coop2-recovery.pdf (See FAQ #1)
Must be coordinated with local EMA officials – no “sign off”
Community involvement
• Check ODH website for list of existing coalitions
What does training encompass?
• Initial and Annual
• Exercises and Drills
• All Staff, but responsibilities may be delineated
Emergency Rule – FAQ
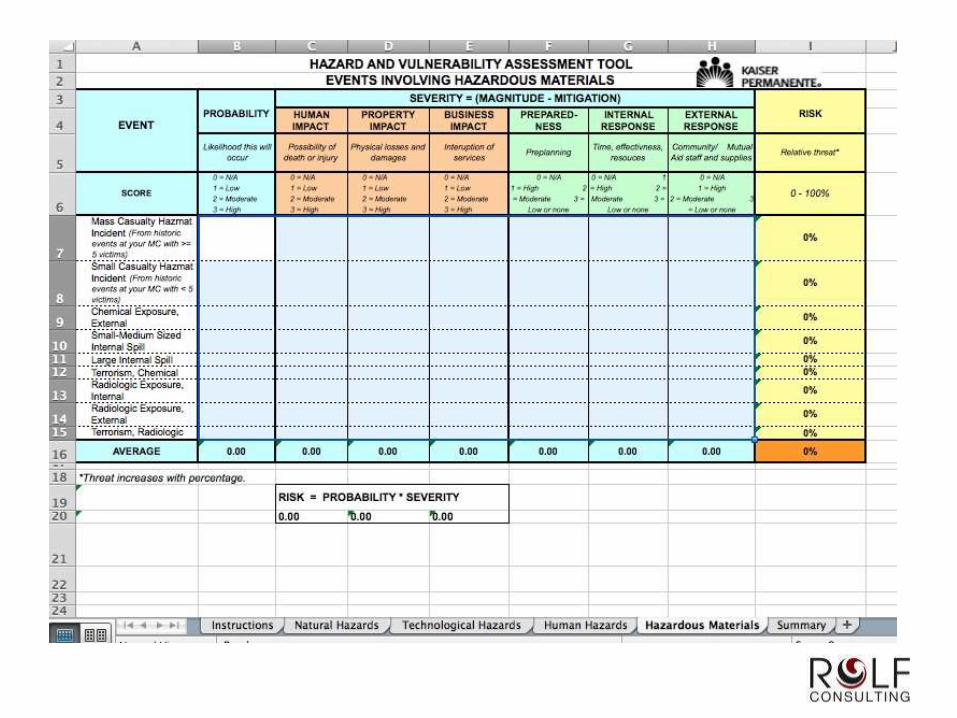
Hazard Vulnerability Assessment (HVA)
• All Hazard Approach
• No specific form recommended
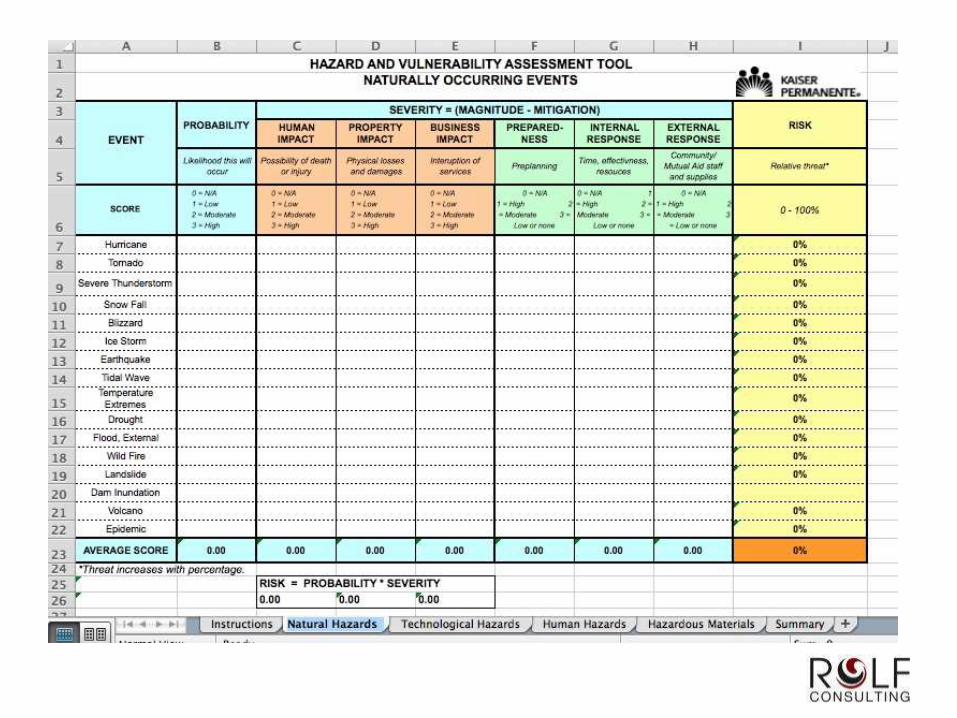
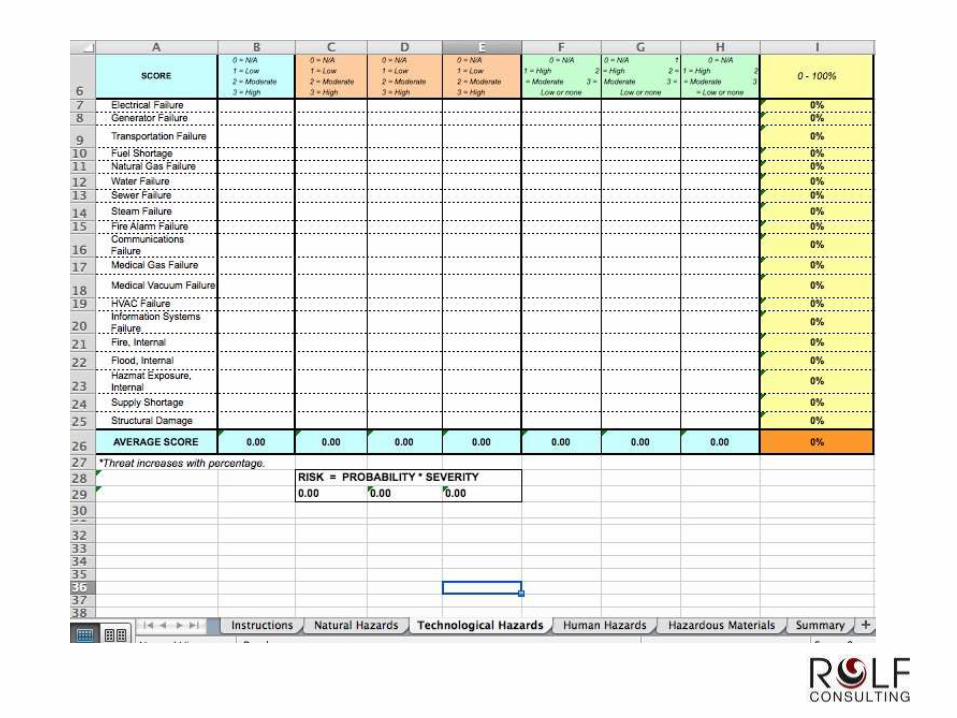
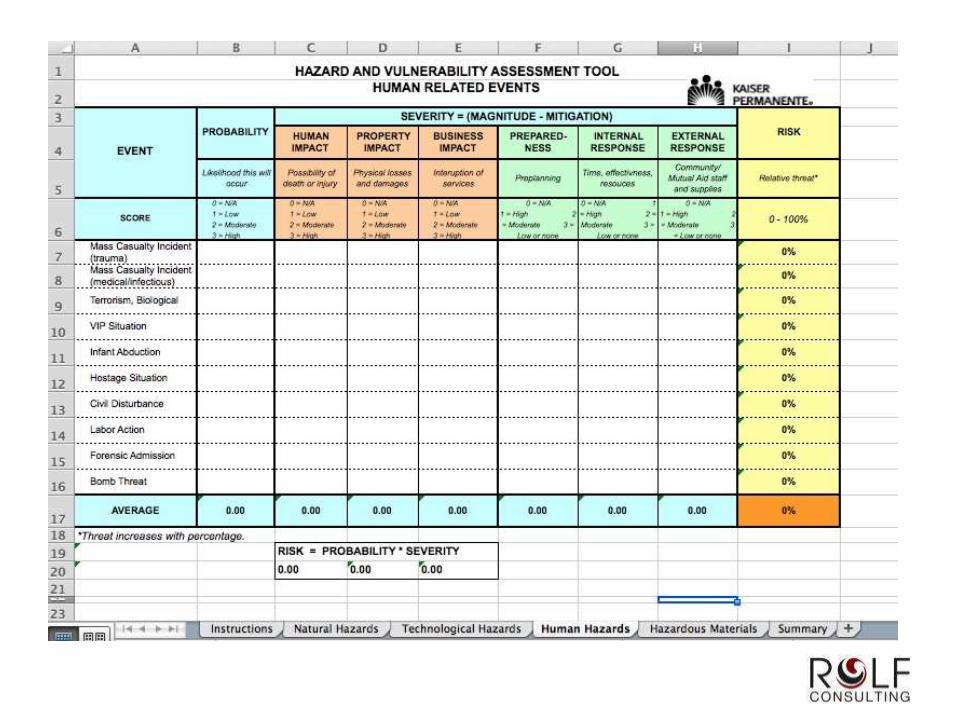
• Good example: Kaiser Permanente HVA
• http://www.calhospitalprepare.org/hazard-vulnerability-analysis
Typical HVA Components
• Natural Hazards
• Technological Hazards
• Human Hazards
• Hazardous Materials
Emergency Rule – FAQ
Generator for Hospitals, CAH, LTC – may be necessary to
power HVAC system (not explicit in other provider types)
Mandatory Generator vs. Mandatory Alternate Source
of Energy to Maintain Temperatures
• Alt energy source required to maintain temperatures to
protect individuals and storage of provisions
• Must be able to maintain temperatures in emergency
• Could involve heating and cooling in loss of power
• Need to evaluate during risk assessment
• ***NEW GUIDANCE PROVIDED IN APPENDIX Z***
Generator Clarification
This specific standard does not require facilities to have or install generators or any other specific type of energy source
Facilities must establish policies and procedures that determine how required heating and cooling of their facility will be maintained during an emergency situation, as necessary, if there were a loss of the primary power source
If portable generators used, should be operated, tested, and maintained in accordance with manufacturer, local and/or State requirements.
If permanent generator used, must meet NFPA
standards.
Emergency Rule – FAQ
Safe storage of “provisions” means food, water,
pharmaceuticals or medications and medical supplies
No specific quantities of medical supplies (e.g. xx days)
are specified.
Examples of facility or community-based exercises:
• Earthquake, Hurricane, Tornado, Flood
• Blizzard*
• Fire
• Cyber Attack
• Infectious Disease Outbreak
• Medical Surge
• Active Shooter
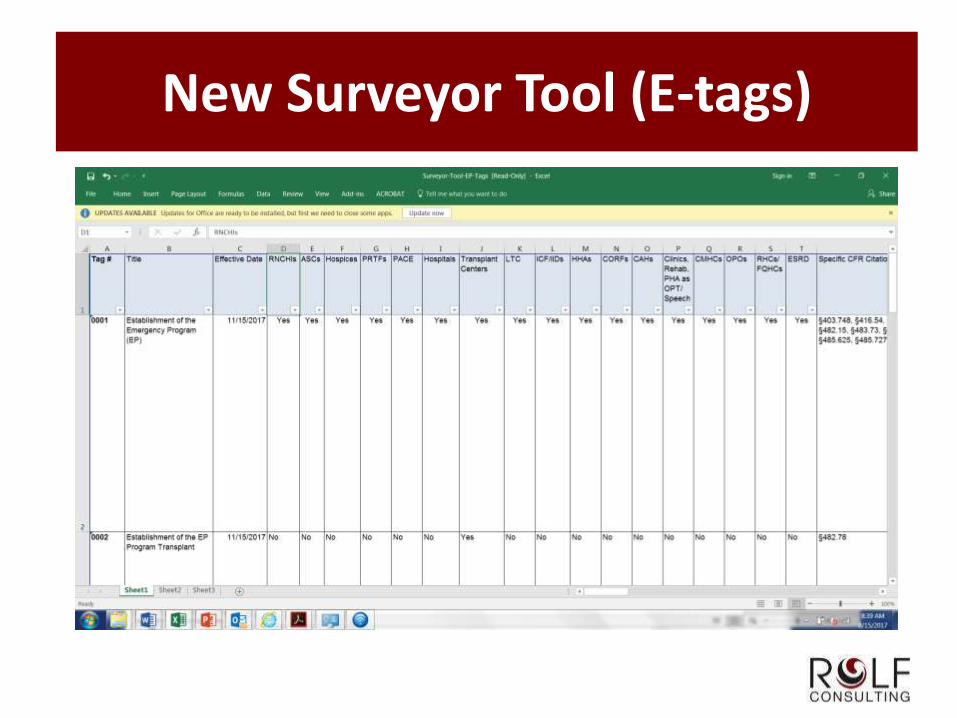
New Surveyor Tool (E-tags)
Other Resources
OHCA Website / Training Opportunities
“CMS Emergency Preparedness Rule” / Google for website
• Frequently Asked Questions
• Table of Requirements
• Hazard-specific guidance
• Templates and Checklists
Hazard Vulnerability Analysis Tools
• Provider / trade associations (e.g., AHCA)
• Many websites (e.g., Kaiser Permanente, OSHA, FEMA, etc.)
Incident Command System
• FEMA.gov “ICS Resource Center”
Technical Resources, Assistance Center and Information Exchange
• ASPR TRACIE www.asprtracie.hhs.gov

Questions?