Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Emotion recognition in children and adolescents withattention-deficit/hyperactivity disorder (ADHD)
Christina Schwenck • Thekla Schneider • Jutta Schreckenbach •
Yvonne Zenglein • Angelika Gensthaler • Regina Taurines •
Christine M. Freitag • Wolfgang Schneider • Marcel Romanos
Received: 31 January 2013 / Accepted: 23 February 2013 / Published online: 9 March 2013
� Springer-Verlag Wien 2013
Abstract Children with attention-deficit/hyperactivity
disorder (ADHD) are impaired in social adaptation and
display deficits in social competence. Deficient emotion
recognition has been discussed to underlie these social
problems. However, comorbid conduct problems have not
been considered in the majority of studies conducted so far,
and the influence of medication on emotion recognition has
rarely been studied. Here, emotion recognition perfor-
mance was assessed in children with ADHD without
medication compared with children with ADHD under
stimulant medication and a matched control group. In order
to rule out confounding by externalizing symptoms,
children with comorbid conduct problems were excluded.
Video clips with neutral faces developing a basic emotion
(happiness, sadness, disgust, fear and anger) were pre-
sented in order to assess emotion recognition. Results
indicated between-group differences neither concerning the
number of correctly identified emotions nor concerning
reaction times and their standard deviations. Thus, we
suggest that ADHD per se is not associated with deficits in
emotion recognition.
Keywords ADHD � Emotion recognition �Conduct problems � Stimulant medication �Psychopharmacotherapy
Introduction
Attention-deficit/hyperactivity disorder (ADHD) comprises
symptom clusters of inattention, hyperactivity and impul-
sivity. The disorder is rather common in childhood and
adolescents and affects about 5–12 percent of this age
group (Biederman and Faraone 2005; Schachar and Tan-
nock 1995). Psychopharmacotherapy with stimulant med-
ication such as methylphenidate is highly effective in
reducing the core symptoms and is recommended to be
applied in severe cases combined with behavioral thera-
peutic measures according to most existing guidelines
(Kendall et al. 2008).
Children with ADHD show a high rate of social prob-
lems, and reduced social competence was found to be
highly associated with the disorder (Lee et al. 2012). This
result was observed by self-ratings as well as in parent and
teacher ratings. More precisely, children with ADHD were
found to be less accepted by peers and they are perceived
as less socially competent than comparison groups (DuPaul
C. Schwenck � Y. Zenglein � A. Gensthaler � C. M. Freitag
Department of Child and Adolescent Psychiatry, Psychosomatics
and Psychotherapy, Goethe-University, Frankfurt/M., Germany
C. Schwenck � T. Schneider � R. Taurines � M. Romanos
Department of Child and Adolescent Psychiatry,
Psychosomatics and Psychotherapy, University of Wurzburg,
Wurzburg, Germany
C. Schwenck (&)
Klinik fur Psychiatrie, Psychosomatik und Psychotherapie des
Kindes- und Jugendalters Johann, Wolfgang Goethe-Universitat
Frankfurt/M., Deutschordenstraße 50 (Haus 92),
60528 Frankfurt a. M., Germany
e-mail: [email protected]
T. Schneider
Department of Psychology, University of Konstanz,
Constance, Germany
J. Schreckenbach � W. Schneider
Department of Psychology, University of Wurzburg,
Wurzburg, Germany
J. Schreckenbach
Department of Child and Adolescent Psychiatry, Psychosomatics
and Psychotherapy, University of Rostock, Rostock, Germany
123
ADHD Atten Def Hyp Disord (2013) 5:295–302
DOI 10.1007/s12402-013-0104-z

et al. 2004; Hoza et al. 2005). Furthermore, these problems
are known to be a significant predictor of serious negative
outcomes in later adolescence and adulthood (Greene et al.
1997; Mrug et al. 2012). Social problems were found at
higher rates in those individuals with ADHD who exhibit
comorbid externalizing disorders, such as conduct disorder
and oppositional defiant disorder (Booster et al. 2012). This
association is of particular relevance considering the large
percentage of children with ADHD showing symptoms of
conduct disorder and vice versa (Hinshaw 1987; King et al.
2005; Taurines et al. 2010). In regard to therapeutic options
for the treatment of social problems, pharmacological
treatment with methylphenidate was found to reduce these
problems in children and adolescents with ADHD to a
significant extent (Pelham et al. 2001), although surpris-
ingly, psychotherapeutic treatments such as social skills
trainings did not have an additional effect on social diffi-
culties of the children (Abikoff et al. 2004; Storebø et al.
2011). The poor effectiveness of psychotherapy on social
difficulties could be attributed to the fact that the core
deficiencies underlying social problems in ADHD have not
been identified so far and, therefore, were not targeted by
psychotherapeutic treatments.
Different factors linked to emotional processing have
been discussed to underlie the social malfunctioning of
children with ADHD. Among others, deficient emotion
recognition has been suggested to play a central role for
social malfunctioning (Dadds et al. 2012). According to the
model of the ‘‘violence inhibition mechanism’’ (VIM),
intact emotion recognition is required for the inhibition of
aggressive behavior, and deficiencies might lead to
aggressive reactions toward others (Blair et al. 2004). A
large number of studies have been conducted on emotion
recognition in ADHD so far, the majority showing defi-
ciencies in ADHD compared to controls (Taurines et al.
2012). This applies to a larger number of incorrect
responses in identifying an emotion (Singh et al. 1998),
higher reaction times (RT) (Kats-Gold et al. 2007), simple
emotion recognition in static pictures (Corbett and Glidden
2000; Yuill and Lyon 2007) as well as complex emotion
recognition in a social context (Fonseca et al. 2008). Some
of the studies found a deficient performance for specific
emotions, respectively, joy and surprise (Sinzig et al. 2008)
as well as anger (Singh et al. 1998), but other studies did
not differentiate for specific emotion dimensions (Cadesky
et al. 2000; Dyck et al. 2001).
Despite the large number of studies in this field of
research, important factors that may have a significant
influence on emotion recognition in children and adoles-
cents with ADHD have been neglected so far: first of all,
only one of the studies controlled for symptoms of conduct
problems (Cadesky et al. 2000). As children with ADHD
and comorbid conduct problems were found to show higher
rates of social problems (Booster et al. 2012), the
assumption that comorbid conduct problems might have an
influence on emotion recognition deficits seems to be
likely. The authors of the only study controlling for con-
duct problems (Cadesky et al. 2000) differentiated a group
with pure ADHD, a group with pure conduct problems, a
group with combined symptomatology and a control group
(CG). Surprisingly, results indicated that the groups with
ADHD only and conduct problems only were outperformed
by controls, although children with combined symptom-
atology did not differ from the CG. However, the authors
presented static pictures of emotional faces to their par-
ticipants, which allowed for evaluating the number of
correctly identified emotions/number of errors without any
reaction time information. Another problem of the pre-
sentation of static pictures to assess emotion recognition is
the low ecological validity: in social interaction of daily
life, facial expressions change rapidly and usually do not
maintain the same. Interestingly, the errors children with
ADHD made were random and comparable to controls, but
children with conduct problems specifically displayed high
error rates for the emotion ‘‘anger.’’ Further studies either
did not report comorbidity (Corbett and Glidden 2000;
Kats-Gold et al. 2007; Shapiro et al. 1993) or did not
consider comorbid disorders as independent factors in their
analyses (Fonseca et al. 2008; Sinzig et al. 2008; Yuill and
Lyon 2007). To our knowledge, in none of the studies,
conduct problems were an exclusion criterion. Therefore,
though externalizing comorbidity was found to have a large
influence on the degree of social problems in children with
ADHD (Booster et al. 2012), this factor has not been
considered by the majority of studies on emotion recog-
nition, and the only study (Cadesky et al. 2000) conducted
on this research question has not been replicated yet.
Second, only one previous study has investigated the
influence of stimulant medication on emotion recognition
performance (Hall et al. 1999). The authors of the study
compared a group with ADHD, a group with ADHD and
comorbid learning disorders, and a CG. Children with
ADHD were tested twice, once with medication and once
without. Results indicated no differences in the recognition
of emotions in human faces, neither between groups nor as
a function of medication. Again, a set of static pictures
showing different emotions was used in the study to
measure emotion recognition performance. The results of
the study seem to be surprising taking the positive influ-
ence of pharmacological treatment on social problems into
account (Pelham et al. 2001), and results have not been
replicated so far. All other studies either consistently tested
children without medication (Fonseca et al. 2008; Kats-
Gold et al. 2007; Sinzig et al. 2008; Yuill and Lyon 2007)
or do not report about the procedure in regard to medical
status (Shapiro et al. 1993; Singh et al. 1998).
296 C. Schwenck et al.
123

In summary, deficient emotion recognition may play an
important role in increased rates of social problems of
children and adolescents with ADHD. Although various
studies have been conducted reporting deficient emotion
recognition in patients with ADHD, important factors that
might influence emotion recognition have yet insufficiently
been accounted for. Therefore, the aim of the current study
is to assess emotion recognition performance in children
and adolescents with ADHD excluding comorbid conduct
problems to avoid confounding. Furthermore, we assess the
influence of psychopharmacological treatment on emotion
recognition performance. Based on previous research, we
expected to find deficient emotion recognition performance
in children with ADHD without medication compared to
controls. Due to the lack of studies on the influence of
stimulant medication on emotion recognition in children
with ADHD, no specific hypothesis was formulated, and
effects were assessed in an exploratory way. For our study,
we adopted a research paradigm with moving instead of
static emotional expressions, which, on the one hand,
allowed us to assess RT additionally to the number of
correctly identified emotions and, on the other hand, yiel-
ded a higher ecological validity. Past studies on looking
behavior in children with autism have shown substantial
differences in regard to the material—static pictures or film
clips—that had been applied, with differences primarily
found in studies with moving stimuli (Rice et al. 2012; Van
der Geest et al. 2002).
Methods
Participants
Participants were part of a large sample of children and
adolescent with different psychiatric disorders and a non-
clinical CG. The current study focuses on the subsample
(n = 84) of children, adolescents with ADHD (n = 56) and
participants without any psychiatric diagnosis (n = 28). A
part of the non-clinical CG served as CG in another publi-
cation (Schwenck et al. 2012). Children with ADHD were
recruited from the Department of Child and Adolescent
Psychiatry, University of Wurzburg, Germany, and through
local Child and Adolescent Psychiatrists. Children had been
assessed by mental health professionals. The standard
clinical assessment consisted of a clinical examination and
psychological tests. Furthermore, observational information
of the children’s behavior, objective tests as well as self-
reports, school and parent reports were considered in the
diagnostic process. Diagnoses of ADHD were made
according to DSM-IV TR criteria (314.00 and 314.01)
(American Psychiatric Association 2000), and 10 children
with combined type, 2 children with predominantly
hyperactive-impulsive type (ADHD-C) and 44 children
with predominantly inattentive type (ADHD-I) took part in
the study. Children of the CG had scores below the cutoff
for both clusters at the FBB-ADHD.
Most of the children (n = 47) in the clinical groups
were taking medication targeting ADHD symptomatol-
ogy, and only six participants were drug naıve. Children
of the clinical groups who were medically treated were
randomly asked either to take their medication or to taper
medication at least 24 h (48 h if medicated with extended
release methylphenidate) prior to testing. We decided to
use an independent study plan to avoid learning effects as
a consequence of repeated examinations and in order to
avoid drop outs due to motivational deficits which might
have resulted from an additional measurement point after
the clinical characterization and intelligence test and the
first trial of the emotion recognition task. All children
who were tested under medication were taking methyl-
phenidate in the recommended dose range and with sat-
isfying clinical effects, and one child was additionally
taking atomoxetine. One child of the group that was
tested without medication was usually taking dexamfeta-
mine, all other children, who were medically treated, were
taking methylphenidate. The diagnosis of conduct disor-
der/oppositional defiant disorder or autism served as an
exclusion criterion, because these disorders are known to
be associated with deficits in emotion recognition. The
CG was recruited by an ad in the local newspaper. All
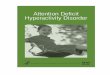
Table 1 Number of participants, gender, medication status (stimu-
lants or atomoxetine) and means (standard deviations) of age and IQ
in regard to group
Group
ADHD-
MED-
ADHD-
MED?
CG
n (girls/boys) 28 (9/19) 28 (9/19) 28 (9/19)
Currently treated with
ADHD-relevant
medication
19 28 0
Medication naive 6 0 28
Age (months) 148.43
(28.60)
147.75
(32.46)
149.93
(30.63)
IQ 105.89
(12.68)
100.46
(11.66)
103.93
(11.72)
FBB-ADHD inattention raw
sum (max. = 27)
18.41
(4.22)
19.49
(3.58)
3.88
(3.62)
FBB-ADHD hyperactivity/
impulsivity raw sum
(max. = 33)
9.92
(8.07)
13.55
(8.28)
3.66
(4.32)
ADHD-MED- attention-deficit/hyperactivity disorder no medication,
ADHD-MED? attention-deficit/hyperactivity disorder with medica-
tion, CG control group, FBB-ADHD observer rating scale for ADHD
Emotion recognition in ADHD 297
123

participants and their parents agreed to participate in the
study, and written informed consent was obtained from
parents. The study was approved by the local Ethics
Committee of the University of Wurzburg.
In total, the sample consisted of 84 children aged
8.2–17.3 years (mean age 12.39 years, SD = 2.52 years).
There were no group differences for age (F(2,81) = .04,
p = .964) or IQ (F(2,81) = 1.46, p = .238), measured with
the Wechsler Intelligence Scale for Children (Petermann
and Petermann 2007), and groups were matched for gender
and subtype. Descriptive statistics in regard to the number
of participants, medication status, age, IQ and ADHD
symptomatology are demonstrated in Table 1.
In regard to the FBB-ADHD, groups differed on the
scale inattention (F(2,80) = 142.37, p \ .001), and post hoc
tests indicated that the two clinical groups showed more
symptoms of inattention than the CG, although they did not
differ from each other. Furthermore, between-group com-
parisons showed differences in regard to the scale hyper-
activity/impulsivity (F(2,80) = 13.42, p \ .001). Again,
children of the two clinical groups showed more symptoms
of hyperactivity/impulsivity compared to the CG, although
they did not differ from each other.
Materials
Clinical assessment
Twenty-eight children with ADHD without medical treat-
ment (ADHD-MED-), 28 children with ADHD and
medical treatment (ADHD-MED?), and 28 typically
developing children (CG) participated in the current study.
All participants of the clinical group had been diagnosed
previously by experienced clinicians according to DSM-IV
TR criteria. The children were additionally assessed by the
following diagnostic measures:
Observer rating scale for ADHD (Dopfner et al. 2008)
The FBB-ADHD (translation: ‘‘observer rating scale for
ADHD’’) consists of 20 items containing symptoms of
inattention, hyperactivity and impulsivity based on the
diagnostic criteria of DSM-IV (American Psychiatric
Association 2000) and ICD-10 (World Health Organization
1993). Observers (in this study parents) have to rate each
item on a 0–3 point scale. Answers with scores of 2 or 3 are
evaluated as clinically relevant. A cutoff of 6 critically
answered items for each cluster of symptoms (inattention, 9
items; hyperactivity and impulsivity, 11 items) is recom-
mended for categorical diagnosis. Parents were instructed
to rate the behavior of their children as if they had not
taken their medication.
Child behavior checklist (Achenbach 1991)
The child behavior checklist (CBCL) is a parent-reported
measure for screening of child psychiatric symptomatology
and contains 113 items that have to be rated on a three-
point Likert scale. For this study, the broad-band categories
internalizing and externalizing problems as well as the total
score were used to exclude participants with psychiatric
symptoms of the non-clinical CG. Children from the CG
were excluded from the study if they had T-scores larger
than 63 in at least one of the broad-band categories or the
total score.
Assessment of emotion recognition: Morphing Task
(MT)
The MT is a self-developed task in which children were
shown 60 film clips each of 9-s length with a neutral facial
expression changing continuously to an emotional expres-
sion. Participants were supposed to press a key as soon as
they had recognized which emotion was presented and to
name the correct emotion. Stimuli were presented with the
computer program presentation (version 0.71), and RT and
the identified emotions were recorded.
Pictures from the Karolinska Directed Emotional Faces
Set (Lundqvist et al. 1998) served as stimulus material.
These pictures were found to be valid and reliable in past
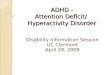
Table 2 Means (SD) of the dependent measures of the Morphing
Task
ADHD-MED- ADHD-MED? CG
Reaction times in ms
Happiness 3,681 (594) 3,537 (781) 3,773 (685)
Sadness 6,822 (1,245) 6,806 (1,360) 6,684 (1,575)
Disgust 5,634 (1,054) 5,407 (1,065) 5,401 (939)
Fear 7,380 (1,794) 7,069 (1,749) 7,194 (1,633)
Anger 7,216 (1,220) 7,112 (1,662) 7,277 (2,170)
Standard deviations of reaction times
Happiness 933 (313) 862 (369) 978 (485)
Sadness 2,100 (657) 2,258 (1,232) 2,274 (1,500)
Disgust 1,487 (522) 1,566 (727) 1,619 (1,074)
Fear 2,353 (846) 2,875 (2,239) 2,750 (1,714)
Anger 2,094 (730) 2,448 (1,704) 2,679 (2,593)
Number of correctly identified emotions (max. = 12)
Happiness 11.86 (.45) 11.89 (.32) 11.78 (.64)
Sadness 8.36 (2.60) 8.89 (2.22) 8.67 (1.75)
Disgust 6.50 (2.93) 6.71 (2.85) 6.79 (2.69)
Fear 7.54 (2.95) 7.71 (3.17) 7.07 (3.11)
Anger 9.61 (1.81) 9.29 (2.05) 9.64 (1.79)
ADHD-MED- ADHD without medication, ADHD-MED? ADHD
with medication, CG control group
298 C. Schwenck et al.
123

research (Goeleven et al. 2008). In the current study, we
selected a neutral and an emotional picture of 30 different
individuals and morphed the neutral expression to the
emotional one using the computer program Winmorph
3.01. The target emotions were anger, happiness, sadness,
fear and disgust, and we produced six different films for
each emotion. All film clips were presented twice, and
within each episode, we used a random order of film clips
that was the same for all participants. RT, standard devi-
ations of reaction times (SDRT) and the number of correctly
identified emotions (NC) within each emotional category
served as dependent measures.
Prior to the presentation of the target stimuli, we pre-
sented ten stimuli without any facial expression but geo-
metric figures (e.g. circle, triangle) changing into animals
(e.g. elephant, duck). Employing this procedure, we were
able to ensure that between-group differences on RT were
specific to emotion recognition in human faces of the target
films.
Results
Means and standard deviations of the dependent measures
are presented in Table 2, and correlation analyses of the
dependent variables are provided in Table 3. Descriptively,
clear ceiling effects can be observed for the number of
correctly identified happy facial expressions, which were
identified with the smallest RT and SDRT by all groups.
Whereas children reacted most slowly to angry and fearful
facial expressions, they conducted the highest number of
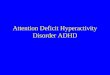
errors at the identification of disgusted expressions. Small
to medium intercorrelations were found for reaction time
measures, whereas intercorrelations between the numbers
of correctly identified emotions revealed not existent to
small.
Initial examination of the dependent measures indicated
that all RT measures were normally distributed (KS tests: all
p [ .05). Therefore, groups were compared by planned
contrasts according to the hypothesis (ADHD-MED-
[ ADHD-MED? = CG) in regard to mean RT within each
emotional category. Prior analysis of variance (ANOVA) of
the control items did not result in any RT differences
between groups (F(2,81) = 1.57, p = .214). Therefore, all
potential between-group differences of the test items could
be attributed to the emotional content of the stimuli.
Between-group comparisons indicated comparable emotion
recognition performances for the groups ADHD-MED?,
ADHD-MED- and the CG for the emotion happiness
(t(81) = -1.19, p = .237), sadness (t(81) = .16, p =
.871), disgust (t(81) = -.47, p = .641), fear (t(81) = -.55,
p = .586) and anger (t(81) = -.34, p = .738).
Examination of the distribution of SDRT and the NC
indicated that empirical data significantly differed from
normal distribution for almost all emotional categories.
Therefore, Kruskal–Wallis tests were conducted to com-
pare groups. According to the results of these between-
group comparisons, groups did not differ in SDRT for the
emotions happiness (v2(2) = 1.26, p = .533), sadness
(v2(2) = .62, p = .732), disgust (v2(2) = .01, p = .997),
fear (v2(2) = .36, p = .837) and anger (v2(2) = .04,
p = .978). The same applies for the NC, where there were
no between-group differences for happiness (v2(2) = .32,
p = .854), sadness (v2(2) = .94, p = .627), disgust
(v2(2) = .15, p = .926), fear (v2(2) = .60, p = .742) and
anger (v2(2) = .57, p = .752).
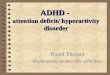
Finally, the relative number of confusions of happiness,
sadness, fear, disgust and anger with the respective other
emotions was compared between groups. Percentages of
actual and identified emotions by group are presented in
Table 4.
Results indicate that groups equally confused happy,
disgusted, fearful and angry facial expressions with all
respective other emotions (all p [ .05). However, there
was a small between-group difference in actual sad facial
expressions identified as angry facial expressions
(F(2,79) = 3.14, p = .049, g2 = .07). Descriptively, chil-
dren of the group ADHD-MED? mistook sad faces less
commonly as angry faces than the group ADHD-MED-.
However, an alpha-corrected post hoc test was only mar-
ginally significant (p = .054).
Discussion
The aim of the current study was to assess emotion rec-
ognition performance in children and adolescents with
Table 3 Correlation analyses of dependent measures reaction times
and number of correctly identified emotions
Happiness Sadness Disgust Fear Anger
Reaction times (ms)
Happiness – .51** .44** .50** .45**
Sadness – .67** .58** .70**
Disgust – .66** .76**
Fear – .60**
Anger –
Number correct
Happiness – .18 .19 .24* .20
Sadness – -.09 .23* -.07
Disgust – .32** .24*
Fear – .12
Anger –
* p \ .05, ** p \ .01
Emotion recognition in ADHD 299
123

ADHD without comorbid conduct disorder or oppositional
defiant disorder and to evaluate the influence of medication
on emotion recognition performance, as emotion recogni-
tion had been shown to be associated with social func-
tioning (Blair et al. 2004; Dadds et al. 2012). A task with
moving instead of static facial expressions was adopted in
order to assess the speed and its variation of the identifi-
cation additionally to the number of correctly identified
emotions and to adopt a measure of high ecological
validity.
No differences were found between children with
ADHD without medication and a non-clinical CG matched
for age, gender and IQ, neither in regard to RT nor in
regard to the variation of the RT or the number of correctly
identified emotions. This result applies for all basic emo-
tions assessed in this study: happiness, sadness, disgust,
fear and anger. These findings are in contrast to most
previous studies (Fonseca et al. 2008; Kats-Gold et al.
2007; Singh et al. 1998; Taurines et al. 2012). A possible
reason for distinct findings may be the use of short film
clips with moving faces rather than static pictures that the
majority of studies had used before. Because emotions
have to be recognized within short time spans in every day
life, we assumed a higher ecological validity in material
with moving faces. Emotion recognition in moving faces
and under time pressure may thus be more difficult than
under conditions with static pictures and without time
constrictions, and past studies on children with autism and
controls have shown differences only when film clips had
been applied, whereas with static pictures, no differences
have been found (Rice et al. 2012; Van der Geest et al.
2002). However, this assumption may have been incorrect,
and the use of distinct material may account for the non-
finding. On the other hand, we did not detect any floor
effects in the number of correctly identified emotions for
neither emotion and, on the contrary, showed ceiling
effects in the identification of happiness. Therefore, this
aspect seems rather unlikely to be responsible for the dif-
fering results. Future studies may directly compare emotion
recognition in materials with static facial expressions and
film clips to bring light into this methodological issue.
Furthermore, the application of eye tracking technology
would shed light on possible differences in the exact
looking and fixation behavior of children with ADHD
compared to other groups. Though this technology is pri-
marily used under laboratory conditions, as future pros-
pects, it would be a tremendous progress to develop the
possibility of eye tracking in the field and therefore every
day life of the children.
Another difference between our study and others is the
exclusion of children with a comorbid conduct disorder or
oppositional defiant disorder. According to recent research
(Booster et al. 2012), social problems of children with
ADHD are particularly high if externalizing disorders are a
comorbid condition. Only one study on emotion recogni-
tion accounted for conduct problems (Cadesky et al. 2000),
and the results were inconclusive, because the groups with
either ADHD or conduct disorder underperformed in the
emotion recognition task, but children with combined
disorders did not differ from healthy controls. In our study,
we treated conduct problems as an exclusion criterion. Our
non-finding in light of the previous investigations may
indicate that conduct problems more than ADHD-associ-
ated functions could be responsible for emotion recognition
deficiencies. However, further studies with specific
research designs are needed to prove this assumption and
replicate our results.
Furthermore, we did not find any influence of medica-
tion on emotion recognition performance. We had decided
to apply an independent study plan with comparable, but
different groups tested with or without medication. We did
that in order to avoid learning effects by repeated mea-
surements of the same tests. However, this procedure might
have led to a larger between-group error variance, which
we could have avoided by dependent groups and by a
counterbalanced measurement procedure. On the other
hand, a comparable study used a dependent and counter-
balanced study plan to assess the influence of medication
Table 4 Actual and identified emotions (in %) by group
Actual emotion Identified as
Happiness Sadness Disgust Fear Anger
ADHD-MED-
Happiness 98.81 .60 .30 .30 .00
Sadness 1.19 69.64 9.82 14.58 4.76
Disgust 2.08 14.58 54.17 2.38 26.79
Fear 3.27 5.36 26.49 62.80 2.08
Anger .60 12.20 3.57 3.57 80.06
ADHD-MED?
Happiness 99.11 .60 .00 .30 .00
Sadness 2.38 74.11 9.23 13.10 1.19
Disgust 5.06 10.12 55.95 1.79 27.08
Fear 4.17 4.76 24.70 64.29 2.08
Anger .30 12.80 5.95 3.57 77.38
CG
Happiness 98.15 .93 .00 .00 .93
Sadness 1.85 72.22 10.19 11.73 4.01
Disgust 3.27 13.10 56.55 2.08 25.00
Fear 4.17 6.55 27.98 58.93 2.38
Anger .30 10.42 6.55 2.38 80.36
Bold values indicate percentage of correctly identified faces by
emotion and group
ADHD-MED- ADHD without medication, ADHD-MED? ADHD
with medication, CG control group
300 C. Schwenck et al.
123

on emotion recognition and did not find any differences
either (Hall et al. 1999). So, it might be concluded that
medical treatment affects the core deficits of ADHD but
does not influence peripheral domains that are rather intact.
The positive effects of methylphenidate on social problems
found in previous studies seem to positively affect basic
processes other than emotion recognition. Of course, this
interpretation is speculative, and more research is neces-
sary to confirm this assumption and to replicate the findings
of our study.
There are general limitations of our study that we would
like to mention: first, we treated comorbid conduct prob-
lems as an exclusion criterion but did not include a group
of children with pure conduct disorder and without any
ADHD symptomatology or a group with combined disor-
ders. Our interpretation that conduct problems might be
more responsible for emotion recognition deficiencies than
ADHD symptomatology is rather indirect, and a study that
compares all three groups with a CG would be helpful to
confirm our interpretation. Furthermore, as already men-
tioned, a dependent study plan might have reduced error
variance in the assessment of the influence of medication.
Finally, the administration of participants to the two clin-
ical groups was not perfectly random. Nine participants
were not pharmacologically treated when the study was
conducted. These children were administered to the group
ADHD-MED-. All other children (n = 47) were ran-
domly assigned. This procedure might have influenced
results. Furthermore, the majority of our participants were
diagnosed with ADHD predominantly inattentive subtype.
This has to be kept in mind because results can be gen-
eralized only in regard to this proportion that is not
representative.
Keeping these limitations in mind, the present study
provides continuative insights into research on emotion
recognition ability in children and adolescents with
ADHD and a CG. To our knowledge, this study for the
first time assessed emotion recognition in ADHD and the
influence of medical treatment adopting a research para-
digm of high ecological validity and controlling for
comorbid conduct problems. In our study, we did not find
any between-group differences neither for the factor
group nor for the factor medication. Groups did not differ
in regard to the number of correctly identified emotions,
RT or the variability of RT. Unlike other studies on this
field of research, we had defined conduct problems as an
exclusion criterion, which might have led to these dif-
fering results. As social problems are known to strongly
predict negative outcomes in later adolescence and
adulthood (Greene et al. 1997; Mrug et al. 2012), we
believe that it is important to study possible underlying
deficient processes such as emotion recognition but also
others such as emotion regulation in future research and
to assess the differential influence ADHD symptomatol-
ogy and comorbid disorders have on these processes, as
deficits in emotion recognition might not be associated
with ADHD symptomatology per se.
Acknowledgments We thank all participants and their families for
their participation in the study. Our sincere thanks go to all colleagues
from collaborating institutes for their cooperation and support.
References
Abikoff H, Hechtman L, Klein RG et al (2004) Social functioning in
children with ADHD treated with long-term methylphenidate
and multimodal psychosocial treatment. J Am Acad Child
Adolesc Psychiatry 43:820–829. doi:10.1097/01.chi.0000128
797.91601.1a
Achenbach TM (1991) Manual for the child behavior checklist/4-18
and 1991 profile. University of Vermont, Burlington
American Psychiatric Association (2000) Diagnostic and statistical
manual of mental disorders (DSM-IV), 4(null) ed. American
Psychiatric Press, Washington
Biederman J, Faraone SV (2005) Attention-deficit hyperactivity
disorder. Lancet 366:237–248
Blair RJR, Mitchell DGV, Peschardt KS et al (2004) Reduced
sensitivity to others’ fearful expressions in psychopathic indi-
viduals. Pers Individ Differ 37:1111–1122. doi:10.1016/
j.paid.2003.10.008
Booster GD, DuPaul GJ, Eiraldi R, Power TJ (2012) Functional
impairments in children with ADHD: unique effects of age and
comorbid status. J Atten Disord 16:179–189. doi:10.1177/10870
54710383239
Cadesky EB, Mota VL, Schachar RJ (2000) Beyond words: how do
children with ADHD and/or conduct problems process nonverbal
information about affect? J Am Acad Child Adolesc Psychiatry
39:1160–1167
Corbett B, Glidden H (2000) Processing affective stimuli in children
with attention-deficit hyperactivity disorder. Child Neuropsychol
(Neuropsychology, Development and Cognition: Section C)
6:144–155. doi:10.1076/chin.6.2.144.7056
Dadds MR, Cauchi AJ, Wimalaweera S et al (2012) Outcomes,
moderators, and mediators of empathic-emotion recognition
training for complex conduct problems in childhood. Psychiatry
Res 199:201–207. doi:10.1016/j.psychres.2012.04.033
Dopfner M, Gortz-Dorten A, Lehmkuhl G et al (2008) Diagnostik-
System fur psychische Storungen nach ICD-10 und DSM-IV fur
Kinder und Jugendliche-II (DISYPS-II). Huber, Bern
DuPaul GJ, Volpe RJ, Jitendra AK et al (2004) Elementary school
students with AD/HD: predictors of academic achievement.
J Sch Psychol 42:285–301. doi:10.1016/j.jsp.2004.05.001
Dyck MJ, Ferguson K, Shochet IM (2001) Do autism spectrum
disorders differ from each other and from non-spectrum
disorders on emotion recognition tests? Eur Child Adolesc
Psychiatry 10:105–116
Fonseca D, Seguier V, Santos A et al (2008) Emotion understanding
in children with ADHD. Child Psychiatry Hum Dev 40:111–121.
doi:10.1007/s10578-008-0114-9
Goeleven E, De Raedt R, Leyman L, Verschuere B (2008) The
Karolinska directed emotional faces: a validation study. Cogn
Emot 22:1094–1118. doi:10.1080/02699930701626582
Greene RW, Biederman J, Faraone SV et al (1997) Adolescent
outcome of boys with attention-deficit/hyperactivity disorder and
social disability: results from a 4-year longitudinal follow-up
study. J Consult Clin Psychol 65:758
Emotion recognition in ADHD 301
123

Hall CW, Peterson AD, Webster RE et al (1999) Perception of
nonverbal social cues by regular education, ADHD, and ADHD/
LD students. Psychol Sch 36:505–514
Hinshaw SP (1987) On the distinction between attentional deficits/
hyperactivity and conduct problems/aggression in child psycho-
pathology. Psychol Bull 101:443
Hoza B, Mrug S, Gerdes AC et al (2005) What aspects of peer
relationships are impaired in children with attention-deficit/
hyperactivity disorder? J Consult Clin Psychol 73:411–423. doi:
10.1037/0022-006X.73.3.411
Kats-Gold I, Besser A, Priel B (2007) The role of simple emotion
recognition skills among school aged boys at risk of ADHD.
J Abnorm Child Psychol 35:363–378. doi:10.1007/s10802-
006-9096-x
Kendall T, Taylor E, Perez A et al (2008) Diagnosis and management of
attention-deficit/hyperactivity disorder in children, young people,
and adults: summary of NICE guidance. BMJ 337:a1239. doi:
10.1136/bmj.a1239
King S, Waschbusch DA, Frankland BW et al (2005) Taxonomic
examination of ADHD and conduct problem comorbidity in
elementary school children using cluster analyses. J Psychopathol
Behav Assess 27:77–88. doi:10.1007/s-10862-005-5382-0
Lee SS, Falk AE, Aguirre VP (2012) Association of comorbid anxiety
with social functioning in school-age children with and without
attention-deficit/hyperactivity disorder (ADHD). Psychiatry Res
197:90–96. doi:10.1016/j.psychres.2012.01.018
Lundqvist D, Flykt A, Ohman A (1998) The Karolinska directed
emotional faces. Karolinska Institute, Department of Clinical
Neuroscience, Stockholm
Mrug S, Molina BSG, Hoza B et al (2012) Peer rejection and
friendships in children with attention-deficit/hyperactivity disor-
der: contributions to long-term outcomes. J Abnorm Child
Psychol 40:1013–1026. doi:10.1007/s10802-012-9610-2
Pelham WE Jr, Waschbusch DA, Hoza B et al (2001) Effects of
methylphenidate and expectancy on performance, self-evalua-
tions, persistence, and attributions on a social task in boys with
ADHD. Exp Clin Psychopharmacol 9:425
Petermann F, Petermann U (2007) Hamburg-Wechsler-Intelligenztest
fur Kinder (HAWIK-IV). Hogrefe, Gottingen
Rice K, Moriuchi JM, Jones W, Klin A (2012) Parsing heterogeneity
in autism spectrum disorders: visual scanning of dynamic social
scenes in school-aged children. J Am Acad Child Adolesc
Psychiatry 51:238–248. doi:10.1016/j.jaac.2011.12.017
Schachar R, Tannock R (1995) Test of four hypotheses for the
comorbidity of attention-deficit hyperactivity disorder and
conduct disorder. J Am Acad Child Adolesc Psychiatry 34:
639–648
Schwenck C, Mergenthaler J, Keller K et al (2012) Empathy in
children with autism and conduct disorder: group-specific
profiles and developmental aspects. J Child Psychol Psychiatry
53:651–659
Shapiro EG, Hughes SJ, August GJ, Bloomquist ML (1993)
Processing of emotional information in children with attention-
deficit hyperactivity disorder. Dev Neuropsychol 9:207–224.
doi:10.1080/87565649309540553
Singh SD, Ellis CR, Winton ASW et al (1998) Recognition of facial
expressions of emotion by children with attention-deficit hyper-
activity disorder. Behav Modif 22:128–142. doi:10.1177/0145
4455980222002
Sinzig J, Morsch D, Lehmkuhl G (2008) Do hyperactivity, impulsiv-
ity and inattention have an impact on the ability of facial affect
recognition in children with autism and ADHD? Eur Child
Adolesc Psychiatry 17:63–72. doi:10.1007/s00787-007-0637-9
Storebø OJ, Skoog M, Damm D et al (2011) Social skills training for
attention deficit hyperactivity disorder (ADHD) in children aged
5 to 18 years. Cochrane Database Syst Rev 7(12):8223
Taurines R, Schmitt J, Renner T et al (2010) Developmental
comorbidity in attention-deficit/hyperactivity disorder. Atten
Def Hyperact Disord 2:267–289. doi:10.1007/s12402-010-
0040-0
Taurines R, Schwenck C, Westerwald E et al (2012) ADHD and
autism: differential diagnosis or overlapping traits? A selective
review. Atten Defic Hyperact Disord 4:115–139. doi:10.1007/
s12402-012-0086-2
Van der Geest JN, Kemner C, Verbaten MN, Van Engeland H (2002)
Gaze behavior of children with pervasive developmental disor-
der toward human faces: a fixation time study. J Child Psychol
Psychiatry 43:669–678
World Health Organization (1993) The ICD-10 classification of
mental and behavioural disorders: diagnostic criteria for
research. World Health Organization, Geneva
Yuill N, Lyon J (2007) Selective difficulty in recognising facial
expressions of emotion in boys with ADHD. Eur Child Adolesc
Psychiatry 16:398–404. doi:10.1007/s00787-007-0612-5
302 C. Schwenck et al.
123