Embed Size (px)
DESCRIPTION
ENA Connection 2012
Citation preview
If You Build It, They Will Drum
the Official Magazine of the Emergency Nurses Association
December 2012 Volume 36, Issue 11
connection
Members in Motion: Emergency Nurse From Kentucky Wins Top Magnet Honor PAGE 4
Nurses Don’t Forget Each Other After Colorado Theater Massacre PAGE 8
Colleagues in Mexico See ENA As Having the Answers PAGE 37
INSIDE FEATURES
The Beat Goes On From the 2012 Annual Conference
Coverage and Photos From San Diego
Pages 18-34


Official Magazine of the Emergency Nurses Association 3
It seems like yesterday that I began the year as your
2012 ENA president. So much has been done to move
our specialty forward in the short space of one year,
all due to the extraordinary team of which I was
privileged to be a part.
Many of ENA’s accomplishments are described in
ENA’s Annual Report, but there are some very special
people behind the accomplishments whom I would
like to thank:
• First and foremost, ENA members — thank you for
your membership! When we are talking to regulators
and legislators, being able to say that we represent
more than 41,000 emergency nurses is powerful, and
they listen.
• Members of the national ENA Board of Directors,
who make sacrifices and devote many hours to the
mission of our association.
• ENA staff at national headquarters. Behind every
successful year at ENA, there are great ENA staff
members.
• Our corporate sponsors and supporters.
• Colleagues, and especially the Massachusetts
ENA State Council for its unwavering, unconditional
support. (I will be home soon!)
• The President’s Advisory Group for its wise
counsel and problem-solving skills.
• The ED nursing director of the ED where I work
for all her wisdom and support during this year.
• The members, staff and board liaisons
comprising 34 committees, work teams and special-
interest groups working on many critical projects.
• State council and chapter leaders. Your
leadership and hard work is appreciated.
• The ENA members at the state and local chapters
who create ‘‘family’’ and silently, selflessly volunteer
their time and energy to our association.
• Emergency nurses everywhere who work on the
front lines to deliver safe practice, safe care.
• The 2012 Leadership and Annual Conference
committee members, staff, hospitality volunteers and
corporate support for two very successful conferences.
• The team effort of the staff, partnering with key
government agencies and associations, to put on the
first Workplace Violence Prevention Summit. We had
several ‘‘firsts’’ this year of which we can be proud.
• Our nursing organization partners who have
collaborated on position statements, legislative
initiatives, advocacy projects and ENA products and
toolkits.
• And last, but not the least, my family and the
home and work families of all of our national board
members who pitch in to allow us to travel and work
as hard as we do all year.
As important as what ENA members contributed to
our specialty, their support for each other was equally
impressive.
At times our own light goes out and is rekindled by
a spark from another person. Each of us has cause to
think with deep gratitude of those who have lighted the
flame within us.
– Albert Schweitzer
When I recently called an ENA state president in
the hospital after a bad car crash, another emergency
nurse answered the phone. She was ‘‘specialing’’ the
state president, along with other emergency nurses
who took turns around the clock. They would plan
another schedule when she was discharged and take
turns bringing her meals. This state president had
always taken care of the ENA members in her state,
and it went without saying that she would have done
the same for them in a heartbeat.
At the wake of a friend, a friend I never would
have known if it were not for ENA, members from
across the state were there to honor his life and say
goodbye. Each laid a white rose on his casket and
read from the moving ‘‘Nightingale Tribute’’ in a show
of solidarity, similar to the solidarity that police and
firefighters possess. In the aftermath of Hurricane
Sandy, I heard from two members who had lost their
homes during the storm, and we were able to put
Dates to Remember
PAGE 4Free CE of the Month
PAGE 4Members in Motion
PAGE 6Pediatric Update
PAGE 10ENA Research
PAGE 11ENA Committee Spotlight: Historical Perspectives Work Team
PAGE 16Academy of Emergency Nursing
PAGE 35ENA Foundation
PAGE 36State Connection
PAGE 38Board Highlights
Monthly Features
Jan. 15, 2013 Deadline for poster submissions for 2013 Annual Conference in Nashville, Tenn.
March 11, 2013 Deadline for proposed bylaws and resolutions for 2013 General Assembly at Annual Conference in Nashville, Tenn.
PAGE 7Board Writes: Changing the Triage Paradigm
PAGE 8After the Aurora Theater Massacre: In Tending to Shooting Victims, Nurses Don’t Forget Each Other
PAGES 12-13What’s to Come at Leadership Conference
PAGES 14-15Advocacy Section
14 Reaping What’s Been Sown
14 New Hampshire ENA Helps Pass Prescription Drug Monitoring Legislation
15 What Does My Neighbor, the Nurse, Think About Health Care Reform?
PAGE 17Preparing to Present Your Resolution at General Assembly
PAGES 18-342012 Annual Conference Section
18 General Assembly Speeches and Debate
23 IENR Research and Evidence-Based Poster Winners
24 National ENA Award Winners 25 Lantern Award Winners
26 Opening Session
27 Closing Session
28 ENA Foundation
29 Concurrent Sessions
32 Town Hall Meeting
PAGE 37Colleagues in Mexico See ENA as Having the Answers
ENA Exclusive Content
Thank You For an Amazing Year!
LETTER FROM THE PRESIDENT | Gail Lenehan, EdD, MSN, RN, FAEN, FAAN
We make a living by what we get. We make a life by what we give. – Sir Winston Churchill
2012 ENA President Gail Lenehan presents the State President’s Award to Maureen Curtis Cooper, BSN, RN, CEN, CPEN, FAEN, Massachusetts ENA State Council president, at General Assembly in San Diego in September.
Continued on page 9

December 20124
ENA Connection is published 11 times per year from January to December by: The Emergency Nurses Association
915 Lee Street Des Plaines, IL 60016-6569
and is distributed to members of the association as a direct benefit of membership. Copyright© 2012 by the Emergency Nurses Association. Printed in the U.S.A.Periodicals postage paid at the Des Plaines, IL, Post Office and additional mailing offices.
POSTMASTER: Send address changes to ENA Connection915 Lee StreetDes Plaines, IL 60016-6569ISSN: 1534-2565Fax: 847-460-4002 Web Site: www.ena.orgE-mail: [email protected]
Non-member subscriptions are available for $50 (USA) and $60 (foreign).
Editor in Chief:Amy Carpenter AquinoAssistant Editor:Josh GabyWriter:Kendra Y. MimsEditorial Assistant:Renee HerrmannBOARD OF DIRECTORSOfficers:President: Gail Lenehan, EdD, MSN, RN,
FAEN, FAANPresident-elect: JoAnn Lazarus, MSN,
RN, CEN
Member Services: 800-900-9659
Secretary/Treasurer: Deena Brecher, MSN, RN, APRN, ACNS-BC, CEN, CPEN
Immediate Past President: AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN
Directors:Kathleen E. Carlson, MSN, RN, CEN, FAEN Ellen (Ellie) H. Encapera, RN, CEN Mitch Jewett, RN, CEN, CPEN Marylou Killian, DNP, RN, FNP-BC, CENMichael D. Moon, MSN, RN, CNS-CC, CEN,
FAENMatthew F. Powers, MS, BSN, RN, MICP, CENKaren K. Wiley, MSN, RN, CEN
Executive Director: Susan M. Hohenhaus, LPD, RN, CEN, FAEN
Sen. Tom Jensen, chairman of the
Kentucky Senate Judiciary
Committee, leaned over the table.
“Tell me, Ms. Robinson, what
do you want?” he asked.
Linda Robinson, BSN, RN,
CEN, CFN, a staff and charge
nurse with the St. Elizabeth
Healthcare Emergency
Department in Covington, Ky.,
had come before the Judiciary
Committee last summer seeking
support for a bill that would
make it a felony to attack an ED
health care worker in Kentucky.
But after testimony from Robinson and a cadre of
supporters she’d assembled for her cause, the
trouble was this: Kentucky simply wasn’t putting any
more felony laws on the books.
What Robinson wanted, she answered, was to
give police the authority to remove a violent person
from the ED without witnessing the incident
themselves or requiring the assaulted health care
worker to sign a complaint. Jensen’s response: Write
that up and I’ll sign it.
So Robinson regrouped. A little more than a year
later, attacking an ED health care
worker is now a fourth-degree
probable-cause misdemeanor in
Kentucky, punishable by a $1,000
fine and up to a year in jail.
Kentucky emergency departments
can return to safety a whole lot
easier now.
And Robinson, the driving force
behind the law, is a 2012 Magnet
Nurse of the Year. She received her
award from the American Nurse
Credentialing Center on Oct. 12 in
Los Angeles, where she also spoke
at the ANCC National Magnet
Conference on the topic of creating
a successful workplace violence
prevention program.
Robinson’s Magnet honor — one of five
bestowed annually — is in the category of Structural
Empowerment, and one need only examine her
long crusade against ED violence to understand
what that means. Fed up with the violence she saw
in her department, she began developing an
in-house violence-prevention program at St.
Elizabeth Covington in 2003. In 2007, she answered
a call in ENA Connection and found herself a key
player on the ENA Workplace Violence Work Team.
Two years later, she became an expert adviser for a
NIOSH-funded study on workplace violence
interventions with the University of Cincinnati.
“What I found, with all the work that I had done,
is that the violence was not really getting a whole
lot better,” she said. “The police would come and
they weren’t able to remove the violent person. And
then it dawned on me: The community has no idea
how violent the ER is. The ER is a microcosm of the
community — it’s a reflection of the community you
serve. And I said, ‘You know, we need to reach out
to the community.’ ”
She started with local legislators. After
approaching State Sen. John Schickel at a football
Kentucky Nurse’s Quest for Protection Earns Her Magnet Nurse of the Year Honor
Linda Robinson, BSN, RN, CEN, CFN
Continued on page 7
Head over to www.ena.org today to
take this month’s new free continuing
education course, ‘‘Service and Quality,’’
presented by Jeff Strickler, MA, RN, CEN,
CFRN. The e-learning course is worth
1 contact hour and aims to give you a
stronger understanding of quality and
service
concepts,
along with
important
strategies you
can use to
spice up
customer service and patient satisfaction
in your department.
To take the course and earn your
credit:
• Go to www.ena.org/freeCE,
where you’ll log in as an ENA
member (or create a new account).
• Add the course to your cart and
“check out” (no charge for members).
• Proceed to your personal learning
page to start or complete any course
for which you have registered or to
print a certificate when you’re done.
• To return to your personal learning
page at a later time, go to www.
ena.org and find ‘‘Go to Your
Personal Learning Page’’ under the
Courses & Education tab.
ENA’s back catalog of free CE covers
a variety of topics, including emergency
department flow, cardiocerebral
resuscitation, team-building, infection
prevention and more. Complete the
same checkout process for any course
you wish to take. These are absolutely
free to ENA members — one of the
many ways we’re committed to helping
you be the best at what you do.
Questions? Send an e-mail to
SPOTLIGHT ON YOU!Do you have a professional or educational
achievement you want your fellow ENA
members to know about? Do you want to sing
the praises of a member colleague who has
received a new degree, promotion or award?
We encourage you to submit these items to
[email protected] for inclusion in monthly
roundups in the new “Members in Motion”
section. Include names, credentials, a short
explanation of the accomplishment and a
high-resolution photo (if available), along with
contact information for follow-up by the ENA
Connection staff for select features.
By Josh Gaby, ENA Connection


December 20126
The 2012 ENA Annual Conference included a variety of pediatric content,
ranging from the unexpected (‘‘Strokes in Little Folks’’ by Rhonda Morgan)
to the mysterious (‘‘Things Are Not Always As They Seem’’ by Deena
Brecher) to the higher-frequency presentations (‘‘You Stuck What,
Where?’’ by Jeff Solheim). This year I was only able to attend a fraction of
the courses that interested me (because of the number of great sessions
offered) so for the first time, I decided to purchase a DVD of the entire
Annual Conference.* I am enjoying Annual Conference again at my
convenience.
I’d like to share some random pediatric ‘‘takeaway points’’ from three
of the 2012 Annual Conference sessions, with brief implications for
practice. In the words of Solheim, ‘‘It’s all about sharing knowledge and
advancing practice.’’ Consider this a small gift of knowledge, courtesy of
ENA’s 2012 Annual Conference, in the spirit of the holiday season.
From “Challenging Pediatric Presentations: What the Horses Can Teach Us About These ‘Zebras,’” presented by Barbara Weintraub, MPH, MSN, RN, APN, CEN, CPEN, FAENDon’t stress about the fact that you may not be an expert about every
specific and/or exotic pediatric condition. Apply what you know about
healthy, ‘‘normal’’ kids. Having a strong knowledge base of pediatric and
adult norms (in development, anatomy and physiology and vital signs)
will help when you are confronted with more challenging presentations.
For example, if a well-looking 4-year-old child presents with a history
of intermittent vomiting for one day, but his labs reveal a glucose of 30
and a bicarbonate level of 8, a red flag should go up to say, ‘‘These labs
are out of proportion to his illness.’’ Children’s glucose levels rarely go
below 50, even when they are ill. When the labs ‘‘don’t make sense,’’
such as in this scenario, metabolic disorders must be ruled out.
Although metabolic disorders (a.k.a. inborn errors of metabolism) are
individually rare, they are collectively fairly common, and children with
metabolic disorders can get sick very quickly, especially when they are
experiencing vomiting or diarrhea. Any sick child with a known history
of a metabolic disorder should be considered high-risk until proven
otherwise.
From “You Stuck What, Where? How? Why? Chatting About Foreign Objects,” presented by Jeff Solheim, MSN, RN-BC, CEN, CFRN, FAENMost of us know by now that batteries and magnets of any type are
high-risk foreign bodies (batteries can release toxic acid within hours, and
if more than one magnet is ingested, they can attract one another and
cause intestinal necrosis). However, vegetative foreign bodies (fruits,
vegetables, seeds) also can be quite high-risk. Vegetative matter expands
and absorbs surrounding fluid, becoming not only a high infection risk
but also more difficult to remove with time. Adding to the challenge is the
fact that vegetative matter is typically not visible on X-ray (neither are
aluminum and some wooden objects).
The new copper zinc pennies are toxic to the GI tract and need to pass
within 24 hours. In adults, objects longer than 6 cm typically cannot turn
the corner of the duodenum, and objects wider than 2 cm typically won’t fit
through the pylorus. Small foreign bodies in the nose can be ‘‘sucked up’’
and aspirated, especially if the patient cries or snorts (which is difficult to
control with children, especially, so expedite their treatment when possible).
From “Things Are Not Always As They Seem,’’ presented by Deena Brecher, MSN, RN, APRN, CEN, CPEN, ACNS-BCInfants: Make sure you unwrap swaddled babies so that you can fully
assess them (work of breathing, color, etc.). Infants are obligate nose
breathers until about 2 months of age; if their nose is full of mucous, they
will choose not to eat. Nasal congestion alone can cause respiratory
distress in infants. Glucose should be considered a vital sign in any very
ill-appearing infant; they release glucose into the bloodstream in response
to stress, and they also metabolize it quickly.
Children in general: Children compensate very well when they are ill,
until they don’t anymore. They typically ‘‘hold on to’’ normal blood
pressures until they have lost about 25 percent of their blood volume, so a
low BP is a late sign of deterioration. Pediatric vital signs (especially heart
rates) vary a great deal in response to fever, crying, pain, etc. If you find
yourself ‘‘rationalizing’’ an abnormal set of vital signs, be sure to reassess
them later. Do not let yourself rationalize more than once, because
sometimes the abnormal vital signs offer a clue to what is really going on
inside the child.
Brecher also shared some advice that could benefit us all: ‘‘We all make
mistakes … we need to admit them, share them with one another, learn
from them and report them (including near-misses) so that systems can be
improved and others may avoid making the same mistakes.’’ Sounds like a
great New Year’s resolution to me.
Happy holidays,
Elizabeth
* DVDs of 2012 Annual Conference presentations are available
at www.AVMGonline.com or 800-283-2864.
PEDIATRIC UPDATE | Elizabeth Stone Griffin, BS, RN, CPEN
Pediatric Content at 2012 Annual Conference
A Gift of Knowledge

Official Magazine of the Emergency Nurses Association 7
‘‘Triage is a process, not a place.’’ How many
times have you heard that phrase?
As I travel around the country in my role
as a consultant, I have the opportunity to visit
many emergency departments. A theme I see
in most is the mandatory triage process. No matter how busy the
department, patients are required to stop and be ‘‘triaged.’’ Why is that? Is
it because we always have done it this way, or is it because it is the best
care for our patients?
We all know that triage means ‘‘to sort.’’ The triage process is
something we adopted from the military. It was used in battle to
determine who could be treated and returned to battle. Emergency
departments began using triage to determine the sickest patients who
needed immediate attention when we didn’t have enough resources to
care for all. That process has evolved into triage being a place where all
patients walking into the ED must stop to be screened before being
placed in a bed in the ‘‘back.’’
Triage has become a bottleneck. The triage nurse is collecting
information not to decide acuity but to fulfill regulatory requirements,
with such questions as: ‘‘Do you feel safe at home? Do you use drugs or
alcohol? Are you sexually active?’’
In many emergency departments, the triage nurse knows more about
the patient than the primary care nurse. The triage nurse becomes the
person who bonds with the patient. I ask you to consider what happens
when we try to change this process, when we try to move to a rapid
triage process and when we expect the primary care nurse to ask the
assessment questions. As emergency nurses, we revolt. We say: ‘‘What is
the triage nurse doing? How can I be expected to ask all of these
questions? I’m too busy!’’
If we, as a profession, are going to respond to the changes in the
health care environment, we have to be open to changing the way we do
business. We have to be open to innovation and be willing to change the
status quo. Why do patients need to stop in triage when there are open
beds in the back? Why should the triage nurse collect all of the patient
information when the primary care nurse should be the one asking those
questions?
If we want to be part of the solution to throughput issues, we have to
be willing to change our practice, to change our paradigm. This is an
exciting time for change. There are many new processes being
implemented — such as nurse first, pivot nurse, team triage, input process
and split flow — that will impact what we now know as triage.
Obviously, there is no perfect process, no process that will work in all
emergency departments. ENA’s responsibility as an organization is to
provide you with the information and the data about these processes, to
enable you to make informed decisions about what will work best in your
emergency department. We are doing just that by providing educational
opportunities at our conferences related to best practices in triage. We
have partnered with Elsevier to bring you online triage education, and
most recently we added a special assessment category to the ENA
Emergency Nursing Scope and Standards of Practice. It is your
responsibility to become familiar with these resources and make us aware
of new ones. Help us to help you.
Changing the Triage Paradigm
BOARD WRITES | JoAnn Lazarus, MSN, RN, CEN, 2012 President-elect
game in the fall of 2010, she
outlined her plans to him in a
meeting a week later and won his
fervid cooperation. The Kentucky
ENA, the Kentucky Hospital
Association, the Kentucky American
College of Emergency Physicians,
the Kentucky Association of Chiefs
of Police, jailers, St. Elizabeth
Healthcare, domestic violence
groups and nurses across the state
all lined up behind their bill.
Despite the “no more felonies”
obstacle, which Jensen warned of
ahead of time, Robinson worked
the phones, urging emergency
nurses all over the state to call their
legislators and demand the bill be
heard. It worked. And now that it’s
law, she believes it can work for
more people. The next step in her
efforts isn’t to purse felony status
— which remains unlikely — but to
expand the probable-cause
component to include all Kentucky
hospital staff, not just those in
the ED.
“We have to keep our nurses
safe. We have to keep our health
care staff safe,” Robinson said.
“These are givers. These are people
who want to give. They’re people
who care.
“We created this culture of
allowing people to behave however
they wanted to behave in the
emergency room. And you’ve heard
that term: ‘It’s part of your job.’ It’s
not part of the job, and the culture’s
changing.”
In nominating Robinson for
Magnet recognition, Jane Swaim,
MS, RN, St. Elizabeth’s senior vice
president and chief nursing officer,
said Robinson “exemplifies the true
meaning of being a Magnet Nurse.”
Wrote Swaim: “She is passionate
about nursing, committed to the
issue of workplace violence
prevention and makes us all realize
that one nurse really can make a
difference.”
Kentucky Gov. Steve Beshear (seated) signs Senate Bill 58 into law on June 11, with Linda Robinson standing behind him.
Members in Motion Continued from page 4
December 20128
In Tending to Shooting Victims, Nurses Don’t Forget Each Other‘‘Can you come in? There’s been a shooting at
the Aurora mall.’’
That was the only information Cheryl Stiles,
MAOM, RN, CPEN, director of emergency
services at Children’s Hospital Colorado,
received when her unit secretary called shortly
after 1 a.m. July 20 to inform her that a mass
casualty shooting had occurred. Stiles realized
the shooting was a large-scale event before she
made it to the hospital. As she drove by the
Town Center at Aurora shopping mall, she saw
flashing lights, police cars and EMS vehicles
everywhere.
When Stiles arrived
at the hospital, she
witnessed what she
described as one of the
‘‘most compelling
moments of the night.’’
A portion of her team
— nurses, physicians
and techs — was
huddled outside of the
ambulance entrance.
They had just stabilized the final patient from
the shooting — a multi-weapon assault by an
apparent lone gunman in a packed movie
theater — and had taken a brief moment to
support each other as a team.
‘‘When I arrived, they were hugging each
other and taking a moment to pause and reflect
on the events of the night,’’ she said. ‘‘They
were taking care of each other and then quickly
moved back inside to continue their efforts.
Witnessing the teamwork, mutual respect and
the staff reaching out to each other in support
so that they could continue to take care of the
patients who were involved in the shooting, as
well as the patients already in the emergency
department, was undoubtedly one of the most
touching moments in my career.’’
After being briefed, Stiles immediately
assessed the situation, examined resources and
supplies to make sure the ED was prepared for
possible additional patients and examined the
ongoing needs of patients, families and staff.
Along with the 11 emergency nurses who
worked during the crisis, there were physicians,
advanced practice nurses, critical-care and float
nurses, mental health counselors, clinical
medical technicians, unit secretary staff, licensed
clinical social workers, the ED clinical manager
and the nursing disaster preparedness/mass
casualty representative.
‘‘When I came upon the event, it was
overwhelming, and I felt like the proud ‘mother’
of the unit,’’ Stiles said. ‘‘I was proud of every
individual and honored to witness the
unparalleled teamwork on behalf of our patients
and their families and driven by our hospital
mission. The priority was providing safe patient
care, keeping communication lines open and
assessing the ongoing physical and emotional
needs of patients, families and staff.’’
The ED staff consists of providers, nurses,
techs, mental health counselors and
administrative and support staff who are very
invested in mass casualty and disaster
preparedness. All nursing staff members are
certified in Basic Life Support, the Trauma
Nursing Core Course, Pediatric Advanced Life
Support and Advanced Cardiac Life Support,
and the majority are also Emergency Nursing
Pediatric Course-certified. Additionally, 58
percent of the ED RN staff members are
certified in their specialty area.
From the moment the first victim walked into
the ED and told the triage nurse about the
shooting, the staff focused and placed calls to
mobilize internal resources in order to prepare
for a mass influx of patients. Patients who were
not critical and not part of the shooting were
moved from the ED trauma/resuscitation area to
exam rooms within the department.
After the Aurora Theater Massacre
By Kendra Y. Mims, ENA Connection
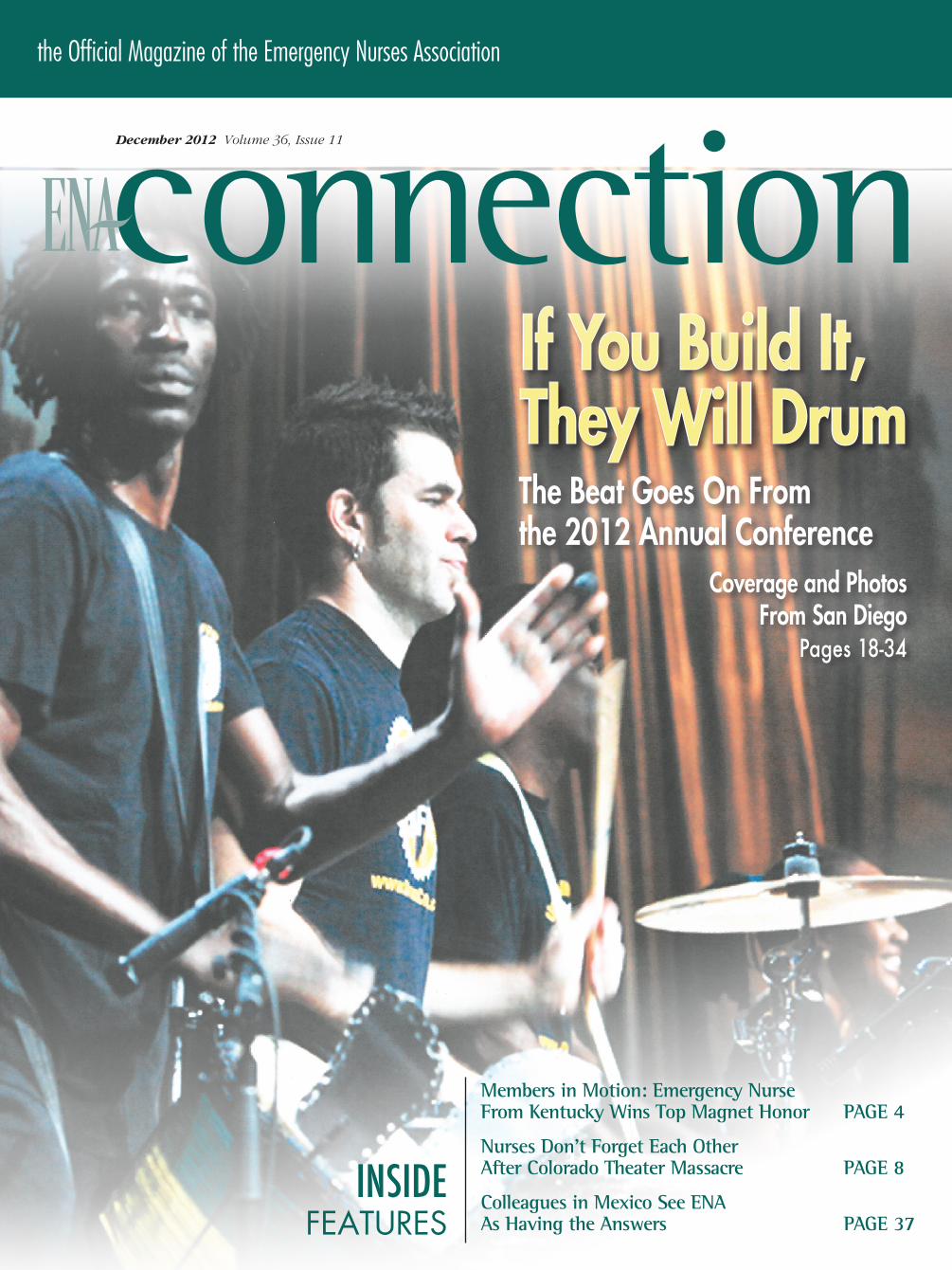
The ED staff at Children’s Hospital Colorado, where six victims of the July 20 theater shooting were taken.
Beth Maldonado, LCSW, the employee assistance program manager at Children’s Hospital Los Angeles, delivers cards signed by hundreds of employees from Children’s Hospital Los Angeles to Bob Flory, director of spiritual care and bereavement services at Children’s Hospital Colorado.
Cheryl Stiles, MAOM, RN, CPEN
Ph
oto
by S
teve
Ka
st, C
hil
dre
n’s
Hos
pita
l Col
ora
do

Official Magazine of the Emergency Nurses Association 9
Letter From the President Continued from page 3
As patients began arriving, there were many unanswered questions and
very limited information from the scene. People were concerned about
the possibility of multiple shooters. The total number of victims was
unknown. There were rumors of gas canisters and unknown chemicals
that may have been released in the theater. Stiles said they eventually
learned that the alleged shooter’s apartment — located a few blocks west
of the medical campus — was booby-trapped with explosives, which
heightened everyone’s awareness.
‘‘We are a Level 1 pediatric trauma center, and we see some of the
most severely injured patients who are referred from within a six-state
region, so we constantly prepare to care for patients who are critically ill
or injured,’’ Stiles said. ‘‘We train and prepare our entire emergency
careers for mass casualty events and attend drill after drill. We expect to
provide exceptional care to our patients. However, I am not sure that you
can ever adequately prepare for the global effects that result from a tragic
event such as the one that our community endured. We are very flexible,
by nature, and always expect the unexpected — we are great at this. But
the ramifications of this event were so large-scale.’’
Children’s Hospital Colorado received six patients — one child and five
adults — who ranged from fair to critical condition upon arrival. One of the
biggest challenges for Stiles and her staff was not being able to adhere to
their philosophy of family-centered care due to extenuating circumstances.
‘‘We whole-heartedly believe in family-centered care, and we support
and advocate for family presence at the bedside. The family is an integral
part of their child’s care plan and decision-making,’’ she said. ‘‘Personally,
it was exceedingly difficult to have families that had arrived and to not be
able to immediately reunite them with their respective family member
because of the active crime scene. In this case, the police followed crime
scene protocols and made the decision as to when we could
reunite families. While we understood the rationale, we were
challenged by the gut-wrenching feelings that resulted.’’
Although other incidents have sent more patients to Children’s
Hospital Colorado at one time, the theater shooting was on a
different level. The hospital was flooded with more than 1,000
phone calls (about 200 per hour) from as far away as Egypt and
Paris; many came directly into the emergency department. Some
were calls of support, while others were frantic calls from families
who wanted to know if a loved one had been involved in the
shooting. Calls and e-mails poured in from peers across the
country, local hospitals and many ENA members, including
several supportive calls from 2012 ENA President Gail Lenehan,
EdD, MSN, RN, FAEN, FAAN.
In addition, staff also received more than 30 different cards with
hundreds of notes of support from Children’s Hospital Los Angeles.
‘‘These words of encouragement and support meant so much to our
team,’’ Stiles said.
She still has difficulty finding words to describe the support.
‘‘One of the things that really affected us when we received this
outpouring of support was to look at paying it forward the next time
something unimaginable happens,’’ she said. ‘‘We can show that same
love and support that we received from others and pay it forward.’’
Some of her staff were very affected by the shooting days and weeks
after the incident and experienced difficulty being alone. Children’s
Hospital Colorado offered support through its Resiliency Education &
Support Team and the ED’s Resiliency Committee. Staff also had the
opportunity to meet with social workers and attend debriefings.
‘‘We had some staff that took some time off and took care of
themselves,’’ Stiles said. ‘‘We were very supportive.’’
She’s proud of how the ED staff responded and believes everyone on
the team did a ‘‘tremendous job’’ in taking care of the patients.
‘‘Our staff, and emergency staff in general, work very well under
pressure. They’re always an amazing, compassionate team,’’ Stiles said.
‘‘But the team spirit is heightened when you’re going through something
like this together. It was clearly evident that night. The support we
received internally from our hospital and our network of care was
overwhelming.
‘‘In those situations, you do what you need to, you focus, and you care
for the patients the way you should — the manner in which you would
expect to be treated and the way you’ve been trained. The last thing you
think about is yourself.’’
them in touch with each other.
During visits to emergency departments across the country, as
well as internationally, there was always an immediate
connection, a strong sense of camaraderie, a genuine caring . . .
and virtually all of the very same challenges.
From day one, serving as your president has been busier than
I could have imagined, and equally rewarding. None of us
reaches a destination or makes a difference by traveling the road
alone. As my 2012 ENA presidency comes to a close, I appreciate
the full power of the collective hard work of the board of
directors and the ENA staff at national headquarters, and the
wisdom of individual members.
I am grateful to all those who placed your trust in me. Your
commitment and passion to emergency nursing have inspired me
and our organization to stay strong. Be proud of the difference
you make for patients and for one another.
And thank you for an amazing year!Blanket Warmers | ISO 13485:2003 Certified | 262-251-8356 | www.enthermics.com
The science of warming blankets has turned into an intelligent art form. The new Enthermics DC Series features:
Individual zoned heatingProgrammable controlsEnergy-efficiencyErgonomic door release
And with an aesthetically pleasing design, the Enthermics DC Series is the intelligent choice in blanket warming.
Intelligent blanket warming
The true Nurse’s Aide
Smart. Affordable. Precise.
December 201210
You’re working in
the ED when a
10-year-old patient
comes in with a
head injury
sustained playing soccer. He’s alert and
oriented, with a mild headache, no loss of
consciousness and no vomiting. He’s got a little
retrograde amnesia. The child looks a little pale,
but he’s mentating well.
In triage, his vital signs are within expected
limits. His parents tell you, ‘‘We’re here for the
CT scan.’’
You know that a CT scan delivers a large
dose of radiation, and that given his
presentation, he may not need to undergo the
risks of CT scanning. But how do you make that
case to the parents, who are worried about their
child, and the provider, who may defer to the
parents’ wishes in the interest of patient
satisfaction?
Evidence to support best practices is critical,
and the type of research evidence that you look
for and can use to support practice changes is
important. In the age of nearly unlimited access
to information, sifting through evidence to
decide what is valid and valuable can be
challenging.
Appropriate literature can be found in several
places. In terms of practice issues, a database
that holds clinical nursing and medical articles is
the most useful. CINAHL, PubMed and
Journals@OVID are all good sources. Another
good source, the Centers for Disease Control
website (www.cdc.gov), often has up-to-date
information, epidemiological data and practice
guidelines.
Searching the LiteratureThe search terms you choose will help you find
articles on your topic of interest. In this case,
you’re interested in the benefits vs. risks of
scanning children’s heads. Start with, ‘‘Head
injury, pediatric head injury and computed
tomography scanning in head injury.’’ It’s also
helpful to look at guidelines from the American
Academy of Pediatrics, the Academy of
Emergency Physicians and the American
College of Radiology.
ENA RESEARCH | Lisa Wolf, PhD, RN, CEN, FAEN, Director of the ENA Institute for Emergency Nursing Research
What Is ‘Evidence’?
The Emergency Nurses Association is proud to present the release of the 4th edition of the Emergency Nursing Pediatric Course.It has been revised and updated, evidence-based, and continues to incorporate various teaching and learning styles.
• A portion of the course will be presented in an online format through ENA’s Center for e-Learning.
• Pediatric Clinical Considerations is nowcase-based using group discussion.
• The adolescent patient is addressed witha separate chapter and lecture.
• Triage is now Prioritization with a focus on the process, rather than the place.
Upon successful completion of ENPC, RN participants are veri� ed for four years, receive a veri� cation card and earn up to 16 contact hours.
This course brings the emergency nurse a resource for treating the pediatric patients arriving to emergency departments every day.
To verify why ENPC is right for you and toview course schedules, please visit
www.ena.org/coursesandeducation
The Emergency Nurses Association is
accredited as a provider of continuing nursing
education by the American Nurses Credentialing
Center’s Commission on Accreditation.
Official Magazine of the Emergency Nurses Association 11
Evaluating EvidenceResearch articles are structured to tell you about
the research question, the background of the
problem or what’s already been studied, and the
way in which the problem was studied (the
methods). Part of the value of the evidence is
how well the study was done. In other words,
was the question useful and well-framed? Was
the number of people studied (the sample size)
adequate to say anything about the problem? Did
the researchers answer the question? Was their
answer similar to or different from other
researchers studying the same thing?
What’s Out There?In this case, there are a large number of articles
in the PubMed database reporting the usefulness
of clinical-decision rules for this population. All
report that clinical decision-making tools to
determine high- and low-risk pediatric head
injury patients are sensitive enough to find the
children for whom benefit outweighs risk.
These studies tend to have large numbers of
patients and identify risk factors that would
direct a clinician to obtain a head CT, while
noting that in the absence of these factors, the
child has a very low risk of clinically important
head injury.
How to Incorporate Findings Into PracticeOnce you have a number of research reports that
seem to suggest the same thing, and are the
result of well-planned, well-done studies, you
can draw some conclusions about changing
practice. It is important to not base the decision
to implement change on the results of one study,
unless the study is so large and so well-done that
professional practice organizations are suggesting
changes.
What Next?Present these findings to your nursing manager
and medical staff and suggest implementation of
these guidelines. You may also want to contact
your local pediatric groups and discuss the
process, so that they don’t send patients to the
ED ‘‘for a CT scan.’’
Evidence-guided practice can streamline
processes and reduce risk for patients. Keeping
current with research that provides a practice
framework also can foster more collegial
communication with providers and improve
emergency nursing practice.
The Research Column in Connection has
been designed to give succinct, useful
information about the research process and
how research can be useful to the bedside
emergency nurse. Please send topic
suggestions to [email protected].
ENA COMMITTEE SPOTLIGHT
Historical Perspectives Work Team
Members of the Historical Perspectives Work Team who met in October stop at the Anita Dorr crash cart and 25th anniversary quilt displayed in the ENA headquarters lobby. From left, 1990 President Joanne Fadale, BSN, RN, FAEN; Audrey Snyder, PhD, RN, CEN, ACNP-BC, CCRN, FAEN, FAANP; board liaison Kathleen Carlson, MSN, RN, CEN, FAEN; and co-chairperson Diane Schertz, BS, RN, FAEN. Not pictured are co-chairperson Kay McClain, MS, RN, CEN, FAEN; and Mildred Fincke, BSN, RN.
When did ENA get started? What’s Etcetera?
Why is there a quilt hanging in the lobby of
ENA headquarters? How many members did
ENA have in 1989?
If you have questions about ENA’s history
or if you need background information for
committee work or a research project, you’ll
soon be able to obtain this information from
www.ena.org.
In May, ENA President Gail Lenehan,
EdD, MSN, RN, FAEN, FAAN, named a
Historical Perspectives Work Team
comprised of ENA Academy members (Kay
McClain, MS, RN, CEN, FAEN and Diane
Schertz, BS, RN, FAEN, co-chairpersons;
Patricia Clutter, MEd, RN, CEN, FAEN;
Joanne Fadale, BSN, RN, FAEN; and Audrey
Snyder, PhD, RN, CEN, ACNP-BC, CCRN,
FAEN, FAANP) to make recommendations
regarding the development of a sustainable
system that ensures the appropriate retention
of important ENA documents and other
historical materials.
Many documents, publications,
photographs, memorabilia, audiovisual items
and speeches will be posted to ENA’s website
in early 2013.
In addition, duplicate materials are sent to
the archives at the University of Virginia
School of Nursing, Center for Nursing
Historical Inquiry, established in 1991 to
support historical scholarship in nursing.
ENA makes an annual financial
contribution toward support of UVA’s work
in processing, preserving and making ENA’s
collection open to scholars, historians,
faculty and students, and materials sent from
ENA are described and catalogued in the
Center by an archivist and stored in secure,
climate-controlled rooms. The Center is a
national resource open to visiting scholars,
faculty, students and others interested in the
history of nursing and is open to visitors
Monday through Friday. Contact www.
nursing.virignia.edu/research/cnhi to
schedule a visit or to obtain more
information.
If you need any early history or
background information, contact Ginger
Burns, special projects manager, who serves
as ENA’s archivist, at [email protected].

ENA Reception Featuring Ignite® Sessions
What is Ignite®? Imagine that you’re in front of an audience made up of your friends and fellow colleagues
in emergency nursing; about to present a 5-minute talk on the thing you’re most passionate about – emergency nursing! Specifically; “What Makes an Emergency Nurse Unique.” You’ve brought 20 slides, which advance every 15 seconds whether you’re ready or not. You have a few last-minute butterflies, but off you go—and the crowd loves it. Welcome to Ignite.
Do you wish to share your take on “What Makes an Emergency Nurse Unique” through this rapid-paced presentation style? Be a part of this unique opportunity as ENA will be hosting a reception, February 28 from 6-8 p.m. in the exhibit hall.
To participate, speakers must agree to be video recorded and understand their video will be posted publicly to the internet. For complete details on participating, visit www.ena.org/lc and click the “Participate in Ignite” link before January 11, 2013.
Register today for ENA Leadership Conference 2013 by scanning the QR code or at www.ena.org/lc
FOR COMPLETE ENA LEADERSHIP CONFERENCE 2013 DETAILS, PLEASE VISIT WWW.ENA.ORG/LC
Important Dates to Remember
Registration .....................................Now Open
Early Discount Rate Closes ....... Jan. 16, 2013
State and Chapter Leaders Conference ........... Feb. 27 – 28, 2013
Presessions ................................ Feb. 28, 2013
Educational Sessions ............ Mar. 1 – 3, 2013
Exhibit Hall ...................Feb. 28 – Mar. 2, 2013
2013 ENA ANNuAl CoNFERENCE Nashville, TN • Sept. 17 – 21, 2013
ENA lEADERShIp CoNFERENCE 2014 Phoenix, AZ • Mar. 5 – 9, 2014
Each year, ENA Leadership Conference attracts emergency nurse leaders from across the United States as well as across the globe. Each attendee, new or returning, comes to conference with one common goal in mind; to strengthen their leadership knowledge. Regardless of the location, we know you choose Leadership Conference for the experienced faculty, the engaging and insightful educational sessions giving you the information crucial to your practice. You will have the opportunity to earn contact hours and to gain a new outlook on existing emergency department procedures.
Each one of these factors helps you strengthen your leadership skills and helps you elevate your career today, tomorrow and in the future. Join us for ENA Leadership Conference, February 27 – March 3, 2013 in Fort Lauderdale, FL to take advantage of:
• NEW! Jam, Hand-off and Deep Dive Sessions providing a variety of course length and formats for a unique learning experience
• NEW! ENA Reception Featuring Ignite® Sessions
• Innovative Opening Keynote Speaker – Carmine Gallo presenting “The 7 Principles of Inspiring Leaders”
• And much more…
SAVE
– T h E –
DATE
FOLLOW THE ACTION #ENALC13
Social Media presence at ENA leadership Conference 2013
Our social media presence will be even larger than ever. You will want to follow the ENA Facebook and Twitter pages for the latest information about conference. In addition, we will have Foursquare restaurant deals near the Fort Lauderdale convention center and hotels.
Tell us what is important for you. We would love to hear from you. Please share your thoughts on our Facebook page at facebook.com/enaorg or on our Twitter page at twitter.com/enaorg.
Networking 101: The Challenge of Networking
Attending for the first time or attending alone? The key to a successful meeting experience is connecting with peers and colleagues to exchange ideas and
solutions about common challenges. Networking opportunities are available to you at every turn. From the classroom to the social functions and in between.
NEW FOR 2013! Take advantage of a special opportunity at the Welcome party to connect with leaders and attendees from your state early in the evening. To find out all the exciting things happening at ENA Leadership Conference 2013, go to www.ena.org/lc.
WWW.ENA.ORG/LC
ENA
WHY YOU NEED TO ATTEND ENA LEADERSHIP CONFERENCE 2013
REGISTER TODAY FOR ENA LEADERSHIP CONFERENCE 2013 AT WWW.ENA.ORG/LC

ENA Reception Featuring Ignite® Sessions
What is Ignite®? Imagine that you’re in front of an audience made up of your friends and fellow colleagues
in emergency nursing; about to present a 5-minute talk on the thing you’re most passionate about – emergency nursing! Specifically; “What Makes an Emergency Nurse Unique.” You’ve brought 20 slides, which advance every 15 seconds whether you’re ready or not. You have a few last-minute butterflies, but off you go—and the crowd loves it. Welcome to Ignite.
Do you wish to share your take on “What Makes an Emergency Nurse Unique” through this rapid-paced presentation style? Be a part of this unique opportunity as ENA will be hosting a reception, February 28 from 6-8 p.m. in the exhibit hall.
To participate, speakers must agree to be video recorded and understand their video will be posted publicly to the internet. For complete details on participating, visit www.ena.org/lc and click the “Participate in Ignite” link before January 11, 2013.
Register today for ENA Leadership Conference 2013 by scanning the QR code or at www.ena.org/lc
FOR COMPLETE ENA LEADERSHIP CONFERENCE 2013 DETAILS, PLEASE VISIT WWW.ENA.ORG/LC
Important Dates to Remember
Registration .....................................Now Open
Early Discount Rate Closes ....... Jan. 16, 2013
State and Chapter Leaders Conference ........... Feb. 27 – 28, 2013
Presessions ................................ Feb. 28, 2013
Educational Sessions ............ Mar. 1 – 3, 2013
Exhibit Hall ...................Feb. 28 – Mar. 2, 2013
2013 ENA ANNuAl CoNFERENCE Nashville, TN • Sept. 17 – 21, 2013
ENA lEADERShIp CoNFERENCE 2014 Phoenix, AZ • Mar. 5 – 9, 2014
Each year, ENA Leadership Conference attracts emergency nurse leaders from across the United States as well as across the globe. Each attendee, new or returning, comes to conference with one common goal in mind; to strengthen their leadership knowledge. Regardless of the location, we know you choose Leadership Conference for the experienced faculty, the engaging and insightful educational sessions giving you the information crucial to your practice. You will have the opportunity to earn contact hours and to gain a new outlook on existing emergency department procedures.
Each one of these factors helps you strengthen your leadership skills and helps you elevate your career today, tomorrow and in the future. Join us for ENA Leadership Conference, February 27 – March 3, 2013 in Fort Lauderdale, FL to take advantage of:
• NEW! Jam, Hand-off and Deep Dive Sessions providing a variety of course length and formats for a unique learning experience
• NEW! ENA Reception Featuring Ignite® Sessions
• Innovative Opening Keynote Speaker – Carmine Gallo presenting “The 7 Principles of Inspiring Leaders”
• And much more…
SAVE
– T h E –
DATE
FOLLOW THE ACTION #ENALC13
Social Media presence at ENA leadership Conference 2013
Our social media presence will be even larger than ever. You will want to follow the ENA Facebook and Twitter pages for the latest information about conference. In addition, we will have Foursquare restaurant deals near the Fort Lauderdale convention center and hotels.
Tell us what is important for you. We would love to hear from you. Please share your thoughts on our Facebook page at facebook.com/enaorg or on our Twitter page at twitter.com/enaorg.
Networking 101: The Challenge of Networking
Attending for the first time or attending alone? The key to a successful meeting experience is connecting with peers and colleagues to exchange ideas and
solutions about common challenges. Networking opportunities are available to you at every turn. From the classroom to the social functions and in between.
NEW FOR 2013! Take advantage of a special opportunity at the Welcome party to connect with leaders and attendees from your state early in the evening. To find out all the exciting things happening at ENA Leadership Conference 2013, go to www.ena.org/lc.
WWW.ENA.ORG/LC
ENA
WHY YOU NEED TO ATTEND ENA LEADERSHIP CONFERENCE 2013
REGISTER TODAY FOR ENA LEADERSHIP CONFERENCE 2013 AT WWW.ENA.ORG/LC

December 201214
One benefit of going to a
national meeting such as
the ENA Annual Conference is the networking
opportunity. You meet emergency nurses from
all over the country and the world. Engaging
with each other, we realize we do not exist in
isolation. Big inner-city hospital or small, rural
critical access facility, we all seem to have
similar concerns. Too many patients, limited
staffing, impossible demands and learning new,
paperless documentation systems are a few of
the common difficulties.
Hardly a few minutes are spent without
hearing a conversation about emergency
department care of patients who are mentally
ill. The volume of patients presenting with
mental health issues, and the care required, are
additional pressures on already under-resourced
EDs challenged by de facto mission creep. How
did health care professionals and workplaces,
communities, voters and governments ignore
the fractured aspects of health care, allowing
inequities in care delivery to get so skewed?
This article revisits past policies to understand
what transpired, bringing us to the present.
The movement to deinstitutionalize mental
health patients began around 1956 when the
state and local public mental hospital patient
population was 559,000.1 Of this total, a
substantial number of patients were housed in
‘‘back wards’’ for many years. Back wards were
notorious for inhumane treatment; patients were
not expected to recover, and custodial care was
provided, with no actual treatment taking place.
By 1980, the process of moving people out of
these facilities to care in community-based
services reduced the number of patients in
public mental hospitals to 154,000.
While states initiated transferring patients out
of public institutions, the progress was slow.
The process only quickened during the 1960s
and 1970s with the involvement of the federal
government. Created by Congress and
appointed by President Dwight D. Eisenhower,
the Joint Commission on Mental Illness and
Health reported in 1961 the need for a national
mental health program of research and of ‘‘fully
staffed, full-time mental health clinics (later
called community mental health centers), to be
available to each population of 50,000, or
approximately 3,000 to cover the nation.”2 The
thought was that with promising medications
(e.g., thorazine) and better treatment modalities,
people could be treated in community facilities.
In 1963, the CMHC legislation was enacted
with funding for construction of CMHCs. In
1965, CMHC staffing legislation finally was
enacted. The CMHCs were to provide only five
essential services: inpatient, outpatient,
emergency, partial hospitalization, consultation
and education on mental health. No
pre-admission and post-discharge services for
state mental hospital patients, nor rehabilitation
or case management services, were mandated
for the transition. While deinstitutionalization
accelerated, the funds did not follow the
patients.
Many state budget directors saw the decision
to put patients out into the field as a chance to
decrease their budgets. Exacerbating the fiscal
failure was a naïveté for what would be needed
to help people exiting state hospitals, e.g.,
wraparound services, including job training,
housing and continued counseling.
What finally has resulted is the continuing
elimination of state institutions with the majority
of the financial burden falling on Medicaid
rather than a mental health funding stream.
State funding of mental health services in 2005
was 30 percent less — when adjusted for
inflation — than in 1955.
As emergency nurses, we are faced with
caring for these patients in a fragmented,
broken system. This is not just a mental health
crisis; this unfinished business plays out in the
ED. ENA, in collaboration with other
stakeholder organizations, must stand together
nationally and locally, advocating for access to
quality care for all our patients, lobbying for
remedies to problems still in need of system
change.
References
1. Koyanagi, C. (2007, August.) Learning from
history: Deinstitutionalization of people with
mental illness as precursor to long-term care
reform. Retrieved from www.kff.org/
medicaid/upload/7684.pdf.
2. Smucker, B. (2007, July.) Promise, progress,
and pain – a case study of America’s
community mental health movement from
1960 to 1980. Retrieved from
mentalhealthhistory.org/Promise_
Progress_Pain.pdf.
Reaping What’s Been Sown
ADVOCACY
By M. Ben Melnykovich, BSAS, RN, Member, ENA Government Affairs Committee
Prescription drug abuse has
become a leading health problem
in the United States. In 2010, New
Hampshire alone had 174 deaths
as a result of prescription
overdoses. There are now more
deaths in New Hampshire from
prescription drug overdose than
motor vehicle crashes. Opiods,
specifically methadone and
oxycodone, are the most prevalent
drugs leading to death. To aid in
the detection of fraudulent
requests for controlled substances,
48 states have prescription drug
monitoring programs in place,
with New Hampshire and Missouri
being the only exceptions. This
means that savvy patients in the
Northeast take a short trip to New
Hampshire not only for tax-free
shopping but also to avoid
detection in their quest for opiates.
After several years attempting to
pass legislation establishing a PDM
in New Hampshire, bills were again
introduced in 2012. New
Hampshire ENA had identified this
bill as a high legislative priority
early in the year. Members
contacted their legislators,
encouraging them to support the
bill. In April, New Hampshire
Government Affairs Chairperson
Jean Proehl, MN, RN, CEN, CPEN,
FAEN, testified at a legislative
hearing to describe the impact of
prescription drug abuse in New
Hampshire emergency departments.
Success was realized in the
spring when the bill passed in
both houses of the legislature. On
June 12, NH-ENA President Stacey
Savage, BSN, RN, CPEN, watched
as Gov. John Lynch signed this
bill in to law. (Search for Gov.
Lynch and SB 286 at Youtube.com
to view the signing video.)
In October, New Hampshire
ENA and three other nursing
organizations received Advocacy
in Action awards for their work
toward the passage of this bill.
NH-ENA is now participating in
committee work to accomplish the
goals of the legislation.
Reference
Governor’s Commission on Alcohol
and Drug Abuse Prevention,
Intervention, and Treatment. (2012,
Jan). A Call to Action: Responding
to New Hampshire’s Prescription
Drug Abuse Epidemic. Concord,
NH: Author.
New Hampshire ENA Helps Pass Prescription Drug Monitoring Legislation
Official Magazine of the Emergency Nurses Association 15
Every nurse knows the experience of being
asked a general health question by a neighbor,
friend or patient with the expectation that your
knowledge, education or clinical expertise will
clarify a complicated topic. What is more
complex than the Patient Protection and
Affordable Care Act? Since its enactment in
March 2010, and more recently, since the
Supreme Court decision in June 2012, nurses
have been asked to comment, explain or clarify
PPACA issues.
According to the ENA 411 Key Contact
program, ‘‘As an emergency nurse, you speak
with the authority of one whose perspective is
broad, observing and connected with people
from throughout the community, touching
individuals from all types of families and
situations, economic strata, occupations and
education.”1 Are you ready for that
responsibility? This article, though expressing
my opinion only, may be helpful when you are
asked the inevitable questions.
If you are anything like I am, you had good
intentions of reading the PPACA when it was
adopted and then when it was published as the
906-page Public Law 111–148.2 ENA
summarized the law for members at members.
ena.org/government/healthcarereform/
Pages/Default.aspx. The March 2010 ENA
Washington Update described the law’s reform
elements (www.ena.org/government/
washington/Documents/2010/03-2010.pdf).
The following is what I was thinking in
early July 2012 based on the 10 titles in the
PPACA3:
Title I: Quality, Affordable Health Care For All Americans• Pre-existing illnesses won’t prevent you from
obtaining insurance coverage.
• Lifetime or annual limits no longer will be an
issue for those with chronic, lifetime illnesses
or injuries and for the families of those
patients.
• Preventive health services are now being
covered.
• Insurance coverage will extend to young
adults on their parents’ plan.
Title II: Role of Public Programs• It’s beneficial that the Children’s Health
Insurance Program will be expanded
Title III: Improving the Quality and Efficiency of Health Care• It’s interesting to consider what types of new
Patient Care Models will be developed.
Title IV: Prevention of Chronic Disease and Improving Public Health• It’s exciting to consider how prevention and
public health innovation and expansion of
primary care options will improve the nation’s
health, relieving some ED pressure.
Title V: Health Care Workforce• It’s about time the health care workforce
received appropriate educational funding.
Title VI: Transparency and Program Integrity• It goes without saying that the law must
include integrity in all issues.
Title VII: Improving Access to Innovative Medical Therapies• It’s fascinating that access to innovation in
medical therapies will be expanded to include
a broader patient population.
Title VIII: Class Act• I’m a nurse, not an attorney or legislator, so I
cannot at this time begin to comment on this
title, which describes a self-funded, voluntary
long-term care insurance choice in the event
of a disability.
Title IX: Revenue Provisions• Unless we find the funding, progress will
not occur. This title makes health care more
affordable for families and small business
owners.4
Title X: Strengthening Quality, Affordable Health Care for All Americans• It’s a goal for all of us because we are going
to be patients one day.
As sure as nothing is perfect, there are still
many features in the PPACA that will benefit us as
providers of health care. On the day after the
Supreme Court decision, a few neighbors were
enjoying a lovely evening in our common
courtyard, and though two of them were
attorneys, they were interested in what I had to
say about the PPACA because I am a nurse.
References
1. Emergency Nurses Association. (n.d.). EN411.
Retrieved from www.ena.org/government/
EN_411/Pages/Default.aspx.
2. The Patient Protection and Affordable Care
Act (P.L. 111–148). (2010, March.) Retrieved
from www.gpo.gov/fdsys/pkg/PLAW-
111publ148/pdf/PLAW-111publ148.pdf.
3. HealthCare.gov. (n.d.). The health care law &
you: Read the law. Retrieved from www.
healthcare.gov/law/full/index.html.
4. The Congressional Budget Office. (n.d.).
Affordable Care Act. Retrieved from www.
cbo.gov/topics/health-care/affordable-
care-act/reports.
What Does My Neighbor, the Nurse, Think About Health Care Reform?By Elisabeth K. Weber, MA, RN, CEN, Member, ENA Government Affairs Committee
ADVOCACY

December 201216
Congratulations to the 14 new
fellows in the Academy of
Emergency Nursing, who were
inducted during the regal 1st
Annual Awards Gala in San
Diego. This black-tie optional
event, hosted by the always humorous Terry Foster, MSN, RN, CEN, FAEN,
was a fitting venue to celebrate the lifetime contributions of these new
fellows.
The Academy of Emergency Nursing honors nurses who have made
enduring, substantial contributions to emergency nursing and who
continue to advance the profession of emergency nursing.
Induction as a fellow into the Academy often marks the pinnacle of the
inductee’s career. The collective wisdom and contributions of the AEN’s
101 fellows is astounding. This 2012
cohort is no exception; the caliber of
each of these inductee’s is amazing, and
as a group, unstoppable.
To our new FAENs, I hope that you
take your induction into the AEN not just
as a remarkable achievement, but as a challenge to recognize your
continued potential.
2012 Academy Inductees
• Meredith Jaye Addison, MSN, RN, CEN, FAEN — Hillsdale, Ind.
• Rita T. Anderson, RN, CEN, FAEN — Surprise, Ariz.
• Liz Cloughessy, AM, MHM, RN, FAEN — Glenwood, NSW, Australia
• Christine M. Gisness, MSN, RN, BC, FNP-C, CEN, FAEN — Roswell, Ga.
• Diane Gurney, MS, RN, CEN, FAEN — Hyannis,
Mass.
• Andrew D. Harding, MS, RN, CEN, NEA-BC,
FACHE, FAHA, FAEN — Bridgewater, Mass.
• Cindy L. Hearrell, MSN, RN, CEN, FAEN —
Fredericksburg, Va.
• J. Jeffery Jordan, MS, MBA, RN, CEN, CNE, EMT-P,
FAEN — Macomb, Okla.
• Fred Neis, MS, RN, CEN, FACHE, FAEN — Prairie
Village, Kan.
• India J. Taylor Owens, MSN, RN, CEN, NE-BC,
FAEN — Fairland, Ind.
• Gwyn Parris-Atwell, MSN, RN, FNP-BC, CS, CEN,
FAEN — Alloway, N.J.
• Judith A. Scott, MHA, BSN, RN, PHN, FAEN
— Penn Valley, Calif.
• Paula Tanabe, PhD, MPH, MSN, RN, FAEN —
Durham, N.C.
• Mary Ann Teeter, MEd, RN, FNP-C, CEN, CNRN,
FAEN — Elmira, N.Y.
A segment of the fellow application weight is ‘‘the
potential for sustained contributions to the Academy
of Emergency Nursing and the advancement of the
emergency nursing profession.’’ John F. Kennedy
once said, ‘‘The ancient Greek definition of happiness
was the full use of your powers along lines of
excellence.’’
Your powers of excellence have been
acknowledged. Serving as a FAEN provides a
tremendous opportunity to make a difference at the
local, state, national and international levels.
Congratulations on your induction into this prestigious
group. You decide whether it is a final achievement
or a sign of the amazing things yet to come.
Look for profiles and photos of the 2012
fellows in the February issue of ENA Connection.
Check out great gift ideas for friends and colleagues this holiday season.
Two easy ways to order:Phone: 800-900-9659 Monday through Friday 8:30 a.m. - 5:00 p.m. CT www.ena.org/shop
Shop Marketplace
By Kathleen Flarity, ARNP, PhD, CEN, CFRN, FAEN, Chairperson-elect, Academy of Emergency Nursing
101 Fellows in the Academy of Emergency Nursing

Official Magazine of the Emergency Nurses Association 17
The experts at Shriners Hospitals for Children know every second counts in the survival and recovery of pediatric burn patients. The sooner a child reaches Shriners Hospitals for Children, the better the chances for a full recovery.
As the leading pediatric burn care hospitals in the world, Shriners Hospitals for Children provide a full range of services to care for children with burn injuries.
Call your nearest Shriners Hospitals for Children for information regarding immediate assistance about referral procedures and educational opportunities, for emergency room staff.
Their lives are in your hands. Don’t waste a moment. CALL NOW.
Cincinnati877-947-7840
Boston617-726-3575Galveston409-770-6773
Sacramento916-453-2111
When 10-year old Earl accidentally set his
sustained third-degree burns over much ofhis body.
emergency roomnurse referred Earl to Shriners Hospitals for Children. Her quickand decisive action saved his life.
shriinnneerrsshhosppitttaaalllsssfffooorrrccchhhiiilllllddddddrrrrreeeeennnnn....ooooorrrrggg
Have you ever considered
proposing a resolution for General
Assembly? The opportunity is open
to any member of our professional
organization; however, it is not as
easy as merely identifying a need.
How does one go about putting
together the proposed resolution
and moving it through to successful
adoption by the General Assembly?
In Louisiana, we began by
discussing the challenge with our
ENA board liaison, Mitch Jewett,
RN, CEN, CPEN. He suggested we
poll our members about their
concerns. From that assessment, we
developed a proposal to submit to
the ENA Resolutions Committee.
The resolution was vetted, and
recommendations for change were
relayed. Based upon those
suggestions, we worked with the
committee to firm up the statements
and supporting research.
Upon notification that our
resolution had been accepted,
preparations began for presentation
to General Assembly and defense
of the resolution during debate.
Finally, the day for presentation
arrived. We expected lively debate,
remembering to remain professional
and not take the statements made by
the opposition personally. This may
have been the most difficult of all
tasks associated with the process
and required both mental preparation and patience. During the debate, our
delegation took notes of the remarks and the state represented, along with the
names of those speaking either in support or in opposition. These notes were
vital in the resolution assistance session and for caucusing the next morning.
During the resolution amendment assistance session held that evening,
other delegates and Resolutions Committee members provided input. The
statements were amended to more clearly define the resolution and request.
Our next tasks were to explain the amendments to our delegates, have them
prepared to introduce those when appropriate, and to supply the
amendments and explanation for all delegates.
We successfully moved our resolution forward, and now ENA will
address the issue that we identified: defining the components of safe
discharge from the emergency department.
This process engaged all of our members, especially our delegates. It is
impressive to see the renewed spirit of ownership that has been evidenced
since we began the journey.
ENA has issued the next call for resolutions, which are due March 11,
2013. Why don’t you resolve to get involved?
At Your FingertipsSeveral resources for members
interested in writing a
resolution are at www.ena.
org/statecouncils/
GeneralAssembly/Pages/
ResolutionsBylaws.aspx.
Topics include the following:
• Call for Bylaws and
Resolution Proposals: Deadline
March 11, 2013, 5 p.m. CST
• Bylaws Amendments and
Resolutions Guidelines —
Revised October 2012
• Bylaws Amendment
Proposal 2013 - Template
• Resolution Proposal 2013
– Template
• General Assembly Standing
Rules of Procedure —
Amended Sept. 12, 2012
• Tips On Using References
• Parliamentary Procedure
Basics: “Speaking the Delegate’s
Language”
• Examples: Bylaws
Amendments and Resolutions
Proposals
• ENA Position Statements
– Reviewing current position
statements before drafting
proposals is recommended.
Preparing to Present Your Resolution at General AssemblyBy Deborah Spann, RN-BC, CEN, Louisiana ENA State Council
December 201218
By focusing on engaging members and the
profession of emergency nursing, ENA has
amassed an impressive list of accomplishments.
In her Sept. 12 address to the 697 delegates
comprising this year’s General Assembly, 2012
President Gail Lenehan, EdD, MSN, RN, FAEN,
FAAN, announced several initiatives that have
elevated ENA’s status among emergency nurses
and outside organizations.
‘‘Our Nurse Practitioner in Emergency Care
Committee’s dream has come true,’’ Lenehan
said. ‘‘Today we are formally announcing that the
American Nurses Credentialing Center and ENA
will embark on a new portfolio credentialing
program for emergency nurse practitioners.
Credentialing by portfolio is a growing trend that
allows for a more robust proof of competency,
and ANCC is the authority in this method.’’
After inviting the committee members present
to stand and be recognized for their hard work,
Lenehan said the credential could become reality
within a year.
Some of the other accomplishments Lenehan
highlighted were the release of the ENPC 4th
edition; the current TNCC revision; a landmark
position statement on weighing pediatric patients
in kilos only; the creation of a Conference Site
Selection Committee, which selected Phoenix as
the Leadership Conference 2014 venue; the first
Workplace Violence Prevention Summit and the
new member benefit of monthly free CE. She
noted that ENA’s landmark position paper on
weighing children in kilos only also has been
signed by the American College of Emergency
Physicians, the Institute for Safe Medication
Practices and the American Academy of Pediatrics.
‘‘It’s rare to have a physician group sign on to
a nursing group’s position unless it’s a joint
consensus statement,’’ she said.
The National Quality Forum is also
considering adding its endorsement.
She reported on other collaborations with the
Centers for Disease Control on traumatic brain
injury, Emergency Medical Services for Children
on the pediatric toolkit and the NQF on
regionalization of emergency care.
‘‘The general direction of this organization is
one that everyone in this room should leave
feeling very excited about,’’ Lenehan said. ‘‘The
high-level connections we’re shoring up — with
colleagues at associations and regulators in key
positions — have already elevated us to new
positions.’’
On a personal note, Lenehan shared that one
of the most gratifying aspects of the year was the
opportunity to reach out and connect with
nurses involved in crisis situations, to make that
crucial connection and to represent ENA.
‘‘I’ve been reminded as I visit EDs across the
country and beyond that there is so much more
that binds us together than pulls us apart,’’ she
said, ‘‘so many of the common struggles and
successes. The commonalities are everywhere.’’
Lenehan closed by thanking several people,
including the ENA Board of Directors, Executive
Director Susan M. Hohenhaus, LPD, RN, CEN,
FAEN, ENA staff, state and chapter presidents, the
Massachusetts ENA State Council and her family.
‘‘Thank you for the privilege of serving as
your 2012 president,’’ she said. ‘‘It’s been quite
a ride!’’
President’s Address: Elevating ENAGENERAL ASSEMBLY: SAN DIEGO
Past ENA presidents listen as Gail Lenehan, EdD, MSN, RN, FAEN, FAAN, addresses the General Assembly.
By Amy Carpenter Aquino, ENA Connection
Bringing greetings from ‘‘the fabulous staff at
ENA headquarters,’’ Executive Director Susan M.
Hohenhaus, LPD, RN, CEN, FAEN, reported on
the business of the association to the General
Assembly delegates Sept. 12.
‘‘If you had any doubts about the road map
for the future of ENA, please download our
strategic plan from the ENA website,’’
Hohenhaus said. She pointed out that the first
arm of the plan’s triangle is investment, and
explained that while the 2012 budget shows a
deficit, it was intentional and will enable the
organization to focus on developing the two
main areas of human resources and technology.
Executive Director: Talent, Technology Investments Add Up to a Stronger ENABy Amy Carpenter Aquino, ENA Connection
Susan M. Hohenhaus, LPD, RN, CEN, FAEN

Official Magazine of the Emergency Nurses Association 19
‘‘This moment is a mountain-top experience for
me, and I thank God for this honor,’’ said 2012
President-elect JoAnn Lazarus, MSN, RN, CEN, as
she addressed the 697 General Assembly
delegates gathered at the San Diego Convention
Center on Sept. 13. Giving special recognition to
her family and friends, Lazarus thanked everyone
who supported her on her leadership journey.
‘‘Because of you, I am here today,’’ she said.
Mentoring and leadership form the basis of
Lazarus’ 2013 vision for ENA, with a special focus
on providing members with the resources they
need to be effective leaders. She emphasized the
importance of mentors to emergency nurses, who
are shaped by preceptors, managers and others
who supported them early in their career. She
asked attendees to consider what they are doing
to leave a legacy, how they want others to
remember them.
‘‘The fact that each of you is in this room, that
makes you a part of the leadership of ENA of
more than 40,000 emergency nurses,’’ Lazarus
said. ‘‘Leadership is at the core of what we do,
whether it is formal or informal.’’
Lazarus said creating opportunities for
mentorship and leadership development for
members, as well as strengthening strategic
partnerships, will help ensure ENA’s future.
‘‘Many of you find yourselves as leaders in your
state organization or in your hospitals without the
support and/or tools to do the job you want to
do,’’ she noted. ‘‘You may feel you do not have
the knowledge or resources to be successful. . . . I
believe it is our responsibility as your professional
organization to provide you with those tools and
resources. The viability of this organization is
dependent upon it.’’
Lazarus invited delegates to help her continue
the ENA legacy by spreading awareness of both
the organization’s mission to advocate for patient
safety and excellence in emergency nursing
practice, and its strategic initiatives.
‘‘I believe we need to focus more on taking
care of the needs of our membership,’’ she said.
‘‘If we work together to create a safe environment
where we can give quality patient care, and at the
end of the day feel good about what we have
done, we have been successful.’’
Lazarus also prepared members for changes,
including revising and redesigning organizational
operations. These changes are vital to attracting
and developing new leaders, she said.
‘‘People want to be part of something that is
meaningful and purposeful,’’ she said. ‘‘So how
do we ensure that ENA meets those needs? We
have to become more innovative if we are to
survive. We have to take risks.’’
Lazarus explained the meaning of the small
turtle pins handed out to each delegate as she
urged attendees to reflect on their roles as leaders
and mentors once they returned home.
‘‘Behold the turtle,’’ she said, quoting James B.
Conant. ‘‘He makes progress only when he sticks
neck out.’’
Taking Care of Our Members General Assembly Talks TNCC, Pain Management in the ED and More
Executive Director: Talent, Technology Investments Add Up to a Stronger ENAThese fortifications will leave ENA better prepared
to enter the implementation stage of its strategic
plan in 2013, guided by its four organizational
priorities.
In the area of talent, Hohenhaus reported on
the recent addition of key staff, including Betty
Mortensen, MS, BSN, RN, FACHE, chief nursing
officer; Dr. Paula Karnick, PhD, ANP-BC, CPNP,
director of education; and Dr. Lisa Wolf, PhD, RN,
CEN, FAEN, director of the Institute for
Emergency Nursing Research. They join Kathy
Szumanski, MSN, RN, NE-BC, director of the
Institute for Quality, Safety and Injury Prevention.
‘‘We are now fully staffed in our nursing
Continued on page 34
By Amy Carpenter Aquino, ENA Connection
JoAnn Lazarus, MSN, RN, CEN
The delegates of the 2012 ENA General
Assembly considered several
resolutions concerning such issues as
TNCC eligibility, use of protocols in
the ED setting, health care worker
fatigue and care of the bariatric and
obese patient.
‘‘Today we need to do the serious
business of the General Assembly,’’ said
Jeffery J. Jordan, MS, MBA, RN, EMT-P,
CEN, chairperson of the Resolutions
Committee, as he presented the first of
several bylaw amendments and
resolutions for delegates’ consideration
Sept. 13, following a day of proposal
hearings in San Diego.
The assembly voted to postpone
indefinitely a proposal to allow the
General Assembly to elect the ENA
Board of Directors and Nominations
Committee. During the initial hearing
of the proposed resolution Sept. 12,
co-author Jason Moretz, BSN, RN, CEN,
CTRN, said the amendment was ‘‘not
about taking something away from our
members. This is about making sure
we get the greatest leaders elected.
Despite our greatest efforts, our voting
percentage remains low. As members,
we entrust this body with defining our
practice; it is reasonable that we would
trust them to elect the leaders that
would lead us into the future.’’
Several delegates said they could
not support denying members the
right to vote in their national election,
but some offered ideas to encourage
voting.
‘‘Voting is a problem, but this is not
the solution,’’ said delegate Teresa
Sullivan, who suggested moving the
national election voting to the Annual
Conference and offering live, online
voting for members at home. Other
Continued on page 33
By Amy Carpenter Aquino, ENA Connection

December 201220
In choosing the 2012 Anita Dorr Memorial
Lecture speaker, ENA President Gail Lenehan,
EdD, MSN, RN, FAEN, FAAN, wanted ‘‘someone
with the same vision, passion and commitment
as the leaders and extraordinary talent I see
throughout this room — someone who can
speak on prevalent issues that we face in our
health care settings on a daily basis.’’
ANA President Karen Daley, PhD, MPH, RN,
FAAN, more than fit the bill. With 26 years of
emergency nursing experience and as a vocal
advocate for legislation mandating the use of
safer needles in the health care setting, Daley
has demonstrated unwavering resolve toward
improving occupational safety health.
Daley shared her riveting story of suffering a
1988 needlestick injury following a blood draw
on a patient in the ED. Recalling that she was
able to get the patient’s blood on the first draw,
Daley said she deposited the used needle in the
box on the wall behind her.
‘‘I felt a sharp stick in my index finger, and I
knew right away that it was a pretty deep
puncture,’’ she said. ‘‘The blood came out of the
side of the glove.’’
Three months later, after suffering vague
symptoms of nausea, weight loss and abdominal
pains, Daley received life-changing news: She
tested positive for both HIV and hepatitis C.
Daley recalled that with the shock fresh in
her mind, ‘‘All I could think about was that I
was never going back to the ED again.’’
During her recovery, while under the care of
an infectious disease specialist at Massachusetts
General Hospital, Daley worked with her state
nurses association to propose legislation
requiring hospitals to report every workplace
injury. The bill passed into law within the year
and remains one of the strongest workplace
injury reporting laws in the country, she said.
Daley then turned her attention to the
national level because ‘‘I knew what had
happened to me was happening at EDs all
around the country,’’ she said. When she
received the opportunity to address the ANA
constituency, Daley said it illustrated for her the
collective power of a national organization.
‘‘I said, ‘I’ll go anywhere, anytime to address
nurses on this issue, because we have safety
devices and only 15 percent of hospitals are
using them.’ ”
After years of advocacy work, Daley was
invited to the White House to witness President
Bill Clinton sign the Needlestick Safety and
Prevention Act in November 2000.
‘‘I wish that 12 years later I could say this
was a past issue, but the work continues,’’
Daley said, urging emergency nurses to follow
through with reporting all sharps injuries, as
data collection is necessary to benchmark
progress. ‘‘We know the injuries are still
occurring, and we still know that under-
reporting is a huge issue,’’ she said.
‘‘We as nurses should never underestimate
our individual power as a constituent or the
power of a collective voice,’’ she said, adding
that nurses need to add their voices to the
political process to remain engaged and
empowered. ‘‘Our strength is in our numbers,
expertise and credibility.
‘‘Thank you again for the opportunity to
speak to you about an issue that affects all of us
in our practice.’’
The 2012 Judith C. Kelleher Award Goes to ...
The Road to Sharps Injury Prevention
Every year during ENA’s Annual Conference, the
Judith C. Kelleher Award is given to a member
who has consistently demonstrated excellence in
emergency nursing and has made significant
contributions to the profession that are destined
to impact the future of emergency nursing. ENA
President Gail Lenehan, EdD, MSN, RN, FAEN,
FAAN, proudly presented this award to Diane
Gurney, MS, RN, CEN, FAEN, during this year’s
Anita Dorr Memorial Lecture and Luncheon.
Lenehan shared Gurney’s many
accomplishments and contributions to the
emergency nursing profession on a state and
national level, as well as the common themes of
inspiration and admiration found throughout her
nomination letters.
‘‘I personally witnessed Diane’s hard work and
dedication, and the excellence in the results of
that hard work. Others have as well,’’ Lenehan
stated. ‘‘Diane is exactly who the Kelleher Award
was meant to honor and is truly deserving.’’
Gurney cheerfully accepted her award, stating
that she felt honored as the 33rd award recipient.
She shared the overwhelming feeling she
experienced when she received the phone call
that she was the 2012 winner — which happened
at the ENA headquarters office while she was
sitting next to the Anita Dorr crash cart.
Gurney’s work for ENA not only has inspired
others — it also has inspired her.
‘‘During some difficult hours and days, my
work with ENA kept me focused and moving
forward,’’ she said. ‘‘I’m humbled to be accepting
such a prestigious award. Thanks to all who have
shared my journey.’’
By Kendra Y. Mims, ENA Connection
ANITA DORR MEMORIAL LECTURE
Diane Gurney, MS, RN, CEN, FAEN, (right) with 2012 President Gail Lenehan, EdD, MSN, RN, FAEN, FAAN.
Karen Daley, PhD, MPH, RN, FAAN, president of the American Nurses Association, with Susan M. Hohenhaus, LPD, RN, CEN, FAEN, at the Anita Dorr Memorial Lecture and Luncheon.
By Amy Carpenter Aquino, ENA Connection
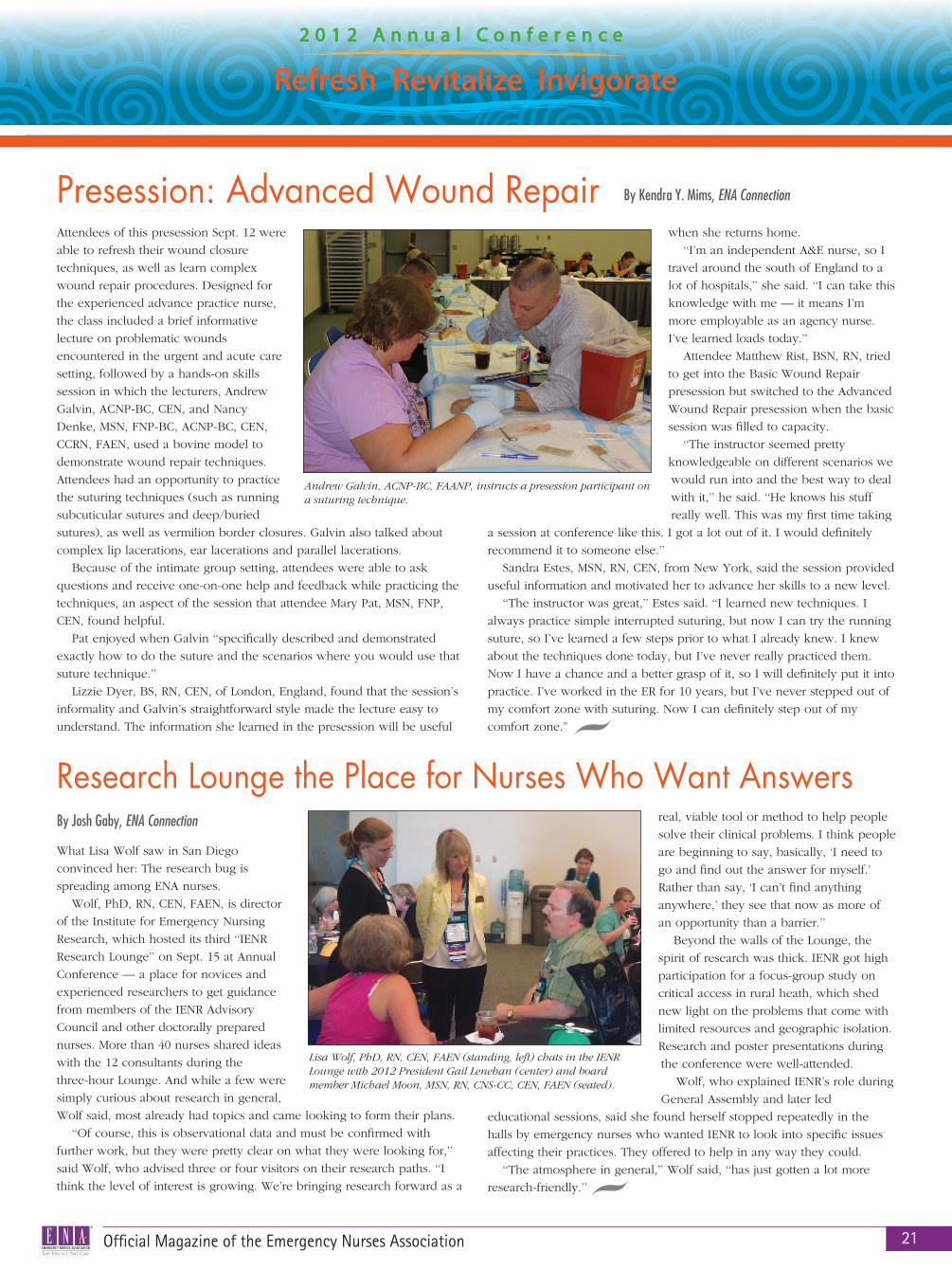
Official Magazine of the Emergency Nurses Association 21
What Lisa Wolf saw in San Diego
convinced her: The research bug is
spreading among ENA nurses.
Wolf, PhD, RN, CEN, FAEN, is director
of the Institute for Emergency Nursing
Research, which hosted its third ‘‘IENR
Research Lounge’’ on Sept. 15 at Annual
Conference — a place for novices and
experienced researchers to get guidance
from members of the IENR Advisory
Council and other doctorally prepared
nurses. More than 40 nurses shared ideas
with the 12 consultants during the
three-hour Lounge. And while a few were
simply curious about research in general,
Wolf said, most already had topics and came looking to form their plans.
‘‘Of course, this is observational data and must be confirmed with
further work, but they were pretty clear on what they were looking for,’’
said Wolf, who advised three or four visitors on their research paths. ‘‘I
think the level of interest is growing. We’re bringing research forward as a
real, viable tool or method to help people
solve their clinical problems. I think people
are beginning to say, basically, ‘I need to
go and find out the answer for myself.’
Rather than say, ‘I can’t find anything
anywhere,’ they see that now as more of
an opportunity than a barrier.’’
Beyond the walls of the Lounge, the
spirit of research was thick. IENR got high
participation for a focus-group study on
critical access in rural heath, which shed
new light on the problems that come with
limited resources and geographic isolation.
Research and poster presentations during
the conference were well-attended.
Wolf, who explained IENR’s role during
General Assembly and later led
educational sessions, said she found herself stopped repeatedly in the
halls by emergency nurses who wanted IENR to look into specific issues
affecting their practices. They offered to help in any way they could.
‘‘The atmosphere in general,’’ Wolf said, ‘‘has just gotten a lot more
research-friendly.’’
Presession: Advanced Wound Repair
Research Lounge the Place for Nurses Who Want Answers
Attendees of this presession Sept. 12 were
able to refresh their wound closure
techniques, as well as learn complex
wound repair procedures. Designed for
the experienced advance practice nurse,
the class included a brief informative
lecture on problematic wounds
encountered in the urgent and acute care
setting, followed by a hands-on skills
session in which the lecturers, Andrew
Galvin, ACNP-BC, CEN, and Nancy
Denke, MSN, FNP-BC, ACNP-BC, CEN,
CCRN, FAEN, used a bovine model to
demonstrate wound repair techniques.
Attendees had an opportunity to practice
the suturing techniques (such as running
subcuticular sutures and deep/buried
sutures), as well as vermilion border closures. Galvin also talked about
complex lip lacerations, ear lacerations and parallel lacerations.
Because of the intimate group setting, attendees were able to ask
questions and receive one-on-one help and feedback while practicing the
techniques, an aspect of the session that attendee Mary Pat, MSN, FNP,
CEN, found helpful.
Pat enjoyed when Galvin ‘‘specifically described and demonstrated
exactly how to do the suture and the scenarios where you would use that
suture technique.’’
Lizzie Dyer, BS, RN, CEN, of London, England, found that the session’s
informality and Galvin’s straightforward style made the lecture easy to
understand. The information she learned in the presession will be useful
when she returns home.
‘‘I’m an independent A&E nurse, so I
travel around the south of England to a
lot of hospitals,’’ she said. ‘‘I can take this
knowledge with me — it means I’m
more employable as an agency nurse.
I’ve learned loads today.’’
Attendee Matthew Rist, BSN, RN, tried
to get into the Basic Wound Repair
presession but switched to the Advanced
Wound Repair presession when the basic
session was filled to capacity.
‘‘The instructor seemed pretty
knowledgeable on different scenarios we
would run into and the best way to deal
with it,’’ he said. ‘‘He knows his stuff
really well. This was my first time taking
a session at conference like this. I got a lot out of it. I would definitely
recommend it to someone else.’’
Sandra Estes, MSN, RN, CEN, from New York, said the session provided
useful information and motivated her to advance her skills to a new level.
‘‘The instructor was great,’’ Estes said. ‘‘I learned new techniques. I
always practice simple interrupted suturing, but now I can try the running
suture, so I’ve learned a few steps prior to what I already knew. I knew
about the techniques done today, but I’ve never really practiced them.
Now I have a chance and a better grasp of it, so I will definitely put it into
practice. I’ve worked in the ER for 10 years, but I’ve never stepped out of
my comfort zone with suturing. Now I can definitely step out of my
comfort zone.”
By Kendra Y. Mims, ENA Connection
Andrew Galvin, ACNP-BC, FAANP, instructs a presession participant on a suturing technique.
Lisa Wolf, PhD, RN, CEN, FAEN (standing, left) chats in the IENR Lounge with 2012 President Gail Lenehan (center) and board member Michael Moon, MSN, RN, CNS-CC, CEN, FAEN (seated).
By Josh Gaby, ENA Connection
December 201222
ENA Presents the First Advanced Practice Cadaver Lab
For the first time at the ENA Annual Conference,
advanced practice registered nurses had the
opportunity to register for the Advanced
Practice Cadaver Lab. Through the expertise of
ENA faculty members Robert A. Leach, MSN,
RN; Kathleen M. Flarity, PhD, ARNP, CEN,
CFRN, FAEN; and Arlo F. Weltge, MD, MPH,
FACEP, along with the support offered by
Vidacare, an ENA Strategic Sponsor, attendees
were able to participate in this exciting new
opportunity and receive CEs.
The two sold-out sessions gave participants
a chance to improve practitioner skills using
unembalmed cadavers to simulate the anatomy
and feel of an actual patient. Attendees learned
advanced emergency procedural skills through
hands-on labs in a small group setting, which
allowed one-on-one interaction with the
instructors. Some of the procedures covered in
the three skills stations included intraosseous
catheter placements, venous cutdowns, tube
thoracostomy, lateral canthotomy, advanced
airway insertion and central venous access.
Although Darryl Sol, MSN, CNS, FNP-C, has
attended several ENA conferences over the
years, he began attending more emergency
medicine conferences instead to refresh his
advanced nursing skills. He said the opportunity
to participate in an advanced cadaver lab this
year attracted him back to the ENA Annual
Conference.
‘‘The advanced cadaver lab was a great
opportunity,’’ Sol said. ‘‘It’s one of those things
where you’re proud of the organization and you
want to participate, but sometimes those
advanced skills aren’t there, so this was a great
thing. The course itself was great. The instructors
were very knowledgeable and helped us one-on-
one even though we were in a group. They were
willing to take us to the side and help us. All the
skills that we learned were important, and we
don’t often use them a lot, so I was happy to
revisit them. It was a great review.’’
By Kendra Y. Mims, ENA Connection
Official Magazine of the Emergency Nurses Association 23
IENR Presents 2012 Poster AwardsThe Institute for Emergency Nursing
Research presented the 2012
Research and Evidence-Based
Practice Poster Awards on Sept. 14
at the ENA Annual Conference in
San Diego. Recipients were chosen
from 44 Evidence-Based Practice
topics and 10 research topics.
Evidence-based Practice Poster Award WinnerNancy Homan, MSN, MBA, RN,
APRN-BC, an advanced practice
nurse for Emergency Services,
Christiana Care Health System in
Newark, Del., received the
Evidence-Based Practice Poster
Award for “We All Fall Down, But
for Very Different Reasons.”
“We had a serious fall with
injury,” Homan said, “and I was part
of the root cause analysis. Then, I
was assigned falls for the whole
unit. It was just something that fell
into my lap.”
Homan’s experience with her
hospital’s falls committee led to a
year-long study of all the factors
surrounding falls in her ED,
including age, shift and sight, as
well as possible causes such as
mobility, reason, cognition and
intoxication. She also began
including the story that accompa-
nied each report of an ED fall, to
give her a more complete picture.
As a result, her ED added a falls
icon to its ED tracker, which she
said was a helpful way to communi-
cate patient information. Her ED
also added its own scale, based on
red, yellow and green stoplight
colors, as a quick visual method for
categorizing patients regarding their
potential for sustaining a falls injury.
Homan’s goal of sharing her data
with emergency nursing colleagues
was amplified by the fact that there
is little data available on ED falls.
“I only found one article related
to emergency department falls.” she
said. “When I got to the conference,
people were very excited because
there just isn’t much out there on
falls.”
Homan was so surprised to
receive the award for the best
Evidence-Based Practice Poster that
she did not even
realize she won,
even after seeing
the blue ribbon
tacked to her
poster.
“It was a really
neat experience,”
she said. “This
was my first
national ENA
conference. It was great to meet
with people who have a like
mind-set and see people from
different parts of the country, and
also to see that my hospital is pretty
progressive. You don’t appreciate
that until you look at other
hospitals.”
Homan appreciated the positive
feedback her poster received from
attendees, including several who
asked her to send them the infor-
mation. She was also contacted by
the author of the only other article
she found on the topic of falls in
the ED.
Homan is already working on
another project to submit for the
2013 ENA Annual Conference in
Nashville, Tenn.
Research Poster AwardThe Research Poster award went to
Elizabeth T. Dugan, PhD, RN, chief
nurse executive of Inova Loudon
Hospital in Leesburg, Va., who
presented “The Relationship
Between Quality of Care in the
Emergency Department and
Timeliness of Intervention for
Patients with Severe Sepsis.”
Dugan’s poster, based on her
doctoral dissertation study,
focused specifically on “how the
timeliness of care impacted
outcomes – such as length of stay
and mortality – but also how the
volume of the ED at the time
impacted the timeliness of care for
the septic patient.”
Dugan’s study included all five
hospitals within the Inova Health
System and was sparked by the
system’s initiative to reduce
mortality in specific categories,
including sepsis. She collected data
for 14 months and was surprised by
the results.
“I really thought that I would
find that crowding increased length
of stay, increased mortality,” she
said. “I did not find that. What I
found – and it was an unexpected
finding – was that what really
impacted timeliness of care, more
than crowding, was the identifica-
tion of sepsis in triage.”
“We implemented several years
ago, as well as many other
hospitals, a sepsis screening process
in triage,” Dugan said. “What I
found was, if the sepsis screening
triage process works, and the nurse
identifies the patient positive for
sepsis or potentially for severe
sepsis, they will alert the doctor and
get things rolling according to the
interventions that have been
identified.”
Dugan said she also found that a
delay in triage in recognition of
sepsis caused a delay in treatment.
“I found that only a third of the
patients were accurately identified
with a positive sepsis screen in
triage,” she said. “So we are really
missing a lot of people.”
Dugan said she felt honored and
surprised to receive the poster
award and enjoyed the opportunity
to present to ENA members.
“You know, you do a lot of
work, and then you put it on a shelf
in a dissertation book,” she said.
“So I really appreciated being able
to share my findings at the confer-
ence via the poster, and really had
a great time engaging with the
attendees. Everyone that came out
was having the same concerns and
issues, and they were really
engaged around the screening
process.
“This was probably the best
poster session I have seen, and I go
to a lot of different conferences.”
IENR Thanks 2012 Poster JudgesThe IENR gratefully acknowledges the
following individuals for serving as
poster judges for the 2012 ENA Poster
Awards Program:
James Bockeloh, DNP, RN, APRN-BC,
FNP-BC; Darlene Bradley, PhD, MSN,
RN, CEN, CCRN, FAEN; Laura Criddle,
PhD, RN, CEN, CPEN, CFRN, ACNP-BC,
CCNS, CCRN, FAEN; Renee Holleran,
PhD, APRN, FNP, CEN, CFRN, CCRN,
FAEN; Mary Kamienski, PhD, APRN,
CEN, FAEN; Elyse Kemmerer, PhD; Anne
Manton, PhD, RN, APRN, FAEN, FAAN;
Diana Meyer, DNP, RN, CEN, CCRN,
FAEN; Elizabeth Mizerek, MSN, RN,
EMT-B, CEN, CPEN; Patricia Normandin,
DNP, MSN, RN, CEN, CPEN; Andrea
Novak, PhD, RN-BC, FAEN; Ryan
Oglesby, PhD, MHA, RN, CEN, NEA-BC;
Diane Salentiny-Wrobleski, PhD, RN,
APRN, CEN, ACNS-BC, CCNS; Mary
Sigler, EdD, RN, CRNP; Audrey Snyder,
PhD, RN, ACNP-BC, CEN, CCRN, FAEN,
FAANP; Dawn Specht, PhD, MSN, RN,
CNS, CEN, CCNS, CCRN; Stephen
Stapleton, PhD, MSN, MS, BSN, BS, RN,
CEN; Debbie A. Travers, PhD, RN, CEN,
FAEN; Jeanne Venella, DNP, MS, RN,
CEN, CPEN; and Sarah Wilkey, DNP,
FNP, RN.
By Amy Carpenter Aquino, ENA Connection
Nancy Homan, MSN, MBA, RN, APRN-BC
Elizabeth T. Dugan, PhD, RN
December 201224
National ENA Awards
President’s Award— 2012 ENA President Gail Lenehan, EdD, MSN, RN, FAEN,
FAAN, is pictured with her husband, Joseph M. Lenehan, MD, recipient of the
President’s Award, and their daughter, Kate Lenehan.
Nursing Professionalism Award — Anne Stefanoski, BSN, RN, CEN
Frank L. Cole Nurse Practitioner Award— Kathy J. Morris, DNP, APRN, FNP-C, FAANP
Behind the Scenes Award — Robert Breese, CCEMTP, FP-C
Nurse Manager Award— Leslie A. Christiansen, BS, RN, CEN
Rising Star Award — Kristen Connor, BSN, RN, PHN, CEN
Nursing Practice Award— Judith Common, RN, CEN, CPEN, CA/CP SANE, SANE-A, SANE-P
Nursing Research Award — Michelle A. Marini, MSN, RN, CPNP, CPEN, and Amy W. Truog, BSN, RN, CPEN
Nursing Education Award — Timothy J. Murphy, MSN, RN, ACNP - BC, CEN
Team Award — Mid Maryland Chapter, Annual Barbara Proctor Memorial Educational Day Team Members: Sandra M. Waak, RN, CEN; Linda Arapian, MSN, RN, CEN, CPEN, EMT-B; Lisa Tenney, BSN, RN, CEN, CPHRM; Anne May, BSN, RN. Not pictured: Emilie Crown, BA, RN, CEN; Pamela S. Fox, BSN, RN, CEN, CPEN; and Lucy McDonald, RN, CPEN, CPN, EMT-B.
Lifetime Achievement Award— Sharon McGonigal, RN, CEN
Not pictured:
Gail P. Lenehan Advocacy Award — Joyce Foresman-Capuzzi, MSN, RN, CCNS, CEN, CPN, CTRN, CCRN, CPEN, SANE-A, EMT-P
Nursing Competence in Aging Award — Donna M. Roe, DNP, ARNP-BC, CEN
ENA Foundation State Challenge Awards — Left: Mike Hastings, MS, RN, CEN, president of Kansas ENA State Council, which raised highest amount per capita. Right: Pat Nierstedt, MS, RN, CEN, president of New Jersey ENA State Council, which raised the highest total.

Official Magazine of the Emergency Nurses Association 25
Lantern Awards
Advocate Good Shepherd Hospital Emergency Department — Barrington, Ill.
Boston Children’s Hospital Emergency Department — Boston
Indiana University Health Methodist Hospital Emergency Medicine and Trauma Center — Indianapolis
Beaumont Health System – Grosse Pointe Emergency Center — Grosse Pointe, Mich.
Cedars Sinai Medical Center, Ruth and Harry Roman Emergency Department — Los Angeles
Chandler Regional Medical Center Emergency Department — Chandler, Ariz.
Children’s Medical Center Dallas, Seay Emergency Center — Dallas
Cincinnati Children’s Hospital Emergency Department – Burnet Campus — Cincinnati
ENA Celebrates the ‘Best In Class’ at GalaMore than 300 people walked down
the red carpet in their finest attire
for ENA’s first annual Awards Gala
on Sept. 15. The evening started
with a reception with hors
d’oeuvres, followed by pictures
taken by ENA’s ‘‘paparazzi,’’ red
carpet interviews by the master of
ceremonies, Terry Foster, MSN, RN,
CEN, CCRN, FAEN, and a delicious
dinner.
It was a proud night for many in
the ballroom. The special evening
honored individuals for their
accomplishments over the last year.
The awards program included
commemorating ENA Individual
Award winners, Lantern Award
recipients, Academy of Emergency
Nursing inductees and the ENA
Foundation State Challenge Award
winners.
ENA President Gail Lenehan,
EdD, MSN, RN, FAEN, FAAN, hosted
the event with Foster and presented
the awards. Foster’s humor and
jokes provided comedy for the
evening and kept the audience
entertained and amused.
‘‘Madame President, with all due
respect, I did not see an award for
Best in Humor!’’ Foster told
Lenehan. ‘‘But seriously, heartfelt
congratulations to all of you . . .
especially those who were induced,
I mean inducted into the Academy.’’
As the event ended, Lenehan and
Foster expressed their appreciation
to the attendees and
congratulated them for their
achievements and successes.
‘‘We’ve come to the close of the
best event of the whole week, and
the best group to share it with.
Thank you all for being part of
ENA’s First Annual Gala!’’ Lenehan
said. ‘‘We are so much better for
knowing you all, and emergency
nursing is so much better for your
accomplishments.’’
Kendra Y. Mims

December 201226
2012 ENA President Gail Lenehan, EdD, MSN,
RN, FAEN, FAAN, welcomed attendees to the
Annual Conference after the Drum Café
performance, announcing exciting initiatives and
highlights from throughout the year.
Among them were ENA’s improvement of
access to information through new technology,
the advancement of emergency nursing globally
(TNCC is being taught in 13 countries) and ENA’s
advancement of the future of emergency nursing
through 34 committees, education and an
investment in staff (ENA now has nine highly
qualified nurses on staff).
Lenehan also was excited to announce that
ENA is offering free CEs for members and
moving to one national conference in 2015.
Lenehan shared that right before she took the
stage, ENA Executive Director Susan M.
Hohenhaus, LPD, RN, CEN, FAEN, told her that
ENA had been awarded the 2012 Susan Harwood
Training grant from the Occupational Health and
Safety Administration, which provides funds to
develop workplace violence training materials.
‘‘We have the blueprint to move our
organization from great to greatest,’’ she said. ‘‘I
know that we have the right professionals with
the right talents to accomplish this together and
we will continue to develop and enhance
strategic partnerships.’’
After acknowledging ENA’s partnerships with
organizations such as The Joint Commission, the
American Nurses Association and the American
College of Emergency Physicians, Lenehan also
acknowledged all of the delegates who
convened for the two-day General Assembly.
‘‘These are [nearly] 700 of our most engaged
emergency nurses, and you would have been so
proud of their thoughtful, very informed and
very intelligent debate on our resolutions and
bylaws,’’ she said. ‘‘We came up with some very
good decisions which will move our specialty
profession forward.’’
Lenehan presented the President’s Award to
the individual who gave her inspiration and
unconditional support throughout the year.
‘‘This award goes to my husband, Dr. Joe
Lenehan, and to all of the other spouses,
partners and significant others for whom ENA
stands for ‘Every Night Alone,’ ’’ Lenehan said.
She closed her speech by urging the audience
to make the most of the conference.
‘‘Thank you for coming, thank you for being
an important part of this conference and thank
you to those who are members,’’ she said. ‘‘You
make this conference and all that ENA does
possible.’’
‘We Have the Blueprint to Move Our Organization From Great to Greatest’By Kendra Y. Mims, ENA Connection
OPENING SESSION
Proof That We’re All Beating the Same Drum
The hall exploded with the sound
of hundreds of drums and
boomwhackers Sept. 13 as
conference attendees participated in
the Opening Session’s highly
acclaimed entertainment, the Drum
Café, the global leader in interactive
drumming.
After ENA’s Executive Director
Sue Hohenhaus, LPD, RN, CEN,
FAEN, welcomed attendees to the
conference, Drum Café took the
stage and began its world-
renowned performance, which
provided a fun atmosphere and
engaged the audience in team-
building through music. Every seat
in the room was equipped with a
drum or boomwhacker, which
emergency nurses used to create
music with Drum Café for the first
hour of the session.
Natalie Spiro, leader of Drum
Café, discussed the importance of
using music as a universal language.
‘‘What you just experienced right
now was harmonizing as one ENA
to this universal language of rhythm
and drumming,’’ she said. ‘‘This is a
language that transcends all barriers
and boundaries across geography,
across job function to effective
communication, collaboration and
teamwork. For every single person
in this room, it’s all about refresh,
revitalize and invigorate.’’
Before beginning the
performance, audience members
raised their hands and recited: ‘‘We
have compassion and respect, we
work to improve public health, we
exercise sound judgment, and
we’ve got rhythm. We are
drummers.’’ Chants of, ‘‘We are ENA
and we’re No. 1; yes, we are ENA
and we rock,’’ filled the room as the
audience followed Drum Café’s lead
to play the ‘‘heartbeat, pulse and
infrastructure of ENA’’ in the center
of their drums.
Drum Café integrated ENA’s
tagline and vision into the team-
building event, along with the
conference’s theme. As the
audience chanted ‘‘refresh,
revitalize, invigorate,’’ some were
pulled out of their seats to join
Drum Café in the front of the room.
‘‘I’m amazed at what you do
every day,’’ Spiro said. ‘‘Some of you
are seeing over 300 patients a day.
You are so special, so valued and so
critical to providing the care for the
people in your community.’’
By Kendra Y. Mims, ENA Connection
Natalie Spiro, who leads the Drum Café, moves up the aisle during Opening Session as conference attendees follow along.

Official Magazine of the Emergency Nurses Association 27
Refreshing Message From Wine to Water FounderClosing out the 2012 Annual Conference with
keynote speaker Doc Hendley was a refreshing
way to conclude the fun-filled and exciting week
of learning, growing and reconnecting in San
Diego.
Like every attendee in the audience, Hendly
also has experience in making a difference and
changing lives. The Harley-riding bartender
created Wine to Water, a non-profit organization
that has provided tens of thousands of people
around the world with clean drinking water. He
opened up his talk with a brief video that
showed work he has done in Haiti and other
areas, such as digging wells.
Hendley’s intense, emotional stories of taking
personal risks in places such as Darfur to provide
people with clean water highlighted the power of
having courage even in the most dangerous
situations. His down-to-earth and humble attitude
and his evident passion for helping those who are
less fortunate captivated and invigorated the
audience. He also shared the concepts of building
relationships that he learned while bartending and
the importance of focusing on people.
‘‘It doesn’t matter how passionate you are
about what you’re doing or what reasons you
got into something at the beginning — there’s
going to come those days when you just don’t
want to get out of bed,’’ he said. ‘‘There’s going
to come those days when you say, ‘I didn’t sign
up for this.’ But it’s at those times when it’s so
vital to surround ourselves with people who
believe in us more than we believe in ourselves.
That was a huge lesson for me to learn.’’
Hendley pointed out the usual questions that
people ask themselves when they look into a
mirror: What have I done? What can I do? Who
am I?
‘‘You have a unique ability with what you do
every single day to change the world around you
through people, through relationships, through
the lives that you touch every day,’’ he told the
audience. ‘‘I want to encourage you. When you
get back, don’t look at all the stuff in the past.
Start with today. Start with tomorrow. And use
the resources that you have to make a huge
impact on your community and your world.’’
Attendee Cindy Lefton, PhD, RN, from
Missouri, described the closing speaker in three
words: dynamic, humble and passionate.
Although Hendley is not an emergency nurse,
Lefton felt the audience could definitely relate to
his message.
‘‘He talked about helping people when times
are really difficult and resources are difficult,’’ she
said. ‘‘It’s all about digging deeper in yourself to
find that skill set and energy to face whatever
adversity is before you.’’
By Kendra Y. Mims, ENA Connection
CLOSING SESSION
Closing Session speaker Doc Hendley, founder of Wine to Water, encourages emergency nurses to use their resources and look only to the future.

December 201228
Creating a Bigger Boom By Kendra Y. Mims, ENA Connection
Laura Giles, BS, RN, 2012 ENA Foundation chairperson, asked audience members to sound
their instruments if they either made a contribution or were the recipient of an ENA
Foundation scholarship or research grant. The sounds of drums and boomwhackers, used
during the Opening Session Drum Café presentation, could be heard throughout the room.
‘‘Wow, I am impressed,’’ Giles said. ‘‘But I must say, wouldn’t it be fantastic if we could
make even more noise? I would love to hear this room explode with the sound of every
drum. And I’m confident that we have the ability to create a bigger boom.’’
Attendees continued banging their drums in excitement as Giles shared how the
generous contributions and the dedication of donors have helped the ENA Foundation
achieve many accomplishments in 2012, including providing 20 Annual Conference
scholarships, 47 academic scholarships and five research grants to members. Giles also
discussed the success of the 2012 State Challenge.
‘‘We reached our goal and raised over $116,000,’’ she said. ‘‘One hundred percent of these
funds will go toward supporting scholarship applications and research grants in 2013.
Because we raised more money this year, we will have more to give back to you next year.’’
Giles ended her speech by sounding her drum for the members, the ENA Foundation
Board of Trustees and Management Board and everyone else who contributed to making
2012 a successful year.
‘‘It all adds up,’’ she said. ‘‘Your donation — large or small — makes a difference in the
number of scholarships and research grants we can fund. Please consider making the ENA
Foundation one of your charities of choice today and in the future.’’
ENA FOUNDATION
SPARKLE AND SHINE: Attendees fill out bids for jewelry items during the ENA Foundation Jewelry Auction held at Annual Conference in San Diego. States, chapters and individuals donated 171 pieces of jewelry, which raised more than $20,500 for the ENA Foundation to be used toward grants and scholarships for emergency nurses.
TAKE ME OUT TO THE
BALLGAMEIt was root, root, root for the ENA Foundation on Friday night, Sept. 14, at Petco Park, where more
than 740 emergency nurses joined the ENA Foundation in watching the San Diego Padres
host the Colorado Rockies.

Official Magazine of the Emergency Nurses Association 29
Tales from the ED: Creating Your Happily Ever AfterAttendees of the ‘‘Plot or Character?’’ session
learned how to identify and solve clinical
problems by using storytelling to determine if
the problems derive from a character-driven or
plot-driven story.
‘‘Storytelling is a valuable source of
information. It can highlight processes or
players that are problematic,’’ said Lisa Wolf,
PhD, RN, CEN, FAEN, director of the ENA
Institute for Emergency Nursing Research.
“Storytelling is powerful. It helps us connect
and recognize each other as one of us. It helps
us to vent and helps relieve stress.’’
When using stories to identify problems,
Wolf said, the first step is recognizing whether
you are dealing with a process or character
problem.
‘‘Read the story — the chart — to find the
villain,’’ she told the audience.
A character or villain could include anyone
from personnel, septic patients or heroic nurses
to colleagues, visitors, unaware nurses or
inattentive doctors. On the other hand, plot-
driven problems can stem from the environment
of care, terrible dialogue, procedures, props, the
setting or individual and environmental factors.
What are some solutions for these stories?
Wolf recommended fixing processes (such as
hand-offs) for plot-driven stories or educating,
disciplining or removing the villains in character
stories.
She encouraged the audience to write down
critical elements of their stories and compare
them with others to discover similarities in
characters, plots, villains and settings. She also
reminded attendees to remember the ‘‘moments
of grace’’ stories, which include good processes,
good staffing and good knowledge, and to
recognize the heroes in these stories.
‘‘These are equally important stories to
analyze because they tell you things that are
going well,’’ Wolf said.
Kendra Y. Mims
You Stuck What Where?Have you ever come across a patient who had a
flying insect in his ear or had to treat a child
with a bead lodged in her nose?
‘‘You Stuck What Where? Chatting About
Foreign Objects,’’ a fast-track session, was
packed with audience members interested in
exploring the recognition and treatment of
patients presenting with foreign bodies. Jeff
Solheim, MSN, RN-BC, CEN, CFRN, showed
vivid pictures of patients who experienced
foreign bodies in their nose, ears, eyes and GI
tracts. Solheim discussed how to detect
the symptoms of foreign objects in these
areas, as well as upper-airway
obstruction for children and adults.
Attendees received a brief overview
on the removal of foreign bodies, as
well on as the removal of insects from
the external ear. The session also
included esophageal vs. tracheal
obstruction x-rays and how to identify
the differences between the two, and a
brief discussion on the complications of
GU and rectal insertions and symptoms
of toxic shock syndrome.
Attendee Erin Scarlett, BS, RN, CEN, said
Solheim kept the session interesting by covering
a number of different areas as well as treatment
options. Attendees left the session knowing
some of the symptoms of foreign bodies and
how to remove them.
Kendra Y. Mims
Emergency Nurses Play ‘Jeopardy’ From naming famous fictional doctors on
television to identifying medication that has
resulted in more deaths than illegal drugs,
attendees of the ‘‘Emergency Nursing Jeopardy’’
session had a chance to learn about emergency
medicine topics in a game format. Some
attendees volunteered to play on teams to earn
points, while the majority played along silently
as audience members. Active players were
drawn from the list of volunteers and split into
three teams based on work shift: the AMs, the
PMs and the Nights.
Nurses took well to the fun, interactive
session in which the teams played two rounds
that included categories of Too Fast, Too Slow,
Pretend RNs, Eponyms, Pretend MDs,
Toxicology, Math is Hard and more. As the
session’s lecturer and game host, William
Hampton, DO, MM, BA, AS, presented the
questions, players used an electronic game
system to buzz in and earn points.
Trauma was the category of the ‘‘Final
Jeopardy’’ round. The big question of the game
was, ‘‘What is the
second-most
common cause of
traumatic death in
the age group of 1
to 4 years old?’’
The Nights were
the only team to
answer correctly
(drowning);
however, all team
players walked
away with a prize.
‘‘I come to these conferences because I love
all of you dearly — I love working with nurses,
and I feel a great camaraderie here,’’ Hampton
said as he presented gifts to all of the team
players at the end of the game. The AMs
received coffee mugs, the PMs took home
inspirational notebooks with ‘‘Lost Proverbs of
the ED’’ and the Nights received Snuggies with
the ENA logo.
Christine McEachin, MBA, RN, of Michigan,
said she enjoyed how the session used a
game-style approach as a learning tool.
‘‘I like that it was a light-hearted approach
to a serious topic of what we do in emergency
nursing,’’ she said. ‘‘I learned a ton of stuff
— for example, the antidote for calcium
channel blocker. I do mostly trauma now, so for
Concurrent Sessions
Continued on page 30
The Nights wearing their Snuggies qfter “Emergency Nursing Jeopardy.”

me that was great because I didn’t know that.
There were some things we did definitely
know, but then other things we learned, like
the rhythms, because he picked rhythms that
are not as common of presentation, and it was
good to realize they don’t all look the same.’’
Kendra Y. Mims
‘The No. 1 Suicide Magnet’In ‘‘A View From the Golden Gate Bridge: A
Forensic Look at Suicide,’’ speaker Cheryl
Randolph, MSN, RN, CEN, CPEN, CCRN,
FNP-BC, opened with scenes from ‘‘The
Bridge,’’ a 2006 documentary by Eric Steel
which included one year’s worth of filming at
the iconic bridge, focusing on the suicides and
attempted suicides.
‘‘The Golden Gate Bridge is what we call a
suicide magnet,’’ Randolph said, ‘‘meaning that
it’s a specific geographic area that tends to draw
those individuals who are contemplating or
want to kill themselves. It indeed is the No. 1
suicide magnet on planet Earth.’’
Randolph pointed out that in the medical
literature, the term ‘‘commit suicide’’ is not used.
‘‘One either attempts suicide, or they
complete suicide, meaning that they did die,’’
she said. Patients also may make a suicide
gesture, which has low lethality and is often
made to seek attention.
There is no exact count, but estimates put the
number of people who have jumped off the
Golden Gate Bridge and ended their lives since
1937 at 1,500, with an average of 27 per year.
This does not include unconfirmed suicides.
The 240-foot plunge from the pedestrian area
of the bridge takes about four seconds, and
people fall at a rate of 75 miles per hour, with
an impact force of 15,000 pounds per square
inch. Randolph showed slides of some of the
types of devastating injuries suffered by people
who have jumped, including burst lacerations,
internal hemorrhage and burst evulsions.
‘‘By jumping at these great forces, injuries are
catastrophic,’’ she said. ‘‘Organs burst, bones
break, great vessels are pierced. Sometimes
there is not a lot of outward trauma on the
body, but the body will be just covered in
hematoma. The body will be black and blue.’’
In addition to the injuries, people who jump
from the bridge are also at risk of dying from a
combination of drowning and hypothermia,
Randolph said. The water near the bridge is
generally about 47 degrees, and those who
plunge in tend to go to a significant depth of at
least 100 feet.
While the California Coast Guard has two
ships standing by 24 hours a day to respond to
people who jump from the bridge and can
reach the area within five minutes, ‘‘as you
know, five minutes, with someone who has
these catastrophic injuries, more likely than not,
the damage is already done and this person has
expired,’’ Randolph said.
‘‘Initially I was disappointed that it was a
replacement session,’’ said attendee Linda Whitt,
BSN, RN, CEN, of Virginia. ‘‘But I did learn a lot
about the etiology of death from this particular
mechanism. I was enlightened, also, about the
increased likelihood of people in my profession
committing suicide — the doctors and nurses
— and that it’s the fourth-leading cause of
death. So I’m glad I stayed.’’
Amy Carpenter Aquino
Connecting with Patients and Families in Tough SituationsThis fast-track session focused on helping
families and patients work through crisis,
sudden death and end-of-life decisions and how
emergency nurses can improve their experience
during difficult times.
Presenter Suzanne O’Connor, MSN, RN, APN,
shared her experience with comforting the
parents of patients in critical condition.
Though O’Connor talked about the
importance of assuring families that their loved
one is in good hands, she also warned the
about making promises.
‘‘I would never say to someone, ‘He’s going
to be all right,’ because they will hold you to
that,’’ she said.
“When a loved one is dying in the ED,
always switch your care from intensive help
with the patient to now taking care of the
family. Focus on the family. They are the ones
who are going to remember this night. The
patient is going to die, so we need to transfer
our care over to the wife, the mother
or whoever you’re working with.’’
O’Connor also offered tips on gaining a
patient’s trust: listening to his or her perspective
before offering one; underpromising and
overdelivering (e.g., estimating wait times);
following through and being consistent as a
team; being honest; building confidence,
managing priorities and never losing hope.
‘‘Patients need to feel confident and trust us,’’
O’Connor said. ‘‘The No. 1 person is you, the
consistent relationship. You are the No. 1
consistent voice and face that they want to
connect with and the face and voice of that ER
experience. Update them often about what you
know. Information is the No. 1 need.’’
She also discussed studies showing that
patients find it comforting when nurses explain
the benefits of medications and tests, as well as
when they address them by their first name.
The session ended with a brief Q&A.
Attendees asked about approaching families to
donate organs, working with social workers and
dealing with denial about a dying loved one.
‘‘I do it slowly and in increments and through
pictures and drawings,’’ O’Connor told the
attendee who asked for advice about denial. ‘‘I
say, ‘It’s pretty serious and here’s what we are
worried about.’ Let them stay with their denial,
but talk about your concerns for their loved one.
Ease into it as slowly as you can. Use a key
family member who has the most influence.
‘‘They will never, ever forget you as an ED
nurse,’’ she told attendees. ‘‘You will always be
a valuable memory for them.’’
Kendra Y. Mims
December 201230
Concurrent Sessions
Concurrent Sessions Continued from page 29

Official Magazine of the Emergency Nurses Association 31
Killer Headache‘‘I was looking at my colleague, and pieces of her started to disappear.’’
Thinking that her retinas were detaching, Mary Ann Teeter, MSEd., RN,
CEN, CNRN, FNP-C, immediately called her ophthalmalogist, who
examined her and diagnosed her with an ocular migraine.
‘‘I thought, ‘I need to find out more about this,’ ” said Teeter, an
emergency nurse since 1976, who presented this fast-track session with a
focus on how migraine is related to stroke.
Migraine is the result of cranial blood vessel vasodilation, and the
neurogenic inflammation exacerbates the pain, she said. She described the
two types of migraines — with aura and without aura — and the four
stages of migraine, with slide illustrations of the brain affected by migraine.
Patent foramen ovale — a hole between the left and right atria of the
heart that fails to close after birth — is the main stroke risk factor for
patients with a history of migraine, Teeter said.
‘‘We find that a lot of our younger patients — 30s, 40s, 50s — who
come in with symptoms of stroke have PFO,’’ she said.
Teeter showed a slide of a CT scan of brain showing hydopense areas
in the right occipital lobe consistent with a recent posterior cerebral artery
ischemic infarct. She pointed out the dying and dead brain tissue of the
infarct.
She shared common triggers for migraine as well as management
medications and techniques.
‘‘There are apps out there for migraine management,’’ Teeter
said. ‘‘You can be mobile and manage that as well.’’
“I thought it was really good,” attendee Deborah Skeen, BSN,
RN, CEN, of Colorado, said of the session. ‘‘I never realized there
was a connection between migraine and stroke. It was helpful
for me to learn that it’s the patients who have auras that are
especially the ones to look out for. … I thought it was good to
point out the symptoms that could come across for an ocular
stroke or a hemiplegic migraine or a real stroke; it helps you
keep the good differentials in your mind when people come in
with those symptoms.’’
Amy Carpenter Aquino
The Most Bizarre and Unusual Trauma Case Studies in Emergency Medicine 2012 Nearly every seat was filled for this concurrent session jam-
packed with information on how to treat the most difficult
trauma cases, culminating with a review of the care of victims
from the 9/11 terrorist attack on the Pentagon.
Allen C. Wolfe, MSN, RN, CFRN, CCRN, CMTE, focused on
airway management — which he called ‘‘the defining skill in
emergency medicine’’ — in many of the case studies he presented.
In the case of a 24-year-old male who blew off his face with a
shotgun, Allen described the difficulty of intubating a patient
with no facial structure. During the treatment, a nurse suggested
intubating the patient from the front, and Allen showed the
actual video made of the inverse intubation of a gunshot wound
to the face. He also showed slides of CT scans taken following
several hours of surgery, showing the reconstruction of the
patient’s jaw from his fibia.
Allen also presented the case of a male construction worker
who was brought into the ED after surviving a plaster explosion.
Photos showed the man’s face completely covered by a white
plaster used for bridge construction. Concerned about the
patient’s airway, Allen described how he and another nurse pulled enough
of the hardened plaster away to intubate him. Allen then called the
hospital’s burn unit for advice on how to approach removing the rest of
the hardened plaster, and was told to apply mayonnaise. He ran down to
the cafeteria, got a tub of mayo, ‘‘and believe it or not, we put it on and
the plaster came right off his face,’’ Allen said.
Allen concluded his lecture with a review of the treatment of nine victims
from the 9/11 attack on the Pentagon, from the initial call to Washington
Hospital Center to patient resuscitation in the ED and their outcomes.
‘‘There was not one broken bone, not one brain injury — only burns,’’
Allen said. All the patients suffered severe damage to their hands from
using them to find their way out of the building.
While the physical and emotional toll on emergency staff caring for
those patients on that day cannot be overstated, ‘‘the rewards are
immense,’’ he said.
Amy Carpenter Aquino
Whatcha Lookin’ At, Doc?There is never one right answer, only a better answer, when deciding
which test to run on a patient who presents to the emergency department
with unexplained pain or illness. In this session, William A. Gluckman,
S e p t e m b e r 1 1 - 1 5 • S a n D i e g o
2 0 1 2 A n n u a l C o n f e r e n c e
RefreshRevitalizeInvigorate
Concurrent Sessions
Continued on page 34

Hundreds of Annual Conference attendees filled
the room for the Sept. 15 town hall meeting in San
Diego. Members brought several questions and
comments to the ENA Board of Directors on topics
ranging from the Government Affairs Committee
annual workshop and recognition of ENA national
award winners to General Assembly resolutions
and access to ENA staff in the exhibit hall.
The board, led by 2012 ENA President Gail
Lenehan, EdD, MSN, RN, FAEN, FAAN, extended
the time allotted by 30 minutes to accommodate
all members who wished to express their views.
‘‘We know people have a lot on their mind, and we want to hear about
anything you want to talk about,’’ she said.
Before hearing questions, Lenehan explained that JoAnn Lazarus, MSN,
RN, CEN, 2012 president-elect, and Deena Brecher, MSN, RN, APRN,
ACNS-BC, CEN, CPEN, had met
previously with several GAC
chairpersons, who had given the board
members ‘‘quite a bit of feedback.’’
Because that discussion was held
separately, questions about the GAC
workshop would be heard at the end of
the town hall meeting.
One member asked why there was not
more recognition of the national ENA
award winners.
‘‘I will be at the Gala, but for the rest
of my colleagues who cannot make the
event tonight, they should be aware of
who the winners are,’’ she said.
In addition to recognition at the Sept. 15 Gala, all national ENA award
winners are recognized on page 24 in this issue of ENA Connection.
Member Elizabeth Whetzel, RN, asked the board about progress on her
resolution, Emergency Nursing and Forensic Nursing, which was
approved by the 2011 General Assembly.
‘‘We don’t seem to have a good process for providing
feedback on resolutions that have gone through,’’ she said.
Lenehan said ENA was working on improving the process of
reporting progress on resolutions, while board member Ellen H.
Encapera, RN, CEN, reported that the forensic nursing resolution
had inspired ENA to work with the International Association of
Forensic Nursing. ENA Executive Director Susan M. Hohenhaus,
LPD, RN, CEN, FAEN, explained that ENA began a dialogue with
IAFN halfway through the year and that the organizations were
working to share resources and expertise.
A member from Louisiana asked why ENA staff did not have a
designated spot in the Exhibit Hall at this conference, in contrast
with previous ENA conferences. Nancy Bonalumi, MS, RN, CEN,
FAEN, an ENA past president, added that she and other members
missed the opportunity for face-to-face contact with staff.
Hohenhaus explained that ENA has been scaling back on the
ENA Pavilion area of the Exhibit Hall as attendee evaluations
showed that traffic in the pavilion did not justify the amount of
staff resources dedicated to maintaining the space. A member of
the new ED Operations Work Team suggested posting times
when staff would be available to meet with members, similar to
how poster presenters are scheduled to meet with attendees. Jill
McLaughlin, BSN, RN, CEN, CPEN, suggested taking advantage
of technology, such as Web conferencing and Skype, to connect
attendees and ENA staff at the new Digital Den.
Kay Ella Bleecher, MSN, RN, CEN, FNP-C, NREMT-P, PHRN,
requested that board members share notice of when they plan
to represent ENA at other organizational conferences.
‘‘If you’re sending someone from national to our state, we
would like to meet and greet them,’’ she said.
The board heard attendees’ comments on nine different
topics and also encouraged members to send additional
questions, concerns and feedback to them via e-mail.
‘‘Know that we take your comments to heart,’’ Lenehan said.
Attendees Turn Out For Spirited Town Hall Meeting
ENA Foundation Thanks You for Your 2012 Jewelry Auction SupportThe 2012 ENA Foundation board sincerely thanks you for your support for this year’s successful jewelry auction. From necklaces to watches to duck calls, the jewelry auction was a success.
The jewelry auction received 171 donated items and raised over $20,580. Proceeds from this fundraising event will directly support the mission of the ENA Foundation to provide education scholarships and research grants in the discipline of emergency nursing.
Your support makes a difference. We look forward to the next Jewelry Auction at the 2013 ENA Annual Conference, September 19-21 in Nashville, TN.
December 201232
By Amy Carpenter Aquino, ENA Connection
Conference attendees fill the room Sept. 15 for the annual town hall meeting, which shed light on a variety of topics.

Official Magazine of the Emergency Nurses Association 33
delegates suggested returning to paper ballots.
‘‘Thank you, everyone, for your great
comments yesterday concerning strategies for
how to move our election forward,’’ Moretz said.
The assembly passed as amended the
resolution Care of the Bariatric/Obese
Patient, authored by Joan Somes and the
Minnesota ENA State Council. The amended
clause called for ENA to ‘‘identify currently
available literature/education related to
prevention, assessment and safe care of the
bariatric/obese patient so that these concepts
can be incorporated into the appropriate new
and revised ENA products and programs.’’
The proposed resolution, TNCC Eligibility,
authored by the Massachusetts ENA State
Council and Diane Gurney, MS, RN, CEN, FAEN,
elicited impassioned debate culminating in
approval of wording that went beyond the
original language in supporting the resolution,
to say ‘‘only RNs or international equivalents
may hold TNCC provider status.’’ The Assembly
voted down a clause which would have allowed
upper-level nursing students to ‘‘take TNCC
content and testing over the course of a college
term as an emergency nursing elective taught by
a TNCC instructor without receiving verification
status/provider card.’’
The General Assembly passed as amended
the resolution Care of the Patient With
Chronic Pain, authored by the Arizona ENA
State Council, Tiffiny Strever, BSN, RN, CEN,
and Maureen O’Reilly Creegan, MSN, RN,
CNS-C, CEN, CCRN, FAEN. This resolution
asked for a review of the current research on
the care of patients with chronic pain in the
emergency department and dissemination of the
information as appropriate.
‘‘This proposed resolution is meant to
address our knowledge deficit related to best
practice to meet the needs of the pain patient in
the ED,’’ said supporter Charlann Staab, MSN,
BSN, RN, CFRN, of Arizona. ‘‘Chronic pain
management has drastically changed over the
last 10 years. Without having that current
information validated, it’s difficult to share and
incorporate it to reach optimal care.’’
The amendment inserted words ‘‘taking into
consideration state regulatory concerns that
affect the emergency care management of
chronic pain,’’ explained Deborah Spann, ADN,
RN, CEN, of Louisiana.
Delegates approved as amended the
resolution Use of Protocols in the ED Setting,
authored by Barry Hudson, BSN, RN, CPEN, and
Cam Brandt, MS, RN, CEN, CPEN, which called
for ‘‘collaboration with other professional
groups to develop operational definitions for
protocols and their impact on emergency
nursing practice and therefore the development
of a position statement supporting the use of
protocols in the ED setting.’’
‘‘I think this is extremely timely,’’ said
Maryland delegate Mary Alice Vanhoy, MSN,
RN, CEN, CPEN, NREMT-P. ‘‘For those of you
who follow the managers listserv, there are
consistent questions about who has protocols
and how to implement them.’’
‘‘Without protocols, my practice would be
dead in the water,’’ said a delegate who
identified himself as a flight nurse. ‘‘I’d be
forced to put oxygen on people and put them
on backboards. There is no need to go back to
the 1970s in our practice.’’
The General Assembly approved as amended
Defining Wait Time for ED Services,
authored by Meghan Long, BSN, RN, CEN, and
Nicole McGarity, RN, CEN, which called for ‘‘the
development of consensus statement definition,
in collaboration with appropriate emergency
care stakeholders, for a consistent ED metric
regarding the term ‘wait time’ as used in
emergency care settings.’’
McGarity said that after discussions with ENA
Executive Director Susan M. Hohenhaus, LPD,
RN, CEN, FAEN, about using technology to
facilitate meetings, the financial implications of
the resolution would be nominal.
‘‘I really think this is important work, and I
appreciate you working on the price tag,’’ said
Marcus Godfrey, RN, president of the California
ENA State Council.
The General Assembly passed as amended
the resolution Safe Discharge From the ED,
authored by Dawn McKeown, RN, CEN, CPEN,
and Deborah Spann, ADN, RN, CEN. The
original proposal called for the ENA Institute for
Emergency Nursing Research to ‘‘investigate
options for outside grant funding for the
research needed to promote nursing
competence for discharging patients; and
publish the findings for use as resources in the
development of ED policies and procedures.’’
The amendment, suggested by IENR Director
Lisa Wolf, PhD, RN, CEN, FAEN, allows ENA to
expand the resources used in the investigation
to other ENA departments and personnel.
The General Assembly also passed the
resolutions Healthcare Worker Fatigue,
authored by the Tennessee ENA State Council,
the Utah ENA State Council and Beth Broering,
MSN, RN, CEN, CPEN, CCNS, CCRN, FAEN; and
Palliative Care, authored by Colleen Vega, RN,
CEN; Kim Sickler, MS, RN, CEN; and Garrett
Chan, PhD, RN, CNS, CEN, FAEN, as well as a
number of consent agenda items consisting of
various bylaws amendments. It rejected the
proposed bylaws amendment Resolutions
Committee Responsibility, authored by the
ENA Board of Directors, which would have let
the committee independently propose
amendments.
The deadline for 2013 proposed bylaws
amendments and resolutions is March 11.
General Assembly Debate Continued from page 19

December 201234
New ENA monthly offering for FREE Continuing Education with contact hours for our members.
• Available December 1Service and Quality1.0 contact hour Jeff Strickler, MA, RN, CEN, CFRN
Don’t miss out on enhancing your education. Go to www.ena.org/FreeCE for additional free continuing education opportunites.
The Emergency Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
DO, MBA, FACEP, presented several different
cases to attendees, asked them which test they
would perform, then showed them what to look
for on the corresponding radiograph.
Attendees correctly guessed that a 23-year-old
female patient presenting with RLQ pain for two
days could be suffering from an ectoptic
pregnancy. After running a lab test to confirm that
the patient is pregnant, an ultrasound should be
performed, said Gluckman.
‘‘Ultrasound is the best test for evaluating
gynecological and ovarian cases,’’ he said. ‘‘CT is
better for bowel and most solid organs.’’
Gluckman showed attendees ultrasounds of a
normal-looking early pregnancy and then showed
the difference in the ultrasound of an ectopic
pregnancy, pointing out the pseudo-gestational
sac in the ectopic pregnancy.
Attendees shouted ‘‘Gallbladder!’’ when
Gluckman presented the case of a premenopausal
42-year-old female patient who weighed 240
pounds, had recently eaten a fast food meal and
complained of several hours of pain and vomiting.
Gluckman showed a normal ultrasound of a
gallbladder filled with bile fluid and explained
that fluid appears black on an ultrasound. He then
showed an abnormal ultrasound of a gallbladder,
which showed no free fluid and pinpointed the
shadowing that indicated a gallstone.
‘‘It was good, it was informative,’’ said Emma
Gonzalez, RN, of Texas. ‘‘Usually it’s just the doctors
reading the X-rays, and sometimes they don’t get to
it quite right away, so if you know what to look for
you can grab your doc and go, ‘Hey, this is weird.
Can you come look at this with me?’ ’’
Amy Carpenter Aquino
leadership,’’ Hohenhaus said, adding that Wolf is ENA’s first
remote employee, telecommuting from her home on the
East Coast.
ENA spent significant time investigating its information
technology capabilities and limitations this year and found
that the organization was lacking in some areas, Hohenhaus
said. Guided by the principles of simplicity and constant
communication, ENA introduced several new devices and
technologies, including video conferencing and team sites
for committees, which reduced travel requirements and
lowered costs. Other advancements, such as a more
integrated use of ENA’s social media platforms, have
propelled the organization forward, she said. Further
technological enhancements and a focus on leadership
development and teamwork training — with new advocacy
and increased educational opportunities — will ensure an
even stronger future for ENA.
Noting that ‘‘ENA’s financial health matters to you,’’
Hohenhaus described the organization’s commitment to
revenue-sharing with state councils and developing an
educational design that includes blended learning, as well
as plans to revive the GENE and CATN programs.
‘‘We learned that we were a bit hasty in retiring CATN,’’
she said. ‘‘Our team is working on revising, refreshing and
renewing the program. GENE is also being revised and will
be more interactive.’’
Noting that the date of her presentation, Sept. 12, was
her one-year anniversary as ENA’s executive director,
Hohenhaus thanked the ENA Board of Directors, especially
2012 President Gail Lenehan, for their leadership and
support during ‘‘an incredibly fast-paced year.’’
Concurrent Sessions Continued from page 31
Talent and Technology Continued from page 19
Photo coverage of 2012 Annual Conference supplemented by Bruce Hood of Stryker.

Official Magazine of the Emergency Nurses Association 35
A Gift That Keeps Giving The holiday season is the perfect time to give
back and make a difference. If you are among
the many shoppers searching for special gifts for
family, friends or colleagues, consider making a
holiday donation to the ENA Foundation.
Donations are a great gift to
honor a special nurse, mentor
or another important person
in your life. Your contribution
to the ENA Foundation makes
a difference in your profession
and can make someone’s
holiday even more special.
ENA member Dorothy Duncan, DNP, RN,
CEN, ACNP-BC, CCRN, said she and her
husband engage in philanthropy usually by
donating to schools. This year, they decided to
place the ENA Foundation on their holiday list
as a charity of choice. At the 2012 ENA Annual
Conference, Duncan noticed that the New York
ENA State Council had established the academic
scholarship to remember fellow first responders
who lost their lives on Sept. 11, 2001.
In 2011, the New York State Council decided
to begin fundraising efforts to permanently
endow the 9/11 scholarship. They recently
reached the halfway mark to ensure that
emergency nurses never forget that fateful day
by honoring its memory.
Duncan felt the cause was very honorable,
and it inspired her to make a donation to the
ENA Foundation in honor of all 13 nurses in her
emergency department’s leadership group. Each
nurse received a Never Forget commemorative
pin. The rest of her staff, which consists of about
35 workers, received a Stretcherside Miracle pin.
Duncan’s staff was moved. As she explained why
she felt compelled to give
back, several were in tears.
Duncan said her staff felt
honored to wear their pins,
and she is proud to see
them displayed on their IDs.
Duncan also wears her pin
with pride as she believes
people should never forget about September 11.
‘‘That is the biggest thing,’’ Duncan said. ‘‘I
just think it’s very important to never forget
these kinds of very noble acts on the behalf of
first responders and emergency personnel,
HAZMAT and all types of response personnel.
This is a wonderful way to remember. This is a
very worthwhile cause. I would recommend
that people give back to the ENA Foundation all
the way.’’
As you reflect on those who have crossed
your path this past year, do you recall someone
who has motivated or inspired you? Mentored
or helped you to grow professionally or
personally? Paying homage to others by making
a contribution to the ENA Foundation is a gift
that definitely keeps giving.
Your donation
makes a difference.
Since 1991, the ENA
Foundation has given more
than $2 million in educational
scholarships and research grants to
emergency nurses. This year alone,
the ENA Foundation has funded 86
educational scholarships and research grants
in the total amount of $246,800. This could not
have been possible without the generous
donations received from individuals, ENA state
councils and chapters, corporations and friends of
emergency nursing.
The ENA Foundation offers the following
premium items, which make great holiday gifts
for your friends, family or colleagues:
• Donate $30 and you can elect to receive a
4GB thumb drive.
• Make a $10 donation to receive the Never
Forget commemorative pin.
• Make a $5 donation and you can select the
Stretcherside Miracle Pin.
There is still time to make your year-end gift.
You can make your donation on behalf of
yourself, or you can honor or remember
someone special to you by visiting
www.enafoundation.org today.
Every dollar counts toward advancing the
emergency nursing profession, this holiday
season and beyond.
By Kendra Y. Mims, ENA Connection
December 201236
ENA STATE CONNECTION
San Antonio ENA Chapter Submitted by Steven J. Jewell, RN
The San Antonio ENA marked a busy three months. The chapter hosted
an excellent CEN Review course in August for more than 78 nurses,
presented by Jeff Solheim, MSN, RN, CEN, CFRN, RN-BC, FAEN. In
September, the SA ENA held a two-hour Forensic Nursing in the ER
seminar that hosted 47 members.
With TNCC, ENPC, monthly meetings, seminars, Safety Whys
babysitting training courses and certification review courses, San Antonio
has provided more than 250 hours of continuing education and
community education for the region.
On Nov. 11, more than 40 medical and nursing professionals, provided
by the SA ENA, provided care for the San Antonio Rock & Roll Marathon.
The SA ENA is also excited to announce that its board of directors
approved a 2-1/2 day educational conference scheduled for May 8-10, 2013,
to be held at the Historic Menger Hotel. The conference will include a
three-hour educational seminar for managers, directors and chief nursing
officers, covering topics such as management, education and retention/
recruiting. The next two days will provide 11.75 continuing education
hours on topics including trauma, pediatrics, adults and forensics.
For more information, contact Steven J. Jewell, RN, at
Utah ENA Dixie Chapter Submitted by Debbie Young, BSN, RN
The Utah ENA Dixie Chapter held its sixth annual Southwest
Emergency/Trauma Conference Sept. 29 in St. George, Utah. This
anticipated all-day event was well-attended by emergency nurses and local
EMS and paramedics interested in the latest and greatest in emergency and
trauma care.
Topics this
year included
life flight in
Southern Utah,
pediatric triage
and
assessment,
rapid ECG
interpretation,
massive
transfusion protocol, respiratory emergencies and trauma assessment and
treatment. Many thanks to Cindy Hurst, ADN, RN, chapter president, and
Vikki Webster, BSN, RN, CEN, president-elect (both pictured below), who
spent countless hours preparing and organizing the conference. Not only
was it a success and offered the opportunity to earn continuing education
credits, it gave attendees a chance to network and see colleagues.
Development of the Lantern Award program criteria funded in part by Stryker, an ENA Strategic Sponsor.
B ecome a Lantern Award recipient
Apply today. Applications are due February 20, 2013.
DOES YOUR EMERGENCY DEPARTMENT
DESERVE RECOGNITION FOR
Exemplary Practice and Innovation?
To learn more and apply, visit : www.ena.org/IQSIP/LanternAward
T he ENA Lantern Award recognizes exemplary emergency departments that demonstrate exceptional performance and innovative practice in the core areas of:
• Leadership
• Practice
• Education
• Advocacy
• Research A Coaching Guide is now available to help you identify how best to demonstrate your emergency department’s achievements.
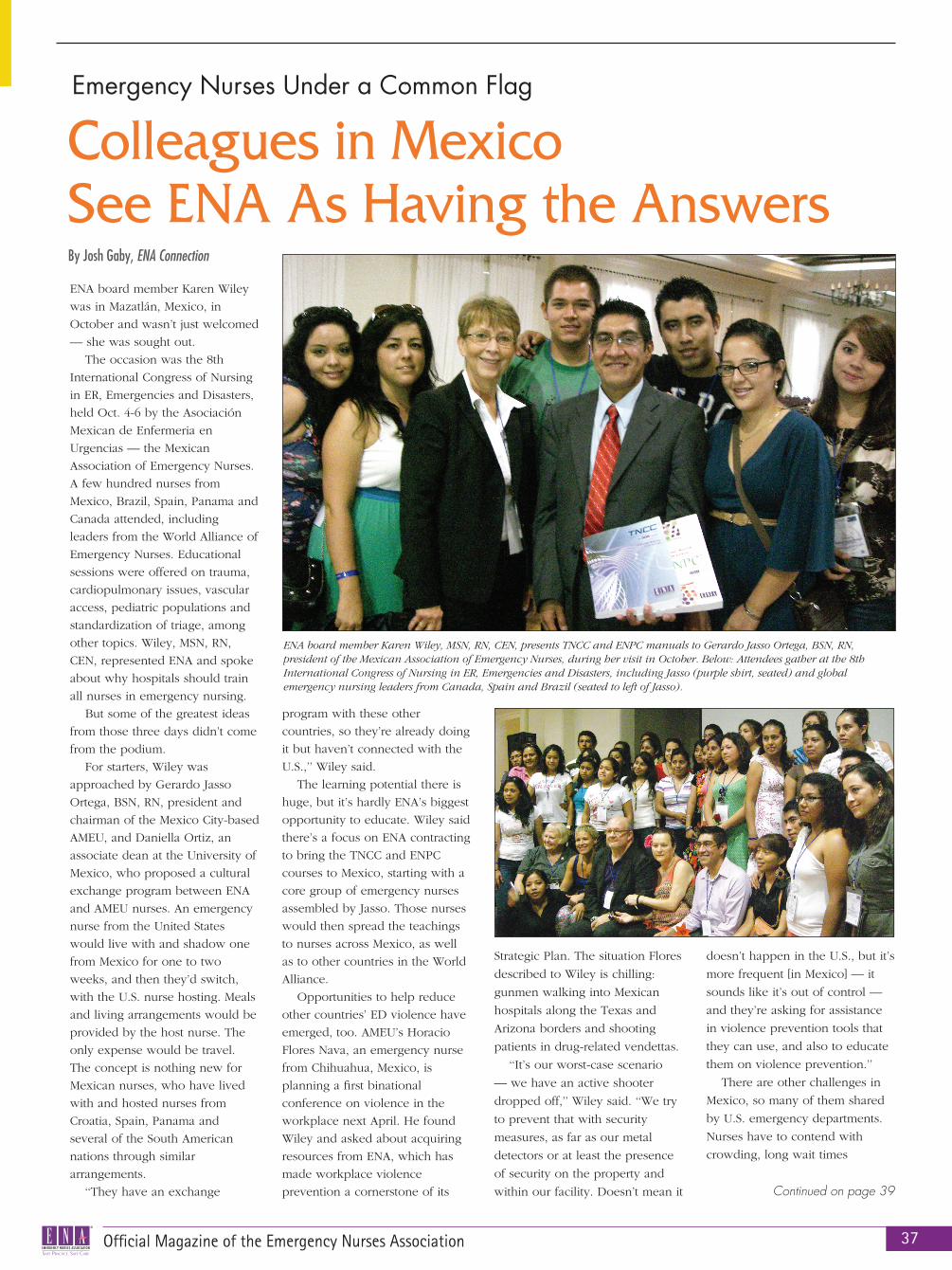
Official Magazine of the Emergency Nurses Association 37
ENA board member Karen Wiley
was in Mazatlán, Mexico, in
October and wasn’t just welcomed
— she was sought out.
The occasion was the 8th
International Congress of Nursing
in ER, Emergencies and Disasters,
held Oct. 4-6 by the Asociación
Mexican de Enfermeria en
Urgencias — the Mexican
Association of Emergency Nurses.
A few hundred nurses from
Mexico, Brazil, Spain, Panama and
Canada attended, including
leaders from the World Alliance of
Emergency Nurses. Educational
sessions were offered on trauma,
cardiopulmonary issues, vascular
access, pediatric populations and
standardization of triage, among
other topics. Wiley, MSN, RN,
CEN, represented ENA and spoke
about why hospitals should train
all nurses in emergency nursing.
But some of the greatest ideas
from those three days didn’t come
from the podium.
For starters, Wiley was
approached by Gerardo Jasso
Ortega, BSN, RN, president and
chairman of the Mexico City-based
AMEU, and Daniella Ortiz, an
associate dean at the University of
Mexico, who proposed a cultural
exchange program between ENA
and AMEU nurses. An emergency
nurse from the United States
would live with and shadow one
from Mexico for one to two
weeks, and then they’d switch,
with the U.S. nurse hosting. Meals
and living arrangements would be
provided by the host nurse. The
only expense would be travel.
The concept is nothing new for
Mexican nurses, who have lived
with and hosted nurses from
Croatia, Spain, Panama and
several of the South American
nations through similar
arrangements.
‘‘They have an exchange
program with these other
countries, so they’re already doing
it but haven’t connected with the
U.S.,’’ Wiley said.
The learning potential there is
huge, but it’s hardly ENA’s biggest
opportunity to educate. Wiley said
there’s a focus on ENA contracting
to bring the TNCC and ENPC
courses to Mexico, starting with a
core group of emergency nurses
assembled by Jasso. Those nurses
would then spread the teachings
to nurses across Mexico, as well
as to other countries in the World
Alliance.
Opportunities to help reduce
other countries’ ED violence have
emerged, too. AMEU’s Horacio
Flores Nava, an emergency nurse
from Chihuahua, Mexico, is
planning a first binational
conference on violence in the
workplace next April. He found
Wiley and asked about acquiring
resources from ENA, which has
made workplace violence
prevention a cornerstone of its
Strategic Plan. The situation Flores
described to Wiley is chilling:
gunmen walking into Mexican
hospitals along the Texas and
Arizona borders and shooting
patients in drug-related vendettas.
‘‘It’s our worst-case scenario
— we have an active shooter
dropped off,’’ Wiley said. ‘‘We try
to prevent that with security
measures, as far as our metal
detectors or at least the presence
of security on the property and
within our facility. Doesn’t mean it
doesn’t happen in the U.S., but it’s
more frequent [in Mexico] — it
sounds like it’s out of control —
and they’re asking for assistance
in violence prevention tools that
they can use, and also to educate
them on violence prevention.’’
There are other challenges in
Mexico, so many of them shared
by U.S. emergency departments.
Nurses have to contend with
crowding, long wait times
Emergency Nurses Under a Common Flag
By Josh Gaby, ENA Connection
Colleagues in Mexico See ENA As Having the Answers
ENA board member Karen Wiley, MSN, RN, CEN, presents TNCC and ENPC manuals to Gerardo Jasso Ortega, BSN, RN, president of the Mexican Association of Emergency Nurses, during her visit in October. Below: Attendees gather at the 8th International Congress of Nursing in ER, Emergencies and Disasters, including Jasso (purple shirt, seated) and global emergency nursing leaders from Canada, Spain and Brazil (seated to left of Jasso).
Continued on page 39
December 201238
Board Meeting Actions and HighlightsThe ENA Board of Directors met Aug. 22 via teleconference. All members
of the board were present and took the following actions:
• Approved the July 18 board of directors meeting minutes as corrected.
• Adopted the independent auditors’ report on the 2011 financial
statements as presented.
• Approved that ENA continue membership in the Institute of Medicine
Forum on Medical and Public Health Preparedness for Catastrophic
Events for one year.
• Referred the Rapid Practice Reference on Hemolysis back to the Clinical
Practice Committee for reconsideration because of the board’s concerns.
• Ratified Joanne Fadale, BSN, RN, as the replacement Retired Emergency
Nurses Special Interest Group facilitator, as presented.
The ENA Board of Directors met Sept. 11 in San Diego. All board
members were present and took the following actions:
• Approved development of a project plan for an Institute for Emergency
Nursing Education.
• Approved the following board governance policies:
° Conducting ENA Board of Director Business that Requires a Vote via
° Etiquette for Electronic Communication
• Approved the newly created position statement definitions, including
joint and consensus statements, as written.
• Approved the new Weighing Patients in Kilograms position statement as
written.
• Approved the following revised position statements as written:
° Specialty Certification in Emergency Nursing
° Professional Liability and Risk Management
• Approved sunsetting the following position statements:
° Autonomous Emergency Nursing Practice (3/2005)
° Care of the Older Adult (5/2012)
° Family Presence (9/2010)
° Hazardous Material Exposure (10/2009)
° Improving External Coding In Hospital Discharge and ED Data
Systems (4/2009)
° Prehospital EMS (12/2008)
° Smallpox Vaccination (12/2005)
° Substance Abuse (7/2010)
• Approved the following topics for Emergency Nursing Resources
in 2013:
° Acute Pain Management
° De-escalation
° Pediatric Dehydration
• Supported the Position Statement Review Committee’s request to decline
the development of an ENA position statement on the care of the stroke
patient in the ED as outlined in General Assembly Resolution 11-105,
and charged the Clinical Practice Committee with developing a clinical
practice rapid practice reference related to the care of the stroke patient
in the ED.
• The following represent actions to various requests from external
organizations that were supported by the Executive Committee:
° An invitation from Emergency Medical Services for Children to have an
ENA representative on the Organizational Panel during its Annual
Program Meeting, May 8-11, in Bethesda, Md. Deena Brecher, MSN,
RN, APRN, ACNS-BC, CEN, CPEN, represented ENA.
° An invitation from the Forum of Nursing Workforce Centers to attend
its 2012 Annual Conference June 27–29, in Indianapolis. Gail Lenehan,
EdD, MSN, RN, FAEN, FAAN, represented ENA.
° An invitation to attend the Department of Health/Human Services and
Assistant Secretary for Preparedness and Response Meeting on The
Impact of Drug Shortages on Emergency Care April 16, in Washington,
D.C. A workgroup was established from the attendees of this meeting
and a subsequent meeting was held July 12 – 13, in Washington, D.C.
Mary Alice VanHoy, MSN, RN, CEN, CPEN, NREMT-P, represented ENA
at these events.
° An invitation to attend a Health Resources and Service Administration
Affordable Care Act Discussion with Nursing Organizations hosted by
Dr. Mary K. Wakefield, April 30, in Washington, D.C. Susan M.
Hohenhaus, LPD, RN, CEN, FAEN, represented ENA.
° A request from the American Psychiatric Nurses Association for a letter
of support for an AHRQ grant application for a three-year project to
compile a toolkit of materials on pain assessment.
° An invitation to participate in the American College of Emergency
Physicians Geriatric ED Work Group to describe the standards for a
geriatric ED. Betty Mortensen, MS, BSN, RN, FACHE, represented ENA.
° An invitation from the National Council of State Boards of Nursing to
attend its APRN Roundtable meeting April 25 in Chicago. Betty
Mortensen, MS, BSN, RN, FACHE, represented ENA.
° An invitation from the National Institute of Occupational Safety and
Health to attend the National Conference for Workplace Violence
Prevention and Management in Healthcare Settings May 11 – 13, in
Cincinnati. AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, represented
ENA.
° An invitation from Dignity Health to present at its ED Summit May 31
– June 1, in Las Vegas. Gail Lenehan, EdD, MSN, RN, FAEN, FAAN,
represented ENA.
° An invitation from the American Nurses Association to support the
Joining Forces initiative of the White House and the first lady.
° A request from the American Nurses Association to endorse the
document Professional Nurse Coach Role: Defining Scope of Practice
and Competencies.
° A request to send a letter of support for a SAMHSA grant application
from the ENA president on behalf of the Center for Pediatric Traumatic
Stress, Children’s Hospital of Philadelphia, which will serve as a Level
II center in the National Child Traumatic Stress Network.
° A request from Duke University and the University of Cincinnati to
support a grant application for “Comparing Pain Management
Protocols for Sickle Cell Disease Patients in the Emergency
Department” with a letter from the ENA president.
° A request for a letter of endorsement from the Centers for Disease
Control and Prevention regarding its National Hospital Ambulatory
Medical Care survey.
° An invitation from the Pediatric Nursing Certification Board to attend
the Institute of Pediatric Nursing Invitational Forum, Nov. 1-2, in
August and September 2012

(particularly in the public hospitals), geriatric and pediatric issues and
the puzzle of accommodating behavioral health patients, most of
whom end up on regular hospital floors. The suicide rate among these
patients is high, Wiley said.
What hampers Mexican emergency nurses is a lack of resources,
from air conditioning to continued education. But they make up for it
in the simple stuff that bonds the profession. Wiley is recommending
including Jasso and other international colleagues in educational
sessions at Leadership Conference 2013 in Fort Lauderdale, Fla., and at
next year’s General Assembly in Nashville, Tenn., with interpreters on
hand to help them share their insights and experiences.
The lesson is that there’s much to be learned from each other. So
different, yet so alike.
‘‘I wasn’t aware of how unified emergency nurses are in their
passion,’’ Wiley said. ‘‘When I was asked to go to Mexico, I felt a crack
in the door — a door opened partway to the international community
and to Mexico. But once I arrived and met them and saw all the nurses
that attended from the other countries as well as throughout Mexico, I
thought, ‘Oh!’ — an entire door just kind of opened onto another
world. We had the same connection with emergency nursing and ENA
because they were just as passionate about emergency nursing as we
are. To me, it was like you never left your own emergency department.
It was like meeting people that you worked with daily. You just felt
that same connection.’’
Washington, D.C. Paula Karnick, PhD, ANP-BC, CPNP will represent
ENA.
° An invitation from RAND Health (under contract with the Centers for
Medicare and Medicaid Services) to suggest topic areas and items for
inclusion in a survey of patient experiences with emergency
department services.
° An invitation from Urgent Matters to designate two representatives to
its editorial board. AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN, and
JoAnn Lazarus, MSN, RN, CEN, will represent ENA.
• The following requests were not supported by the Executive Committee:
° An invitation from the Commission on Collegiate Nursing Education to
nominate candidates for its Board of Commissioners and the 2013
Nominating Committee.
° An invitation from the American Association for Emergency Psychiatry
to attend and speak at its Third Annual National Update on Behavioral
Emergencies Dec. 5-7, in Las Vegas.
° A request from the Society for Academic Emergency Medicine for
endorsement of its 2012 Consensus Conference, May 9-12, in Chicago.
° An invitation from the Vascular Disease Foundation to attend and
speak at the 2012 VESSEL Annual Meeting Sept. 21-23, in Tyson’s
Corner, Va.
° A request from the American Academy of Neurology for endorsement
of the guideline, ‘‘Update: Evaluation and Management of Concussion
in Sports.’’
Highlights of the next scheduled board of directors meeting will be
published in a future issue of ENA Connection.
Emergency Nurses Under a Common Flag Continued from page 37
The Board of Certification for Emergency Nursing (BCEN®) certifications help you take the next step in your career.Demonstrate your commitment to competency; earn a BCEN certification today.
Earn Your Mark of Distinction
Find out more...www.BCENcertifications.org
December 201240
During a recent conversation with a friend and co-worker, we were
discussing how we dealt with the uncertainty caused by the economic
meltdown in 2009. He said, ‘‘There was so much that I knew I couldn’t
control. I couldn’t control what was happening to the stock market, the
value of my home or to the employment status of my loved ones, so I
simply focused on what I could control. I did everything I could to
increase and enhance quality time with my family. I started running and
eating better so I could get in better control of my body. I devoured all
kinds of books to keep my mind sharp. We started paying closer attention
to our family finances. Basically I ‘cleaned my house’ and controlled my
controllables, hoping that the rest would work itself out, and my family
would be in a better place when it did.’’
This was an interesting perspective, and I often find myself applying
the same principle. When I have a big project, sometimes the best place
for me to focus is at home, and away from the distractions at the office.
However, pulling out my laptop is not the first thing I do — I clean my
house. I have to get everything else in order before I can focus on the
task at hand.
It’s no secret that the health care environment is undergoing drastic
change. We have reached the point where one Baby Boomer turns 65
every 10 seconds 1, obesity has risen to over 30 percent in some states 2,
nine out of 10 hospitals report ED boarding 3 and in 2020 we will have a
nursing shortage that is projected to reach 1 million.4 To pile on, the many
models of care and the uncertainty surrounding the Affordable
Care Act are causing more questions than answers.
In a time of such uncertainty, and when the issues and
complexities in health care seem so daunting, maybe the best
thing we can do is get back to the basics. What are the things in
your daily activities that you have complete control over? What
can you focus on doing better? Are you doing the things necessary
to take better care of yourself so you can take better care of your patients?
Of course, controlling the controllables sounds simple enough, but
making a change and sticking to it is often easier said than done. One of
the most difficult challenges with change is breaking old habits. As a
medical device manufacturer, we are constantly under regulatory scrutiny,
and compliance is key. We have found that the secret to compliance is to
make the complex problem as simple as possible. If those implementing it
realize it is to their direct benefit, and that the change will make their daily
activities simpler, safer and more efficient, it becomes very natural.
2012 will be wrapping up before we know it, and the only guarantee in
the coming year is that there will be change. As we set our goals for 2013,
let’s focus on controlling the controllables and making the complexities of
our personal and professional lives as simple as possible, so we are ready
to embrace the changes ahead.
References
1. AARP. (n.d). Boomers at 65: Celebrating a milestone birthday. Retrieved
from www.aarp.org/personal-growth/transitions/boomers_65/
2. Centers for Disease Control and Prevention, Vital Signs. (n.d). U.S. state
info: Adult obesity. Retrieved from www.cdc.gov/vitalsigns/
AdultObesity/StateInfo.html
3. Rabin, E., Kocher, K., McClelland, M., Pines, J., Hwang, U., Rathlev, N.,
... Weber, E. (2012). Solutions to emergency department ‘boarding’ and
crowding are underused and may need to be legislated. Health Affairs,
31(8), 1757–1766.
4. American Hospital Association. (2007.) When I’m 64: How Boomers will
change healthcare. Retrieved from www.aha.org/content/00-
10/070508-boomerreport.pdf
Grow your career when you become part of ENA Leadership Conference Faculty. Share your leadership knowledge, experience and skills to help grow the profession of emergency nursing.
Do you have specific knowledge in a particular area of emergency nursing, management or policy?
Has a particular experience given you new insights into a current issue or trend and led to new best practices?
Do you have experience dealing with leadership challenges and issues?
Establish Yourself as a Leader
Submission Deadline is March 25, 2013
• Management• Operations• Government affairs• Technology• Team building• Research• Education
• Advance practice• Orientation• Retention• Community relationship building• Customer satisfaction• Personal and professional development
Find full information and course proposal guidelines at www.ena.org and click on Leadership Conference 2014 Call for Course Proposals in the Calls and Opportunities Section. We look forward to hearing your cutting-edge course ideas.
Share your insights related to current issues, trends, and best practices as a faculty member at ENA Leadership Conference 2014, March 5-9 in Phoenix, Arizona
Topic areas:
Join the faculty for ENA Leadership Conference 2014, Phoenix, March 5-9
Controlling the Controllables
2012 ENA State Council and Chapter Innovation Grant Recipients AnnouncedThe recipients of the ENA
Innovation Grant awards for
state councils and chapters
have been announced.
Selection of the award
recipients involved many
factors to ensure alignment
with ENA’s mission, strategic
plan, goals, activities, budget
and sustainability. The
winners are:
• Head Injury Prevention
Campaign – Alabama State
Council, Audra Lowery Ford,
president: $5,490
• Violence Survey in
California’s Emergency
Departments – California
State Council, Marcus
Godfrey, president: $7,118
• Injury Prevention Radio
Ads – Central Minnesota
Chapter, Colleen Seelen,
immediate past president:
$5,412
• Multi-faceted Video
Communication – Talk
Fusion – Missouri State
Council, Teresa M. Coyne,
president-elect: $10,000
• Web/Virtual Meeting
Plan and System – New York
State Council, Kathy Conboy,
president-elect: $5,000
• Web Conferencing –
Texas State Council, Rhonda
Manor-Coombes, web
chairperson: $1,980
• Trauma Trot and Kids
Safety Expo – Shenandoah
Chapter, Brenda Hoops,
president, and Paula Neher,
chapter member: $5,000
• Washington ENA and
British Columbia ENA
Emergency Nursing Confer-
ence – Washington State
Council, Roger Casey,
president: $10,000
By Kim Edwards, Associate Marketing Communications Manager, Stryker Medical
Recruitment Ads
Recruitment Ads
Recruitment Ads

be happy.
You know us as recognized ED leaders who guide hospitals toward real and
effective change. Now we would like to get to know you. Blue Jay Consulting is
looking for professionals with the leadership insight and clinical experience to
bring process improvements to our clients, and the passion and commitment to
enhance the overall quality of emergency care. If you consider yourself among
the best in your field, you’ll find yourself in good company at Blue Jay Consulting.
Join the strongest team in the industry and... be happy.
www.bluejayconsulting.com
Contact Jim Hoelz or Mark Feinberg at 407-210-6570 to discuss how we can capitalize on
one another’s strengths.
“ As a Blue Jay Consultant, I apply the skills and experience I have gained in my nursing career every day. Each assignment brings new challenges and opportunities to make a difference for ED staff and the patients they care for. My work touches the lives of many people. I love what I do and the colleagues and clients I work with.”
— N A N C Y B O N A L U M I , R N , M S , C E N
Director
Blue Jay Consulting, LLC
When you’re on the right team, happiness ensues.