Embed Size (px)
DESCRIPTION
ENA Connection - October 2012
Citation preview

INSIDE FEATURES
the Official Magazine of the Emergency Nurses Association
October 2012 Volume 36, Issue 9
connection
Sidestepping Potential Pitfalls in Research PAGE 4
ENA Launches the ENPC Revision Course PAGE 8
Sharing the Innovations and Best Practices of the 2012 Lantern Award Recipients PAGE 26
ENA Foundation’s 2012 Scholarship and Research Grant Recipients PAGE 36
Here Comes the StunPreparing Now Means Your ED Won’t Be Blown Away When Calamity Turns the Community Upside-DownSpecial Disaster Readiness Section, Pages 10-23

Stryker is proud to be an ENA Strategic Sponsor and support nursing excellence through important initiatives such as the ENA Workplace Injury Prevention Toolkit and the ENA Lantern Award. Program Criteria for the ENA Lantern Award funded, in part, by Stryker.
Reinventing Patient Transport
Stryker is proud to be an ENA Strategic Sponsor and support nursing excellence through important initiatives such as the ENA Workplace Injury Prevention Toolkit and the ENA Lantern Award. Program Criteria for the ENA Lantern Award funded, in part, by Stryker.
Stryker has been your partner in patient transport for over 70 years. We understand that when you are transporting patients, the details really matter.
In our latest innovation, Stryker partnered with the Michael Graves Design Group to focus on just that - the details.
Together, we designed a solution that delivers functional beauty, exceptional durability, intuitive operation, and enhanced safety for caregivers and patients.
We are committed to caring for the caregivers and their patients, and we are changing the way patients are transported... again.
For more information, contact [email protected].

Official Magazine of the Emergency Nurses Association 3
This year at ENA’s Annual
Conference in San Diego,
Karen Daley, president of
the American Nurses
Association and a longtime
friend and emergency nurse colleague, delivered the
Anita Dorr lecture. Her personal story is a poignant
reminder of what could happen to any one of us.
In the summer of 1998, while working in the ED,
Daley was stuck by a needle protruding from a sharps
container. A few months later, she learned that her
flu-like symptoms were because of Hepatitis C and
HIV. She didn’t know whether she would live or die.
What she did know for sure was that her injury had
been preventable. She was determined to tell her
story so others would be protected, and she became
an activist. As the then-president of a state nurses
association, she had a voice, which she used to the
fullest and lobbied for the Federal Needlestick Safety
& Prevention Act of 2001.
Daley’s talk reminded me of how far we’ve come,
but also of how far we have to go.
While the rate of sharps injuries seems to be going
down, in 2010 in Massachusetts alone there were
2,947 sharps injuries among hospital workers (250 of
them in the emergency department), and 53 percent
of the sharps injuries reported involved sharps
without any sharp injury prevention features.1
We do not know how many of those sharps
injuries resulted in illness or even death.
Massachusetts does not have those figures. A 1998
CDC study found that, of health care workers who
had been exposed to blood in the workplace, 2-4
percent developed Hepatitis C infections, which have
a high rate of chronicity and potential for chronic liver
disease and liver cancer.2
Labels for sharps are misleading, since there is no
definition and no standard specification for a ‘‘safety
needle’’ or ‘‘safety device.’’ Some so-labeled can be
even more dangerous than the old needles,
particularly if the device requires a second hand to
somehow cover the needle.
In contrast, look at the attention to the safety of the
public. Over the last few years, as many as 1.5 million
baby strollers have been recalled because three
children sustained fingertip amputations and two
adults smashed their fingers in hinges on the stroller,
according to news reports. There was no need to pass
legislation to reduce the number of dangerous
strollers or increase efforts to educate consumers to
better operate the strollers with retrofitted ‘‘safety
hinge’’ devices.
Would we tolerate a situation in which the general
population was at similar risk in their daily lives, of
being stuck with a needle contaminated with tainted
blood? Would we be as complacent as we have been
with our nursing and physician colleagues?
Look at the attention to the safety of workers in
industry. When a friend who had worked for years as
an occupational health and safety nurse in industry
began to work with a nursing association and visited
hospitals, she was amazed at what she found. Nurses
and other staff might be told to follow a certain
detailed safety regimen, but it was sometimes
followed with ‘‘when possible.’’ If it wasn’t possible to
follow the guideline, the health care worker was told,
‘‘Be careful.’’
The public, and much of industry, is afforded
passive (automatic) protection by such features as
airbags and meat-slicing guards, and nurses deserve
no less.
The authors of an in-depth safety study concluded
that ‘‘we provide clear evidence that passive [fully
automatic] safety engineered devices (SEDs) are more
effective than active [requiring the user to activate]
SEDs for needlestick injuries (NSI) prevention. Passive
devices require no input from the user, and this is
Dates to Remember
PAGE 4ENA Research
PAGE 6Pediatric Update
PAGE 11Feedback Frame
PAGE 28ENA Call For ...
PAGE 31ENA Connected
PAGE 32Washington Watch
PAGE 34Academy of Emergency Nursing
PAGE 36ENA Foundation
PAGE 38State Connection
PAGE 40Board Highlights
Monthly Features
Oct. 8, 2012 Course proposal deadline for those seeking to be selected as faculty for 2013 Annual Conference in Nashville, Tenn.
Oct. 24, 2012 Deadline to apply to become a contributing author of forthcoming Emergency Nurse Advanced Critical Thinking (ENACT) course (www.ena.org).
March 15, 2013 Deadline for proposed bylaws and resolutions for 2013 General Assembly at Annual Conference in Nashville, Tenn.
PAGE 8ENA Launches the ENPC Revision Course
PAGES 10-23Disaster Preparedness Section
10 Board Writes: Are You Ready for the Real Thing? Considerations for Disaster Preparedness Exercises
12 The Use of SBAR to Facilitate Patient Communication During a Disaster
14 Disaster Nursing Education: We Must Be Working, Learning as One 16 Measuring the Effectiveness of a Communitywide Disaster Drill
18 Focus on Hurricane Preparedness
20 Mass Casualty Patient Decontamination
22 Ready or Not: What Does It Take to Make Your ED Ready?
23 Building Relationships in Advance Aids Disaster Planning
PAGE 262012 Lantern Award Recipients: Sharing Innovations and Best Practices
PAGE 30Go Global With TNCC and ENPC
PAGE 35Spotlight on the Nominations Committee
PAGE 37Leadership Conference 2013 Advance Program Is Going Digital
ENA Exclusive Content
An Ounce of Prevention LETTER FROM THE PRESIDENT | Gail Lenehan, EdD, MSN, RN, FAEN, FAAN
Emergency Nurses Week™ – Oct. 7-13Emergency Nurses Day® – Oct. 10
The ENA Board of Directors congratulates all emergency nurses. Emergency Nurses: Every Patient + Every Time = Making a Difference
Continued on page 40

October 20124
Why do we do research?
a) Research is all about getting answers.
b) Research is all about getting the ‘‘right’’
answers.
You have set up your study to answer your
question, gone through the Institutional Review
Board and had your abstract (results pending)
accepted to a conference. You start to analyze
all your carefully collected data, waiting for the
answer to your question to reveal itself. And …
you don’t find what you thought you would
find. Or not enough of what you thought you
would find to analyze properly. Or you don’t
find anything that made a difference. Or not
enough of a difference to justify the cost.
Researchers go to a lot of effort to set up
their studies so that they are using the right
method to answer the right question. Well-done
research studies can take a considerable amount
of time to collect data, depending on the
method. However, once the data is analyzed,
it’s important to look at what the data reveals,
regardless of whether that’s the answer the
researcher is ‘‘hoping’’ for.
For example, we recently did a study of what
we thought was the implementation of nurse-
delivered Screening, Brief Intervention and
Referral to Treatment, using a mentoring system
to facilitate practice changes in emergency
departments. We wanted to find out if the use
of regional remote mentors increased the use of
SBIRT in emergency departments. We had more
than 100 sites agree to participate in the study,
but only 55 sites filled out the initial survey.
After a period of encouragement, and data from
about half the regional mentors, we received
follow-up data from only about 22 sites. This
was not enough data from which to draw any
real conclusions.
Was this a useless study? Once we sat and
thought about what had happened, we realized
that far from giving us no information, this
process had provided enormous insight into
factors that might challenge or enhance other
study protocols conducted in emergency
departments. For example, involving people
remotely was not as successful as we had
expected. Only half of the remote mentors were
able to engage their sites in the project. These
challenges to implementation and data
collection suggest that on-site mentoring might
be a better method, and that on-site
infrastructure and support for these kinds of
practice-changing initiatives are prerequisites to
adequate data collection on the effectiveness of
the project.
We found out that it’s easy to get people to
go to one class or view one webinar, but the
more content that we asked them to absorb, the
less ability there was to maintain consistent
participation over time. Lesson learned:
Condense all the information into one session
when possible. Another lesson learned: If
there’s not a big incentive to participate, it’s not
reasonable to ask people to do a lot of work,
especially for a sustained period of time. These
three really important pieces of information will
allow us to plan the next study based on what
worked, what didn’t and where the gaps in
understanding now lie.
Research studies can look really good on
paper. They can be well planned and well
developed. Before you begin to plan your
study, however, it’s useful to look at any
‘‘lessons learned’’ literature to see if other
researchers may have documented challenging
issues with the implementation of a similar
study. All results are useful. Use other
researcher’s findings to make sure you
approach your own research with the best
possible understanding of potential pitfalls.
ENA Connection is published 11 times per year from January to December by: The Emergency Nurses Association
915 Lee Street Des Plaines, IL 60016-6569
and is distributed to members of the association as a direct benefit of membership. Copyright© 2012 by the Emergency Nurses Association. Printed in the U.S.A.Periodicals postage paid at the Des Plaines, IL, Post Office and additional mailing offices.
POSTMASTER: Send address changes to ENA Connection915 Lee StreetDes Plaines, IL 60016-6569ISSN: 1534-2565Fax: 847-460-4002 Web Site: www.ena.orgE-mail: [email protected]
Non-member subscriptions are available for $50 (USA) and $60 (foreign).
Editor in Chief:Amy Carpenter AquinoAssistant Editor, Online Publications:Josh GabyWriter:Kendra Y. MimsEditorial Assistant:Dana O’DonnellBOARD OF DIRECTORSOfficers:President: Gail Lenehan, EdD, MSN, RN,
FAEN, FAANPresident-elect: JoAnn Lazarus, MSN, RN,
CEN
Member Services: 800-900-9659
Secretary/Treasurer: Deena Brecher, MSN, RN, APRN, ACNS-BC, CEN, CPEN
Immediate Past President: AnnMarie Papa, DNP, RN, CEN, NE-BC, FAEN
Directors:Kathleen E. Carlson, MSN, RN, CEN, FAEN Ellen (Ellie) H. Encapera, RN, CEN Mitch Jewett, RN, CEN, CPEN Marylou Killian, DNP, RN, FNP-BC, CENMichael D. Moon, MSN, RN, CNS-CC, CEN,
FAENMatthew F. Powers, MS, BSN, RN, MICP, CENKaren K. Wiley, MSN, RN, CEN
Executive Director: Susan M. Hohenhaus, LP.D., RN, CEN, FAEN
All Results Are Useful
ENA RESEARCH | Lisa Wolf, PhD, RN, CEN, FAEN, Director of the ENA Institute for Emergency Nursing Research
Sidestepping Potential Pitfalls
The Research Column in Connection
has been designed to give succinct,
useful information about the research
process and how research can be
useful to the bedside emergency nurse.
Please send topic suggestions to

@ToshibaMedicalyoutube.com/toshibamedical
THE INFINIX-i: RADIAL
WITHOUT LIMITS.
Toshiba’s Infinix™-i puts the tools for successful transradial intervention
at your fingertips. Combining unsurpassed C-arm positioning with
high-quality imaging, Infinix-i enables left and right side access without
compromise. At Toshiba, we’re making radial access intervention
more efficient than ever – for your patients, your clinical team and
your practice. medical.toshiba.com

October 20126
When a gunman opened fire in a movie theater in Aurora, Colo.,
this past summer, the youngest victim was 6 years old. As emergency
departments in the community sprang into action, each facility
went immediately into disaster response mode. If the same thing
happened in your community, would your facility have the
resources, equipment and staff on hand to care for the child?
IntroductionThe National Pediatric Readiness Project is working to ensure that
emergency departments nationwide know what is necessary to care
for children, and it is building a clearinghouse of resources to help
all facilities become ‘‘pediatric ready.’’
The first step in the project is an assessment. Beginning in
January 2013, emergency departments nationwide will
receive a special online assessment which holds much
promise for improving pediatric emergency care. The
National Pediatric Readiness Project is a multi-phase,
ongoing quality-improvement initiative by the
American Academy of Pediatrics, American College of
Emergency Physicians, Emergency Medical Services
for Children and ENA. It will measure each hospital
emergency department’s readiness to treat children
based on whether it has essential resources identified
by the 2009 Guidelines for the Care of Children in the
Emergency Department Joint Policy Statement.1
Because an ED’s ability to care for children on a
day-to-day basis is linked to its ability to provide care
in the event of a disaster, the National Pediatric
Readiness Project believes that every facility, whether
urban, suburban or rural, should participate.
The goal of this first phase is to survey every
hospital emergency department nationwide that cares for children.
Participating EDs also will receive detailed feedback and have access to
quality-improvement resources, which will help them address any areas
needing improvement. The ultimate goal of the Peds Ready Project is to
ensure that all EDs, regardless of their size and location, are prepared for
pediatric patients.
Assessment Details and BenefitsThe secure, Web-based assessment, which will roll out on a staggered
timeline beginning in January 2013, will serve as the first crucial step of this
project. The state of California served as the pilot for the Peds Ready Project
in 2012, boasting an impressive 90 percent response rate. In 2013, the
assessment will be sent to ED medical and nursing leaders in the remaining
states and U.S. territories; it is advised that the recipients in each facility
collaborate to complete it by printing it before completing it online.
Only one entry per hospital will be permitted. Each participating facility
will receive immediate feedback in the form of a pediatric readiness score
(based on a weighted, 100-point scale). This score will include point
values for the seven sections outlined in the National Guidelines (e.g.,
staffing, QI policies, equipment and supplies). In addition, upon
completion, each participating facility will receive
a gap analysis detailing hospital-specific needs and
recommendations to enhance pediatric readiness.
The assessment will be confidential; no identifying
hospital information will be released. However,
overall results will be available online, thus
allowing participating facilities to benchmark with
other facilities nationwide based on pediatric
patient volume.
ENA’s RoleAs one of the key organizations supporting the
Peds Ready Project, ENA plays a vital role in its
success. ENA is reaching out to its membership
on the national and state levels to help support
the Peds Ready Project by educating themselves,
helping educate others and offering support to
those who will be completing the surveys. Every emergency department,
regardless of size and location, wants to deliver the best possible care to
children. Let’s work together on this national effort to improve pediatric
care by supporting the Peds Ready Project.
The Peds Ready Project represents an unprecedented opportunity to
empower hospitals nationwide, regardless of their size and location, to
provide the best possible care for children seeking their help.
For more information, visit www.pediatricreadiness.org for the
schedule, printable versions of the assessment and supporting resources.
References
1) Joint Policy Statement: Guidelines for Care of Children in the
Emergency Department. American Academy of Pediatrics, Committee on
Pediatric Emergency Medicine, American College of Emergency
Physicians Pediatric Committee and Emergency Nurses Association
Pediatric Committee. Pediatrics 2009;124;1233; originally published
online September 21, 2009.
2) National Pediatric Readiness Project website:
www.pediatricreadiness.org.
PEDIATRIC UPDATE | Elizabeth Stone Griffin, BS, RN, CPEN
A National Assessment of ED Pediatric Readiness

© 2012 Össur
SPINAL SOLUTIONS BY ÖSSURProven patient protection, now with adjustability.
MIAMI J®
ADVANCEDPHILADELPHIA®
ADJUSTABLE
MIAMI J ADVANCED:- Based on the original Miami J phenotyping system- Covers 85% of all patient sizes- Single Sorbatex pads (1 front, 1 back) for easy and effective skin care- Flex-edge technology for maximum patient comfort- NEW anti-tampering locks for improved patient safety
PHILLY ADJUSTABLE:- From the original Philly Trache Collar company- Covers 95% of all patient sizes- Proven Plastazote® interface ensures skin-friendly protection- Height adjustable front and circumference for maximum patient comfort
FOLLOW ÖSSUR ON Learn more about Össur spinal solutions today!USA 800 233 6263 CANADA 800 663 5982 WWW.OSSUR.COM
MIAMI J®
ADVAAANCNCNCEEDEDDPHILADELPHIA®
AAAADJDJDJJUSUSUSTATAT BLE

October 20128
By Kendra Y. Mims, ENA Connection
ENA Launches the ENPC Revision Course ENA is excited to announce that the highly anticipated Emergency Nursing
Pediatric Course 4th edition is now available for participants. The ENPC
Revision Work Team Committee and ENA staff members started the
revision process two years ago. The instructor rollout of the ENPC 4th
edition was launched Aug. 27, and Sept. 1 marked the first day that course
directors could hold 4th edition classes. This is the course’s first revision
since 2004.
ENPC 4th edition provides emergency department personnel with the
knowledge and tools needed to prepare for pediatric patients, following
the Guidelines for Care of Children in the Emergency Department created
by the Emergency Nurses Association, the American Academy of Pediatrics
and the American College of Emergency Physicians. The ENPC 4th edition
is taught using online learning, lectures, videos, group discussion and
hands-on skill stations (i.e., management of the ill or injured pediatric
patient and the pediatric clinical considerations) to encourage participants
to integrate their psychomotor abilities into a patient situation in
a risk-free setting.
What’s New in the 4th Edition Participants will be excited to know that three new chapters have been
added to the 4th edition: environmental emergencies, disaster and
adolescent. The environmental lecture will look at bites and venomation,
and the disaster lecture will use case studies to identify the risks associated
with the pediatric population. The adolescent chapter is an exciting
highlight for emergency nurses, said Nancy Denke, MSN, ACNP, CEN,
FAEN, chairperson for the ENPC Revision Work Team.
‘‘In the adolescent chapter, we talk about the challenges in treating
adolescent patients and the common problems you’ll see with taking care
of the adolescent child,’’ Denke said. ‘‘I think the adolescent chapter has
been one of those chapters that has been lacking. We really need the
information to care for those children better than we have been and make
emergency personnel better at preparing to care for adolescent patients in
the emergency department, whether they work in a rural, urban or
pediatric center.’’
ENA’s Nursing Education Editor, Marlene Bokholdt, MS, RN, CPEN,
CCRN, agrees that the new adolescent chapter is one of the most
significant highlights of the revision.
‘‘I think that a lot of people think of pediatrics as little kids,’’ Bokholdt
said. ‘‘It really isn’t. It is birth to adulthood, and that adolescent population
has kind of gotten lost in the shuffle. It wasn’t part of the previous edition,
so we’re very excited that it’s in the fourth edition and it does have some
excellent information and real concrete tips and information that will help
anyone take care of this population.’’
There are four lectures (pain, environmental emergencies, toxicological
emergencies and stabilization and transport) that are presented in a
webinar format, which the learner is expected to watch and complete
before coming to the live class. Participants will be awarded CEs for these
lectures after watching and completing them online, and they will also
receive separate CEs for their attendance in the live course.
Other notable changes include the behavioral emergencies chapter
(previously psychiatric emergencies), which focuses on accessing children
with behavioral health issues and also includes a section on autism; the
special-needs child section is now integrated with all of the lectures, as
opposed to being a separate lecture, as in the previous editions; and
triage, which was previously part of the ill and injured skill station, is now
an interactive lecture that will include case scenarios and group discussion
of triage. The Jeopardy® game has been eliminated from this edition and
replaced with clinical considerations/vignettes — a brief interactive
overview in which the students will look at rapid-sequence intubation,
airway management, vascular access and more.
One major change that occurred from the revision process is that the
ENPC 4th edition will not offer a reverification course. Due to ANCC
guidelines, ENA is not able to offer contact hours for reverification courses
after Dec. 31. The ENA Board of Directors voted in July 2012 to
discontinue TNCC and ENPC reverification courses after that date.
Therefore, there can be no 3rd edition ENPC reverification courses or 6th
edition TNCC reverification courses held after Dec. 31.
ENA is exploring new ways to provide ongoing continuing education
related to the courses and has directed that no more than four years will
lapse between each new version of the TNCC and ENPC courses.
Participants will be able to continue to challenge the two-day provider
courses, as allowed by each individual course director.
For more information about the exciting ENPC 4th Edition, please visit
www.ena.org/coursesandeducation/ENPC-TNCC/enpc/Pages/
aboutcourse.aspx.
Course HighlightsHighlights of ENPC include:
• Completing an observational or across-the-room assessment
• Identifying subtle changes that indicate deterioration
• Developmental approach to pediatric care
• Cultural considerations in pediatric care
• Pain assessment and management for children
• Techniques for family-centered care
Names of all involved in the revision process:
Nancy Denke, MSN, RN, FNP-C, ACNP-BC, FAEN, Chair
Paul C. Boackle, BSN, RN, CCRN, CEN, CFRN, CPEN, CTRN
Angela M. Bowen, BSN, RN, CPEN, NREMT-P
Cam Brandt, MS, RN, CEN, CPEN, CPN Julie L. Miller, RN, CENDianne Molsberry, MA, RN
ENA Board LiaisonsDeena Brecher, MSN, RN, APRN, CEN, CPEN
Tiffany Strever, BSN, RN, CEN
ENA StaffBetty Mortensen, MS, BSN, RN, FACHEMarlene Bokholdt, MS, RN, CPEN, CCRNRenee Herrmann, MA
Curriculum ConsultantVicki C. Patrick, MS, RN, ACNP-BC, CEN, FAEN

KARL STORZ Endoscopy-America, Inc., 2151 E. Grand Ave, El Segundo, CA 90245, USA, Phone: (424) 218-8100, Fax: (800) 321-1304, E-Mail: [email protected] STORZ GmbH & Co. KG, Mittelstraße 8, D-78532 Tuttlingen/Germany, Phone: + 49 7461 / 70 80, Fax: 07461 / 70 81 05, E-Mail: [email protected] STORZ Endoscopy Canada, Ltd., 2345 Argentia Road, Suite 100, Mississauga, Ontario, Canada L5N 8K4, Phone: (800) 268-4880, Fax: (905) 858-0933KARL STORZ Endoscopia, Latino-America, 815 NW 57 Ave, Suite #480, Miami, Florida 33126-2042, USA, Telefono: (305) 262-8980, Telefax: (305) 262-8986
www.karlstorz.comA-0112002 © 2012 KARL STORZ Endoscopy-America, Inc.
C-MAC® –Make your Video Laryngoscope a SYSTEM! A Single Instrument is not Airway Management

October 201210
Disaster Preparedness
Are You Ready for the Real Thing?
Terrorist attacks in the United States, including the Oklahoma City
Bombing on April 19, 1995, and the 9/11 attacks, have caused a renewed
sense of urgency in disaster-preparedness training for emergency
departments across the country. In response to these acts of terrorism, the
Department of Homeland Security developed resources to help health
care providers prepare for disasters, including giving millions of dollars in
grants to health care organizations. However, these grants required that
any disaster exercises resulting from the grant funds must focus on
terrorism threats (U.S. Department of Homeland Security Office for
Domestic Preparedness, 2003). This resulted in a large number of
healthcare organizations focusing on biological or chemical threats, using
the grant funding to assist in the purchase of decontamination equipment.
While these real potential threats deserve our consideration, what does
the actual data say about disasters that have occurred in the United States?
There have been 281 disasters in the United States since 2000 (EM-DAT,
2012) and 16 terrorist-type attacks in the United States from 2002 to 2010
(Kimery, 2011). Clearly the more prominent problem is disasters that do
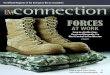
not involve acts of terrorism. Table 1 highlights the number of fatalities
and injured associated with some of the disasters that occurred since 2005.
To further complicate this issue, the Institute of Medicine (2006) found
that most emergency departments were inadequately prepared for a major
disaster. This is despite the fact that numerous regulatory agencies
mandate that hospitals provide disaster training to their employees.
Goodhue, Burke, Channbers, Ferrer, and Upperman (2010) reported that
emergency-preparedness plans tested by hospitals vary in quality since
the implementation methods range anywhere from tabletop exercises to
full-scale disaster scenarios. Numerous researchers have found that the
focus of these methods typically is on the overall management and
coordination of a disaster rather than the clinician’s role in patient care
and triage (Kaplan, Connor, Ferranti, Holmes, & Spencer, 2012).
Even with full-scale disaster scenarios, hospital personnel often do not
treat the volunteer patients with the same level of attention that would be
required in a real disaster. It is not uncommon to hear comments such as,
‘‘I have real patients to take care of,’’ or, “This is a waste of time because
it is not realistic.’’ Both of these statements have some merit. Yes, staff do
have patients that are already in the emergency department that require
attention, and yes, the scenarios are artificial when using live patients
because the staff cannot insert intravenous lines, obtain blood specimens
and perform other invasive procedures that would be required in a real
disaster. Unfortunately, this prevents fully identifying the challenges that
would arise in a real disaster when surge capacity is reached. So what can
you do about this?
Using unconventional approaches to disaster-preparedness training that
have evolved from modalities used by the military and institutions of
higher education may be the answer. Preparation is essential before
implementing the actual disaster-preparedness scenario. This requires that
staff are informed about the expectations that will be required from them
during the exercise, as well as familiarizing them with the disaster
preparedness plan. It should be stressed that staff should consider
simulated patients as ‘‘real’’ patients as much as possible, even when the
emergency department is busy. This may require that coaches be
strategically placed throughout the department to help staff meet the
needs of the actual patients in the department, as well as meet the
expectations for the disaster exercise. Remember, the goal is to tax the
system to identify problems that may need to be addressed
in the event of a ‘‘real’’ disaster. Implementation of the
disaster exercise is greatly enhanced if simulators are used
in conjunction with live patients.
This type of disaster-preparedness exercise requires
creativity in the planning process. In addition to some of
the issues already identified, planners need to remember
that in a real disaster, supplies and personnel may be
scarce, electricity and water may not be easily accessible,
and disposing of human waste may not be through
traditional venues. Furthermore, 75-85 percent of your
patient volume during a disaster will be self-referred and
not arrive by EMS (American College of Physicians, 2009).
Just because we have always done it this way does not
Date Disaster Location Fatalities Injured
July 20, 2012 Movie Theater Shooting
Aurora, Colo. 12 58
May 22, 2011 Tornado Joplin, Mo. 158 1,000
Sept. 23, 2008 Train Collision in Chatsworth area
Los Angeles 25 135
Oct. 21, 2007 Wildfire Potrero, Calif. 5 55
Aug. 29, 2005 Hurricane Gulf Coast 1,836 Unknown
Table 1: Number of fatalities and injured associated with selected disasters in the US since 2005
Considerations for Disaster Preparedness Exercises
By Michael D. Moon, MSN, RN, CNS-CC, CEN, FAEN, ENA Board of Directors
Board Writes

Official Magazine of the Emergency Nurses Association 11
Disaster Preparedness Disaster Preparedness
Are You Ready for the Real Thing?
The Emergency Nurses Association is proud to present the release of the 4th edition of the Emergency Nursing Pediatric Course.It has been revised and updated, evidence-based, and continues to incorporate various teaching and learning styles.
• A portion of the course will be presented in an online format through ENA’s Center for e-Learning.
• Pediatric Clinical Considerations is nowcase-based using group discussion.
• The adolescent patient is addressed witha separate chapter and lecture.
• Triage is now Prioritization with a focus on the process, rather than the place.
Upon successful completion of ENPC, RN participants are veri� ed for four years, receive a veri� cation card and earn up to 16 contact hours.
This course brings the emergency nurse a resource for treating the pediatric patients arriving to emergency departments every day.
To verify why ENPC is right for you and toview course schedules, please visit
www.ena.org/coursesandeducation
The Emergency Nurses Association is
accredited as a provider of continuing nursing
education by the American Nurses Credentialing
Center’s Commission on Accreditation.
mean that we should continue with the same process.
That just lends itself to obtaining the same outcomes.
Without practice that involves nontraditional
approaches in managing scarce resources, including
personnel, your facility may be unable to maintain
sustained operations for extended periods during
surge capacity (Goodhue et al., 2010). Successful
disaster preparedness training involves creative
thinking in the planning, development,
implementation and evaluation of realistic disaster
scenarios that represent the full continuum of
possibilities. Do not be afraid to step out of the box
and your comfort zone. You will be glad you did in
the event of a ‘‘real’’ disaster.
References
American College of Emergency Physicians (2009).
ACEP best practices for hospital preparedness.
Retrieved August 5, 2012 from www.acep.org/
clinical---practice-management/best-practices-
for-hospital-disaster-preparedness
EM-DAT (2012). Natural disasters in the United States
from 2000-2011. Retrieved August 5, 2012 from
www.emdat.be
Goodhue, C.J., Burke, R.V., Channbers, S., Ferrer,
R.R., & Upperman, J.S. (2010). Disaster Olympix:
A unique nursing emergency preparedness exercise.
Journal of Trauma Nursing, 17(1), 5-10.
Institute of Medicine (2006). The future of emergency
care: Key finding and recommendations.
Washington, DC: Author.
Kaplan, B.G., Connor, A., Ferranti, E.P., Holmes, L., &
Spencer, L. (2012). Use of an emergency
preparedness disaster simulation with undergraduate
nursing students. Public Health Nursing, 29(1),
44-51.
Kimery, A. (2011). Frequency of attacks in US
dropped steadily after 9/11: Increased globally since
2004. Homeland Security Today US. Retrieved
August 5, 2012 at www.hstoday.us
U.S. Department of Homeland Security Office for
Domestic Preparedness (2003). Homeland security
exercise and evaluation program, volume I:
Overview and doctrine. Washington, D.C.: Author
Feed
bac
k Fr
ame
Call for NominationsEmergency Nurses Association/Blue Jay
Consulting Award for Outstanding Emergency
Department Nurse Leader of the Year
To view additional information and submit
a nomination for this award visit www.ena.org
and click on the About tab, then Awards.
Deadline for Nominations is Monday, Nov. 12, 2012

October 201212
Disaster Preparedness
Communication
failures are often at
the top of the list of
challenges following a
hospital disaster drill
of real event. Effective
communication, along
with teamwork, is
essential for the delivery of high-quality care,
patient safety and seamless transfer of patients
during the chaos of a disaster.
In September 2008, Hurricane Ike was
predicted to hit the southern portion of the
Florida Keys as a Category 4 hurricane, with
maximum sustained winds of 145 mph (230
km/h). This prediction activated the evacuation
plan of the Lower Keys of Florida, including
Lower Keys Medical Center, the only hospital in
the lower southern chain of the Florida Keys,
roughly 162 miles from Miami.
The logistics of transportation methods, patient
preparation and family notification, receiving
hospitals and fiscal outcomes was the beginning
of a 24/7 assessment and evaluation process on
how to best care for the patients that needed
continued inpatient medical care at a hospital out
of harm’s way.
One key lesson learned from this evacuation
was that a method was needed to communicate
patient information without having to spend days
printing out the complete medical records of a
large number of patients.
As patients move among specialized services
within a hospital, and as shifts of medical
personnel come and go, there are numerous
episodes in which responsibility for the patient
passes from one health professional to another
and where patient information is exchanged.
During a disaster, this normal exchange of
communication is disrupted. As patients are
evacuated to another hospital or facility,
communication of patient information becomes
a challenge. The use of electronic medical
records poses unique situations in both clinical
information sharing and fiscal data validation.
During the evacuation and receipt of patients
from the Florida Keys, the decision was made to
initially print and send with the patient the
medical administration record, a face sheet with
patient demographics and financial information,
and the last 48 hours of progress notes. These
records were placed in a sealable plastic bag,
labeled with the patient’s name and sent with
the patient. Following an after-action-review of
the evacuation event, the nurses receiving the
evacuated patients stated that they had more
questions than answers regarding the patient’s
plan of care and clinical situation.
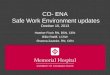
A solution to this challenge was the revision
and use of the SBAR or Patient Transfer
Summary reporting form. SBAR stands for
Situation, Background, Assessment and
Recommendation (see image below).
The SBAR is a familiar communication and
hand-off reporting tool to many nurses and
allied health professionals. Reports show that
simple, familiar tools will be more readily used
during disasters and with fewer errors. The
SBAR is used in most hospitals in south Florida,
so it was a natural choice for the exchange of
timely, accurate patient information in a way
that is familiar to all members of the health
care team.
The Use of the SBAR to Facilitate Patient Communication During a Disaster
By Sharon Saunderson Coffey, MSN, RN, CEN, CHEP, Emergency Management and Preparedness Committee
SBARRegion VII Health/MedicalPatient Transfer Summary
Patient Name Gender r M r F Age
Transferring Hospital Transferring Hospital’s Pt’s MR#
Transfer Reason:
Transfer Date: Time:
Code Status: r Full r Do Not Attempt Resuscitation (r Documents attached) r Do Not Intubate (r Documents attached)Isolation: r Airborne r Droplet r Contact Organism
Allergies (medication, latex, environmental, other):Allergy bracelet on? r Yes r No
Current Diagnosis(es)
Brief Summary Hospital Stay
P-12148 - 119970 - 8/2009
Current Vital Signs: Time:________ Temp: ________ Pulse Rate:_______ Resp Rate:_______ Blood Pressure:_______ Pulse Ox:_______
Cardiac Rhythm FiO2
Vent Settings Bipap / CPAP settingsCurrent IV’s 1 2 3 4LocationDate of insertionFluid Infusing
Current Medications r MAR Attached
Pain Score at Transfer Time + Route of Last Pain Med Given Med given(Use 0-10 Pain Scale)Current Drains 1 2 3 4
LocationDate of Insertion Pertainent Behav. Health Assessment / Issues
Valuables r Yes r No Clothing r Yes r No Dentures r Yes r NoGlasses r Yes r No Hearing Aids r Yes r No Personal DME r Yes r No List on back /Narrative
Report given to: Phone #: Time:Attending Physician notified of transfer r Yes r No Who _______________________ Phone ____________ Time _______Family notified of transfer? r Yes r No r N/A Who was notified? Complete Medical Record Transferred r Yes r NoSpecial considerations/recommendations:
Transferring Nurse/PhysicianSignature: Print: Date: Time:
Receiving Nurse/PhysicianSignature: Print: Date: Time:
Situation
Background
Assessm
entR
ecomm
endations
(See reverse side for additional information)
SBAR
Patient Hand-Off Reporting Form

Disaster Preparedness Earn Your Mark of DistinctionHighlight your professional accomplishments
Distinguish yourself in the workplace
Make a commitment to prepare for a Board of Certification for Emergency Nursing certification and take the next step in your career.
www.BCENcertifications.org
Set yourself and your health care facility apart — get certified today!
“RNs with a BCEN credential are the best of the best!”

October 201214
Disaster Preparedness
Disaster Nursing Education
After returning home from my last disaster
response in September 2011, I decided to review
articles and take a look at some of the
educational objectives of disaster education.
We are all well aware of the American
Association of Colleges of Nursing’s new
requirements to include disaster education in the
nursing curriculum. However, many schools are
not sure how they should accomplish this and/
or how they can meet requirements in an
already bulging nursing curriculum.
The International Nursing Coalition for Mass
Casualty Education created educational
competencies in regard to nurses responding to
mass casualty incidents. The coalition included
accrediting bodies and nurses from different
sectors (i.e., public – governmental and military;
private, academic) and different specialties.
However, the coalition was discontinued due to
the lack of funding, and each university and
group went about interpreting and setting its
own standards for its curriculum. We need to
continue the goal of getting us all on the same
sheet of music.
There are no exact disaster nursing
competencies for nurses. In other words, the
main problem is that all of us think we have the
answer, and no one is taking a stand. Because
of the varied types of nursing educational
programs throughout the United States, and the
different state and federal mandates for nursing,
there is not a clear picture. The goal is to get
everyone ready for a disaster response as a
single entity working toward one goal — the
ability to work as a team in a disaster.
We have an overwhelming amount of interest
in the area. However, what we don’t have is a
consensus of what the educational requirements
are. During this review, it was found that
faculties lack knowledge on disaster response
planning, in which case many students are not
getting the disaster education and those who are
receive only four to five hours (Schmidt et al.,
2011).
In reviewing schools in the tri-state area, we
have found that most students are getting about
two to four hours of disaster education. It is
usually in a lecture format, with little to no
interaction. At Binghamton University, we have
a nursing program that is averaging 12 hours of
disaster education, including lecture material,
online course work through the Federal
Emergency Management Agency, covering
Incident Command System and National Incident
Management System.
Many schools are trying to change the
curriculum but are unsure how. There is a need
for selected core competencies for every student
nurse and nurse in practice. So many regulations
have been placed on today’s educators and
nurses that many nurses feel they are overtasked
with a burdensome workload. In the case of
disaster preparedness, we need to get it right.
We are headed toward catastrophic problems,
as our globe is starting to realize. We have
nurses who need the background and basic
disaster education to be a part of the disaster
response. Plans for disaster nursing education
must not be placed on a shelf and forgotten
after they leave school or take their
examinations.
Many educators have suggested that each
school could mandate a disaster education
course and then allow the student or nurse to
learn in the field.
In an article by Tillman (2010), she discusses
the need for nurses to be a major responder and
be part of a team response. The American
Nurses Association validated the preparation in
its policy ‘‘Standards of Care under Extreme
Condition: Guidance for Professionals during
Disasters, Pandemics and Other Extreme
Emergencies’’ (ANA, 2008). Tillman (2010) also
includes major competencies of triage, a
personal emergency plan, psychological
considerations and ethical considerations.
In another article of interest, Schmidt (2007)
describes a wonderful program and experiment
taking place with the work of the American Red
Cross and 12 universities across the United
States. The students are being asked to take a
course entitled ‘‘Sheltering and Disaster Health
for Nursing Students.’’ This program is only four
hours long, and although it may be helpful to
the Red Cross’ needs to assist in supporting
sheltered patients, we may not really be
We Must Be Working, Learning as OneBy Laura Terriquez-Kasey, MSN, RN, CEN, and Tak Man Yan, BSN, RN
Flight nurses and medics assist members of a disaster medical assistance team as part of the response effort following Hurricane Ike in 2008.
Joce
lyn
Au
gust
ino/
FEM
A

Official Magazine of the Emergency Nurses Association 15
Disaster Preparedness Disaster Preparedness
preparing future RNs, LPNs and students for the
injury and triage concerns related to a large-scale
disaster.
After reviewing the document by Association
of Community Health Nursing Educators (2009)
in the “Essentials of Baccalaureate Nursing
Education for Entry-Level Community/Public
Health Nursing,” the recommendations seem
perfectly appropriate. It contains much of the
required material, including the legal and ethical
concern while providing disaster nursing care. It
needs to expands its view and include the
Disaster Preparedness Cycle and Paradigm as
described and taught in the AMA course on Basic
Disaster Life Support and the Advanced Disaster
Life Support. After taking the BDLS and ADLS, it
is apparent to me that the disaster paradigm
taught in the program should be adopted as part
of the nursing curriculum.
The other items we should include are the
need for careful, deliberate triage during a mass
casualty situation and the categories of care. There
needs to be an increased level of competency
required for the basics of chemical, biological,
radiological, nuclear and explosion. We need to
include discussions and tabletop drills with
discussion of surge capacity issues and the use of
partnerships with local communities.
We need to mandate the use of FEMA’s
Emergency Management Institute courses. Each
public health department needs to be included
in the essential partnerships. Nurses, as well as
all members of the healthcare teams, need to be
more knowledgeable about their responsibilities.
Recent experiences after Katrina in 2005 and
in upstate New York after the flooding in 2006
and 2011 have left each of us with a desire to
include essential education to the new nurses
coming into the arena of health care. It should
be obvious that we are still unprepared for
disaster work after seeing the lack of
preparedness in some of our excellent schools.
Many schools have good intentions but lack the
expertise in their faculty to provide the education
required. Faculty need to be knowledgeable in
order to assist students in improving their
knowledgebase.
These steps, along with the AACN’s new
recommendations for the nursing curriculum, are
essential to providing the nurses with critical
thinking abilities during an actual event. It is an
important idea that we continue disaster
education. A question that still remains is: How
do we educate the other nurses who have
already been in the workforce and are unaware
of the changing factors or requirements in
disaster preparedness?
References
Dallas, C.E., Coule, P., James, J.J., Lillibridge, S.,
Pepe, P.E., Schwartz, R.B., et al (Eds) (2007).
Basic Disaster Life Support. United States of
America: American Medical Association.
Schmidt, C.K., Davis, J.M., Sanders, J.L.,
Chapman, L.A., Cisco, M.C., Hady, A.R., (2011).
EXPLORING nursing students’ level of
preparedness for disaster response. Nursing
Education Perspectives, 32(6), 380-383.
Schmidt, C.K. (2007). Strategies to Prepare
Nursing Students to Respond to Disasters.
Dean’s Note, 28(3). Retrieved on 7 August 2012
from www.ajj.com/services/publishing/
deansnotes/jan07.pdf
Association of Community Health Nursing
Educators. (2009). Essentials of Baccalaureate
Nursing Education for Entry-Level Community/
Public Health Nursing. Retrieved 5 August 2012
from achne.org/files/
EssentialsOfBaccalaureate_Fall_2009.pdf
Tillman, P. (2010). Disaster preparedness for
nurses: A teaching guide. (2011). Journal of
Continuing Education in Nursing, 42(9),
404-408.
Bibliography
American Nurses Association. (2008). Adapting
Standards of Care Under Extreme Conditions:
Guidance for Professionals During Disaster,
Pandemics and Other Extreme Emergencies.
Retrieved 5 August 2012 from nursingworld.
org/MainMenuCategories/WorkplaceSafety/
DPR/TheLawEthicsofDisasterResponse/
AdaptingStandardsofCare.pdf
Mexican Association of Emergency Nurses
College of Emergency Nursing Australasia Ltd.
Australian College of Emergency Nursing (ACEN)
College of Emergency Nurses - New Zealand
National Emergency Nurses’ Affiliation, Inc. (NENA)
Royal College of Nursing
AFFILIATES:
EMERGENCY NURSES:
Every Patient + Every Time = Making a Difference.
www.ena.org/enweek
Emergency Nurses Week™
October 7-13, 2012
Emergency Nurses Day®
Wednesday, October 10, 2012
12462_EN Week 1-2 pg island ad_FInal.indd 1 7/9/12 9:57 AM

October 201216
Disaster Preparedness
Measuring the Effectiveness of a Communitywide Disaster Drill
Consistently seeing and evaluating the different
pieces is part of an effective disaster drill. We
all hope we don’t need the disaster response.
However, more often than not, we are seeing
the terrible effects of not preparing
appropriately for a disaster.
Teamwork and effectively preparing the
different parts of the teams is critical to a good
unified response. What matters is that your
teams work together and that they can work in
a flexible mode. Many of us have had the
rudimentary essential lectures in class and in
the field, but until we experience the actual
event or participate in a realistic drill, we are no
match for the real response necessary when the
disaster strikes us. The ‘‘lessons learned’’
portion and debriefing or ‘‘hot wash’’ are the
key components to the proper evaluation
process of a disaster drill.
In many cases, the leadership potential and
the ability to compromise and critically think
are noted to display, at times, a striking
acuteness to the effect of the education and
training received.
Drill preparation is also critical for an
effective response. Each team must display
good leadership skills and the ability to work
well with others. Everybody needs to get out of
their bubble and work as a team with the ability
to provide continuum of care — triage and
re-triage and effectively treat and respond to
clients’ ongoing needs. Another essential piece
of all of this is the preparation of the groups
before the drill. Planning and placing obstacles
in the way of the providers is critical in order to
test the effectiveness of each group.
Before you start the planning portion of the
drill, all of the essential needs for the drill
should be identified. Designing an effective drill
must include the leaders and community
representatives. Allowing each group to
effectively educate its own group is all part of
the process in preparing for the real disaster.
When the disaster drill is designed, it must be
clear what the objectives of the drill are for
everyone. We also must take the time to
provide the methods and tools we will use in
clearly measuring the response.
The Methods of Measurement must be clear
to each responder and reflect back to the
essentials taught to all responders. Set some
clear learning objectives for the drill.
1. Try to use the Disaster Paradigm (AMA
2007) to assist all responders in learning the
basic concepts. Consider sending faculty
and emergency staff to assist all in the
expansion of knowledge across the health
continuum.
2. Triage procedures, classification of clients
into categories to allow us to respond
rapidly and effectively.
3. Consider educating all in Mental Health First
Aid procedures before a disaster.
4. Prepare all responders with knowledge of
the equipment that will be used.
5. What are the basic emergent skills required
by all staff at their level of education?
6. Carefully clarify roles and responsibilities for
all responders.
7. Test each portion of the responders’
learning process.
8. Review of the policy and procedures: Are
they clearly identified for the team?
9. The actual planning of a drill must reflect
back to the community.
10 Perform a hazard assessment.
11. Consider all awareness-level training to be
reviewed for basic issues related to CBRNE.
Example: Review the idea of (RAIN)
Recognize Avoidance, Isolation, and
Notification.
‘‘Remember each worker responding to an
event can also become a casualty if not taught
to prevent the possibility of being exposed’’
(Ryan, and Glarum 2008). If you live next to a
chemical factory, then perhaps that should be a
thought when you consider planning the drill. If
your disaster drill committee feels the need to
practice responding to a hazardous material
situation, then it should consider the possible
hazards in the community. If there is a large
airport and or train station, then perhaps
considering an airplane crash or a train accident
is appropriate.
12. Review command and control and ICS
roles for everyone.
This is important to make sure each
community prepares itself for the possible
natural disasters and terrorism in its own
community. Most communities should start with
a single event related to a disaster drill. Then all
can focus on the major problems at hand.
By Laura Terriquez-Kasey, MSN, RN, CEN, Emergency Management and Preparedness Committee
Emergency responders test their preparedness in a community mock disaster drill.
Den
nis
Sa
bo/S
hu
tter
stoc
k.co
m

Official Magazine of the Emergency Nurses Association 17
Disaster Preparedness Disaster Preparedness
Creating a disaster drill planning team that
includes a member from all parties is critical to
the success of the drill. Make sure you involve
citizens and clients as volunteers. Look around
for volunteers from the community, as they may
have an interest, and it does raise awareness in
the community by having multiple groups
participating.
Consider setting up a clear exercise guideline.
Use a scenario summary or timeline to assist all
the players. Brief each group alone so that all the
groups know what is required of them.
Consider setting up specific evaluation
packets for each evaluation team. Make sure you
have clear, delineated evaluation questions and
guidelines. Review the materials.
This makes the drill more realistic. Example:
Try to have EMS use actual treatment tags for the
triage and role playing.
We need volunteers to play the roles of the
injured. Try to use seniors and children as well
as students and community workers in this role.
It will be important to brief each in their role and
the changes that they must perform if possible.
Use small index cards as coaching cards for the
players. Using simulation mannequins is critical
to the learning process if you cannot perform a
large drill. If possible, have a moulaged team
work with the players ahead of the actual drill.
This may allow each player to look more realistic
and also allow the player time to learn their role.
In some cases it’s necessary to have team
evaluators at different sites throughout the drill.
You may need a team of evaluators at triage, a
team evaluating the EMS portion of a drill,
another team at each nursing care area and
finally a team that evaluates and coaches the
command staff team. Each evaluation team
should have a specific marking on them and be
clearly given yes and no questions/answers.
Consider leaving areas open for judgment and
feedback. Consider allowing each evaluation
team 30 minutes to prepare their return
information for the hot wash of the drill.
After the drill, each team should be asked to
submit an after-action report to the disaster
planning committee to discuss the drill and
review the learning process and be allowed to
make recommendations to the disaster
committee for the next drill.
References
Dallad, C.E., Coule, P., James, J.J., Lillibridge,S.,
Pepe, P.E., Schartz, R.B., et al. (2007). Basic
Disaster Life Support. United States of
America: American Medical Association.
Glarum, J.R. (2008). BioSecurity and
BioTerrorism Containing and Preventing
Biological Threats. In Bio Security and
BioTerrorism Containing and Preventing
Biological Threats (p. 122). Burlington MA.:
Eleseiver.
Tools for Evaluating Core Elements of Hosptials
Disaster Drills. Retrieved Aug. 5, 2012, from
AHRQpublication 08-0019: www.ahrq.
gov/prep/drillelements/
Bibliography
Coping with a Disaster or Traumatic Event.
(2012, Aug 5). Retrieved Aug. 5, 2012, from
CDCMental Health/Trauma and Diaster Event.:
http://emergency.cdc.gov/mentalhealth/
Tools for Hospitals Health Care Systems. (2012,
Aug. 5). Retrieved 2012 from www.AHRQ.
gov: www/ahrq.gov/research/hospdrills.
htm, Johns Hopkins University Evidence
Based Practice Center Baltimore, Maryland
(2008).
Series Public Health Emergency Preparedness
Research Resources and Tools “Hospital
Assessment and Recovery Guide,” AHRQ,
HHS, Prepared by Abt Associates Inc.,
Cambridge MA. May 2010.
Series Public Health Emergency Preparedness
Research Resources and Tools “Hospital
Evacuation Decision Guide,” Prepared for
AHRQ, HHS, Prepared by AbT. Associates Inc.
Cambridge, MA.
.
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O R T L A U D E R DA L E , F L F E B R U A R Y 2 7 – M A R C H 3
E N A L E A D E R S H I P C O N F E R E N C E 2 0 1 3
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
Offering Educational and Networking Opportunities for Current and Future Emergency Nurse Leaders.
E N A L E A D E R S H I P C O N F E R E N C E 2 0 13
F O RT L A U D E R DA L E , F L F E B R U A RY 2 7 – M A R C H 3
For more information, scan QR code, or visit
www.ena.org/lc

October 201218
Disaster Preparedness
Weather-related natural disasters, such as
hurricanes, are omnipresent, and their effect
on human lives and property damage is
inevitable. Advances in technology and
meteorology enable public health officials, health care planners and other
organizations to develop advanced warning systems, activate coastal
shelter plan operations and hurricane preparedness in order to decrease
mortality and morbidity.
Hurricane CategoriesA hurricane watch is issued for a coastal area when there is a threat of
hurricane conditions within 36 hours, and a hurricane warning is issued
when conditions are expected in 24 hours or less. The Regional
Specialized Meteorological Centers (U.S. National Hurricane Center,
U.S. Central Pacific Hurricane Center, Japan Meteorological Agency, India
Meteorological Department, Meteo France and Australia & New Zealand
Meteorological Service), Canada Hurricane Center, Philippine Atmospheric
Geophysical and Astronomical Services Administration are responsible for
tracking, naming tropical cyclones and issuing warnings and advisories
to protect life and property.
Hurricanes are categorized according to wind strength using the
Saffir-Simpson Hurricane Wind Scale:
Hurricane ImpactThe American Society of Civil Engineers made a study of the property
damage caused by hurricanes from 1900 to 2005 and placed the Great
Miami Hurricane of 1926 on the top with $140-157 billion in damages
(adjusted for inflation in 2005), and Hurricane Katrina as the second most
destructive storm in U.S. history at a cost of $81 billion in damages.
Although Category 4 or 5 hurricanes can cause serious damage, Category
1 or 2 hurricanes can be as costly and devastating. A Category 3 hurricane,
Hurricane Katrina cost the lives of 1,836 people.
Coastal Storm Plan Sheltering System The hurricane sheltering plan provides an orderly method of evacuating
people living in low-lying areas and moving them into hurricane shelters.
Solar systems are set up with associated hurricane shelters. As the center
of the solar system, the evacuation center serves as the entry point into
the solar system and its respective hurricane shelters. The evacuation
center is the place where all staff report and obtain task assignments and
just-in-time training. The evacuation center serves as the location for the
following activities during an event:
• Central screening for identifying and addressing evacuees with health
and medical, pet and family reunification issues
• Supply requests
• Troubleshooting
• Dispatching training staff and evacuees to a hurricane shelter
• Managing census of the mini-shelter system
• Arranging for the release of evacuees at the closure of the hurricane
shelters
• Reports to the city’s emergency operation center.
On Aug. 25, 2011, with Hurricane Irene threatening a full-force hit, the
governors of New York, New Jersey and Connecticut declared a state of
emergency. New York City was ready with ‘‘evacuation contingencies’’ for
low-lying areas that are home to 250,000 people and made plans to shut
down the transit system. The New York City Office of Emergency
Management ordered nursing homes and hospitals located within the
evacuation zone to evacuate residents and decrease their caseloads.
The Baruch College Evacuation Center was one of the New York City
evacuation centers that demonstrated a well-organized evacuation
operation. The evacuation center was run by staff from the New York City
Housing Authority, a teacher (Angela Becham), New York City Medical
Reserve Corps volunteers (Dr. Eugenia Siegler, Leslie Lieth, PNP, and
Angeli Medina, RN), mental health staff, social workers, Community
Emergency Response Team volunteers and a nurse volunteer from
Sweden. When the worst was over, the mayor lifted the evacuation order
and the 9,000 people who stayed in the hurricane shelters and the 370,000
evacuees were able to return. The New York City coastal storm sheltering
operation worked well during Hurricane Irene; there were no reported
deaths or serious injuries during the hurricane watch.
What to Do Before and During the StormA. Prepare a family disaster plan that outlines what to do and how to
communicate with each other. Make sure that your apartment or home
Focus on Hurricane PreparednessBy Angeli Medina, MPA, BSN, RN, CEN, Emergency Management and Preparedness Committee
Type of Tropical Cyclone
Category Potential Damage
Wind Speed (mph)
Hurricane 1 Minimal 74- 95
Hurricane 2 Moderate 96- 110
Hurricane 3 Extensive 111- 130
Hurricane 4 Extensive 131- 155
Hurricane 5 Catastrophic 156+
The remains of the Biloxi Bay Bridge in Mississippi in the aftermath of Hurricane Katrina, which made landfall as a Category 3 storm.

Official Magazine of the Emergency Nurses Association 19
Disaster Preparedness Disaster Preparedness
is properly insured.
B. Know where to go. Stay with friends or
relatives who live outside the evacuation
zone areas; otherwise, report to an
evacuation center.
C. Keep ready a Go Bag that includes the
following:
• Copies of important documents in a
waterproof container
• Set of car and house keys, AM/FM radio,
batteries, whistle, flashlight
• Child care and special needs supplies
• First-aid kit, bottled water, nonperishable
food
D. Have an emergency supply kit. When
instructed to stay home, keep enough
supplies to survive for at least three days.
• One gallon of drinking water per person/day
• Nonperishable food
• First-aid kit, flashlight, battery-operated AM/
FM radio, batteries, whistle
• For disinfecting water ONLY, if directed to
do so by the health officials, keep iodine
tablets or one quart of unscented bleach
with eyedropper
• Phone that does not rely on electricity
E. If you do not live in an evacuation zone,
assemble an emergency supply kit.
F. If you live in a high-rise apartment
outside the evacuation zone, be prepared
to take shelter on or below the 10th floor. If
you live in a high-rise building located in the
evacuation zone, heed evacuation orders.
Other ConsiderationsA. Secure your home
• Keep lightweight objects inside the house.
• Anchor unsafe items, i.e. gas grill (turn off
propane tanks).
• Place valuables in waterproof containers.
• Shutter windows securely and brace
outside doors.
B. Assist persons with disability or special
needs.
C. Evacuate immediately when asked to do so.
D. Address pet care and bring pet supplies
when evacuating with your pet, i.e., leash,
muzzle, food, proof of shots, cage.
Resources
• en.wikipedia.org/wiki/Tropical_cyclone
• en.wikipedia.org/wiki/List_of_United_
States_hurricanes
• National Weather Service (September 2006).
“Hurricanes … Unleashing Nature’s Fury: A
Preparedness Guide” (PDF). National Oceanic
and Atmospheric Administration. Archived
from the original on February 26, 2008.
• National Hurricane Center. (2005). Glossary of
NHC/TPC Terms. National Oceanic and
Atmospheric Administration. www.nhc.noaa.
gov/aboutgloss.shtml
• NYC Office of Emergency Management
www.NYC.gov/oem
• Department of Homeland Security www.
ready.gov
• National Hurricane Center/Tropical Prediction
Center
www.nhc.noaa.gov
• National Weather Service www.weather.gov
• Federal Emergency Management Agency
www.fema.gov, www.floodsmart.com
• Natural Hazards Review, Journal of the
American Society of Civil Engineers,
“Normalized Hurricanes Damage in the
United States: 1900-2005
• New York Regions Prepares for Hurricane
Irene by James Barron, New York Times,
August 25, 2011
• Advance Hurricane Shelter Training for
Operators, Coastal Storm Plan, NYC OEM,
6/5/07
• Hurricane Irene Passes New York, MTA
Scramble to Reset Commute by Colleen Long
and David B. Caruso, 8/28, AP/The
Huffington Post
• Disaster Nursing and Emergency Preparedness
by Tener Goodwin Veenema, 2nd Edition
Established in 1991, the mission of the ENA Foundation is to provide educational scholarships and research grants in the discipline of emergency nursing.
Your Dollars = Your Future Investing in a nurse today is an immeasurable
contribution to the future of emergency nursing and patient care.
Invest in the future of your profession.Support the ENA Foundation.
Donate Now.
www.enafoundation.org

October 201220
Disaster Preparedness
4 Questions of Mass Casualty Patient Decontamination
Hospitals across the nation continue to work
hard to improve their preparedness for a mass
casualty incident or a mass contaminated
casualty incident related to either a man-made or
natural disaster. Since Sept. 11, 2001, billions of
dollars have been spent to improve the response
capability for such incidents. The primary focus
has been the incident scene. Thus, the patient
decontamination needs have been incident-
scene-centric.
However, OSHA statistics show that up to 80
percent of patients and others who are
contaminated will leave the scene before first
responders arrive. Almost all of these people
will eventually end up at a hospital
contaminated. The American Hospital
Association report identified that most hospitals
were well prepared for a low-intensity, short-
duration event, but there was inadequate
planning for the true large-scale events that
would require entire community involvement.
They went on to define a mass casualty event to
be a community-wide concern, necessitating a
response that incorporates multiple resources
within the community. This was based on the
possibility that a mass casualty situation may
actually have to be addressed for days or weeks
rather than hours.
Furthermore, the mass casualty incident may
overwhelm the capacity of all the hospitals in the
region, not just the local hospital. This would
greatly impact the capabilities of the local hospital
to provide service. Their conclusion was that
more community-wide planning was needed to
properly prepare hospitals for high-intensity and
long-duration events. While this article was
written in 2000, we still see the same problems.
Most hospitals have improved by embracing
the Hospital Incident Command System, which
provides for better communication and operations
during disasters and mass casualty incidents. There
are four key questions that each hospital needs to
incorporate into its emergency operations plan
regarding patient decontamination:
How Many?How many patients can you decontaminate
during a MCCI? This is a complicated question.
Considerations need to include the following:
1. Your hospital surge capacity.
2. Your plan for moving or dealing with patients
when you exceed both your operating
capacity and your surge capacity. (Are these
capabilities different if on back-up
generators?)
3. Your staffing pool and available staff.
4. Your plan to bring in volunteers to assist staff.
5. The size of your staging/triage area for
decontaminated patients. (You may have
the capacity to decontaminate 100 patients
an hour, but can you treat/release or admit
100 patients an hour? If not, where do you
place these overflow patients where they
can monitored by professional staff and
have access to bathrooms, water and food
as their numbers increase?)
6. The number of injured who are
decontaminated at the scene and
transported clean to your hospital.
7. Basic supply levels.
8. Estimated resupply delivery times and
methods.
9. Where will patients go upon discharge? How
will they get there?
10. Where will you place the discharged patients
who are awaiting transport to shelters? What
if they refuse to leave?
11. How will you deal with family?
12. Will treatment be given before
decontamination? (Note: Any equipment
used will be lost as contaminated – oxygen
tanks, beds, cots and more.)
13. Where will contaminated human remains be
staged? (You will need a separate storage
method and place for contaminated human
remains.)
14. How will your staff communicate within the
mass gathering areas of patients (post-
decontamination, triage and staging area for
discharged patients)?
How Long?How long can your hospital operationally
maintain a mass patient decontamination line?
There are several key components that will be
factors in answering this question. Your
decontamination operation depends on
specialized PPE/equipment which is in limited
supply at your hospital. How long can you
maintain your mass decontamination efforts if
level-C PPE is required? This will be based on
the number of filters, batteries, protective suits
and boots your facility has in stock.
Another factor is the amount of available and
trained staff. During an MCCI, the hospital
patient load is surging. This requires additional
staff in all areas of operation. How many staff
members are required to maintain your mass
decontamination line? How often are they
swapped out? If you are using level-C PPE,
swap-outs will likely be on an hourly basis. In
extreme temperature situations, it may need to
be more frequent. These staff members need
technical decontamination as they swap out.
You should also maintain a partially dressed
safety response team to deal with staff
decontamination emergencies.
What If?What happens to your mass decontamination
line when an anxious, contaminated patient
pulls off a staff member’s PAPR hood, or a
patient decontamination team member goes
down, becomes contaminated or suddenly
displays signs and symptoms of chemical or
radiation exposure? Many patients may feel
personally violated by the decontamination
process. What if the contaminated patients
refuse to disrobe or give up personal items?
What if a group of contaminated patients
becomes violent and/or attempts to storm its
way into the ED demanding treatment?
Rebmann & Mohr report that fewer than 50
percent of Missouri nurses have received training
in MCI or MCCI hospital response. Furthermore,
fewer than 25 percent have received hands-on
training in clinical disaster management. How
will the remaining staff react to this situation? It is
By Paul Meek, MA, BSN, BEd, RN, CEN, CLNC

Official Magazine of the Emergency Nurses Association 21
Disaster Preparedness Disaster Preparedness
very conceivable that your decontamination staff
could begin to refuse to don PPE and
decontaminate patients. They may fear for their
lives and voice concern that the level of PPE,
level of training and/or security is inadequate.
Can you force your minimally trained staff to
risk their lives and health to perform patient
decontamination? Remember, as the number of
patients decontaminated increases, so will the
demand on your supplies and staff. What
happens when your facility can no longer staff
the mass patient decontamination line? You must
have detailed in your plan the number of staff
required to safely maintain your mass patient
decontamination line.
What Then?
Having identified needs, we must find
solutions that can prevent or resolve these
situations during an MCCI. You need to develop
a plan to move discharged patients and family
members away from your hospital, as you will
not be able to both surge and shelter. Your
emergency plans need to include requesting a
shuttle that will transport these discharged
patients, worried wounded and family members
to the established local shelters.
Furthermore, you need to plan if you want to
move admitted patients. You can try to call the
local air ambulance, but they will likely be
dispatched from the multi-agency coordination
system. If NDMS is activated and an ESF 8 Aerial
Point of Embarkation is established, you still
will need to request transport or arrange
transport from your hospital to the APOE. If
your mass patient decontamination line fails,
you must have a plan for the contaminated
patients who will continue to arrive at your
hospital. One option would be a shuttle that
would take these contaminated patients,
worried wounded and family members to a
mass decontamination site.
ConclusionEvery hospital in our nation has a limit for
how long or how many patients it can
decontaminate in a MCCI. As such, data needs
to be collected so that emergency preparedness
planners can develop strategies to better assist
hospitals in the MCCI incident. Hospitals need
to embrace their designation as critical
infrastructure/key resources and step forward in
their planning by requesting assistance from
local, state and federal agencies in times of
disaster, terrorist attack and other emergencies.
The 2009 U.S. National Health Security
Strategy states: ‘‘Government at all levels has an
inherent responsibility, particularly in helping
build and strengthen the systems (e.g., plans,
people, and equipment) that help prevent (e.g.,
through biosafety, biosecurity, nonproliferation
of WMDs, and other measures), protect against
(e.g., through community interventions,
including medical countermeasures), respond
to, and recover from health incidents.”
The time has come for hospital MCI and
MCCI plans to develop ways to innovate,
incorporate and communicate their potential
needs to the local and state emergency planners
and their state National Guard before the next
disaster or terrorist attack.
References
Powers, R. (2009). Evidence-based ED Disaster
Planning. Journal of Emergency Nursing,
35(3), 218-223.
(2005). OSHA Best Practices for Hospital-Based
First Receivers of Victims from Mass Casualty
Incidents Involving the Release of Hazardous
Substances: Occupational Safety and Health
Administration, 1-30.
(2009). National Health Security Strategy of the
United States of America. United States
Department of Health and Human Services,
1-44.
(2000). Hospital Preparedness for Mass Casualty:
Final Report. The American Hospital
Association, 1-58.
Darr, K. (2006). Katrina: Lessons from the
Aftermath. Hospital Topics: Research and
Perspectives on Healthcare, 30-33.
Rebmann, T. & Mohr, L. B. (2008). Missouri
Nurses’ Bioterrorism Preparedness.
Biosecurity and Bioterrorism, 6(3), 243-251.
Disaster Nursing and Emergency Preparedness for Chemical, Biological, and Radiological Terrorism and Other Hazards (3rd Edition) Editor - Tener Goodwin Veenema, PhD, MPH, MS, CPNP
This brand new edition has strengthened its pediatric focus with updated and expanded chapters on caring for children’s physical, mental, and behavioral health following a disaster. New chapters address climate change, global complex human emergencies, caring for patients with HIV/AIDS following a disaster, information technology and disaster response, and hospital and emergency department preparedness.
The text provides a vast amount of evidence-based information on disaster planning and response for natural and environmental disasters and those caused by chemical, biological, and radiological elements, and disaster recovery.
760 pagesISBN: 978-0-470-27949-6©2012
Price: $110ENA Member Price: $99
Free Shipping! Offer ends October 31, 2012
To order, visit www.ena.org/shop and mention this ad in the comment section or call 800-900-9659 (M-F 9 a.m. - 5 p.m. CT).
Special Offer for the MonthMarketplace

October 201222
Disaster Preparedness
What Does It Take to Make Your ED Ready?
The television reporter’s interview in the
Louisiana State University Health–Shreveport
Emergency Department began with a weighty
question: ‘‘So what goes into making the
emergency department prepared for a disaster
or mass casualty like the recent and tragic
shooting in Aurora, Colo.? Are we ready?’’
The reporter was aware of the heroic
response required by emergency nurses, doctors
and other first responders in Aurora in July and
wanted to learn more about local and regional
ED and hospital planning for a similar threat.
We discussed planning and preparedness for
various hazards.
What do you think it takes? What are the
potential hazards, considerations and roles for
the ED?
Recent Incidents and Hazards Threatening the EDImagine yourself as an emergency nurse in the
following incidents:
• Bomb: On July 19, a 50- to 60-pound pipe
bomb was carefully removed from the trunk of
a visitor’s car in the St. Mary’s Hospital
(Rochester, Minn.) parking garage. Threats exist
outside and sometimes within the hospital.
When it comes to bombings, the CDC has
referred to bombings as the ‘‘expected surprise.’’
• Tour Bus MCI: On Aug. 3, 38 people were
transported to local EDs and trauma centers
after a double-decker bus slammed into a
bridge pillar support while speeding down an
Illinois highway. School bus accidents occur
almost weekly somewhere in the country,
resulting in numerous pediatric injuries.
• IT Systems Failure: On Aug. 3, the Los
Angeles Times reported dozens of hospitals
across the U.S. lost access to critical electronic
medical records during a major, five-hour
computer outage later attributed to human
error. The outage raised concerns about data
stability and security weaknesses potentially
compromising patient care.
• Hazmat: On Aug. 1, the Houston-area
Danbury Hospital ED was reported shut down
after word was received of several incoming ill
patients who had been exposed to an unknown
white powder. A decontamination unit was
established by hazmat teams at the hospital.
• Hurricane: On Sept. 2, the East Jefferson
Hospital (Metairie, La.) emergency department
reported seeing the types of injuries associated
with hurricane debris cleanup. Hurricane Isaac
injuries in the ED included traumas resulting
from debris removal, with increased numbers of
lacerations, plus back injuries resulting from
falls from ladders.
• Power Failure: On July 15, Doctor’s
Hospital (White Rock, Texas) was reported to
have experienced an electrical power failure
after a storm. A backup emergency generator
then failed, leaving dependant systems without
power for about two hours.
• Tornado: On June 28, security-camera
video from the ED waiting area of St. John’s
Regional Medical Center in Joplin, Mo., which
was hit by a devastating tornado May 22, 2011,
was posted on the Internet. Viewers can watch
as the still room becomes suddenly engulfed in
the storm, with chairs, curtains and debris
swirling violently.
ED disaster responses can result from
multiple natural, man-made and/or
technological threats. Multiple populations can
be affected, including pediatric, adult and the
elderly. Emergency nurses need to be prepared
for the ‘‘all hazards’’ response. A starting place
for all hazards principles and strategy is found
in the ENA Emergency Management and
Preparedness for All Hazards position statement.
The ENA ‘All Hazards’ Position StatementMany excellent resources for disaster and
emergency management applicable to the
emergency nurse can be found at www.ena.
org. One in particular, ENA’s Emergency
Management and Preparedness for All Hazards
position statement, offers significant
considerations and concepts for an emergency
nurse to ‘‘be prepared.’’
Within the ENA position statement is a
background description of the emergency nurse
role in the phases of disaster mitigation,
preparedness, response and recovery. The
statement also provides 13 focus areas detailing
the ENA position.
Position statement component topics
addressed include the following:
• The primary importance of individual
preparedness
• Considerations for ongoing preparedness
training and education
• The National Incident Management System
• Implications for resource allocation during
disaster
• Importance of the hazard vulnerability
analysis
• Evaluating and testing emergency response
plans
• Recognizing needs of special and
vulnerable populations
• Planning for the ability to self-sustain for
96 hours
• The volunteer response including
Ready or Not?
By Knox Andress, BA, RN, AD, FAEN

Official Magazine of the Emergency Nurses Association 23
Disaster Preparedness Disaster Preparedness
deployment and engagement
• Standards of Care in disaster
• Mass Casualty triage
• Continuing education and training
A starting place for appreciating response
needs for emergency nurses is the ENA
Emergency Management and Preparedness for
All Hazards position statement.
Resources
http://kaaltv.com/article/stories/S2696701.
shtml?cat=10151
http://www.usatoday.com/news/nation/
story/2012-08-02/megabus-
crash/56715768/1?csp=hf
http://articles.latimes.com/2012/aug/03/
business/la-fi-hospital-data-outage-20120803
http://www.myfoxhouston.com/
story/19184465/2012/08/02/hazmat-
teams-shut-down-er-of-angleton-hospital
http://www.nola.com/hurricane/index.
ssf/2012/09/high_number_of_injuries_
from_i.html
http://watchdogblog.dallasnews.com/
2012/07/power-failure-sends-regulators-to-
doctors-hospital-in-e-dallas.html/
http://www.wtsp.com/news/national/
article/261482/81/Caught-on-camera-ER-
camera-during-tornado
http://www.ena.org/SiteCollection
Documents/Position%20Statements/
AllHazards.pdf
Readers may contact the
author at [email protected].
Follow Knox Andress @ENAdman.
By Carl Schramm, RN, EMT-B Emergency Management and Preparedness Committee
Building Relationships in Advance Aids Disaster Planning
We all have disaster/emergency response plans for our facilities to address
a wide range of emergencies, ranging from natural disasters to industrial
accidents to terrorist attacks. How realistic are these plans?
A good, comprehensive plan must include not only a facility’s resources
but the resources available from outside facilities and agencies. When a
disaster occurs, one facility’s resources can quickly be stretched to the
limit. Augmenting and replenishing these resources can be extremely
difficult, if not impossible, during a disaster. To strengthen our capabilities,
we need to coordinate with outside facilities and agencies.
The key to successful coordination is building professional relationships
before a disaster occurs, when you have the time necessary to develop a
good working relationship and address potential problems. Emergency
managers need to sit down with the leaders of outside resources to share
their emergency response plans.
External resources need to be evaluated and understood to ensure that
they are going to be able to assist our facilities during emergency
operations. It is important to know exactly what an agency is going to
send when it is called to assist during an emergency. For example, can the
agency send supplies, equipment and/or personnel? Which ones and how
much? Will the type of emergency have an effect on the resources an
outside agency can send?
Evaluate the type of equipment used by an outside facility or agency to
ensure that its equipment is compatible with your own. What brand of
chemical suits does it use, what level of protection do the suits offer, and
how many does it stock? It does no good to call in outside assistance that
cannot work with your existing responders.
Know in advance the types of communication equipment other facilities
and agencies have. Is it possible to communicate with each other if
traditional communication methods go down? If not, can something be
done to accomplish this, such as adding frequencies to existing radios?
Just having contact information for the leaders of these outside facilities
and agencies can be vital during an emergency.
To help operations run smoothly during an emergency, we need to
determine to what level each facility or agency has trained its personnel.
The requirements for these training levels are vague at best, and there can
be a wide range of interpretation of requirements. For example, while the
objective of decontamination is to remove contamination, not every
program teaches decontamination by using the same steps or in the same
order.
During an emergency, the police and fire departments and emergency
medical services each have to address different aspects of an emergency
incident and use resources and personnel differently. Depending on the
nature of the emergency, these outside facilities and agencies may not
always have the ability to send the same assistance to any one facility. We
need to realize that these responsibilities can cause outside agencies to
commit more of their resources to their primary objectives.
Having an understanding of the different responsibilities and objectives
of these outside agencies is beneficial during an emergency. We can better
understand why outside agencies handle an emergency the way they do,
and they will better understand why we do what we do. We can modify
how we handle an emergency to allow us to better coordinate our
operations. Having an understanding that emergency medical responders
have to follow specific protocols when they are in the field, and that they
do not operate under the same rules as the nurses who work in the
emergency department, is important. This understanding and respect of
each other’s responsibilities will prevent conflict during an emergency and
help everyone to use resources as efficiently as possible.
Developing and maintaining emergency/disaster response plans is a
difficult and time-consuming assignment. But without taking these
considerations into account, it will be hard to have a truly effective,
comprehensive plan. When an emergency occurs, no one wants to wait
for help, only to find out it was either not what they were expecting or
not coming at all. We need to prepare as best we can for anything to
happen at any time.

Robert Breese, CCEMTP, FP-CBehind the Scenes Award
Kathy J. Morris, DNP, APRN, FNP-C, FAANPFrank L. Cole Nurse Practitioner Award
Joyce Foresman-Capuzzi, MSN, RN, CCNS, CEN, CPN, CTRN, CCRN, CPEN, SANE-A, EMT-PGail P. Lenehan Advocacy Award
Diane L. Gurney, MS, RN, CEN, FAENJudith C. Kelleher Award
Sharon McGonigal, RN, CENENA Lifetime Achievement Award
Leslie A. Christiansen, RN, BS, CENNurse Manager Award
Donna M. Roe, DNP, ARNP-BC, CENNursing Competence in Aging Award
Timothy J. Murphy, MSN, RN, ACNP-BC, CENNursing Education Award
Judith Common, RN, CEN, CPEN, CA/CP SANE, SANE-A, SANE-PNursing Practice Award
Anne Stefanoski, BSN, RN, CENNursing Professionalism Award
Michelle A. Marini, RN, MSN, CPNP, CPENNursing Research Award
Amy W. Truog, RN, BSN, CPENNursing Research Award
Joseph M. Lenehan, MDPresident’s Award
Kristen Connor, RN, PHN, BSN, CENRising Star Award
Sandra M. Waak, RN, CENLinda Arapian, RN, MSN, CEN, CPEN, EMT-BLisa Tenney, RN, BSN, CEN, CPHRMAnne May , RN, BSNEmilie Crown, RNPamela S. Fox, RN, BSN, CEN, CPENLucy McDonald, RN, CPEN, CPN, EMT-BTeam Award
Achievement Awards
Meredith Jaye Addison, MSN, RN, CEN, FAEN
Rita T. Anderson, RN, CEN, FAEN
Audrey Elizabeth Cloughessy, AM, MHM, RN, FAEN
Christine M. Gisness, MSN, RN, BC, FNP-C, CEN, FAEN
Diane L. Gurney, MS, RN, CEN, FAEN
Andrew D. Harding , MS, RN, CEN, NEA-BC, FACHE, FAHA, FAEN
Cindy L. Hearrell, MSN, RN, CEN, FAEN
J. Jeffery Jordan, MS, RN, MBA, CEN, CNE, EMT-P, FAEN
Fred Neis, MS, RN, CEN, FACHE, FAEN
India J. Taylor Owens, MSN, RN, CEN, NE-BC, FAEN
Gwyn Parris-Atwell, MSN, RN, FNP-BC, CS, CEN, FAEN
Judith A. Scott, MHA, BSN, RN, PHN, FAEN
Paula Tanabe, PhD, MPH, MSN, RN, FAEN
Mary Ann Teeter , MEd, RN, FNP-C, CEN, CNRN, FAEN
Academy of Emergency Nursing Inductees
Advocate Good Shepherd Hospital Emergency Department (Barrington, IL)
Beaumont Health System – Grosse Pointe Emergency Center (Grosse Pointe, MI)
Boston Children’s Hospital Emergency Department (Boston, MA)
Cedars-Sinai Medical Center, Ruth and Harry Roman Emergency Department (Los Angeles, CA)
Chandler Regional Medical Center Emergency Department (Chandler, AZ)
Children’s Medical Center of Dallas, Seay Emergency Center (Dallas, TX)
Cincinnati Children’s Hospital Emergency Department – Burnet Campus (Cincinnati, OH)
Indiana University Health Methodist Hospital Emergency Medicine and Trauma Center (Indianapolis, IN)
Lantern Awards

Robert Breese, CCEMTP, FP-CBehind the Scenes Award
Kathy J. Morris, DNP, APRN, FNP-C, FAANPFrank L. Cole Nurse Practitioner Award
Joyce Foresman-Capuzzi, MSN, RN, CCNS, CEN, CPN, CTRN, CCRN, CPEN, SANE-A, EMT-PGail P. Lenehan Advocacy Award
Diane L. Gurney, MS, RN, CEN, FAENJudith C. Kelleher Award
Sharon McGonigal, RN, CENENA Lifetime Achievement Award
Leslie A. Christiansen, RN, BS, CENNurse Manager Award
Donna M. Roe, DNP, ARNP-BC, CENNursing Competence in Aging Award
Timothy J. Murphy, MSN, RN, ACNP-BC, CENNursing Education Award
Judith Common, RN, CEN, CPEN, CA/CP SANE, SANE-A, SANE-PNursing Practice Award
Anne Stefanoski, BSN, RN, CENNursing Professionalism Award
Michelle A. Marini, RN, MSN, CPNP, CPENNursing Research Award
Amy W. Truog, RN, BSN, CPENNursing Research Award
Joseph M. Lenehan, MDPresident’s Award
Kristen Connor, RN, PHN, BSN, CENRising Star Award
Sandra M. Waak, RN, CENLinda Arapian, RN, MSN, CEN, CPEN, EMT-BLisa Tenney, RN, BSN, CEN, CPHRMAnne May , RN, BSNEmilie Crown, RNPamela S. Fox, RN, BSN, CEN, CPENLucy McDonald, RN, CPEN, CPN, EMT-BTeam Award
Achievement Awards
Meredith Jaye Addison, MSN, RN, CEN, FAEN
Rita T. Anderson, RN, CEN, FAEN
Audrey Elizabeth Cloughessy, AM, MHM, RN, FAEN
Christine M. Gisness, MSN, RN, BC, FNP-C, CEN, FAEN
Diane L. Gurney, MS, RN, CEN, FAEN
Andrew D. Harding , MS, RN, CEN, NEA-BC, FACHE, FAHA, FAEN
Cindy L. Hearrell, MSN, RN, CEN, FAEN
J. Jeffery Jordan, MS, RN, MBA, CEN, CNE, EMT-P, FAEN
Fred Neis, MS, RN, CEN, FACHE, FAEN
India J. Taylor Owens, MSN, RN, CEN, NE-BC, FAEN
Gwyn Parris-Atwell, MSN, RN, FNP-BC, CS, CEN, FAEN
Judith A. Scott, MHA, BSN, RN, PHN, FAEN
Paula Tanabe, PhD, MPH, MSN, RN, FAEN
Mary Ann Teeter , MEd, RN, FNP-C, CEN, CNRN, FAEN
Academy of Emergency Nursing Inductees
Advocate Good Shepherd Hospital Emergency Department (Barrington, IL)
Beaumont Health System – Grosse Pointe Emergency Center (Grosse Pointe, MI)
Boston Children’s Hospital Emergency Department (Boston, MA)
Cedars-Sinai Medical Center, Ruth and Harry Roman Emergency Department (Los Angeles, CA)
Chandler Regional Medical Center Emergency Department (Chandler, AZ)
Children’s Medical Center of Dallas, Seay Emergency Center (Dallas, TX)
Cincinnati Children’s Hospital Emergency Department – Burnet Campus (Cincinnati, OH)
Indiana University Health Methodist Hospital Emergency Medicine and Trauma Center (Indianapolis, IN)
Lantern Awards

October 201226
The ENA Lantern Awards, first presented in
2011, were envisioned as a means of recognizing
exemplary emergency departments. In addition,
the awards provide an opportunity for
identifying outstanding, novel practices from
those EDs that achieve Lantern Award
designation. Based on a systematic review of
each application, which is subjected to a blinded
review process by multiple reviewers and
evaluated against preset evidence-based criteria,
the awards recognize EDs that exemplify
exceptional practice and innovative performance
in the core areas of leadership, practice,
education, advocacy and research. Here are
some of the initiatives that made these 2012
recipients exemplary:
Advocate Good Shepherd Hospital Emergency Department (Barrington, Ill.)Advocate Good Shepherd Hospital is a not-for-
profit hospital in the Chicago suburbs, serving
almost 34,000 patients in the ED each year. It’s
an accredited trauma and stroke center. Twenty-
one percent of patients presenting to the ED are
admitted. Within the general ED, 5 percent of
visits are pediatric patients under age 18.
Staff and leaders identified opportunities for
planning and collaboration to address the needs
of patients at both ends of the age spectrum.
Following a hazard vulnerability analysis, a
disaster drill was planned to include more than
20 children to test the hospital’s response to a
disaster involving unaccompanied children.
Lessons learned from the multi-disciplinary,
intradepartmental and intra-agency drill resulted
in changes implemented to the pediatric
decontamination process, as well as the child
identification process. Having children
participate in pediatric disaster preparedness
exercises is one effective strategy for meeting
the needs of the community during a disaster
response.
Regarding older adult patients, analysis and
review of data revealed that falls among this
population were the primary causative factor for
trauma admission, with 51 percent of these falls
occurring in the community and 25 percent of
trauma admissions coming from one specific
senior living facility. Staff members embarked on
a training initiative to present the Matter of
Balance program at the identified facility. The
program, which teaches strategies to overcome
the fear of falling, helps set realistic goals for
increasing activity, as well as strength and
balance, with the goal of reducing the risk of
falling. Six months after initiating this
collaboration, there was a 62 percent
decrease in fall admissions, and the affected
facility reported a 77 percent decrease in total
falls. Due to this success, the team has taught
the Matter of Balance program at other senior
living facilities and senior community centers in
10 different cities in and around their service
area.
Beaumont Health System – Grosse Pointe Emergency Center (Grosse Pointe, Mich.)Beaumont Health System in Grosse Pointe,
Mich., is a not-for-profit facility that has nearly
37,000 patient visits to its ED yearly. Sixty-nine
percent of the patients admitted to the hospital
come through the ED, and almost 30 percent of
ED patients are admitted.
The ED at Beaumont Health System – Grosse
Pointe has proven that strong, committed,
involved and visionary leadership can inspire
staff engagement to improve practice, safety and
satisfaction for patients, families and staff. The
staff works collaboratively to own its department
by assuming responsibility for various services,
such as stroke and chest pain certifications. The
ENA Emergency Nursing Scope and Standards of
Practice, as well as ENA position statements and
toolkits, have been cited as foundational
resources for many activities and best practices
implemented in the emergency department. The
ED successfully advocated for legislation in
collaboration with the Michigan ENA State
Council to increase penalties for violence against
health care workers. In addition, Beaumont
described a clear commitment to training of ED
and security staff on de-escalation and
prevention of violent incidents. As a result,
incidents have been declining, and patients and
staff are safer.
Beaumont also described a longstanding
support of family presence that is hospital-wide,
including comprehensive support for patients
and families in a needs-based model. An
impressive component of its family presence
program is family-member follow-up for up to a
year.
Boston Children’s Hospital Emergency Department (Boston)Boston Children’s Hospital is a not-for-profit,
academic medical center that is a designated
trauma center. It is recognized as a Magnet
facility and has also received the Beacon Award.
The ED sees just under 59,000 patients annually,
and 58 percent of hospital admissions present
through the ED.
The team at Boston Children’s Hospital ED
recognizes the challenges immunocompromised
patients pose when they present to the
emergency department with a fever. Time to
antibiotics is critical to outcomes. Clinical
practice guidelines set a target for antibiotic
administration within 60 minutes of arrival to the
ED. A one-year retrospective chart analysis
demonstrated that this time was exceeded more
than 50 percent of the time. A multidisciplinary
team mapped the current process for antibiotic
administration and identified barriers to meeting
the target time. Interventions implemented
included a fast-pass system, ANC pre-notification
calls, communication enhancements between
team members, retraining of nurses on porta-
cath access, pharmacy prioritization of Fever and
Neutropenia template orders and reinforcement
of topical cream application by parents before
ED arrival. As a result, the mean time to
antibiotic delivery dropped from 99 minutes to
49 minutes, and the percent of patients who met
the target time to antibiotics rose from 50
percent to 80 percent.
Cedars-Sinai Medical Center, Ruth and Harry Roman Emergency Department (Los Angeles)Cedars-Sinai Medical Center is a 952-bed,
not-for-profit, non-academic teaching hospital
and is also a designated trauma, chest pain and
stroke center. The Ruth and Harry Roman ED at
Cedars-Sinai serves almost 84,000 patients
annually. Like many hospitals, Cedars-Sinai has
experienced long waits for availability of
inpatient beds. It was noted that it knew its
process needed improvement, as it typically took
more than six hours to admit an ED patient.
The organization implemented a project to
address patient flow called the Toes Out-Toes In
initiative. Using the Toyota Production Process
Improvement Methodology, it engaged a
Sharing Innovations and Best PracticesAuthored by the 2012 ENA Lantern Award Committee: Gwyn Parris-Atwell, MSN, RN, FNP-BC, CS, CEN, chairperson; Denise M. Bajer, MSN, RN, CEN, NE-BC; Jennifer M. Davis, MSN, MPH, RN, EMT-P, CEN; Susan K. Ebaugh, MSN, APRN, CEN, ACNS-BC; Andorra L. Foley, MSN, RN, CEN; Tami L. Morin, MS, BS, RN, CPEN; Teresa O’Neill, MSN, MBA, RN; India J. Owens, MSN, RN, CEN, NE-BC; Cheryl Rourke, MSN, RN, NE-BC; Barbara A. Weintraub, MSN, MPH, RN, APRN, CEN, CPEN, ACNP-BC, FAEN; and Matt Powers, MS, BSN, RN, CEN, MICP, Board of Directors liaison
2012 Lantern Award Recipients

Official Magazine of the Emergency Nurses Association 27
multidisciplinary team to
eliminate waste in its bed
turnaround process. The
team used rapid
improvement events to
make multiple process
changes, leading to
tremendous improvement
in throughput. Changes
were made to the
discharge computer entry,
eliminating steps and
resulting in an average
one-hour reduction in
turnaround times, as well
as providing real-time
notification of the
discharge.
A housekeeping discharge team was also
created, decreasing room cleaning times from
75 to 45 minutes. This department’s staffing was
changed to provide increases at peak times,
mimicking the hotel industry. Only clean and
ready rooms were then assigned for patient
placement. Additionally, a culture change took
place, including having the staff in the medical/
surgical/monitored units call the ED for report
within 20 minutes of an ED admission
notification, essentially ‘‘pulling the patient’’ to
the open bed. Within one year, this organization
had reduced the turnaround time to 110
minutes on average. Drilling down further into
the outlier data, Cedars-Sinai Medical Center has
been able to trim further waste, now averaging
88 minutes to admit an ED patient. One
important change was to eliminate the no-fly
zone where floor nurses would not take report
15 minutes before or after the change of shift.
This initiative helped to eliminate some of the
bottleneck issue of patients waiting to go to
their rooms from the ED and facilitated timelier
placement.
Chandler Regional Medical Center Emergency Department (Chandler, Ariz.)Chandler Regional Medical Center is a 209-bed,
not-for-profit, non-academic teaching hospital in
Chandler, Ariz. Sixty-three percent of hospital
admissions originate in the ED, which serves
nearly 63,000 patients a year.
The emergency nurses are continually
developing and implementing ideas to improve
patient outcomes and quality of care. In
response to news that antivenom was being
discontinued due to a lack of state funding, one
of the nurses became very concerned, as they
see a pediatric and older adult population that
often needs the drug. She took the initiative to
find out about a newly available investigational
antivenom. Steps were taken to design a
research study and get approval from the
Institutional Review Board. The physicians and
nurses in the ED eagerly participated in the
research, and the project became a huge
collaborative effort not just between the ED staff
and pharmacy, but also with other area
hospitals and the Poison Control Center. Many
envenomed patients arrive in a life-threatening
condition requiring transfer to an ICU; yet with
the antivenom protocol developed through the
research conducted, patients are now
discharged within four hours of arrival to the
ED with fewer complications.
Children’s Medical Center of Dallas, Seay Emergency Center (Dallas)The Seay Emergency Center at Children’s
Medical Center of Dallas is a not-for-profit,
academic medical center in the Southwest
serving more than 118,000 children per year.
This designated trauma center and Magnet-
status medical center admits 11 percent of its
inpatients through the ED.
Patient safety is a top priority at this facility.
With more than 88,000 doses of medication
administered in the emergency center in January
2012 alone, medication safety has been a major
focus, with several initiatives implemented to
prevent medication errors, increase reporting
and support a just culture. One initiative
involves ED staff on the hospital’s High Alert
Medication Committee, which shares data as
well as identifies trends and opportunities for
improvement. An initiative to reduce the
incidence of incorrect weights being entered
into the electronic health care record resulted
from the work of this committee. After review
of the issues, improvements were identified,
including the use of an alert activated when a
patient falls outside the normal range for his or
her age, and a request for a second entry. In
addition, steps were initiated to introduce
electronic scales that transfer data directly into
the EHR, reducing human error.
Other efforts to eliminate and reduce the
number of medication errors also have
contributed to a significant decrease in errors at
this facility over the last two years. Some
examples are the implementation of a barcode
system, effective use of the EHR to provide
defaults and prompts for high
alert medications, and the
addition of a pharmacist in
the emergency department
24/7.
Cincinnati Children’s Hospital Emergency Department – Burnet Campus (Cincinnati)Cincinnati Children’s Hospital
is a not-for-profit, academic
medical center that is a
designated trauma center.
The Burnet Campus ED
serves about 89,000 children
a year, with 14 percent of
those patients being admitted.
Cincinnati Children’s employs the innovative
practice of using postcards to close the
communication gap and improve patient
satisfaction. An interdisciplinary team that meets
weekly to review patient satisfaction data
recognized that identifying a patient’s chief
complaint was only a small part of the puzzle.
They began by collecting patients’ and families’
expectations of the visit on postcards. These
postcards are then used as a way to
communicate the families’ unstated
expectations. For example, their child’s primary
physician may have sent them to the ED with
the expectation that the ED would start an IV
and give their child fluids. The cards also serve
as a tool that alerts the staff to the families’
concerns. As emergency nurses, we know that
some of our patients come through our door for
reassurance. Perhaps their cousin was
diagnosed with cancer after exhibiting similar
symptoms. The staff is alerted early on, through
the postcards, that reassurance is a primary
need of the patient and family. This tool has
taken some of the guess work out of meeting
patients’ expectations at Cincinnati Children’s,
resulting in enhanced patient satisfaction scores
and a feeling by staff that it is better able to
meet patients’ needs.
Safety is also a top priority in any high-
functioning ED. The interdisciplinary team at
Cincinnati Children’s recognized that when
stress levels are high, miscommunication is
more common. This led to the implementation
of a shared-mental-model process during
stabilization of critically ill or injured patients.
The shared mental model begins with a history
and primary assessment using a team model led
by a nurse and physician. The physician then
asks for everyone’s attention while a shared
mental model is performed. The physician
shares aloud the initial assessment and plans.
The team quickly reaches agreement on next
steps together. A sharing of the mental model
typically occurs within five to seven minutes of Continued on page 40

October 201228
Watch for ENA’s call for candidates seeking election in 2013 to serve on
the board of directors and on the Nominations Committee. Application
information for candidates will be available this month at www.ena.org.
Open board positions include president-elect, secretary/treasurer and
two three-year-term director positions. The officer positions are one-year
terms with the president-elect continuing on to the presidency the
following year, then an additional year as immediate past president.
Depending upon the outcome of the officer elections, additional director
seats may be available for terms equal to the unexpired terms of the
vacating directors. The candidates receiving the next highest number
of votes would fill these positions.
Qualifications for all board of director positions include current ENA
membership and membership for five consecutive years prior to
submitting a candidate application; a current unencumbered RN license;
attendance within the last three years at one ENA General Assembly as
a delegate, alternate delegate or member of the board of directors; and
having served in an elected or committee position on the local, state or
national level within the past five years. Candidates for the position of
president-elect and secretary/treasurer currently must be serving as a
voting member of the national ENA board of directors. More qualification
details are listed within the current ENA bylaws at www.ena.org.
Application ProcessInterested members are required to complete and submit an application
with a professionally taken digital portrait photograph (details will be
included on the application form) to [email protected]. The deadline for
submission will be posted on the ENA Web site as soon as it is available.
Watch for the application form available this month at www.ena.org.
A candidate screening process is conducted on all board of director
and Nominations Committee candidates. The screening process includes a
limited background check verifying personal identity, professional licensure,
current employer, highest academia and a criminal history check.
Accepted candidates for the board of directors are encouraged to attend
the Candidates Election Forum Saturday, March 2, at Leadership
Conference 2013 in Fort Lauderdale, Fla.
Making a CommitmentServing on the ENA board of directors and Nominations Committee in any
capacity requires a significant time commitment. Board service involves
in-person meetings, reading correspondence, completing projects and
talking to members on a variety of issues.
Prior to running for national office, candidates are encouraged to
discuss the role and responsibilities with their employers and negotiate the
time they will be away from work. The support of the candidate’s
employer and family is essential in meeting the responsibilities of
a board member.
Board of Director ResponsibilitiesThe ENA bylaws determine the official duties of the board of directors.
The major responsibilities of the board include all duties entrusted to
officers and directors of a corporation, including determining association
policy, providing oversight of the financial affairs of the association and
reviewing and evaluating the strategic plan.
The ENA board of directors conducts its official business meetings with
all information and agenda items distributed electronically. Board
members are required to work with this technology.
Board MeetingsBoard members are required to attend scheduled board of directors
meetings. Expectations for these meetings include the following:
• Attendance at the August Nursing Organizations Alliance annual Nursing
Alliance Leadership Academy conference (for incoming officers and
directors).
• Submission of agenda items based upon member needs or current
trends in emergency health care.
• Required attendance at the year-end 2013 board of directors meeting
and board member orientation.
• Thorough review of the board agenda materials prior to the meeting.
• Utilization of contacts, resources, state presidents and other members
to obtain a broader perspective on agenda topics.
• Recommendation of potential strategies, charges and projects for
consideration in the strategic planning process.
• Familiarity with current technology (smart devices) and access to
the Internet.
Committee DutiesEach board member is assigned liaison responsibilities for two to four
national committees or work teams. The role of the board liaison is to
represent the board’s position on the committee’s charges, to participate in
committee assignments, to assist the committee’s staff liaison in reporting
committee activities to the board and to mentor committee members as
future chairpersons and/or board members.
The president also may ask board members to represent ENA at
meetings of affiliate or allied organizations. Typically, assignments are
based upon a board member’s area of expertise.
State ResponsibilitiesEach board member, excluding the president, serves as board liaison for
five to six states. Board members are encouraged to have frequent contact
with state presidents to exchange information about activities and the
needs of members at the local and state levels.
ENA Call for…
2013 ENA Board of Director and Nominations Committee CandidatesNote: Amendments to the current ENA bylaws that may change candidate eligibility requirements were decided at the 2012 General Assembly, Sept. 12-13. For updated information, please check www.ena.org.

Official Magazine of the Emergency Nurses Association 29
Continued on page 39
2013 ENA Board of Director and Nominations Committee CandidatesNote: Amendments to the current ENA bylaws that may change candidate eligibility requirements were decided at the 2012 General Assembly, Sept. 12-13. For updated information, please check www.ena.org.
The ENA General Assembly meets yearly before the start of the ENA Annual
Conference to determine official association policy and positions by reviewing,
debating and voting on proposed bylaws amendments and resolutions.
Bylaws amendments may be proposed by the board of directors, state
councils, association chapters or five active members of the association.
Resolutions may be submitted by any active ENA member. Others who may
submit resolutions include the ENA board of directors, state councils, chapters,
the Journal of Emergency Nursing editorial board and ENA committees.
The Resolutions Committee is available to help ENA members with
developing proposed bylaws amendments and resolutions. This assistance
provides members with the resources to effectively write proposed bylaws
amendments and resolutions in the proper format before the deadline. If you
are interested in bringing a proposed bylaws amendment or resolution to the
2013 General Assembly, it is recommended that you begin drafting your
proposal and working with the Resolutions Committee at least three months
before the submission deadline. Please contact ENA Component Relations at
[email protected] to obtain assistance from the Resolutions
Committee.
All proposed bylaws amendments and resolutions must be submitted in the
proper template form and must follow the format as outlined in the Resolutions
and Bylaw Guidelines. The guidelines may be found at www.ena.org in the
General Assembly area (members only). Final submissions must be e-mailed to
ENA headquarters at [email protected] by 5 p.m. CT, March 11,
2013.
Formal consideration of proposed bylaws amendments and resolutions will
occur at the 2013 General Assembly, Sept. 18-19, in Nashville, Tenn. This is
your opportunity to bring important professional emergency nursing issues to
the 2013 General Assembly.
ENA Call for…
Proposed Bylaws Amendments and ResolutionsSubmission Deadline: March 11, 2013
Nominations Committee ResponsibilitiesNominations Committee Member Election
Members will be elected to serve for a two-year term on the Nominations
Committee by geographic regions 2, 4, 6 and the past board member
position. The state breakout by region is available at www.ena.org/
about/elections/Documents/NomComRegionalMap.pdf.
The Nominations Committee is charged to do the following:
• To review, ratify and present a qualified slate of election candidates for
each position in the election of officers, directors and the Nominations
Committee.
• Review candidate applications for ENA national elections, according to
established policies and procedures.
• Encourage and mentor candidates throughout the election cycle.
• Conduct and facilitate the Candidates Election Forum for the Leadership
Conference 2013.
• Promote membership interest, education and voting participation.
• Provide a status report at ENA board of director meetings.
• Review and provide input on all policies and procedures related to the
elections process.
As we look to the future, ENA remains dedicated to strong leadership
among its members. The nominations process is one step to ensuring that
our national volunteer leaders are highly qualified and prepared for this
responsibility. The Nominations Committee encourages members to vote
in the 2013 election.
If you have questions or need assistance, please contact Executive
Services at 800-900-9659, ext. 4095, or e-mail [email protected].
Barry Hudson, BSN, RN, CPEN, immediate past president of the Texas ENA State Council, addresses the 2012 ENA General Assembly in San Diego.

October 201230
Thinking back
almost 25 years
since finishing my
nursing program, I never imagined doing
anything that would impact health care in
another country.
In 1999 there was an open call in ENA
Connection for members who had achieved
faculty status in TNCC or ENPC to submit a
letter for consideration to be a part of a team of
instructors that would take a course to another
country. The open call did not list where or
when the next course dissemination would
occur.
I remember sitting at my computer on a
Friday morning in November 2001, reading an
e-mail from ENA regarding bringing TNCC to
Portugal in February 2002. Before I hit the reply
key, I discussed with my wife traveling to
Europe in the era of post-9/11 and other
significant terrorist events. As much as this was
a concern, I felt the ability to teach TNCC in
Portugal would be a unique opportunity.
Since that trip, I have been fortunate to
return to Portugal to teach ENPC in 2006, and I
was the team leader for a 2010 trip to teach
TNCC in Korea. Over the last 10 years, TNCC
has spread to 14 countries and ENPC has spread
to six countries. This October, ENA will bring
TNCC to Kenya.
Trips to disseminate TNCC and ENPC are
filled with challenges and a lot of work. The
process starts with a request from the host
country to have either TNCC and/or ENPC
brought to them. The ENA national office has a
screening process for countries requesting the
courses, which validates nursing practice
standards and that the host country has the
infrastructure to maintain teaching either
TNCC and/or ENPC after the initial course
dissemination.
The basic schedule of a course dissemination
is to hold a provider course for 16 students. At
the end of the first course, the team of faculty
will select eight students who will then take the
first instructor course. These eight will then be
mentored and signed off as instructors, teaching
in the second provider course. The team of
faculty will then select four of the new
instructors to be mentored in teaching the
second instructor course. At the end of the trip,
the team of faculty will have taught two
provider courses for 32 students and two
instructor courses, making eight instructors, with
four of them signed off as faculty. This will
allow the course to continue to develop in the
host country. Since my first trip to Portugal in
2002, the Portuguese TNCC instructors have
since taught more than 100 TNCC courses.
Canada, the UK and Australia have very active
TNCC and ENPC programs.
Teaching internationally offers exciting,
memorable moments as well as challenges. On
Go Global With TNCC and ENPCBy Ray Bennett, BSN, RN, CEN, CFRN, CTRN, NREMT-P
A TNP station overseen by new TNCC instructors Maj. Eun-goung Ann and Lt. Col. Myoung-Ran Yoo in Daejeon, Korea, in August 2010.
Alzira Silva leads the scenario and Patricia Gaspar serves as the patient during a 6th edition TNCC instructor update in Oporto, Portugal, in April 2008.

Official Magazine of the Emergency Nurses Association 31
all three of my trips there have been obstacles,
such as translation issues, to overcome. In
preparing for our trip to Korea, we discovered
that they did not have rescue airways, such as
the Combi-tube or King Tubes, so we had to
pack these items. On all trips we found that
while understanding spoken English was
common for our international colleagues, using
English conversationally was not.
We spend approximately nine of the 15 days
on the ground teaching. These are long days,
often lasting 10 hours, in addition to evening
preparation meetings. However, each trip allows
for some down time to explore the host country
and socialize with our new international
colleagues.
As I reflect on each of my three trips, I feel
lucky to have had the opportunity to provide
trauma and pediatric nursing education, which in
turn will improve the quality of health care being
provided in emergency departments around the
globe. E-mail and social networking sites allow
me to maintain contact with my international
colleagues, who are now great friends with
commons goals.
This fall, ENA will post another open call for
TNCC and ENPC faculty for future international
dissemination trips. Even though ENA does not
have any definitive countries requesting a trip
at this time, the organization would like to
maintain a current database of members who are
interested in improving the quality of health care
around the world. I encourage ENA members to
apply. The memories will last a lifetime.
You likely have been in this situation: You notice when checking your
social media channel of choice that one of your friends or colleagues has
posted something questionable. How do you react? It’s a tough situation,
to be sure, especially given the instantaneous nature of social media.
This is the reason that social media policy has become so vital for many
organizations, hospitals and companies.
The pace at which social media networks are growing is
unprecedented, and there are increasing ways for not just text but
multimedia to be shared. Consequently, one of the best strategies is to
create a policy that is specific in its expectations and corresponding
penalties that are applicable to all situations. It’s not so much that policies
need to be reinvented for this technology, but expounded upon to capture
the very nature of what that technology allows its user to do.
Beyond an organization standpoint, a personal level of self-policing
measures can go a long way. The first and most important is to never
share anything with a social media outlet that you wouldn’t want shared
with everyone in your organization. While this may seem to be common
sense, there are a surprising number of cases where those very actions
have occurred with disastrous results.
Another proactive way to maintain privacy, and one that has become
increasingly popular, is simply keeping a private profile that’s completely
separate from your public, or professional, profile. That allows a certain
degree of freedom, though there is still risk in anything that gets
published online.
Because of all of these factors, it is impossible to say one policy works
better than another. However, the best thing that anyone can do is to
always be mindful of what is posted; and if you have clear consequences
in place for those who violate terms, ensure that quick and decisive
actions take place.
As this is a constantly evolving issue, I would be interested in hearing
what you are doing personally or within your organization in terms of
social media policy. There is no right or wrong approach, and it is always
fascinating to hear what else is out there.
Send your feedback to [email protected] or post on the ENA
Facebook page (www.facebook.com/enaorg).
ENA Connected
By Thomas Barbee, ENA Digital Marketing Manager
If this article described something that would interest you, watch for an e-mail – “Call for
TNCC/ENPC Faculty” – coming from ENA in late 2012, asking for TNCC/ENPC faculty who are
interested in participating in an international dissemination.
Ray Bennett presents the SHOCK lecture in Daejeon, Korea, with Taehoon Park assisting with translation.
How Sound Is Your Social Media Policy?

WASHINGTON WATCH | Kathleen Ream, MBA, BA, Director, ENA Government Affairs
In March 2006, the Emergency Nurses Association, along
with the American College of Emergency Physicians, urged
the Senate to exclude Section 202 of H.R. 4437, the Border
Protection, Antiterrorism, and Illegal Immigration Control
Act of 2005, from any bill that was passed on this issue. In
a letter dated March 28, 2006, the two organizations stated
that the language in this section could inadvertently place
emergency nurses and physicians and their hospitals in
untenable positions while attempting to comply with
existing federal laws, primarily EMTALA.
If it had been included in the final bill, which it wasn’t,
Section 202 of H.R. 4437 would have expanded current
immigration law by criminalizing anyone who attempted
to provide “assistance” or “harbored” an illegal immigrant.
ENA and ACEP noted in their letter that providing needed
and legally required health care to an illegal alien could
meet this definition and, thereby, criminalize the care
provided by emergency nurses and doctors.
Six years have passed and emergency personnel are
still faced with immigration legislation that may put
them in untenable positions.
In 2012, America’s attention was focused
on the Supreme Court’s review of Arizona’s SB
1070 immigration law. What many Americans
didn’t know was that other immigration bills
had also worked their way through the
Arizona legislature in 2012. Of particular
importance to emergency department health
care providers was a bill requiring EDs or
hospitals to report illegal immigrants.
SB 1445 stated, ‘‘If a person who
seeks or is receiving emergency or
nonemergency care at a hospital
cannot provide valid health insur-
ance information, the hospital
admissions officer or representative
must reasonably confirm during the
course of the person’s admission or
treatment that the person is a citizen
of the United States, a legal resident of
the United States or lawfully present
in the United States.’’
According to the bill,
if the hospital/ED cannot
confirm legality, it must
immediately contact immi-
gration or law enforcement.
The hospital also would be
required to annually submit
a report on the number of
patients seen who did not
show proper valid informa-
tion and the number of calls
made to immigration or law
enforcement. This bill was
assigned for review to three committees in the legislature:
Health Care and Liability Reform, Government Reform and
Rules. It died in committee (www.azleg.gov, 2012).
The U.S. Department of Homeland Security estimates
that there are 11.5 million illegal immigrants in the United
States.1 In 2009, Modern Healthcare noted that at least one
third of all immigrants lack health care.2 Among Mexican
immigrants, this number is even higher, with an equal or
greater-than-50-percent uninsured rate. Arizona is one of
seven states with the highest illegal immigrant population.
The others are California, Texas, New York, Florida,
Illinois and New Jersey.
Undocumented immigrants tend to use the emergency
department more often than all other uninsured patients.3
The ED is a safety net for all the underinsured and unin-
sured, required by the Emergency Medical Transport and
Labor Act to provide evaluation and emergency care to all
who enter the facility (www.ena.org/government/
emtala/Pages/Default.aspx).
As professional nurses, we are advocates for safe,
competent, available emergency care for our patients.
Certainly, we have multiple reporting requirements in our
practice. A myriad of state and federal regulations requires
us to report child and adult abuse, sexual assault, animal
bites, knife and gun wounds and burns, for example. All
of these are meant to protect patients and society. It
should not be a part of our practice to be responsible for
immigration enforcement.
As emergency nurses, we need to take responsibility for
our profession and our practice. It is imperative that nurses
do not remain legislatively illiterate. We are leaders and
advocates for those who need us most. Become aware of
the bills in your state and have a strong voice on issues.
The Emergency Nurses Association and the ENA Govern-
ment Affairs Committee are here to help you.
As Margaret Mead said, ‘‘Never doubt that a small group
of thoughtful, committed citizens can change the world.
Indeed, it is the only thing that ever has.’’
References
1. United States Department of Homeland Security. (2012).
Statistics. Retrieved July 6, 2012, from www.dhs.gov/
index.shtm.
2. Carlson, J. (2009). Immigrants are missing quotient in
reform talks. Modern Healthcare, 39(25), 18.
3. American College of Emergency Physicians. (2012).
Illegal immigrant care in the emergency department.
Retrieved July 6, 2012, from www.acep.org/content.
aspx?id25206.
Article by Rita Anderson, RN, CEN, FAEN, ENA Government Affairs
Massachusetts ED Costs Increase DramaticallyA new report finds that unnecessary ED costs in
Massachusetts have gone up by about 35 percent, or
nearly $150 million between FY 2006 and 2010. The
From the States
October 201232
Be Alert for State Legislation Impacting ED Nursing Practice

Division of Health Care Finance and Policy report
found there were nearly 2.5 million ED visits in
FY 2010, and about half those visits were
preventable or avoidable.
State lawmakers say that they expect the costs
to go down. The Senate’s Health Care Financing
Committee Chairman, Richard Moore, says the state’s
new health care law will promote access to primary
care doctors and reduce ED visits.
Despite increasing costs, the report found that the
number of ED visits is decreasing. It also recommends
that there should be a greater availability of health
care services to reduce unnecessary costs.
Massachusetts Law Includes Ban on Mandatory OvertimeOn Aug. 6, Massachusetts Gov. Deval Patrick (D)
signed into law the state’s much-anticipated health
care cost containment bill – SB 2400 – that includes
a ban on mandatory overtime for RNs. Under the
new law’s provision banning mandatory overtime,
a hospital cannot, except in the case of a declared
emergency, require a nurse to work beyond his or
her scheduled shift, and no nurse can be required
to work more than 12 hours in a 24-hour period.
Hospitals that assign a mandatory overtime shift are
required to report those incidents to the
Massachusetts Department of Public Health, along
with the justification for its use. Any nurse can
refuse overtime without fear of retribution or
discipline of any kind from his or her employer.
A number of scientific studies published in the
last decade have documented the dangers and costs
of mandatory overtime. The studies included
findings that nurses working mandatory overtime are
three times more likely to make costly medical
errors, and that such overtime was associated with
an increased risk of catheter-related urinary tract
infections and bedsores, both preventable medical
complications. In addition, a report issued by the
Institute of Medicine in 2002 linked mandatory
overtime and the under-staffing of nurses to
thousands of patient deaths each year, and called
for prohibition of the practice.
Official Magazine of the Emergency Nurses Association 33
ENA wishes to express its sincere gratitude to these 2012 sponsors.* Thanks to their generous support, ENA is able to continue to provide relevant
services and educational programs to improve your practice of emergency nursing.
Strategic Sponsors
Strategic Supporters
Conference Sponsor
*As of print time
Conference Supporter

October 201234
We are all back at work after being
professionally refreshed, revitalized
and invigorated at the 2012 ENA
Annual Conference in San Diego.
The 1st Annual Awards Gala was a
wonderful way to conclude our time
in sunny California. Terry Foster, MSN,
RN, CEN, CCRN, FAEN was an excellent master
of ceremonies as we welcomed our eighth class
of fellows into the Academy of Emergency
Nursing.
Now is the time for our 2013 class of fellows
to start preparing their application for admission
into the AEN. Will you be in the ninth class of
inductees? Information and applications are
now available at www.ena.org under “Calls
and Opportunities.” The deadline to submit
online applications is 5 p.m. (CT) on Friday,
Nov. 30, 2012.
Are You Ready to Apply?One criterion for admission into the AEN
requires substantial and enduring contributions
to the emergency nursing profession.
Contributions and impact can be in broad
categories of practice, education, research,
leadership and/or public policy. This requires
being active not only on the local level but also
on the regional, national and/or international
level as well. Have you been an active member
of ENA for the last three consecutive years
without any gaps in membership? (International
applicants must be ENA members for one year
and members in their country’s emergency
nurses association for the last three consecutive
years.) Has your substantial and enduring
contribution made a significant impact on
emergency nursing? Is your curriculum vitae
current and, most important, does it reflect your
significant contributions to our profession?
Another criterion requires potential for future
contributions. Admission into the AEN truly
honors your impact on the profession. Moving
forward as a fellow, you will be called upon to
freely share your expertise with ENA and its
members.
Have you cultivated two sponsors? One
sponsor must be a current fellow of the AEN. If
you do not know a current fellow, there are
ways to meet and work with one. Fellows are
active on national ENA committees and in all
areas of practice. Consider applying for the
EMINENCE mentoring program, where you are
paired with a fellow to work on your project of
choice. Network with fellows at national
conferences. It is often so surprising to discover
that your clinical problem is a national clinical
problem, and there are fellows who can
collaborate with you or guide you to new
heights.
In these times of economic hardship, it
would be remiss not to mention financial
readiness. The AEN budget is maintained by
fellow annual dues and ENA. To be a fellow in
good standing requires maintaining membership
in ENA and paying annual AEN dues (currently
$100). You might want to consider lifetime
memberships in both.
The Academy of Emergency Nursing’s ninth
inductee class will be required to attend the
induction in Nashville, Tenn., during the 2013
ENA Annual Conference. Inductees’ presence
also is requested at AEN annual business
meetings held in conjunction with the ENA
Annual Conference.
If after some consideration you have
discovered that your body of work as an
emergency nurse has been substantial and
enduring with a significant impact, you have a
plan for potential future contributions and you
have two sponsors who know your work, this
may be the year for your application. The
following are some tips to help you realize your
professional goal as you complete the
application process:
DeadlinesBe aware of the deadlines. Communicate these
deadlines to your sponsors. Allow yourself
enough time to write, rewrite and edit a
thoughtful statement. Fall is a busy time of year
for everyone. Do not expect your sponsors to
drop everything to meet a short deadline. Your
poor planning does not create an emergency for
your sponsors.
Content and Word LimitsBe aware of the word limits for each section:
• Criterion 1, Active Involvement –
400-word limit
• Criterion 2, Enduring and
Substantial Contributions –
750-word limit
• Criterion 3, Potential for Sustained
Contributions – 300-word limit
Do not exceed word limits. Your application
and two letters of support are the only materials
used to determine eligibility. Even if your
contributions are known but not included in the
statements, they cannot be considered.
Proofread your application. Have an
uninterested party proofread it as well. In this
day of abbreviated e-mail messages, it is easy to
omit a verb or noun or include an incomplete
sentence. Be sure spelling and grammar are
correct and use correct punctuation.
Criterion 3, Potential for Sustained ContributionsPay special attention to this section. Rather than
restate items from the enduring and substantial
contributions statement, outline clear and
attainable goals that demonstrate how you will
impact the future of emergency nursing. Future
contributions can be made in the areas of
practice, education, research, leadership or
public policy.
SponsorsSponsors should be individuals who know you
and your professional contributions. Share your
criterion statements with your sponsors so their
statements enhance and highlight the impact of
your contributions. Letters of support should
speak to these items and not simply restate your
three criterion statements. Make the most of
your statements so your AEN reviewer can truly
understand why you are an excellent candidate.
Before You Hit Send• Did you follow the application instructions?
• Did you e-mail your CV separately?
• Have you budgeted money to attend the 2013
ENA Annual Conference in Nashville?
By keeping these tips in mind, you will avoid
common pitfalls that can derail a worthy
application to the Academy of Emergency
Nursing. As a current fellow and member of the
Academy Board, I look forward to welcoming
you among the ninth class of inductees.
Tips for a Successful Application to the Academy of Emergency NursingBy Maureen Curtis Cooper, BSN, RN, CPEN, CEN, FAEN AEN Board Member at Large, Academy of Emergency Nursing

Official Magazine of the Emergency Nurses Association 35
The ENA Nominations Committee is the
only committee elected by the ENA member-
ship. While the committee members are very
visible during election time, especially at the
Candidates’ Election Forum at Leadership
Conference, the members continue working
on the election process throughout the year.
In fact, as soon as one election is completed
in mid-June, the committee begins working on
the next election, said Louise Hummel, MSN,
RN, CEN, CNS, 2012-2013 Nominations
Committee chairperson.
“I don’t know if the membership under-
stands what goes on behind the scenes,” said
Hummel, as she prepared to attend the 2012
General Assembly, where the committee was
presenting bylaws amendment proposals to
the delegates gathered in San Diego. “We’re
reviewing candidate applications; we work
with the candidates to help them prepare for
the forum; and each candidate has a
committee member assigned to him or her,
and that person acts as the intermediary
throughout the election process.”
Monthly – or even more frequent – confer-
ence calls are just part of the committee’s
ongoing commitments. Prior to writing and
submitting proposed bylaws amendment(s) to
the General Assembly for consideration,
committee members must review current
election rules and conduct necessary research.
The committee looks at election candidate
applications for completeness, which includes
verifying that each candidate’s membership is
current and that the candidate has the qualifi-
cations to run for ENA office, said Hummel.
The Nominations Committee also has the
responsibility for writing the questions the
candidates will answer at the Candidates’
Election Forum, which is held annually at
Leadership Conference.
“We write questions that are specific to the
president-elect, questions that are specific to the
secretary/treasurer and questions that are
specific to the director candidates,” said
Hummel.
In deciding which topics to cover in their
questions for the various candidates, Hummel
said the Nominations Committee considers
current issues in emergency nursing, hot topics
in the association, as well as national trends in
the practice. The committee also solicits
questions from the audience via a questionnaire
distributed during the Candidates’ Election
Forum for consideration in using at the next
year’s forum.
“We ask the audience what they would like
to hear addressed by the candidates, and then
we compile them, look them over and say,
‘Maybe this would make a good question for
next year,’” said Hummel. “We may tweak it a
little bit, but we enjoy taking suggestions from
the membership, because they are voting for
their future leaders. We want to be able to find
out what issues they want addressed.”
The Nominations Committee – which
increased its visibility with a new badge holder
ribbon at the 2012 Annual Conference in San
Diego last month – has been working tirelessly
to improve the voting turnout for the ENA
national election. Hummel was thrilled when
the election results jumped an entire percent-
age point this year. She credits several reasons,
including moving to an all-electronic ballot
and broadcast e-mails sent to remind members
to vote as well as e-mails highlighting the
election candidates.
“We are always open to suggestions from
the membership,” said Hummel, adding that
members can contact the committee at
Hummel also thanked the dedicated
Nominations Committee members whose
terms of service recently ended: Gail Carroll,
BSN, RN, CEN, and Carlene Kincaid, BSN, RN,
CEN.
The Nominations Committee’s responsibili-
ties include but are not limited to the
following:
1. Conduct a fair and equitable national
election, including the review of all
candidate applications and ratifying the slate
of candidates according to established ENA
bylaws, policies and procedures.
2. Review and update election rules and
procedures as needed.
3. Collaborate with staff to investigate ideas
and invest in methods that may promote
greater voter interest, visibility of candidates,
exchange of information and participation
in the election process.
4. Review and update the national candidate
application for content, ease of use and
effectiveness and assist potential candidates
throughout the election cycle.
5. Plan, promote and facilitate the 2013 Candi-
dates’ Election Forum at the annual
Leadership Conference.
6. Provide progress reports to the ENA Board of
Directors throughout the year.
ENA Nominations Committee: The Work Doesn’t End After the Votes Are TalliedBy Amy Carpenter Aquino, ENA Connection
Louise Hummel, MSN, RN, CEN, CNS Chairperson
Region 1
Cathy C. Fox, RN, CEN, CPEN Region 4
Ellen E. Ruja, MSN, RN, CEN, FAEN Region 6
Terry M. Foster, MSN, RN, CEN, CCRN, FAEN Region 3
Lucinda W. Rossoll, MSN, RN, CEN, CPEN, CCRN Region 5
Tiffiny Strever, BSN, RN, CENPast ENA Board Member
Scott E. Stover, MSN, MBA, ACNS-BC, CENRegion 2

October 201236
The ENA Foundation would like to extend a special thank you
to the individuals, state councils, local chapters, industry and
friends of emergency nursing who have supported the profession
through their generous donations. Because of your contributions and
passion to promote the advancement of the profession, our applicants are
afforded the opportunity to receive educational scholarships and research
grants in the discipline of emergency nursing.
The ENA Foundation is excited to announce the following 2012
scholarship and research grant recipients and share how our donors
are making a difference:
Academic Scholarship RecipientsNon-RN Scholarships• California State Council – Bryan Stow Scholarship – $5,000
Nathan Dreesmann, EMT – Washington
• New York State ENA September 11 Scholarships – $2,500 each
Khristeen Sproul, EMT – New York
Jon Manzano, NREMT-B – California
• ENA Foundation Non-RN State Challenge Scholarships –
$2,500 each
Deya Montalvo, EMT-B, Paramedic – California
Dana Johnson, EMT-B – Colorado
Matthew Onofrio, NREMT-P – Iowa
Jillian Conley, EMT-B – New Jersey
Undergraduate Scholarships• Charles Kunz Memorial Undergraduate Scholarship – $3,000
Rita Anderson, RN, CEN – Arizona
• Betty J. Smith, RN (Lt. Army Nurses Corps, WWII) Memorial
Scholarship – $3,000
Mark J. Smith, RN, CEN – North Carolina
• Board of Certification for Emergency Nursing (BCEN)
Scholarship – $3,000
Adam Bruhn, RN, CEN – Nebraska
Graduate Scholarships• Stryker Masters in Healthcare Scholarship – $5,000
Kristen Connor, BSN, RN, CEN, PHRN – California
• Board of Certification for Emergency Nursing (BCEN)
Masters in Healthcare Scholarship – $5,000
Cheyenne Brown, BS, RN, CEN – Utah
• AnnMarie Papa Stretcherside Miracle Scholarship – $5,000
Kimberly Johnson, BSN, RN – Michigan
• Board of Certification for Emergency Nursing (BCEN)
Scholarships – $5,000 each
Diane Blackman, BSN, RN, CEN – Pennsylvania
Joyce Fuss, BSN, RN, CEN, CPEN – Indiana
Jonathan Green, BSN, RN, CEN, CCRN – New York
Lynn Sayre Visser, BSN, RN, CEN, CPEN – California
• Colorado State Council – Colorado Rocky Mountain
Scholarship – $5,000
Cindi Warburton, BSN, RN, CEN – Oregon
• Kentucky State Council – Kentucky ENA Founders
Scholarship – $5,000
Dawn McKeown, BSN, RN, CEN, CPEN – Louisiana
• Maryland State Council – Maryland ENA State Council
Scholarship – $5,000
Megan Doede, BSN, RN, CEN – Maryland
• Minnesota State Council – “Pathways IV” Scholarship – $5,000
Mary Jagim, BSN, RN, CEN, FAEN – North Dakota
• Mississippi State Council – Sonja O. Adkins Mississippi State
Scholarship – $5,000
Jennifer Denno, BSN, RN, CEN – California
• New Jersey State Council – Emergency Care Scholarship – $5,000
John R. Stott II, BSN, RN, CEN, CPEN – New Jersey
• New Jersey State Council – New Jersey State Challenge
Scholarship – $5,000
Julie Ann Dale, MSN, RN, CEN – Missouri
• Northern Chapter (NJ) – Mary Kamienski Scholarship – $5,000
Dawn M. Sullivan Wright, BSN, RN, CEN – Indiana
• West Central Chapter (NJ) – Jeanette Ash Scholarship – $5,000
Jill McLaughlin, BSN, RN, CEN – New York
• South Carolina State Council – Antoinette Ruff-Johnson Memorial
Scholarship – $5,000
Kathy Van Dusen, BSN, RN, CEN – California
• Tennessee State Council – Tennessee State Challenge
Scholarship – $5,000
Kylie Kersten, BSN, RN – Arizona
• Texas State Challenge – Vicki Patrick Legacy Scholarship – $5,000
Tiffany Young, BSN, RN – North Carolina
• ENA Foundation Graduate State Challenge Scholarship – $5,000
Jennifer Lechota, BSN, RN – Michigan
• Board of Certification for Emergency Nursing (BCEN)
Scholarship – $4,000
Reagan Norman, BSN, RN, CEN – Indiana
• Physio-Control, Inc. Scholarships – $3,000 each
Nancy Alexander, BSN, RN, CEN – Ohio
Andrew W. McLuckie, BSN, RN, CEN, CPEN, CCRN – Pennsylvania
• Gisness Advance Practice Scholarship – $3,000
Terry Stigdon, BSN, RN, CPEN – Indiana
• Karen O’Neil Memorial Scholarship - $3,000
Theresa Sexton, RN, CEN – Massachusetts
• ENA Foundation State Challenge Scholarships – $3,000 each
Amanda Brothwell, BSN, RN, CEN, CPEN – Nevada
Lori L. Carlen, BSN, RN, CEN – Nebraska
Theresa Del Biondo, RN – Pennsylvania
Jenna Hannity, BSN, RN, CEN – Washington
Ruth Keniston, RN – California
Rachael M. Young, BSN, RN, CEN – Illinois
Katie Zielinski, BSN, RN – California
2012 Scholarship and Research Grant Recipients

Official Magazine of the Emergency Nurses Association 37
Doctoral Scholarships• Pamela Stinson Kidd Memorial Doctoral Scholarship – $10,000
Laura E. Gallagher, MSN, RN, CNS, CEN – South Carolina
• Board of Certification for Emergency Nursing (BCEN) Doctoral
Scholarships – $5,000 each
Linda Roney, MSN, RN-BC, CPEN – Connecticut
Jennifer Williams, PhDc, RN, ACNS-BC, CEN – Missouri
• Hill-Rom Doctoral Scholarships –
$4,000 each
Kayla Thompson, BSN, RN, CEN – North Dakota
Patti Van Auker, MSN, RN, CEN – New York
Continuing Education Scholarship Recipients• Vidacare Annual Conference Scholarships – $500 each
Janice Alley, RN, CEN – Virginia
J. Richard Beshore, BSN, RN – California
Brandon “Kit” Bredimus, BSN, RN, CEN, CPEN – Texas
Teresa Brunt, RN – Utah
Kaleigh Byrne, BSN, RN – Virginia
Jenny Edmonds, EN, RN – United Kingdom
John Fraleigh, BSN, RN, CFRN – Arizona
Peter Giordano, BSN, RN – Illinois
Crista Jimenez, BSN, RN, CEN – Florida
Sherri Mimbs, RN – Florida
Andrea Rich, BSN, RN, CEN, CFRN – Arizona
Shannon Mazza Roberson, BSN, RN, CPEN – North Carolina
Deborah Robichaux, RN, CEN, CCRN – Georgia
Laura St. Clair, MA, BSN, RN – Wyoming
Jeanne Venella, DNP, MS, RN, CEN, CPEN – New Jersey
Michael Zonak, RN – New Jersey
Research Grant Recipients• ENA Foundation / Sigma Theta Tau International Research Grant
– $6,000
Jessica Draughon, MSN, RN – Maryland
• ENA Foundation / Sigma Theta Tau International Research Grant
– $3,000
Mary Johansen, PhD, NE-BC, RN – New Jersey
• Industry Supported Research Grant – Supported by Stryker – $5,000
Recipient not selected as of press time.
As a donor, you can make a difference in the future of emergency
nursing. Your donation will help to provide funding for research that can
improve the quality of patient care, build future leaders, support education
that can change the practice of medicine in the future and much more. If
you would like to join others in making a difference in emergency
nursing, the ENA Foundation has opportunities. Please visit
www.enafoundation.org to find out how you can contribute to
advancing emergency nursing.
With the ever-changing landscape of our
members who are becoming more
technologically savvy, ENA has listened by
putting the Conference Program for Leadership
Conference 2013 online at www.ena.org/lc.
Traditionally, we have
mailed out the Conference
Program with the October
issue of ENA Connection,
but by putting the program
online, you are guaranteed
to have the Conference
Program at your fingertips 24/7. This also
allows us to make the latest updates to the
program anytime, day or night.
Besides putting the Conference Program
online, we are also refreshing and updating the
look and feel of the program for a better
overall read. We are boiling over with
excitement about the new Conference Program
and we want to share some of those new
features, such as:
• Bulleted copy – For more detailed and
precise course information with more focus
on the objective of the course.
• Easier read – More course listings on a page
which will help you determine which
courses to take. This allows us to have fewer
pages in a more condensed format.
• Schedule-at-a-Glance – Think ‘‘TV Guide’’
format: better visual with side-by-side
information on when and where education
sessions and special events occur.
• Social media – A much larger social media
presence for not only ENA but to follow
keynote speakers, etc.
• Much more!
We could not be prouder of the
accomplishments we made this past year at
our Leadership and Annual conferences, but
there is much more work to be done to make
2013 even better. We hope you enjoy this
digital Conference Program.
Leadership Conference 2013 Conference Program Is Going Digital

October 201238
Arizona ENA State CouncilSubmitted by Tomi St. Mars, MSN, RN, CEN, FAEN
One of the many challenges that emergency nurses face on a daily basis
surrounds the management of pain for patients coming to the emergency
department. The patient with chronic pain is especially challenging for
emergency physicians and nurses alike. The ED is not the best environment
to fully assess, diagnose or provide definitive pain management.
Recently, AZ ENA representatives attended a collaborative, one-day
forum to discuss the scope of the problem, barriers in proper management,
standards of care and the resources in place to monitor ED prescription
drug use. The goal is to develop statewide guidelines for care of the
chronic pain patient and increase prescriber participation with the
prescription drug monitoring program. Currently, only 15.6 percent of all
prescribers are registered to use the system.
The July 18 forum was organized by the Arizona Department of Health
Services and provided representation from more than 60 health care
providers, which included ACEP, the Board of Pharmacy, AZENA, AHCCCS
(Arizona Medicaid), Indian Health Services, behavioral health organizations,
nursing and executive management from hospital systems throughout
Arizona, as well as DEA enforcement personnel. This collaborative activity
began with two emergency physicians recognizing a problem, developing
a program and providing insight to the implementation program currently
in use at one hospital system. Through education, a spark has ignited. One
such presentation to the AZENA membership in January 2012 grew to
include the forum in July and a proposed resolution presented at the ENA
General Assembly in September.
Florida ENA State CouncilSubmitted by Pattie Stadler, MS, BSN, RN, CEN, CCRN,
and Terri McGowan-Repasky, MSN, RN, CNS, CEN
Leading by Example
Every new year brings an opportunity to develop and grow strong leaders
within our organization. In the spring, the Florida Emergency Nurses
Association Executive Committee presented our Chapter Leaders
Orientation program. Chapter leaders from around the state were invited.
Florida is a three-tier state with 16 chapters. Two leaders from every
chapter were invited to attend the all-day workshop.
Topics included the following:
• Overview of ENA and FENA, including responsibilities of GA delegates
• Chapter Management/Responsibilities and Strategic Planning
• Responsibilities of Treasurer (chapter and state)
• Responsibilities of Secretary (chapter and state)
• Government Affairs and Resources
• Overview of ENA and FENA websites
This day offered more than just education; it provided an opportunity
to network and put faces and names together. State leaders had the
opportunity to meet and exchange ideas with the executive team in
a comfortable setting.
Florida: Manasota ChapterSubmitted by Jennifer Sweeney, MSN, BA, RN, CEN
On May 10, the Manasota Chapter of the Florida ENA State Council
co-provided the 2012 Nurses’ Week Research Conference with Sarasota
Memorial Healthcare System in Sarasota, Fla. The theme of the conference
was ‘‘The Power to Change Using Research.’’ This event brought together
nurses from all over the west coast of Florida to celebrate the value of
evidence-driven professional nursing practice. The event included
presentations from several nationally recognized speakers, as well as 14
poster presentations from local nurses who have made a meaningful
impact on professional nursing practice through the implementation of
evidence-based initiatives.
Poster presentations
highlighted evidence-based
projects, including the use of
high-fidelity simulation to
enhance ACLS team training,
Neonatal Abstinence Syndrome,
Preventing Falls, Emergency Obstetric ACLS skills, nursing knowledge of
geriatric-specific issues in acute care, and more. The Manasota Chapter was
thrilled to have the opportunity to collaborate with Sarasota Memorial
Health Care system in this highly successful professional nursing event. In
total, more than 50 nurses from all over the southwest Florida area joined
us in celebrating and supporting the value of evidence-based nursing
practice. We look forward to an even larger event in 2013.
North Carolina ENA State CouncilSubmitted by Mary Lou Forster Resch, BSN, RN, CEN
North Carolina had a great time in San Diego. We are honored and proud
to have had a voice in the decision-making process of our professional
organization. Thanks to everyone who stopped by our fundraising booth
and supported our endeavors.
Our membership blitz ran Sept. 1-30. We will award a free ENA
membership to the nurse who recruited the most new members.
We invite you all to Wrightsville Beach on Nov. 9 for our 8th Annual Fall
Conference. The planned presession is an ENPC Instructor Course, which we
hope to present at a very affordable fee. We have borrowed the ‘‘pay it
forward’’ concept from Leadership Conference and incorporated it into our
State of the State presentation. For more information, visit www.nc-ena.com.
Texas ENA State CouncilSubmitted by Christine Russe, MSN, RN, CEN, CPEN
The TENA Nursing Practice Committee was charged in 2012 with
submitting two position statements:
1 - Position Statement: Social Networking (statement addresses social
networking and potential privacy issues in the emergency care setting).
2 - Position Statement: Wireless Telecommunication Devices (statement
addresses any device that makes or receives phones calls, leaves
messages, sends text messages, capable of browsing the internet, or
downloads and allows for the reading of and responding to e-mail).
These ratified position statements were presented to and unanimously
approved by the TENA State Council on July 14.
These two Texas ENA position statements are a first for the Texas ENA.
They are the results of more than two years of diligent work by the Texas
ENA Nursing Practice Committee. The TENA Nursing Practice Committee
plans to provide additional position statements in the future. Thank you to
everyone who contributed to these TENA statements. These new TENA
position statements will soon be posted at www.txena.org. A Nurse’s
Guide to the Use of Social Media pamphlet by National Council of State
Board of Nursing was also disseminated to attending members. If you are
ENA STATE CONNECTION
Manasota (Florida) Chapter members Maribeth Desiongco, MA, RN-BC (left) and Jennifer Sweeney, MSN, RN, CEN, present the poster “A Hybrid Program Utilizing Heart Code ACLS & BLS with Simulation to Validate Competency.”

Official Magazine of the Emergency Nurses Association 39
interested, additional copies may be obtained
free from NCSBN website.
Submitted by Rhonda Manor-Coombes,
BSN, RN
On July 14, the Texas ENA 3rd Quarter State
Council Meeting was held in Lubbock, Texas,
with two members attending the meeting via
WebEx. As press secretary/media chair, I was
charged with making participation possible for
those members unable to attend a state council
meeting.
WebEx is a Web conferencing tool that
combines desktop sharing via Web browsing and
phone conferencing. The only need is a
computer and reliable Internet access. I was able
to share my documents with the attendees after
they logged in. I could intermittently send chat
messages to the attendees to make sure that they
were still participating. The attendees were also
able to send me questions or comments that I
would then share with the council and delegates.
Monitoring participation is crucial, especially if
the member is to receive credit for attending a
state quarterly meeting. The only issue was
sound quality. While the attendees were able to
hear using a USB microphone I had attached to
my computer, they had a hard time hearing those
members who spoke softly.
One of ENA’s Strategic Plan priorities is to
expand and fortify ENA’s membership. I truly
believe that with remote access, this can be
accomplished. All in all, I would say that this
was a success. The idea of members remotely
accessing the meeting is a huge step and a
benefit for our members.
Virginia ENA State CouncilSubmitted by Janice McKay, RN, CEN, CFRN
Emergency department nurses see the
consequences of alcohol-related crashes, the
loss of life or crippling injuries and are in favor
of methods to decrease and prevent alcohol-
related crashes. Members of the Virginia State
Council were asked to support the House Bill
279 and Senate Bill 378 and contact their state
legislators to have these bills passed to prevent
drunk driving in Virginia.
Effective July 1, first-time driving-under-the-
influence offenders in Virginia may be
mandated by the court to have an ignition
interlock device installed in their vehicle for
resumption of driving privileges. Previously, the
law was a fine no less than $250, jail time and
suspension of their driving license for a year,
with stricter penalties determined by the blood
alcohol content of the offender. The ignition
interlock system was used as an option for
second-time offenders but is now required by
the court. Currently, 15 states have laws
mandating the use of interlock systems for
first-time convictions, and now Virginia joins
these states.
The ignition interlock system is used to limit
drunk driving since it has been documented that
DUI offenders will continue to drive under the
influence. The ignition interlock device requires
the driver to take an alcohol breath test every
time he or she gets behind the wheel, and it will
also do random tests or ‘‘rolling retest’’ while
driving to ensure the driver isn’t drinking while
driving. These devices are more effective than
license suspension because DUI offenders will
continue to drive under a suspended license.
Studies have shown that states using the ignition
interlock system can decrease DUIs by 66 percent.
Linda Whitt, BSN, RN, CEN, an emergency
nurse of more than 40 years, has seen the
consequences of driving under the influence
and the tragedies from alcohol-related crashes;
knowing her mother was an offender of
drinking and driving, she had an ignition
interlock device placed in her mother’s vehicle.
Whitt believes this device works and said, ‘‘I am
happy to say that she never hurt anyone
because I had the ignition interlock device
installed on her car to keep her from being able
to start the car while intoxicated.’’ Whitt said
she would not have been able to live with
herself if something happened while her mother
was driving under the influence, knowing she
had a problem and didn’t do anything about it.
Virginia’s goal is to decrease the number of
alcohol-related crashes and fatalities. Although
these have decreased over the years, the
ignition interlock can prevent more lives from
being lost in senseless crashes from DUIs.
Statistics from the Virginia Department of Motor
Vehicles and the Virginia Highway Safety Office
for 2011 reports that Virginia had more than
8,400 alcohol-related motor vehicle crashes
resulting in 245 fatalities and 5,465 injuries.
Although we won’t totally eliminate driving
under the influence, having a voice to decrease
DUI-related crashes by showing our support of
these bills acknowledges ENA’s mission in
injury prevention and saving lives.
New ENA monthly offering for FREE Continuing Education with contact hours for our members.
• Available October 1 – Improving the ED Flow 1.0 contact hour Barbara Weintraub, RN, MPH, MSN, APN, CEN, CPEN, FAEN
Don’t miss out on enhancing your education. Go to www.ena.org/FreeCE for additional free continuing education opportunites.
The Emergency Nurses Association is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.

October 201240
2012 Lantern Recipients Continued from page 27
ENPC 4th Edition Instructor Update
the beginning of care; however it can be
requested at any time, by anyone on the
treatment team. Performing a shared mental
model keeps the team grounded, allowing for
focus on the primary needs of the patient and
allows staff to hone in on the plan, providing the
opportunity to contribute suggestions.
Indiana University Health Methodist Hospital Emergency Medicine and Trauma Center (Indianapolis)Indiana University Health Methodist Hospital
Emergency Medicine and Trauma Center is part
of a not-for-profit, Magnet-designated academic
medical center and has an annual census of
108,000 emergency patients. Forty-nine percent
of hospital admissions come through the ED.
Success in improving patient flow is
demonstrated by the fact that the emergency
department has no boarded patients. Through a
strong shared governance model, collaborative
decision-making and staff nurse autonomy were
utilized in developing evidence-based strategies to
solve barriers to throughput and patient
satisfaction.
As part of a throughput improvement project,
a multidisciplinary team was established to
develop an escalation plan that included senior
leadership. All nursing directors were educated
on the National ED Overcrowding Score.
Through review of their processes, they realized
the need for a new nursing position, director of
operations. New processes were developed
following a root cause analysis which revealed
bottlenecks and discharge barriers. Their analysis
also showed the need for an upgraded bed
tracking system to expedite and improve bed
turnaround time, length of stay and ED length of
stay. As a result of these initiatives, the ED
decision-to-admit to arrival-in-an-inpatient-bed
time has been reduced by two hours. In
addition, ED door-to-provider time has decreased
from 17 minutes to four minutes, and the LWBS
rate dropped from 2 to 1.3 percent.
ENA Lantern Award ProgramFor more information about the ENA Lantern
Award Program, please visit www.ena.org/
IQSIP/LANTERNAWARD/.
particularly important when
healthcare personnel are working
long hours or night shifts, as well
as in emergency situations, all of
which are associated with a
higher rate of NSIs. Furthermore,
passive devices eliminate the
need for intricate training. The
drawback of higher cost might
be offset by lesser training
requirements and by cost savings
associated with a reduction in
NSIs (eg, serological tests,
counseling, post-exposure
prophylaxis, time off work, and
treatment).’’ 3
These costs don’t even include
the cost of one nurse who
becomes infected with HIV or
hepatitis C, or the human toll. If
we take safety seriously, we need
to recognize that products that are
not passively designed and
require training put nurses at risk.
In this study, “passive devices
were associated with the lowest
NSI incidence rate. Among active
devices, those with a
semiautomatic safety feature
were significantly more effective
than those with a manually
activated toppling shield, which
in turn were significantly more
effective than those with a
manually activated sliding
Shield.”3
A syringe with a retractable
needle is one example of a
passive device. When the
plunger of the syringe is pushed
down to deliver medication, it
triggers the needle to
automatically retract from the
patient before it is pulled out. So,
in the end, there is no
contaminated needle to harm
anyone. The needle is
immediately and safely enclosed
in the syringe. This type of
syringe has been available for
years, and yet, is still not
standard in hospitals.
The prevention of sharp
injuries and resulting illnesses
should begin long before nurses
hold a device in their hands.
Manufacturers have a need and a
responsibility to make devices
that are truly safe. Emergency
nurses are at special risk. They
deserve the same robust
protection that the public and
industry enjoy.
Letter From the President Continued from page 3
Board Meeting Actions and HighlightsThe ENA Board of Directors met July 18 via teleconference. All board
members were present and took the following actions:
• Approved the June 21 board of directors meeting minutes as written.
• Approved the Leadership Conference 2013 budget as presented.
• Approved a request to support the American College of Emergency
Physicians’ clinical policy: Critical Issues in the Prescribing of Opioids
for Adult Patients in the Emergency Department.
• Referred board governance policy 3.14, Board of Directors Stipends,
back to the Governance Committee.
• Approved a restructure of ENA committees as amended.
• Approved the following actions related to Trauma Nursing Core Course
and Emergency Nursing Pediatric Course Reverification as presented.
° TNCC and ENPC reverification will no longer be offered after
Dec. 31, 2012.
° Continuing education updates will be offered in place of the
reverification courses.
° New editions of the courses will be available every four years.
• Ratified Judith Halpern, MS, RN, APRN, as a replacement member for
the Emergency Nursing Resources Committee as presented.
• Ratified Carey Goryl, MSW, CAE, chief executive officer (International
Association of Forensic Nurses) and Kim Day, RN, FNE A/P, CFN,
SANE-A, SANE-P (IAFN) as the replacement Forensic Special Interest
Group co-facilitators as presented.
• The board agreed to continue appointing ENA representatives to the
American College of Emergency Physicians’ committees.
Highlights of the next scheduled board of directors meeting will be
published in a future issue of ENA Connection.
July 2012
References
1. Massachusetts Department of Public
Health Occupational Health
Surveillance Program. (2010). Sharps
Injuries among Hospital Workers in
Massachusetts, 2010: Findings from
the Massachusetts Sharps Injury
Surveillance System.
2. NIOSH Alert: Preventing Needlestick
Injuries in Health Care Settings.
(n.d.). Retrieved from
www.cdc.gov/niosh
3. Needlestick Injury Rates According
to Different Types of Safety-
Engineered Devices: Results of a
French Multicenter Study
William Tosini, MD; Celine Ciotti,
RN; Floriane Goyer, RN; Isabelle
Lolom, MSc; Franc¸ois L’Heriteau,
MD; Dominique Abiteboul, MD;
Gerard Pellissier, PhD; Elisabeth
Bouvet, MD.

Recruitment Ads

Recruitment Ads

Recruitment Ads

be happy.
You know us as recognized ED leaders who guide hospitals toward real and
effective change. Now we would like to get to know you. Blue Jay Consulting is
looking for professionals with the leadership insight and clinical experience to
bring process improvements to our clients, and the passion and commitment to
enhance the overall quality of emergency care. If you consider yourself among
the best in your field, you’ll find yourself in good company at Blue Jay Consulting.
Join the strongest team in the industry and... be happy.
www.bluejayconsulting.com
Contact Jim Hoelz or Mark Feinberg at 407-210-6570 to discuss how we can capitalize on
one another’s strengths.
“ As a Blue Jay Consultant, I apply the skills and experience I have gained in my nursing career every day. Each assignment brings new challenges and opportunities to make a difference for ED staff and the patients they care for. My work touches the lives of many people. I love what I do and the colleagues and clients I work with.”
— N A N C Y B O N A L U M I , R N , M S , C E N
Director
Blue Jay Consulting, LLC
When you’re on the right team, happiness ensues.