Embed Size (px)
Citation preview

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 1
European Curriculum of Geriatric Emergency Medicine (ECGEM)
Produced by the European Task Force on Geriatric Emergency Medicine (ETFGEM).
With the collaboration of the European Society for Emergency Medicine (EuSEM) and the
European Union of Geriatric Medicine Society (EUGMS).
Chairs:
Abdelouahab Bellou, Professor of Emergency Medicine, MD, PhD, Chair of the Section of
Geriatric Emergency Medicine of EuSEM.
Simon Conroy, Honorary Professor of Geriatric Medicine, MD, PhD, Chair of the Geriatric
Emergency Medicine Interest Group of EUGMS.
Members of the ETFGEM:
EuSEM: Jay Banerjee (UK), Abdelouahab Bellou (FR/USA, Chair), Olivier Ganansia (FR),
Alexandre Jeleef (FR), Christian Nickel (SW), Marc Sabbe (BE), Richard Wolfe (USA).
EUGMS: Anna Björg Jónsdóttir (IS), Simon Conroy (UK, Chair), Maria Fernandez (ES), F. Javier
Martín-Sánchez (ES), Simon Mooijaart, (NL), Fredrik Sjöstrand (SE), Regina Roller-
Wirnsberger (AU).
Introduction: This curriculum is intended to outline competencies that will be relevant to
the care of older people (>65 years of age) especially those with frailty, in emergency care
including pre-hospital care and in emergency departments. This curriculum should be used
in conjunction with the European Curriculum for Emergency Medicine (in due course
ECGEM will be incorporated into the wider curriculum).
Published: April 2016

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 2
Contents
Page Chapter
3 Pre-hospital care
4 Primary clinical assessment and stabilisation of life threatening conditions
4 Secondary clinical assessment
5 Clinical assessment in older people – what’s different?
7 Non-specific presentations
8 Management of geriatric syndromes
9 Pitfalls in the management of common conditions – ‘atypical presentations’
9 Comprehensive Geriatric Assessment
10 Risk benefit analysis
10 Medication: review and reconciliation
11 Pain management
11 Palliative Care
11 Ethical issues, including advance directives
12 Transitions of care and disposition

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 3
Pre-hospital care # Competencies
1 To understand the risk of under-triage in older people (i.e. vital signs may be in the normal range, but not normal for that patient - e.g. normotension in someone with systolic hypertension)
2 To recognise the need to take a collateral history or documentation about the patient’s usual status and medical history
3 To understand the importance of obtaining an accurate medication history including an assessment of compliance
4 To recognise the importance of capturing the home environment including formal and informal caregivers as part of the pre-hospital assessment
5 To be aware of the potential existence of resuscitation order or advance directive that may be in the person home
6 To understand the importance of sensory impairments in older people and the need to ensure patients are conveyed with their sensory appliances
7 To be able to recognise high risk presentations in older people which may not be identified using traditional triage scores
8 To be aware that conventional physiological parameters may be inadequate to identify older people with severe illness
9 To be aware that abnormal physiological parameters may be long-standing in older people
10 Injury mechanisms cannot be used to reliably triage as older people are susceptible to significant trauma from low energy mechanisms
11 To ensure that every patient has careful assessment, not based on age
12 To be aware that geriatric syndromes such as falls and confusion can be associated with serious underlying problems and act as markers of future prognosis

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 4
Primary clinical assessment and stabilisation of life threatening conditions # Competencies
13 To know the effects of altered anatomy on airway management (dentition, microstomia, macroglossia, cervical spondylosis and associated reduced neck extension)
14 To be able to adjust rapid sedation medication according to age associated changes in pharmacodynamics & pharmacokinetics
15 To recognise that shock and hypoperfusion can exist in older people despite blood pressures in the normal range
16 To be aware of the risk of masked cerebral injury (e.g. normal Glasgow Coma Score in people with falls on anticoagulation) related to cerebral atrophy and cognitive impairment
17 To institute appropriate early monitoring and testing with the understanding that older people may present with muted signs and symptoms (e.g. absent pain and neurologic changes) and are at risk of occult shock
18
To appreciate the importance of hypothermia as a presenting feature that is associated with high morbidity and
mortality
Secondary clinical assessment # Competencies
19 To be aware of altered anatomy (e.g. arthritis), physiology, changes related to prosthetic devices (e.g. pacemakers) and the effects of medication when interpreting the secondary survey
20 To know common patterns of injury in older people for example, ground level falls with serious sequelae

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 5
Clinical assessment in older people – what’s different? # Competencies
Communication and history taking
21 The practitioner will be able to recognise the presence of sensory impairment (hearing, sight, speech) or cognitive impairment that impairs communication
22 To be able to adapt communication in older people taking account of hearing/sight impairments, speech difficulties, aphasia, and cognitive disorders (e.g., using family/friend, writing, to clean and adjust a hearing aid)
23
Document history obtained from nursing homes about the acute events necessitating ED transfer including goals of visit, medical history, medications, allergies, cognitive and functional status, advance care plan, and responsible primary care provider
Geriatric syndromes – ‘identification of typical presentations in older people’
24 To be aware of locally acceptable methods of identifying frail older people
25 To be able to use a locally acceptable tool to identify older people with frailty who will need a more holistic assessment
26 To follow locally devised pathways that lead to an enhanced multidimensional assessment in older people
27 Generate an age-specific differential diagnosis for older patients presenting to the ED with general weakness, immobility, dizziness, falls, or altered mental status
28 To be aware of adverse reactions to medications, including drug–drug and drug–disease interactions, as part of the initial differential diagnosis
29
To understand the danger of labelling or diagnosing older people as having 'social admissions', as these patients will often have a complex interaction of comorbidities, polypharmacy and environmental factors that have precipitated their visit to the ED
30 To be able to apply scores assessing the risk of adverse outcomes in older people attending emergency departments, including risk following discharge from the ED and risk of adverse outcomes following admission from the ED
Effect of comorbid conditions
31 To assess and document the presence of comorbid conditions (e.g., pressure ulcers, cognitive status, falls in the past year, ability to walk and transfer, and social support) and include them in medical decision-making and plan of care
32 To develop plans of care that anticipate and monitor for predictable complications in the patient’s condition (e.g. gastrointestinal bleed causing ischemia)
European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 6
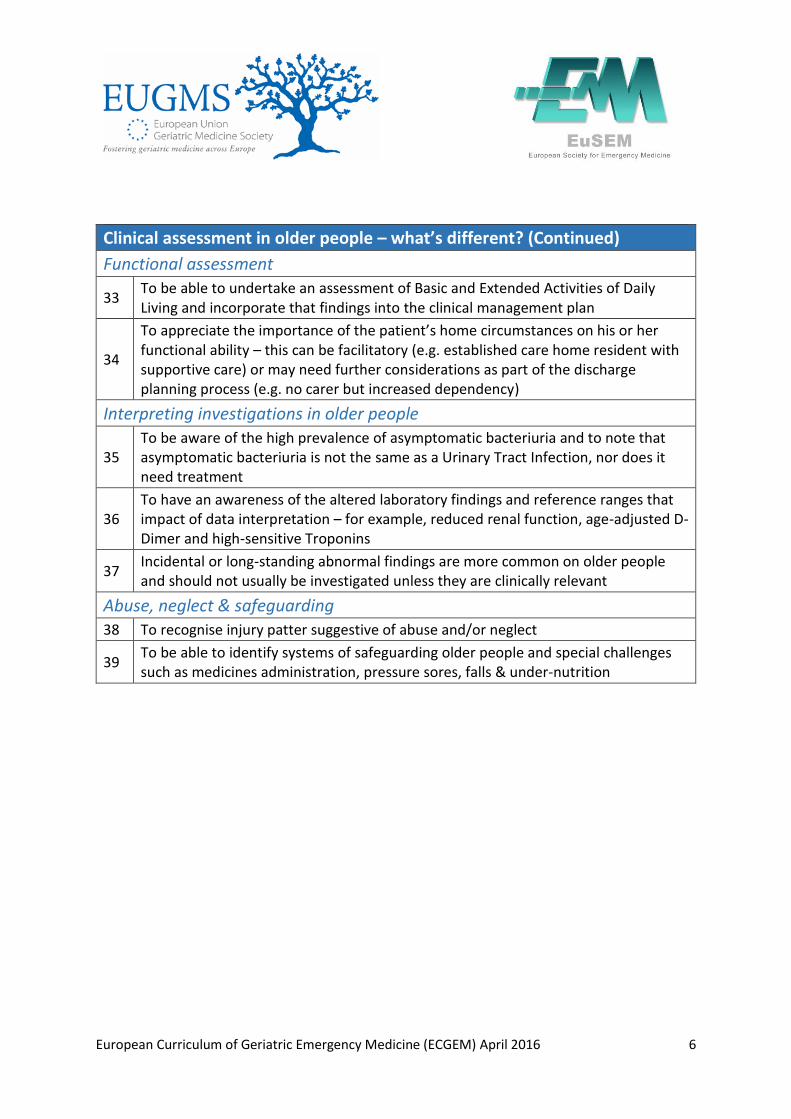
Clinical assessment in older people – what’s different? (Continued)
Functional assessment
33 To be able to undertake an assessment of Basic and Extended Activities of Daily Living and incorporate that findings into the clinical management plan
34
To appreciate the importance of the patient’s home circumstances on his or her functional ability – this can be facilitatory (e.g. established care home resident with supportive care) or may need further considerations as part of the discharge planning process (e.g. no carer but increased dependency)
Interpreting investigations in older people
35 To be aware of the high prevalence of asymptomatic bacteriuria and to note that asymptomatic bacteriuria is not the same as a Urinary Tract Infection, nor does it need treatment
36 To have an awareness of the altered laboratory findings and reference ranges that impact of data interpretation – for example, reduced renal function, age-adjusted D-Dimer and high-sensitive Troponins
37 Incidental or long-standing abnormal findings are more common on older people and should not usually be investigated unless they are clinically relevant
Abuse, neglect & safeguarding 38 To recognise injury patter suggestive of abuse and/or neglect
39 To be able to identify systems of safeguarding older people and special challenges such as medicines administration, pressure sores, falls & under-nutrition

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 7
Non-specific presentations # Competencies
40 Generate a differential diagnosis recognising that signs and symptoms such as pain and fever may be absent or less prominent in older people with acute coronary syndrome, acute abdomen, or infectious processes
Trauma
41 Injuries tend to be under-recognised and under-managed in older people, especially those with frailty or cognitive impairment, and their outcomes are worse – clinicians should demonstrate greater awareness in this population
42
To know that older people are at increased risk from traumatic brain injury because of more friable blood vessels and medication affecting bleeding status, features of TBI may be masked in this population due to cerebral atrophy ‘accommodating’ intra-cranial collections
43 To appreciate that older people are at greater risk of complication from blunt trauma, such as pneumonia following rib fracture or solid organ injury
44 To demonstrate an understanding that low-injury trauma is the commonest cause of pelvic fractures and such injuries are associated with an increased risk of haemorrhage
45 To appreciate that earlier recognition of trauma and appropriate assertive management increase the chances of a good recovery
46 To demonstrate ability to recognise patterns of trauma (physical/sexual, psychological, neglect/abandonment) that are consistent with elder abuse. Manage the abused patient in accordance with the rules of the state and institution

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 8
Management of geriatric syndromes # Competencies
Falls balance and gait disorders 47 To be able to use a framework for the initial assessment of falls in older people
48 To be able to differentiate syncopal falls from non-syncopal falls, cognisant of complicating factors such as associated amnesia or cognitive impairment)
49 To be aware of the importance of a medication review in people with falls
50 To follow locally devised pathways that lead to an enhanced multidimensional assessment in older people with falls
Cognitive and behavioural disorders
51 Assess and document current mental status and any change from baseline with special attention to determine if delirium exists or has been superimposed on dementia
52 Devise a differential diagnosis for older people with new cognitive or behavioural impairment, including self-neglect; initiate a diagnostic workup and treatment
53
Assess and correct factors causing agitation in older people such as untreated pain, hypoxia, hypoglycaemia, use of restraints (e.g. monitor leads, blood pressure cuff, pulse oximetry, intravenous access, and urinary catheters), environmental factors (light, temperature), and disorientation
54 To be able to differentiate delirium from dementia and to be familiar with tools for supporting this process
55 To be able to formulate a list of differential diagnoses for delirium with special consideration of infection, polypharmacy and metabolic abnormalities such as hyponatraemia
56 Describe a range of non-pharmacological approaches to the management of agitation in older people
57
To be aware of the need for, and be able to access support for people with dementia and their carers, including postdiagnostic support and advice, personalised services, peer support, housing support, housing-related services and
telecare

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 9
Management of geriatric syndromes (Continued)
Mood disorder – depression and anxiety
58 To be able to routinely assess for mood disorders including depression and anxiety in older people attending ED
59 To know referral pathways for people with mood disorder that need additional support
Substance abuse
60 To understand that alcohol abuse occurs in older people and alcohol intoxication can complicate the clinical presentation as well as being a risk factor for injury
Skin care/pressure sores
61 Appreciate that skin damage can occur within 40 minutes or quicker in older people on hard trolleys/spinal boards, with additional pre-disposing factors such as diabetes
62 Pressure sores can be a source of occult sepsis
Pitfalls in the management of common conditions – ‘atypical presentations’ Be aware of the potential dangers in common presentations in older people – some selected examples of how different things can present are described below:
# Competencies
63 Abdominal pain – think aortic aneurysm, heart attack, constipation
64 Diarrhoea – think mesenteric ischaemia, sepsis or constipation with overflow more than gastroenteritis
65 Vomiting – avoid anti-dopaminergic drugs in people with Parkinson’s disease
66 Back pain – think aortic aneurysm, insufficiency fractures or cord compression
67 Non-specific weakness may not be benign and needs careful evaluation
68 Chest pain – likely to be cardiac even if non-cardiac sounding
Comprehensive Geriatric Assessment # Competencies
69 To be able to describe the domains of Comprehensive Geriatric Assessment (CGA) – namely medical, psychological/cognitive, functional, social and environmental issues
70 To be aware of locally agreed pathways to access CGA both in-hospital and in the community setting

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 10
Risk benefit analysis To be able to carefully consider the competing risks associated with standard, protocol driven treatment in older people, for example:
# Competencies
71 To be able to weigh up the risk of bleeding associated with ‘triple therapy’ (Aspirin, Clopidogrel and Low Molecular Weight Heparin)
72 To appreciate the risk of routine urinary catheters to assess fluid status, that may increase the risk of catheter associated UTI and sepsis
73 To appreciate that urinary catheters can cause substantial problems with detrusor instability and urinary incontinence as well as impairing dignity and increasing the risk of falls
74 Identify and implement measures that protect older people from developing iatrogenic complications common to the ED including invasive bladder catheterisation, spinal immobilization, and central line placement
Medication: review and reconciliation # Competencies
75 To be aware that medication can be a common cause of presentations e.g. bleeding with anti-coagulants, hypoglycaemia with anti-diabetic medication or toxicity associated with drugs with narrow therapeutic windows
76
To be aware of the importance that medication reconciliation adds to the clinical assessment and management of older
people
77 Describe the changes in pharmacokinetics and pharmacodynamics seen in older people
78 Prescribe appropriate drugs and dosages considering the current medication, acute and chronic diagnoses, functional status, and knowledge of age-related physiological changes (renal function, central nervous system sensitivity)
79 Compliance – awareness that older people may not be taking medication as prescribed because of a range of reasons including side-effects
80 Search for interactions and document reasons for use when prescribing drugs that present high risk either alone or in drug–drug or drug–disease interactions (e.g. benzodiazepines, digoxin, insulin, NSAIDs, opioids, and warfarin)
81
To understand the need and be able to access support newly prescribed drugs to older people and caregivers at discharge, checking that they understand how and why the drug should be taken, the possible side effects, and how and
when the drug should be stopped

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 11
Pain management # Competencies
82 Define the effects of age, body size, organ dysfunction and concurrent illness on drug distribution and metabolism
83 To be aware of the importance of early analgesia in preventing delirium – e.g. fascio-iliac block for hip fracture
Palliative Care
# Competencies
84 To be able to work within a multidisciplinary team incorporating patient preferences to determine when escalation of care is indicated, and when it may not be appropriate
85 Know how to access the local pathways for hospice care and how to manage older people in hospice care while in the ED
86 Know when to institute or seek developing an end of life care plan
Ethical issues, including advance directives # Competencies
87 To understand the local/national legal position of advance directives and Power of Attorney
88 To be able to formulate a best interest’s decision in the emergency context
89
To be able to understand ethical dilemmas around standards of care versus goals of care (for example, best practice management of an acute coronary syndrome may not be appropriate or relevant in an older person with end stage dementia who has a limited life expectancy for whom the goals of care may be comfort related)

European Curriculum of Geriatric Emergency Medicine (ECGEM) April 2016 12
Transitions of care and disposition # Competencies
For every care transition (intra- or extra hospital), the practitioner will be able to formulate the following information:
91 Physiological parameters with the individualised clinical interpretation
92 Clinical narrative including communication needs and key informants
93 Medication and any changes
94 Thoughts about discharge planning and the home environment
95 Escalation status including advance care plans
96
To assess and document suitability for discharge considering the ED diagnosis, including cognitive function, the ability in ambulatory patients to ambulate safely, availability of appropriate nutrition/social support, and the availability of access
to appropriate follow-up therapies
97 Discharge planning should include an assessment of whether the patient is able to give an accurate history, participate in determining the plan of care, and understand discharge instructions
98 Provide skilled nursing homes and primary care providers with an ED visit summary and plan of care, including follow-up when appropriate





























