Embed Size (px)
Citation preview
Evaluation of the urologic patient
• Urinary tract is divided into upper and lower urinary tract
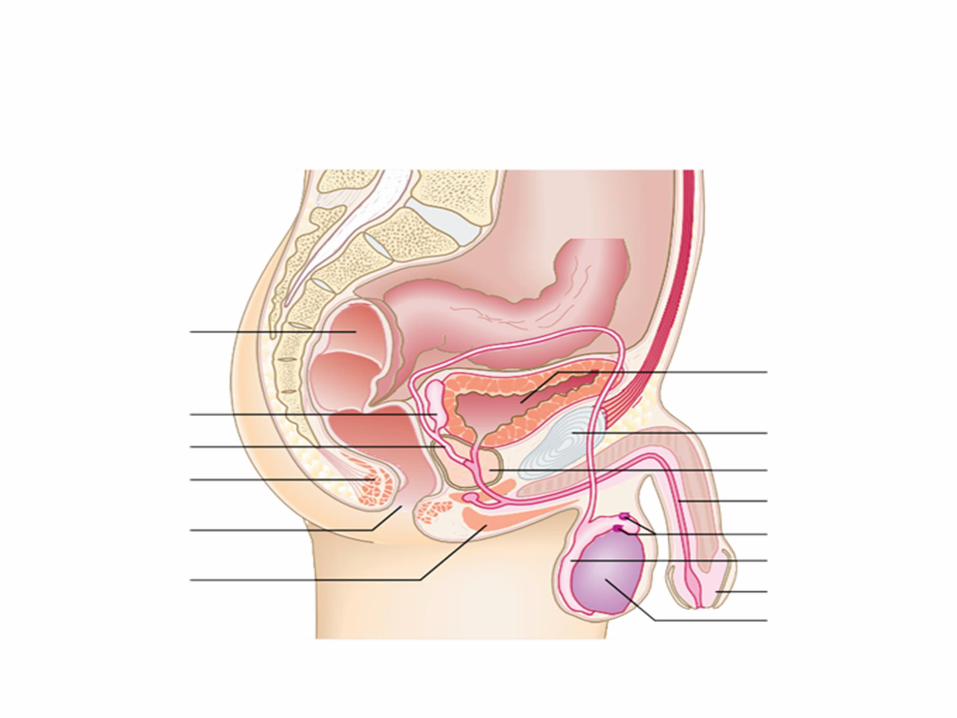
• Upper urinary tract involve kidneys and ureters while lower urinary tract involve bladder and urethra and prostate in male
• The kidneys form urine which travel down the ureter and will be stored in the bladder, the bladder can stretch and once full, the urine will flow through the urethra and then out
• Kidney's are paired, ovoid fist sized retroperitoneal structures , locate in posterior abdomen on each side of vertebral column
• The kidneys are responsible for filtering the blood, and excretion of waste product and regulating blood pressure and electrolytes and PH balance, also producing erythropoietin and activation of VIT D
• The RT kidney is 1-2cm below the LT one and extend from 1st to 3rd lumbar vertebrae, the LT kidney from 12th thoracic to 3rd lumbar vertebrae
• Each kidney is about 12 cm in length 6 cm in width and 3 cm in thickness, and weight 150 gm
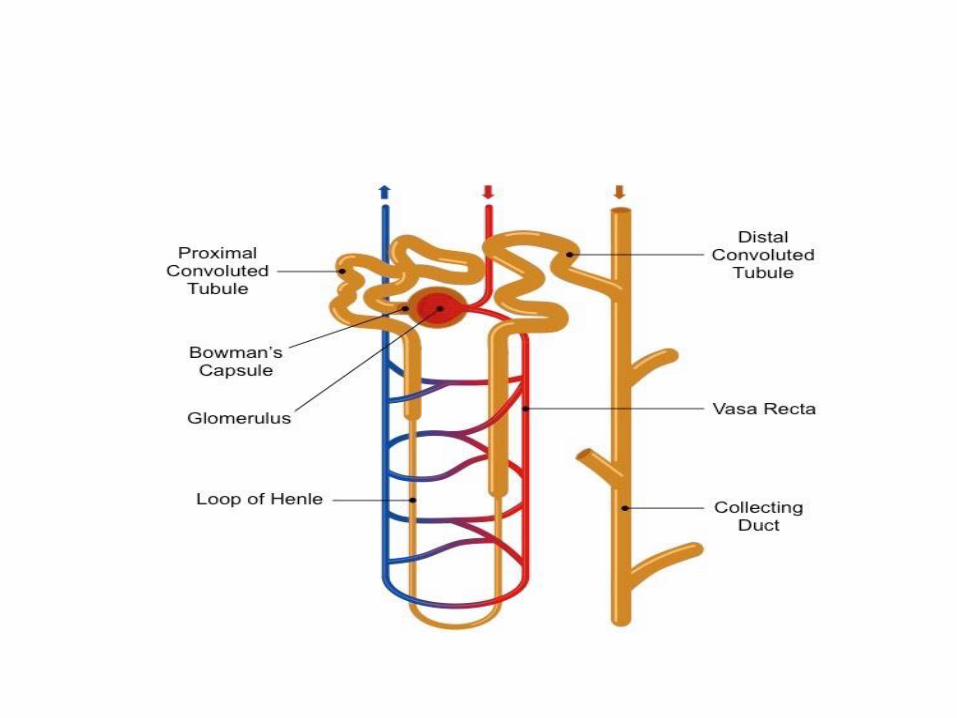
• The functional unit of the kidney is called nephron
• Each kidney has about one million nephron , and these structures filter our blood and secrete waste and allow absorption of things into the blood stream
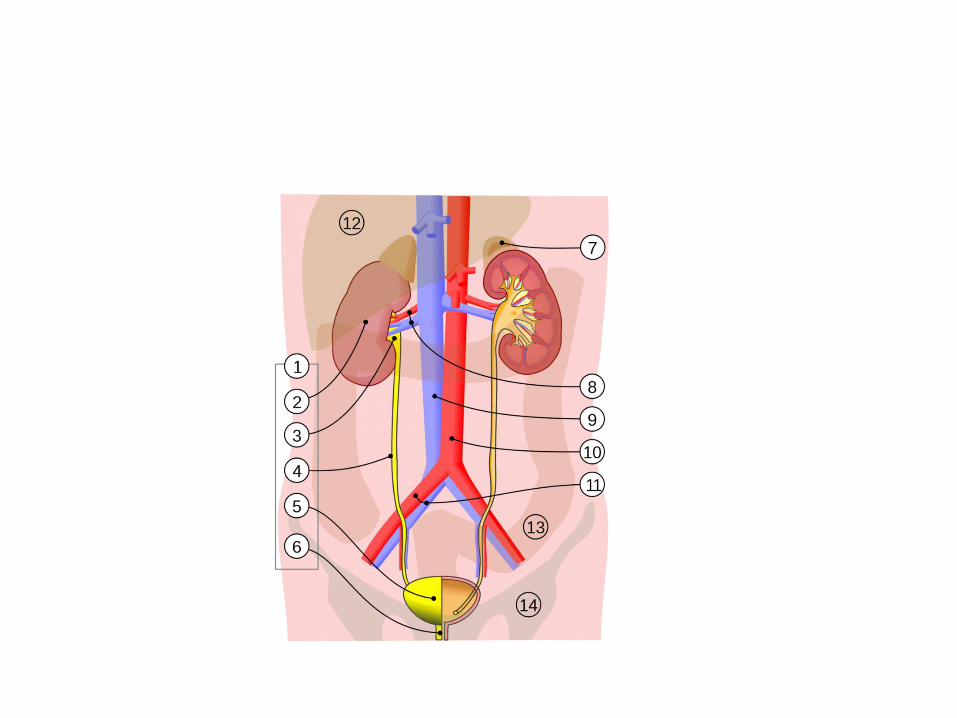
• Ureter : is bilateral muscular duct that carry urine from kidney to bladder
• In adult it is about 22-30 cm in length with diameter 1.5-6 mm
• The ureter has three sites of constrictions ( narrow area) PUJ, VUJ, when crossing iliac bifurcation these area are potential sites for obstruction by stones
• The ureter is divided into upper and middle( over the sacrum) and lower segment
• Also divided according to anatomic terminology into abdominal, pelvic ureter, and intramural segment
• The basic approach of urologic patient include:
• History
• Physical examination
• Lab investigation
• Radiological assesment
Chief complaint
• Pain: pain from GU tract is usually caused by inflammation or obstruction
• Urinary stones cause sever pain when obstruct the urinary tract, however non obstructing stones are totally asymptomatic
• Urinary retention from prostatic obstruction is quit painful• Inflammation of GU tract is usually sever when involve the
parenchyma of the solid organ and so pyelonephritis ,prostatitis, epididymitis is quit painful
• Inflammation of mucosa of hollow organ such as bladder and urethra usually produce discomfort but the pain is not as sever .
• Tumor is painless unless cause obstruction or invasion of nerve , and so pain of GU malignancy is a sign of advanced disease
Renal pain
is usually cause by acute distension of renal capsule from generally obstruction or inflammation
Usually located in the flank area which is the area between the 12th rib and iliac bone
And radiate to upper abdomen and umbilicus and may be referred to the testis due to common innervation of renal pelvis and testicle (T11-T12)
Pain due to inflammation is steady in nature while due to obstruction fluctuate in intensity
• Pain of renal origin may associate with nausea and vomiting ,because reflex stimulation of celiac ganglia or proximity of GI organ
• Renal pain could be confused with pain of intraperitoneal pathology: ptn with renal pain prefer to move around holding the loin area (rolling sign), and usually colicky in nature
• Intraperitoneal pain radiate to shoulder and steady, ptn prefer to lie motionless
• Renal pain could be confused with pain resulting from irritation of costal nerves mostly T10-T12 which is not colicky and the radicular pain is altered by changing position
• Shingle which caused by varicella zoster virus that cause chickenbox
• Firstly it cause burning pain which followed by skin rash involve flank area
• Usually unilateral
Ureteral pain
• usually secondary to obstruction, the pain caused by distension and hyperperistalsis and spasm of smooth muscle as it attempt to relieve obstruction which usually caused by stone or blood clot
• The site of radiation depend on location of obstruction, stone obstructing the PUJ cause severe pain witout radiation to the groin
• Stone at mid ureter tends to radiate to the groin and so may mimic appendicitis or diverticulitis
• Distal ureteric stone the pain radiate to the groin or testicle
• Stones at VUJ cause irritative voiding symptom and suprapubic pubic pain may mimic urethritis or cystitis
• Vesical pain: overdistension(AUR), inflammation, • Inflammatory condition of bladder usually cause
intermittent suprapubic discomfort• Strangury: sharp stabbing suprapubic pain at the
end of voiding in ptn with cystitis• Constant suprapubic pain that not associated
with lower abdominal swelling is rarely of urological origin
• Slowly progressive bladder distention frequently cause no pain
• Prostatic pain• Poorly localized pain usually secondary to
inflammation• Associate with irritative voiding symptom as
frequency and dysuria and in severe case may produce urinary retention
• Penile pain: in flaccid penis could be due to bladder or urethral inflammation, or paraphimosis
• In erect penis : peyronie disease or priapism
• Scrotal pain: could be acute or chronic
• Acute testicular pain usually secondary to torsion ot testicle or testicular appendex, epididymoorchitis
• Chronic testicular pain usually result from non inflammatory condition such as hydrocele or varicocele
• Because testicle arise in close proximity to the kidney, pain from the kidney may be referred to testicle
• Hematuria it is the presence of blood in urine
• Hematuria in adult is symptom of malignancy until proven otherwise
• The mcc of GH over age of 50 is bladder cancer
Lower urinary tract symptom
• Irritative symptom
• Frequency: the most common urological symptom
• Normal adult voids 5-6 times per day
Frequency is either due to increase urine output (Polyuria) or decreased bladder capacity
• Nocturia: is one or more rise from sleep , and clinically significant if 2 or more
• As with frequency it could be caused by increase urine output or decrease bladder capacity
• Nocturnal polyuria is more than one third of urine output
• Nocturea without frequency may occur in ptnwith CHF and peripheral edema in whom urine output increase in night when they are supine
• This aggravated by decreasing concentrating ability at night in geriatric ptn
• Dysuria: painful urination usually felt over urethral meatus and caused by inflammation
• Urgency: strong desire to void
• Obstructive symptom
• Poor stream ,hesitancy, intermittency, post void drippling, straining, incomplete voiding
• Straining: use of abdominal muscle to urinate which are used only at the end of voiding
• Intermittency: involuntary start stop of urinary stream
• Postvoid dribbling: terminal release of drops of urine at the ending of voiding
• Poor stream: decrease the force of urination• Hesitancy: delay in the initiation of urination• Obstructive and irritative symptom(LUTS): are not
specific for prostate problem as could be result from another cause of BOO, or neurological disease or even bladder tumor
• Incontinence : involuntary loss of urine
• Continuous incontinence: due to fistula that bypass the urethral sphincter most commonly vesicovaginalfistula, or ectopic ureter in female
• Stress incontinence: leakage of urine with increase abdominal pressure
• Urge incontinence: urine leak preceded by strong desire to void
• Overflow incontinence: in ptn with chronic retention
• Enuresis: incontinence that occur during sleep
• Hematospermia: is the presence of blood in semen, mostly result from non specific inflammation of prostate and seminal vesicle frequently after period of sexual abstinence
• If persist for more than several weeks it should be investigated
• Pneumaturia: presence of gas in urine, cause by recent catheterization, fistula with intestine, infection with gas forming organism