Embed Size (px)
Citation preview

Exacerbation of Avellino Corneal Dystrophy After LASIKin North America
Christopher S. Banning, MD(* Woon Cho Kim(† J. Bradley Randleman, MD(*Eung Kweon Kim, MD, PhD,‡ and R. Doyle Stulting, MD, PhD*
Purpose: To report the first case of Avellino corneal dystrophy
exacerbation after LASIK in a white or North American patient.
Methods: Case report and literature review.
Results: A 25-year-old white female developed progressive corneal
opacities after LASIK. Preoperative examination had revealed only
subtle white corneal opacities in each eye. The patient_s mother had
similar corneal opacities. DNA analysis of the patient revealed a
heterozygous mutation at the R124H location in the BIGH3 gene.
Conclusions: LASIK can exacerbate Avellino corneal dystrophy
and should be avoided in patients with this condition. A careful
history and genetic analysis can identify affected patients and those
at risk.
Key Words: Avellino dystrophy, BIGH3 gene, LASIK
(Cornea 2006;25:482Y484)
Avellino corneal dystrophy is an autosomal dominantstromal corneal dystrophy originally described in des-
cendants of the Avellino, Italy region.1 This dystrophy iscaused by a specific mutation at codon 124 of the BIGH3 geneon chromosome 5.2,3 Avellino dystrophy shares clinicalfeatures with both granular and lattice corneal dystrophies.BIGH3 gene analysis has been used to differentiate thesedisorders because of the unique mutation associated witheach dystrophy.2,3
Exacerbation of Avellino dystrophy after LASIK hasbeen reported in Koreans.4,5 Jun et al described 7 patients withAvellino dystrophy that developed worsening of their diseaseafter LASIK.5 The number of affected patients is growingrapidly, now with more than 30 cases in Korea with knowndisease exacerbation after LASIK (E.K. Kim, unpublisheddata). Herein, we describe the first reported case ofexacerbation of Avellino dystrophy after LASIK in either awhite patient or one from North America. Potential mechan-isms of disease progression and treatment strategies arediscussed.
CASE REPORTA 25-year-old white female was referred to the Cornea
Service at Emory University for evaluation of decreased vision inboth eyes 14 months after uneventful bilateral LASIK for arefractive error of approximately Y8.00 D OU. The treatingphysician had observed B2 or 3 small, white, central, subepithelialopacities[ in both eyes preoperatively.
Two months postoperatively, the patient complained of mildglare in both eyes when outdoors. Uncorrected visual acuity(UCVA) was 20/25jOD and 20/20jOS. Examination showedmild dry eye, but no corneal opacities were noted in the medicalrecord. She was treated with artificial tears.
Over the next several months, the patient noted progressiveloss of vision and increasing glare in both eyes. Six monthspostoperatively, UCVA was 20/25jOU. Numerous white, central,subepithelial opacities were now seen in both corneas, and thepatient was diagnosed with mild diffuse lamellar keratitis.Loteprednol etabonate 0.2% was initially prescribed twice dailybut was discontinued, and the opacities progressed.
By 1 year postoperatively, UCVA had fallen to 20/50 ODand 20/70 OS. Manifest refraction of Y1.75 + 0.75 � 138 OD andY1.75 + 0.75 � 055 OS yielded visual acuities of 20/20 in each eye.Further progression of the corneal opacities in each eye promptedreferral to the Cornea Service at Emory.
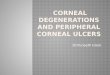
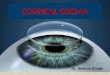
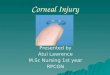
At this examination, UCVA was 20/60 OD and 20/70 OS,improving to 20/20 in each eye with refraction (Y2.00 + 1.00 � 132OD and Y2.00+ 0.75 � 054 OS). Slit-lamp examination showeddiscrete corneal opacities within and posterior to the interfacebetween the flap and stromal bed in each eye (Figs. 1Y3). Theopacities were white, granular in appearance, 0.1Y0.3 mm indiameter, and the intervening stroma was clear. The ophthalmologicexamination was otherwise unremarkable. The patient_s family his-tory was pertinent for an undetermined corneal abnormality in hermaternal grandfather and mother. Neither of these family membersever received treatment of this condition. Slit-lamp examination ofthe patient_s mother revealed similar corneal deposits in each eye.
Venous blood was drawn from the patient and extracted DNAsent for polymerase chain reaction testing and DNA sequencing ofthe BIGH3 gene. Her DNA was heterozygous for the R124H(Avellino dystrophy) mutation and negative for the R555W (granulardystrophy) mutation.
After discussion with the patient, spectacle correction wasprescribed and observation of the corneal deposits was recom-mended. She was discouraged from pursuing LASIK enhancement.Her examination has remained stable over the ensuing 7 months.
DISCUSSIONThis is the first reported case of exacerbated Avellino
dystrophy after LASIK in North America or in a whitepatient; however, others will undoubtedly follow with the
CASE REPORT
482 Cornea & Volume 25, Number 4, May 2006
From the *Department of Ophthalmology, Emory University, Atlanta, GA;†Emory University, Atlanta, GA; and the ‡Department of Ophthalmology,Institute of Vision Research, Yonsei University, Seoul, Korea.
Received for publication March 3, 2005; accepted August 12, 2005.Financial Support: None.Reprints: Chris Banning, 1365B Clifton Road NE, Suite 4500, Atlanta, GA 30322
(e-mail: [email protected]).Copyright * 2006 by Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

increasing numbers of LASIK procedures being performed.Some of these patients will be difficult to recognizepreoperatively because of minimal corneal involvement.
Insight into factors that trigger phenotypic expressionof stromal dystrophies is growing. Transforming growthfactor beta (TGF-A) is a family of cytokines produced byepithelial cells and keratocytes that is involved in the cornealwound healing response.6 The activity of TGF-A increases inresponse to corneal injury6 and excimer laser surgery.7,8
TGF-A directly activates the BIGH3 gene causingoverexpression of the gene product keratoepithelin.9 Specificmutations in this gene have been shown to cause Avellinodystrophy, along with forms of lattice dystrophy, granulardystrophy, and corneal dystrophy of Bowman_s mem-brane.2,10,11 Upregulation of TGF-A, therefore, should enhanceabnormal corneal protein deposition in these dystrophies.
LASIK could exacerbate stromal dystrophies by severalmechanisms. Flap creation triggers release of pro-inflammatorycytokines, including TGF-A, through epithelial and stromalcellular injury. The interface between the flap and stromal
bed also likely enhances protein deposition by serving as apotential space for accumulation.12 Choi et al have alsorecently shown that ultraviolet (UV) light exposure increasesTGF-A1 production in cultured human corneal fibroblasts.13
This discovery has potentially deleterious implications for theuse of the 193 nm excimer laser in patients with mutations ofthe BIGH3 gene. The recurrence of stromal dystrophiesafter phototherapeutic keratectomy, sometimes quickly afterablation and more dense than prior to ablation,14,15 may beexplained by UV exposure.16
Treatment options for exacerbation ofAvellino dystrophyafter LASIK include observation or debridement of the flapinterface. Jun et al5 performed flap elevation with manualdebridement of the deposits on 1 patient. Although much of theinterface was cleared and visual acuity improved in this patient,the deposits reaccumulated and vision declined to the pre-debridement level within 6 months. Another patient who wastreated with debridement and mitomycin C has remainedrecurrence-free for greater than 6 months.5
Inoue et al14 have shown that recurrence afterphototherapeutic keratectomy tends to be less severe inpatients with heterozygous mutations of the BIGH3 gene inAvellino dystrophy than it is in patients with homozygousmutations. This genetic determination may guide the formand timing of treatment and also provide prognosticinformation. These patients should avoid LASIK enhance-ments and environmental UV exposure. If elevation of theflap is performed for enhancement or interface debridement,mitomycin C or specific TGF-A blocking antibodies shouldbe used.17
CONCLUSIONSLASIK may be contraindicated in patients with
Avellino dystrophy because it can exacerbate the depositionof corneal opacities postoperatively. Preoperative evaluationof LASIK candidates should include a careful family historyand corneal examination. Genetic testing is indicated in those
FIGURE 1. Slit-lamp view right eye of central, granular-appearing corneal opacities 14 months after LASIK.
FIGURE 2. Magnified view of right cornea reveals discreteopacities with clear intervening stroma.
FIGURE 3. External view of left eye reveals fewercentral opacities.
Cornea & Volume 25, Number 4, May 2006 Exacerbation of Avellino Corneal Dystrophy
* 2006 Lippincott Williams & Wilkins 483
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

who may carry the genetic mutation for Avellino dystrophy,even if there are minimal or no corneal abnormalities present.
REFERENCES1. Holland EJ, Daya SM, Stone EM, et al. Avellino corneal dystrophy;
clinical manifestations and natural history. Ophthalmology. 1992;99:1564Y1568.
2. Munier FL, Korzatska E, Djemai A, et al. Kerato-epithelin mutations infour 5q31-linked corneal dystrophies. Nat Genet. 1997;15:247Y251.
3. Konishi M, Yukihiko M, Yamada M, et al. The classic form of granularcorneal dystrophy associated with R555Wmutation in the BIGH3 gene israre in Japanese patients. Am J Ophthalmol. 1998;126:450Y452.
4. Wan XH, Lee HC, Stulting RD, et al. Exacerbation of Avellino cornealdystrophy after laser in situ keratomileusis. Cornea. 2002;21:223Y226.
5. Jun RM, Tchah H, Kim T, et al. Avellino corneal dystrophy after LASIK.Ophthalmology. 2004;111:463Y468.
6. Song QH, Sing RP, Richardson TP, et al. Transforming growthfactor-beta1 expression in cultured corneal fibroblasts in response toinjury. J Cell Biochem. 2000;77:186Y199.
7. Kaji Y, Mita J, Obata H, et al. Expression of transforming growth factor bsuperfamily and their receptors in the corneal stromal wound healingprocess after excimer laser keratectomy. Br J Ophthalmol. 1998;82:462Y463.
8. Kaji Y, Soya K, Amano S, et al. Relation between corneal haze andtransforming growth factor-b1 after photorefractive keratectomy andlaser in situ keratomileusis. J Cataract Refract Surg. 2001;27:1840Y1846.
9. Skonier J, Neubauer M, Madisen L, et al. cDNA cloning and sequenceanalysis of beta ig-h3, a novel gene induced in a human adenocarcinomacell line after treatment with transforming growth factor-beta.DNA Cell Biol. 1992;11:511Y522.
10. Stone EM, Mathers WD, Rosenwasser G, et al. Three autosomaldominant corneal dystrophies map to chromosome 5q. NatGenet. 1994;6:47Y51.
11. Dighiero P, Valleix S, D_Hermies F, et al. Clinical, histologic, andultrastructural features of the corneal dystrophy caused by theR124L mutation of the BIGH3 gene. Ophthalmology. 2000;107:1353Y1357.
12. Lee ES, Kim EK. Surgical do_s and don_ts of corneal dystrophies. CurrOpin Ophthalmol. 2003;14:186Y191.
13. Jung S, Choi S, Kim EK, et al. TGF-A1 concentration is increased afterUVB irradiation in hTERT immortalized human fibroblasts. InvestOpthalmol Vis Sci. 2004;45:E-Abstract 3783.
14. Inoue T, Watanabe H, Yamamoto S, et al. Different recurrence patternafter phototherapeutic keratectomy in the corneal dystrophy resultingfrom homozygous and heterozygous R124H BIG-H3 mutation. Am JOphthalmol. 2001;1332:255Y257.
15. Dogru M, Katakami C, Nishida T, et al. Alteration of the ocular surfacewith recurrence of granular/avellino dystrophy after phototherapeutickeratectomy: report of five cases and literature review. Ophthalmology.2001;108:810Y817.
16. Stojanovic A, Nitter TA. Correlation between ultraviolet radiation leveland the incidence of late-onset corneal haze after photorefractivekeratectomy. J Cataract Refract Surg. 2001;27:404Y410.
17. Moller PT, Cavanagh HD, Petroll WM, et al. Neutralizing antibody toTGFbeta modulates stromal fibrosis but not regression of photoablativeeffect following PRK. Curr Eye Res. 1998;17:736Y747.
Banning et al Cornea & Volume 25, Number 4, May 2006
484 * 2006 Lippincott Williams & Wilkins
Copyr ight © Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.