Embed Size (px)
Citation preview

Uveal extranodal lymphoma—Coutinho et al 623
Extranodal B-cell lymphoma of the uvea: a case report
Anamaria B. Coutinho,*† MD; Cristina Muccioli,* MD, PhD;
Maria Cristina Martins,* MD, PhD; Rubens Belfort Jr.,* MD, PhD;
Ana Estela Sant’Anna,* MD, PhD; Miguel N. Burnier, Jr.,† MD, PhD, FRCSC
ABSTRACT • RÉSUMÉ
Case report: Ocular involvement by non-Hodgkin’s lymphoma is a rare conditionthat can result from a primary intraocular lymphoma of the retina or an intraocularmanifestation of systemic lymphoma. Uveal involvement is seldom the initialmanifestation of extranodal lymphoma.We describe an 80-year-old patient with ablind and painful left eye and a history of recurrent uveitis. After ultrasoundevaluation, the eye was enucleated and histopathologic examination revealed amalignant B-cell lymphoma of the uveal tract. The patient has been followed for 8 years after surgery, but she has had no further systemic manifestations oflymphoma and has not required subsequent treatment.
Comments: Primary extranodal lymphoma can be easily mistaken for recurrentuveitis or primary intraocular lymphoma of the retina and central nervous system;it is a differential diagnosis to be considered in cases of recurrent uveitis-likesymptoms evolving to blind painful eye.
Observation : L’atteinte oculaire d’un lymphome non-Hodgkinien est une pathologierare qui peut découler d’un lymphome intraoculaire primitif de la rétine ou d’unemanifestation intraoculaire d’un lymphome systémique. L’atteinte uvéale estrarement la manifestation initiale d’un lymphome extranodal. Nous décrivons le casd’un patient de 80 ans ayant une cécité douloureuse de l’œil gauche et des anté-cédents d’uvéite récurrente. Après évaluation ultrasonique, l’œil a été énucléé etl’examen histopathologique a révélé un lymphome malin à cellules B du tractus uvéal.Le patient a été suivi pendant 8 ans après la chirurgie, mais n’a pas eu d’autres mani-festations systémiques de lymphome et n’a pas requis de traitements ultérieurs.
Commentaires : Le lymphome extranodal primitif peut être pris facilement parerreur pour une uvéite récurrente ou un lymphome intraoculaire primitif de larétine et du SNC; c’est un diagnostic différentiel à considérer pour les cas desymptômes apparemment d’uvéite récurrente qui évoluent en cécité douloureuse.
Ocular involvement by non-Hodgkin’s lym-phoma is a rare condition, constituting less
than 1% of all lymphomas. It becomes a challengingdiagnosis because this tumor mimics either chronicor posterior uveitis.1–3 Ocular lymphoma may alsopresent different cytomorphologic features accordingto the site of tumor involvement and, in someinstances, may spread to the eye from periocularlymphoma such as mycosis fungoides.
Intraocular lymphoma can be further classified
From *the Department of Ophthalmology, Federal University of SãoPaulo, São Paulo, Brazil, and †the Henry C. Witelson Ocular PathologyLaboratory, MUHC, McGill University, Montreal, Que.
Originally received Nov. 11, 2003Accepted for publication Jan. 6, 2005
Correspondence to: Dr. Anamaria B. Coutinho, 3775 University St., Rm.216, Montreal QC H3A 2B4; fax (514) 398-5728; [email protected]
This article has been peer-reviewed.Can J Ophthalmol 2005;40:623–6
either as primary B-cell lymphoma of the retina andcentral nervous system (CNS) or extranodal lym-phoma of the uvea, or as secondary B-cell lymphomathat represents a uveal manifestation of systemic lym-phoma.2,4 Uveal involvement is seldom the initialmanifestation of extranodal lymphoma; it can easilybe mistaken for recurrent uveitis or primary intra-ocular lymphoma of the retina and CNS.5–7
This report aims to highlight the clinical andhistopathologic features of a patient with a mas-querading ophthalmic syndrome that proved to be aprimary isolated extranodal uveal lymphoma.
CASE REPORT
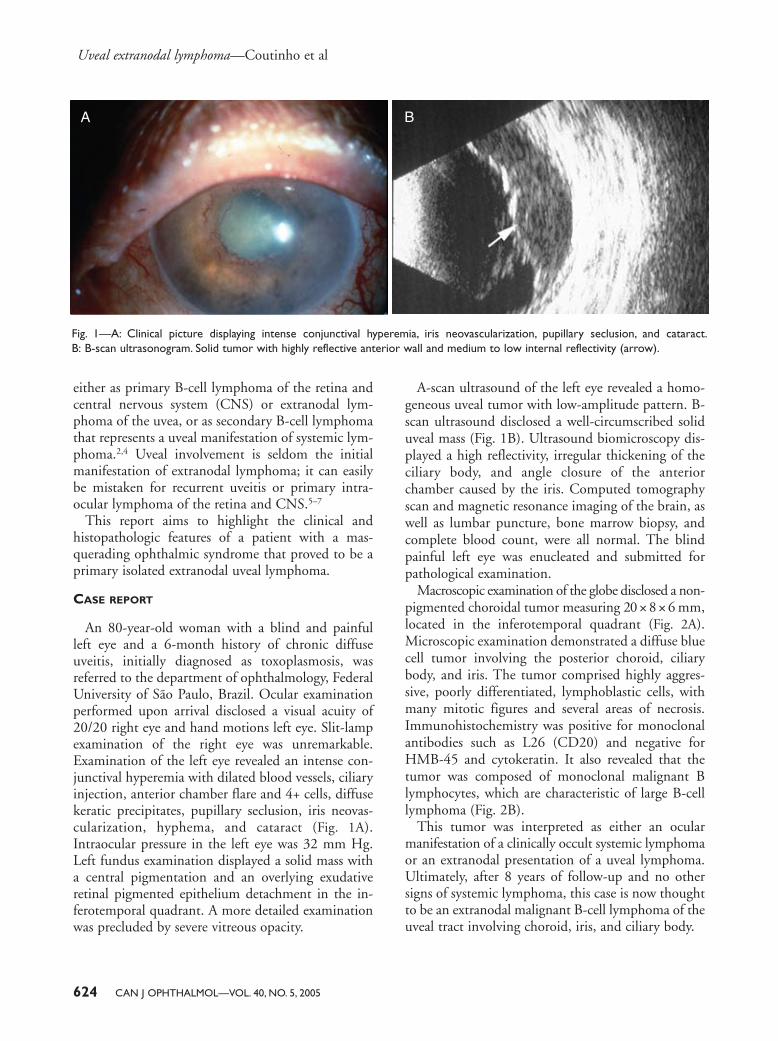
An 80-year-old woman with a blind and painfulleft eye and a 6-month history of chronic diffuseuveitis, initially diagnosed as toxoplasmosis, wasreferred to the department of ophthalmology, FederalUniversity of São Paulo, Brazil. Ocular examinationperformed upon arrival disclosed a visual acuity of20/20 right eye and hand motions left eye. Slit-lampexamination of the right eye was unremarkable.Examination of the left eye revealed an intense con-junctival hyperemia with dilated blood vessels, ciliaryinjection, anterior chamber flare and 4+ cells, diffusekeratic precipitates, pupillary seclusion, iris neovas-cularization, hyphema, and cataract (Fig. 1A).Intraocular pressure in the left eye was 32 mm Hg.Left fundus examination displayed a solid mass witha central pigmentation and an overlying exudativeretinal pigmented epithelium detachment in the in-ferotemporal quadrant. A more detailed examinationwas precluded by severe vitreous opacity.
A-scan ultrasound of the left eye revealed a homo-geneous uveal tumor with low-amplitude pattern. B-scan ultrasound disclosed a well-circumscribed soliduveal mass (Fig. 1B). Ultrasound biomicroscopy dis-played a high reflectivity, irregular thickening of theciliary body, and angle closure of the anteriorchamber caused by the iris. Computed tomographyscan and magnetic resonance imaging of the brain, aswell as lumbar puncture, bone marrow biopsy, andcomplete blood count, were all normal. The blindpainful left eye was enucleated and submitted forpathological examination.
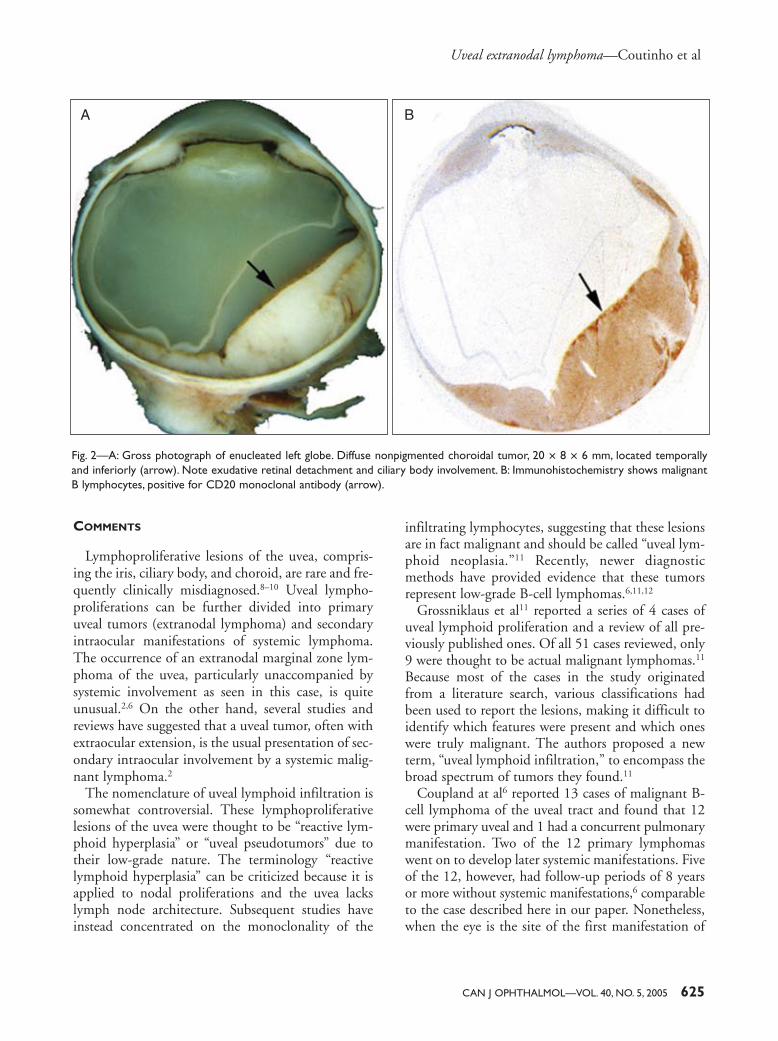
Macroscopic examination of the globe disclosed a non-pigmented choroidal tumor measuring 20 × 8 × 6 mm,located in the inferotemporal quadrant (Fig. 2A).Microscopic examination demonstrated a diffuse bluecell tumor involving the posterior choroid, ciliarybody, and iris. The tumor comprised highly aggres-sive, poorly differentiated, lymphoblastic cells, withmany mitotic figures and several areas of necrosis.Immunohistochemistry was positive for monoclonalantibodies such as L26 (CD20) and negative forHMB-45 and cytokeratin. It also revealed that thetumor was composed of monoclonal malignant Blymphocytes, which are characteristic of large B-celllymphoma (Fig. 2B).
This tumor was interpreted as either an ocularmanifestation of a clinically occult systemic lymphomaor an extranodal presentation of a uveal lymphoma.Ultimately, after 8 years of follow-up and no othersigns of systemic lymphoma, this case is now thoughtto be an extranodal malignant B-cell lymphoma of theuveal tract involving choroid, iris, and ciliary body.
Uveal extranodal lymphoma—Coutinho et al
624 CAN J OPHTHALMOL—VOL. 40, NO. 5, 2005
Fig. 1—A: Clinical picture displaying intense conjunctival hyperemia, iris neovascularization, pupillary seclusion, and cataract.B: B-scan ultrasonogram. Solid tumor with highly reflective anterior wall and medium to low internal reflectivity (arrow).
A B
COMMENTS
Lymphoproliferative lesions of the uvea, compris-ing the iris, ciliary body, and choroid, are rare and fre-quently clinically misdiagnosed.8–10 Uveal lympho-proliferations can be further divided into primaryuveal tumors (extranodal lymphoma) and secondaryintraocular manifestations of systemic lymphoma.The occurrence of an extranodal marginal zone lym-phoma of the uvea, particularly unaccompanied bysystemic involvement as seen in this case, is quiteunusual.2,6 On the other hand, several studies andreviews have suggested that a uveal tumor, often withextraocular extension, is the usual presentation of sec-ondary intraocular involvement by a systemic malig-nant lymphoma.2
The nomenclature of uveal lymphoid infiltration issomewhat controversial. These lymphoproliferativelesions of the uvea were thought to be “reactive lym-phoid hyperplasia” or “uveal pseudotumors” due totheir low-grade nature. The terminology “reactivelymphoid hyperplasia” can be criticized because it isapplied to nodal proliferations and the uvea lackslymph node architecture. Subsequent studies haveinstead concentrated on the monoclonality of the
infiltrating lymphocytes, suggesting that these lesionsare in fact malignant and should be called “uveal lym-phoid neoplasia.”11 Recently, newer diagnosticmethods have provided evidence that these tumorsrepresent low-grade B-cell lymphomas.6,11,12
Grossniklaus et al11 reported a series of 4 cases ofuveal lymphoid proliferation and a review of all pre-viously published ones. Of all 51 cases reviewed, only9 were thought to be actual malignant lymphomas.11
Because most of the cases in the study originatedfrom a literature search, various classifications hadbeen used to report the lesions, making it difficult toidentify which features were present and which oneswere truly malignant. The authors proposed a newterm, “uveal lymphoid infiltration,” to encompass thebroad spectrum of tumors they found.11
Coupland at al6 reported 13 cases of malignant B-cell lymphoma of the uveal tract and found that 12were primary uveal and 1 had a concurrent pulmonarymanifestation. Two of the 12 primary lymphomaswent on to develop later systemic manifestations. Fiveof the 12, however, had follow-up periods of 8 yearsor more without systemic manifestations,6 comparableto the case described here in our paper. Nonetheless,when the eye is the site of the first manifestation of
Uveal extranodal lymphoma—Coutinho et al
CAN J OPHTHALMOL—VOL. 40, NO. 5, 2005 625
Fig. 2—A: Gross photograph of enucleated left globe. Diffuse nonpigmented choroidal tumor, 20 × 8 × 6 mm, located temporallyand inferiorly (arrow). Note exudative retinal detachment and ciliary body involvement. B: Immunohistochemistry shows malignantB lymphocytes, positive for CD20 monoclonal antibody (arrow).
A B

the lymphoma, systemic involvement can occur laterin the disease progression.2,13
Occasionally, ocular involvement can be the initialpresentation of a particular disease.10,13,14 In suchcases, choroidal involvement in the form of a solitaryamelanotic mass or diffuse choroidal thickeningcould be mistaken for an ocular melanoma.11,13
The correct diagnosis of this case was only estab-lished by histopathologic examination of the enucleatedglobe, which disclosed typical findings of malignantB-cell lymphoma in the uveal tract. The patient receivedno further treatment. Eight years of follow-up haveshown no systemic involvement, and all laboratoryfindings for systemic lymphoma remain negative.Ocular examination of the remaining eye is still un-remarkable. The classification of this condition as anextranodal uveal lymphoma without systemic mani-festation seems to be the appropriate nomenclature.5–7
This case, besides its unusual nature, emphasizesthe possibility for differential diagnosis of uveitismasquerading as other conditions in elderly patients.Such conditions include primary lymphoma of theretina and CNS, and less commonly, an ocular man-ifestation of a systemic lymphoma or a primary extra-nodal uveal lymphoma.
REFERENCES
1. Gill MK, Jampol LM. Variations in the presentation ofprimary intraocular lymphoma: case reports and a review.Surv Ophthalmol 2001;45:463–71.
2. Burnier MN Jr, Blanco G. Masquerade syndrome: intraocularlymphoma. In: Yanoff M, Duker JS, eds. Ophthalmology. 1sted. Philadelphia, Pa: Mosby-Wolfe; 1999:chap 24, sect 1–4.
3. Nevins RC, Frey WW, Elliot JH. Primary solitary intraocularreticulum cell sarcoma (microgliomatosis). Trans Am AcadOphthalmol Otolaryngol 1968;72:867–76.
4. Shields JA, Shields CL. Intraocular lymphoid tumors andleukemias. In: Shields JA, Shields CL, eds. IntraocularTumors: a Text and Atlas. Philadelphia, Pa: WB Saunders;1992:489–512.
5. Frederick DR, Char DH, Ljung BM, Brinton DA. Solitaryintraocular lymphoma as an initial presentation of widespreaddisease. Arch Ophthalmol 1989;107:395–7.
6. Coupland SE, Foss HD, Hidayat AA, Cockerham GC,Hummel M, Stein H. Extranodal marginal zone B cell lym-phomas of the uvea: an analysis of 13 cases. J Pathol 2002;197:333–40.
7. Beasley H. Lymphosarcoma of the choroids. Am JOphthalmol 1961;51:1294–6.
8. Cooper EL, Riker JL. Malignant lymphoma of the uveal tract.Am J Ophthalmol 1951;34:1153–8.
9. Jakobiec FA, Sacks E, Kronish JW, Weiss T, Smith M.Multifocal static creamy choroidal infiltrates: an early sign oflymphoid neoplasia. Ophthalmology 1987;94:397–406.
10. Ciulla TA, Bains RA, Jakobiec FA, Topping TM, GragoudasES. Uveal lymphoid neoplasia: a clinical-pathologic correla-tion and review of the early form. Surv Ophthalmol 1997;41:467–76.
11. Grossniklaus HE, Martin DF, Avery R, et al. Uveal lymphoidinfiltration: report of four cases and clinicopathologic review.Ophthalmology 1998;105:1265–73.
12. McLean IW, Burnier MN, Zimmerman LE, Jakobiec FA,eds. Tumors of the Eye and Ocular Adnexa. Atlas of TumorPathology; Series 3. Washington, DC: Armed Forces Instituteof Pathology; 1994:155–214.
13. Nussenblatt RB, Whitcup SM, Palestine AG. Masqueradesyndromes. In: Nussenblatt RB, Whitcup SM, Palestine AG,eds. Uveitis: Fundamentals and Clinical Practice. 2nd ed. St.Louis, Mo: Mosby; 1996:385–95.
14. Whitcup SM, Smet MD, Rubin BI, et al. Intraocular lym-phoma: clinical and histopathologic diagnosis. Ophthalmology1993;100:1399–1406.
Key words: intraocular lymphoma, uveal lymphoma, extranodallymphoma
Uveal extranodal lymphoma—Coutinho et al
626 CAN J OPHTHALMOL—VOL. 40, NO. 5, 2005

![Primary extranodal marginal zone Bcell lymphoma … palatal soft tissues [5]. Extranodal marginal zone lymphomas (ENMZL) constitute a heterogeneous group ... Characterization of oral](https://img.pdfslide.net/doc/110x75/5af0b8a07f8b9ac62b8f041e/primary-extranodal-marginal-zone-bcell-lymphoma-palatal-soft-tissues-5-extranodal.jpg)