Embed Size (px)
Citation preview

Immunology and Cell Biology
(2003)
81
, 192–195
Research Article
Fc
γ
RIIA polymorphisms in
Streptococcus pneumoniae
infection
F A N G F A N G Y U A N ,
1
M E L A N I E W O N G ,
2
N A T A L I A P E R E R V A ,
1
J O A N N A K E A T I N G ,
1
A N D R E W R D A V I S ,
1
J E N N Y A B R Y A N T
1
a n d J O H N S S U L L I V A N
1
1
Australian Red Cross Blood Service-Endeavour, Sydney and
2
The Children’s Hospital, Westmead, New South Wales, Australia
Summary
Invasive pneumococcal disease continues to be a major cause of morbidity and mortality among childrenand adults worldwide. Effective host defence against
Streptococcus pneumoniae
depends on immunoglobulinG-mediated phagocytosis of the bacteria and it has been shown
in vitro
that the Fc
γ
RIIA polymorphism (Fc
γ
RIIA-R131
vs
Fc
γ
RIIA-H131) determines the capacity of immunoglobulin G2-mediated phagocytosis via this receptor. Inthis study, we evaluated Fc
γ
RIIA polymorphisms in children with pneumococcal sepsis and a number of controlgroups in order to investigate a possible association of Fc
γ
RIIA genotypes with
Streptococcus pneumoniae
infection. The distribution of the genotypes differed in these populations. The frequency of homozygosity forFc
γ
RIIA-R/R131 in the patients was significantly higher than that in the healthy random donor population (43%
vs
21%,
P
< 0.05). The frequencies of Fc
γ
RIIA-H/H131 were similar among all groups of individuals, while theincidence of the heterozygous Fc
γ
RIIA-R/H131 was lower (35%
vs
52%,
P
< 0.05). Thus, it appears that theFc
γ
RIIA-H131 polymorphic form, even in the heterozygous form, may be protective for pneumococcal sepsisand children with Fc
γ
RIIA-R/R131 genotype could be more at risk of infection with invasive
Streptococcuspneumoniae.
Key words
:
Fc
γ
RIIA, genotype, pneumococcal sepsis.
Introduction
Streptococcus pneumoniae
is the major cause of pneumoniathroughout the world and also a common cause of otitis media,bacteraemia and meningitis. Immunoglobulin G2 is the pre-dominant subclass of antibodies produced by the immunesystem in response to bacterial polysaccharide antigens
1,2
andthe Fc
γ
RIIA receptor plays a crucial role in the phagocytosisof IgG2-opsonized bacteria since it is the only receptor able tointeract with IgG2 antibodies. Fc
γ
RIIA contains allelic poly-morphisms (arginine ‘R’ or histidine ‘H’ at amino acidposition 131) with different capacities for IgG2 binding andphagocytosis, as the affinity of Fc
γ
RIIA-H131 for IgG2 ishigher than that of Fc
γ
RIIA-R131. These polymorphismshave been reported to be associated with phagocytosis of
Streptococcus pneumoniae
mediated by antipneumococcalsera
in vitro
, with much higher phagocytic activity for thehomozygous Fc
γ
RIIA-H/H131 cells than for the Fc
γ
RIIA-R/R131.
3–5
Phagocytosis of IgG2 opsonized pneumococci bypolymorphonuclear leucocytes is the main host defenceagainst invasive pneumococcal diseases, in view of theincreased susceptibility to infection with encapsulated bac-teria observed in children with low IgG2 levels
3
and in IgG2deficient individuals.
6
Because effective
in vitro
phagocytosishas also been shown to be associated with IgG2 levels and notwith IgG1 levels,
5
IgG1 anticapsular antibodies may be less
protective. Fc
γ
RIIA polymorphisms of pneumococcalpatients could contribute to an underlying susceptibility toinvasive
Streptococcus pneumoniae
infection. The dominantIgG1 isotype of anticapsular polysaccharide response in chil-dren could also contribute to an increased susceptibility toinfections with
Streptococcus pneumoniae
. Although theeffects of Fc
γ
RIIA genotypes have been studied
in vitro
usingIgG2-mediated phagocytosis of
Streptococcus pneumoniae
byneutrophils,
3–5
little is known about how such polymorphismsinfluence outcome in paediatric patients who actually havepneumococcal sepsis. In this study, we evaluated the Fc
γ
RIIApolymorphisms in paediatric patients from the Children’sHospital at Westmead, New South Wales, Australia, whowere suffering from pneumococcal sepsis with blood culturepositive for
Streptococcus pneumoniae
, and in blood donorswho have high levels of specific antibodies against pneumo-coccal polysaccharide. The aims of this work were to investi-gate whether Fc
γ
RIIA polymorphism is associated withsusceptibility to infection with
Streptococcus pneumoniae
andto study a possible correlation between the polymorphism andthe high level of antipneumococcal antibodies in exposed buthealthy individuals.
Materials and Methods
We studied a total of 63 paediatric patients (age range 1–118 months)who were diagnosed as having pneumococcal bacteraemia (bloodculture positive for
Streptococcus pneumoniae
), and 34 blood donorswho had high levels of antipneumococcal polysaccharide antibodiesby ELISA (unpubl. data). Two control groups consisted of 20anonymous children (2 months old) who were involved in a vaccine
Correspondence: Dr Fang Fang Yuan, Tissue Typing R & D,ARCBS-Endeavour, 153 Clarence Street, Sydney, NSW 2000, Aus-tralia. Email: [email protected]
Received 6 December 2002; accepted 4 March 2003.

Fc
γ
RIIA genotypes and
S. pneumoniae
193
program and 58 normal random blood donors regardless of theirpneumococcal antibody status. Informed consent was obtained fromblood donors as well as from patients’ parents/guardians according tothe guidelines of the Institutional Human Ethical Committee, Austral-ian Red Cross Blood Service and the Institutional Review Committeeof the Children’s Hospital at Westmead, Australia, respectively.
Sequence specific polymerase chain reaction (SSP) was per-formed to classify the Fc
γ
RIIA-R-H131 genotype. DNA wasextracted from whole blood using a standard salting-out procedure.The following pairs of primers were designed to amplify Arg or Hisallele of Fc
γ
RIIA gene: sense for Arg allele (5
′
-aaatcccagaaattctcccg-3
′
);sense for His allele (5
′
-aaaatcccagaaattctccca-3
′
); antisense for Arg orHis allele (5
′
-tgtccatcccctcttctcc-3
′
). A pair of amplification controlprimers was included in all PCR giving rise to a 796-bp fragment ofHLA DRB1 gene.
7
The PCR was performed by adding 1
µ
L DNAinto a 13
µ
L solution containing 67 mmol/L Tris Base pH 8.8,16.6 mmol/L Ammonium Sulphate, 2.5 mmol/L Magnesium Chlo-ride, 0.1% Tween 20, 200
µ
mol/L of each dNTP, 39 pmoles of eacholigonucleotide, 26 pmoles of each control primer, 1.5 U PerkinElmer's Taq polymerase (Roche Molecular Systems, Inc. Branch-burg, NJ, USA). The PCR conditions were as follows: 96
°
C for1 min; 5 cycles of 96
°
C for 25 s, 70
°
C for 45 s, 72
°
C for 45 s; 21cycles of 96
°
C for 25 s, 65
°
C for 50 s, 72
°
C for 45 s; 4 cycles of 96
°
Cfor 25 s, 55
°
C for 1 min, 72
°
C for 2 min; then a final extension at72
°
C for 10 min Amplified product was identified on a 2% agarosegel.
Statistical analysis
Data were analysed for differences in distribution of Fc
γ
RIIA geno-types among groups using the chi-squared test (2
×
3 contingencytables and
χ
2
analysis). Frequency of Fc
γ
RIIA genotype (e.g.Fc
γ
RIIA-R/R131
vs
combined Fc
γ
RIIA-R/H131 and Fc
γ
RIIA-H/H131) was compared among groups using Fisher’s Exact Test (2
×
2contingency tables, one-sided). Differences were considered signifi-cant when
P
< 0.05.
Results
The distribution of Fc
γ
RIIA genotypes and allele frequenciesamong the patients, blood donors with antipneumococcalantibodies and two groups of controls were analysed. Thedifferent Fc
γ
RIIA genotypes are illustrated in Fig. 1. Asdisplayed in Table 1, distribution of Fc
γ
RIIA genotypes(Fc
γ
RIIA-R/R131, Fc
γ
RIIA-R/H131 and Fc
γ
RIIA-H/H131)among 63 patients was 43%, 35% and 22%, compared with30%, 50% and 20%, respectively, among control children(
P
> 0.05), as well as compared with 21%, 52% and 27%,
respectively, among normal random blood donors (
P
< 0.05).The frequency of the R/R131 genotype was higher in patientsthan in other groups, although the difference reached statisti-cal significance only between patients and normal randomblood donors (43%
vs
21%,
P
< 0.05). The frequency of theR/H 131 genotype was lowest in patients (35%), was low inblood donors with the antibody (41%) while control childrenand normal random blood donors were in higher frequenciesof the R/H 131 genotype (50% and 52%, respectively), whilethe difference reached statistical significance only betweenpatients and normal random blood donors. The frequencies ofH/H 131 genotype were similar among all groups of individ-uals. There was variation at the allele frequency level, how-ever, there were no significant differences between the groups.
Discussion
Although the effect of Fc
γ
RIIA polymorphisms on the
in vitro
phagocytosis of
Streptococcus pneumoniae
has been studiedextensively and the
in vivo
studies reported by Yee’s groupshowed an association with bacteremic pneumococcal pneu-monia,
8
little is known about its influence on clinical outcomein paediatric patients with pneumococcal septicaemia and ifthere is an association in individuals with high levels ofantibodies against pneumococcal polysaccharide but withouthistory of pneumococcal pneumonia. The association ofFc
γ
RIIA genotype with
Streptococcus pneumoniae
infectionwas evaluated in this study. Our results show that paediatricpatients with pneumococcal sepsis display a high frequency
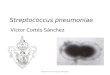
Figure 1
Sequence specific polymerase chain reaction (SSP)genotyping of the Fc
γ
RIIA gene. Example of SSP genotyping ofthe Fc
γ
RIIA gene was demonstrated in eight subjects. (a) R131allele specific amplification (low band, 188 bp). (b) H131 allelespecific amplification (low band, 189 bp). Positive control ampli-fication, HLA DRB1 gene (high band, 796 bp).
Table 1
Distribution of Fc
γ
RIIA genotypes and allele frequencies in patients with
Streptococcus pneumoniae
(SP) and control groups
Genotype
n
(%)* Allele frequency R/R131 R/H131 H/H131 R131 H131
Children with SP (
n
= 63) 27 (43%) 22 (35%) 14 (22%) 0.60 0.40Blood donors with anti-SP antibody (
n
= 34) 11 (32%) 14 (41%) 9 (27%) 0.53 0.47
Controls:
Healthy children (
n
= 20) 6 (30%) 10 (50%) 4 (20%) 0.55 0.45Normal random blood donors (
n
= 57) 12 (21%) 30 (52%) 16 (27%) 0.47 0.53
*Difference of genotype distribution between patients with SP and normal random blood donors was significant (
P
= 0.03); in comparisons withnormal random blood donors, frequencies of Fc
γ
RIIA-R/R131 versus non-Fc
γRIIA-R/R131 and FcγRIIA-R/H131 versus non-FcγRIIA-R/H131among patients with SP showed significant differences (P = 0.008 and 0.046, respectively).

194 FF Yuan et al.
of the FcγRIIA R/R131 genotype but a similar distribution ofH/H131 to control groups. This suggests that FcγRIIA poly-morphism could be important in the defence against invasivepneumococcal infection in vivo, and this is in agreement withYee et al.8 who have found that patients with bacteremicpneumococcal pneumonia have much higher frequency of theFcγRIIA-R/R131 genotype.
Furthermore, the frequency of R/H131 genotype is signif-icantly lower in our patient group, apart from similar fre-quency of H/H131 genotype among the patients and thecontrols, may suggest that the FcγRIIA with H131 allele, evenin a heterozygous form, could have a protective role inStreptococcus pneumoniae infection. Rodriguez et al. showedthat FcγRIIA-H/H131 homozygous polymorphonuclear cells(PMN) and cells transfected with FcγRIIA-H/H131 genewere better able to phagocytose the opsonized Streptococcuspneumoniae in vitro than FcγRIIA-R/R131 cells.4 In vitro,FcγRIIA polymorphisms have been shown to be important inthe defence against other encapsulated bacteria such as groupB type III streptococci,3 and also it has been shown that theH/H131 genotype may be protective in infection with severemeningococcal diseases,9 while the R/R131 genotype isrelated to more severe forms of meningococcal disease.10,11
Furthermore, the frequency of FcγRIIA-H/H 131 phenotypewas shown to be significantly lower in 48 paediatric patientswith recurrent bacterial respiratory tract infections comparedto the controls.12 In those pneumonia patients with theFcγRIIA-H/H 131 genotype, other factors may contribute tothe development of pneumococcal pneumonia such as thelevel of specific antibody since IgG2 deficiency could alsoincrease the risk of pneumococcal diseases, although thispossibility has not been investigated in our patients.
Despite the increased invasive pneumococcal infectionsfound among HIV infected individuals, it does not appear tobe associated with FcγRIIA genotypes. Increased susceptibil-ity to Streptococcus pneumoniae is thought to be caused by adecrease in their serotype-specific immunoglobulin gene VH3expression.13 HIV infected individuals are more vulnerable toall infections because of their overall poor immune response.It was also found that the genotypes did not contribute topneumococcal infections in African American children withsickle cell disease.14 In contrast to the groups in these otherstudies, pneumococcal pneumoniae is the primary disease inour patient group and our findings directly indicate an associ-ation between susceptibility to infection with Streptococcuspneumoniae and polymorphisms in the FcγRIIA gene.
The difference in distribution of FcγRIIA genotypesbetween blood donors with high levels of specific antibodyand random blood donors did not reach statistical signifi-cance, therefore, this polymorphism may not influence thelevels of antipneumococcal antibodies present in this group ofblood donors. Although the IgG2 antibody levels have beenreported to be related to G2m allotypes,15 the high affinitygenotype (H/H131) was found to have lower IgG2 levels.16 Itwas also shown that not all high levels of specific antibodiesby ELISA correlated to high functional titres,17,18 therefore,whether the low affinity genotype (R/R131) is correlated tohigh functional titre of the antibody requires further investiga-tion. However, the high antibody levels in these blood donorsmay reflect an earlier exposure to Streptococcus pneumoniae.The higher frequency of R/R131 and lower frequency of R/H,
in comparison with normal random blood donors, maysuggest they could be susceptible to pneumococcal infectionsin less severe forms. It may also suggest that individualscould compensate for the less favourable genotype R/R131 bymaking much more antibody in order to achieve equivalentfunctional activity. A similar lack of association of R/R131genotype and moderate systemic meningococcal disease hasbeen reported.9,11
FcγRIIA genotypes exhibit ethnic variation with anincreased frequency of the H/H131 in Japanese and Chinesepopulations compared with Caucasian populations.19 Distri-bution of FcγRIIA genotype in Sydney blood donors is verysimilar to that among other Caucasian populations, includingDutch, German and American populations and among Afro-Americans.19 In this study the frequency of the FcγRIIA R/R131 genotype was slightly but not significantly higher in thechildren’s control group than in normal random blood donors(30% vs 21%, P = 0.28). These children were relativelyhealthy but their susceptibility to other infections was notinvestigated.
In summary, our present finding suggests that childrenwith the FcγRIIA-R/R131 genotype could be more at risk ofinvasive Streptococcus pneumoniae infection and individualswith the FcγRIIA H-131 polymorphic form could be moreprotected from invasive pneumococcal diseases. Prospectivestudies to evaluate the level of functional specific antibodiesin pneumococcal patients with different FcγRIIA genotypeswill more fully clarify the relationship of FcγRIIA genotypesto clinical outcome in at risk patient groups.
Acknowledgements
This work was supported in part by a grant from the Cooper-ative Research Centre for Vaccine Technology. The authorswish to thank Jonathan Moses for assistance with PCR primerdesign.
References
1 Jefferis R, Kumarartne DS. Selective IgG subclass deficiency:quantification and clinical relevance. Clin. Exp. Immunol. 1990;81: 357–67.
2 Siber GR, Schur PH, Aisenberg AC, Weitzman SA, Schiffman G.Correlation between serum IgG2 concentrations and the antibodyresponse to bacterial polysaccharide antigens. N. Engl. J. Med.1980; 303: 178–82.
3 Sanders LAM, Feldman RG, Voorhorst-Ogink MM et al. Humanimmunoglobulin G (IgG) Fc receptor IIA (CD32) polymorphismand IgG2-mediated bacterial phagocytosis by neutrophils. Infect.Immun. 1995; 63: 73–81.
4 Rodriguez ME, van der Pol WL, Sanders LAM, van deWinkel JGJ. Crucial role of FcγRIIa (CD32) in assessment offunctional anti-Streptococcus pneumoniae antibody activity inhuman sera. J. Infect. Dis. 1999; 179: 423–33.
5 Jansen WTM, Breukels MA, Snippe H, Sanders LAM,Verheul AFM, Rijkers GT. Fcγ receptor polymorphisms deter-mine the magnitude of in vitro phagocytosis of Streptococcuspneumoniae mediated by pneumococcal conjugate sera. J. Infect.Dis. 1999; 180: 888–91.
6 Abadi J, Zhong Z, Dobroszyzki J, Pirofski LA. FcγRIIa poly-morphism in human immunodeficiency virus-infected children withinvasive pneumococcal disease. Pediatr. Res. 1997; 42: 259–62.

FcγRIIA genotypes and S. pneumoniae 195
7 Bunce M, O’Neill CM, Barnardo MC et al. Phototyping: com-prehensive DNA typing for HLA-A, B, C, DRB1, DRB3, DRB4,DRB5 & DQB1 by PCR with 144 primer mixes utilizingsequence-specific primers (PCR-SSP). Tissue Antigens 1995; 46:355–67.
8 Yee AMF, Phan HM, Zuniga R, Salmon JE, Musher DM.Association between FcγRIIa-R131 allotype and bacteremicpneumococcal pneumonia. Clin. Infect. Dis. 2000; 30: 25–8.
9 Platonov AE, Shipulin GA, Vershinina IV, Dankert J, van deWinkel JGJ, Kuijper EJ. Association of human FcγRIIa (CD32)polymorphism with susceptibility to and severity of meningo-coccal disease. Clin. Infect. Dis. 1998; 27: 746–50.
10 Bredius RGM, Derkx BHF, Fijen CAP et al. Fcγ receptor IIa(CD32) polymorphism in Fulminant meningococcal septic shockin children. J. Infect. Dis. 1994; 170: 848–53.
11 Domingo P, Muniz-Diaz E, Baraldes MA et al. Associationsbetween Fc gamma receptor IIA polymorphisms and the risk andprognosis of meningococcal disease. Am. J. Med. 2002; 112:19–25.
12 Sanders LAM, van de Winkel JG, Rijkers GT et al. Fcγ receptorIIa (CD32) heterogeneity in patients with recurrent bacterialrespiratory tract infections. J. Infect. Dis. 1994; 170: 854–61.
13 Abadi J, Freiedman J, Jefferis R, Rodriguez-Barradas MC, Pirof-ski L. Human antibodies elicted by a pneumococcal vaccineexpress idiotypic determinants indicative of VH3 gene segmentusage. J. Infect. Dis. 1998; 178: 707–16.
14 Norris CF, Surrey S, Bunin GR, Schwartz E, Buchanan GR,McKenzie SE. Relationship between Fc receptor IIA poly-morphism and infection in children with sickle cell disease.J. Pediatr. 1996; 128: 813–9.
15 Konradsen HB, Oxelius V-A, Hahn-Zoric M, Hanson LA. Theimportance of G1m and 2 allotypes for the IgG2 antibody levelsand avidity against pneumococcal polysaccharide type 1 withinmono- and dizygotic twin-pairs. Scand. J. Immunol. 1994; 40:251–6.
16 Parren PW, Warmerdam PA, Boeije LC et al. On the interactionof IgG subclasses with the low affinity FcγRIIa (CD32) onhuman monocytes, neutrophils, and platelets. Analysis of a func-tional polymorphism to human IgG2. J. Clin. Invest. 1992; 90:1537–46.
17 Johnson SE, Rubin L, Romero-Steiner S et al. Correlation ofopsonophagocytosis and passive protection assays using humananticapsular antibodies in an infant mouse model of bacteremiafor Streptococcus pneumoniae. J. Infect. Dis. 1999; 180: 133–40.
18 Vernacchio L, Romero-Steiner S, Martinez JE et al. Comparisonof an opsonophagocytic assay and IgG ELISA to assessresponses to pneumococcal polysaccharide and pneumococcalconjugate vaccines in children and young with sickle cell dis-ease. J. Infect. Dis. 2000; 181: 1162–6.
19 Van der Pol WL, van de Winkel JGJ. IgG receptor poly-morphisms: risk factor for disease. Immunogenetics 1998; 48:222–32.