Embed Size (px)
Citation preview

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 1
FUNCTIONAL NEUROLOGY ANATOMY AND CENTRAL NEUROLOGICAL PATHWAYS (MODULE ONE)
Transcript – Cerebellum
Presentation by Dr. Brandon Brock
Okay, good morning everybody. For those of you, wherever you may be, maybe it’s evening time where you’re at; I don’t even know. So whether you’re in a different country, streaming, here with us…
We had a good time last night, we had a good time yesterday. Thank you for the pictures that people have been posting, that have been very entertaining. Please post more. It’s cool just to see, kind of, your environment.
Yesterday we took you on this journey through the paradigm. The thought process. How do you determine a functional condition versus a pathological condition? How do you look at cell types that need to be activated? When is a metabolic factor going to come into play?
What’s really going to be fun is in the coming months when we teach you: “Hey, if you think that metabolic factor’s there, this is how you work through it. And if you think that they’re overlapped, this is the one you do first, then this is the one you do second, then this is the one you do third.”
So teaching people how to prioritize those factors, and layer those factors, makes this a blast. And it really does make it an art. So when you have that person that has functional neurological capacity that’s been destroyed or damaged, or somehow compromised, you can now say, “I know where the problem is, and I can either directly activate it or indirectly activate it. And if there’s a roadblock in the way called a metabolic condition, I can work on that. And if there’s multiple metabolic conditions, I can work on all of them in a systematic fashion.”
And as you go through that, you can use your skill set.
So you’ve got to… unfortunately you’re cross-training a little bit. That’s what this whole program is going to be. It’s an integrated neurological approach, which makes it a million times more fun, at least for me. That’s my opinion, okay? It may not be fun for you. I hope it is, okay?
We’re going to give you a bigger story, a bigger picture. And we’re going to fill in more holes, and fill in some blanks that you may have if you’re just doing one or the other. And I think that’s what the whole complementary system is designed to do.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 2
So as we did this yesterday, we talked about the individual cells, the ability for the cell to make energy, to have mitochondrial function, to not have free radical damage. And then we talked about receptor types. They can either make things go good or go bad. And NMDA receptors.
Can somebody shut that door in the back? Thanks.
NBDA receptors can either activate the gene response with plasticity, or if too much calcium comes in, it can start to destroy the cell. Now, there are certain neurodegenerative medications that stop those NBDA receptors from allowing too much calcium influx to come in. I think I can say it – there’s a drug called Namenda. And it’s used in the degenerative population, and it stops those NMDA receptors from allowing calcium to come in. There’s a magnesium plug on these receptors, and that’s why we use a lot of magnesium sometimes to slow down excitotoxicity. It’s even used in some seizure types of events. For example, with pregnant women, or those who are in labor, sometimes they’re use, you know, magnesium of a variety of types to actually slow down, you know, hypertension that can turn into eclampsia that can turn into a problem.
So sometimes we have to recognize the fact that those cells need to be stabilized while they’re being activated, so that they don’t become erratic. But for the most part, when it comes to neurology, we’re learning how to say, “This is your cortex,” and if it’s frontal, it looks like this. And you have a general idea of that. And if the frontal system is starting to decay, or dysfunction, or spire fontaneously – spire fontaneously, that’s a paraphasic error! – if it’s starting to fire spontaneously, then we know what it looks like. We know what seizure activity looks like. We know what epileptiform activity. We know what it’s starting, you know, to become from a clinical perspective. Same thing with parietal lobe, same thing with temporal lobe, and then even occipital lobe. Occipital lobe is not quite as prone, even though occipital lobe is very prone for migraines. That’s why a lot of people have optical, you know, prodromes, where they actually see, like, little spots and stuff like that.
So we’re kind of setting the stage now, to go down a little bit deeper. So we were going to go from the rooftop down. So we’re going to do basal ganglia today. Dr. Kharrazian’ll do that. I’m going to do cerebellum today, right now, and then I’m going to start you on the vestibular system, and I’m going to make sure you understand all ocular movements. My kids painted me some eyeballs. This one right here has a little bit of damage to the pupil, but that’s okay. They wanted to participate.
So, I’ll teach you what muscles do what, really quickly, and you can just run through that. We cannot get you into ocular training, optokinetics, eye exercises and all that stuff if you don’t understand which canal is linked to which muscle, to which eye position. So I’m going to spend quite a bit of time doing that today with you as well.
So today, for me, it’s cerebellum, and then the vestibular system. Down lower. Dr. Kharrazian’s going to bring a lot of the basal ganglia into it, and we’re going to end the day pretty much the same way we did yesterday, where we summarize the whole weekend for you, and then we answer a few more questions, and then we’ll be gone, but we’ll give you some homework assignments too. And a lot of the homework assignments will be posted on the member section.
So you see, it’s an ongoing journey. I want everybody to understand that right from the get-go. It’s an ongoing journey from the cell to the cortex to the areas to the subcortical areas to the whole orchestration. We move down, and we say, “How do we evaluate it next module, then we move to other systems, and we go all the way through things like neuro-autoimmunity, and the spinal cord, and the peripheral nerve, and peripheral nerve conditions, and many, many, many therapeutic modules. And every time I see a weak spot, we’ll just make a little video.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 3
Alright, so we have a lot of work to do, but the work will be up there for you. Alright?
Okay, so off we go into cerebellum land. Everybody grab your cerebellum. You probably can’t; there’s skull [in the way]. But it’s in the back. It’s at the base of the brain. So we know it’s used for all [sorts of] things. The old-school thought used to say things like this: “The cerebellum is one hundred percent just used for motor function.” But we know as we go more lateral in the cerebellum, it’s also used for coordination of thoughts, coordination of planning, and it loves to go to the contralateral frontal lobe, and it runs through the midbrain. So it goes brbrbrbrp, and it goes over to the contralateral frontal lobe, and the frontal lobe depends on it, because the frontal lobe has to do this: coordinate all motor output. And by the way, some of your motor output is the execution of planning.
So the cerebellum says, “Hey man, look. This is how you did it before. Let me tell you how you can do it again without hitting your own thumb with a hammer. Change your trajectory a little bit this way, stop on the target here.” See, the cerebellum loves to give you enough information to where you can start and stop, just like that. It’s not necessarily the total initiator, like what we see with the frontal eye fields, but it controls a lot of stuff in the brainstem.
So look at it like this: The brainstem is just a factory, and it’s got a lot of factory workers in it. They’re called nuclei, right? Cranial nerve nuclei. They have a midlevel manager that comes over and kind of looks at them, some of them. It’s called the cerebellum. And then we have corporate, and that’s called the cortex. And the cerebellum communicates with corporate, and corporate says, “Hey, good job.” Or the corporate says, “I don’t know if this is going to work.” But sometimes the midlevel manager can give corporate the wrong message, so the whole thing dysfunctions, and you have things like dysmetria, or dysdiadochokinesia. And by the way, you can even have dysmetria of thought, not just movement.
So what we’re finding is this: The cerebellum has everything to do with cortex, and the cortex has a lot to do with cerebellum, and the cerebellum is the guy that organizes it and says it needs to change, it needs to be different, it needs to be faster, it needs to be slower, it needs to fire down to give tone to your spine, it needs to fire to give you certain activation of your eyes. We don’t want our eyes jumping back and forth because they can’t fixate on a target, because as soon as they go over here and you realize it, it’s got to go back over here, and then you start getting oscillations.
So I’m going to go through a load of terms and what they mean, and show you how to test them. Because this is really a big area for what a manual therapist does. For those of you that are chiropractic, cerebellum is everything. Cerebellum can create all kinds of posturing abnormalities, it can create tremors, it can create abnormal thoughts. And when you do your frontal lobe questionnaires and evaluations that we’ll give you, you’ve always got to think: “What does the cerebellum doing?” And if you go back and you have a lot of cerebellar problems and a lot of frontal problems, you’ve got to think to yourself, “I wonder if the cerebellum is contributing to the frontal problems?”
And then you may have to take it a step back and say, “Wow, this person’s cold, gaining weight, losing their eyebrows. I wonder if they have, you know, some sort of metabolic condition?” And you check their thyroid, and you realize they have TG and TPO antibodies, and they have Hashimoto’s, and their TSH is 95. And so they’re starting to go downhill. And then you realize, “Wow, man, I wonder if that thyroid has anything to do with their neurological function?” And then you find that they have some sort of cross-reactivity, or some sort of development of a cerebellar antibody. So then you go, “Wow, there cerebellum is being affected by a metabolic condition, and that metabolic condition is something that’s being affected by autoimmunity.” And because of all of that, their frontal lobe is an innocent secondary bystander of a decrease of cerebellar function because of the autoimmunity.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 4
And then you take it a little bit further, and you’re like, “Wait a minute, they’re not even absorbing B vitamins, because they have hypochlorhydria, because T4 has a lot to do with production of stomach acid. So the story builds and builds and builds. We give you one layer. Learn it. We give you another layer. Learn it. Some of you are going to be like, “Oh, I love that stuff. I’ve been to a thyroid class,” and some people are going to say, “Oh, I love that. I’m a neurology diplomate. I already know that.” You may know parts of it, but we’re going to start integrating it more and more and more as we go. Okay?
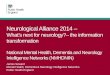
So. This is the cerebellum, right here. And you can see it integrates right… I’m sorry, no laser pointer. You’re going to have to tell me that again, see? Hey look, I’m learning. If you look right here it just integrates… this isn’t a very good picture; this is just sort of a real specimen here that you can just see how it just kind of goes right off the back of the brain stem, and it integrates right into this pontine area.
So today we’re going to do these. These are going to be my goals.
We’re going to do… review the anatomy, mainly the layers and the nuclei, and what do they mean, and why do they do what they do. What do basket cells do, what do stellates, what are purkinjes, what’s fastigial, globose, emboliform, dentate? We’re going to talk about what all of those are, what they do, and why the cerebellum is organized the way it is.
And then I’m going to review the physiology with that anatomy, and within that review of physiology and anatomy, we see pathology. So I’ll explain the pathology in the middle of the story of saying, “This is how it works.”
And then every module from here on out, there’ll probably be a mention of the cerebellum. I can just probably tell you that. Because it’s one of those areas, if there’s deafferentation, it gets hammered. If there’s blood sugar problems, it gets hammered. If there’s autoimmunity, it’s very prone. If somebody gets spinal cord damage, it starts to be deafferentated.
There’s all kinds of genetic issues. I’ll tell you right now: if someone walks in with ataxia, here’s a clinical gem for you. If somebody walks in with ataxia, an ataxic gait, so it’s like they can’t walk on a tightrope, and you’re like, “Man, this looks cerebellar,” they finger-to-nose, dysdiadochokinesia, they have ocular problems, and you’re like, “This is ataxia” – and don’t worry, we’re going to talk about ataxia a lot – the first thing I do is, I say, “Take off your shoes.” Take off their shoes. If it’s, you know, some sort of inherited type of problem, they’ll have high arches and hammertoes a lot of times. You go back out to the lobby, you ask everybody and their family to take their shoes off, and half of them have it and half of them don’t. And you’re like, “Drn-drn-drn-drn-drn.” You know, you start playing the banjo.
Well, if they don’t have that, then you have to say to yourself, “Hey, are you a drinker?” And you look on their nose and see if they have busted petechiae, and see if they’re starting to get really thin legs. If they’ve been replacing booze for food for more than nine months, the anterior lobe of the cerebellum starts to deteriorate, and your lower extremities become affected more than your arms.
Well, if that’s not there, then I start asking them questions like this: “Hey, how’s your gut feel?” “My gut feels terrible.” “Well, what do you mean?” “Well, every time I eat something it makes me feel… makes my joints hurt, my stomach hurts every time I eat.” And so now you start thinking, “Wait a minute. Could there be a gastrointestinal link to their cerebellum?”
Now, I need you understand that in ninety-nine point nine percent of the world of the medicine, that is considered a vast leap. But in the world of the literature, it’s not a vast leap. So now you do things, and you say, “Hey look, are you just inflamed? Because maybe you have dendritic cell sensitization? Sure,

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 5
maybe you have some sort of a leaky gut, or do you actually have celiac disease and do you have tissue transglutaminase-6 antibodies which go to the brain, and the cerebellum suffers tremendously.
Well, maybe you don’t have any of that. And maybe you just have SCA – spinal cerebellar atrophies. We’ll talk about all of them and how to test them. You will have ataxic patients. I just want to tell you: You do this work long enough, you’ll have ataxic patients, and I want to give you a way to rip through the differentials.
You see, we’re not at the point yet where we can really play the differential diagnosis game very well, but what we’ll start doing every morning to warm up is, we’ll spend thirty minutes doing the differential diagnosis game. And I’ll just say, “Patient has this, this, and this. What do you think?” And we’ll run through the whole previous module in fifteen minutes, just by doing that little sort of dance. So we can keep the song going, continuous.
This portion of the brain, if you’re in natural medicine, if you’re in functional medicine, if you’re in neurology of any type and you have a semi-busy day, you will see cerebellar aberrancies all the time. The good news about it is this. It’s very plastic, it recovers well, as long as you get away the offending metabolic agent. Otherwise don’t count on it. Okay?
So what do you see? And by the way, we’re not here to make you a neuro-radiologist. Let the neuro-radiologist read the images, and then you get the images and look at them, please. Is that fair enough? They’ll just give it to you on a CD now.
Okay, first of all, right here: how does this cerebellum look? Right here? Okay, that’s not the cerebellum, right? Just checking to make sure everybody’s awake. Is this the cerebellum? Okay. That’s not exactly what I would call a super-duper ballin’ cerebellum. That’s more like this: atrophied, a little bit of it. Now, you’ve got to remember, certain slices will look different as you go through it. But you start to see some of the fullness of the cerebellum is starting to be lost. Volume loss. Sometimes the tonsils will herniate down, sometimes you’ll get a Chiari malformation. We will go through all of those things later on.
So the anatomy of it is, there’s different regions. And I like to just kind of break it up not by giving you every single external landmark, because that’s very academic. What I want to do is give you the zones, and talk about what the zones do, and then how they control function and what that looks like pathologically.
So, the cerebellum is basically divided into a midline region, and intermediate region, and a lateral region. And then right in the middle we have fastigial nuclei. And then we have a vermal region down below. And then we have a nodulus, which is a little bump. And then outside of the vermal region, we have an inter-mediate region that has two nuclei. They’re called the interposed nuclei. It’s the globus and emboliform.
And then we go a little bit more lateral and we have this awesome thing called the dentate system. The dentate system develops with language, with frontal lobes, and it gives the frontal lobes the ability to have some organization, some semblance, and execution of planning in an appropriate fashion.
So, the frontal lobe has a sidekick called the cerebellum. And it really wouldn’t be all that great of a frontal lobe if it didn’t have it. Now, for those kids that don’t get out and get active, and they don’t develop their cerebellum , because activation and running and playing and doing all those things makes your cerebel-lum develop. The cerebellum goes right up to your mesencephalon, and that makes dopamine. And then dopamine, through the reticular activating system on the front, fires right up to the frontal lobe and it goes whoooh, and it activates. So, we have noradrenergic and we have dopaminergic activation, and then we have cerebellar projections to their frontal lobe, and it all starts to develop. And the frontal lobes inhibit impulsivity and give us attention. So now do you see why it’s important to get kids out and run and play and do things?

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 6
I mean, this is sort of like pediatric treatment 101. Of course, the more specific it is, and the more novel it is, and the more engaged it is, the better it is. But here’s what we’re finding: lots of neuro autoimmunity in these pathways that keep them from doing what they’re supposed to do with activation. Did you hear what I just said? We are finding roadblocks to activation of these pathways.
So let me just step back for a second, and say, “Remember what I just said? The cerebellum fires into the brainstem, and the pons and medulla are highly serotonergic with the raphe nuclei. You go up to the roof of the brainstem, and in the front of the mesencephalon is where dopamine is made, to go to the basal ganglia that Dr. Kharrazian’ll talk about later on, that will give you motor function. And if you go just inside the substantia nigra pars compacta.
There’s the mesolimbic nuclei, where now dopamine goes up to the nucleus accumbens – remember that guy I told you yesterday, it makes you happy? Well, whenever it goes up, regardless, that striatal palatal pathway fires up to the frontal lobe, and it goes, “Hey, frontal lobe, be activated.” The cerebellum activated the brainstem, the brainstem said, “Hey frontal lobe, be activated,” and there’s certain medications that make that dopamine more prevalent. They’re called ADD drugs. What they do is, they drive dopamine up to the frontal lobe, and everybody’s like, “Why would you want to activate a brain in a kid that’s hyperactive?” Because the higher-functioning brain allows you to dampen the output of the overactivity. This is also why people get hooked on things, because dopamine is a very, very happy thing. If you don’t have it, you get road rage. Maybe if you have too much you get road rage. Maybe you just have road rage. I don’t know.
So, we have the vestibulocerebellum. This is the flocculonodular lobe – I’ll show you a picture in a second – but it fires into the vestibular system and the fastigial nuclei. So really, here’s these midline nuclei, and what they do is this: They fire in to give you eye function, so if you have vestibular function, if I move my fun, I have a vestibulo-ocular response, which I’m going to describe to you in so much detail, you will know it really well. And how to use it therapeutically and how to use it diagnostically.
But when you have a vestibulo-ocular response, you have to remember that not all of these canals are perfect, and not everything is perfectly aligned like you see in a book. So the cerebellum comes around, and it calibrates everything to be appropriate for what your brain perceives as your reality. If you lose the cerebellum, you don’t get that any more, so now all your vestibular activity becomes in error. It’s just not perceived right. Or maybe your eyes don’t move right. Or maybe you lose the smoothness of movements. We’ll go through what all those are. But that midline area controls your eyes, it controls that vestibular system, it also fires down and starts to control the tone of your spine. So people that start to get really poor core musculature, my question is: Is that a reflection of the midline cerebellum? We’ll show you how to test it.
Is that making sense?
So for years – and I’m going to go to the chiropractic profession, and I know not everybody’s a chiropractor, but it’s a manual therapy thing. How has it really worked? Has it really taken a bone off of a nerve? Probably not. But what it has done is afferentated a system. And when you afferentate it, it can recalibrate, activate those nuclei that come down, those vestibular systems that come down, and then it reactivates tone, and then your perception changes, and now you don’t get the proprioceptive error of a segment, and you don’t subluxate, which is probably more than likely a movement disorder.
That’s a pretty deep concept. Trust me, it’s going to get a little bit easier. I’m giving some of you that are just starting out in the morning a little bit of a very polite jumpstart.
So, when we do this, we’ve got to remember that the vestibulocerebellum goes to the vestibular system, the spinocerebellum has a lot to do with the fastigial system. Now it goes out a little bit more lateral to

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 7
the interposed nuclei, and it receives some input from the periphery. And then the cerebrocerebellum, it actually goes to the cortex. And one hemisphere of the cerebellum will communicate with the other, and they will talk to each other about what’s going on.
If you take the cerebellum, and you take it and stretch it out and lay it flat, it will have the same surface area as one hemisphere. And it probably has more nuclei in it than any other region of your brain. The cerebellum is the little brain. Many, many creatures that aren’t as – and I’m not going to use the word ‘evolved’ because I don’t know what you believe in – but that are not as sophisticated neurologically as us, they have a mesencephalon and a cerebellum and very little cortex. The bigger you get this way, that’s why you usually see, like, cartoon characters, they have this giant, like, head, I guess they think that the bigger your frontal lobe is, the more, you know, you’re from another part of the world, or universe. You’re going to be smarter.
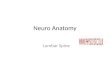
So here it is. You can see this midline vermal region, and then you can see this paravermal region, and look at this gigantic lateral hemisphere. So this is vestibular, vestibulospinal, and then – let me go back – cortical. As you come here, this is the cerebellum taken off and looking at it, and you again can see the vermis as it comes through. These right here are the tonsils. These will sometimes herniate down to the foramen magnum, and as we go back – let me get a lateral view for you.
This right here is your anterior cerebellum to your legs, this is the big outer area right here which goes to the cortex, and all of this stuff goes to midline structures: eyes, spine, parasympathetics, you know, brainstem everything. Right in here.
So these are the people you heard Dr. Kharrazian talking about yesterday. They’re up on their feet, and twenty-five minutes later, they’re like this: “Oh God. Pfblpfbl. I’ve been to the mall for thirty minutes with my wife. I feel like I’m gonna die.” And she’s over there like this: “ch ch ch, flipping through everything.” You’re like, “God, I hate her midline cerebellum. Mine sucks. It’s time to get in the gym and do some core stability exercises.”
I mean, listen. There’s been so much talk about a specific eye movement doing this, or a specific eye movement doing that, and getting this and getting that. We’ve found this: frontal lobe activity gives you the ability to fixate, period. Doesn’t really matter which direction you go. And when you have good core stability, and it fires up to the cerebellum, and it recalibrates all those nuclei, they do better.
So core stability in midline cerebellar function is great. So we’re going to teach you how to do some of these tests standing and lying. Because it might go from the midline to the intermediate. And then we’re going to teach you how to do very, very brought-in distal types of things. The hand is very cortical and very dentato. From here to here is very interpose. Here and here is very fastigial. So look at it, and it’s not hard. The midline cerebellum goes to the midline body. The intermediate cerebellum goes to the intermediate body. The lateral cerebellum – these are your hands, folks.
When you watch a baby, you know when they’re going to learn to talk, because they start using their hand. As soon as they start using their hand, they’re developing the areas right around Broca’s, and boom! they start to talk. Now, why in the world would they even get to that? The very first thing they do is, they hold their head up and they’re like this [wobbles head]. You know, you’ve seen… everybody’s… who here has kids? I’ve had two. I was scared to hold the first one, because I was way too young. Then I got into pediatrics, and I would, like, swing ’em around by one leg, you know? But the kid’s sitting there like this, you know, and they can just look at you, and their pupils aren’t reacting. And then over time, they get that ability to hold themselves upright. So now the midline cerebellum is like, “Woo hoo, we’re being activated! This is great!”

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 8
So, areas 3, 4, and then all the way down to areas 12 and 6, they’re all activated. Tongue. And those are all in an embryologic, homologous column with your ventral horn cells that give you intrinsic muscle tone of your spine. Non-volitional. So you’re just upright, and you’re like, “Cool.” Baby can hold their head up, and now they’re starting to sit, and they don’t fall over, and now they can start to use their arms. Now, when they start to use their arms, their vermal region is now spilled over to the interpose region, and activated it, and now they’re going to start to use their shoulders, but their hands are like this [holds hands flat out to sides]. Now, And they can’t, you know… they move really slow. But they’re using their shoulders, and they’re using their hips.
Then you put them on their belly, and they learn to do things like pull their knees up, and they develop curves, they learn to lift their head up so they’re developing their cerebellum even more. And then as soon as they can get up, sit up, recognize you, and perceive information posteriorly, the back of the brain and the cerebellar regions start to orchestrate into a ventral stream, and it comes up to the cortex, and now the dorsolateral system starts to activate and the kid says this: “I want macaroni and cheese, and I want to grab a fork.” So the dentate system kicks in, and it grabs a fork, and it goes, “Nom, nom, nom.”
And they know how to chew because it’s already a reflexogenic activity. So when you learn,… when I teach you later on pediatric stages of development, I’m just going to teach it to you through “How does the cerebellum develop it?” And by the way, when that frontal lobe develops, it comes down and you have all your corticoreticular fibers, now we have 5, 7, 9, and 10. They all develop. 5, 7, 9, 10. They’re all a little bit lateral to 3, 4, 6, and 12. I’ll draw out the brainstem. I’ll show you how to draw the motor, the sensory, the top, the bottom, all of it. You can do it in ten minutes.
Okay. So when that cortex develops, you can now make saliva, you can now chew, you can now swallow, you can now digest, and you now get vagal function. Cool. That means your guts are starting to develop, that means, when you have descending vagal function, that your P450 system is starting to biotransform out bad things. That means your spleen is starting to help control and regulate your immune system and your cytokines. That means your gut’s starting to move and you’re pushing things through, and you’re developing a microbiota.
The cerebellum is part of all of it. It helps us develop, and it helps the cortex develop. And if we can learn to dice it apart, it’s not so scary. So here it is: beautiful, beautiful, beautiful, from the side. Now, does this look like the picture I showed you a minute ago? Of the real one? No. That person was suffering, from something. Deafferentation. Antibodies. Inherited. We don’t know. But right here we have this nice fat anterior lobe, we have this nice posterior region, we have our fissures that you can see, but they’re not too deep. And it fires right into… there’s three peduncular systems, or there’s three arms. They come in to the brainstem, one down low, one right here, one up high. And I’ll show you more about those in just a little bit.
So check it out. Here’s the vermis. Here’s the fastigial nuclei. Here’s the intermediate hemisphere; this is where the interposeds are. And then here’s lateral; this is where the dentate is. Look at this. Spinal and trigeminal inputs, right in here.
Now, the cerebellum also does things like calm anxiety, reduce sympathetic stress. And when you do things like stroke a baby’s face, hold them down so that they have good tone, put pressure on them so they have good feedback, you start seeing that midline cerebellum go whoosh. And now the baby’s like this: “Ah, limbic system is calm,” and “AH,” they’re, you know, not going to go crazy. And then the pheromones from the mother, that the father doesn’t have – it’s like, “Why don’t I hold the baby?” and they don’t do that.
It’s one of these really awesome systems. And then the mother has this awesome anterior cingulate system that knows how to control that baby’s cerebellar input to the parasympathetic system, and the control over the amygdalar system that creates anxiety.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 9
So as you have this, we also – down here, don’t forget this region right here, okay? And this is, you know, your flocculonodular region, and it does things like go straight to the vestibular nuclei. Balance and eyes, balance and eyes. So it goes into the vestibular nuclei and it says this: “If I fall one way, I have reactions with my limbs. If I move my head one way, my eyes have the ability to do the equal and opposite reaction.” Okay?
So here’s kind of what it looks like when you cut it apart. And most of the surface area is an outer layer, and then pathways and some other nuclei, and then deep down we have the deep cerebellar nuclei. So I’ve got some really good animations that I’ll show you on this.
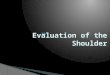
So, this again is a nice picture. This is the spinocerebellum, this is the cerebrocerebellum. This down deep is the vestibulocerebellum. This is kind of looking at it from a different way. The bottom, right down here, vestibulocerebellum, flocculonodular region. This is the vermal region. It’s got the fastigial nuclei in it. This is the lateral. Now look at this: This lateral dentate deals with planning. What do you think planning has to do? Planning, modulation, voluntary activity, all of these things. I have every region broken down and what it does clinically, so that you don’t have to guess. So right now it’s kind of just small-talking through it.
Now, the vestibulocerebellum has the flocculonodular lobe. That’s in the middle. And the vestibular and the fastigial nuclei, that’s where it goes to. Sorry, it’s not “spano-,” it’s “spino-” cerebellum – got to at least make one typo. Vermal and paravermal regions, they go to the fastigial nuclei, and they still go down to the spine, but they receive information from the spine too.
See, that vestibulocerebellum is just information that it goes straight out to the vestibular system, and it goes down into the nuclei that relate to vestibular reflexes. But then you go up to that vermal region, those fastigial nuclei, and they’re receiving information from the spinocerebellar pathways to integrate, to go back down.
And remember, in your spine you have intrinsics and extrinsics. Extrinsics give me the ability to move. Intrinsics you cannot volitionally move. You can’t say, “Laterally bend T4 on T5.” But if you move your extrinsics, your intrinsics can reflexogenically cooperate. Or not cooperate. That creates a real problem.
And then the cerebrocerebellum goes to the lateral hemisphere. I think you guys are getting the point of how it’s all connected.
So, this right here is your peduncular system. I just wanted to kind of show you this, then I’m going to go back. These are the ways the cerebellum… it’s just like this. If I plug a plug into the wall – it’s got three little prongs – and it connects into the system, your cerebellum connects just like this and it has three highways, depending on where things are going, or where things are coming in, but we have three of these. And you can see these guys highlighted right here. And in the midst of this, we are going to discuss all of these peduncular regions, and everything, and I’m going to go through these pathways too. So you’ll see what they mean here in a second.
So let’s review some of the terminology. Some of the things that the cerebellum does is control gait. Now, let me ask you this. Ready? Cortical fist, right here, circumduction gait. Is this cerebellar? No. That’s corticospinal or cortical. Or internal capsule. I’ll show you all the different levels of where… this is the motor output systems are being damaged, not the motor coordinative systems. Okay?
Cerebellar damage usually creates hypotonia. You tap a reflex, it’ll be maybe a little pendulous. You feel for muscle tone, it’s just not so good. Your heel-to-shin starts to kind of be off a little bit. Your finger-to-nose is not that great. You know, your rapid alternating movements are not so good. I’m going to go through what each one of them means. So you’re going to know this: What test goes to which part of the cerebellum, and what it does. That’s – remember – pointing to where something is and what it does.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 10
So posture is a big deal. And when cerebellum is damaged, people will fall to one side, they may become ataxic, they may get core instability, they may do things like this [demonstrates head tremor]. You see this? What is this? It’s a titubating midline tremor. The other day I was watching this gal, and she was doing some things, and she did something that was highly, highly, highly detailed. She was putting her glasses on her head and trying not to poke her eye, her ear, and as soon as she did this [approaches head with hand], I saw this [demonstrates tremor]. I was like, “Whoa-ho-ho-ho, whoa, whoa, whoa.” That’s like cerebellar disease ten years before it becomes like a really, really big deal. And you’ll see people, they’ll go and they’ll reach for something, and they’ll go like that, and you’re like, “Whoa, did you see that? Moment of intention tremor.” Or breakdown.
I have all the tremors and a way to show you how to just break them all down, and again, less than five minutes. Does it remerge? Does it not remerge? Is it with intention, not intention? Is it in the midline? Is it not in the midline? How many hertz does it oscillate at? And you can just identify it, and say, “It’s seven hertz, ten hertz, one hertz tremor.” And you’ll know where it is.
Okay, so don’t worry about tremors. Let’s just get through cerebellum. You’ll hear me jump ahead of myself – it’s part of it though.
So gait and posture. And most of the gait is this: As you walk, your feet should be about the same width as your shoulders or just inside. So you walk. And there’s normal arm swing. If you can’t… if you don’t have arm swing, that could be cortical stuff. So if you see somebody walking like this, and they have a flat face, you’re like, “Whoa, look at that frontal lobe!” But if they’re all like this, and they have a good arm swing, but they have a wide-base gait, you’re like, “Whoa, look at that cerebellum!” You starting to see the difference?
Now, if they’re waddling like this – and I know people… I’m going to get emails; I’m going to get made fun of, so just let ’em go, here we go – if they’re waddling like this, this is a primary muscle disease gait. They can’t activate their primary hip flexors and movers, so they can’t go up stairs. And then you start to see them lose muscle proximal to distal. That’s primary muscle disease. Ventral horn cell disease is distal to proximal. Everybody comprende? Alright.
So, with gait, it’s mainly ataxic. They might be unstable. Their core stability is off. One good test I love to do is have them lie down, do half of a crunch, and they’ll start doing this [demonstrates tremor]. It’s called dyssynergia. Try it later on. Last time I tried this was with Cedermark, and he of course held the sit-up for like twenty minutes, and I was like, “Okay, get off the stage. You’re in too good a shape.” But you’ll come up and you’ll hold it, and you’ll see people, they’ll break down. They can’t… it’s dyssynergia. It’s a sign of this: Your cerebellum’s not that great.
Most people when you’re getting back into shape, the very beginning of it is neurological activation back to the neuromusculoskeletal system before you’re actually getting better neuromusculoskeletal tone. Or muscle… you know, the muscle fabric is increasing. It’s crazy. A lot of being out of shape is being out of neurological shape. A lot of being back in shape is neurological activation. And by the way, it’s a heck of a lot harder to get into shape when you’re older and your cerebellum’s not responding as well. So, quit the booze, control your autoimmunity, activate your core, and go from there. Quit the booze, you know, some. I gotta be realistic here.
So now, ocular function. Listen, I’ll show you the ocular function things that go wrong. You know, a lot of people try to make this really hard. I’ve got to be honest with you. They think it’s special if they can make this hard. It’s not as hard as you think. Let’s just put it to you that way, okay? So we’ll go through that. But remember, there’s ocular function problems and there’s tremors.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 11
Now, with the basal… I’m just going to give you a couple of rules, and these rules will bend some. With basal ganglionic tremors, remember the basal ganglia give you the ability to start and stop, or to initiate movement and stop movement, right? So when you have, like, the direct pathway is shut down, or the indirect pathway is shut down, things will happen. so without stealing Dr. Kharrazian’s thunder, there’s two basal ganglionic pathways: the direct, which says go, and the indirect, which says stop. The direct means move, the indirect means stop. So which one, if the direct pathway’s greater than the indirect pathway, what do you think you’re going to have? Hyperkinesias or not? Yeah. Like OCD. And ticks. And PANDAS. And emotional problems. And here’s what we’re finding: We do indeed have antibodies to dopamine receptors, or calcium-calmodulin, that produces dopamine, and we get massive D1 overactivation of D2, and the person’s just constantly going. Tk tk tk tk. And they’re doing all these things.
Now, if somebody’s D1 system is not going, because they have no dopamine, because they have Parkinson’s, they’re like this [demonstrates slack posture] and soon as they stop, they get a tremor, and their head comes forward because their center of pressure perceived is backwards, so their anterior muscles activate, and they’re like this [demonstrates tremor]. And they’re perceived so far backwards that they can’t start going forward. So in order to start walking, they have to go like this [demonstrates jiggling] and then walk. And you can see their face is flat, and they can’t look up well, which is why their head is starting to tilt like this, to get a different type of vestibular response to drive their eyes up. And then when they have to look up, they do this [demonstrates arching].
But at rest, the direct and indirect system is in balance, so you see a tremor. With a cerebellar person, they’re like this. They have no tremor, but as soon as they go to do something, you see the decomposition of what they’re doing. And I’ll show you how that works in a second, okay? So there’s differences.
The cerebellum says this: The more fine-tuned you are, and the more detailed you are, and the more you have to do, the more it breaks down. The basal ganglia just says this: “Hey man, I’m just going to control whether you’re activated or not activated” And the brain loves for the indirect pathway through the hyperdirect system to be super activated, so you can just sit there and be like this: “Whew, let’s just chill,” and you’re not going like this: “tchk tchk tchk tchk,” or that BeeGees song is going through your head, or, you know, you have some sort of other hyperkinetic, like choreaform type of tremor. So we’ll show you all the different types of tremors.
Smoothness of muscle, smoothness of movement and muscle tone. So these are things that we have to go through. So, here it is. This is one of your money slides right here. Your cerebellum controls muscle tone on one side.
So it’s like the person’s got hypotonia and they’ve got a finger-to-nose problem, and they’re dysmetric, and their heel-to-shin is off. You start thinking, “Wow, one cerebellar hemisphere is gone.” Or it’s just in the legs, and you’re like, “Wow, the anterior lobe is gone.” Or, both sides are affected, and you’re like, “Wow, there’s global cerebellar degeneration.” Or when they’re upright you see it, and then when they lie down it goes away, and you’re like, “Wow, this may be a little more lateral versus medial.” Okay?
So, when you see things like balance and equilibrium, and fine movement decomposition and muscle tone changes, you have to start saying this: “That’s what is going on; now why?” Don’t just say, “Ah, it’s a cerebellar lesion. Let’s just go fix it.” Really. There’s probably a reason. Why? Does everybody’s cerebellum just go blblblbtt? No. You could be a couch potato and there’s still people that have cerebellums that are completely functional, and they don’t get a tremor and titubate and have all that stuff. There is a reason. This course is going to dive into the whys. Okay?

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 12
It’s located above the brainstem, or behind the brainstem, which means it does this: it integrates into all of your nuclei that do things like autonomic control. So people with cerebellar damage may have parasympathetic or sympathetic imbalance.
By the way, the cerebellum is highly cholinergic, highly GABAergic, and highly serotonergic. Anybody ever heard of drug discontinuation syndrome? Okay. “Had a little bit of bout of depression. I took an SSRI. And now I quit, and every time I move, I feel like my body’s three seconds behind me.” We call it the whirlies, and it sucks. It can last up to a month to two months. This is why some people don’t get off of them. The cerebellum – it’s ability to calibrate vestibular systems and to give the rest of the brain the understanding of movement is not off, because it’s been dependent on a serotonergic-based med. So they move, and all of a sudden the body goes vvlllippp behind it. Ssvvpp behind it. Anybody ever had patients describe that? Okay, several. They’re not happy, are they?
Okay. So, it is beneath the occipital lobe and the base of the skull, so it’s infratentorial. It contains more nerve cells than the rest of the brain combined. Do you think it’s important? They’re finding… listen, I can’t even go into everything the cerebellum does. We’re finding this: It does way more than we ever thought it does, with cognition, with all kinds of limbic function, with everything.
Okay, so when we look at the cerebellum again, it quickly processes information received from the rest of the brain, and includes it into sensory areas, motor area, cognitive areas, and emotional areas. So what it does is this: It receives information, and it says this: “Boy, that was wrong. Let me repackage this, and then send it back out to everywhere else,” and the brain’s like, “Oh, okay, cool.” It gives you your ability to learn. This is why people with bad cerebellum’s don’t learn as well as those that have great cerebellums. Is that cool? Have a good cerebellum! If I could give you one for Christmas, I would.
Signs and symptoms. Nystagmus. In-gaze. I’m going to show you the difference between – listen, nystagmus is going to be a very fun lecture. I’m going to give it to you in a way that you will know it, okay? But it gives you tremors, abnormal eye movements, ataxia, and you’re uncoordinated. the output of all deep cerebellar nuclei is excitatory. That’s why you have a purkinje… So here I am. I’m a deep cerebellar nuclei, and I’m like, “I’m going out. Psssht! Everything that comes in activates me, and I’m going straight out. And then right above me is this: a Purkinje system that says this: ‘na na na na na na na, wait a minute. You’ve been activated? Let me tone you down a little bit.’ “ So the Purkinje system slows it down. But then there’s other cells called basket and stele cells, and they say, “No no no no, wait a minute, Purkinje cells. let me turn you down.” So it’s a three-layered thing.
So if I’m activating my bicep, my brachialis needs to fire, but other areas need to be inhibited. So the deep cerebellar nuclei go out to the brachialis, and then you go up and you have fibers that go like this, and they go down to other columns, and it can bring to threshold other muscles that synergistically move with the primary muscle. And it all fires into the midline cerebellum so that when I reach out and grab something my core will activate and I won’t go like this and herniate a disk. The whole cerebellum works together to give me core, shunt, spurt, stability, activity. So. Lots of bad disks and bad backs because of this.
So, the output’s excitatory, and it goes to the basal ganglia, which we talked about. It goes to the motor cortex, which we talked about. This is it. The cerebellum goes to the cortex. The cerebellum goes to the brainstem. The cerebellum goes to the basal ganglia, because the basal ganglia have to do with movement, so the cerebellum says, “Hey, check this out.” It goes to the cortex because the cortex has to know how to, you know, program things and put packages together that equal motor output. And here’s the cool thing: This is all happening at once, and as I’m moving, I’m constantly receiving feedback, it’s being integrated, pre-packaged, and as I go, it’s corrected. And if it’s not, and if it’s not, and if it’s not, and if it’s not… Do you start to see that? The cerebellum gives everything the ability to orchestrate. It kind of is this: the conductor.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 13
“You’re going to do this, You’re going to do this, I’m receiving information by what I hear,” and it’s conducting the whole thing. It is really a big deal in a little package, right underneath the thickest part of your head.
Anybody every talk to a board-certified skull-based surgeon? They’re like, “It’s like digging through concrete to get through that area.” Okay? There’s a reason why there’s a whole extra year of fellowship to become a person that can just do that.
This is a slide that I hope you have forever. We made… I put it in the diagram section. You can just own it. You can laminate it. Some of these slides, you’ll take out and you’ll laminate and you’ll put them in a separate book and you’ll keep them forever, because you’ll flip to it all the time. Especially when we start giving you labs, lab values, patterns, this that and the other, you’ll really enjoy it.
Well, here it is, guys! This is just as simple as I can make it. Why talk about all of it when you can just put it in a diagram? You’re going to see this: The more and more we do this, the more and more diagrams we’re going to make. Because really, what we say about it, you can just go back and listen again. And we’re even having to learn that. It’s like, we don’t even realize that our voices are going to be able to be reheard. That’s sometimes scary. It’s like, “Edit that!”
But the titubation is this. The tremor is kinetic tremors and tension tremors, all the things that require detailed activity. Sometimes you may have both basal ganglionic and cerebellar stuff, so it almost looks essential. It can become imbalanced. You can have dystonia, abnormal posturing. You can have a lot of things with this.
So impaired check. So the person comes up like this, and you hit one arm and it comes down, and it comes up and it goes like that. And you’re like, “Is that level? “ They’re like, “Absolutely.” And you’re like, “Whoa, really?” And then if they have a parietal lobe lesion, they’ll do things like this, “I’m there!” And you’re like, “Where?” You’re like, “And right in front of me!” And they’re pointing to, you know, like, over here off the side of the boat. So we can do some really cool tests. Look: “How’s your parietal lobe? How’s your cerebellum? Can you go to your nose? Are you dyspraxic or dysdiadochokinetic?” You can do it so quick, Why not do it on everybody?
So listen: Next module, I’m going to run through several sections of… hey, I know the physical exam’s a pain in the butt, but how can you do it super fast, and while you’re doing it, all of these little areas flip back, pt tt tt tt, right after another, and you’re like, “I know that, I know that, I know that, I know that.” So now you don’t just have a physical exam and a checklist, like, “I did it, I don’t know what it means, but I did it.” As you check it off and do it, and as you ask questions, you’ll be able to visualize in your own right brain, right about here, the pathways and the areas.
Here’s how I do neurology: When I do it, it’s like flipping a screen up in front of me, and I can kind of see the different areas. But if I read about it, I can’t remember anything. For those of you that are having a hard time learning it, get more right-brain activity, and just understand it and be able to perceive it in your own mind, okay?
Now, you can become dysarthric, because the muscles of speech have to have coordination. Look at this. Is this a problem? How many people are like this: “Ah ah ah ah”? What does alcohol do to your cerebellum? It kind of turns it off. How many of you are like, even last night, you’re talking to that person; they’re like, “Ah aha eh eh,” and you’re like, “Whoa! Dysarthria induced by alcohol! Way to go, man. Your cerebellum’s probably not as good as you think it is.”

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 14
Dyssynergia. It’s that thing like I told you about the sit-up. Or they may be doing curls, and they’re like, “Holy crap, what’s wrong with me?” You’re like, “Dude, you’re out of shape. And you’re not just out of shape muscle-wise, your cerebellum’s going, ‘I didn’t know you did these activities!’ “
Cognitive changes. There is some thought out there that maybe things like schizophrenia is dysmetria of thought. How you can overshoot a movement, can you overshoot a thought? There’s a lot to those conditions, don’t get me wrong. I’m not trying to oversimplify it. What I’m trying to do is let you know the greatness of the cerebellum.
Dysmetria, dysphasia… now, swallowing is a major thing. Now, you guys saw the video the guy showed you yesterday, with the tremor. He couldn’t swallow, he couldn’t talk, he had no epiglottal function. His brainstem is starting to become deteriorated, and his cerebellum can’t do it any more. We’re having to work with him, but he had no fuel for delivery. Think about it. Again, swallowing one out of eight bites. Try it for a week. You’re eliminating seven-eighths of your calories.
Ataxia. I just showed you that eye finding. We will go over those. We have a whole module on eye movements.
So some of these things that are more complicated than others I won’t dive into, but I just want you to know, you have eye findings.
Here’s a couple things you may have: You typically don’t get just nystagmus, like – I get to do it. My balls. They got painted. Heheh – Okay. Which way’s the fast phase? To the right. This is usually peripheral ves-tibular imbalance. I’m going to go through that later on. I’m going to show you, “Okay, here’s the vestibular system and here’s what it means. Is it central or peripheral?” Just like the nervous system: is it central or peripheral?
What the cerebellum loves to do is things like this: The cerebellum has a problem, so you may get vertical nystagmus, or you may just have things like this [demonstrates eye movement]. What’s this? An oscillation. Because by the time the information is given from the cerebellum to every other place, it’s too late, so it goes a little bit past, and then it gets a correction, and then it goes back and it’s a little bit past, and it gets a correction, and it’s a little bit past. So you get a square wave, micro- or macrosaccadic oscillation around a target. It can’t do it. It’s like, “Oh crap.” And when the lights are on, the more you try to fixate, the more difficult it is. That is different than a peripheral-vestibular lesion, where you have this nystagmus, and then you go just a little bit downstream and fixate on a target, and they’re like, boom, stable. You turn out the lights, and all of a sudden they start going crazy again. So I’m going to show you a couple of rules about that, okay?
The other thing about the cerebellum is, it coordinates smooth movements, so your pursuits look like this [demonstrates jerky eye movement]. It’s almost like a saccadic pursuit, which means it’s a rapid movement within the pursuit. So if the eye cannot keep up with the target, it has to have a catch-up saccade. And sometimes it’ll go past that, and it’ll become paradoxical, and it’ll become hypermetric. So here’s what we found with the cerebellum: It’s really good at giving programs to stop targets. So when you say, “Hey, go look at the target,” and they go like this, and they go just past it, and you’re like, “Whoo, cerebellum.” There it was. Did you see that?
Now, there’s other things that can make that happen, but we’re giving it to you layer by layer.
And then the other thing is this: When you hold gaze, it’ll break down pretty quickly. So there’s things in the eyes that we’ll be able to see that will reflect upon the cerebellum. But if you look at this, and there’s one, two, three, four, five, six, seven, eight, nine, ten, eleven, twelve, thirteen, you have seven or eight of

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 15
these things, is it really difficult to say, “Hey, the cerebellum’s messed up”? No. If it’s midline versus lateral, you can start to pick it out.
Let’s keep going.
So here’s your damage. Postural sway. Anterior to posterior sway with some variations; we see that a lot. So they may have these anterior to posterior sways, and then when they have bad tone you may see them kind of do this, they try to bring their legs out wider because they’re a little bit ataxic. They’re hypotonic, so they have a decreased resistance in limb movement. They have asthenia, which is weakness, fatigue, and coordination issues.
Now, let me tell you something. You have a thyroid patient. And now all of a sudden that thyroid patient is like, “I’m weak. I can’t use my arms and legs the way I used to.” You start thinking, “Uh-oh. Is their cerebel-lum now getting dinged?” Because there’s a high correlation between cross-reaction and mimicry between thyroid and cerebellum. Now listen: It’s really not a joke. It is there in a lot of patients, so you need to start listening. Now, if you start getting those symptoms, and you find cerebellum and nobody’s ever had their thyroid checked, you might want to go the other way.
Please, everybody understand that. Because that will take you into a whole different world. Now you go in there and you activate the cerebellum and you’re like, “It did great.” A week later it’s back to where it was. You’re like, “Why did that happen?” You activate it again, and it comes back a week later, it’s like, “Why did that happen?” Because they’re having flare-ups, man. Their autoimmunity is not under control. Controlling autoimmunity, a lot easier said than done.
So if I have an asthenic response, I start saying to myself, “Whoa whoa whoa whoa whoa. What is really going on here? Are there B vitamins? Am I losing thiamine because I’m drinking? Do I have antibodies because of Hashimoto’s?” What is it – you know – spinocerebellar ata… what is it that’s making the person feel like their arms weigh a thousand pounds and they can barely move? Start looking at cerebellum.
Speech and swallowing. Used to have a family member, X. I’ve got to be nice on video. This particular individual had a grandmother, and she was very flat and very slow and very apraxic, and I’m like, “Oh man, this…” And so we would go out to eat, and they’re like, “Let’s go out to eat,” and I’m like, “No. No.” They’re like, “What do you mean you don’t go out to eat with my family?” I go, “She’s going to choke, and they’re going to ask me to do the Heimlich. I already can tell.” I mean, I was like already prepared. I’m like, “No, please. Let’s… can we just, like, bring some soup? Some thin liquids?”
So we’re sitting there, and sure enough, we’re eating, and she comes up, and I’m like “Oh God, here it goes.” Chew, chew, swallow. The swallowing mechanism is not coordinated. And she’s like this: “Ahhh-er-er.” I go, “Oh no.” I’m like, “I’m a chiropractor.” You know, I pulled that move. So I’m like, “Oh my God!” So you go over there, and you know she’s so frail, the second you do the Heimlich maneuver, what’s going to happen? So I broke some ribs. Krkrkrkrk.
Now here’s the deal: That’s the last time we’re going out to eat. When I have a cerebrofrontal problem like that. Swallowing is scary. If somebody’s getting choked a lot, they need to have certain studies. Maybe an endoscopy, maybe a barium swallow. They need to look and make sure there’s no constrictures, they need to make sure that they don’t have, you know, dysrhythmia of peristalsis of it going down. There’s a lot of things that can happen. You can help those things from the functional neurological realm, but if it’s there, you need to image it and find out.
Now, one more thing. If you see blatant cerebellar findings in children, always do an MRI. They usually don’t have enough time to get autoimmunity. They usually don’t have enough time to deafferentate. They

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 16
may get some developmental abnormalities, but they’ve been there forever. If they get sudden or rapid cerebellar findings, please do an MRI, because a lot of times it’s tumor.
Adults, they’re like, “Ah, I developed this over the last, you know, three or four years,” and you can go back and say, “Well there’s some sort of something or other going on.” You don’t find masses near as common. Okay?
So, we go through here: Cognition. The contralateral frontal lobe may shut down. Now, can I ask frontal lobe questions and you know a little bit about them? Yeah. So now it’s like this: The person’s right frontal lobe is showing signs of not being so great. Now their left cerebellum is showing signs of not being so great. What came first? And then you’re like this: “Wait a minute, what else is going on?” Well, they’re constipated. Well, is that because the parasympathetics are not right, so they’re not voiding? So we’ll teach you how to check autonomics. Dr. Kharrazian’s going to go through them later.
Do you start to see how, when you put multiple things together, you can triangulate the area? It’s not as simple as just saying, “This symptom, go here.” You’re going to learn to say, “This symptom and this symptom and this symptom and this symptom, they intersect here.” That’s one area connected to another area. When it’s all spread out and doesn’t make sense, is it demyelination? Is it neurodegeneration? Is it systemic inflammation? It’s not well defined to one area.
Now, that’s the complexity of it, and on day two we jump to a little bit of a different level.
Eye movements. There may be certain types of nystagmus. They’re usually not horizontal; they’re usually vertical. With cerebellar, they’re usually in-gaze if they’re in the horizontal plane, and when you have volitional movements, you lose the smoothness of pursuits. I don’t care if you know any of that right now, because we’re going to get to it, okay? I promise.
And then titubation. It’s a postural 2 to 3 hertz. What’s a hertz? How many times per second? How many times, right there? One thousand. It’s about 2 hertz. It’s about 5 hertz. 7 hertz. Do you see how you can start to say, “That’s a so-many-hertz tremor”? Well, I’m just going to sit up here and say, “I’m going to do a certain movement,” and you’re going to say, “Boom! that part of the brain.” And then I’m going to do another type of thing, and you’re going to tell me where it is. And then I’m going to do another type of thing, and you’re going to tell me where it is. And another type of thing, and tell me…
So when you’re walking through the mall, and you’re like, “Wow, look at that subthalamic choreaform tremor,” and they’re doing this thing, you’re going to be like, “I know exactly where it is, and I know the vasculature that goes to it, and I know what could happen to it, and I even know other things that could cause that, including homocysteine problems, vascular problems, and everything else.” So it all just goes pfft, and it flips up as a bundle, not as secularized things that you have to try to put together in your own mind.
You can’t learn that way. That’s why I’m already giving you a preview of what it looks like to be bundled. Okay? And I’m not talking about fees right now.
So, ataxic. That’s a balance problem, or a gait problem.
Dysmetria. So I want you to know the words. Inaccurate judgment of distance. Poot! You’re like, “Whoa!” So some of the tests I like to do is, “Okay, go finger-to-nose.” And they do it, and here’s what a lot of people will do to cheat [demonstrates fast finger-to-nose]. And they ground their finger on their nose so you don’t see their intention tremor. Now listen, I’m fixing to give you a Brockism, and if you don’t like it, or if somebody else doesn’t like it, don’t do it. But you can do finger-to-nose and just say, “Touch it lightly.” Okay? And

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 17
then say, “Stop an inch before your nose.” And if they touch their nose, it will slow down the intention tremor, because it’s grounded. It stops. But if you stop a little bit before the nose, you’ll see it break down the longer they hold it, so you’ll see this [demonstrates tremor]. And then you see… sometimes people will start doing all of this crazy stuff, right? And you’re like, “That’s a system…”
Now, let’s go back to what we looked at yesterday. Are cells fatiguing? Could it be pathological? Well, it’s always pathological. But it’s functional. If you see that in kids, go check it out. If you see it in adults, find out why. You do a scan, it’s normal. You’re like, “Wow, these are your cell bodies that aren’t working the right way. Why? Why?” You go through, and you’re like, “Man, they’ve got antibodies. Why?” “They’re cross-reactive. There’s food.” “That’s just the way they are.” “They have a thyroid problem.” “They’re not getting B vitamins.” “They’re not actually getting the components necessary to make their brain grow.” “They have some sort of dysglycemia.” Or, “They have homocysteinemia.” “They have something going on that’s systemic.”
You’ve got to eliminate those things if you want the cerebellum to start to remodel.
The dyssynergia, the decomposition of acceleration, deceleration, and timing… again, I like to hold a crunch and do this, and you see the dyssynergia. It’s so cool. Try it later on, man. You want to help a cerebellum? Do some planking. Do some midline core activation. You see these people try to hold a sit-up, and it’s just ridiculous. I mean, you’ll try it later on, and you’ll be like, “Holy cow!” Like, hold a semi sit-up, and you start going , “Arrhhh!” Some of you are going, “I can’t even do a sit-up, so it doesn’t matter.” Okay? Hook your feet up and just barely do a crunch, and you’ll find yourself doing this [demonstrates head tremor], okay?
Rebound. Tsch tsch. Coming back up to same place. Obviously eyes closed, right? Because otherwise they’ll use their visual system, say, “Hey, it has to go right there.” So impaired check. That’s difficulty determining the movements. So the rebound, difficulty returning back to this place, and then the impaired check is, it goes up too far. So watch: You hit it, that’s just abnormal rebound. You hit it, that’s abnormal check. That’s just like saying, “Go to a target,” and they go to the target, and it goes, “Wrow wrow.” It’s hypermetric. You start looking at those things and you go, “Wow, the cerebellum is really , really not so goo.”
So let me ask you a couple things. We’ve got some really talented people that do scoliosis work. Where do you think scoliosis lives? Not in the spine, neurologically? It’s highly midline cerebellar. And then, when the cerebellum gets offset, the other side of the cortex starts to become off, so now the intrinsics start to atrophy, so you get the convexity and the concavity, and then you lose the A-to-P curves, because the cerebellum. And by the way, when you do those x-rays, A- to-P x-rays, if you’ve lost your lordosis, just count on it getting worse. So crazy.
So, tremor. We have different types: 2 to 5 hertz, 5 to 10 hertz. It’s 2 to 5 hertz proximal, 5 to 10 hertz distal. Amplitude varies with position. More detailed, it gets worse, like I just showed you. It’s different than the basal ganglia. I told you that also. And it also differentiates from the midbrain. So it’s three places you can get tremors. Or actually, there’s more. You can have a midbrain tremor, a rubral tremor, you can have a cerebellar tremor, and a basal ganglionic tremor. I promise you, promise you, promise you, we will drill it so much that you’ll be like, “Basal ganglia!” I mean, this is like, you’ll be very quick at it. You have to be, because if you treat the wrong area, you could accelerate the tremor.
How many people suffer from some sort of a tremor? Oh my… It’s like… I can’t even… I don’t know the exact percentage of the population that has a movement disorder, but a bunch. And what usually happens? They end up on beta blockers, or benzodiazepines, or they end up on dopaminergic medications, and a lot of times when people end up on dopamine medications, they end up, they have a resting tremor, and now they take too much medication, so now they start doing this [swivels from hips]. I call it the Axel Rose.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 18
They get a hyperkinetic… [sings] Mr. Brownstone… I’ve got another career coming on, man. I’m done. This is my last module. I’m going on the road. Let’s listen.
No, but what happens is, when they get too much dopamine, now they become hyperkinetic, and you’re like, “Whoa, you’re overmedicated!” But as soon as they come off, they crash, because now their receptors have done what? Completely remodeled based upon the drug! Doctors are very, very bad off, saying, “Hey man, your tremor’s still there a little bit? Let’s give you more.” Or, “You’re really not happy yet? Let’s give you a little bit more.” Or, “You’re really not doing good? Let’s add another medication on, an SDRI.” Oh, and then they say, you know, they’re on four medications. They’re on one that deals with acetylcholine, one that deals with dopamine, and one that deals with other receptors to inhibit them. So it’s just… it becomes a crazy journey, and the patient comes in and they’re all confused. They’re like, “I had one tremor, now I’ve got another type of tremor, and now this type of tremor is making that tremor tremor.” And you’re just like, “Wha… okay.”
And so unwinding an overmedicated Parkinsonian patient becomes hard. Because to fix them, sometimes you have to take them back to bradyphrenia and bradykinetic, so they’re like this: “I-don’t-want-to-be-like-this-again-man-why-are-you-doing-this,” and you’re like, “Well, you can be Axel Rose again if you want.” They’re like, “Okay. I’d rather be Axel Rose.”
We found that one of the things that we have to do is just get the medication in sync with the neurological care, and just give them the best function, and make every dose last as long as it can. Because the more and more intolerant they get, the dosage doesn’t last very long, so they start increasing the dosage, because the pharmacokinetics reduce in between their dosages of, like, their L-dopa. Meh.
So anyway, this is my vestibulocerebellum. It controls the axial region, That’s the spine, right? And it gives me equilibrium and gait. And gait. So right here, midline cerebellum. Information from the labyrinthine system of the ears, information from the nodulus, which also gives me labyrinthine input. And when this area starts to kind of crash, we get things like the vestibular becomes abnormal so my VOR changes, my axial muscles change, and my vestibular reflexes change. So that means you start to sway, your eyes become abnormal, so all of your midline things are abnormal. You eyes are homologously linked with your core. So, in my later module on the vestibular section, I’ll break that down for you a little bit more. Okay?
The vermis gets messed up. If you see titubation, it’s vermal.
Ataxia of stance, midline.
Head tilt can be midline. It can also be other things.
Dysarthria, midline.
So when you start seeing those things – whoops, I’ll go back – you’re like, “Wow, the midline cerebellum looks terrible, they have an oculomotor disturbance, they’ve got gait problems, they’re titubating, the midline cerebellum’s breaking down.” And if their legs are more involved than anything else, you know the anterior lobe is going away.
So the dorsal vermis and flocculonodular lobe, they can get ocular flutter. I’ll show you what that looks like later on.
Oscillations. This is really a lot of eye stuff. They get dysmetric flutter, oscillations, and bad pursuits. That’s whenever you say, “Hey man, I’m in the dorsal vermis and flocculonodular region, versus the parafloccular

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 19
region.” No not only will I give you the midline region, I’ll tell you how to break that region down into sections. Okay?
So let’s pause for a second, because I’ve given you a lot of information so far. I want to stop. We’re in the second hour, okay?
The cerebellum deals with – not necessarily the execution, it deals with this: Let’s make this great. Let’s bowl a strike, not hit the gutter, every single time. Let’s learn. And it gives me the ability to have, you know, tone in my core, tone in my arms, good motor program and sequencing so everything looks smooth. You realize that movement is just a bunch of starts and stops that happen so rapidly that you can’t see them. But if there’s a delay in that communication, you see the start and stop, and now that’s this.
So, do they have dyssynergia? Do they have dysmetria? Does it decay into dysdiadochokinesia? Do rapid alternating movement fatigue so now you lose it all, and it’s like rrrrrr? Do they have any of the findings we looked at yesterday that’s the cortex, along with the cerebellum? When you bring things in nice and tight and you start to do them like this, are you isolating more of the lateral portions than the medial portion, and is it looking more at the parietal and frontal systems? If you have facial masking and slow movements like this, and freezes and hesitations, and you come down here and you do this, it’s probably not cerebellar; it could be frontal. Are you starting to see now how it’s not always what you think it is? There’s other stuff that kind of goes in with it.
Welcome to functional neurology. Do not get frustrated. I want to highlight that. We are going to layer it and layer it and layer it, over and over and over.
So, here’s this vestibular component, and it goes out to the vestibular system, and it ascends up, and this goes up to the MLF. This right here moves your eyes laterally through 6, it goes through the medial longitudinal fasciculus, and hits 3. So when one eye moves lateral, the other eye moves medial. That’s part of your vestibulo-ocular response. Now, in MS this will demyelinate. So when one eye goes lateral, the other eye doesn’t go medial. That’s called an internuclear ophthalmoplegia. I’ll show you that in the eye movements later on. As these go down, the vestibular nuclei give your ventral horn cells the ability to react to rapid perturbations. So whenever certain things happen, they don’t react, and they fall. Okay?
Hey, what do you think a good way to save yourself from falling is? Bring your legs further apart, so that you don’t fall to one side or the other. Okay? Gives you more stability.
So, the spinal cerebellum, this is midline, and it gives gait instability, ataxia of the trunk, titubations. When you rapidly move eyes to a target and they have to stop on that target, they go past it, and they get vertiginous. However, these findings can or may improve when lying down. When you stand up, you load the midline cerebellum, and if it doesn’t load right, it breaks down. When you lie down, you don’t depend on that as much, so you don’t see the pathology. So I do a lot of my cerebellar tests standing and lying. Anybody else do that? Okay, a few of you. Well, we’ll show you that. Okay?
Alright. So now the spinocerebellum: shoulders, hips, and spine. This is the globose and interpose, right? This is this [rotates shoulders]. Am I moving my hands right now? No, I’m moving my shoulders. These are globose emboliform intermediate regions. Okay? Right now, this is distal. You bring it in more and stabilize it, this is even more lateral cerebellum, okay?
So anyway. The fastigial nucleus goes to the vestibular nuclei, the pontine area; the globose emboliform it goes to the shoulders and the hips, all the way down to the wrists and the ankles.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 20
Boy, we’re going to show you so much saccadic dysmetria. Just listen to this sentence: “The vestibulocer-ebellum supplies tonic modulation to the medial vestibular nucleus.” There’s four of them right there. Right in the pons. But it goes to the medial vestibular nucleus. Now, I will eventually, over time, break down every nucleus, all the ascending and descending components between all of them, and what the eye movements look like when they’ve been damaged or changed. Okay? So just… I’m going to try to do it in a way where I’m not reading to you from Lindsay. Okay?
Anyway, so this breaks down for control over eye movements. It’s important for stopping a saccade. A saccade is this: There’s a target over here, and my brain already knows I’m going to go to it, so it’s an all-or-none movement, so it goes vvvpp, and it looks over there. And it has to stop immediately on the target. With frontal demise, a lot of times the latency, the time it takes to get going, it’s like vrrrrr, and then you see it go. And then you’ll have a breakdown in velocity with certain things, a breakdown and a latency. But then there’s accuracy, the ability to stop on the target. Sometimes it will stop short, and you have to have a couple of catch-ups, and sometimes it’ll go beyond it and then yoyo back. Well, we see that a lot with cerebellar lesions. And the thing is, I can’t ask you to go buy twenty thousand dollars worth of equipment, so we’re going to have to teach you how to do it on each other. Okay?
If you do it a hundred times, you will start to see it. If you never do it, this is just an academic lecture. It’s just an exercise in me reading slides and going through things and talking to you about it.
So we got more stuff that receives information from spinal afferents, and I’ll go through that in a minute. And then the spinocerebellum projects to the red nucleus and the mesencephalon. So now look at this: The cerebellum through the vestibular system goes down and really activates your extensor region. But then it goes up to the contralateral mesencephalon, and the red nucleus comes back over to the flexors. So when your cerebellum is shut down and you lose extensor tone, and then the red nucleus coming back over loses flexor tone, you get a hypotonic limb that’s dysmetric and dysdiadochokinetic. Make sense?
So I’ve got a nice little picture. So the vestibulospinal tracts tracts control the fastigial system and a bunch of other things. This is it. So it goes up to the red nucleus, it goes down to the vestibular nuclei, and it goes over to the reticular formation. And when I say reticular, we start talking about integration now into autonomics.
So is there a correlation between spine, midline cerebellum, and autonomic control? A lot of times there is. Dr. Kharrazian will go more into autonomics here in a little bit.
Now here is the cerebrocerebellum. This is the lateral part. We are awesome, because we have a lateral cerebellum. We have a dentate. Okay? And the dentate gives us things like the cerebrocerebellum. We can have intention tremors, we can have action tremors, we can have hypotonia, we can have dysdiadochoki-nesias. By the way, we can have immune dysregulation. Natural killer cell, B and T cell differentiation. We’ll talk about what the brain does to the immune system, to the best of our knowledge.
I want to highlight that. A lot of people are like this: “Wait a minutes. Whoa whoa whoa whoa whoa whoa whoa wowowowowo wowowo, whoa! You mean, talking about the immunological system has something to do with the brain?” Well, of course it does. Nothing escapes the brain. There’s right-brain control over certain parts, there’s left-brain control over certain parts, there’s cerebellar control over certain parts, and there’s autonomic regulation over certain parts. If you have demyelination over small fibers it’ll do certain things. And we know this: If your vagal output changes, good luck, if you don’t have vagal output. Your gut will get overgrowth, you’ll produce things that break down the barrier systems, you won’t break down proteins, and when that happens you’re going to become inflamed and you’re an autoimmune probability.
These are all of the things. There’s literally a module over each of these areas. I’m giving you the big picture. It is going to be a blast. When you start looking at how to do things like, “I’ve got an autoimmune patient.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 21
I already know these other protocols, but let me start doing some neurological exercises now that might help my patient.” That is called brand new. We’ve been doing it for a little while, and sometimes we just want to activate one hemisphere, because I’m like this: “Their cortisol and their immune system are both not in check, so I’m going to activate one hemisphere.”
Uh-oh. Now everybody says, “You’re crazy.” Well, not according to some of the literature.” Maybe not. I’m throwing that out there just to kind of get the conversation started.
So anyway, here’s the red… I mean, the cerebrocerebellum, and I just showed you what it does. And it really projects upward and it goes to the brain, and it goes to the cortex, and then what happens is this: watch.
Information comes from the cerebrocerebellum, it goes up to the cortex, and the cortex says, “Hey thanks. I like you so much, I’m going to integrate it into everything else that I do, so I’m going to send it back down on to the pontine nuclei, and send it back over to you to tell you what we did with it.” So the cerebellum says, “Look, I don’t think this is working right.” Or, “I’m getting information from the periphery about movement. I need to tell the cortex.” It feeds it over to the cortex, the cortex says, “Great. This is awesome.” It goes back down to the pons, shoots back across, and cerebellum says, “Cool! That’s what the brain did with what I just told it?” That’s a feed-forward mechanism. Really neat stuff. We can use it therapeutically quite a bit.
So look at this: Here’s my dentate. It’s lateral. It feeds up to my red nucleus and my mesencephalon. That gives me flexor tone. That fires up to my thalamus. That goes up to my frontal lobe. That is the dentate… I hate doing this. That is the dentatorubro-thalamocortical pathway. Are you happy, Elaine? Okay. She was talking about it the other day on a visit, and she’s like, “There’s actually such a thing?” There is.
Well, that comes back down to the pons, and the pons is like this: “Cool. Let’s send everything back up through mossy fibers.” That’s just what they’re called because they look mossy. This is the coolest thing. Now, this also allows some of these pontine nuclei to oscillate at certain frequencies, which brings certain parts of the brain in sync. Vvrroom, together.
So these nuclei have certain oscillation speeds. And so when they’re activated by the brain, and they’re turned on, and it activates your reticular system, the whole thing lights up in a certain pattern and your whole brain goes brrrroooo, and it comes online. And when it comes online, now you can bring certain parts together in certain fashions, and now this activates with this activates with this, and it all equals one function. So when you do functional MRI, it’s not just one hemisphere. It’s a little bit here, a little bit there, a little bit here, and a little bit there. How many of you have seen that? And that’s what we’re finding when the cerebello- and the dentatorubro-thalamocortical pathway and the descending pontine system isn’t working, and we don’t oscillate the right way. The whole system starts to kind of shut down. Okay?
Man, love that cerebellum. And really, the guy that does that is the olive. The olive is the big guy that does that. Now, there’s a lot to do with brain activation and proximal muscles. Now, why in the world would a huge amount of brain activation have anything to do with proximal muscle groups? Because they’re the weight-bearing guys that make us move and are used the most.
Listen: all the midline cerebellum fires to my vestibular system to coordinate it, and fire down to give me tone. You go a little bit further into these big primary movers, they activate the brain. You go to these little guys right here, they go to the more lateral part of the brain and anterior part of the brain, and they give us more stuff like language, higher cognition, and higher function.
Are you starting to see some beautiful treatment strategies that we can give people? A leg, a hip, a thought, an eye, a position, a nutrient, a drug? It gets cool. I’m giving it to you this way so you can digest a piece of it, and then put one piece with another piece, like LEGOs. And each person that you work on is a LEGO

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 22
masterpiece. Now, I happen to be a LEGO masterpiece, because I’ve got a ten-year-old. We put things… that’s our bonding time. We do LEGOs. Look, man, I can identify one part of the LEGO, but when I snap it together, and it looks like a Star Wars ship, that’s the person that you’re working on. You took each individual piece, snapped it together, and now you know the nutrient that you need, which part of the brain needs to be activated, how do you sneak in there and do it, if there’s any roadblocks you remove it. Which part of the cerebellum are you going to activate? How are you going to coordinate that with the frontal mechanism? Can you do them both together at the same time or do you have to do one before the other? And you start making this beautiful structure called your therapeutic intervention. Alright?
Very hard to explain, but you’ve got to get the big picture right now, so that you know where you’re going. If I depend on you to understand that big picture, sometimes you’ll just glaze over and not get it.
So, the vermal region. This is right out of a book, man. Okay? Clinical signs according to this sagittal zone. Vermal: dysarthria, head tilt, ataxia – where do you think I got my information from? Paravermal: really dysarthria, but not as much midline. Lateral: all of these things all the way down. Hypotonia. Dysdiadochokinesia. I mean, if you see somebody that comes in, and has dysarthria and not alone, but also has dysmetria, and also has a little bit of a tremor, and is also dysdiadochokinetic, and also has impaired check, you have to say to yourself, “What’s going on with their brain – the rest of it? What’s going on with the contralateral frontal lobe?”
And then you might want to go check a few things and say, “Have you been depressed?” “Oh, a little bit.” “How’s your day-to-day stuff? Have you been organized?” “Not like I should be.” “Hey, you sad?” “A little bit.” “Let me ask you this: are you just sad like the color of everything has been turned down, or are you hopeless?” That’s the difference between serotonin and dopamine. See, people that have low dopamine get hopeless. People that get low serotonin, they just get blue, but the y still have a little hope. Everything just kind of gets bland. When the two are there together, like with insulin resistance, you start to see people get really mentally ill. Who would have ever known that maybe the cerebellum, not feeding into it the appropriate way because of deafferentation, spinal core damage, peripheral nerve damage, not feeding into it, or antibodies, or small vessel disease, would have possibly caused some of that? Are you seeing where I’m going?
Okay. Whenever I start asking you questions like, “Are you seeing where I’m going,” that means that I’m worried about you. Just hang in there. We’re getting close to being done, okay? Now, I know this is like, you’re going, “Wait a minute, yesterday was nice and slow and fun.” Hey, this is much… I have to give you more complication and detail of this, because this is one of the primary areas that you’re going to deal with every module. Too much coffee? Yeah, me too. I’m thinking later on I’m going to have to put something else in my coffee. Okay.
This is just more stuff, so these are just describing nystagmus. When I told you it’s gaze-paretic, rebound nystagmus, downbeat… I’ll show you what all these mean. Periodic alternating nystagmus and then upbeat nystagmus and downbeat nystagmus. If you see upbeat or downbeat nystagmus, you need to get a little bit concerned and try to figure out what the problem is. Obviously with any nystagmus you need to see it.
This is just going through these areas a little bit more, and then bottom line is this: Fastigial, globose, emboliform, and dentate. I made this so you could see it. Fastigial: spine and eyes. Globose: shoulder and hip. Emboliform: elbow and knee. And dentate: hands and feet. Does that make it nice enough and easy enough for you? Out there in streamer land, there you go. Okay?
In the middle, and it spreads out. In the middle, and it comes down, go out a little bit further, here and here, a little bit further, here and here, out the edge, here, and here. These lateral cerebellar regions, if it’s very fragile, I might start out with a midline cerebellar activation, and then work my way out to the lateral

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 23
cerebellar activation. If they can tolerate it, I’ll just go straight to it. I’ll do a wrist, hand, and ankle strategy versus a hip strategy. You got it?
Now, do you think somebody can get chronic hip problems if they have a cerebellar problem? Hypothetically. I use the term “hypothetically” and “theoretically” hopefully appropriately.
So here it is. This is all tied together. The dentate goes over to the parvocellular, it all goes up to the thalamus, it goes up to the motor cortex, it comes back down to the pontine nuclei, and comes over, and then it also goes down to the ventral horn cells and it says, “Hey, ventral horn cells, do it better next time.”
Now, I have not given you the ascending pathways yet, from the ventral horn cells or from spindles up to the cerebellum. I haven’t given you that yet. I’m fixing to. This is just a nice slide to show you how efferent copy, feed forward, all connects together. And we’ve got mossy fibers and climbing fibers we have to talk about. So let’s talk about the layers.
Here we go. Ready?
Inner, granular, Purkinje, and the outer molecular layer. This is their version of it. Let me give you our version of it. I’ve got to give credit: I had a student that followed me around for two years, his name is Carl Robinson, and he basically animated everything I said. So Carl, you’re the man. I believe in giving credit where credit is due.
Now, see how the Purkinje cells are in the Purkinje layer? See how the deep cerebellar nuclei are not in the outer layers, they are lower? So, everything that comes up and activates the cerebellum hits the deep cerebellar nuclei, and then it wants to just go right back out and excite something. But the rest of the cerebellum has to say, “Wait a minute, calm down,” and, “Hey, wait a minute, let’s make everything be timed and controlled with the primary action. Let’s make a brachialis work with the bicep, and let’s make the tricep turn down a little bit, and let’s let the spine be activated, and then let’s let the cortex come to threshold and by the way, let’s do this. You don’t have enough blood to do everything at once, so let’s hit autonomics and time them so that blood goes to the part of the cortex being activated and goes to the limb that goes with that part of the cortex.”
If it becomes abnormal, and you shunt blood to the hand, when you’re really moving your leg, you get inefficiency. The cerebellum helps time that. Cool. I get excited. Okay.
So, here’s what climbing fibers do: They come from that olive, and they come up and they do things like say, “Hey, Purkinje cells!” Let’s let it animate. “Do your thing!” At the same time, they activate the deep cerebellar nuclei, so they come up and they go… Here’s the olive. The climbing fibers come over and they help regulate, so here’s activation here, here’s activation here, and the deep… the Purkinje cells come down and inhibit it.
So, when something comes up and activates these deep cerebellar nuclei, all they want to do is just go crazy and go activated. So the fibers that activate it then go up to the Purkinje system, and the Purkinje system’s like a Renshaw system, and it looks at it and it goes, “Okay. You’ve been activated this much, now let’s inhibit you this much.” Now, remember this: It’s doing it all through neurotransmitters. So if your neurotransmitters are jacked, this won’t work right. And now you get a system that either TNDs and escapes, or won’t summate at all. And when you start getting antibodies to this area, it screws with the surround inhibitory output of the cerebellum. So the Purkinje system is like, “I’m trying to do my job to control this, but it’s just not working very well.” And they go out.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 24
Now, let’s take it a little step further. Here’s deep cerebellar nuclei. Now here’s a thing called a granular cell. The cerebellum doesn’t trust itself. So you’ve got Golgi and granule cells, and they’re all over the place making sure that this thing is orchestrated innately. Woo. That’s why there’s more cells in this part of the brain than anywhere else. I’m telling you: the more you study it, the more you realize, “I think the whole thing begins here.” Okay?
So now we have this: We go out to the outer molecular layer where the basket and stellate cells are. Now, they don’t just go right back down to the Purkinje cell underneath it. They’re going to do this. They go out, and then they go down and they inhibit a Purkinje system to another system.
So here’s my bicep. I’m activating it. It comes up through that Purkinje system, and then it does surround inhibition and slows it down. But the body says, “Wait a minute. I need another mover to go along with that movement so I don’t have dyssynergia.” So it goes out, goes over to another group that controls another muscle group, and the basket and stellate system inhibits the Purkinje system, so it does not inhibit that deep cerebellar nuclei and they come to threshold with the bicep. So now the brachialis moves with the bicep. And it does it in a way that’s orchestrated and twinged and sort of tweaked by other cell bodies that are lying around, like Golgi and granular cells, and it happens nice and smooth. And it doesn’t have dyssynergia. And it’s not dysmetric, it’s perfect, like a ballet dancer. Best cerebellums in the world. Or a gymnast. Fantastic cerebellums. Alright?
Are you starting now to understand a little bit of the reasons behind the pathology? That’s what I really want you to kind of get, okay?
So as we jump through this a little bit more… Ah, this Golgi cell. It says this: “Guys, I don’t trust you. I’m going to actually work and do a little bit of inhibition or activation.” In other words, “I’m going to do this: I’m going to tweak it a little bit, because I don’t think this is right.” And basket cells and stellate cells and Purkinje cells say, “Hey, thanks. We appreciate your input.” The cerebellum is all about training. It’s training. It’s learning. It’s this: “I can learn to be an Olympic athlete.” “I can learn to be a professional bowler.”
And here you have this basket and stellate cells. It inhibits the Purkinje system just like I told you, and gives me all kinds of things. I’ll review this in just a second.
So these slides are… and a lot of people are going to be like, “How do I get this animated slide?” Okay. I have Camtasia on my computer. I will play the slide, record it, and then we’ll post it. Okay? I already know that when you get it you’re like, “Hey, it just looks like this. It doesn’t play on the PDF.” Well , it’s a PDF. This is right out of a book, guys. Look.
So, everything comes up, activates deep cerebellar nuclei, goes up to the Purkinje system, climbing fibers come up and says, “Hey, we gotta stop.” We have granular cells and mossy fibers that say, “Hey, you gotta be activated.” The whole thing is coordinated by basket and stellate cells from other regions. So you have to picture it in one column: One column controls one muscle group or one activity. As things go up, basket and stellate cells go up and say, “Hey, other areas, come up and either help me or don’t.”
So now one area is either activated a little bit by another area, or that other area is stopped. So multiple areas of the cerebellum all come up at different levels, at different frequencies, at different times, to make things smooth and work together. Bicep with the brachialis with the brachioradialis, with the flexor carpi ulnaris, with an abductor policis brevis, with my finger flexors. All to go like this: “Hey!” or, “What’s up?” or “How’s it going?” I mean, all of those things are happening so quickly in the cerebellum. If something goes in there and starts screwing the timing up on that, people are like this [demonstrates uncoordinated movements]. I mean, they can’t do anything, because the cerebellum is not organized enough to say, “Start. Stop. Go. Activate. Synergistically move.”

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 25
It’s all about the coordination, timing, and planning when you execute. When you’re at rest, usually not a big deal. When it starts to go into the basal ganglia and into the mesencephalon, because of transneural changes, then you’ll start to see people at rest, and now it’s kind of moved into an essential component, or a rubral component, or even up to the basal ganglia.
So, these are what the pathways kind of look like when you spread them all out. Spinocerebellum, cere-brocerebellum, and then the paravermal and vermal region.
Okay, now I’ve got twenty minutes to talk to you about how information gets from the limbs to the cerebel-lum. Now, I’m going to say something really quick. I like to give you disclaimers of when something is highly talked about and not talked about in the lecture. I have a whole section on spinal cord that I’m going to be giving you guys. A beautiful section, where you will be able to actually draw it very quickly. I’m big on drawing things fast and making stupid, simple rules that people can remember forever. Some of them are a little explicit, so just be cool. But you will remember it.
The spinocerebellar pathways are awesome, because they give information from the limbs that says this: “This is where it is in space and time.” Why is that important? Okay, look. If I’m going to move… If I’m doing the Captain Morgan, okay? If I’m going to move my foot from here to here, the brain needs to know that as it executes movement strategies, because that’s different if I start from back here and come to here. So while things are happening, and before things are happening, and after things are happening, the information from the spindles of their position have got to be sent to the brain so the brain can say this: “We’ve got to make a motor program based upon where the limb’s at. And by the way, no matter where your limb is at, it’s being fed into the cerebellum realtime, so that it can constantly recalibrate those pathways and make them better. You got that? Okay.
And it does it through the dorsal and the ventral spinocerebellar pathways, and they’re the most lateral. They’re right out there in the lateral portion. So when you start getting extrinsic compression on the spine, like myelopathy – not myopathy, that’s muscle disease, M-Y-O. Myelo-, myelopathy is core disease. So when you start getting extrinsic, that means from the outside in, like from a disc, or from the vasculature that’s compressing it, you may start to see cerebellar findings that are subtle in the limbs before you start to see spasticity or rigidity or hyper-reflexive findings. But people overlook it because they don’t do a freaking heel-to-shin test.
Now, in the future modules, I’m going to set a table up here right in the middle. The camera will go right on it, and we’re going to run through every single test, over and over and over. And you can watch it over and over and over. Okay? Is that fair enough? And you can go back and replay it, and send me messages, like, “Dr. Brock, you did not do that right.” And I’ll be like, “Okay.” Then we’ll record it again, and over and over.
But this information comes up, and it says, “Hey look.” The information from the leg goes through the dorsal spinocerebellar pathway; the information from the upper limbs really goes through the dorsal columns, but not through the dorsal column pathway. There’s a cuneocerebellar pathway that just runs with those other path.. . the fibers. Okay?
Now, there’s also a ventral spinocerebellar pathway. I’ll get to that in a second.
So, just know this: Mossy fibers are the type of cerebellar inputs that relay everything that enters the cerebellum which comes from the inferior olive. Remember that guy that goes fwoomp? Lights up and makes the whole brain kind of come alive? This includes your spino- and your cuneocerebellar tracts, your labyrinthine and vestibular nuclei, your pontocerebellar afferents – it all comes through mossy fibers.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 26
Climbing fibers are those cerebellar inputs from the contralateral inferior olivary nuclear complex of the rostral medulla.
So this is kind of telling you just where they come from.
Mossy fibers. They come up, they modulate the Purkinje system, and the deep cerebellar nuclei, and they help control synergistic and antagonistic muscle function, like I just told you the whole story, okay? And they modulate the surround inhibition, which is from Purkinje cells, to give me smooth coordination and movement like I just explained. It puts in concert the feed forward, information from the cerebellum and the contralateral cortex back, efferent copy, which is information to the red nucleus that does not go to the cortex and comes back, and then realtime input coming in through the spinocerebellar pathways.
So, have you guys ever just done something reflexogenically, like caught a football, and you’re like, “I didn’t even thing about that”? That’s one spinocerebellar pathway that doesn’t require as much cognition. When you’re learning a new thing, it requires more cognition. So you start activating one system more than the other. All of it requires realtime feedback to the spinocerebellar or cuneocerebellar system.
So these are just the fiber types. Here’s the two pathways, or the multiple pathways. The dorsal spinocer-ebellar is legs. So now listen: Here’s a case study. Person comes in, they have heel-to-shin problems, okay? They’re like this, they’re all over the place, and I’ll show you a proper way to do a heel-to-shin test later on, okay? But their finger-to-nose and everything else is good. Where do you think the compression is if it’s in the spinal cord? Is it up high at C3? Or is it down low like at T2? Well, it could be either if the lesion is just compressing the dorsal portion where the information runs from the legs. So you have to correlate that now with a dermatome, and with other things like muscle stretch reflexes and sensory findings. Oooh.
What if somebody’s just losing it in their arms but not their legs, and they’ve lost vibration and joint position sense but not pain and temperature? Now they have dorsal column damage and that is where you now have to differentiate the different types of sensory fibers. Don’t worry, I’m going to give you another lecture on that later on and you’ll know it, okay?
Whew, man, I know. It’s almost time for a break. You guys are hanging in there great.
The ventral – so if I go a little bit front, the ventral spinocerebellar pathway is lower extremity, crossed ipsilateral. Now, information from the dorsal horn and the flexor reflex afferents goes over across… Take the ventral spinocerebellar pathway and remember this: It kind of comes in, goes over, crosses over, then goes up and then crosses back over to the cerebellum. And it kind of preserves function for one side if it gets damaged. That’s how important it is. Alright? When I do spinal cord I’ll show you different ways to differentially diagnose it. Here they are right here.
So anyway, we have all these pathways. We have spinoreticular, we have rubrospinal, we have deep cerebel-lar nuclei. All of these things are going to start to come to light whenever I go from the cerebellum, give you all the stuff to do clinically, and then I go into the brainstem, and I show you all the brainstem nuclei, and how they interact with the cerebellum. You’ll get another fresh perspective of the cerebellum from the brainstem looking in, or looking out. Right now I’m giving you information just about the cerebellum itself, and what the cerebellum does when it looks into the brainstem. And then you have to realize that information comes up from your limbs to your cerebellum, because your cerebellum can’t tell your cortex what to do if it doesn’t know what your limbs are doing while it’s doing it. Does that make sense?
So, when you damage your spinocerebellar pathways, it doesn’t necessarily make you spastic. It doesn’t necessarily make you rigid. It just does this: The information that’s coming up from the brain to coordinate movement can’t be done. So it looks like a cerebellar lesion. So you have to be able to do this, ladies and

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 27
gentlemen: “Do I have cerebellar findings in my limbs? And cerebellar findings that are up above the fora-men magnum?” That’s a cerebellar lesion. If I just have stuff that looks like spinal cord, but not the rest of the cerebellum, and I’ve got hyperreflexia and sensory disassociated loss, that’s spinal cord.
So I’m going to be able to say this: “Person’s got a cerebellar lesion. Is it spinal cord? Is it peripheral nerve? Is it real cerebellum? Or is it an ascending pathway that goes to the cortex?” Uh-oh, I just went beyond pointing to one area and saying, “Hey, this does that.” See, the cerebellar lecture, you can’t just do that. You can’t segregate all the function without telling the big story, because if you do, you’ll never understand the big story. It’s better just to tell all the specifics with the big story, and talk about how function integrates, and then do it over and over and over, so you can say, “Hey look, midline cerebellar lesion.” “Paravermal cerebellar lesion.” “Lateral cerebellar lesion.” “Flocculonodular lesion.” “Hey, spinal cord, not actual true cerebellum.” Or, “Hey, this is actually dentatorubro-thalamocortical damage, and now look at what the brain’s doing with the cerebellum.”
So you start to go through and say, “Is it here? Is it down here? Is it around here? Is it damage from the peripheral nerve coming in? Or is it just problems back here?” That’s the dance. Are you starting to feel it just a little bit? Do not let your frustration sink in too deep. I know a lot of you who are just now starting. The cerebellum ties into everything. That’s why we did it after the lobes of the brain, because hey, it goes into the lobes of the brain, but it helps us introduce you to autonomics, it helps us introduce you to the basal ganglia, like we’re doing this afternoon, it helps us introduce you to the vestibular system like we’re doing this afternoon, and then it lets us transition below the foramen magnum and go into the spinal cord.
We are the cerebellar masters. As functional medicine people, and as receptor-based therapists. I’m just going to say “receptor-based therapists” and I don’t care if you’re a chiropractor or what. Physical therapist, occupational therapist, naturopath, medical doctor. You can activate a receptor to create a neurological plastic response. Okay?
Well, here’s what your mossy fibers do. I just wanted to make… I put a lot of writing on there, and I hate people to have to write it and conceptualize it on their own, so what I did is, I just made a little thing here that says, “Here’s everything that makes a mossy fiber, and here’s what it does.
And here’s what your climbing fibers do. And we’ve already talked about that. And here is where they run. Now, this was not an easy diagram to make. Climbing fibers come in through the inferior olive, then goes through the inferior cerebellar peduncle; it comes over and activates the interposed nuclei, activates the Purkinje system, activates basket and stellate cells, granular cells control that, and it goes to multiple areas so that my deltoid goes intact with my supraspinatus, so that it goes intact with my bicep, so that it goes intact with my teres, so that as I move all the muscles of my shoulder and all seventeen muscles that relate to my scapular movement, they all go in fashion and they don’t freeze, stop, or I get abnormal scapular mechanics with shoulder mechanics, and I’ll get, like, AC joint pathology, type II acromion, too much flexor tone over extensor tone, and I start to tear my supraspinatus; I get abnormal scapular mechanics, which puts too much pressure on my clavicle… You starting to see some things that break down biomechanically?
Man, we could have a whole class just on biomechanics and brain. And by the way, we probably will. But we can’t do it until you start saying, “That’s what the cerebellum does and that’s what the cortex does.” So when we start talking about biomechanics, and we start talking about a dropped foot, and an internally rotated femur, and an externally rotated tibia where your screw-home mechanism dies off, and now you get a dropped arch, and now as a result you lean one way and you subluxate your SI joint, and now you compensate with a head mechanism and it hurts your suboccipital region, and you’re like, “How does that relate to the brain?” When you start learning all the neurology, you really can understand biomechanics. It’s really tough to understand biomechanics without knowing neurology.

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 28
Wow. And I’ll even say this: Anybody doing chiropractic should know the brain. Because that truly is neurology. Okay?
Now, I’m just going to go a little bit further. I’ve got about six minutes left. Remember this slide? Oh crap! Now we’re back to GAD antibodies? Listen: Your cerebellum has to have GABA, because it has to stop things. It has to have a surround inhibitory mechanism. When you lose GABA, you get escape. Those deep cerebellar nuclei, they’re like this: “Party on, man!” Poof! and they just take off. That is parasympathetics. Now somebody gets overload, and now they may pass out. Now you activate it just a little bit, and wham! Vasculature changes, they pull blood, it doesn’t get to the head, and prprprpr, down they go.
Are you starting to see how bad GAD antibodies can be? GAD, the guy that helps me take glutamate and convert it to GABA. There’s lots of activation going on. That’s why we don’t give alpha ketoglutarate to everybody, because it turns straight into glutamate. So if I give you that, and you’ve got GAD antibodies, you become very excited but not too inhibited. And those people are like this: “Where’s the benzos?” Alright?
So, GABA inhibits these deep cerebellar nuclei. If that doesn’t happen, things like vertigo happens. Well, why would vertigo happen? If my eyes are not in check, and my vestibular system’s not in control, and my eyes move one way, it’s just like the room moving the other. And now you’re like, “Wow, God, the room is spinning. What’s going on?” And if that information is not in sync with the brain, the brain says, “I don’t even know where we’re at. I can’t even perceive things.” And then, if things don’t project down to the actual… the vestibulospinal pathways, we become a little bit, like, gait-disoriented, so we can’t walk the right way and our reflexes, based upon where we’re at, become abnormal.
So what happens is, we get increased activation of the midbrain, because the deep cerebellar nuclei go whoosh, straight up to the midbrain. That can actually activate the sympathetic chain, which can release epinephrine and norepinephrine. And now we get things like anxiety, heart rate, and increased metabolic rate. Now we get things like my vagal system gets activated, and I get things like nausea. Whoa. Wait until Dr. Kharrazian shows you about the amygdalar pathways and the limbic pathways that go into the IML and how plastic they get. There’s been a lot of myths in the IML and sympathetics and autonomics. We’re going to break a lot of those today.
So, all of the muscle spindles, all of the frontal lobe, all of the vestibular nuclei, they come into the cerebel-lum, the cerebellum says, “Hey thanks. Vestibular system, I’m going to do this for you and make you better, so that you can perceive the world the right way. Hey, thanks for giving me this information, leg. I’m going to make you move the right way by telling the cortex.” And then it gets all the information, it goes over to the cortex, and the cortex says, “Hey cool, thanks. I can give this to the supplementary and premotor areas, and now they can execute movement the right way, and everybody’s good, and by the way, I’ll give you a copy of what I did so that you know it, so you don’t have to do it again.”
And the whole thing is going like this, over and over and over, and inside that cerebellum it’s this: Deep cerebellar nuclei, going. Purkinje system saying, “No, stop.” Basket and stellate systems, bringing the other surrounding areas up or down to work synergistically with the one area being activated. And when you do that, it’s all times out and you’re smooth, and you’re not dysmetric, and you’re not dyssynergetic. And you can stop on a target so you don’t have saccadic hypermetria. And so when you move your leg, you don’t have an abnormal heel-to-shin. And so when you’re walking, you don’t have gait ataxia. And when you’re sitting here, you’re not going back and forth because your eyes are going back and forth and you’re not titubating based upon your eye instability and you can’t fixate. Whew.
And the whole time, you’d better have a thyroid. And the whole time, you’d better have vasculature. And the whole time, you’d better not let your cholesterol go up, with fibrinogen, with CRP, with homocysteine, because if you do, you might get basilar insufficiency, and all the vasculature, including the posterior-inferior

MODULE ONE TRANSCRIPT – CEREBELLUM | COPyRIghT © 2016 FUNCTIONAL NEUROLOgy SEMINARS LP | PAgE 29
and the anterior-inferior cerebellar artery might get blocked. Oooh. Cerebellar stroke. I’ve got four videos of cerebellar strokes. One of them was a linguistics major that went to Cornell. He came in, couldn’t walk, had no tone in his core. He now walks, and he now talks, even though he’s very aprosodic. He was super left-brain dominant. So when his cerebellum crashed, his whole brain crashed. His right-brain was already insufficient, so when he started talking again, he just-started-talking-like-this. And I’m like, “Hey man, we got the cerebellum going again. How about some right-brain exercises?” We started doing that, and he was like, “I LIKE this, a whole LOT,” and so it was just like “Wow, man.” It was like R2-D2 turned into C3PO.
So, know that you are learning about the cerebellum and how it all fits together and works into the frontal lobes, and now other sensory systems are coming up into the parietal lobes, and it’s all matching together, and how all of these sensory tests are going to matter. How all of these movement tests are going to matter. And how, when you put that together with the frontal lobe, it’s going to matter. So what we’re trying to teach you to do is take this beautiful thing called the brain, and say this: “Where’s the freaking problem?”
But sometimes you have to know all of the areas and all of the symptoms to say, “It triangulates right here.” And if it doesn’t make any sense, then you have to say, “It’s something systematic.” Maybe it’s inflammation. Maybe it’s neurodegeneration. And then if you neurodegenerated and area that didn’t… this is what we’re worried about with these iPhones, is that people aren’t developing memory for numbers, and they’re not remembering numbers for facts and figures. So if those don’t develop, and you get a little bit demented later on, how quickly will that function go away? [snap] Just like that. It’s called digital dementia. Look it up. There’s people up in northern Europe that are doing research on it.
I don’t want to make this a big deal about that, but what I want you to understand is that everything we taught you yesterday is coordinated with everything that we’re teaching you right now, and the vestibular system is a slave of the cerebellar system. That’s why we’re teaching it later. And by the way, autonomics are all as a result of what we’ve taught you so far, so we’re going to give it to you last. There was a thought process into why it all went the way it went.
See, a lot of times people will just do autonomics by itself, or cerebellum by itself. But this first module, what we wanted to do is this: Get the paradigm to you, get the philosophy to you, and then talk just enough about all of it to say, “This is how it all fits together. Now we’ll start getting more specific on one area, because you’ve got the big picture,” and what I just gave you is the big picture of the little brain that does a lot.
That’s the end of the cerebellum. Thank you very much.
FunctionalNeurologySeminars.com Courses.FunctionalNeurologySeminars.com