Embed Size (px)
Citation preview
OATS Surgery: What to Know Before Your Procedure When harm occurs to a part of the knee that cannot be repaired traditionally, you have a few options to recover. Osteochondral autograft transfer system (OATS) surgery is a knee repair surgery that uses the patient’s own cartilage to fill in areas where it has been worn down or damaged. This is performed to improve one’s mobility and activity level, as well as to reduce the risk of further damage.
Quick Introduction of what Happens in OATS
If your doctor has recommended OATS, it means that there has been injury to your joint surface. This happens in high impact collisions between the major bones of the knee, likely after or during a severe meniscus tear. This procedure is different from a more common ligament tear surgery where the ligament is replaced or repaired. The joint surface is the main component of weight bearing in the knee and consists of the major bones, covered in a thin layer of cartilage. In this particular surgery, plugs, an undamaged piece of bone and cartilage, are used to replace a damaged area. These are taken from a non-‐weight bearing part of the knee and placed into a defect.
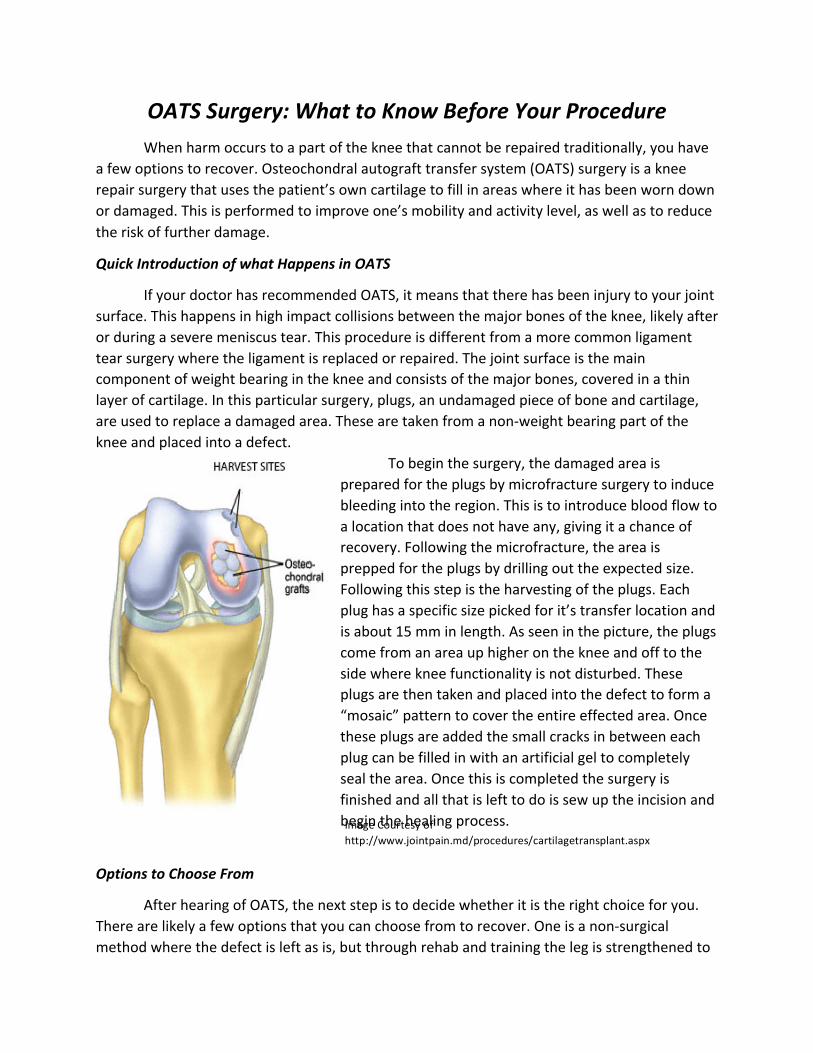
To begin the surgery, the damaged area is prepared for the plugs by microfracture surgery to induce bleeding into the region. This is to introduce blood flow to a location that does not have any, giving it a chance of recovery. Following the microfracture, the area is prepped for the plugs by drilling out the expected size. Following this step is the harvesting of the plugs. Each plug has a specific size picked for it’s transfer location and is about 15 mm in length. As seen in the picture, the plugs come from an area up higher on the knee and off to the side where knee functionality is not disturbed. These plugs are then taken and placed into the defect to form a “mosaic” pattern to cover the entire effected area. Once these plugs are added the small cracks in between each plug can be filled in with an artificial gel to completely seal the area. Once this is completed the surgery is finished and all that is left to do is sew up the incision and begin the healing process.
Options to Choose From
After hearing of OATS, the next step is to decide whether it is the right choice for you. There are likely a few options that you can choose from to recover. One is a non-‐surgical method where the defect is left as is, but through rehab and training the leg is strengthened to
Image Courtesy of http://www.jointpain.md/procedures/cartilagetransplant.aspx
help support the joint. A second option is to have an arthroscopic procedure to clean the area to remove any possible loose bodies and to try to smooth the joint surface. The last and final option is to get the OATS procedure done, which has the best chance of a full recovery. The previous two leave a serious risk of re-‐injury or an increase in defect size and pain over time. There is not yet an established base of information on OATS, but it has been known to have varying results. As more journals with success rates, recovery times and pain levels are completed, a benchmark can be set. Some people have easily been able to return immediately to normal activity after a six-‐month period, but others had increasing problems and never returned to pre-‐surgery strength.
Length and Difficulty of Recovery
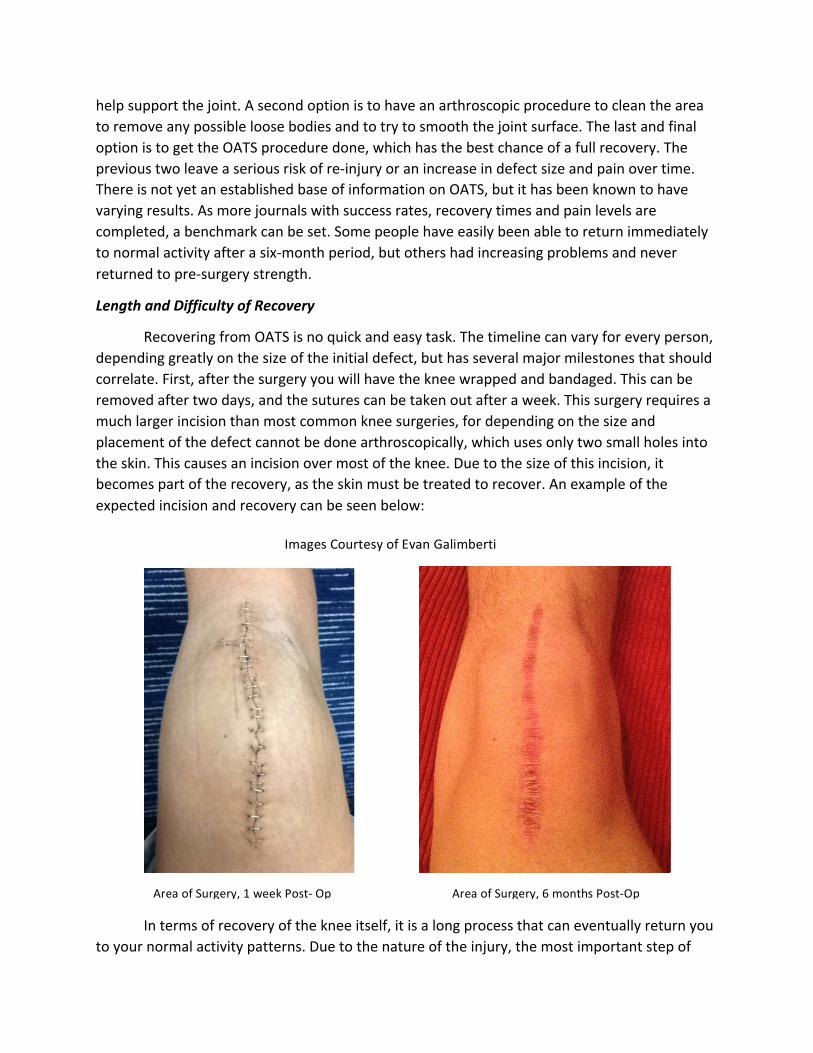
Recovering from OATS is no quick and easy task. The timeline can vary for every person, depending greatly on the size of the initial defect, but has several major milestones that should correlate. First, after the surgery you will have the knee wrapped and bandaged. This can be removed after two days, and the sutures can be taken out after a week. This surgery requires a much larger incision than most common knee surgeries, for depending on the size and placement of the defect cannot be done arthroscopically, which uses only two small holes into the skin. This causes an incision over most of the knee. Due to the size of this incision, it becomes part of the recovery, as the skin must be treated to recover. An example of the expected incision and recovery can be seen below:
In terms of recovery of the knee itself, it is a long process that can eventually return you to your normal activity patterns. Due to the nature of the injury, the most important step of
Area of Surgery, 1 week Post-‐ Op Area of Surgery, 6 months Post-‐Op
Images Courtesy of Evan Galimberti

recovery is to keep from putting pressure on the repaired defect until it has had time to fuse with the surrounding tissue. It is usually six to eight weeks before any weight can be placed on the leg. During this time it is important to begin rebuilding the muscle. The quadriceps loses muscle mass faster than any other muscle in the body, at up to 3% of mass per day of decreased use. For the first one to two weeks, the leg will feel difficult to bend and the quadriceps will likely be unable to contract. After the second week, a stationary bike can be helpful in regaining motion. Simple resistance training with weights can be done until the six to eight weeks are up then one week of crutches can be used to put half of your weight onto the leg. Depending on how this goes the next week can be your first week of putting full weight on the leg. At this point activity can slowly be increased until the six-‐month mark, where depending on your success light jogging can begin until a full range of activity is regained.














![Am Zementwerk Ernst-Thälmann-Straße...2018/08/16 · > ' d Z º ] v P v U Mainzerhofstraße 12, 99084 Erfurt Herr Bernd Peupelmann, 03672-47870 bernd.peupelmann@leg-thueringen.de](https://img.pdfslide.net/doc/110x75/606594c201a1a23b914a0030/am-zementwerk-ernst-thlmann-strae-20180816-d-z-v-p-v-u.jpg)












![How to Make Homemade Biodiesel - Sites at Penn Statesites.psu.edu/.../sites/55100/2016/06/How-to-Make-Homemade-Biodi… · Retrieved from [7] How to Make Homemade Biodiesel Biodiesel](https://img.pdfslide.net/doc/110x75/5b1671a27f8b9a776d8bfbff/how-to-make-homemade-biodiesel-sites-at-penn-retrieved-from-7-how-to-make.jpg)

