Embed Size (px)
Citation preview

Postpartum Hemorrhage
Gayle Olson, M.D.
Department of Obstetrics and Gynecology
University of Texas Medical Branch
Galveston, Texas USA.
Texas 2Step. 2013

Objectives
• Define hemorrhage
• Diagnose postpartum hemorrhage
• Strategies to prevent hemorrhage
• Discuss management options

Maternal Mortality
• Every minute a woman dies
• 529,000 women per year
• 20 suffer injury, infection or disease
• 10 million women per year
www.who.int accessed 2011


Direct Complications of
Childbirth
• Account for 70% mortality
• Fateful Five
• Hemorrhage (25%)
• Infection (15%)
• Unsafe abortion (13%)
• Eclampsia (12%)
• Obstructed labor (8%)
www.who.int accessed Fall 2011

Causes Maternal Death
Asia/Africa
Morbidity Percentage
Haemorrhage 31
Anemia 12.8
Other indirect causes of
deaths 12.5
Sepsis/infection 11.6
Obstructed labour 9.4
Hypertensive disorders 9.1
Khan KS et al. WHO analysis of causes of maternal death: a
systematic review. Lancet, 2006, 367:1066–1074

Causes Maternal Death
Developed Countries
Morbidity Percentage
Other direct causes of
deaths 21.3
Hypertensive disorders 16.1
Embolism 14.9
Other indirect causes of
deaths 14.4
Haemorrhage 13.4
Abortion 8.2
Khan KS et al. WHO analysis of causes of maternal death: a
systematic review. Lancet, 2006, 367:1066–1074

Impact of Hemorrhage on
HealthCare
• 3% of all deliveries.
• Transfusion increased
• 2.4 per 1,000 in 1998-1999
• 4.6 per 1,000 in 2004-2005
• Hysterectomy increased 15%
• Responsible for 10-13% of all deaths

Causes and Predisposing Factors of
Hemorrhage
Placentation
Previa, Accreta,
Percreta
Abruption
Ectopic pregnancy
Hydatidiform mole
Other
Obesity
Previous PPH
Severe preeclampsia,
sepsis,
renal insufficiency
AFE
Von Willebrand

Causes and Predisposing Factors of
Hemorrhage
Trauma
CD or hysterectomy
Episiotomy, forceps,
vacuum, cervical tear
Atony
Overdistended uterus,
LGA, multiples, clots
Induction
Halogenated agents
Exhausted
myometrium

Postpartum Hemorrhage
Definitions
• One or both:
• 10% change in Hct between admission and
postpartum
• need for erythrocyte transfusion
• EBL ≥500 mL for SVD: ≥1000 mL for CD
• Early (within 24 hrs) versus late (24 hrs to
6 weeks)
ACOG Educational Bulletin # 243; 1998
Rath. Acta Obstetricia et Gynecol Scandinavica 2011

Early vs Late PPH
Primary, Early or Acute
Within 24h PP
90% cases
Associated with more bleeding
Secondary or Late
24h – 12 wks pp
1-3% of deliveries
Infection
Retained products
Abnormal uterine involution

Failures in Treatment:
• Lack of consensus for PPH definition
• Lack of local ease-to-use action plans
(protocols)
• Underestimating the extent of hemorrhage
• Delay in blood transfusion/coagulation
factors (or not available)
• Lack of adequate education and training
Rath. Acta Obstetricia et Gynecol Scandinavica 2011

Mistakes Identified by Simulation
Error Percent
Underestimate blood loss 95
Unfamiliar with prostaglandin administration 82
Late transition to the operating room 82
Delayed administration of blood products 66
Unfamiliar dosing of ergot myometrial contractors 60
Essential blood tests carried out 44
Under detection of consumption coagulopathy 36
Source of bleeding not explored 35
Urinary bladder not drained 32
Maslovitz et al. Obstet Gynecol 2007;109:1295-300

Blood Volume in Pregnancy
Parameter % change
Blood volume Increase 45
Plasma volume Increase 55
RBC volume Increase 30
Estimated total blood volume 95mL/Kg during pregnancy
Compared to 75mL/Kg for non-pregnant adult women
An average increase of approx 1250 mL
Replacement considered at 15-20% loss of EBV
A Practical Approach to Obstetric Anesthesia 2009

Allowable Blood Loss (ABL)
EBV x (Hi - Hf)
Hi = ABL Hi = initial Hct
Hf = final lowest acceptable Hct
95 mL/Kg Assume 70kg EBV 6,650
6650 x (30 - 24)
30
= 1,330 mL (20%)

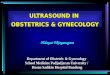
Estimating Blood Loss
4x4 hold ~ 10 mL blood
Ray-techs ~ 10-20 mL blood
Lap sponges ~ 100 mL blood
25 mL 50 mL 75 mL 100 mL
A B C D

Clinical Staging of Postpartum Hemorrhage
Severity Findings SBP % loss Blood Volume
Normal Palpitations,
dizziness,
tachycardia
Normal 10-15 500-1000ml
Mild HR < 100 bpm
Vasoconstriction
Slightly low 15-20% 1000-1500ml
Moderate
HR= 100-120 bpm
Restlessness
Oliguria
70-80
25-35% 1500-2000ml
Severe
HR > 120 bpm
Consciousness
Anuria, air hunger
< 60
≥ 35% 2000-3000ml

Management
Prevent
Mechanical
Medical
Surgical

Impact and Action
• California -2002 and 2003
• 10 of 98 pregnancy-related deaths,
• 70% preventable with improved care
• Maternal Quality Care Collaborative
(CMQCC)

The CMQCC Staged
Approach
• Stage 0 – Active management 3rd stage
• Stage 1 – EBL limits exceeded, stable
• Stage 2 – Continued bleeding, unstable
• Stage 3 – Major obstetric hemorrhage
• EBL > 1500, unstable, coagulopathy
Mhyre J. Anesth 2011

Modified Early Obstetric Warning Scores (MEOWS)1
Contact a physician for early intervention if the patient scores ≥2 at any time
Score 2 1 0 1 2
Pulse ≤40 41-50 51-100 101-120 or
10-20%
increase
>120 or >20%
increase
SBP ≤85 or
>20% decrease
85-100 101-150 151-160 >160
DBP <45 45-80 81-100 >100
SpO2 <95% 95-100%
RR ≤10 11-20 21-30
Temp ≤35.0 35.1-
35.9
36.0-37.9 ≥38.0
CNS Normal Responds Pain response
Anesthesiology 2011, ASA Annual Meeting
Rath. Acta Obstetricia et Gynecol Scandinavica 2011

Prevention
AMTSL
• Prophylactic oxytocin
• Controlled cord traction
• Uterine massage

Mechanical
Bimanual Compression
Operative Obstetrics 1995

Use of AMTSL Tsu VD. J Obstet Gynaecol Res 2006
Outcomes AMTSL Districts Control Districts
Number N=1,236 N=2,371
Bleeding - normal 81.0 81.0
Bleeding-high normal 15.6 14.6
Moderate hemorrhage 2.7 3.8
Severe hemorrhage 0.7 0.5
Third stage > 30 min 1.1 4.6
Third stage > 15 min 5.4 46.7
Effects of AMTSL on PPH and duration of the third stage of labor

Prophylactic Oxytocin Cotter AM et al. Cochrane Database of Systematic Reviews
2001
Oxytocin vs no uterotonics RR 0.50 [95% CI 0.43-0.59]
RR 0.60 [95% CI 0.44-0.87]
RR 0.50 [95% CI 0.39-0.64]
Oxytocin vs ergot alkaloids Little evidence to support
using one drug over the
other
Oxytocin + ergometrine vs
ergot alkaloids
Little evidence to support a
synergist effect

Medical Management Uterotonic Agents
Drug Route Dose NTK
Oxytocin IV, IM, IMM 10-40 U in LR Ø bolus, water
intoxication
Methylergonovine IM, IMM 0.2 mg
Ø IV, hypertension,
coronary insufficiency
Hemabate (15-methyl-PGF2 ) IM, IMM
0.25 mg
Every 15-90 min
max 8 doses
Ø cardiac, pulmonary,
renal or hepatic diseases
Dinoprostone (Prostin E2, PGE2)
rectal,
vaginal
20 mg, every 2
hours
Ø hypotension
Misoprostol (PGE1) rectal,
sublingual
400 – 800 g oral
routes, 800-1000
rectal routes.
Shivering, fever, diarrhea,
increasing with dose


Route of administration Misoprostol (PGE1)
Chong YS. European J Obstet Gyn Reprod Buil 2004

Uterine Packing
Operative Obstetrics 1995

Late - Mechanical Aortic Compression
20 normal non-bleeding parturients
Aortic compression with closed fist at umbilicus
Leg blood pressure
obliterated in 55%
significantly reduced in 10%
Femoral pulse obliterated in all
Systemic blood pressure not significantly affected
Riley & Burgess. Anaesth Intensive Care 1994;22:571-5


SOS Bakri
Tamponade Balloon Catheter
Cook OB/GYN (www.cookmedical.com)

The ebb™ Complete Tamponade System

Uterine Balloon Tamponade Alone Doumouchtsis et al. Obstet Gynecol Surv 2007;62:540-7

Surgical Management of
PPH
D&C if retained products
Repair of lacerations
Uterine compression sutures
Arterial ligation
• Uterine, tubo-ovarian, hypogastric
Pelvic embolization
Hysterectomy
B. Sibai

Uterine Compression Suturing Techniques
• B-Lynch Brace
• Hayman (vertical sutures)
• Cho (multiple square)
• Ouahba et al (2 transverse & 2 lateral)
B. Sibai

•Technique: #2
chromic on a 75 mm
heavy round bodied
needle
•Test: bleeding controlled
by bimanual compression
B-Lynch Suture
B-Lynch C. Br J Obstet Gynecol 1997;104:372-375.

B. Sibai

Zheng J, etal. BJOG 2010

Uterine Compression Suture Alone Doumouchtsis et al. Obstet Gynecol Surv 2007;62:540-7

Uterine Sandwich Nelson & O’Brien. Am J Obstet Gynecol 2007

Blood Supply to Uterus, Cervix, & Vagina
• Uterine fundus
• Uterine arteries (90%)
• Ovarian arteries (10%)
• From aorta
• Internal iliac artery
• Uterine artery
• Cervical branches
• Vaginal branches
• Multiple collaterals
B. Sibai

Postpartum Hemorrhage Hypogastric Artery Ligation
• Pulse pressure 85%
• Blood flow 48%
• Convert arterial flow to venous-like flow
• Allows hemostasis by clot formation


Uterine Artery Ligation



Efficacy of Reported Methods to Control PPH
(mainly uterine atony)
%
Uterine Balloon tamponade 77-88
Uterine compression sutures 84-95
Uterine devascularization 50-60
Uterine Arteries
Utero-ovarian vessels
Hypogastric 50-90
Uterine artery embolization 70-90
Hysterectomy ~100

Placenta Accreta

Placenta Accreta Predisposing Factors
• Placenta previa (by far the most important)
• Uterine scar (previous cesarean section,
myomectomy, metroplasty)
• Advanced maternal age
• Placenta overlying uterine scar
• Multiparity (95 % occurred in multiparae)
• Previous uterine curettage

Ultrasound Findings Suggestive of Accreta
Placental lacunae
• Loss of retroplacental hypoechoic zone
Previous cesarean & previa
• Low-lying gestational sac
• Intraplacental lakes with turbulent flow
• Absent decidua basalis
— Myometrial thickness < 1 mm
Loss of smooth interface with bladder
Focal nodular projections into bladder
• Percreta
B. Sibai













Massive Transfusion Protocol
Activation
• Active bleeding
• SBP < 90 mmHg
• Ph < 7.1
• Base deficit > 6 meq/L
• Temperature < 34º C
• INR > 2
• Platelets < 50,000/mm3

Massive Transfusion Protocol
• Adopts Hemostatic Resuscitation
concepts
• Limits aggressive crystalloids
• Introduces early use of FFP
• Ratio of PRBC:FFP 1:1
• Early use of rFVIIa

rFVIIa

Optimize Factor VII action
Hgb ≥ 7 g/dL
Fibrinogen > 50 -100 mg/dL
Pt & PT < 1.5 x mean control
Platelet count > 50,000 mm3
Normal ionized calcium levels
Serum K+ < 5 mEg/L
Temperature > 32º C and pH > 7.2
B. Sibai

Massive Transfusion Protocol
Obstetrics
PRBC FFP Platelets Cryoprecipitate
Round 1 6 units 6 units 6 units 10 units
Round 2 6 units 6 units 20 units
Round 3 Recombinant activated Factor VII (40 mg/kg)
Round 4 6 units 6 units 6 units 10 units
Round 5 6 units 6 units 10 units
Round 6 Recombinant activated Factor VII (40 mg/kg)
UTMB Blood Bank

Complications from Massive Transfusion
PRBCs
• DIC (dilutional)
• Hypothermia (blood stored at 1-6°C)
• Acidosis (pH of PRBC 6.9-7.0)
• Hypocalcemia (citrate binds to Ca++)
• Hyperkalemia (K+ leaves RBC in stored blood)
• Transfusion-related acute lung injury (TRALI)
B. Sibai

Abdominal Compartment
Syndrome • Third spacing colloids/crystalloids
• Bowel edema, ascites, ileus
• Increased intrabdominal pressure
• Compression abd and retroperitoneal
vessel
• Drop in CO, ↓ BP, oliguria, hypoxemia
• Intraabdominal pressure > 20mmHg + organ
compromise
• Surgical decompression

Assess blood loss & vital signs
Call for help and avoid Chaos
Large bore IV access + fluids
Obtain blood/products
Retained tissues
Previa-accreta
Lacerations
· Cervical/vag
· Perineal
· Extension at c/s
Uterine rupture
Coagulopathy
• Abruptio
• AFE/AFLP
• Anticoagulation
• Bleeding
• VW disease
Atony inversion
• Blood products
•Surgery
• Resuscitation
• Supportive care

30 y/o, 39 weeks, Prev CD x 3, ultrasound
report normal, for repeat, its you, scub tech,
anesthesia, small hospital-USA, you find

Summary
Suspicion of Hemorrhage
• Avoid Chaos
• Transfer to a tertiary care center
• Multidisciplinary team: Anesthesia,
blood bank, Interventional Radiology,
Pediatrics
• Surgical planning, OR preparation
• Postpartum diligence

Thank You

Also Consider:

Thromboelastogram
• Whole blood
hemostasis testing
• Measures
mechanical
properties of a clot
• Time to fibrin
formation
• Strength of the clot
• Fibrinolysis Haemonetics


Femoral Balloons

Prophylactic Balloon Catheters Zacharias et al. Am J Obstet Gynecol 2004
Cases Controls P
Estimated blood loss (ml) 3450 3320 NS
Transfused units of
PRBCs (median)
3 3 NS
Minutes in operating room 180 135 NS
Intensive care unit 33% 14% NS
Postoperative day
discharged (median)
6 5 NS

Acute Normovolemic
Hemodilution
• Presumption of bleeding
• Hemoglobin > 10g/dL
• No evidence of cardiovascular disease
• Remove 500-1000 mL whole blood
• Colloid 1:1 ratio replacement
• Crystalloid 3:1 ratio replacement
• Stable when stored for up to 6 hours

Intraoperative Cell Salvage
• Collects blood aspirated from the
surgical site
• Filters and concentrates PRBC
• Hematocrit 55-80%
• No current evidence of iatrogenic AFE

Ligasure

LigaSure
• Pressure +energy for tissue fusion
• Permanently fuses vessels to 7mm
• Seal cycle 2-4 seconds
• Automatically stops when seal complete

• RCT of TXA for PPH
• Ongoing
• Enrollment 15,000