Embed Size (px)
DESCRIPTION
Here is a free sample chapter from the "Educational Review Manual in Obstetrics and Gynecology" published by Castle Connolly Graduate Medical Publishing (CCGMP)www.ccgmp.com.The digital edition of this manual is now FREE for all doctors: www.ccgmp.com Visit our Facebook page: www.facebook.com/ccgmp
Citation preview
Obstetrics and Gynecology - 2009Editor-in-Chief
Rogerio A. Lobo, M.D.Professor of Obstetrics & Gynecology,College of Physicians and Surgeonsof Columbia University, New York, NY

CHAPTER 9: OBSTETRIC COMPLICATIONS 217
Contents
1. Cervical Insufficiency
2. PretermLabor
3. Post-termPregnancy
4. Hypertensive Disorders of Pregnancy
5. Intrauterine Fetal Demise
6. IntrauterineGrowthRestriction
7. Multiple Pregnancy
8. Premature Rupture ofMembranes
9. AntepartumHemorrhage
10. References
11. Questions
Chapter9:Obstetric
ComplicationsErrol R. Norwitz,MD,PhD
Men-Jean Lee,MD
1. Cervical Insufficiency
Cervical insufficiency (also known as cervical incom-petence) is defined as a functional weakness of thecervix resulting in a failure to carry a pregnancy toterm.1, 2 It complicates 0.1%-2% of all pregnancies,and is estimated to be responsible for 15% of deliver-ies between 16 and 28 weeks of gestation.3-5 The clas-sic presentation is that of painless cervical dilatationand shortening without evidence of uterinecontractions.6
Etiology
Some risk factors for cervical insufficiency aredescribed (Table 1), but most patients have no riskfactors.1, 2
The exact etiology of cervical insufficiency has notbeen elucidated.6
Diagnosis
Cervical insufficiency is a clinical diagnosis charac-terized by acute, painless dilatation of the cervix, usu-ally in the mid-trimester (generally between 16-24weeks), culminating in fetal membrane prolapseand/or premature rupture of the membranes (PROM)with resultant preterm and often previable delivery.
Management
Cervical cerclage has become the mainstay for themanagement of cervical insufficiency. If the priorpreterm delivery was the result of preterm labor (docu-mented active contractions) and not cervical insuffi-ciency, cerclage placement is not indicated.2
Types of CerclageProphylactic (elective) cervical cerclage is indicatedin women with a history of prior pregnancy loss and/orpreterm delivery with a history consistent with cervicalinsufficiency, because the probability of recurrence ofcervical insufficiency in a subsequent pregnancy is15%-30%.1, 7, 8 Prophylactic cervical cerclage is placedmost commonly at 13-16 weeks of gestation, at whichtime the complication rate is low (<1%).2 Prophylacticcerclage for diethylstilbestrol (DES) exposure (whenthe patient was exposed in utero to DES taken by hermother) alone remains controversial. Most cliniciansbelieve that a history of in uteroDES exposure per se(without a history of prior pregnancy loss) is not anindication for prophylactic cerclage placement. Simi-larly, elective cerclage has not been shown to be benefi-cial in women with multiple pregnancies without aprior history of cervical insufficiency.9-12
The primary indication for emergent (salvage, res-cue) cervical cerclage is premature effacement and/ordilatation of the cervix in the absence of labor prior to28 weeks gestation. It is associated with a less than50% success rate. Poor prognostic features include cer-vical dilatation >4 cm and prolapsed membranes. In
218 OBSTETRICS ANDGYNECOLOGY—2009
Table 1
Risk Factors for Cervical Insufficiency
Congenital Acquired
Müllerian abnormalities Cervical trauma (prior surgical or(congenital cervical hypoplasia or aplasia) obstetric trauma)
In uterodiethylstilbestrol (DES) exposure Connective tissue abnormalities(Ehlers-Danlos syndrome)
CHAPTER 9: OBSTETRIC COMPLICATIONS 219
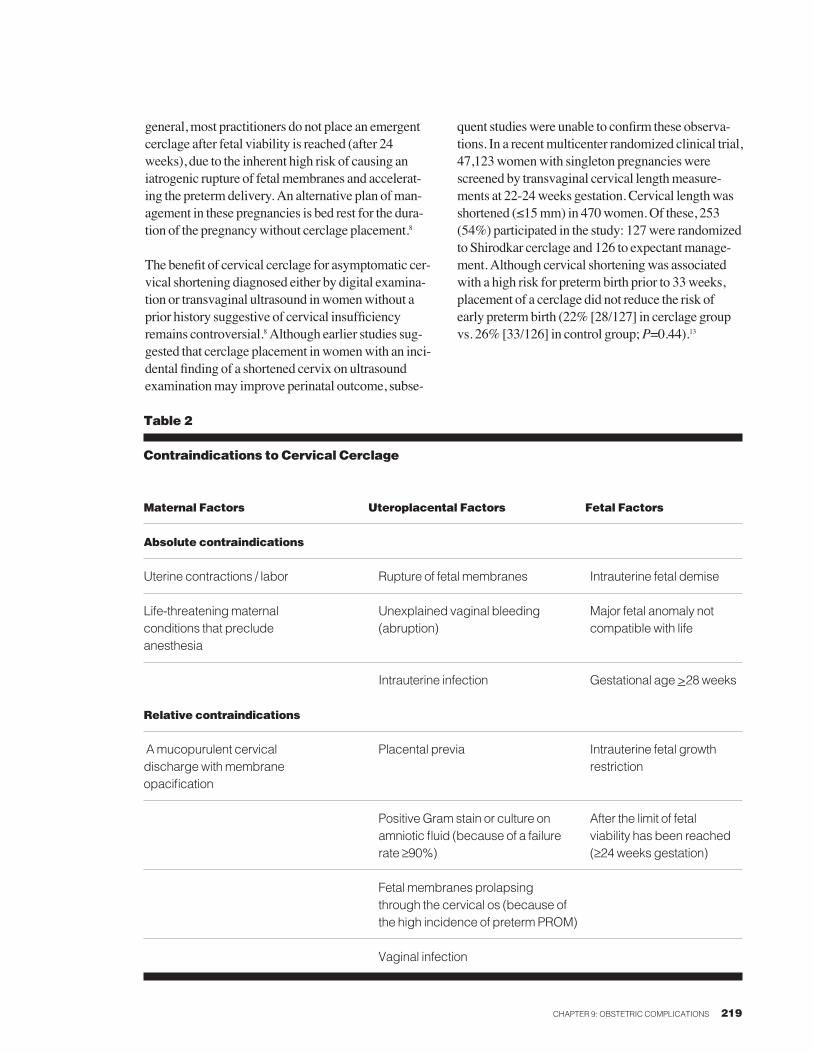
general, most practitioners do not place an emergentcerclage after fetal viability is reached (after 24weeks), due to the inherent high risk of causing aniatrogenic rupture of fetal membranes and accelerat-ing the preterm delivery. An alternative plan of man-agement in these pregnancies is bed rest for the dura-tion of the pregnancy without cerclage placement.8
The benefit of cervical cerclage for asymptomatic cer-vical shortening diagnosed either by digital examina-tion or transvaginal ultrasound in women without aprior history suggestive of cervical insufficiencyremains controversial.8 Although earlier studies sug-gested that cerclage placement in women with an inci-dental finding of a shortened cervix on ultrasoundexamination may improve perinatal outcome, subse-
quent studies were unable to confirm these observa-tions. In a recent multicenter randomized clinical trial,47,123 women with singleton pregnancies werescreened by transvaginal cervical length measure-ments at 22-24 weeks gestation. Cervical length wasshortened (≤15 mm) in 470 women. Of these, 253(54%) participated in the study: 127 were randomizedto Shirodkar cerclage and 126 to expectant manage-ment. Although cervical shortening was associatedwith a high risk for preterm birth prior to 33 weeks,placement of a cerclage did not reduce the risk ofearly preterm birth (22% [28/127] in cerclage groupvs. 26% [33/126] in control group;P=0.44).13
Table 2
Contraindications to Cervical Cerclage
Maternal Factors Uteroplacental Factors Fetal Factors
Absolute contraindications
Uterine contractions / labor Rupture of fetalmembranes Intrauterine fetal demise
Life-threateningmaternal Unexplained vaginal bleeding Major fetal anomaly notconditions that preclude (abruption) compatible with lifeanesthesia
Intrauterine infection Gestational age>28weeks
Relative contraindications
Amucopurulent cervical Placental previa Intrauterine fetal growthdischargewithmembrane restrictionopacification
PositiveGramstain or culture on After the limit of fetalamniotic fluid (because of a failure viability has been reachedrate ≥90%) (≥24weeks gestation)
Fetalmembranes prolapsingthrough the cervical os (because ofthe high incidence of pretermPROM)
Vaginal infection
Contraindications. Contraindications to cerclage arelisted in Table 2. Intra-amniotic infection is an abso-lute contraindication to cerclage placement,14, 15 andthe presence of bacteria on Gram stain or a positiveculture from preoperative amniocentesis is associatedwith a failure rate of >90%. Preoperative amniocente-sis in asymptomatic patients with cervical insuffi-ciency may be considered prior to emergent cerclageplacement. Although ACOG supports cervical cer-clage placement up to 28 weeks gestation, many prac-titioners would not recommend cerclage placementbeyond the limit of fetal viability (≥24 weeks),because the risk of complications outweighs thepotential benefit.7, 16 Furthermore, placement of a cer-clage in a patient that is in preterm labor (actively con-tracting) is contraindicated due to the risks of cervicaltrauma and/or uterine rupture caused by maternal con-tractions against a surgically sutured cervix.
Technical considerations. Once the decision has beenmade to proceed with cerclage placement, a preopera-tive ultrasound examination should be performed toconfirm fetal viability and exclude major structuralanomalies. Regional anesthesia is preferred to generalendotracheal anesthesia because of the decreasedmaternal morbidity. Prophylactic tocolysis may beused to inhibit transient uterine contractions associ-ated with emergent cerclage placement, but there is noobjective evidence that tocolysis improves outcome.Prophylactic broad-spectrum antibiotics are recom-mended for emergent cerclage placement. However,there are insufficient data to recommend routine useof prophylactic antibiotics for elective cerclage place-ment. If the fetal membranes are found to be prolaps-ing through the external os, the risk of iatrogenic rup-ture of the fetal membranes may be as high as 50%.Trendelenburg position,17 retrograde filling of thebladder,18 placement of a 30 mLFoley cathetertrancervically past the internal os and filling the bal-loon,19 placement of a moistened sponge forceps intothe cervical os,20 and/or therapeutic amniocentesis21-23
can be used to reduce the fetal membranes prior to cer-clage placement. In addition, the edges of the cervixcan be grasped by sponge forceps to build length tothe cervix for cerclage placement.24
Transvaginal cervical cerclage has been the mainstayfor the management of cervical insufficiency. Thereare 2 basic types of transvaginal cerclage placementtechniques: Shirodkar and McDonald.25 The choice of
cervical cerclage is best left to the discretion of theobstetric care provider, especially in the setting of aprophylactic cerclage. The selection of the type of cer-clage placement for emergent cases may be limited bythe thickness and length of cervical tissue availablefor suture placement. The choice of suture materialhas evolved over the decades from fascia lata or silk tocurrently a wide selection of non-absorbable sutures,including Mersilene® tape (Dacron® tape), Prolene®
(monofilament), and Ethibond® (braided, coatedpolyester).26 The choice of suture is based on practi-tioner preference and choice of technique. Shirodkarcerclage is a single suture placed submucosallyaround the cervix at the level of the internal os aftersurgically reflecting the bladder anteriorly and the rec-tum posteriorly.27 The suture can be secured anteriorlyor posteriorly, and the mucosal incisions closed.McDonald cerclage is 1 or more purse-string suturesaround the cervix placed without dissection of thebladder or rectum.20 These 2 types of cerclage arelikely equally efficacious, but have never been tested“head-to-head” in a well-designed clinical trial.Transabdominal cerclage has not been compareddirectly with transvaginal cerclage, and is a far moreinvasive procedure requiring a laparotomy and subse-quent cesarean delivery. Transabdominal cerclageshould therefore be reserved for women in whom aprophylactic cerclage is indicated but technicallyimpossible to place transvaginally or that have failedprevious prophylactic transvaginal cerclageplacement.28, 29
Once a cerclage is in place, weekly or biweekly fol-low-up visits for cervical examinations are probablysufficient in the absence of clinical symptoms. Cervi-cal assessment may be by simple bimanual examina-tion or by ultrasound to assess the length of cervix,any loosening of the suture or prolapse of membranesthrough the suture, tearing of the cervix, loss of thesurgical knot, or loss of the suture. Modified bed restand “pelvic rest” (no coitus, tampons, or douching)are usually recommended until a favorable gestationalage is reached, but without proven benefit. The cer-clage is usually removed electively at 37 weeks gesta-tion, but earlier removal may be necessary in the eventof premature uterine contractions. In the setting ofpreterm PROM, evidence of amnionitis shouldprompt immediate removal of the cerclage. In pretermPROM without evidence of infection, the risk of pre-mature delivery with removal must be weighed
220 OBSTETRICS ANDGYNECOLOGY—2009
CHAPTER 9: OBSTETRIC COMPLICATIONS 221
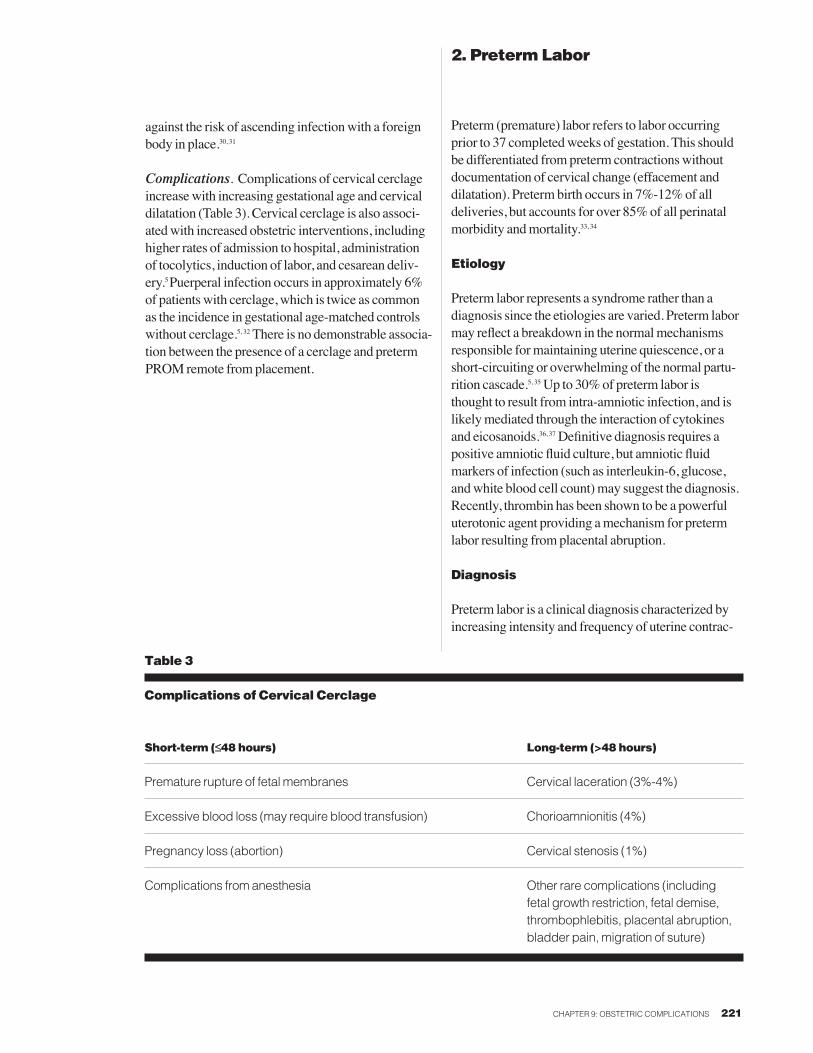
Table 3
Complications of Cervical Cerclage
Short-term (≤≤48 hours) Long-term (>48 hours)
Premature rupture of fetal membranes Cervical laceration (3%-4%)
Excessive blood loss (may require blood transfusion) Chorioamnionitis (4%)
Pregnancy loss (abortion) Cervical stenosis (1%)
Complications from anesthesia Other rare complications (including fetal growth restriction, fetal demise, thrombophlebitis, placental abruption, bladder pain, migration of suture)
against the risk of ascending infection with a foreignbody in place.30, 31
Complications. Complications of cervical cerclageincrease with increasing gestational age and cervicaldilatation (Table 3). Cervical cerclage is also associ-ated with increased obstetric interventions, includinghigher rates of admission to hospital, administrationof tocolytics, induction of labor, and cesarean deliv-ery.5 Puerperal infection occurs in approximately 6%of patients with cerclage, which is twice as commonas the incidence in gestational age-matched controlswithout cerclage.5, 32 There is no demonstrable associa-tion between the presence of a cerclage and pretermPROM remote from placement.
2. Preterm Labor
Preterm (premature) labor refers to labor occurringprior to 37 completed weeks of gestation. This shouldbe differentiated from preterm contractions withoutdocumentation of cervical change (effacement anddilatation). Preterm birth occurs in 7%-12% of alldeliveries, but accounts for over 85% of all perinatalmorbidity and mortality.33, 34
Etiology
Preterm labor represents a syndrome rather than adiagnosis since the etiologies are varied. Preterm labormay reflect a breakdown in the normal mechanismsresponsible for maintaining uterine quiescence, or ashort-circuiting or overwhelming of the normal partu-rition cascade.5, 35 Up to 30% of preterm labor isthought to result from intra-amniotic infection, and islikely mediated through the interaction of cytokinesand eicosanoids.36, 37 Definitive diagnosis requires apositive amniotic fluid culture, but amniotic fluidmarkers of infection (such as interleukin-6, glucose,and white blood cell count) may suggest the diagnosis.Recently, thrombin has been shown to be a powerfuluterotonic agent providing a mechanism for pretermlabor resulting from placental abruption.
Diagnosis
Preterm labor is a clinical diagnosis characterized byincreasing intensity and frequency of uterine contrac-

222 OBSTETRICS AND GYNECOLOGY—2009
tions leading to effacement and dilatation of thecervix, and culminating in expulsion of the productsof conception prior to 37 weeks of gestation.
Management
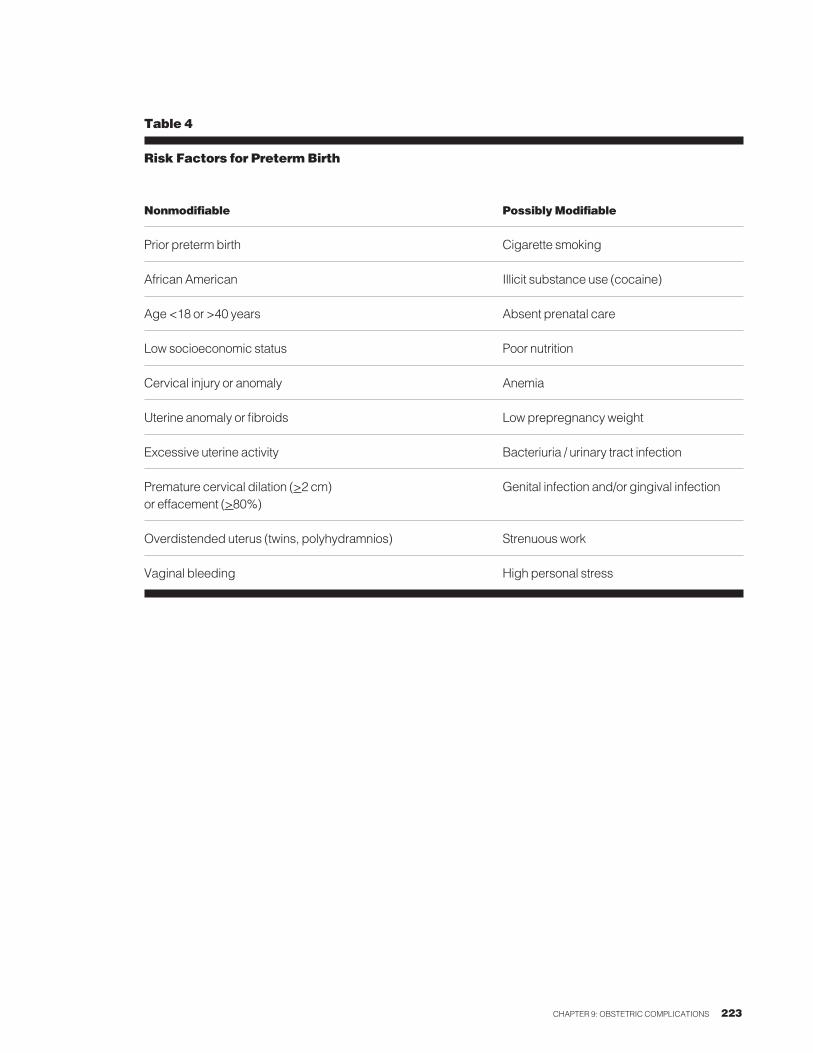
ScreeningSeveral risk factors for preterm labor have beendescribed (Table 4). However, risk factor screeningalone will fail to identify over 50% of pregnancies thatdeliver preterm.38, 39 As such, a number of modalitieshave been developed in an attempt to identify womenat high-risk of preterm birth (Table 5).40-50 Currently,the most reliable screening tests include serial sono-graphic measurement of cervical length42, 43 and/ormeasurement of fetal fibronectin (fFN) in cervicov-aginal secretions.46-48
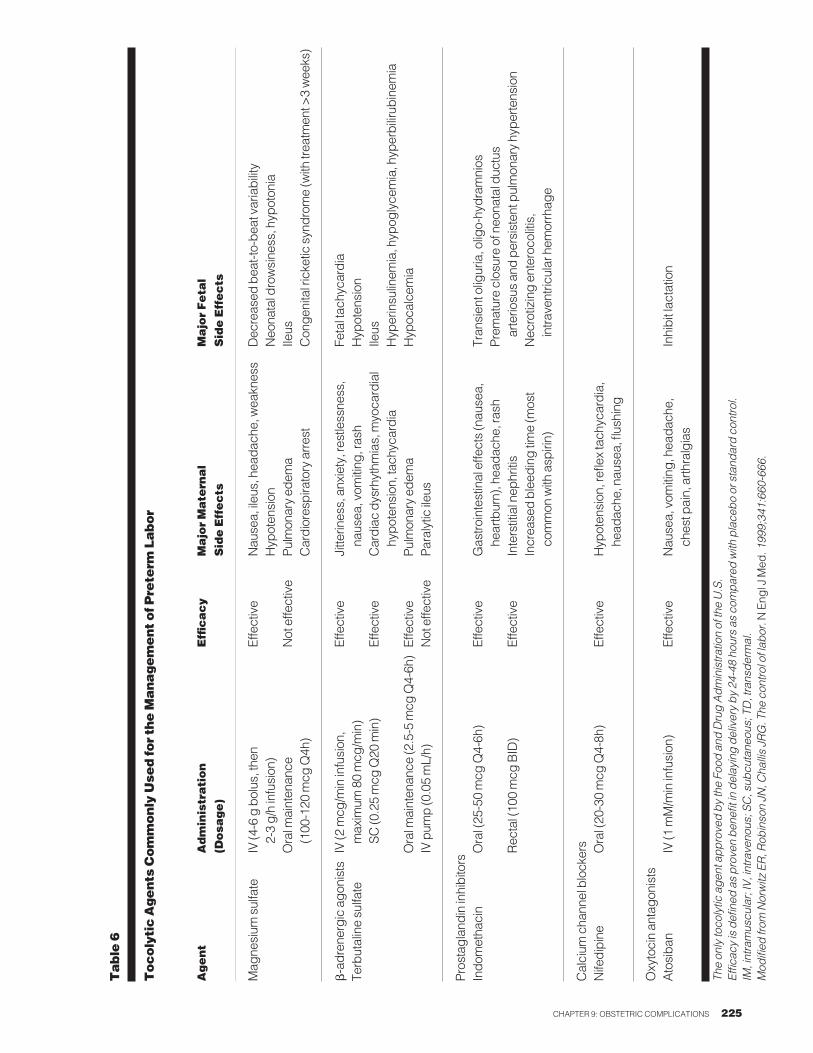
Clinical ManagementIn the setting of preterm labor, bed rest and hydrationare commonly recommended but without proven effi-cacy.51 Pharmacologic tocolytic therapy remains thecornerstone of modern management. Although anumber of alternative agents are now available (Table6), only ritodrine hydrochloride has received approvalfrom the Food and Drug Administration (FDA) of theUnited States (FDA) for the treatment of pretermlabor. The risks and benefits of the individual drugshave been reviewed in detail elsewhere.35, 52-54 All ofthe recommended agents appear equally effective indelaying delivery for 24-48 hours, thereby creating awindow of opportunity for antenatal corticosteroidadministration. There is no good clinical evidence thatany of these agents can prolong pregnancy beyond 48hours and prevent preterm delivery.55 Since no singleagent has a clear therapeutic advantage, the side-effectprofile of each of the drugs will often determine whichto use in a given clinical setting.
Intravenous magnesium sulfate as a continuous infu-sion has a wide margin of safety and has traditionallybeen regarded as the first-line agent for use in pretermlabor in North America. More recently, however, thisagent has fallen out of favor because of its potentialrisk of maternal cardiopulmonary failure from over-dose or neonatal rickets and neurologic injury fromprolonged or excessive use.56, 57 Adrenergic agonistsare commonly used (eg, subcutaneous terbutaline inan injection, continuous infusion or oral administra-
tion), but have a higher incidence of adverse effects,including maternal tachycardia, EKG changes, andhyperglycemia.55, 58, 59 Indomethacin, although effec-tive, may be associated with fetal complications suchas oligohydramnios and premature closure of the duc-tus arteriosus, as well as serious neonatal complica-tions, such as patent ductus arteriosus that is refrac-tory to pharmacological therapy, especially if givenshortly prior to delivery.60-63 Calcium channel block-ers (nifedipine and amlodipine) are becomingincreasing popular agents for tocolysis, since they canbe orally administered, but maternal hypotension andcardiac arrhythmias are a concern.64, 65 Promisingnewer agents include oxytocin receptor antagonists(used commonly in Europe) and selective cyclooxy-genase-2 inhibitors.66, 67
A single course of antenatal glucocorticoidsdecreases the incidence of respiratory distress syn-drome (RDS), intraventricular hemorrhage (IVH),and necrotizing enterocolitis (NEC) by 50%, and isrecommended for all pregnancies at high risk ofdelivering before 34 weeks gestation with intactmembranes and before 32 weeks gestation withpreterm PROM.68-70 Maximal benefit is achieved 24-48 hours after the initial dose. This effect lasts for 7days, but it is unclear what happens thereafter.Repeated courses of steroids are not generally recom-mended, although a single rescue dose (or rescuecourse) may be appropriate if the initial course wasadministered prior to 28-30 weeks gestation.71, 72
Tocolysis should be continued until preterm labor hasbeen effectively halted, or empirically until 48 hoursafter the first dose of corticosteroid. Maintenancetocolytic (including terbutaline pump or chronic oraltocolysis) therapy has not been shown to confer anytherapeutic benefit73, 74 and poses a risk of adverse sideeffects. Similarly, concurrent use of 2 or moretocolytic agents has not consistently been shown to bemore effective than a single agent and exposes theparturient to cumulative risk of side effects, includingpulmonary edema.75, 76 The use of sequential therapy,however, may be beneficial if initial therapy is unsuc-cessful.77 Although effective in the setting of pretermPROM, there is no role for broad-spectrum antibiotictherapy to prolong latency in preterm labor with intactmembranes.78
CHAPTER 9: OBSTETRIC COMPLICATIONS 223
Table 4
Risk Factors for Preterm Birth
Nonmodifiable Possibly Modifiable
Prior preterm birth Cigarette smoking
African American Illicit substance use (cocaine)
Age <18 or >40 years Absent prenatal care
Low socioeconomic status Poor nutrition
Cervical injury or anomaly Anemia
Uterine anomaly or fibroids Low prepregnancy weight
Excessive uterine activity Bacteriuria / urinary tract infection
Premature cervical dilation (>2 cm) Genital infection and/or gingival infectionor effacement (>80%)
Overdistended uterus (twins, polyhydramnios) Strenuous work
Vaginal bleeding High personal stress
224 OBSTETRICS AND GYNECOLOGY—2009
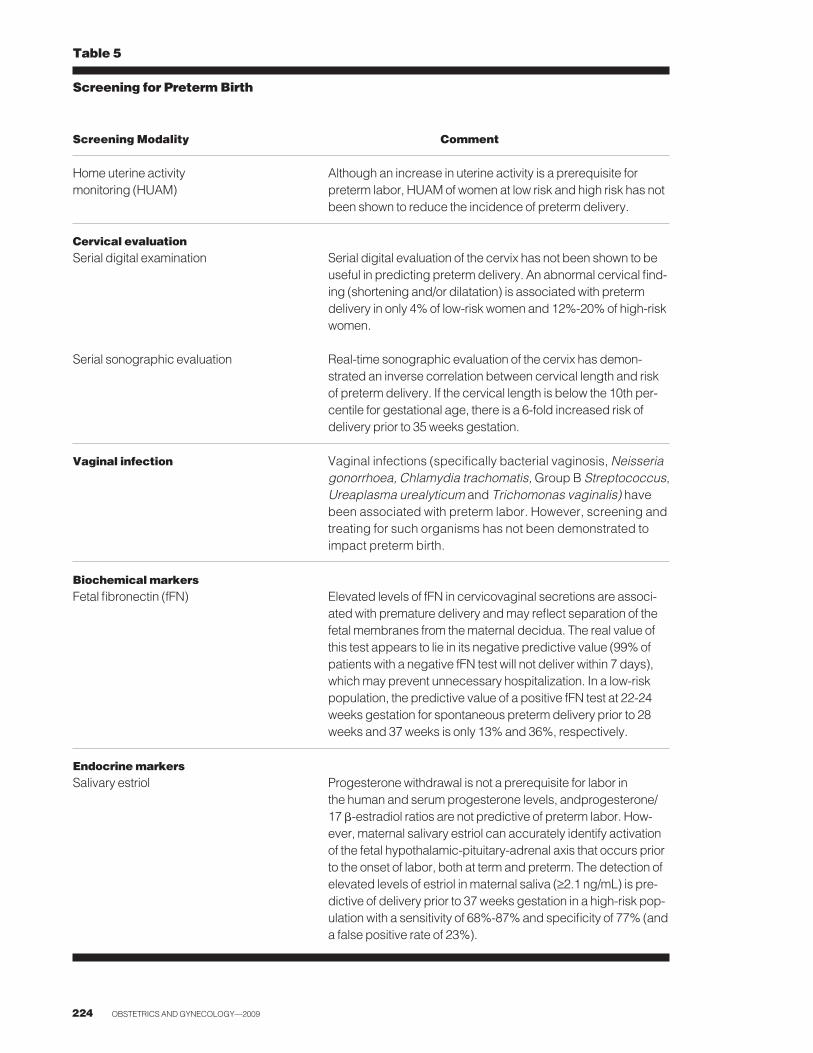
Table 5
Screening for Preterm Birth
Screening Modality Comment
Home uterine activity Although an increase in uterine activity is a prerequisite for monitoring (HUAM) preterm labor, HUAM of women at low risk and high risk has not
been shown to reduce the incidence of preterm delivery.
Cervical evaluationSerial digital examination Serial digital evaluation of the cervix has not been shown to be
useful in predicting preterm delivery. An abnormal cervical find-ing (shortening and/or dilatation) is associated with preterm delivery in only 4% of low-risk women and 12%-20% of high-risk women.
Serial sonographic evaluation Real-time sonographic evaluation of the cervix has demon-strated an inverse correlation between cervical length and riskof preterm delivery. If the cervical length is below the 10th per-centile for gestational age, there is a 6-fold increased risk ofdelivery prior to 35 weeks gestation.
Vaginal infection Vaginal infections (specifically bacterial vaginosis, Neisseriagonorrhoea, Chlamydia trachomatis, Group B Streptococcus, Ureaplasma urealyticum and Trichomonas vaginalis) havebeen associated with preterm labor. However, screening andtreating for such organisms has not been demonstrated toimpact preterm birth.
Biochemical markersFetal fibronectin (fFN) Elevated levels of fFN in cervicovaginal secretions are associ-
ated with premature delivery and may reflect separation of thefetal membranes from the maternal decidua. The real value ofthis test appears to lie in its negative predictive value (99% ofpatients with a negative fFN test will not deliver within 7 days),which may prevent unnecessary hospitalization. In a low-riskpopulation, the predictive value of a positive fFN test at 22-24weeks gestation for spontaneous preterm delivery prior to 28weeks and 37 weeks is only 13% and 36%, respectively.
Endocrine markersSalivary estriol Progesterone withdrawal is not a prerequisite for labor in
the human and serum progesterone levels, andprogesterone/17 �-estradiol ratios are not predictive of preterm labor. How-ever, maternal salivary estriol can accurately identify activationof the fetal hypothalamic-pituitary-adrenal axis that occurs priorto the onset of labor, both at term and preterm. The detection ofelevated levels of estriol in maternal saliva (≥2.1 ng/mL) is pre-dictive of delivery prior to 37 weeks gestation in a high-risk pop-ulation with a sensitivity of 68%-87% and specificity of 77% (anda false positive rate of 23%).
CHAPTER 9: OBSTETRIC COMPLICATIONS 225
Table 6
Tocolytic Agents Commonly Used for the Management of Preterm
Labor
Agent
Administration
Efficacy
Major Maternal
Major Fetal
(Dosage)
Side Effects
Side Effects
Mag
nesium
sulfate
IV (4
-6 g bolus
, the
nEffective
Nau
sea, ileu
s, hea
dach
e, wea
knes
sDec
reas
ed bea
t-to-be
at variability
2-3 g/h infusion
)Hyp
oten
sion
Neo
natal drowsine
ss, hyp
oton
ia
Oral m
ainten
ance
Not effe
ctive
Pulm
onary ed
ema
Ileus
(100
-120
mcg
Q4h
)Cardiores
piratory arres
tCon
genital ricke
tic syn
drom
e (w
ith trea
tmen
t >3 wee
ks)
�-adren
ergic ag
onists
IV (2
mcg
/min infusion
,Effective
Jitte
rines
s, anx
iety, res
tlessne
ss,
Fetal tac
hyca
rdia
Terbutaline su
lfate
max
imum
80 mcg
/min)
naus
ea, vom
iting
, ras
hHyp
oten
sion
SC
(0.25 mcg
Q20
min)
Effective
Cardiac
dysrhythm
ias, m
yoca
rdial
Ileus
hypo
tens
ion, tach
ycardia
Hyp
erinsu
linem
ia, hyp
oglyce
mia, hyp
erbilirub
inem
iaOral m
ainten
ance
(2.5-5 m
cg Q4-6h
)Effective
Pulm
onary ed
ema
Hyp
ocalce
mia
IV pum
p (0.05 mL/h)
Not effe
ctive
Paralytic
ileu
s
Pros
taglan
din inhibitors
Indo
metha
cin
Oral (25
-50 mcg
Q4-6h
)Effective
Gas
trointestinal effe
cts (nau
sea,
Tran
sien
t olig
uria, olig
o-hy
dram
nios
heartburn), hea
dach
e, ra
shPrem
ature clos
ure of neo
natal duc
tus
Rec
tal (10
0 mcg
BID)
Effective
Interstitial nep
hritis
arterio
sus an
d pe
rsistent pulmon
ary hy
perte
nsion
Increa
sed blee
ding
time (m
ost
Nec
rotizing en
teroco
litis,
common
with
asp
irin)
intra
ventric
ular hem
orrhag
e
Calcium
cha
nnel block
ers
Nife
dipine
Oral (20
-30 mcg
Q4-8h
)Effective
Hyp
oten
sion
, refl
ex tach
ycardia,
head
ache
, nau
sea, flus
hing
Oxytocin an
tago
nists
Atosiba
nIV (1
mM/m
in infusion
)Effective
Nau
sea, vom
iting
, hea
dach
e,Inhibit lac
tatio
nch
est p
ain, arth
ralgias
The only tocolytic agent approved by the Food and Drug Administration of the U.S.
Efficacy is defined as proven benefit in delaying delivery by 24-48 hours as com
pared with placebo or standard control.
IM, intramuscular; IV, intravenous; SC, subcutaneous; TD, transdermal.
Modified from
Norwitz ER, Robinson JN, Challis JRG. The control of labor. N
Eng
l J M
ed.1999;341:660-666.
3. Post-term Pregnancy
Post-term (prolonged) pregnancy refers to a preg-nancy that has extended to or beyond a gestational ageof 42.0 weeks (294 days) from the first day of the lastmenstrual period.79, 80 In the United States, around10% of all singleton pregnancies continue beyond 42weeks of gestation and 4% continue beyond 43 completed weeks in the absence of obstetric interven-tion.79, 80 Post-term pregnancy should be differentiatedfrom a post-mature pregnancy, which is a distinct clin-ical fetal syndrome consisting of a fetus that has wrin-kled, peeling skin with a thin body, and meconium-stained skin and nails that is diagnosed postnatally.81, 82
Etiology
Primiparity and prior post-term pregnancy are themost common identifiable risk factors for a post-termpregnancy. Rarely, post-term pregnancy may be asso-ciated with placental sulfatase deficiency or fetalanencephaly (in the absence of polyhydramnios).Genetic predisposition may also play a role. However,in the vast majority of cases, the cause of post-termpregnancy is unknown.79
Diagnosis
Accurate pregnancy dating is critical to the diagnosis.The incidence of post-term pregnancy depends uponthe patient population, including such factors as thepercentage of primigravid women, women with preg-nancy complications, the prevalence of ultrasoundassessment of gestational age and the frequency ofspontaneous preterm birth. Local practice patterns,such as the rates of scheduled cesarean delivery androutine labor induction, will also affect the overallincidence of post-term birth.
Complications
Post-term pregnancy is associated with both fetaland maternal risks. Perinatal mortality (stillbirthsplus early neonatal deaths) at ≥42 weeks of gestationis twice that at term (4-7 vs. 2-3 per 1000 deliveries)and increases 4-fold at 43 weeks and 5- to 7-fold at44 weeks.79, 80, 83 Chronic uteroplacental insuffi-ciency, asphyxia and intrauterine infection all con-tribute to the excess perinatal deaths. Post-terminfants are larger than term infants, with a higherincidence of macrosomia (defined as an estimated
fetal weight > 4500 g84 ) (2.5%-10% vs. 0.8%-1%).85, 86 Complications associated with fetal macro-somia include prolonged labor, cephalopelvic dis-proportion and shoulder dystocia, with resultantrisks of orthopedic or neurologic injury.84 Post-termpregnancies are also at increased risk of umbilicalcord compression from oligohydramnios, nonreas-suring fetal antepartum or intrapartum assessment,meconium aspiration, short-term neonatal complica-tions (hypoglycemia, seizures) and long-term neuro-logic sequelae.
Maternal risks of prolonged pregnancy include anincrease in labor dystocia (9%-12% vs. 2%-7% atterm), an increase in severe perineal injury (3.3% vs.2.6% at term) and a doubling in the rate of cesareandelivery.87-89 The latter is associated with higher risksof complications such as endometritis, hemorrhage,and thromboembolic disease.
Management
An accurately estimated date of delivery should becalculated early in pregnancy. This may be basedupon a known last menstrual period in women withregular, normal menstrual cycles and confirmatoryuterine sizing. Uncertainty in historical or physicaldating parameters should prompt ultrasound assess-ment of gestational age.90
Post-term pregnancy is an accepted indication forantenatal fetal monitoring. ACOG has recommendedthat antepartum fetal surveillance be initiated after 42weeks of gestation, without a specific recommenda-tion regarding type of test or frequency.79, 80 Options forevaluating fetal well-being include weekly or twiceweekly nonstress testing with amniotic fluid volumeassessment, the biophysical profile (BPP) or modifiedBPP, the oxytocin challenge test or a combination ofthese modalities; no single method has been shown tobe superior. Umbilical artery Doppler velocimetrytesting alone has not been shown to be beneficial inmonitoring the post-term fetus.79 It should be notedthat there is insufficient evidence to show that initiat-ing antenatal surveillance between 40 and 42 weeks ofgestation improves pregnancy outcome or confers anybenefit to the fetus.79
226 OBSTETRICS AND GYNECOLOGY—2009

CHAPTER 9: OBSTETRIC COMPLICATIONS 227
Delivery is recommended when the risks to the fetusby continuing the pregnancy are greater than thosefaced by the neonate after birth. Both expectant man-agement and labor induction are associated with lowcomplication rates in low-risk post-term gravida.91-93
Factors that need to be considered include gestationalage, results of antepartum fetal assessment, favorabil-ity of the cervix, and maternal preference. Deliveryshould be initiated immediately if there is evidence offetal compromise or oligohydramnios. There doesappear to be a small advantage to routine induction oflabor at 41 weeks gestation, regardless of parity ormethod of induction.87, 88 In women with unfavorablecervical exams, the routine use of preinduction cervi-cal ripening has resulted in fewer failed and serialinductions, lower fetal and maternal morbidity, ashorter hospital stay, lower medical cost and possiblya lower rate of cesarean delivery in the general obstet-ric population. The post-term fetus is at increased riskof intrapartum fetal heart rate abnormalities and pas-sage of meconium. For this reason, continuous elec-tronic fetal monitoring in labor is recommended forsuch pregnancies.
4. Hypertensive Disorders of Pregnancy
Hypertensive disorders of pregnancy are the secondmost common cause of maternal death in the UnitedStates (behind venous thromboembolic disease),accounting for 15%-20% of all maternal deaths.94, 95
Hypertension is also associated with high perinatalmortality and morbidity rates, primarily due to iatro-genic prematurity.96 Hypertensive disorders of preg-nancy can be classified into 4 categories:
1.) Chronic hypertension is defined as hypertensionprior to pregnancy and should also be considered inparturients with a sustained BP ≥140/90 prior to 20weeks gestation. Such pregnancies are at increasedrisk of superimposed preeclampsia, uteroplacentalinsufficiency and IUGR, placental abruption and still-birth. Angiotensin converting enzyme (ACE)inhibitors should be discontinued in pregnancy. Thesedrugs have not consistently been associated with anincreased risk of structural anomalies in the firsttrimester over baseline, but exposure in the latter halfof pregnancy has been associated with progressiveand irreversible renal injury in the fetus, includingrenal dysplasia and hypocalcified calvaria resultingfrom the blockade of the conversion of angiotensin 1to angiogensin 2 in the developing kidneys and lowfetal blood pressure on the fetal skull, respectively.97, 98
Because the perinatal mortality associated with mater-nal chronic hypertension is increased above baseline(6-25/1000 vs. 6.4/1000 in normotensive pregnan-cies),99 antepartum fetal testing (weekly non-stresstests, serial ultrasound examinations for fetal growth)should be initiated after 32 weeks gestation. Deliveryshould ideally be achieved by 40 weeks with a favor-able cervix.
2.) Chronic hypertensionwith superimposedpreeclampsia is defined as pre-existing chronic hyper-tension with worsening features during pregnancy,and may be difficult to differentiate from preeclamp-sia.
3.) Pregnancy-induced hypertension (PIH), alsoknown as transient hypertension or gestational non-proteinuric hypertension, refers to persistent elevationof BP ≥140/90 in the third trimester without evidenceof preeclampsia in a previously normotensive woman.It is a diagnosis of exclusion. PIH likely represents anexaggerated physiologic response of maternal cardio-vascular system to pregnancy. It is rarely associatedwith adverse maternal or fetal outcome, but may be

228 OBSTETRICS AND GYNECOLOGY—2009
difficult to distinguish from preeclampsia. PIH (but notpreeclampsia) is associated with an increased risk ofchronic hypertension in later life.
4.) Preeclampsia, also known as gestational protein-uric hypertension, complicates 6%-8% of all pregnan-cies.94, 100, 101 It is an idiopathic multisystem disorderspecific to human pregnancy and the puerperium.More precisely, it is a disease of the placenta since itoccurs also in pregnancies where there is trophoblastbut no fetal tissue (complete molar pregnancies).Preeclampsia is discussed in more detail below.
Etiology
The pathogenesis of preeclampsia remains poorlyunderstood. At present, 5 hypotheses are the subject ofintense investigation:100-103 (1.) genetic imprinting; (2.)immune maladaption; (3.) placental ischemia; (4.)generalized endothelial dysfunction; and (5.) defec-tive-free fatty acid, lipoprotein and/or lipid peroxidasemetabolism. However, there is as yet no single unify-ing theory that can account for all of the findings inpreeclampsia. Although the pathophysiology ofpreeclampsia is not well understood, it is clear that theblueprint for its development is laid down early inpregnancy. It has been suggested that the pathologichallmark is a complete or partial failure of the secondwave of trophoblast invasion from 16-20 weeks ofgestation that, in normal pregnancies, causes destruc-tion of the muscularis layer of the spiral arterioles.104-106
As pregnancy progresses, the metabolic demands ofthe fetoplacental unit increase. Because of the abnor-mally shallow invasion of the placenta in preeclampsiaand the lack of vascular remodeling, the spiral arteri-oles are unable to dilate to accommodate the requiredincrease in blood flow, resulting in “placental dysfunc-tion” that manifests clinically as preeclampsia. Recentdata suggest that excessive placental production of thefms-like tyrosine kinase receptor (also known as solu-ble Flt-1 [sFlt-1]), the soluble form of the vascularendothelial growth factor (VEGF) receptor type I thatbinds both circulating VEGF and placental growth fac-tor, may be responsible for the widespread endothelialinjury that characterizes preeclampsia.107, 108 In this way,sFlt-1 may be the elusive “toxemia factor” ofpreeclampsia. Although attractive, this hypothesisremains to be validated.
Diagnosis
Preeclampsia is a clinical diagnosis encompassing 3elements: (1.) new-onset hypertension (defined as asustained sitting BP ≥140/90 in a previously nor-motensive woman); (2.) new-onset proteinuria (>300mg/24 h or ≥1+ on a clean-catch urinalysis in theabsence of urinary infection); and (3.) nondependentedema.100, 101 However, more recent consensus reportshave suggested eliminating edema as a criterion forthe diagnosis.109 A definitive diagnosis of preeclamp-sia should only be made after 20 weeks gestation. Evi-dence of gestational proteinuric hypertension prior to20 weeks should raise the possibility of an underlyingmolar pregnancy, collagen vascular disease, antiphos-pholipid antibody syndrome, drug withdrawal, multi-ple pregnancy, or chromosomal abnormality (trisomy)in the fetus.
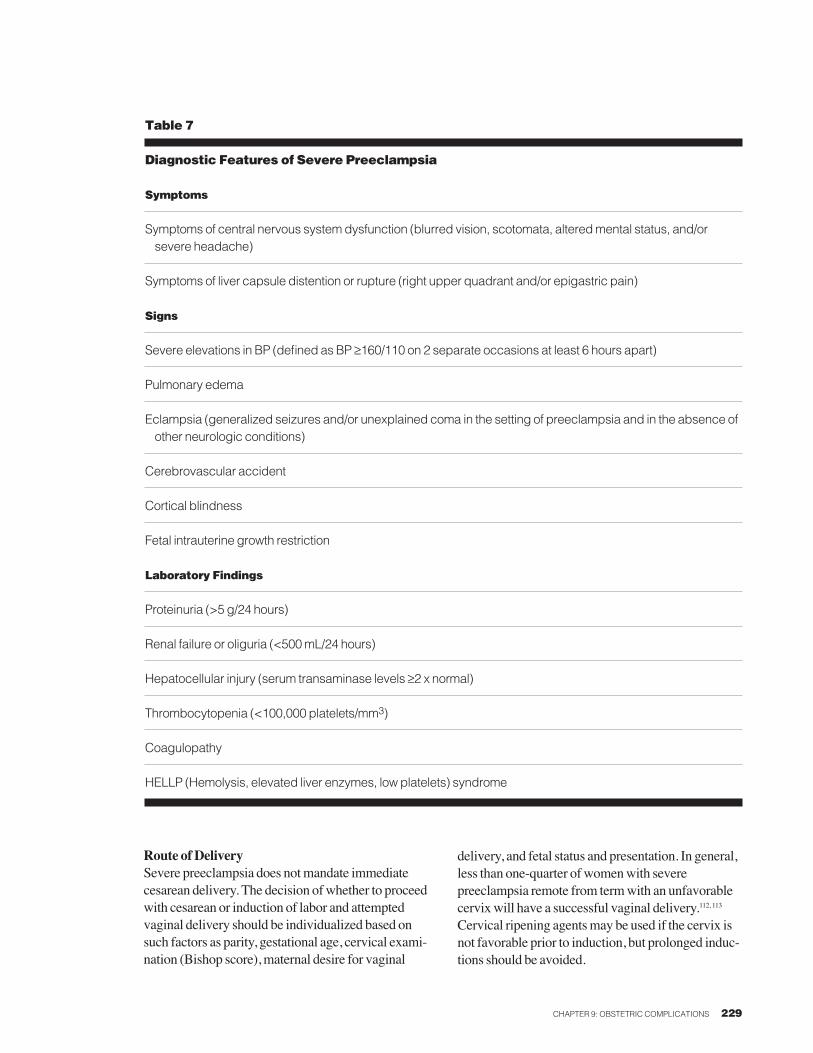
Preeclampsia is classified as either “mild” or “severe”(there is no category of “moderate” preeclampsia). Adiagnosis of severe preeclampsia should be enter-tained in women with new-onset proteinuric hyperten-sion along with 1 or more of a series of complications(Table 7). IUGR was excluded from the criteria in2000 by the National High Blood Pressure in Preg-nancy Working Group because of inconsistencies inits definition, but was still included as a criterion forthe diagnosis of severe preeclampsia by ACOG in2002.101 Mild preeclampsia includes all women withpreeclampsia, but without any features of severe dis-ease.
Management
Timing of DeliveryDelivery is the only effective treatment for preeclamp-sia. Delivery is recommended in women with mildpreeclampsia once a favorable gestational age has beenreached (>36-37 weeks) and in all women with severepreeclampsia regardless of gestational age (with theexception of severe preeclampsia due to proteinuriaalone or IUGR remote from term with good fetal test-ing). There has also been a recent trend towards expec-tant management of severe preeclampsia by BP criteriaalone <32 weeks gestation.110, 111 Every effort should bemade to delay delivery for 24-48 hours to administerantenatal corticosteroids, if indicated.
CHAPTER 9: OBSTETRIC COMPLICATIONS 229
Table 7
Diagnostic Features of Severe Preeclampsia
Symptoms
Symptoms of central nervous system dysfunction (blurred vision, scotomata, altered mental status, and/orsevere headache)
Symptoms of liver capsule distention or rupture (right upper quadrant and/or epigastric pain)
Signs
Severe elevations in BP (defined as BP ≥160/110 on 2 separate occasions at least 6 hours apart)
Pulmonary edema
Eclampsia (generalized seizures and/or unexplained coma in the setting of preeclampsia and in the absence ofother neurologic conditions)
Cerebrovascular accident
Cortical blindness
Fetal intrauterine growth restriction
Laboratory Findings
Proteinuria (>5 g/24 hours)
Renal failure or oliguria (<500 mL/24 hours)
Hepatocellular injury (serum transaminase levels ≥2 x normal)
Thrombocytopenia (<100,000 platelets/mm3)
Coagulopathy
HELLP (Hemolysis, elevated liver enzymes, low platelets) syndrome
Route of DeliverySevere preeclampsia does not mandate immediatecesarean delivery. The decision of whether to proceedwith cesarean or induction of labor and attemptedvaginal delivery should be individualized based onsuch factors as parity, gestational age, cervical exami-nation (Bishop score), maternal desire for vaginal
delivery, and fetal status and presentation. In general,less than one-quarter of women with severepreeclampsia remote from term with an unfavorablecervix will have a successful vaginal delivery.112, 113
Cervical ripening agents may be used if the cervix isnot favorable prior to induction, but prolonged induc-tions should be avoided.
230 OBSTETRICS AND GYNECOLOGY—2009
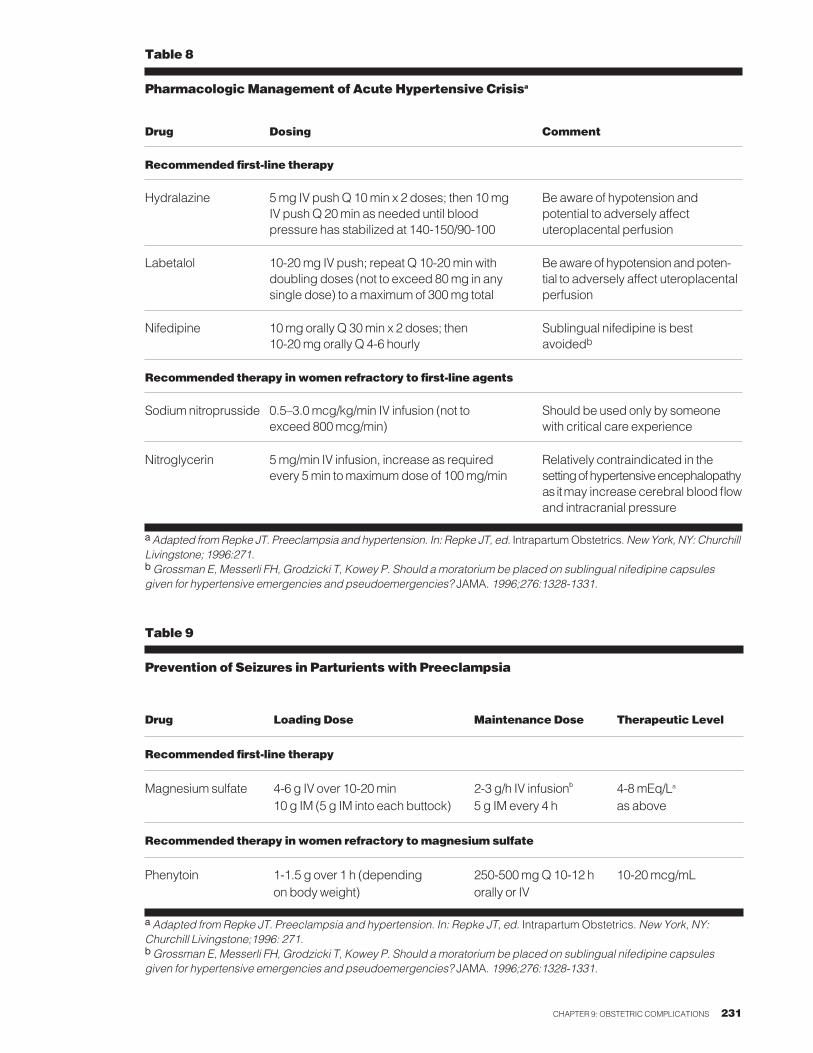
Treatment of Hypertension The use of antihypertensive agents to control mildlyelevated BP in the setting of preeclampsia has notbeen shown to alter the course of the disease, nor todiminish perinatal morbidity or mortality, and mayeven reduce birth weight. However, antihypertensiveagents should be administered to prevent a maternalcerebrovascular accident (stroke) with severe hyper-tension while effecting delivery. Most clinicianswould recommend initiation of antihypertensive ther-apy for a systolic BP ≥160 mm Hg and/or diastolic BP≥110 mm Hg, although these cut-offs have not beentested prospectively.114, 115 Treatment options are sum-marized in Table 8. Sodium restriction and diureticshave no role in therapy. Restricted physical activity(bed rest) can lower BP, although its efficacy forimproving perinatal outcome has not been proven.
Intrapartum Anesthesia Neuraxial techniques (epidural, spinal) can be safelyadministered in the setting of preeclampsia (in theabsence of thrombocytopenia) with close attention tovolume expansion and anesthetic technique.Hypotension is a major concern, because preeclamp-sia causes total body fluid overload but depletedintravascular volume. Airway edema and exacerba-tion of hypertension with intubation can complicateinduction of general anesthesia.
Seizure ProphylaxisSeizure prophylaxis is generally initiated during laboror while administering corticosteroids orprostaglandins prior to planned delivery and contin-ued until 24-48 hours postpartum, when the risk ofseizures is decreased.116 Magnesium sulfate is the drugof choice to prevent seizures (eclampsia) in the settingof mild or severe preeclampsia (Table 9).117, 118 Theincidence of seizures is much lower in women withnonproteinuric mild hypertension (0.1% as comparedwith 1%-2% for severe preeclampsia119), and it is safeto withhold seizure prophylaxis in this setting. Mag-nesium sulfate must be given intravenously or byintramuscular injection, as it is not absorbed orally.Because magnesium is renally excreted, infusion ratesshould be decreased for maternal serum creatininelevels of 1.0 mg/dL or higher.120
Postpartum CarePreeclampsia and its complications resolve followingdelivery, often within a few days. Permanent neuro-
logic sequelae or renal failure are rare. Diuresis (>4liters/day) often heralds clinical resolution. BP thatremains elevated more than 12 weeks postpartum areunlikely to be related to preeclampsia. Patients withsevere hypertension (160/100 mmHg) can be treatedwith oral antihypertensive medications until their 6-week postpartum check, and then weaned off. If theycontinue to require antihypertensive medication, theyshould be referred to an internist for further investigation.121, 122
Recurrence Risk and PreventionThe risk of recurrence of preeclampsia in a subse-quent pregnancy is related to the severity and natureof the presentation and to the gestational age at pre-sentation.123 Preeclampsia is a disorder of placentalimplantation and therefore not entirely preventable.Despite promising early studies, low-dose aspirin(acetylsalicylic acid [ASA]) and/or supplemental cal-cium does not appear to prevent preeclampsia recur-rence in either high- or low-risk parturients.124, 125 Arecent meta-analysis suggests that low-dose aspirin(80 mg per day) may be useful in preventingpreeclampsia, but only in women with prior early,severe preeclampsia.126 Moreover, low-dose aspirin inlow-risk women may increase their risk of placentalabruption. Women at high-risk for preeclampsiashould be seen early in pregnancy to establish accu-rate pregnancy dating, and to perform baseline BP andlaboratory tests. Measurement of BP and urine proteinat regular intervals in the late second and thirdtrimesters is critical for timely diagnosis ofpreeclampsia.
CHAPTER 9: OBSTETRIC COMPLICATIONS 231
Table 8
Pharmacologic Management of Acute Hypertensive Crisisa
Drug Dosing Comment
Recommended first-line therapy
Hydralazine 5 mg IV push Q 10 min x 2 doses; then 10 mg Be aware of hypotension and IV push Q 20 min as needed until blood potential to adversely affect pressure has stabilized at 140-150/90-100 uteroplacental perfusion
Labetalol 10-20 mg IV push; repeat Q 10-20 min with Be aware of hypotension and poten-doubling doses (not to exceed 80 mg in any tial to adversely affect uteroplacentalsingle dose) to a maximum of 300 mg total perfusion
Nifedipine 10 mg orally Q 30 min x 2 doses; then Sublingual nifedipine is best 10-20 mg orally Q 4-6 hourly avoidedb
Recommended therapy in women refractory to first-line agents
Sodium nitroprusside 0.5–3.0 mcg/kg/min IV infusion (not to Should be used only by someone exceed 800 mcg/min) with critical care experience
Nitroglycerin 5 mg/min IV infusion, increase as required Relatively contraindicated in the every 5 min to maximum dose of 100 mg/min setting of hypertensive encephalopathy
as it may increase cerebral blood flowand intracranial pressure
a Adapted from Repke JT. Preeclampsia and hypertension. In: Repke JT, ed. Intrapartum Obstetrics. New York, NY: ChurchillLivingstone; 1996:271.bGrossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsulesgiven for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276:1328-1331.
Table 9
Prevention of Seizures in Parturients with Preeclampsia
Drug Loading Dose Maintenance Dose Therapeutic Level
Recommended first-line therapy
Magnesium sulfate 4-6 g IV over 10-20 min 2-3 g/h IV infusionb 4-8 mEq/La
10 g IM (5 g IM into each buttock) 5 g IM every 4 h as above
Recommended therapy in women refractory to magnesium sulfate
Phenytoin 1-1.5 g over 1 h (depending 250-500 mg Q10-12 h 10-20 mcg/mLon body weight) orally or IV
aAdapted from Repke JT. Preeclampsia and hypertension. In: Repke JT, ed. Intrapartum Obstetrics.New York, NY:Churchill Livingstone;1996: 271.bGrossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsulesgiven for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276:1328-1331.

5. Intrauterine Fetal Demise
Intrauterine fetal demise (IUFD)—also known asstillbirth—is defined in the United States as fetaldemise after 20 weeks gestation and prior to deliv-ery.127 In the United States, the stillbirth rate decreasedfrom 15.8 per 1000 total births in 1960 to 7.5 per 1000births in 1990.99, 128 Risk factors for IUFD includeextremes of maternal age, multiple pregnancy, post-term pregnancy, male fetus, fetal macrosomia andmaternal disease, such as pregestational diabetes, sys-temic lupus erythematosus (SLE) and preeclamp-sia.129, 130
Etiology
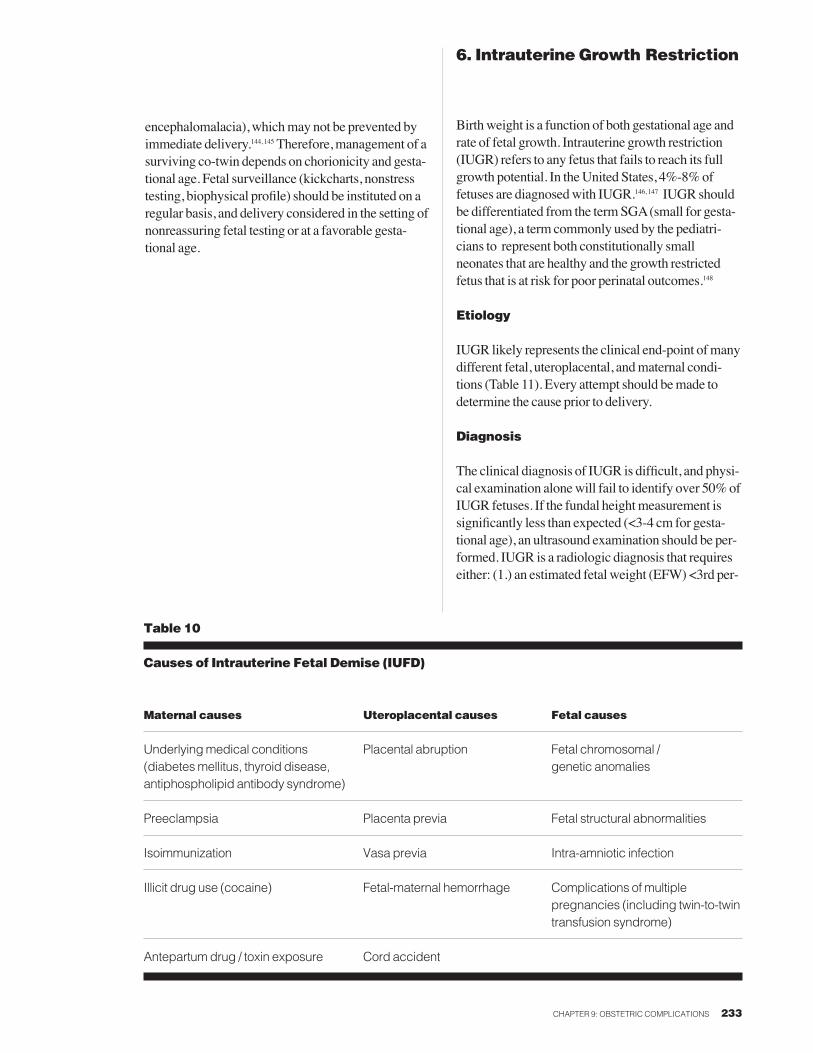
Causes of IUFD can be identified in only around 50%of cases (Table 10). Pathologic examination of thefetus and placenta/fetal membranes is the single mostuseful test to identify a cause for the IUFD. Earlydetection and appropriate management of underlyingmaternal disorders (diabetes, preeclampsia) mayreduce the risk of IUFD.131, 132 Fetal karyotyping shouldbe considered in all cases of fetal death to identifychromosomal abnormalities, particularly in cases withdocumented fetal structural abnormalities. Approxi-mately 6%-10% of stillborn fetuses have abnormalkaryotypes.133 Amniocentesis may be recommendedto salvage viable amniocytes for cytogenetic analysisprior to delivery. Fetal-maternal hemorrhage (fetalcells spilling into maternal circulation) occurs in allpregnancies, but is usually minimal (<0.1 mL totalvolume). In rare instances, fetal-maternal hemorrhagemay be massive, leading to fetal demise. The Klei-hauer-Betke (acid elution) test allows an estimate ofthe volume of fetal blood in the maternal circulation,and should be drawn within 6 - 8 hours of the pur-ported time of bleeding episode due to rapid clearanceof fetal cells from maternal circulation.134 Intra-amni-otic infection resulting in fetal death is usually evidenton clinical exam. Placental membrane culture andautopsy examination of the fetus, placenta/fetal mem-branes and umbilical cord may be useful. Fetal x-raysor MRI may sometimes be valuable if autopsy isdeclined.135, 136
Diagnosis
The inability to identify fetal heart tones or theabsence of uterine growth may suggest the diagno-sis. Ultrasound is the gold standard to confirm an
232 OBSTETRICS AND GYNECOLOGY—2009
IUFD by documenting the absence of fetal cardiacactivity. Other sonographic findings in later preg-nancy may include scalp edema, overlappingsutures and fetal maceration.
Management
Every effort should be made to avoid cesarean deliv-ery in the setting of IUFD. As such, expectant man-agement is often recommended. Latency (the periodfrom fetal demise to delivery) varies depending on theunderlying cause and gestational age. In general, theearlier the gestational age, the longer the latencyperiod. Overall, >90% of women will go into sponta-neous labor within 2 weeks of fetal death. However,many women find the prospect of carrying a deadfetus distressing and want the pregnancy terminated assoon as possible. Management options include surgi-cal dilatation and evacuation or induction of laborwith cervical ripening, if indicated. Around 20%-25%of women who retain a dead singleton fetus for longerthan 3 weeks will develop disseminated intravascularcoagulopathy (DIC) due to excessive consumption ofclotting factors.137, 138 Therefore, delivery should beeffected within this time period.
Death of a Co-twinThe death of 1 twin confers an increased risk of majormorbidity to the surviving twin, including IUFD, neu-rologic injury, multiorgan system failure, thrombosis,distal limb necrosis, placental abruption and prema-ture labor.99-101 The prognosis for the surviving twin isdependent on the cause of death, gestational age,chorionicity and time interval between death of thefirst twin and delivery of the second. Dizygous twinpregnancies do not share circulation, and the death of1 twin may have little impact on the surviving twin.The dead twin may be resorbed completely or becomecompressed and incorporated into the membranes(fetus papyraceus). DIC in the surviving fetus and/ormother is rare.102 On the other hand, some degree ofshared circulation can be demonstrated in almost allmonozygous twin pregnancies, and death of 1 fetus inthis setting carries an increased risk of death of its co-twin due to profound hypotension and/or purportedtransfer of thromboplastic proteins from the dead fetusto the live fetus.143 If it survives, the co-twin, has a 40%risk of developing neurologic injury (multicystic
CHAPTER 9: OBSTETRIC COMPLICATIONS 233
encephalomalacia), which may not be prevented byimmediate delivery.144, 145 Therefore, management of asurviving co-twin depends on chorionicity and gesta-tional age. Fetal surveillance (kickcharts, nonstresstesting, biophysical profile) should be instituted on aregular basis, and delivery considered in the setting ofnonreassuring fetal testing or at a favorable gesta-tional age.
6. Intrauterine Growth Restriction
Birth weight is a function of both gestational age andrate of fetal growth. Intrauterine growth restriction(IUGR) refers to any fetus that fails to reach its fullgrowth potential. In the United States, 4%-8% offetuses are diagnosed with IUGR.146, 147 IUGR shouldbe differentiated from the term SGA (small for gesta-tional age), a term commonly used by the pediatri-cians to represent both constitutionally smallneonates that are healthy and the growth restrictedfetus that is at risk for poor perinatal outcomes.148
Etiology
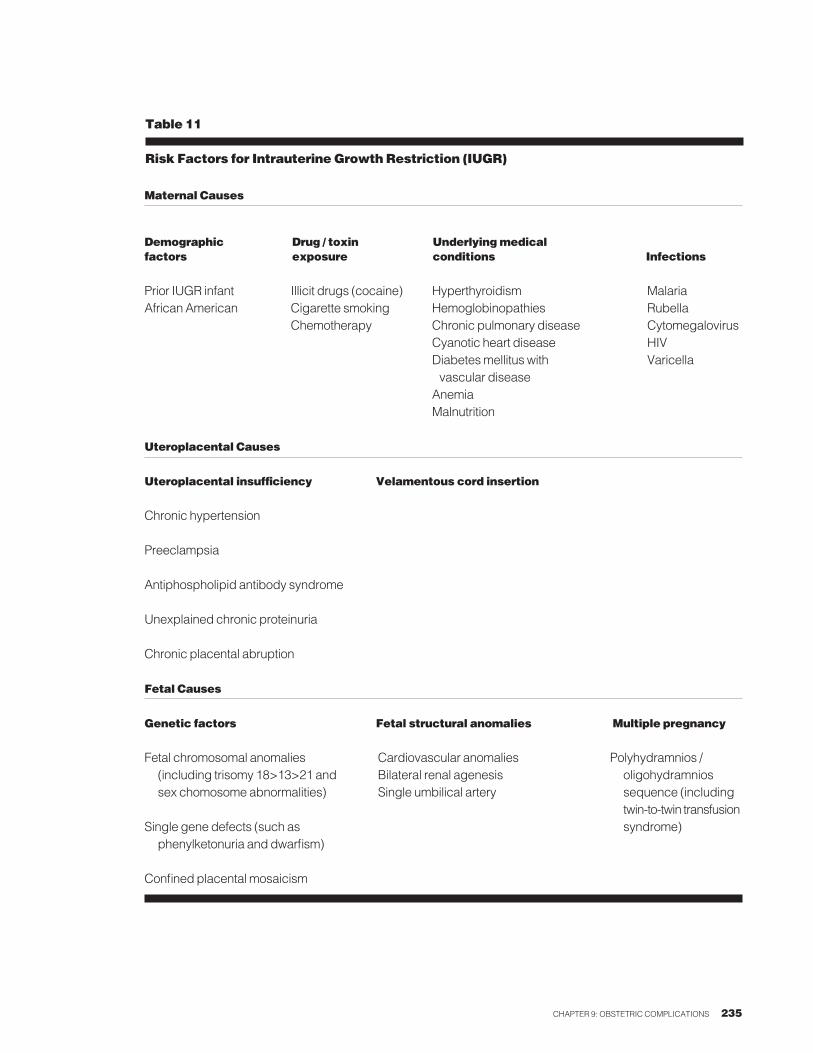
IUGR likely represents the clinical end-point of manydifferent fetal, uteroplacental, and maternal condi-tions (Table 11). Every attempt should be made todetermine the cause prior to delivery.
Diagnosis
The clinical diagnosis of IUGR is difficult, and physi-cal examination alone will fail to identify over 50% ofIUGR fetuses. If the fundal height measurement issignificantly less than expected (<3-4 cm for gesta-tional age), an ultrasound examination should be per-formed. IUGR is a radiologic diagnosis that requireseither: (1.) an estimated fetal weight (EFW) <3rd per-
Table 10
Causes of Intrauterine Fetal Demise (IUFD)
Maternal causes Uteroplacental causes Fetal causes
Underlying medical conditions Placental abruption Fetal chromosomal / (diabetes mellitus, thyroid disease, genetic anomaliesantiphospholipid antibody syndrome)
Preeclampsia Placenta previa Fetal structural abnormalities
Isoimmunization Vasa previa Intra-amniotic infection
Illicit drug use (cocaine) Fetal-maternal hemorrhage Complications of multiple pregnancies (including twin-to-twintransfusion syndrome)
Antepartum drug / toxin exposure Cord accident

centile (2 standard deviations from the mean) for ges-tational age, or (2.) an EFW <10th percentile for gesta-tional age along with evidence of fetal compromise(usually oligohydramnios or abnormal umbilicalartery Doppler velocimetry).146,147,149 Fetuses who are<10th percentile without evidence of compromiseshould be referred to as SGA and not IUGR. Accurategestational age dating is clearly a prerequisite for thediagnosis. A small calcified (Grade 3) placentadetected on ultrasound examination in associationwith a small biparietal circumference may also be sug-gestive of an IUGR pregnancy.150
Complications
IUGR infants have higher rates of perinatal morbidityand mortality as compared with appropriate for gesta-tional age (AGA) fetuses for any given gestationalage. Neonatal morbidity (meconium aspiration syn-drome, hypoglycemia, polycythemia, pulmonaryhemorrhage) may be present in up to 50% of IUGRneonates.146,147,149,151 Premature IUGR infants also havedifficulty with nutritional support, and many developfeeding intolerance and failure to thrive in theNICU.152 Long-term studies show a 2-fold increasedincidence of cerebral dysfunction (ranging fromminor learning disability to cerebral palsy) in IUGRinfants delivered at term, and an even higher incidenceif the infant was born preterm. Epidemiological stud-ies also suggest that these infants may also be at higherrisk for developing chronic disease in adulthood suchas diabetes, hypertension, stroke and coronary heartdisease (the Barker Hypothesis).153
Management
Bed rest and low-dose aspirin have not been shown toprevent IUGR in women at high risk; however, arecent meta-analysis suggests that women with priorhistory of an IUGR pregnancy with early severepreeclampsia may benefit from empiric low-doseaspirin therapy during subsequent pregnancies.126
Principles of management of IUGR pregnanciesinclude identification of women at high risk, earlyantepartum diagnosis, attempts to identify etiology(karyotype, infection, antiphospholipid antibody syn-drome), regular (usually twice-weekly) fetal surveil-lance and appropriate timing of delivery. IUGR maybe the first manifestation of preeclampsia, and such
pregnancies should be followed on a regular basis toexclude this complication.
IUGR fetuses can undergo vaginal delivery andcesarean delivery should be reserved for the usualobstetric indications. However, up to 50%-80% ofIUGR fetuses will show evidence of nonreassuringfetal testing in labor requiring cesarean delivery.146
Timing of delivery also depends on the precise gesta-tional age, any superimposed maternal conditions (eg,severe preeclampsia), the presence or absence ofabnormal umbilical cord Dopplers (reversed end-diastolic flow), whether or not there has been anyinterval fetal growth over a 2- to 3-week period, andwhether or not the IUGR fetus is a singleton vs. a mul-tiple gestation in which the other fetus(es) are growingappropriately.154 If a premature delivery <34 weeks isanticipated, a course of antenatal corticosteroids maybe warranted. Note that antepartum fetal testing(including the BPP and umbilical artery Dopplervelocimetry) may temporarily worsen in the 24-48hours following steroid administration in somefetuses.155
234 OBSTETRICS AND GYNECOLOGY—2009
CHAPTER 9: OBSTETRIC COMPLICATIONS 235
Maternal Causes
Demographic Drug / toxin Underlying medicalfactors exposure conditions Infections
Prior IUGR infant Illicit drugs (cocaine) Hyperthyroidism MalariaAfrican American Cigarette smoking Hemoglobinopathies Rubella
Chemotherapy Chronic pulmonary disease CytomegalovirusCyanotic heart disease HIVDiabetes mellitus with Varicella vascular disease
AnemiaMalnutrition
Uteroplacental Causes
Uteroplacental insufficiency Velamentous cord insertion
Chronic hypertension
Preeclampsia
Antiphospholipid antibody syndrome
Unexplained chronic proteinuria
Chronic placental abruption
Fetal Causes
Genetic factors Fetal structural anomalies Multiple pregnancy
Fetal chromosomal anomalies Cardiovascular anomalies Polyhydramnios /(including trisomy 18>13>21 and Bilateral renal agenesis oligohydramnios sex chomosome abnormalities) Single umbilical artery sequence (including
twin-to-twin transfusionSingle gene defects (such as syndrome)
phenylketonuria and dwarfism)
Confined placental mosaicism
Table 11
Risk Factors for Intrauterine Growth Restriction (IUGR)

7. Multiple Pregnancy
Multiple pregnancies complicate 1%-2% of all deliv-eries and are becoming increasingly common, primar-ily as a result of assisted reproductive technology(ART). This is especially true of higher-order multiplepregnancies (triplets and up) which now constitute0.103% of all births.156 The vast majority (97%-98%)of multiple gestations are twin pregnancies.
Diagnosis
Multiple pregnancy should be suspected in women athigh risk, women with excessive symptoms of preg-nancy (such as nausea and vomiting), or uterine sizelarger than expected. The overall incidence of dizy-gous twinning in the U.S. is around 1 in 89 pregnan-cies, and is influenced by a number of epidemiologicfactors, including a family or personal history of mul-tiple pregnancy, advanced maternal age, multiparity,African American, and ART.157 Monozygous twin-ning, on the other hand, is a random event that occursin around 1 in 300 pregnancies (although the risk maybe increased 2- to 3-fold with in vitro fertilization).158
Ultrasound will confirm the diagnosis.
Zygosity and Chorionicity80% of twin pregnancies are dizygous (derived from 2separate embryos). Perinatal mortality is higher withmonozygous (30%-50%) than with dizygous twins(10%-20%). Chorionicity refers to the arrangement ofmembranes in multiple pregnancies. In monozygoustwinning, the timing of the cell division determinesthe chorionicity. If the zygote divides within 3 days offertilization, the result is dichorionic/diamniotic pla-centation (30% of all monozygous pregnancies); if thedivision occurs between day 3 and day 8, the result is amonochorionic/diamniotic pregnancy (65%);between day 8 and day 13, a monochori-onic/monoamniotic pregnancy ensues (<5%); and ifthe division occurs on or after day 13, incomplete sep-aration (conjoined twins) is the rule (<0.5%). Chori-onicity correlates directly with perinatal mortality,which is especially high with monochori-onic/monoamniotic twins (65%-70%). Chorionicityis determined most accurately by examination of themembranes after delivery. Antenatal diagnosis ismore difficult.159-161 Typically, ultrasound examinationin the first half of the pregnancy can be performed toevaluate the point at which the amniotic/chorionicmembranes arise from the placenta to determine if thefetuses are dichorionic (twin peak or lamda sign) or
monochorionic (no peak, but a thin filmy mem-brane).162 Identification of separate sex fetuses or 2separate placentae confirms dichorionic/diamnioticplacentation.
Complications
Overall, antepartum complications develop in 80% ofmultiple pregnancies, compared with around 30% ofsingleton gestations (Table 12).163 Preterm delivery isthe most common complication, and the risk ofpreterm delivery increases as fetal number increases:the average length of gestation is 40 weeks in single-tons, 37 weeks in twins, 33 weeks in triplets, and 29weeks in quadruplets.164 Fetal growth discordance(defined as a ≥25% difference in EFW betweenfetuses of the same pregnancy) occurs in 5%-15% oftwins and 30% of triplets, and is associated with a 6-fold increase in perinatal mortality.165,166 Cord entan-glement is rare (1 in 25,000 births), but may occur inup to 70% of monochorionic/monoamniotic pregnan-cies, and accounts for >50% of perinatal mortality inthis subgroup.163,167,168 Maternal complications includean increased risk of gestational diabetes, preeclamp-sia, anemia, cholestasis of pregnancy,169 cesareandelivery (due primarily to malpresentation), and post-partum hemorrhage.
Twin polyhydramnios/oligohydramnios(“poly/oligo”) sequence results from an imbalance inblood flow from the “donor” twin to the “recipient.”Both twins are at risk for adverse events. Twin-to-twintransfusion syndrome is a subset of polyhydram-nios/oligohydramnios sequence seen in 15% ofmonochorionic pregnancies,170, 171 and is due to unbal-anced vascular communications between the fetal cir-culations. One twin is usually appropriate for gesta-tional age (AGA) while the other twin is usuallyIUGR. The IUGR twin is typically in the oligohy-dramniotic sac and is compressed against one edge ofthe uterus, also known as the “stuck twin” syn-drome.172 Following delivery, a difference in birthweight of ≥20% or a difference in hematocrit of ≥5g/dL confirms the diagnosis. The larger twin is oftenpolycythemic while the IUGR twin is anemic. Prog-nosis depends on gestational age, severity, and under-lying etiology. Overall perinatal mortality is 40%-80%.173, 174 Treatment options include expectant man-agement, serial amniocentesis of the polyhydramni-otic sac, indomethacin (to decrease fetal urine output),
236 OBSTETRICS AND GYNECOLOGY—2009

laser obliteration of the placental vascular communi-cations or selective fetal reduction.175-178
Management
Gravidas with multiple gestations should be coun-seled about the increased risk of preeclampsia,preterm labor, postpartum hemorrhage, anemia, fetalloss, fetal anomalies, IUGR, and cesarean delivery.Principles of management include early diagnosis,screening for fetal anomalies, determination of chori-onicity, and regular antepartum follow-up (serialultrasound for growth at least every 3-4 weeks toscreen for discordant growth).179 Maternal serumalpha-fetoprotein (MS-AFP) screening for multiplegestation is a reliable screen for neural tube defects;however, serum biochemical marker screening foraneuploidy in the presence of more than one fetus isnot particularly reliable, due to the inherent structureof the test parameters.180 Maternal plasma volume isincreased by 100%-200% with multiple gestation,placing the gravida at higher risk for anemia. Addi-tional folate and iron supplementation should be con-sidered in multiple gestation. Multifetal pregnanciesare at higher risk for cesarean delivery. Patients shouldbe counseled about labor analgesia and anesthesia, thepossible need for emergent delivery, and the need formultiple pediatric teams in the delivery room. There
are several management considerations specific tomultiple gestation, outlined below.
Multifetal Pregnancy Reduction
Overall, 10%-15% of higher-order multiple pregnan-cies (triplets and up) will reduce spontaneously dur-ing the first trimester.164 If not, the option of multifetalpregnancy reduction to twins at 13-15 weeks shouldbe discussed. The benefits of reduction includeincreased length of gestation, increased birth weight,and reduced prematurity and perinatal mortality andmortality.164, 181-183 The procedure-related loss rate priorto 20 weeks may be as high as 15% (range: 5%-35%),which is comparable to the background risk forhigher-order multiple pregnancies.164, 182-185 However,the fetal loss rate increases with advancing gestationat the time of the reduction. Multifetal pregnancyreduction should be distinguished from selective fetalreduction, in which one fetus is selectively terminatedbecause of a known structural or chromosomal abnormality.186, 187
Screening for Congenital Anomalies
Using twin populations, maternal serum alpha-fetoprotein (MS-AFP) and “quadruple panel” screening(MS-AFP, estriol, hCG and activin A) has been stan-
CHAPTER 9: OBSTETRIC COMPLICATIONS 237
Table 12
Complications of Multiple Pregnancy
Maternal complications Uteroplacental complications Fetal complications
Anemia Placenta previa Fetal growth discordance
Hyperemesis gravidarum Preterm PROM IUGR
Gestational diabetes Cord entanglement IUFD of one or both twins
Preterm labor Postpartum hemorrhage Congenital anomalies
Cesarean delivery Twin-to-twin transfusion syndrome

dardized for twins as it is for singletons at 15-20weeks.188, 189 In dizygous pregnancies, the risk of aneu-ploidy (genetic abnormality) is independent for eachfetus. As such, the chance that 1 or both fetuses have akaryotypic abnormality is greater than for a singleton.Amniocentesis is recommended when the probabilityof aneuploidy is equal to or greater than the proce-dure-related pregnancy loss rate (estimated at 1 in270).190, 191 In singleton pregnancies, this balance isreached at a maternal age at delivery of 35 years. Intwin pregnancies, amniocentesis should be offered towomen at approximately 32 years of age.192, 193
Route of Delivery
The recommended route of delivery of twins dependson presentation, gestational age (or EFW), concor-dance, and maternal and fetal well-being. Priorcesarean is not an absolute contraindication to vaginaldelivery of twins.194 Breech extraction of a nonvertex,concordant second twin is a safe procedure,195, 196 butshould only be performed by an experienced obstetriccare provider. Preparation for a possible breechextraction should include an ultrasound machine toassist in evaluation of fetal heart rate and presentation,specialized forceps to assist in delivery of the after-coming head (Piper forceps), an experienced anesthe-siologist and a uterine relaxant, such as intravenousnitroglycerin or halothane by mask. Cesarean deliveryhas traditionally been recommended for multiplepregnancies in which the presenting fetus is not vertexand for all higher-order multiple pregnancies,although vaginal delivery may be appropriate inselected patients.197
8. Premature Rupture of Membranes
PROM refers to rupture of the fetal membranes priorto the onset of uterine contractions.198 It can be clas-sified as term PROM (≥37 weeks) or preterm PROM(<37 weeks). Latency (the time interval betweenPROM and delivery) is dependent on several factors:(1.) gestational age (at term, 50% of women withPROM will go into spontaneous labor within 12 hoursand 95% within 72 hours; latency is generally longerif PROM occurs preterm with 50% of women goinginto labor within 24-48 hours and 70%-90% within 7days)199; (2.) severity of oligohydramnios (severeoligohydramnios is associated with shortened latencyperiod );200 and (3.) number of fetuses (twins have ashorter latency period than singletons).201
Diagnosis
PROM is a clinical diagnosis with evidence of vaginalpooling of amniotic fluid on sterile speculum exami-nation, which is alkaline (vaginal fluid turns yellownitrazine paper blue) and demonstrates “ferning”(microscopic crystallization) on drying. Evidence ofdiminished amniotic fluid volume on ultrasound mayhelp to confirm the diagnosis, but is not a prerequisitefor the diagnosis. Sometimes a gush of fluid can beobserved to emanate from the cervix when a patientcoughs during a speculum exam. The fluid should alsobe categorized as clear, blood-tinged, or meconium-stained. Differential diagnosis includes leakage ofurine and vaginal discharge. If equivocal, an amnio-centesis can be performed with instillation of indigocarmine dye into the amniotic cavity (“amnio-dyetest”). Leakage of the dye into the vagina as evidencedby staining of a tampon within 15-20 minutes willconfirm the diagnosis. The patient should be advisedthat, after an hour or so, her urine may also stain blue.
Term PROM
Rupture of the membranes is a normal physiologicevent at term. Rupture of membranes at term prior tothe onset of uterine contractions (term PROM) occursin 8%-10% of term pregnancies.202 Contraindicationsto expectant management in the setting of termPROM include intra-amniotic infection, non-reassur-ing fetal testing, vaginal bleeding and active labor. Inthe absence of such contraindications, both expectantmanagement and immediate augmentation of laborare acceptable options.203 Severe oligohydramniosmay be associated with umbilical cord compression in
238 OBSTETRICS AND GYNECOLOGY—2009
labor leading to non-reassuring fetal testing andcesarean delivery. In this setting, amnioinfusion withsaline has been shown to decrease the risk of cesareanfor non-reassuring fetal testing (but has not necessar-ily been shown to improve perinatal outcome).
Preterm PROM
Preterm PROM complicates 2%-4% of singleton and7%-10% of twin pregnancies. It is associated with30%-40% of preterm births and 10% of all perinatalmortality.204 Risk factors include prior preterm PROM,unexplained vaginal bleeding, placental abruption(seen in 10%-15% of women with preterm PROM,but may be a result rather than a cause),205 cervicalinsufficiency, vaginal or intra-amniotic infection,amniocentesis, smoking, multiple pregnancy, polyhy-dramnios, chronic steroid treatment, connective tissuediseases (systemic lupus erythematosus, Ehlers-Dan-los syndrome), anemia, low socioeconomic status andunmarried marital status. Factors which are not associ-ated with preterm PROM include coitus, cervicalexaminations, maternal exercise and parity. The recur-rence risk is 20%-30%.204
ComplicationsNeonatal complications are related primarily to pre-maturity, including RDS, IVH, sepsis, pulmonaryhypoplasia (especially with preterm PROM <22weeks) and skeletal deformities/limb strictures(related to severity and duration of preterm PROM).Overall, preterm PROM is associated with a 4-foldincrease in perinatal mortality and a 3-fold increase inneonatal morbidity.204, 206 The fetus is at risk for devel-oping chorioamnionitis, stillbirth from cord accidentor placental abruption, non-reassuring fetal heart ratetracings or precipitous delivery. Maternal complica-tions include increased rates of cesarean delivery,intra-amniotic infection and postpartum endometritis.
ManagementManagement of preterm PROM should be individual-ized. The risk of prematurity should be weighedagainst the risk of expectant management, primarilyintra-amniotic infection.204, 206 Amniotic fluid can beused to assess fetal lung maturity by testing for thelethicin/sphingomyelin (L/S) ratio and presence ofphosphatidyl glycerol (PG). In the setting of expectantmanagement for preterm PROM, new onset uterinecontractions may portend the development of intra-
amniotic infection. Patients should be placed onpelvic rest (no tampons, no douching, no sexual inter-course). A screening sonogram should be performedto determine fetal presentation as non-vertex presen-tation places the fetus at risk for umbilical cord pro-lapse. Hospitalization, bed rest and fetal surveillancehave been the mainstay of management of pretermPROM.204 Areas of controversy in the management ofpreterm PROM include:
1.) Tocolysis. Preterm PROM is a relative contraindi-cation to tocolysis to prevent undue exposure offetuses to infected in utero environment, with subse-quent postnatal risk of neurologic injury and cerebralpalsy.207 Tocolytic agents may delay delivery by 24-48hours in the setting of intact membranes, but do notappear to delay delivery or improve perinatal out-come in pregnancies complicated by pretermPROM.204
2.) Antibiotics. Prophylactic broad-spectrum antibi-otic therapy has consistently been shown to prolonglatency in the setting of preterm PROM,208, 209 and thisappears to translate into an improvement in perinataloutcome. There is currently no evidence to recom-mend 1 antibiotic regimen over another. The mostcommonly used antibiotic regimen is ampicillin anderythromycin for 7 days.
3.) Antenatal corticosteroids. A single course ofantenatal glucocorticoids is recommended for allpregnancies at high risk of delivering before 34 weeksgestation with intact membranes and before 32 weekswith preterm PROM with a view to decreasing theincidence of RDS, IVH and NEC.68-70 The benefit ofantenatal corticosteroids in pregnancies complicatedby preterm PROM at 32-34 weeks gestation is notclear.70
4.) Fetal surveillance. Fetuses in pregnancies com-plicated by preterm PROM are at risk for ascendinginfection, cord accident, placental abruption and (pos-sibly) uteroplacental insufficiency. Amniocentesismay be considered in the setting preterm PROM totest for evidence of intra-amniotic infection and toconfirm fetal lung maturity with a view to affecting anearlier delivery. In some cases, vaginal pooled amni-otic fluid can be aspirated and tested for fetal lungmaturation. Loss of fetal breathing in the BPP was
CHAPTER 9: OBSTETRIC COMPLICATIONS 239
previously hailed as an early sign of intrauterine infec-tion, but more recent studies have refuted this idea.210
In the absence of evidence of uteroplacental insuffi-ciency, fetal surveillance has not been demonstrated toreliably diagnose or predict intra-amniotic infection.Fetal surveillance should therefore be instituted onlyfor the usual obstetric indications, such as fetal non-stress testing (NST) to assess for variable decelera-tions in the setting of oligohydramnios.
9. Antepartum Hemorrhage
Antepartum hemorrhage is defined as vaginal bleed-ing after 24 weeks gestation and before labor, andcomplicates 4%-5% of all pregnancies. Placenta pre-via (20%) and placental abruption (30%) are the mostcommon causes of antepartum hemorrhage. Othercauses include vasa previa, early labor andlesions/lacerations of the lower genital tract.
Placenta Previa
Placenta previa refers to implantation of the placentaover the cervical os in advance of the fetal presentingpart, and complicates 1 in 200 pregnancies.211 Riskfactors include multiparity, advanced maternal age,prior placenta previa, prior cesarean delivery andsmoking. Placenta previa may be asymptomatic ormay present clinically with painless, bright-red vagi-nal bleeding. Fetal malpresentation due to the inabilityof the presenting part to engage the pelvis may furthersuggest the diagnosis. Placenta previa is primarily asonographic diagnosis. Transvaginal sonogram can besafely performed in the setting of abnormal placenta-tion to quantify the distance from the leading edge ofthe placenta to the internal os of the cervix. If the lead-ing edge of the placenta crosses the cervical os, a com-plete previa is diagnosed. If the leading edge of theplacenta is within 2 cm of the cervical os, a marginalprevia is diagnosed.212 Low-lying placenta is definedas a placenta with its leading edge between 2-3 cmfrom the internal cervical os. As the lower uterine seg-ment develops with advancing gestational age, theleading edge of the placenta may appear to “move”further from the internal os.213
ComplicationsMaternal complications include placenta accreta,which refers to abnormal attachment of placental villito the uterine wall in which chorionic villi are directlyattached to the myometrium due to a poorly devel-oped decidua basalis, and Nitabuch’s layer that nor-mally separates the placenta from the uterinemyometrium.214 In the absence of placenta previa, pla-centa accreta is rare (1 in 7000 pregnancies). How-ever, it complicates 5%-15% of pregnancies with pla-centa previa, 25% with previa and 1 prior cesarean,and 60% with previa and 2 or more prior cesareans.215
Neonatal complications include preterm birth andmalpresentation. Fetal anemia may result from vasaprevia associated with a placenta previa, which is anindication for an emergent delivery to prevent exsan-guination of the fetus.216 Placenta previa is not associ-ated with IUGR.217
240 OBSTETRICS AND GYNECOLOGY—2009

ManagementThe goal of antepartum management is to maximizefetal maturation while minimizing risk to mother andfetus. Blind digital vaginal examination should beavoided in all women with antepartum hemorrhageuntil placenta previa is excluded. Non-reassuringfetal testing and excessive maternal hemorrhage arecontraindications to expectant management, and maynecessitate immediate cesarean delivery irrespectiveof gestational age. However, most episodes of antena-tal bleeding are not life-threatening. With carefulmonitoring, delivery can be safely delayed in mostcases. Placenta previa may resolve with time due tocephalic growth of the lower uterine segment, draw-ing the leading edge of the placenta away from theinternal os, thereby allowing vaginal delivery to pro-ceed. Indeed, only 5% of low-lying placentae iden-tified by ultrasound at 14-20 weeks gestation persist toterm (although complete placenta previa is unlikely toresolve).218 Cesarean delivery is generally performedby 37 weeks gestation due to active maternal hemor-rhage or concern over impending risk of maternalhemorrhage. If elective delivery of an asymptomaticpatient is planned prior to 39 weeks gestation, itshould be done only after documentation of fetal lungmaturity.
Placental Abruption
Placental abruption refers to premature separation ofthe placenta from the underlying maternal decidua,and complicates 1 in 120 pregnancies.219, 220 Risk fac-tors include hypertension, prior placental abruption,trauma, smoking, cocaine, uterine anomaly orfibroids, multiparity, advanced maternal age, pretermPROM, bleeding diathesis and an overdistendeduterus (multifetal gestations, polyhydramnios).220 Pla-cental abruption is a clinical diagnosis that mayinclude vaginal bleeding (80%), painful uterine con-tractions (35%), and abdominal tenderness (70%),with or without non-reassuring fetal testing (50%).The amount of vaginal bleeding is not a reliable indi-cator of the severity of the condition, because bleed-ing may be concealed. A retroplacental collection of≥300 mL is necessary for sonographic visualization,and only 2% of placental abruptions can be visualizedon ultrasound. Serial measurements of fundal heightand abdominal girth are useful to monitor large retro-placental blood collections.
Complications. Maternal complications include mor-tality (due to hemorrhage, cardiac failure or renal fail-ure [0.5%-5%]) and coagulopathy (10%). Fetal com-plications include IUFD in 10%-35% of cases due pri-marily to fetal hypoxia, exsanguination and/or com-plications of prematurity. Chronic abruption is alsoassociated with an increased rate of congenitalanomalies and IUGR.219, 221
Management. Hospitalization is indicated to evalu-ate maternal and fetal condition. Mode and timingof delivery depends on the condition of the motherand fetus, and on gestational age. In the setting ofhemodynamic instability, invasive monitoring andimmediate delivery may be necessary. If the abrup-tion is mild and pregnancy is remote from term,expectant management may be appropriate. Placen-tal abruption is a relative contraindication to tocoly-sis, particularly with beta-agonists that may causematernal tachycardia and increased pulse pressureto the site of the abruption. The risk of cesareandelivery is increased primarily due to fetal compromise.
Vasa Previa
Vasa previa refers to the presence of fetal vesselscoursing through the membranes (velamentous inser-tion) overlying the internal os ahead of presenting partof the fetus. Vasa previa is usually asymptomatic, butmay present with painless bright-red vaginal bleed-ing, often associated with diminished fetal movement.Since bleeding is from the umbilical vessels and isfetal in origin, fetal mortality is >75%, due primarilyto fetal exsanguination. Diagnosis is by the bedsideApt test (hemoglobin alkaline denaturation test),which involves adding 2-3 drops of an alkaline solu-tion (NaOH) to 1 mL of blood. If the blood is mater-nal, erythrocytes will rupture and the mixture will turnbrown. Fetal erythrocytes, on the other hand, are resis-tant to rupture and the mixture will remain red. Emer-gent cesarean delivery is indicated regardless of gesta-tional age if the fetus is viable. Brisk vaginal bleedingtemporally related to spontaneous or artificial ruptureof the membranes, particularly in light of a placentaprevia or low-lying placenta, and acute changes infetal heart rate tracing, should prompt consideration ofthis diagnosis.222
CHAPTER 9: OBSTETRIC COMPLICATIONS 241
10. References
1. Shortle B, Jewelewicz R. Cervical incompetence. Fertil Steril. 1989;52(2):181-188.
2. ACOG Practice Bulletin. Cervical insufficiency.Obstet Gynecol. 2003;102(5 Pt 1):1091-1099.
3. Harger JH. Cervical cerclage: patient selection,morbidity, and success rates. Clin Perinatol.1983;10(2):321-341.
4. Golan A, Barnan R, Wexler S, Langer R,Bukovsky I, David MP. Incompetence of theuterine cervix. Obstet Gynecol Surv.1989;44(2):96-107.
5. ACOG Practice Bulletin. Clinical managementguidelines for obstetrician-gynecologist. Num-ber 43, May 2003. Management of pretermlabor. Obstet Gynecol. 2003;101(5 Pt 1):1039-1047.
6. Norman JE. Cervical function and prematurity.Best Pract Res Clin Obstet Gynaecol. May2007.
7. Althuisius SM, Dekker GA. A five century evo-lution of cervical incompetence as a clinicalentity. Curr Pharm Des. 2005;11(6):687-697.
8. Althuisius SM, Dekker GA, Hummel P,Bekedam DJ, van Geijn HP. Final results of theCervical Incompetence Prevention RandomizedCerclage Trial (CIPRACT): therapeutic cer-clage with bed rest versus bed rest alone.Am JObstet Gynecol. 2001;185(5):1106-1112.
9. Dor J, Shalev J, Mashiach S, Blankstein J, SerrDM. Elective cervical suture of twin pregnan-cies diagnosed ultrasonically in the firsttrimester following induced ovulation. GynecolObstet Invest. 1982;13(1):55-60.
10. Lazar P, Gueguen S, Dreyfus J, Renaud R, Pon-tonnier G, Papiernik E. Multicentred controlledtrial of cervical cerclage in women at moderaterisk of preterm delivery. Br J Obstet Gynaecol.1984;91(8):731-735.
11. Rush RW, Isaacs S, McPherson K, Jones L,Chalmers I, Grant A. A randomized controlledtrial of cervical cerclage in women at high risk ofspontaneous preterm delivery. Br J ObstetGynaecol. 1984;91(8):724-730.
12. Roman AS, Rebarber A, Pereira L, SfakianakiAK, Mulholland J, Berghella V. The efficacy ofsonographically indicated cerclage in multiplegestations. J Ultrasound Med. 2005;24(6):763-768; quiz 70-71.
13. To MS, Alfirevic Z, Heath VC, et al. Cervicalcerclage for prevention of preterm delivery inwomen with short cervix: randomised controlledtrial. Lancet. 2004;363(9424):1849-1853.
14. Mays JK, Figueroa R, Shah J, Khakoo H,Kaminsky S, Tejani N. Amniocentesis for selec-tion before rescue cerclage. Obstet Gynecol.2000;95(5):652-655.
15. Romero R, Gonzalez R, Sepulveda W, et al.Infection and labor. VIII. Microbial invasion ofthe amniotic cavity in patients with suspectedcervical incompetence: prevalence and clinicalsignificance. Am J Obstet Gynecol. 1992;167(4 :1):1086-1091.
16. MacDougall J, Siddle N. Emergency cervicalcerclage.Br J Obstet Gynaecol.1991;98(12):1234-1238.
17. Olatunbosun OA, Dyck F. Cervical cerclageoperation for a dilated cervix. Obstet Gynecol.1981;57(2):166-170.
18. Scheerer LJ, Lam F, Bartolucci L, Katz M. Anew technique for reduction of prolapsed fetalmembranes for emergency cervical cerclage.Obstet Gynecol. 1989;74(3:1):408-410.
19. Sher G. Congenital incompetence of the cervicalos: reduction of bulging membranes with a mod-ified Foley catheter. J Reprod Med.1979;22(3):165-167.
242 OBSTETRICS AND GYNECOLOGY—2009
20. McDonald IA. Suture of the cervix forinevitable miscarriage. JObstet Gynaecol BrEmp. 1957;64(3):346-350.
21. Goodlin RC. Cervical incompetence, hourglassmembranes, and amniocentesis. ObstetGynecol. 1979;54(6):748-750.
22. Ochi M, Ishikawa K, Itoh H, et al. [Aggressivemanagement of prolapsed fetal membranes ear-lier than 26 weeks gestation by emergentMcDonald cerclage combined with amniocente-sis and bladder overfilling].Nippon SankaFujinka Gakkai Zasshi. 1994;46(4):301-307.
23. Locatelli A, Vergani P, Bellini P, Strobelt N,Arreghini A, Ghidini A. Amnioreduction inemergency cerclage with prolapsed membranes:comparison of two methods for reducing themembranes.Am J Perinatol. 1999;16(2):73-77.
24. Daskalakis G, Papantoniou N, Mesogitis S,Antsaklis A. Management of cervical insuffi-ciency and bulging fetal membranes.ObstetGynecol. 2006;107(2 Pt 1):221-226.
25. Rozenberg P, Senat MV, Gillet A, Ville Y. Com-parison of two methods of cervical cerclage byultrasound cervical measurement. J MaternFetal Neonatal Med. 2003;13(5):314-317.
26. Iams JD. Abnormal Cervical Competence. 5thed. Philadelphia: Saunders; 2004.
27. Shirodkar V. A new method of operative treat-ment for habitual abortion in the secondtrimester of pregnancy. Antiseptic. 1955;52:299.
28. Benson RC, Durfee RB. Transabdominal cer-vico uterine cerclage during pregnancy for thetreatment of cervical incompetency. ObstetGynecol. 1965;25:145-155.
29. Novy MJ. Transabdominal cervicoisthmic cer-clage: a reappraisal 25 years after its introduc-tion. Am J Obstet Gynecol. 1991;164(6:1):1635-1641; discussion 41-42.
30. McElrath TF, Norwitz ER, Lieberman ES,Heffner LJ. Management of cervical cerclageand preterm premature rupture of the mem-branes: should the stitch be removed?Am JObstet Gynecol. 2000;183(4):840-846.
31. Jenkins TM, Berghella V, Shlossman PA, et al.Timing of cerclage removal after preterm pre-mature rupture of membranes: maternal andneonatal outcomes. Am J Obstet Gynecol.2000;183(4):847-852.
32. Final report of the Medical Research Coun-cil/Royal College of Obstetricians and Gynae-cologists multicentre randomised trial of cervi-cal cerclage. MRC/RCOG Working Party onCervical Cerclage. Br J Obstet Gynaecol.1993;100(6):516-523.
Preterm Labor
33. Rush RW, Keirse MJ, Howat P, Baum JD,Anderson AB, Turnbull AC. Contribution ofpreterm delivery to perinatal mortality. Br MedJ. 1976;2(6042):965-968.
34. Ananth CV, Vintzileos AM. Epidemiology ofpreterm birth and its clinical subtypes. J MaternFetal Neonatal Med. 2006;19(12):773-82.
35. Norwitz ER, Robinson JN, Challis JR. The controlof labor. N Engl J Med. 1999;341(9):660-666.
36. Romero R, Avila C, Brekus CA, Morotti R. Therole of systemic and intrauterine infection inpreterm parturition. Ann NY Acad Sci.1991;622:355-375.
37. Dudley DJ. Pre-term labor: an intra-uterineinflammatory response syndrome? J ReprodImmunol. 1997;36(1-2):93-109.
38. Creasy RK, Gummer BA, Liggins GC. Systemfor predicting spontaneous preterm birth. ObstetGynecol. 1980;55(6):692-695.
39. Mercer BM, Goldenberg RL, Das A, et al. Thepreterm prediction study: a clinical risk assess-ment system.Am J Obstet Gynecol.1996;174(6):1885-1893; discussion 93-95.
CHAPTER 9: OBSTETRIC COMPLICATIONS 243
40. Iams JD, Johnson FF, O’Shaughnessy RW. Aprospective random trial of home uterine activ-ity monitoring in pregnancies at increased risk ofpreterm labor. Part II. Am J Obstet Gynecol.1988;159(3):595-603.
41. Mortensen OA, Franklin J, Lofstrand T, Svan-berg B. Prediction of preterm birth. Acta ObstetGynecol Scand. 1987;66(6):507-512.
42. Iams JD, Goldenberg RL, Meis PJ, et al. Thelength of the cervix and the risk of spontaneouspremature delivery. National Institute of ChildHealth and Human Development Maternal FetalMedicine Unit Network. N Engl J Med.1996;334(9):567-572.
43. Heath VC, Southall TR, Souka AP, Elisseou A,Nicolaides KH. Cervical length at 23 weeks ofgestation: prediction of spontaneous pretermdelivery. Ultrasound Obstet Gynecol.1998;12(5):312-317.
44. Hillier SL, Nugent RP, Eschenbach DA, et al.Association between bacterial vaginosis andpreterm delivery of a low-birth-weight infant.The Vaginal Infections and Prematurity StudyGroup. N Engl J Med. 1995;333(26):1737-1742.
45. Gibbs RS, Romero R, Hillier SL, EschenbachDA, Sweet RL. A review of premature birth andsubclinical infection. Am J Obstet Gynecol.1992;166(5):1515-1528.
46. Lockwood CJ, Senyei AE, Dische MR, et al.Fetal fibronectin in cervical and vaginal secre-tions as a predictor of preterm delivery. N Engl JMed. 1991;325(10):669-674.
47. Goldenberg RL, Mercer BM, Meis PJ, CopperRL, Das A, McNellis D. The preterm predictionstudy: fetal fibronectin testing and spontaneouspreterm birth. NICHD Maternal Fetal MedicineUnits Network. Obstet Gynecol.1996;87(5:1):643-648.
48. Iams JD, Casal D, McGregor JA, et al. Fetalfibronectin improves the accuracy of diagnosisof preterm labor. Am J Obstet Gynecol.1995;173(1):141-145.
49. Goodwin TM. A role for estriol in human labor,term and preterm. Am J Obstet Gynecol.1999;180(1 Pt 3):S208-S213.
50. McGregor JA, Jackson GM, Lachelin GC, et al.Salivary estriol as risk assessment for pretermlabor: a prospective trial. Am J Obstet Gynecol.1995;173(4):1337-1342.
51. Goldenberg RL, Cliver SP, Bronstein J, CutterGR, Andrews WW, Mennemeyer ST. Bed rest inpregnancy. Obstet Gynecol. 1994;84(1):131-136.
52. Besinger RE, Niebyl JR. The safety and efficacyof tocolytic agents for the treatment of pretermlabor. Obstet Gynecol Surv. 1990;45(7):415-440.
53. Higby K, Xenakis EM, Pauerstein CJ. Dotocolytic agents stop preterm labor? A criticaland comprehensive review of efficacy andsafety.Am J Obstet Gynecol. 1993;168(4):1247-1256; discussion 56-59.
54. Hill WC. Risks and complications of tocolysis.Clin Obstet Gynecol. 1995;38(4):725-745.
55. Hollander DI, Nagey DA, Pupkin MJ. Magne-sium sulfate and ritodrine hydrochloride: a ran-domized comparison.Am J Obstet Gynecol.1987;156(3):631-637.
56. Witlin AG, Sibai BM. Magnesium sulfate ther-apy in preeclampsia and eclampsia. ObstetGynecol. 1998;92(5):883-889.
57. Lamm CI, Norton KI, Murphy RJ, Wilkins IA,Rabinowitz JG. Congenital rickets associatedwith magnesium sulfate infusion for tocolysis. JPediatr. 1988;113(6):1078-1082.
58. Faidley CK, Dix PM, Morgan MA, Schechter E.Electrocardiographic abnormalities during rito-drine administration. South Med J.1990;83(5):503-506.
244 OBSTETRICS AND GYNECOLOGY—2009
59. Peterson A, Peterson K, Tongen S, et al. Glucoseintolerance as a consequence of oral terbutalinetreatment for preterm labor. J Fam Pract.1993;36(1):25-31.
60. Vanhaesebrouck P, Thiery M, Leroy JG, et al.Oligohydramnios, renal insufficiency, and ilealperforation in preterm infants after intrauterineexposure to indomethacin. J Pediatr.1988;113(4):738-743.
61. Wiggins DA, Elliott JP. Oligohydramnios ineach sac of a triplet gestation caused byMotrin®—fulfilling Kock’s postulates. Am JObstet Gynecol. 1990;162(2):460-461.
62. Suarez VR, Thompson LL, Jain V, et al. Theeffect of in utero exposure to indomethacin onthe need for surgical closure of a patent ductusarteriosus in the neonate. Am J Obstet Gynecol.2002;187(4):886-888.
63. Itabashi K, Ohno T, Nishida H. Indomethacinresponsiveness of patent ductus arteriosus andrenal abnormalities in preterm infants treatedwith indomethacin. J Pediatr. 2003;143(2):203-207.
64. van Veen AJ, Pelinck MJ, van Pampus MG,Erwich JJ. Severe hypotension and fetal deathdue to tocolysis with nifedipine. BJOG.2005;112(4):509-510.
65. Parasuraman R, Gandhi MM, Liversedge NH.Nifedipine tocolysis associated atrial fibrillationresponds to DC cardioversion.BJOG.2006;113(7):844-845.
66. Al-Omari WR, Al-Shammaa HB, Al-TikritiEM, Ahmed KW. Atosiban and nifedipine inacute tocolysis: a comparative study. Eur JObstet Gynecol Reprod Biol. 2006;128(1-2):129-134.
67. Stika CS, Gross GA, Leguizamon G, et al. Aprospective randomized safety trial of celecoxibfor treatment of preterm labor. Am J ObstetGynecol. 2002;187(3):653-660.
68. Effect of corticosteroids for fetal maturation onperinatal outcomes. NIH Consensus Develop-ment Panel on the Effect of Corticosteroids forFetal Maturation on Perinatal Outcomes. JAMA.1995;273(5):413-418.
69. ACOG committee opinion. Antenatal corticos-teroid therapy for fetal maturation. Number147—December 1994. Committee on ObstetricPractice. American College of Obstetricians andGynecologists. Int J Gynaecol Obstet.1995;48(3):340-342.
70. Lee MJ, Davies J, Guinn D, et al. Single versusweekly courses of antenatal corticosteroids inpreterm premature rupture of membranes.Obstet Gynecol. 2004;103(2):274-281.
71. Committee on Obstetric P. ACOG committeeopinion: antenatal corticosteroid therapy forfetal maturation. Obstet Gynecol.2002;99(5:1):871-873.
72. Vermillion ST, Soper DE, Bland ML, NewmanRB. Effectiveness of antenatal corticosteroidadministration after preterm premature ruptureof the membranes. Am J Obstet Gynecol.2000;183(4):925-929.
73. Rust OA, Bofill JA, Arriola RM, Andrew ME,Morrison JC. The clinical efficacy of oraltocolytic therapy. Am J Obstet Gynecol.1996;175(4 Pt 1):838-842.
74. Guinn DA, Goepfert AR, Owen J, WenstromKD, Hauth JC. Terbutaline pump maintenancetherapy for prevention of preterm delivery: adouble-blind trial. Am J Obstet Gynecol.1998;179(4):874-878.
75. Ogburn PL Jr, Julian TM, Williams PP, Thomp-son TR. The use of magnesium sulfate for tocol-ysis in preterm labor complicated by twin gesta-tion and betamimetic-induced pulmonaryedema. Acta Obstet Gynecol Scand.1986;65(7):793-794.
CHAPTER 9: OBSTETRIC COMPLICATIONS 245
76. Ferguson JE, 2nd, Hensleigh PA, Kredenster D.Adjunctive use of magnesium sulfate with rito-drine for preterm labor tocolysis. Am J ObstetGynecol. 1984;148(2):166-171.
77. Valenzuela G, Cline S. Use of magnesium sul-fate in premature labor that fails to respond tobetamimetic drugs. Am J Obstet Gynecol.1982;143(6):718-719.
78. Gibbs RS, Eschenbach DA. Use of antibiotics toprevent preterm birth. Am J Obstet Gynecol.1997;177(2):375-380.
Post-term Pregnancy
79. ACOG Practice Bulletin. Clinical managementguidelines for obstetricians-gynecologists.Number 55, September 2004 (replaces practicepattern number 6, October 1997). Managementof Postterm Pregnancy. Obstet Gynecol.2004;104(3):639-646.
80. ACOG criteria set. Postterm pregnancy. Number10—August 1995. Committee on QualityAssessment. American College of Obstetriciansand Gynecologists. Int J Gynaecol Obstet.1996;53(1):89-90.
81. Barnes AC. Postmaturity syndrome; the obstetri-cian’s role in management. Calif Med.1956;85(5):289-292.
82. Clifford SH. Postmaturity clinical syndrome andpathologic findings. AMA Am J Dis Child.1953;86(3):319-321.
83. Feldman GB. Prospective risk of stillbirth.Obstet Gynecol. 1992;79(4):547-553.
84. American College of Obstetricians and Gynecol-ogists. ACOG Practice Bulletin No. 22. FetalMacrosomia. Washington, DC:ACOG, 2000.
85. Spellacy WN, Miller S, Winegar A, PetersonPQ. Macrosomia—maternal characteristics andinfant complications. Obstet Gynecol.1985;66(2):158-161.
86. Rosen MG, Dickinson JC. Management of post-term pregnancy. N Engl J Med.1992;326(24):1628-1629.
87. Rand L, Robinson JN, Economy KE, NorwitzER. Post-term induction of labor revisited.Obstet Gynecol. 2000;96(5:1):779-783.
88. Alexander JM, McIntire DD, Leveno KJ. Fortyweeks and beyond: pregnancy outcomes byweek of gestation. Obstet Gynecol.2000;96(2):291-294.
89. Treger M, Hallak M, Silberstein T, Friger M,Katz M, Mazor M. Post-term pregnancy: shouldinduction of labor be considered before 42weeks? J Matern Fetal Neonatal Med.2002;11(1):50-53.
90. American College of Obstetricians and Gynecol-ogists. ACOG Practice Bulletin No. 10. Induc-tion of Labor. Washington, DC:ACOG, 1999.
91. Crowley P. Interventions for preventing orimproving the outcome of delivery at or beyondterm. Cochrane Database Syst Rev.2000(2):CD000170.
92. Hannah ME, Hannah WJ, Hellmann J, HewsonS, Milner R, Willan A. Induction of labor ascompared with serial antenatal monitoring inpost-term pregnancy. A randomized controlledtrial. The Canadian Multicenter Post-term Preg-nancy Trial Group. N Engl J Med.1992;326(24):1587-1592.
93. A clinical trial of induction of labor versusexpectant management in postterm pregnancy.The National Institute of Child Health andHuman Development Network of Maternal-Fetal Medicine Units. Am J Obstet Gynecol.1994;170(3):716-723.
246 OBSTETRICS AND GYNECOLOGY—2009
Hypertensive Disorders of Pregnancy
94. Rochat RW, Koonin LM, Atrash HK, Jewett JF.Maternal mortality in the United States: reportfrom the Maternal Mortality Collaborative.Obstet Gynecol. 1988;72(1):91-97.
95. Berg CJ, Atrash HK, Koonin LM, Tucker M.Pregnancy-related mortality in the UnitedStates, 1987-1990. Obstet Gynecol.1996;88(2):161-167.
96. Lin CC, Lindheimer MD, River P, Moawad AH.Fetal outcome in hypertensive disorders of preg-nancy. Am J Obstet Gynecol. 1982;142(3):255-260.
97. Barr M, Jr. Teratogen update: angiotensin-con-verting enzyme inhibitors. Teratology.1994;50(6):399-409.
98. Quan A. Fetopathy associated with exposure toangiotensin converting enzyme inhibitors andangiotensin receptor antagonists. Early HumDev. 2006;82(1):23-28.
99. Fretts RC. Etiology and prevention of stillbirth.Am J Obstet Gynecol. 2005;193(6):1923-1935.
100. ACOG Practice Bulletin. Chronic hypertensionin pregnancy. ACOG Committee on PracticeBulletins. Obstet Gynecol. 2001;98(1) suppl177-185.
101. ACOG Practice Bulletin. Diagnosis and man-agement of preeclampsia and eclampsia. Num-ber 33, January 2002. American College ofObstetricians and Gynecologists. Int J GynaecolObstet. 2002;77(1):67-75.
102. Dekker GA, Sibai BM. Etiology and pathogene-sis of preeclampsia: current concepts. Am JObstet Gynecol. 1998;179(5):1359-1375.
103. Redman CW, Sacks GP, Sargent IL. Preeclamp-sia: an excessive maternal inflammatoryresponse to pregnancy. Am J Obstet Gynecol.1999;180(2:1):499-506.
104. Meekins JW, Pijnenborg R, Hanssens M,McFadyen IR, van Asshe A. A study of placentalbed spiral arteries and trophoblast invasion innormal and severe pre-eclamptic pregnancies.Br J Obstet Gynaecol. 1994;101(8):669-674.
105. Brosens IA, Robertson WB, Dixon HG. The roleof the spiral arteries in the pathogenesis ofpreeclampsia. Obstet Gynecol Annu.1972;1:177-191.
106. Cross JC, Werb Z, Fisher SJ. Implantation andthe placenta: key pieces of the development puz-zle. Science. 1994;266(5190):1508-1518.
107. Maynard SE, Min JY, Merchan J, et al. Excessplacental soluble fms-like tyrosine kinase 1(sFlt1) may contribute to endothelial dysfunc-tion, hypertension, and proteinuria inpreeclampsia. J Clin Invest. 2003;111(5):649-658.
108. Thadhani R, Mutter WP, Wolf M, et al. Firsttrimester placental growth factor and solublefms-like tyrosine kinase 1 and risk forpreeclampsia. J Clin Endocrinol Metab.2004;89(2):770-775.
109. Report of the National High Blood PressureEducation Program Working Group on HighBlood Pressure in Pregnancy. Am J ObstetGynecol. 2000;183(1):S1-S22.
110. Odendaal HJ, Pattinson RC, Bam R, Grove D,Kotze TJ. Aggressive or expectant managementfor patients with severe preeclampsia between28-34 weeks gestation: a randomized controlledtrial. Obstet Gynecol. 1990;76(6):1070-1075.
111. Sibai BM, Mercer BM, Schiff E, Friedman SA.Aggressive versus expectant management ofsevere preeclampsia at 28 to 32 weeks gestation:a randomized controlled trial. Am J ObstetGynecol. 1994;171(3):818-822.
112. Alexander JM, Bloom SL, McIntire DD, LevenoKJ. Severe preeclampsia and the very low birthweight infant: is induction of labor harmful?Obstet Gynecol. 1999;93(4):485-488.
CHAPTER 9: OBSTETRIC COMPLICATIONS 247
113. Nassar AH, Adra AM, Chakhtoura N, Gomez-Marin O, Beydoun S. Severe preeclampsiaremote from term: labor induction or electivecesarean delivery? Am J Obstet Gynecol.1998;179(5):1210-1213.
114. Sibai BM. Treatment of hypertension in preg-nant women. N Engl J Med. 1996;335(4):257-265.
115. Lindenstrom E, Boysen G, Nyboe J. Influence ofsystolic and diastolic blood pressure on strokerisk: a prospective observational study. Am JEpidemiol. 1995;142(12):1279-1290.
116. Fontenot MT, Lewis DF, Frederick JB, et al. Aprospective randomized trial of magnesium sul-fate in severe preeclampsia: use of diuresis as aclinical parameter to determine the duration ofpostpartum therapy. Am J Obstet Gynecol.2005;192(6):1788-1793; discussion 93-94.
117. Which anticonvulsant for women with eclamp-sia? Evidence from the Collaborative EclampsiaTrial. Lancet. 1995;345(8963):1455-1463.
118. Coetzee EJ, Dommisse J, Anthony J. A ran-domised controlled trial of intravenous magne-sium sulphate versus placebo in the managementof women with severe pre-eclampsia. Br JObstet Gynaecol. 1998;105(3):300-303.
119. Douglas KA, Redman CW. Eclampsia in theUnited Kingdom. BMJ. 1994;309(6966):1395-1400.
120. Sibai BM. Diagnosis, prevention, and manage-ment of eclampsia. Obstet Gynecol.2005;105(2):402-410.
121. Sibai BM, Villar MA, Mabie BC. Acute renalfailure in hypertensive disorders of pregnancy.Pregnancy outcome and remote prognosis inthirty-one consecutive cases. Am J ObstetGynecol. 1990;162(3):777-783.
122. Sibai BM. Chronic hypertension in pregnancy.Obstet Gynecol. 2002;100(2):369-377.
123. Sibai BM, el-Nazer A, Gonzalez-Ruiz A. Severepreeclampsia-eclampsia in young primigravidwomen: subsequent pregnancy outcome andremote prognosis. Am J Obstet Gynecol.1986;155(5):1011-1016.
124. Sibai BM. Prevention of preeclampsia: a big dis-appointment. Am J Obstet Gynecol.1998;179(5):1275-1278.
125. Norwitz ER, Robinson JN, Repke JT. Preven-tion of preeclampsia: is it possible? Clin ObstetGynecol. 1999;42(3):436-454.
126. Askie LM, Duley L, Henderson-Smart DJ,Stewart LA. Antiplatelet agents for preventionof pre-eclampsia: a meta-analysis of individualpatient data. Lancet. 2007;369(9575):1791-1798.
Intrauterine Fetal Demise
127. Spong CY, Erickson K, Willinger M, HankinsGD, Schulkin J. Stillbirth in obstetric practice:report of survey findings. J Matern FetalNeonatal Med. 2003;14(1):39-44.
128. MacDorman MF, Hoyert DL, Martin JA, Mun-son ML, Hamilton BE. Fetal and perinatal mor-tality, United States, 2003. Natl Vital Stat Rep.2007;55(6):1-17.
129. Huang DY, Usher RH, Kramer MS, Yang H,Morin L, Fretts RC. Determinants of unex-plained antepartum fetal deaths. Obstet Gynecol.2000;95(2):215-221.
130. Froen JF, Arnestad M, Frey K, Vege A, SaugstadOD, Stray-Pedersen B. Risk factors for suddenintrauterine unexplained death: epidemiologiccharacteristics of singleton cases in Oslo, Nor-way, 1986-1995. Am J Obstet Gynecol.2001;184(4):694-702.
131. Tenovuo A, Kero P, Piekkala P, Korvenranta H,Erkkola R. Fetal and neonatal mortality of small-for-gestational age infants. A 15-year study of381 cases. Eur J Pediatr. 1988;147(6):613-615.
248 OBSTETRICS AND GYNECOLOGY—2009
132. Spinillo A, Capuzzo E, Piazzi G, Nicola S,Colonna L, Iasci A. Maternal high-risk factorsand severity of growth deficit in small for gesta-tional age infants. Early Hum Dev.1994;38(1):35-43.
133. Wapner RJ, Lewis D. Genetics and metaboliccauses of stillbirth. Semin Perinatol.2002;26(1):70-74.
134. Kolialexi A, Tsangaris GT, Antsaklis A,Mavroua A. Rapid clearance of fetal cells frommaternal circulation after delivery. Ann NY AcadSci. 2004;1022:113-118.
135. Brookes JS, Hagmann C. MRI in fetal necropsy. J Magn Reson Imaging. 2006;24(6):1221-1228.
136. Cernach MC, Patricio FR, Galera MF, MoronAF, Brunoni D. Evaluation of a protocol forpostmortem examination of stillbirths andneonatal deaths with congenital anomalies.Pediatr Dev Pathol. 2004;7(4):335-341.
137. Reid DE, Weiner AE, Roby CC, Diamond LK.Maternal afibrinogenemia associated with long-standing intrauterine fetal death. Am J ObstetGynecol. 1953;66(3):500-506.
138. Pritchard JA. Fetal death in utero. ObstetGynecol. 1959;14:573-580.
139. Carlson NJ, Towers CV. Multiple gestation com-plicated by the death of one fetus. ObstetGynecol. 1989;73(5:1):685-9.
140. D’Alton ME, Newton ER, Cetrulo CL. Intrauter-ine fetal demise in multiple gestation. ActaGenet Med Gemellol (Roma). 1984;33(1):43-49.
141. Bejar R, Vigliocco G, Gramajo H, et al. Antena-tal origin of neurologic damage in newborninfants. II. Multiple gestations. Am J ObstetGynecol. 1990;162(5):1230-1236.
142. Romero R, Duffy TP, Berkowitz RL, Chang E,Hobbins JC. Prolongation of a preterm preg-nancy complicated by death of a single twin inutero and disseminated intravascular coagula-tion. Effects of treatment with heparin. N Engl JMed. 1984;310(12):772-774.
143. Benirschke K. Intrauterine death of a twin:mechanisms, implications for surviving twin,and placental pathology. Semin Diagn Pathol.1993;10(3):222-231.
144. Szymonowicz W, Preston H, Yu VY. The surviv-ing monozygotic twin. Arch Dis Child.1986;61(5):454-458.
145. Ben-Shlomo I, Alcalay M, Lipitz S, LeibowitzK, Mashiach S, Barkai G. Twin pregnanciescomplicated by the death of one fetus. J ReprodMed. 1995;40(6):458-462.
Intrauterine Growth Restriction
146. American College of Obstetricians and Gyne-cologists. ACOG Practice Bulletin No. 12.Intrauterine growth restriction. Washington, DC:ACOG. 2000.
147. Lin CC, Santolaya-Forgas J. Current concepts offetal growth restriction: part I. Causes, classifica-tion, and pathophysiology. Obstet Gynecol.1998;92(6):1044-1055.
148. Clausson B, Gardosi J, Francis A, Cnattingius S.Perinatal outcome in SGA births defined by cus-tomised versus population-based birthweightstandards. Bjog. 2001;108(8):830-834.
149. Pollack RN, Divon MY. Intrauterine growthretardation: definition, classification, and etiol-ogy. Clin Obstet Gynecol. 1992;35(1):99-107.
150. Kazzi GM, Gross TL, Sokol RJ. Fetal biparietaldiameter and placental grade: predictors ofintrauterine growth retardation. Obstet Gynecol.1983;62(6):755-759.
CHAPTER 9: OBSTETRIC COMPLICATIONS 249
151. Lin CC, Santolaya-Forgas J. Current concepts offetal growth restriction: part II. Diagnosis andmanagement. Obstet Gynecol. 1999;93(1):140-146.
152. Lee MJ, Conner EL, Charafeddine L, Woods JR,Jr., Priore GD. A critical birth weight and otherdeterminants of survival for infants with severeintrauterine growth restriction. Ann NY Acad Sci.2001;943:326-339.
153. Godfrey KM, Barker DJ. Fetal programmingand adult health. Public Health Nutr.2001;4(2B):611-624.
154. Odibo AO, Quinones JN, Lawrence-Cleary K,Stamilio DM, Macones GA. What antepartumfetal test should guide the timing of delivery ofthe preterm growth-restricted fetus? A decision-analysis. Am J Obstet Gynecol.2004;191(4):1477-1482.
155. Simchen MJ, Alkazaleh F, Adamson SL, et al.The fetal cardiovascular response to antenatalsteroids in severe early-onset intrauterinegrowth restriction. Am J Obstet Gynecol.2004;190(2):296-304.
156. Mordel N, Ezra Y, Dorembus D, Benshushan A,Schenker JG, Sadovsky E. Triplets are not sorare any more. J Perinat Med. 1992;20(2):117-122.
Multiple Gestation
157. Norwitz E. Multiple Pregnancies: Trends past,present and future. Philadelphia, PA: WB Saun-ders Company; 1998.
158. Derom C, Vlietinck R, Derom R, Van denBerghe H, Thiery M. Increased monozygotictwinning rate after ovulation induction. Lancet.1987;1(8544):1236-1238.
159. Barss VA, Benacerraf BR, Frigoletto FD, Jr.Ultrasonographic determination of chorion typein twin gestation. Obstet Gynecol.1985;66(6):779-783.
160. Winn HN, Gabrielli S, Reece EA, Roberts JA,Salafia C, Hobbins JC. Ultrasonographic criteriafor the prenatal diagnosis of placental chorionic-ity in twin gestations.Am J Obstet Gynecol.1989;161(6:1):1540-1542.
161. Scardo JA, Ellings JM, Newman RB. Prospec-tive determination of chorionicity, amnionicity,and zygosity in twin gestations. Am J ObstetGynecol. 1995;173(5):1376-1380.
162. Wood SL, St Onge R, Connors G, Elliot PD.Evaluation of the twin peak or lambda sign indetermining chorionicity in multiple pregnancy.Obstet Gynecol. 1996;88(1):6-9.
163. Kovacs BW, Kirschbaum TH, Paul RH. Twingestations: I. Antenatal care and complications.Obstet Gynecol. 1989;74(3:1):313-317.
164. Haning RV, Jr., Seifer DB, Wheeler CA, Frish-man GN, Silver H, Pierce DJ. Effects of fetalnumber and multifetal reduction on length of invitro fertilization pregnancies. Obstet Gynecol.1996;87(6):964-968.
165. Hendricks CH. Twinning in relation to birthweight, mortality, and congenital anomalies.Obstet Gynecol. 1966;27(1):47-53.
166. Erkkola R, Ala-Mello S, Piiroinen O, Kero P,Sillanpaa M. Growth discordancy in twin preg-nancies: a risk factor not detected by measure-ments of biparietal diameter. Obstet Gynecol.1985;66(2):203-206.
167. Peek MJ, McCarthy A, Kyle P, Sepulveda W,Fisk NM. Medical amnioreduction with sulindacto reduce cord complications in monoamniotictwins. Am J Obstet Gynecol. 1997;176(2):334-336.
168. Carr SR, Aronson MP, Coustan DR. Survivalrates of monoamniotic twins do not decreaseafter 30 weeks gestation. Am J Obstet Gynecol.1990;163(3):719-722.
169. Gonzalez MC, Reyes H, Arrese M, et al. Intra-hepatic cholestasis of pregnancy in twin preg-nancies. J Hepatol. 1989;9(1):84-90.
250 OBSTETRICS AND GYNECOLOGY—2009
170. Fick AL, Feldstein VA, Norton ME, Wassel FyrC, Caughey AB, Machin GA. Unequal placentalsharing and birth weight discordance in mono-chorionic diamniotic twins. Am J ObstetGynecol. 2006;195(1):178-183.
171. Danskin FH, Neilson JP. Twin-to-twin transfu-sion syndrome: what are appropriate diagnosticcriteria? Am J Obstet Gynecol. 1989;161(2):365-369.
172. Reisner DP, Mahony BS, Petty CN, et al. Stucktwin syndrome: outcome in thirty-seven consec-utive cases. Am J Obstet Gynecol.1993;169(4):991-995.
173. Urig MA, Clewell WH, Elliott JP. Twin-twintransfusion syndrome. Am J Obstet Gynecol.1990;163(5 Pt 1):1522-1526.
174. Gonsoulin W, Moise KJ, Jr., Kirshon B, CottonDB, Wheeler JM, Carpenter RJ, Jr. Outcome oftwin-twin transfusion diagnosed before 28weeks of gestation. Obstet Gynecol.1990;75(2):214-216.
175. Ville Y, Hyett J, Hecher K, Nicolaides K. Prelim-inary experience with endoscopic laser surgeryfor severe twin-twin transfusion syndrome. NEngl J Med. 1995;332(4):224-227.
176. Elliott JP, Urig MA, Clewell WH. Aggressivetherapeutic amniocentesis for treatment of twin-twin transfusion syndrome. Obstet Gynecol.1991;77(4):537-540.
177. Wittmann BK, Farquharson DF, Thomas WD,Baldwin VJ, Wadsworth LD. The role of feticidein the management of severe twin transfusionsyndrome. Am J Obstet Gynecol.1986;155(5):1023-1026.
178. Senat MV, Deprest J, Boulvain M, Paupe A,Winer N, Ville Y. Endoscopic laser surgery ver-sus serial amnioreduction for severe twin-to-twin transfusion syndrome. N Engl J Med.2004;351(2):136-144.
179. ACOG Practice Bulletin #56: Multiple gesta-tion: complicated twin, triplet, and high-ordermultifetal pregnancy. Obstet Gynecol.2004;104(4):869-883.
180. O’Brien JE, Dvorin E, Yaron Y, et al. Differen-tial increases in AFP, hCG, and uE3 in twinpregnancies: impact on attempts to quantifyDown syndrome screening calculations. Am JMed Genet. 1997;73(2):109-112.
181. Melgar CA, Rosenfeld DL, Rawlinson K,Greenberg M. Perinatal outcome after multifetalreduction to twins compared with nonreducedmultiple gestations. Obstet Gynecol.1991;78(5:1):763-767.
182. Boulot P, Hedon B, Pelliccia G, Peray P, Laffar-gue F, Viala JL. Effects of selective reduction intriplet gestation: a comparative study of 80 casesmanaged with or without this procedure. FertilSteril. 1993;60(3):497-503.
183. Smith-Levitin M, Kowalik A, Birnholz J, et al.Selective reduction of multifetal pregnancies totwins improves outcome over nonreduced tripletgestations. Am J Obstet Gynecol.1996;175(4:1):878-882.
184. Evans MI, Dommergues M, Timor-Tritsch I, etal. Transabdominal versus transcervical andtransvaginal multifetal pregnancy reduction:international collaborative experience of morethan one thousand cases. Am J Obstet Gynecol.1994;170(3):902-909.
185. Evans MI, May M, Drugan A, Fletcher JC,Johnson MP, Sokol RJ. Selective termination:clinical experience and residual risks. Am JObstet Gynecol. 1990;162(6):1568-1572; dis-cussion 72-75.
186. Malone FD, Craigo SD, Chelmow D, D’AltonME. Outcome of twin gestations complicated bya single anomalous fetus. Obstet Gynecol.1996;88(1):1-5.
CHAPTER 9: OBSTETRIC COMPLICATIONS 251
187. Evans MI, Goldberg JD, Dommergues M, et al.Efficacy of second-trimester selective termina-tion for fetal abnormalities: international collab-orative experience among the world’s largestcenters. Am J Obstet Gynecol. 1994;171(1):90-94.
188. Wald N, Cuckle H, Wu TS, George L. Maternalserum unconjugated oestriol and human chori-onic gonadotrophin levels in twin pregnancies:implications for screening for Down’s syn-drome. Br J Obstet Gynaecol. 1991;98(9):905-908.
189. Neveux LM, Palomaki GE, Knight GJ, HaddowJE. Multiple marker screening for Down syn-drome in twin pregnancies. Prenat Diagn.1996;16(1):29-34.
190. Tabor A, Philip J, Madsen M, Bang J, Obel EB,Norgaard-Pedersen B. Randomised controlledtrial of genetic amniocentesis in 4606 low-riskwomen. Lancet. 1986;1(8493):1287-1293.
191. Hook EB, Cross PK, Schreinemachers DM.Chromosomal abnormality rates at amniocente-sis and in live-born infants. JAMA.1983;249(15):2034-2038.
192. Rodis JF, Egan JF, Craffey A, Ciarleglio L,Greenstein RM, Scorza WE. Calculated risk ofchromosomal abnormalities in twin gestations.Obstet Gynecol. 1990;76(6):1037-1041.
193. Meyers C, Adam R, Dungan J, Prenger V. Ane-uploidy in twin gestations: when is maternalage advanced? Obstet Gynecol.1997;89(2):248-251.
194. Strong TH, Jr., Phelan JP, Ahn MO, Sarno AP,Jr. Vaginal birth after cesarean delivery in thetwin gestation. Am J Obstet Gynecol.1989;161(1):29-32.
195. Gocke SE, Nageotte MP, Garite T, Towers CV,Dorcester W. Management of the nonvertexsecond twin: primary cesarean section, externalversion, or primary breech extraction. Am JObstet Gynecol. 1989;161(1):111-114.
196. Davison L, Easterling TR, Jackson JC,Benedetti TJ. Breech extraction of low-birth-weight second twins: can cesarean section bejustified? Am J Obstet Gynecol.1992;166(2):497-502.
197. Dommergues M, Mahieu-Caputo D, Mandel-brot L, Huon C, Moriette G, Dumez Y. Deliv-ery of uncomplicated triplet pregnancies: is thevaginal route safer? A case-control study. Am JObstet Gynecol. 1995;172(2:1):513-517.
Preterm Premature Rupture of Membranes
198. Capeless EL, Mead PB. Management ofpreterm premature rupture of membranes: lackof a national consensus. Am J Obstet Gynecol.1987;157(1):11-12.
199. Bengtson JM, VanMarter LJ, Barss VA, GreeneMF, Tuomala RE, Epstein MF. Pregnancy out-come after premature rupture of the membranesat or before 26 weeks gestation. Obstet Gynecol.1989;73(6):921-927.
200. Park JS, Yoon BH, Romero R, et al. The rela-tionship between oligohydramnios and theonset of preterm labor in preterm premature rup-ture of membranes. Am J Obstet Gynecol.2001;184(3):459-462.
201. Bianco AT, Stone J, Lapinski R, Lockwood C,Lynch L, Berkowitz RL. The clinical outcomeof preterm premature rupture of membranes intwin versus singleton pregnancies. Am J Perina-tol. 1996;13(3):135-138.
202. Duff P, Huff RW, Gibbs RS. Management ofpremature rupture of membranes and unfavor-able cervix in term pregnancy. Obstet Gynecol.1984;63(5):697-702.
203. Hannah ME, Hodnett ED, Willan A, Foster GA,Di Cecco R, Helewa M. Prelabor rupture of themembranes at term: expectant management athome or in hospital? The TermPROM StudyGroup. Obstet Gynecol. 2000;96(4):533-538.
252 OBSTETRICS AND GYNECOLOGY—2009
204. ACOG Practice Bulletin No. 80: premature rup-ture of membranes. Clinical managementguidelines for obstetrician-gynecologists.Obstet Gynecol. 2007;109(4):1007-1019.
205. Vintzileos AM, Campbell WA, Nochimson DJ,Weinbaum PJ. Preterm premature rupture of themembranes: a risk factor for the development ofabruptio placentae. Am J Obstet Gynecol.1987;156(5):1235-1238.
206. Ohlsson A. Treatments of preterm prematurerupture of the membranes: a meta-analysis. AmJ Obstet Gynecol. 1989;160(4):890-906.
207. Wu YW, Colford JM, Jr. Chorioamnionitis as arisk factor for cerebral palsy: A meta-analysis.JAMA. 2000;284(11):1417-1424.
208. Mercer BM, Arheart KL. Antimicrobial therapyin expectant management of preterm prematurerupture of the membranes. Lancet.1995;346(8985):1271-1279.
209. Kenyon SL, Taylor DJ, Tarnow-Mordi W.Broad-spectrum antibiotics for preterm,prelabour rupture of fetal membranes: theORACLE I randomised trial. ORACLE Collab-orative Group. Lancet. 2001;357(9261):979-988.
210. Ghidini A, Salafia CM, Kirn V, Doria V, SpongCY. Biophysical profile in predicting acuteascending infection in preterm rupture of mem-branes before 32 weeks. Obstet Gynecol.2000;96(2):201-206.
Antepartum Hemorrhage
211. Sauer M, Parsons M, Sampson M. Placenta pre-via: an analysis of three years’ experience. Am JPerinatol. 1985;2(1):39-42.
212. Bhide A, Prefumo F, Moore J, Hollis B, Thila-ganathan B. Placental edge to internal os dis-tance in the late third trimester and mode ofdelivery in placenta praevia. Bjog.2003;110(9):860-864.
213. Predanic M, Perni SC, Baergen RN, Jean-PierreC, Chasen ST, Chervenak FA. A sonographicassessment of different patterns of placenta pre-via “migration” in the third trimester of preg-nancy. J Ultrasound Med. 2005;24(6):773-780.
214. Gielchinsky Y, Mankuta D, Rojansky N, LauferN, Gielchinsky I, Ezra Y. Perinatal outcome ofpregnancies complicated by placenta accreta.Obstet Gynecol. 2004;104(3):527-530.
215. Ananth CV, Smulian JC, Vintzileos AM. Theassociation of placenta previa with history ofcesarean delivery and abortion: a metaanalysis.Am J Obstet Gynecol. 1997;177(5):1071-1078.
216. Oyelese Y, Smulian JC. Placenta previa, pla-centa accreta, and vasa previa. Obstet Gynecol.2006;107(4):927-941.
217. Wolf EJ, Mallozzi A, Rodis JF, Egan JF,Vintzileos AM, Campbell WA. Placenta previais not an independent risk factor for a small forgestational age infant. Obstet Gynecol.1991;77(5):707-709.
218. Zelop CC, Bromley B, Frigoletto FD, Jr.,Benacerraf BR. Second trimester sonographi-cally diagnosed placenta previa: prediction ofpersistent previa at birth. Int J Gynaecol Obstet.1994;44(3):207-210.
219. Ananth CV, Wilcox AJ. Placental abruption andperinatal mortality in the United States. Am JEpidemiol. 2001;153(4):332-337.
220. Ananth CV, Smulian JC, Demissie K, VintzileosAM, Knuppel RA. Placental abruption amongsingleton and twin births in the United States:risk factor profiles. Am J Epidemiol.2001;153(8):771-778.
221. Ananth CV, Berkowitz GS, Savitz DA, LapinskiRH. Placental abruption and adverse perinataloutcomes. JAMA. 1999;282(17):1646-1651.
222. Oyelese KO, Turner M, Lees C, Campbell S.Vasa previa: an avoidable obstetric tragedy.Obstet Gynecol Surv. 1999;54(2):138-145.
CHAPTER 9: OBSTETRIC COMPLICATIONS 253
11. Questions
1. A 27-year-old woman presents for her first prena-tal visit at 8 weeks gestation. She has a number ofrisk factors for cervical insufficiency. On reviewof her medical and obstetrical history, you con-clude that she is a good candidate for elective cer-vical cerclage. Which of the following elements ofher history support this conclusion?
A. A history of in uteroDES exposure.
B. 3 prior first trimester elective pregnancy ter-minations.
C. A prior 20 week pregnancy loss characterized by painless cervical dilatation.
D. A triplet pregnancy conceived through invitro fertilization.
2. A nulliparous woman presents at 18 weeks gesta-tion complaining of a watery vaginal discharge.Sterile speculum examination reveals a cervixwhich is 1-2 cm dilated and 80% effaced. Afterreviewing the respective risks and benefits, thepatient elects emergent cerclage placement overbed rest. At the time of cerclage placement, how-ever, you notice something which causes you tocancel the procedure. Which of the following clin-ical findings would explain this change in plans?
A. Evidence of uterine contractions.
B. Evidence of a vaginal yeast infection.
C. Fetal membranes visible through the open cervical os.
D. A large cervical ectropion (cervical erosion).
3. A 36-year-old G7P1233 presents at 32-1/7 weeksgestation complaining of increasing abdominalpain and diminished fetal movement for 12 hours.Bimanual examination shows her cervix to be 4cm dilated and 90% effaced. Fetal cardiotocogra-phy shows evidence of uterine contractions everythree minutes. Fetal heart rate tracing is formallyreactive, with a baseline of 140 bpm and no decel-erations. A diagnosis of preterm labor is made.
Regarding the management of preterm labor,which of the following statements are true? (More than 1 statement may be true.)
A. You should recommend strict bed rest andaggressive intravenous hydration as theseinterventions have been shown to preventpreterm birth.
B. You should start IV magnesium sulfate asthis is the only drug approved by the FDA forthe treatment of preterm labor.
C. You should start broad-spectrum antibiotictherapy as this has been shown to prolonglatency.
D. You should administer antenatal corticosteroids.
4. A 28-year-old G4P3 is admitted to labor anddelivery at 29-3/7 weeks gestation with regularpainful uterine contractions every 3 minutes.Bimanual examination shows her cervix to belong and to admit a fingertip. Fetal heart ratetracing is formally reactive with a baseline of130 bpm. A diagnosis of preterm contractions ismade. She has had 3 prior spontaneous pretermdeliveries at 28-31 weeks gestation, and is veryconcerned that this pregnancy will also end pre-maturely. Which of the following statementsabout screening for preterm labor are true?(More than 1 statement may be true.)
A. Her history is highly predictive of pretermbirth. As such, no further screening tests areavailable.
B. A negative test for fetal fibronectin (fFN) incervicovaginal secretions is reassuring.
C. Transvaginal sonography reveals a cervicallength of 3.6 cm. This finding should beviewed as reassuring.
D. Given her increased risk of preterm birth, sheis a good candidate for home uterine activitymonitoring.
254 OBSTETRICS AND GYNECOLOGY—2009
5. A 21-year-old G3P2 with two prior vaginal deliv-eries is admitted to labor and delivery at 41-4/7weeks gestation complaining of decreased fetalmovement. Fetal cardiotocography shows thefetal heart rate to be formally reactive with a base-line of 140 bpm, and the patient reports that she isagain feeling fetal movements. Bimanual exami-nation shows her cervix to be 1 cm dilated and80% effaced. Estimated fetal weight is 4,400 g. Asyou are about to leave, she says: “My sister’s babydied at 41 weeks. Why can’t you induce my labornow, Doctor?” Which of the following statementsare true? (More than 1 statement may be true.)
A. Induction of labor is appropriate, because herpregnancy is post-term.
B. Induction of labor is appropriate to minimizematernal and fetal risks.
C. Induction of labor is appropriate for the indi-cation of impending macrosomia.
D. Induction of labor will not increase her riskof cesarean delivery.
6. A 43-year-old G1P0 presents to your office at 34-5/7 weeks gestation complaining of a severeheadache and flashing lights in front of her eyes.Her supine BP is 140/90 and there is 3+ protein-uria. A diagnosis of preeclampsia is made. Whichof the following statements regarding the manage-ment of preeclampsia are true? (More than 1 state-ment may be true.)
A. She should be delivered immediately bycesarean for a diagnosis of moderatepreeclampsia.
B. You should measure her BP sitting and notlying.
C. You should start antihypertensive therapy inan attempt to improve perinatal outcome.
D. Regional anesthesia is contraindicated.
7. A 36-year-old G6P2 calls the office complainingof no fetal movement for 8 hours. She is at 37weeks gestation. On arrival, you confirm anIUFD. Which of the following statements regard-ing the management of IUFD at term are true?(More than 1 statement may be true.)
A. It is highly likely that a cause for the IUFDcan be identified after delivery.
B. Immediate induction of labor is indicated toprevent coagulopathy.
C. Pathologic examination of the fetus and pla-centa/fetal membranes is the single most use-ful test to identify a cause for the IUFD.
D. A Kleihauer-Betke test should be sent toidentify fetomaternal hemorrhage.
8. An 18-year-old G1P0 presents for her first pre-natal visit. She is complaining of severe morn-ing sickness. On examination, uterine size isgreater than expected for gestational age. Youperform an ultrasound examination and confirma monochorionic/monoamniotic twin gestation.Which of the following complications ofmultiple gestations is specific to monochori-onic/monoamniotic pregnancies?
A. Malpresentation.
B. Twin-to-twin transfusion syndrome.
C. Cord entanglement.
D. Preterm delivery.
9. A 27-year-old G3P1 with a strong family history ofmultiple pregnancy presents for her first prenatalvisit at 12 weeks gestation. Ultrasound examinationconfirms a monochorionic/diamniotic twin preg-nancy. Which of the following statements regardingtwin pregnancy are true? (More than 1 statement may be true.)
CHAPTER 9: OBSTETRIC COMPLICATIONS 255
A. Monozygous twinning is not influenced byepidemiologic or genetic factors.
B. 80% of twin pregnancies are dizygous.
C. Perinatal mortality is higher with monozy-gous than with dizygous twins.
D. Perinatal mortality is highest with monochorionic/monoamniotic twins.
10.A 30-year-old G4P2 presents at 19 weeks gesta-tion with vaginal spotting. She has a history of 2prior cesarean deliveries. Ultrasound examinationreveals a low-lying placenta covering the cervicalos. Fetal well-being is confirmed. Which of thefollowing statements regarding the managementof placenta previa are true? (More than 1 state-ment may be true.)
A. There is a high probability that the placentawill move away from the cervix as the preg-nancy progresses.
B. Given placenta previa and 2 prior cesareandeliveries, the likelihood of placenta acc-reta is 25%.
C. Fetal nonstress testing is indicated after 32weeks, because placenta previa is associatedwith uteroplacental insufficiency and IUGR.
D. Pelvic examination should be deferred in allpatients presenting with antepartum hemor-rhage until placenta previa can be excluded.
Answers
1. C.A history suggestive of cervical insufficiency (ie,acute, painless dilatation of the cervix usually in themid-trimester culminating in prolase and/or PROMwith resultant preterm and often previable delivery) isthe only proven indication for elective cervical cer-clage. If the prior preterm delivery was the result ofpreterm labor and not cervical insufficiency, cerclageplacement is not indicated. Prophylactic cerclage for
DES exposure remains controversial. Most cliniciansbelieve that a history of in utero DES exposure alone(without a history of prior pregnancy loss) is not anindication for prophylactic cerclage placement. Simi-larly, elective cerclage has not been shown to be bene-ficial in women with multiple pregnancies without aprior history of cervical insufficiency.
2. A.The presence of uterine contractions suggests pretermlabor and not cervical insufficiency, and are an abso-lute contraindication to cervical cerclage. Indeed, thepresence of persistent uterine contractions requires theremoval of any cerclage to avoid cervical lacerationand/or uterine rupture. Although intra-amniotic infec-tion is an absolute contraindication to cerclage place-ment, vaginal yeast infection is not. Cervical ectro-pion represents a physiologic extrusion of columnarepithelium out of the cervical canal under the influ-ence of steroid hormones, and should not interferewith cervical cerclage placement. If the fetal mem-branes are found to be prolapsing through the externalos at the time of cerclage placement, the risk of iatro-genic rupture of the fetal membranes may be as highas 50%. Although this is not an absolute contraindica-tion to cerclage placement, the surgeon should pro-ceed with care. A number of techniques have beendescribed in an attempt to reduce the fetal membranesprior to cerclage placement, including Trendelenburgposition, back-filling the bladder, placement of a 30mL Foley catheter or moistened sponge forceps intothe cervical os, and/or therapeutic amniocentesis.
3. D.You should administer antenatal corticosteroids. Asingle course of antenatal corticosteroids decreasesthe incidence of RDS, IVH, and (possibly) NEC by50%, and is recommended for all pregnancies at high-risk of delivering before 34 weeks gestation withintact membranes and before 32 weeks with pretermPROM. Maximal benefit is achieved 24-48 hoursafter the initial dose. This effect lasts for 7 days, but itis unclear what happens thereafter. Repeated coursesof steroids are not generally recommended. Bed rest isrecommended in up to 20% of all pregnancies, with anestimated cost of >$250 million per year in the UnitedStates alone. Despite these recommendations, there isno proven benefit to bed rest in women at risk forpreterm labor. Intravenous hydration is also com-monly recommended in the acute setting, but without
256 OBSTETRICS AND GYNECOLOGY—2009

proven benefit. Broad-spectrum antibiotic therapy hasbeen shown to delay preterm birth and prolonglatency in the setting of preterm PROM < 34 weeks.However, there is no consistent evidence of prolongedlatency in the setting of preterm labor with intactmembranes. As such, broad-spectrum antibiotics arenot recommended for this indication. Pharmacologictocolytic therapy remains the cornerstone of modernmanagement. Although a number of alternativeagents are now available for tocolysis, the only agentthat is approved by the FDA for the treatment ofpreterm labor is ritodrine hydrochloride (which hasbeen off formulary in North America for over 10years, because it is too dangerous to administer inpregnancy). Although the ultimate goal of tocolysis isto delay delivery to term, there is no reliable data tosuggest that any tocolytic agents are able to delaydelivery for longer than 24-48 hours. As such, themost realistic goal of tocolysis is to delay delivery for48 hours to allow administration of antenatal corticos-teroids. No single tocolytic agent has a clear therapeu-tic advantage. As such, the side effect profile of eachof the drugs will often determine which to use in agiven clinical setting. Magnesium sulfate (which actsboth to suppress nerve transmission to uterine smoothmuscle and to lower the concentration of intracellularcalcium within myometrial cells, which is necessaryfor activation of the myosinactin contractile unit) hastraditionally been regarded as the first-line tocolyticagent for use in preterm labor. More recent data sug-gests that nifedipine (a calcium channel blocker) isequally effective and safer, and can be administeredorally. In Europe, the first-line tocolytic agent is atosi-ban, an oxytocin receptor antagonist.
4. B. and C.It is clear from this patient’s history that she is at highrisk of preterm delivery. The screening tests currentlyavailable for prediction of preterm birth fall into 5broad categories:
1.) Risk factor scoring. A number of risk factors forpreterm labor have been identified. However,reliance on risk factors alone will fail to identifyover 50% of pregnancies which deliver preterm,and most women designated at risk will deliver atterm.
2.) Home uterine activity monitoring (HUAM). Anincrease in uterine contractility is a prerequisite forpreterm labor. However, use of HUAM in womenat high risk does not reduce the incidence ofpreterm delivery, but does lead to over-diagnosisof preterm labor, increased obstetric intervention,and increased cost.
3.) Assessment of cervical maturation. Serial digitalevaluation of the cervix is useful if the examina-tion remains normal. However, an abnormal cervi-cal finding (shortening and/or dilatation) is associ-ated with preterm delivery in only 4% of low-riskwomen and 12%-20% of high-risk women. Sono-graphic evaluation of the cervix has demonstrateda strong inverse correlation between cervicallength and preterm delivery. If the cervical lengthis below the 10th percentile for gestational age, thepregnancy is at a six-fold increased risk of deliv-ery prior to 35 weeks gestation.
4.) Biochemical markers. Although a number of bio-chemical markers have been associated withpreterm delivery, only fetal fibronectin (fFN) isestablished as a screening test for preterm deliv-ery. Elevated levels of fFN in cervicovaginalsecretions at 22-34 weeks gestation are associatedwith premature delivery. The real value of this testlies in its negative predictive value (99% ofpatients with a negative fFN test will not deliverwithin 7 days).
5.) Endocrine markers. The detection of elevated lev-els of estriol in maternal saliva (≥2.1 ng/mL) ispredictive of delivery prior to 37 weeks gestationin a high-risk population with a sensitivity of 68%-87%, a specificity of 77% and a false positive rateof 23%. Serial (weekly) measurments may bemore accurate in predicting pretermbirth than asingle measurement. This test is not currentlyavailable in the United States.
5. B. and D.Post-term (prolonged) pregnancy refers to a preg-nancy that has extended to or beyond a gestational ageof 42.0 weeks (294 days) from the first day of the lastmenstrual period. As such, this patient’s pregnancy iscurrently at term, not post-term. Clearly, accuratepregnancy dating is critical to the diagnosis. Post-termpregnancy is associated with both fetal and maternal
CHAPTER 9: OBSTETRIC COMPLICATIONS 257

risks. Perinatal mortality (stillbirths plus early neona-tal deaths) at ≥ 42 weeks of gestation is twice that atterm and increases 4-fold at 43 weeks and 5- to 7-foldat 44 weeks. Chronic uteroplacental insufficiency,asphyxia and intrauterine infection all contribute tothe excess perinatal deaths. Post-term infants arelarger than term infants, with a higher incidence ofmacrosomia (defined as a sonographic EFW >4500g). Complications associated with fetal macrosomiainclude prolonged labor, cephalopelvic disproportion,and shoulder dystocia with resultant risks of orthope-dic or neurologic injury. Post-term pregnancies are atincreased risk of umbilical cord compression fromoligohydramnios, nonreassuring fetal antepartum orintrapartum assessment, meconium aspiration, short-term neonatal complications (hypoglycemia,seizures) and long-term neurologic sequelae. Forthese reasons, there does appear to be a small advan-tage to routine induction of labor at 41 weeks gesta-tion, regardless of parity or method of induction.However, induction of labor for the indication of“impending macrosomia” is not appropriate, and suchan approach has not been shown to decrease cesareandelivery rates or improve perinatal outcome. Routineinduction of labor at 41 weeks will not increase thecesarean rate for multipara and nullipara with a favor-able cervical exam (although the cesarean deliveryrate of primipara with an unfavorable cervical exam islikely to be increased).
6. B.Preeclampsia is a clinical diagnosis encompassing 3elements: 1.) new-onset hypertension (defined as asustained BP ≥140/90 in a previously normotensivewoman); 2.) new-onset proteinuria (>300 mg/24 h or≥2+ on a clean-catch urinalysis in the absence of uri-nary infection); and 3.) non-dependent edema(although this is not a prerequisite for diagnosis). BPshould always be measured in the sitting positionusing the 5th Korotkoff sound (disappearance of pul-sation) to describe the diastolic BP. Preeclampsia isclassified as either “mild” or “severe” (there is nomoderate preeclampsia). This patient has severepreeclampsia by symptoms (headache, visualchanges) and should be delivered immediately. How-ever, immediate delivery need not necessarily meancesarean delivery. Cervical ripening agents may beused if the cervix is not favorable prior to induction,but prolonged inductions should be avoided. Regionalanalgesia can be safely administered in the setting of
preeclampsia (in the absence of thrombocytopenia)with close attention to volume expansion and anes-thetic technique. The use of antihypertensive agents tocontrol mildly elevated BP in the setting ofpreeclampsia has not been shown to alter the course ofthe disease nor to diminish perinatal morbidity ormortality, and may indeed reduce uteroplacental per-fusion. Moreover, the use of such agents may serve toremove the most sensitive index of worseningpreeclampsia. For these reasons, antihypertensivetherapy is not recommended for mild-to-moderatehypertension in the setting of preeclampsia.
7. C. and D.Causes of unexplained IUFD at term can be identifiedin only around 50% of cases. Pathologic examinationof the fetus and placenta/fetal membranes is the singlemost useful test to identify a cause for the IUFD. Fetalkaryotyping should be considered in all cases of fetaldeath to identify chromosomal abnormalities, particu-larly in cases with documented fetal structural abnor-malities. Fetal-maternal hemorrhage occurs in allpregnancies, but is usually minimal. In rare instances,fetal-maternal hemorrhage may be massive, leadingto fetal demise. The Kleihauer-Betke (acid elution)test allows an estimate of the volume of fetal blood inthe maternal circulation and should be sent as soon aspossible since fetal cells are very rapidly cleared fromthe maternal circulation. Intra-amniotic infectionresulting in fetal death is usually evident on clinicalexam. Placental culture and histologic examination ofthe fetus, placenta/fetal membranes, and umbilicalcord may be useful. Immediate delivery is not neces-sary. Overall, >90% of women will go into laborwithin 2 weeks of fetal death. Around 20%-25% ofwomen that retain a dead singleton fetus for longerthan 3 weeks will develop disseminated intravascularcoagulopathy (DIC) due to excessive consumption ofclotting factors. Therefore, delivery should beeffected within this time period.
8. C. Multiple pregnancy should be suspected in women athigh risk, excessive symptoms of pregnancy or uter-ine size larger than expected. Overall, antepartumcomplications develop in 80% of multiple pregnan-cies as compared with around 30% of singleton gesta-tions. Preterm delivery is the most common complica-tion, and the risk of preterm delivery increases as fetalnumber increases. Malpresentation is a common com-
258 OBSTETRICS AND GYNECOLOGY—2009

plication of multiple pregnancies. Cord entanglement,on the other hand, is specific to monochori-onic/monoamniotic pregnancies. Overall, it is a rarecomplication (1 in 25,000 births), but may occur in upto 70% of monochorionic/monoamniotic pregnanciesand is thought to account for >50% of perinatal mor-tality in this subgroup. Twin polyhydram-nios/oligohydramnios sequence results from animbalance in blood flow from the “donor” twin to the“recipient.” Both twins are at risk for adverse events.Twin-to-twin transfusion is a subset of poly/oligosequence seen in 15% of monochorionic pregnancies,and is due to unbalanced vascular communicationsbetween the fetal circulations. Overall perinatal mor-tality is 40%-80%. Treatment options include expec-tant management, serial amniocentesis, indomethacin(to decrease fetal urine output), laser obliteration ofthe placental vascular communications or selectivefetal reduction.
9. All are correct.Of pregnancies with placenta previa, 25% with previaand 1 prior cesarean, and 60% with previa and 2 ormore prior cesareans. Neonatal complications includepreterm birth and malpresentation. However, placentaprevia is not associated with IUGR. Elective cesareandelivery is generally recommended at 36-37 weeksgestation. 80% of twin pregnancies are dizygous(derived from 2 separate embryos). Dizygous twin-ning is influenced by a number of epidemiologic fac-tors, including a family or personal history of multiplepregnancy, advanced maternal age, multiparity,African American, and ART. Monozygous twinning,on the other hand, is a random event that occurs inaround 1 in 300 pregnancies (although the risk may beincreased 2- to 3-fold with in vitro fertilization). Peri-natal mortality is higher with monozygous(30%-50%) than with dizygous twins (10%-20%). Chorion-icity refers to the arrangement of membranes in multi-ple pregnancies. In monozygous twinning, the timingof the cell division determines the chorionicity. If thezygote divides within 3 days of fertilization, the resultis dichorionic/diamniotic placentation (30% of allmonozygous pregnancies); if the division occursbetween day 3 and day 8, the result is a monochori-onic/diamniotic pregnancy (65%); between day 8 andday 13, a monochorionic/ monoamniotic pregnancyensues (<5%); and if the division occurs on or afterday 13, incomplete separation (conjoined twins) is therule (<0.5%). Chorionicity correlates directly with
perinatal mortality, which is especially high withmonochorionic/monoamniotic twins (65%-70%).Chorionicity is determined most accurately by exami-nation of the membranes after delivery. Antenataldiagnosis is more difficult. Identification of separatesex fetuses or two separate placentae confirmsdichorionic/diamniotic placentation.
10. A. and D. Placenta previa refers to implantation of the placentaover the cervical os in advance of the fetal presentingpart. In any patient presenting with antepartum hem-orrhage, pelvic and/or rectal examinations should beavoided until placenta previa is excluded. Placentaprevia is primarily a sonographic diagnosis. Placentaprevia may resolve with time, thereby permittingvaginal delivery. Indeed, only 5% of low-lying pla-centae identified by ultrasound at 14-20 weeks gesta-tion persist to term. Maternal complications includeplacenta accreta, which refers to abnormal attachmentof placental villi to the uterine wall. In the absence ofplacenta previa, placenta accreta is rare. However, itcomplicates 5%-15% of pregnancies with placentaprevia, 25% with previa and 1 prior cesarean, and60% with previa and 2 or more prior cesareans.Neonatal complications include preterm birth andmalpresentation. However, placenta previa is notassociated with IUGR. Elective cesarean delivery isgenerally recommended at 36-37 weeks gestation.
CHAPTER 9: OBSTETRIC COMPLICATIONS 259

260 OBSTETRICS AND GYNECOLOGY—2009