-
Hypersensitivity Reactions
• Gell and Coombs classification:– Type I – IgE mediated
(allergy)– Type II – Antibody-mediated cytotoxic– Type III – Immune
Complex mediated– Type IV – Delayed-Type Hypersensitivity
(DTH)• Types I, II and III are “immediate”• Type IV is
delayed
-
Type I Hypersensitivity
• Antigens are called “allergens”• Unknown why people get
allergies, but there is a
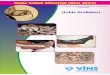
strong genetic predisposition (called atopy)• Hallmark is
inappropriate production of IgE
against allergens that cause mast cell degranulation (see fig
15-2)
• Normally IgE/mast cell activity should be directed against
parasitic infections
-
Type I Hypersensitivity
• Mediators of Type I hypersensitivites– Mast cell granule
contents (early effects)
• Histamine and Heparin - ↑ vascular permeability, smooth muscle
contraction (intestines, bronchi), mucus secretion
• Chemotactic factors – attract eosinophils and neutrophils•
Proteases – mucus secretion, complement activation,
degradation of blood vessel basement membrane
– Later Effects• Leukotrienes and prostaglandins – secreted
after tissue
disruption caused by mast cell degranulation, effects are
similar to histamine
• Arrival of proinflammatory eosinophils and neutrophils
-
Clinical Manifestations of Type I• Systemic anaphylaxis
– Allergen gets into the blood stream– Dyspnea, ↓BP, bronchole
constriction, GI and bladder
smooth muscle contration, shock, death within minutes if
untreated
– Treatment - epinephrine• Allergic rhinitis (hay fever)
– Inhaled allergen triggers reaction in nasal mucosa– Watery
exudate from nose, eyes, upper respiratory
tract, sneeezing and coughing
-
Clinical Manifestations of Type I• Asthma
– Allergic asthma – due to inhaled airborne allergens (pollens,
dust, fumes, etc)
– Intrinsic asthma – triggered by cold, exercise– Reaction
develops in lower respiratory tract– Bronchoconstriction, airway
edema, mucus secretion,
inflammation• Food allergies
– Ingestion of allergen– Vomiting and diarrhea– If allergens are
absorbed into bloodstream, reactions can occur
where allergen deposits• asthma-like symptoms• Urticaria (hives,
wheal & flare response)
-
Clinical Manifestations of Type I
• Atopic Dermatitis (allergic eczema)– Often occurs in young
children– Red skin rash– Strong hereditary predisposition
-
Type I Hypersensitivity• Skin testing
– Potential allergens are injected or scratched into the
skin
– If the patient is allergic a wheal & flare response
occurs
• RIST –radioimmunosorbent test – similar to RIA, non-invasive
way to identify allergies
-
Type I Hypersensitivity
• Treatment– Avoid allergen if possible– Antihistamines, or
anti-prostaglandins– Hyposensitization – injections of low doses
of
allergen may cause a shift from IgE to IgG as the dominant
antibody formed.
-
Type II Hypersensitivity
• Antibody-mediated Cytotoxic HS– Antibodies (IgM or IgG) bind
to cell surface
antigens. Antigen/antibody complex may lead to:
• Complement activation lysis• ADCC• Opsonization
phagocytosis
– These are normal reactions, but when they cause unwarranted
tissue damage, they are considered a hypersensitivity.
-
Type II Hypersensitivity
• Examples of Type II HS:– Transfusion reactions
• To ABO blood groups• To other RBC blood groups
– Hemolytic disease of the newborn (erythroblastosis
fetalis)
– Drug-induced hemolytic anemia (penicillin)
-
Type III Hypersensitivity
• Immune Complex Disease– Antibody (IgG) / attaching to soluble
antigen
leads to complex formation– Immune complexes may deposit in:
• Blood vessel walls (vasculitis)• Synovial joints (arthritis)•
Glomerular basement membrane
(glomerulonephritis)• Choroid plexus
-
Type III Hypersensitivity• Damage occurs due to:
– Anaphylatoxin release due to complement activation (C3a, C5a)
which then attracts neutrophils, and causes mast cell
degranulation
– Neutrophils have trouble phagocytosing “stuck” immune
complexes so they release their granule contents leading to more
inflammation
– Platelet aggregation also results from complement
activation
• These effects are also known as the Arthus reaction
-
Type III Hypersensitivity
• Localized reactions– edema and redness (erythema) and
tissue
necrosis of the affected tissue– Can occur in the skin following
insect bites– Can occur in the lungs
• E.g. “farmer’s lung” from inhaling particles from moldy
hay
-
Type III Hypersenstivity
• Generalized reactions:– Serum sickness (following treatment
with
antiserum to a toxin)– Autoimmune diseases
• SLE• Rheumatoid arthritis
– Drug reactions (penicillin)– Infectious diseases
• Meningitis, hepatitis, malaria, mono etc.
-
Type IV Hypersensitivity
• Delayed type hypersensitivity (DTH)– TH cells that have been
“sensitized” by an antigen
develop a TH1 and (sometimes a TC response) leading to
macrophage recruitment and activation.
– First noticed with reaction to tuberculosis bacteria
(tuberculin reaction)
– Hallmarks of type IV is the large number of macrophages at the
reaction site, and that it takes an average of 24 hrs to manifest
after repeat exposure.
-
Hypersensitivity ReactionsType I HypersensitivityType I
HypersensitivitySlide Number 4Clinical Manifestations of Type
IClinical Manifestations of Type IClinical Manifestations of Type
IType I HypersensitivityType I HypersensitivityType II
HypersensitivityType II HypersensitivityType III
HypersensitivityType III HypersensitivityType III
HypersensitivityType III HypersenstivityType IV
HypersensitivitySlide Number 17