-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
1/20
Treatments for Gestational Trophoblastic DiseaseLaura Kenny,
Michael J Seckl
Expert Rev of Obstet Gynecol. 2010;5(2):215-225.
Abstract and IntroductionAbstract
Gestational trophoblastic disease (GTD) is a relatively rare but
important group of benignand malignant disorders that affect women
of child-bearing potential. Most cases are nowdiagnosed earlier
than previously owing to advances in our knowledge of the disease
andaccuracy of ultrasonography, combined with the high analytical
sensitivity of humanchorionic gonadotrophin assays, although
occasionally patients with metastases present
at a late stage with life-threatening complications. Early
diagnosis and referral to aspecialist center for further management
is vital so that patients can receive the optimalstandard of care.
Patients can be grouped into high- and low-risk categories using
well-established prognostic scoring systems, enabling the minimum
appropriate treatment tobe recommended. Chemotherapy regimens for
the disease are now well established, sothat for the vast majority,
GTD is a curable condition, and patients can be reassured
thatfertility is normally preserved. Regular follow-up by human
chorionic gonadotrophinmeasurement following treatment is important
for the detection of early relapse.Regimens for relapsed disease
are usually successful, but need to be improved for the
infrequent cases that develop multiple drug resistance. In this
article the subtypes of GTD,rationale for treatment, surgery and
drugs used in the condition are discussed.
Introduction
Gestational trophoblastic disease (GTD) spans a spectrum from
two premalignantconditions: partial and complete hydatidiform
moles, to three malignant tumors, namely:invasive mole, gestational
choriocarcinoma and placental-site trophoblastic tumor(PSTT);[1]
the latter three are sometimes referred to as gestational
trophoblastic neoplasia.
Gestational trophoblastic tissue forms from the peripheral cells
of the blastocyst a fewdays after conception. The tissue is divided
into two layers: the outer syncytiotrophoblastcomposed of large
mutinucelated cells and an inner layer of mononucleated cells
thatmigrate out and fuse to form the cytotrophoblast. The
syncytiotrophoblast subsequentlyaggressively invades the
endometrium, generating an intimate connection between thefetus and
the mother, known as the placenta. Normally, the growth of
trophoblastic tissueis tightly regulated by as yet undefined
mechanisms that prevent the development of
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
2/20
distant metastases. Malignant GTD occurs when these controling
mechanisms fail, whichmay result in invasion of trophoblastic
tissue through the myometrium, permittinghematogenous spread and
tumor emboli to form.
The revised International Federation of Gynecology and
Obstetrics (FIGO) classification of GTD was developed in 2000 after
many years of discussion between international expertsin the field,
and is the most appropriate method for categorizing the disease
into high- andlow-risk categories. [2] Successful management of GTD
now means that for the vastmajority of patients the disease is
curable. This has been largely dependent on acombination of
centralized care leading to accumulated knowledge about the
biology,pathology and natural history of the disease. Fertility can
be preserved and normaloutcomes can be expected in subsequent
pregnancies in most cases. [3] The tumors areextremely
chemosensitive; the intensity of treatment is guided by the
prognostic category(which comprises of human chorionic
gonadotrophin [hCG] level, maternal age, length of time elapsed
since previous pregnancy, size of uterine lesion, sites of
metastases andnumber of previous chemotherapy regimens) at the time
of referral. The high sensitivityand specificity of hCG assays
allow the success of treatment to be followed accurately,enabling
the early detection of treatment failure and relapse.
While GTD is a relatively rare diagnosis, higher incidences (up
to one in 300 pregnancies)are seen in certain populations, namely
Brazil, the Philippines and in native AmericanIndians. The
incidence in countries such as Japan appears to be falling,
possibly owing tobetter data collection and reduced dependency on
hospital-based surveys as opposed to
national population data, and possibly owing to dietary
influences. This article focuses onthe Charing Cross Hospital
(London, UK) experience. For a comprehensive review of thegenetic
abnormalities underlying GTD, readers are referred to the paper
published byFisher and Hodges. [4] The various types of hCG assays,
subtypes of GTD, diagnosis,management options, and potential
complications of the disease and treatment will bediscussed.
HCG Assays
-subunit hCG ( HCG) circulates in a variety of isoforms
(hyperglycosylated hCG, nickedhCG, nicked hyperglycosylated hCG,
hCG missing the -subunit C-terminal extension, freea-subunit, free
-subunit, free -subunit missing the C-terminal
extension,hyperglycosylated-free -subunit [ hCG-H] and nicked-free
-subunit) as a result of post-translational modifications (nicked
hCG occurs owing to the action of proteolytic enzymesin the
placental, molar/cancer tissue or in the circulation). [5]
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
3/20
The detection of hCG in normal, early pregnancy is relatively
straightforward, as themolecule is either intact or in the
hyperglycosylated form (hCG-H). However, in cancer,the situation is
more complex, as the assay needs to be sensitive enough to detect
all hCGvariants equally well. The assays that are available
commercially are licensed to detecthCG in pregnancy, but can result
in significant differences in sensitivity when used incancer
patients. Most centers use a commercial assay such as the Siemen
Immulite 1000(Siemens, IL, USA) to measure total hCG; however, no
single hCG test has been approvedfor use in cancer. At Charing
Cross, we use a noncommercial radioimmunoassay (RIA) thatcan detect
a site on HCG that is common to all the known forms of the hormone,
andtherefore does not suffer from false negatives. Our experience
in using the RIA in morethan 35,000 women with GTD has given us
great confidence that we only rarely see falsepositives, and our
comparative work with other assays has shown that our assay
detectsall forms of hCG so far discovered equally, unlike the
commercial assays examined. [6,7]
The false-positive results that can occur with hCG testing are
often due to heterophileantibody production by the patient;
however, these can be excluded by pairedmeasurement of hCG in the
urine and serum as the antibodies are not excreted in theurine. It
should be noted, however, that at low values of real hCG in the
serum, there maybe no hCG detectable in the urine. This problem is
overcome in our RIA by using serialdilutions of the serum; real
hCG, unlike cross-reacting molecules that cause
false-positiveresults, will reduce in accordance with the dilution.
For commercial assays, mostmanufacturer's tests include animal
serum and nonspecific animal antibodies, along withother components
to prevent heterophilic antibody binding, and the incidence of
false-
positive hCG tests has declined. [5] There is a wide variability
between different types of commercial hCG assays with regards to
the sensitivity to detect all 13 dimer and subunitvariants. [6]
RIAs have limited availability outside our center, and for further
informationabout hCG assays, readers are referred to a
comprehensive review on this subject byCole. [8]
The half-life of hCG is 24 36 s, and the amount of hCG produced
corresponds to tumorvolume. Indeed, hCG is still the most valuable
tumor marker available and is moresensitive than any commonly
available imaging technique (a value of 5 U/l corresponds to
a tumor volume of approximately 105
cells[9]
). It is important to remember that hCGproduction is not unique
to pregnancy and GTD; for example, germ cell tumors and 15% of
epithelial cell malignancies also produce the hormone. [10,11]
Partial & Complete Hydatidiform Moles
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
4/20
The incidence of partial moles (PMs) and complete moles (CMs) is
3:1000 and 1:1000 of normal pregnancies, respectively. Genetically
PMs are nearly all triploid and occasionallytetraploid consisting
of both maternal and paternal DNA. In PMs, the uterus is often
notenlarged for gestational age and vaginal bleeding tends to occur
in the second trimester,and occasionally patients present with a
missed or incomplete abortion. [12] In fact, thediagnosis is rarely
suspected until the histology of curettings is available. Clues to
thediagnosis can occasionally be obtained by ultrasound. [13] The
pre-evacuation hCG is over100,000 IU/l at diagnosis in over 90% of
cases. Only 0.5% of PMs require chemotherapyfor postmolar GTD.
[14]
New technologies such as gene-expression microarrays may have a
role in the future forpredicting which patients require hCG
follow-up postevacuation. CMs are nearly alwaysandrogenetic in
origin and result from the fertilization of an ovum lacking
maternal genesby a single sperm, 23X, which then duplicates to form
the homozygote 46XX. [15,16] Veryoccasionally the CM is biparental
in origin, when the maternal nuclear DNA isretained. [17] In 25% of
cases, fertilization can occur by two spermatozoa, resulting in
eitherthe 46XX or 46XY genotype; [18] the 46YY genotype has not yet
been reported in cases of CM.
The classical macroscopic 'bunch of grapes' appearance is
usually seen when CMs presentin the second trimester, and is due to
swelling of chorionic villi. Currently, CMs arenormally diagnosed
in the first trimester when the villi contain little fluid and
present witha threatened abortion or abnormal vaginal bleeding; the
uterus is normally large for
gestational dates. Ultrasound plays an important role in helping
to raise suspicion that apregnancy is abnormal and could be molar,
but in the absence of histology, this imagingmodality is not
diagnostic as reviewed by Sebire and Seckl. [19] Occasionally,
patients maypass grape-like structures or the entire mole. Those
patients with rapid trophoblasticgrowth and extremely high hCG
levels often present with hyperemesis and theca luteincysts (which
may be palpable above the pelvic brim). Previously, patients used
to presentwith preeclamptic toxemia, although this is rarely seen
now owing to earlier diagnosisusing ultrasonography.
Cross-reactivity between hCG and the thyroid-stimulatinghormone
receptor may lead to the development of hyperthyroidism. [20]
The disease can also present at later stages with
life-threatening complications frommetastases owing to a missed
diagnosis; for example, when a spontaneous abortionoccurs at home,
or because full histopathological examination of elective
abortionmaterial is not performed routinely in abortion centers.
The development of a screeningprocedure to avoid subsequent
problems in such centers would avoid thiscomplication. [21] All
patients who have surgery for an ectopic pregnancy should have
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
5/20
material sent for histological analysis to exclude any
underlying molar pregnancy ormalignancy. In many states the in the
USA and Canada, it is a legal requirement that theproducts of
conception are examined by a pathologist; in contrast this is not
mandatory inthe UK, where it is a Royal College of Obstetricians
and Gynaecologists guideline only.Review by an experienced
histopathologist in a recognized center is crucial; this
isespecially true in early pregnancies where the fetal blood
vessels and membranes may stillbe present.
Approximately 16% of patients with CM proceed to develop
malignant disease.Metastases in the pulmonary, cervical and vaginal
regions do occur, but do not mean thatthe mole is invasive, as they
can resolve on the removal of the primary mole. Thedevelopment of
tumor emboli leading to pulmonary metastases can be minimized
byavoiding agents that promote uterine contraction.
Twin pregnancies comprising a normal fetus and hydatidiform mole
do occur inapproximately 1:10,000 1:20,000 pregnancies. Some may
abort in the first trimester andare undiagnosed, or present at the
time of routine ultrasound screening, or may presentas a result of
complications such as bleeding, large for gestational age, or
symptomssecondary to a raised hCG. [22] In our experience at
Charing Cross Hospital, 40% of patientswho choose to continue their
pregnancy result in live births, without increasing the risk of
subsequently requiring chemotherapy for malignant disease. [22]
Invasive Moles/Trophoblastic NeoplasiaThese are definitively
diagnosed on the basis of myometrial invasion on histology.
Thediagnosis may be suspected owing to abnormal ultrasound scan
appearances (large uterusfor gestational age, theca lutein cyst
>6 cm) or plateaued/rising hCG level postevacuationof a mole, or
symptoms such as vaginal bleeding, abdominal distension and pain,
or thosedue to complications. In reality, curettage specimens from
molar evacuation rarely containmyometrium, except in hysterectomy
specimens. The risk of complications is higher inpatients where the
initial diagnosis of molar pregnancy was not made, and are
thereforenot on hCG follow-up. It is important to differentiate an
invasive mole from
choriocarcinoma (see later) and an incomplete abortion. This can
be done by assessing forthe presence of chorionic villi (present in
choriocarcinoma) and p57 immunostaining; asCMs are androgenetic,
only the mitochondrial DNA will stain positive, the rest of the
cellswill be negative.
Choriocarcinoma
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
6/20
Choriocarcinoma is the most aggressive form of GTD owing to
their rapid growth andmetastatic potential. They most commonly
develop after a CM; the incidence of anantecedent history of CM has
been reported in 29 83% of choriocarcinoma cases invarious studies
across the world. [1]
Partial moles and PSTTs rarely give rise to choriocarcinoma.
Choriocarcinomas can occurafter any type of pregnancy usually in
the first year, although in our experience a case of
choriocarcinoma has occurred after an interval of 35 years. The
incidence of choriocarcinoma following term delivery without a
history of CM is approximately1:50,000. The true incidence may
actually be much higher as histology is often difficult toobtain,
but interestingly choriocarcinoma following a full-term pregnancy
is more oftenassociated with aggressive disease. Another classical
presentation that has been describedin post-full-term pregnancy
choriocarcinoma is of secondary postpartum hemorrhage andthe anemic
neonate.
Patients present with symptoms similar to those of hydatidiform
moles, but gynecologicalsymptoms can be absent in up to a third of
cases in those who present withmetastases. [23,24] The disease can
metastasize to any site lungs, brain, liver, skin, heartand cauda
equina. Pulmonary metasases can be parenchymal, pleural or the
result of tumor emboli in the pulmonary arteries. This results in
symptoms of dyspnea, hemoptysisor those of pulmonary artery
hypertension. Cerebral metastases present with convulsions,focal
neurological signs, intracerebral hemorrhage or signs of raised
intracranial pressure.Liver metastases can cause local pain or
referred pain to the right shoulder tip. While
these symptoms or features are not unique to GTD, it is an
important differentialdiagnosis to consider in women of
child-bearing age who present with metastases of unknown primary
origin and can be easily confirmed by serum hCG and tumor
biopsy.The high hCG level can also cause thyrotoxicosis and ovarian
theca lutea cysts.
Infantile and fetal choriocarcinoma has been reported in
approximately 30 cases, both asa secondary from the mother and as a
primary. [25] It appears that the disease can cross theplacenta and
metastasize to the lungs, liver or brain. Treatment is with
cisplatin-basedchemotherapy or excision. A diagnosis should be
suspected in infants with anemia, failure
to thrive, precocious puberty or those as a result of metastases
(e.g., hepatomegaly orhemoptysis). Serum or urine hCG should be
measured in all infants at delivery in maternalcases of
choriocarcinoma, and as the disease can present up to 6 months
postdelivery,consideration should be given to extending the hCG
testing period. [25 27]
Placental Site Trophoblastic Tumor
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
7/20
This is a rare, slow-growing form of GTD that has been proposed
to arise from theintermediate trophoblasts at the implantation
site. [28] They constitute 1% of trophoblasticdisease. PSTT has
been shown to follow term delivery, nonmolar abortion, CM or PM.
[29] Incontrast to other forms of GTD, spread tends to occur late
by local infiltration and via thelymphatics, although distant
metastases can occur. It is important to differentiate fromthe
benign placental-site nodule, which is also composed of
intermediate trophoblastcells. A recent analysis of the entire UK
experience of PSTT has shown that severalvariables, including
number of mitoses per ten high-power fields, hCG level (>4
IU/l), stageand duration from the antecendent pregnancy, are all
important prognostic variables onunivariate analysis. [30] The use
of percentage-free HCG relative to total hCG may beuseful (although
not definitive) for differentiating PSTT from choriocarcinoma and
othertypes of GTD, as this has found to be secreted at a higher
level. [5,31] However, onmultivariate analysis the only prognostic
variable that remains significant is the durationfrom the causative
pregnancy. In a series from our group, women who were more than
48months from the causative pregnancy thus far invariably die
within 6 years of diagnosis of PSTT, while those within 48 months
are nearly always cured. [30]
Like choriocarcinoma, the causative pregnancy may not be the
immediate antecedentpregnancy. [32] PSTT displays a pattern of
vascular invasion, characterized by neoplasticcells migrating
through, and replacing, vessel walls, while maintaining the overall
vasculararchitecture. The tumors are composed mainly of
intermediate trophoblast derived fromcytotrophoblast, and so
produce little hCG. hCG elevation at diagnosis has been found tobe
less than 500 IU/l in over 50% of cases. [33] However, they often
stain strongly for
human placental lactogen and b1-glycoprotein. In contrast to
choriocarcinoma, however,metastases occur late, so the presenting
symptoms are generally gynecological. The mostimportant prognostic
factors for patients with PSTT are stage, myometrial invasion
anddate from antecedent pregnancy (better for those with an
interval
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
8/20
simply represent the differentiating effects of treatment rather
than a separate type of GTD.
It has been proposed that ETT arises from the intermediate
trophoblasts of the chorionicleave. [28] The cells are positive for
cytokeratin, epithelial membrane antigen and inhibin-a,whereas the
trophoblastic markers human placental lactogen, hCG and melanoma
celladhesion molecule are only focally expressed. [36]
Patients are usually of child-bearing age, although a
significant number of cases have beenfound in peri- or
postmenopausal women with a long interval since pregnancy. [38]
Thepresenting signs are vaginal bleeding with a low level of hCG
(
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
9/20
nulliparous cervix is not recommended. Ergometrine is helpful to
minimize bleeding aftersuction evacuation, and the chance of
requiring chemotherapy. If the hCG value falls tonormal then no
further treatment is necessary.
Previously, repeat evacuations in patients with molar
pregnancies were commongynecological practice. This is reasonable
if the initial evacuation was incomplete and thedisease is confined
to the uterine cavity on ultrasound. However, analysis of our data
hasshown that if the hCG is plateaued or rising, unless the hCG is
less than 5000 IU/l, a secondevacuation is very unlikely to be
effective, with approximately 80% of women undergoinga further
evacuation subsequently requiring chemotherapy. [40] Moreover, each
procedurecarries a risk of introducing infection, triggering
hemorrhage and, rarely, uterineperforation. Consequently, second
evacuations should only be performed in rarecircumstances where the
hCG is below 5000 IU/l, the disease is confined to the
uterinecavity and following discussion with a specialist GTD
center. Ultrasound control can aid inthe procedure, giving useful
feedback to reduce the risk of uterine perforation.
Hysterectomy This is indicated for: patients with PSTT or ETT
where the disease isconfined to the uterus (i.e., no evidence on
computed tomography [CT] body/MRI brain orpelvis or [
18F]fluorodeoxyglucose-positron emission tomography [FDG-PET]
scanning); forpatients with invasive GTD who have failed EMA/CO
(which consists of EP, methotrexate[MTX] and actinomycin
alternating weekly with cyclophosphamide and vincristine[formerly
called Oncovin]) chemotherapy, which is confined to the uterus; for
patientswho do not wish to preserve fertility with recurrent
localized GTD; and occasionally for
patients with massive vaginal bleeding. As stated previously,
hysterectomy is preferred forlocalized PSTT as it is relatively
resistant to combination chemotherapy regimens andtends to
metastasize late; however, there have been case reports of cure
with EP/EMA(etoposide and cisplatin/etoposide, MTX and actinomycin
D) chemotherapy. Themanagement of massive (life-threatening)
vaginal bleeding requires a multidisciplinaryapproach between
oncologists, gynecological surgeons and interventional
radiologists.Potential treatment options include hysterectomy or
emergency embolization of theuterine artery. Less severe cases of
vaginal bleeding normally resolve with chemotherapy,transfusion and
bed rest. In addition, we have found that a uterine pack can be
helpful.
Focal Resection of Uterine Disease
There are some women with focal uterine lesions from PSTT who
wish to preserve theirfertility, for whom a fertility sparing focal
uterine resection may be appropriate; however,the multifocality of
the disease can often be difficult to diagnose as it may be missed
byimaging technologies such as ultrasound, MRI and FDG-PET. To
date, this approach hasonly been reported to successfully conserve
fertility in three out of four cases. [41]
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
10/20
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
11/20
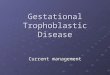
AP MoleAbortion or unknown
Term
Interval (end of AP tochemotherapy in months)
12
hCG IU/l 10 3 104 10 5
Number of metastases 0 1 3 4 8 >8
Site of metastases None, lung,vagina
Spleen, kidney GI tractBrain,liver
Largest tumor mass 5 cm
Prior chemotherapySingledrug
two
drugs
AP: Antecedent pregnancy; hCG: Human chorionic
gonadotrophin.
Figure 1.
Chemotherapy treatment of low- and high-risk gestational
trophoblastic disease.
EMA/CO: see Table 3 for explanation.
CO: Cyclophosphamide and vincristine; EMA: Etoposide,
methotrexate, actinomycin; GTD:Gestational trophoblastic disease;
hGC: Human chorionic gonadotrophin.
Histological evidence of choriocarcinoma
Metastases to brain, liver, GI tract or radiological opacities
above 2 cm on chest x-ray(CXR)
Pulmonary vulval, or vaginal metastases unless hCG falling (in
these cases themeasurement of HCG-H may be useful for determining
the presence of active disease)
Heavy vaginal bleeding, gastrointestinal or intraperitoneal
hemorrhage
Rising hCG postevacuation
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
12/20
Serum hCG above 20,000 IU/l more than 4 weeks postevacuation
(risk of uterineperforation)
Raised hCG 6 months after evacuation even if falling (in these
cases the measurementof HCG-H may be useful for determining the
presence of active disease)
All patients requiring chemotherapy are admitted to hospital for
at least 1 week todetermine whether significant hemorrhage is going
to occur and to deal with any sideeffects. This enables us to
monitor the patients for hemorrhagic or other complications,and
allows time for the patients to become familiar with their
treatment. Patients withlow-risk disease are initially treated at
Charing Cross, but once discharged continuetherapy locally and are
monitored by serial hCG levels at Charing Cross and by
clinicreviews every 6 weeks. Serum hCG levels are checked
twice-weekly during therapy untilthe value normalizes, and then
both serum and urine levels are checked once-weekly untiltreatment
stops 6 8 weeks later and, subsequently, at intervals (the normal
range forserum hCG in our laboratory is 4 IU/l and urine 25
IU/l).
Low-risk PatientsLow-risk patients are treated with cycles of
single-agent MTX 50 mg given byintramuscular injection on alternate
days for four doses, combined with folinic acid (15mg) given orally
30 h post each dose of MTX (). Generally, this treatment is well
tolerated;the potential side effects include mucositis, serositis,
hepatitis and pneumonitis. Mucositis
can be managed by ensuring good oral hygiene and starting the
folinic acid at 24 h post-MTX. Adequate fluid intake (3 l/day) also
helps to prevent against complications. In ourexperience,
significant MTX toxicity occurs in 2% of patients, and this can
warrantswitching to actinomycin D (). MTX can cause significant
delayed photosensitivity;therefore patients are advised to avoid
sun exposure for 1 year following treatment.Actinomycin D tends to
cause more nausea and myelosuppression than is seen with MTX,and
has the additional effect of alopecia.
Box 1. Low-risk gestational trophoblastic disease: first- and
second-line treatment.
Treatment Repeated every 14 days
Low-risk disease first-line treatment:
Methotrexate50 mg by intramuscular injection repeated every 48 h
for a total of four doses
Calcium 15 mg orally 30 h after each injection of methotrexate
(folinic acid)
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
13/20
folinate
Low-risk disease second-line treatment:
Actinomycin D 0.5 mg by intravenous injection daily for 5
days
Box 1. Low-risk gestational trophoblastic disease: first- and
second-line treatment.
Treatment Repeated every 14 days
Low-risk disease first-line treatment:
Methotrexate50 mg by intramuscular injection repeated every 48 h
for a total of four doses
Calciumfolinate
15 mg orally 30 h after each injection of methotrexate (folinic
acid)
Low-risk disease second-line treatment:Actinomycin D 0.5 mg by
intravenous injection daily for 5 days
Methotrexate produces hCG normalization in approximately 67% of
low-risk patientsoverall (i.e., WHO score: 0 6; Charing Cross
prognostic score: 0 8). [42] Drug-resistantdisease is defined as
patients with two rising or plateaued hCG values during treatment.
Inthe study by McNeish et al. , MTX-resistant patients with a hCG
level of less than 100 IU/lwere treated with actinomycin D, and
patients with a hCG above 100 IU/l were treatedwith EMA/CO. Of the
patients who changed to actinomycin D (owing to resistance or
MTXtoxicity), only 6% relapsed after completion of therapy, and for
patients who receivesecond-line treatment with EMA/CO, the
relapse-rate postcompletion is only 1%. [42]
High-risk PatientsOwing to the risk of drug resistance in this
group, patients have been treated since 1979 atCharing Cross with
an intensive chemotherapy regime EMA/CO (). The regimen
ismyelosupressive, but dose intensity can be maintained by using
granulocyte colony-stimulating factors to prevent neutropenia and
neutropenic sepsis, continuing treatmentunless the total white cell
count is less than 2, neutrophils less than 1 and platelets
less
than 75 when dose delays may be required. Patients with liver
metastases are treatedwith EP/EMA chemotherapy (), and may require
a dose reduction depending on liverfunction tests.
Table 3. Etoposide, methotrexate and
actinomycin/cyclophosphamide and vincristinechemotherapy for
high-risk patients.
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
14/20
Regimen Drug Dosage
EMA
Day 1 Etoposide 100 mg/m 2 by iv. infusion over 30 min
Actinomycin D 0.5 mg iv. bolus
Methotrexate 300 mg/m 2 by iv. infusion over 12 h
Day 2 Etoposide 100 mg/m 2 by iv. infusion over 30 min
Actinomycin D 0.5 mg iv. bolus
Folinic acid rescue15 mg orally every 12 h for four doses
(starting 24 h after commencing the methotrexate infusion)
CO
Day 8 Vincristine 1 mg/m 2 iv. bolus (maximum 2 mg)
Cyclophosphamide 600 mg/m 2 iv. infusion over 30 min
For patients with brain metastases the methotrexate dose is
increased to 1 g/m 2 withfolinic acid rescue 30 mg given 8 h
intravenously for 3 days, commencing 32 h after thestart of the
methotrexate infusion. Intrathecal methotrexate 12.5 mg is given on
the COweek provided there is no raised intracranial pressure with
15 mg folinic acid until thehuman chorionic gonadotrophin
normalizes.
CO: Cyclophosphamide and vincristine; EMA: Etoposide,
methotrexate and actinomycin D;iv.: Intravenous.
Table 4. Etoposide and cisplatin/etoposide, methotrexate and
actinomycin Dchemotherapy.
Day Drug Dosage
1 Etoposide 100 mg/m 2 by iv. infusion over 30 min
Actinomycin D 0.5 mg iv. bolus
Methotrexate 300 mg/m 2 by iv. infusion over 12 h
2Folinic acidrescue
15 mg orally every 12 h for four doses (starting 24 h after
commencing the methotrexate infusion)
8 Etoposide 150 mg/m 2 iv. bolus
Cisplatin 75 mg/m 2 iv. bolus
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
15/20
iv.: Intravenous.
There is a risk of respiratory failure in patients with
large-volume lung metastases, or thiscan also occasionally occur
owing to massive pulmonary embolism. Careful attentionshould be
paid to patients' respiratory function, with regular monitoring of
the respiratoryrate and pulse oximetry with arterial blood gases
taken if necessary to check for anychange from baseline after
initiating chemotherapy. Occasionally, we may start treatmentwith
only one or two drugs in patients with very poor respiratory
function to preventperitumoral edema and inflammation that may
occur around tumor deposits in the lungs,and then introduce the
other drugs once the respiratory function has stabilized.Intubation
should be avoided, as the high ventilatory pressures can trigger
fatalintrapulmonary hemorrhage from the friable tumor vasculature;
other strategies that maybe considered are continuous
positive-pressure ventilation or extracorporeal oxygenation.
The cumulative 5-year survival of patients treated with this
schedule is 86.2%, with nodeaths from GTD beyond 2 years after the
initiation of chemotherapy. [43] The earlymortality was due to
respiratory failure, brain metastases, liver failure and
pulmonaryembolism in patients who presented with extensive disease
at first presentation. The factthat previous chemotherapy was a
good prognostic factor (5-year survival 88.9 vs 84.2%)is likely to
be due to patients being on follow-up so that relapse was detected
early, asmost of the deaths in the chemotherapy-naive group
occurred early after the initiation of treatment due to the extent
of disease at the time of diagnosis. [43] The adverse
prognosticfactors were: liver metastases, longer interval from
antecedent pregnancy, cerebral
metastases and term delivery in the antecedent pregnancy. A
total of 83% of women whowere in remission and had
fertility-preserving surgery were able to become pregnant
aftereither MTX or EMA/CO. [44] However, the paper by Bower et al.
shows that treatment withEMA/CO can bring forward the date of the
menopause by 3 years. [43]
The long-term sequelae of this regimen includes an increased
risk of second tumors suchas acute myeloid leukemia (due to EP),
melanoma, breast cancer and colorectal cancer.The overall incidence
of second tumors is estimated to be 1.5-times that of the
generalpopulation. [45]
CNS DiseaseAt Charing Cross, low-risk patients with lung
metastases and all high-risk patients (even inthe absence of lung
metastases) are assumed to be at risk of CNS disease and so
undergoMRI brain scans. If this is negative then the patients are
still considered to be at risk of occult disease and so have a
lumbar puncture to measure the cerebrospinal fluid
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
16/20
(CSF):serum hCG ratio and to give the first dose of intrathecal
MTX (12.5 mg) followed byoral folinic acid 24 h later. If the ratio
of CSF:serum hCG is 1:60 or less then two furtherdoses of
intrathecal MTX are given, usually with the CO arm of EMA/CO
chemotherapy.This completes prophylaxis for potential occult CNS
disease.
Patients with overt CNS disease on MRI, or where the serum:CSF
hCG ratio exceeds 1:60require more intensive therapy. Management of
overt CNS disease is potentiallyhazardous, owing to the risk of
cerebral hemorrhage and death after starting treatment.Despite
this, the long-term survival rate (30+ months) for patients with
brain metastases is80%. [46] The first 3 weeks provide a useful
prognostic indicator; 86 89% of patients whosurvive this period are
cured. [46 48]Early resection of a solitary lesion may be
appropriate inpatients with serious neurological signs. High-dose
dexamethasone (24 mg in divideddoses) can be given to reduce
cerebral edema prior to chemotherapy. The chemotherapyregime is
EMA/CO with a higher dose of MTX (1 g/m 2 given as a 24 h infusion
on day 1)than for patients without brain metastases. Provided there
is no evidence of raisedintracranial pressure, patients at this
center are treated with intrathecal MTX 12.5 mgwith each CO
treatment for three doses only. The use of intrathecal MTX is
controversial,and while used at Charing Cross, is not advocated in
other centers such as Sheffield. [49]
Patients who develop CNS metastases during treatment have a poor
prognosis, as this isindicative of drug resistance. However,
immediate surgery to remove intracerebral lesionsand modified
chemotherapy can be curative in this situation. [47,48]
Stereotacticradiotherapy may have a role to treat isolated lesions
that are inoperable, and which are
present at the end of chemotherapy. Whole-brain radiotherapy, in
our experience, isnever curative and substantially adds to
long-term toxicity, and so is avoided except inrare cases where
palliation is required.
Drug ResistanceHigh-risk patients who develop resistance to
EMA/CO chemotherapy are treated withEP/EMA alternating with 1 day
EMA chemotherapy (see , note the second day of the EMAetoposide,
MTX and actinomycin is omitted to minimize toxicity). The
indications for
changing treatment are similar for those low-risk patients who
change from MTX toactinomycin D; that is, hCG plateau or rise, and
inappropriately slow fall. Alternativechemotherapy regimes for this
patient group and those intolerant of MTX
includepaclitaxel/etoposide alternating with paclitaxel/cisplatin
(), [50] gemcitabine/cisplatin,single-agent paclitaxel and
high-dose chemotherapy using Carbop-EC-T (carboplatin,etoposide,
cyclophosphamide, paclitaxel and prednisolone) or CEM
(carboplatin,etoposide and melphalan) or ICE (ifosfamide,
carboplatin and etoposide) with autologous
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
17/20
bone marrow or peripheral stem cell transplantation. This can
also be complemented bysurgery to remove any residual lesions. Of
this group, 70% will be cured. A study byWang et al. evaluated
paclitaxel/etoposide alternating with the paclitaxel/cisplatin
regimein patients who had failed chemotherapy previously or had
treatment-related toxicity, andfound that the overall survival was
70% (if cisplatin-resistant patients were excluded, and75% for the
two groups, respectively. [51]
Table 4. Etoposide and cisplatin/etoposide, methotrexate and
actinomycin Dchemotherapy.
Day Drug Dosage
1 Etoposide 100 mg/m 2 by iv. infusion over 30 min
Actinomycin D 0.5 mg iv. bolus
Methotrexate 300 mg/m 2 by iv. infusion over 12 h
2Folinic acidrescue
15 mg orally every 12 h for four doses (starting 24 h after
commencing the methotrexate infusion)
8 Etoposide 150 mg/m 2 iv. bolus
Cisplatin 75 mg/m 2 iv. bolus
iv.: Intravenous.
Table 5. Relapse regimen.
Day Drug Dosage
1 Paclitaxel 135 mg/m 2 by iv. infusion over 3 h
Cisplatin 60 mg/m 2 iv. infusion over 3 h
15 Paclitaxel 135 mg/m 2 by iv. infusion over 3 h
Etoposide 150 mg/m 2 iv. infusion over 1 h
iv.: Intravenous.
Surveillance & Follow-upPatients who have an evacuation only
for molar pregnancy are registered and have serialhCG in blood and
urine samples every 2 weeks. This continues until the hCG level
hasnormalized (0 4), following which urine samples are monitored
every 4 weeks. Themonitoring can be discontinued at 6 months
postevacuation if the hCG normalized within
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
18/20
8 weeks postevacuation, or if the hCG falls more slowly,
monitoring can be stopped at 6months postnormalization. A plateau
or rise in hCG levels is indicative of
residual/invasivedisease.
Patients who require chemotherapy are reviewed 6 weeks
postcompletion of treatment(i.e., 12 weeks after hCG levels have
normalized) for a repeat ultrasound scan of pelvis andother imaging
(CXR/CT/MRI if abnormal at baseline). At this point, most women
will havea normal appearance, but a few will have persisting
defects. These are of no consequenceprovided that hCG remains
normal. The hCG levels are then monitored for life as shown in.
Table 6. Human chorionic gonadotrophin follow-up of patients who
have receivedchemotherapy for gestational trophoblastic
disease.
Year Time of follow-up Urine Blood1 Week 1 6 after chemotherapy
Weekly Weekly
Months 2 6 Every 2 weeks Every 2 weeks
Months 7 12 Every 2 weeks
2 Every 4 weeks
3 Every 8 weeks
4 Every 3 months
5 Every 4 months
After year 5 Every 6 months
Contraception & PregnancyThe hormones in the contraceptive
pill are thought to act as growth factors fortrophoblastic tissue.
For that reason, use of the contraceptive pill and
hormone-replacement therapy should be avoided following evacuation
of a molar pregnancy untilthe hCG value has normalized. This also
applies to patients receiving chemotherapy
(where there is an added risk of thromboembolism). A
retrospective study of 611 patientswithin 2 months of molar
evacuation found that oral contraceptive pill users were 2.6-times
more likely to develop recurrent GTD than nonusers. [52] However, a
smallerprospective study by the Gynaecological Oncology Group of
266 patients postevacuationof hydatidiform moles found that there
was no increased risk of relapse using oralcontraception compared
with barrier methods. [53]
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
19/20
We advocate against pregnancy until after the completion of the
surveillance period inthose patients who have had evacuation only,
or 12 months after chemotherapy has beencompleted mainly to avoid
potential teratogenic effects of chemotherapy and
confusionregarding hCG values. If a patient does become pregnant,
it is important for an ultrasoundscan to be performed early to
confirm that the pregnancy is normal. Patients who havehad
evacuation only of their molar pregnancy should have hCG checked at
3 weeks and 3months postdelivery owing to the increased risk of
molar pregnancy. [54]Chemotherapypatients have follow-up
temporarily discontinued during pregnancy until 3
weekspostdelivery.
Treatment with chemotherapy can result in an earlier onset of
menopause. In ourexperience, with single-agent MTX this is by
approximately 1 year, and approximately 3years with EMA/CO.
[55]
PSTT
Patients with PSTT are often cured by hysterectomy if the
disease is limited to theuterus. [33,56,57] In the presence of
metastatic disease we currently use EP/EMA, as PSTTstend to be less
chemosenstive than choriocarcinomas. [30] For this reason, unlike
otherforms of gestational trophoblastic neoplasia where resection
of residual masses appearsto be unnecessary, [58] in PSTT we
recommend the removal of residual masses and a totalabdominal
hysterectomy after completion of chemotherapy. As the disease
representsonly 0.2% of GTD overall, further studies are needed to
optimize its treatment.
Expert CommentaryAll patients with suspected GTD should be
discussed with a GTD center and have theirhistology centrally
reviewed early accurate diagnosis is essential in the management of
this condition. While outcomes have clearly improved over the past
20 years, late and'missed' diagnoses must be avoided to prevent
deaths from this highly treatable disease.One of the key features
in the treatment success of GTD has been the development of
accurate serum and urine hCG measurements to allow clinicians to
follow the diseasecourse and select the appropriate treatment.
However, recent work has shown that care
is required in the interpretation of hCG values obtained from
commercial kit assays owingto the risk of false positives and false
negatives. The most reliable hCG assays for cancershould detect all
hCG types equally well. Currently, the RIA used at Charing Cross
appearsto be very good at this, but there is an obvious need to
develop new assays that can bereadily implemented elsewhere.
-
7/28/2019 Treatments for Gestational Trophoblastic Disease
Cogorno
20/20
The development of centers with experts in the biology,
pathology, biochemistry,radiology, surgery and oncology of GTD,
with access to large databases of patients providean essential
resource for both patients, and referring physicians. There have
beenachievements in international collaborative efforts to
establish a standard of care forpatients with GTD. Further efforts
are necessary to determine the best strategies forpatients with
rarer forms of GTD, drug-resistant disease and management of
cerebralmetastases.
Five-year ViewIn the next 5 years, by assembling an
international database of PSTT, we should expandour knowledge about
this rare variant, helping to identify new prognostic variables
andrefine therapy. We also need to develop new techniques to
distinguish malignant from thebenign moles just after evacuation.
Novel therapeutic approaches are required for those
patients who develop multiple-drug resistance.