Embed Size (px)
Citation preview

14/10/2013
1
GIRO40 8 – 11 October, Edinburgh
Bodily Injury – Where next? Tim Jordan – The MDU
Cherry Chan – Barnett Waddingham
James Turner – The MDU
14 October 2013

14/10/2013
2
14 October 2013 3
Expressions of individual views by members of the Institute and Faculty of Actuaries and its
staff are encouraged.
The information in this presentation is based on our understanding of current taxation law,
proposed legislation and HM Revenue & Customs practice, which may be subject to future
variation.
The views expressed in this presentation by Cherry Chan are those of the presenter.
Questions Comments
Purpose of Presentation
14 October 2013 4
• Long time admirers of the Third Party Working Party
• Compare and contrast Clinical Negligence claims to
Motor Bodily Injury claims
• Wealth of data available on NHSLA claims
• Draw out any insights that will predict future for Clinical
Negligence claims and give insight into future for Injury
claims

14/10/2013
3
Introduction to NHSLA
• The NHS Litigation Authority (NHSLA) was established in
1995.
• Provides indemnity for all claims made against NHS
organisations
• Works to improve risk management practices
• Unlike insurance, claims are met on a discretionary basis
14 October 2013 5
Source: NHSLA Reports
Introduction to NHSLA
• “First, patients who have been injured as a result of
clinical negligence must have access to justice, so that
they can receive proper compensation. Secondly, this
huge area of public expenditure must be kept under
proper control, so that the resources of the health service
are not being squandered unnecessarily on litigation
costs.”
Lord Justice Jackson, 2009
14 October 2013 6
Source: Review of Civil Litigation Costs: Final Report December 2009

14/10/2013
4
Introduction to NHSLA
14 October 2013 7
0
5
10
15
20
25
2008/09 2009/10 2010/11 2011/12 2012/13
£ B
illi
on
s
Financial Year (ended March 31st)
NHS clinical negligence liabilities
CNST Reserve
Ex-RHA Reserve
ELS Reserve
MDU interpretation of NHSLA data
Introduction to NHSLA
• How big is £22 Billion?
14 October 2013 8
Source: Jay Epperhart blog

14/10/2013
5
How does it work?
14 October 2013 9
• CNST is a pay-as-you-go scheme
• Each member’s CNST contribution is determined in the following way:
• The NHSLA Board determines the total amount to be collected based on actuarial analysis of the
estimated value of claim payments in the forthcoming year.
• The total amount to be collected in 2012/13 to cover claim payments and scheme expenses for
CNST is £950m;
• the total amount is then split between members according to their relative risk within the scheme to
determine a basic contribution;
• each member’s basic contribution is adjusted
to allow for:
material favourable or poor claims
experience to date; and
any discount applicable as a result
of the level of Risk Management
achieved by the member.
© NHSLA Annual Report Source: NHS CNST contribution Finance Q and A (1).pdf
Similarities to other liability classes -
PPOs
14 October 2013 10
0
20
40
60
80
100
120
140
160
180
200
2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
No
. o
f P
PO
cla
ims
Settlement Year
NHSLA - Number of PPOs
NHSLA Motor & LiabilitySource: GIRO PPO working party paper 2012 and IUA PPO
Study

14/10/2013
6
Similarities to other liability classes
14 October 2013 11
• February 2012 – NHS Chief Executive
letter regarding promotion of Personal
Injury Services
• August 2013 – Sky News report
suggests still occurring
© Creative Commons
Differences to other liability classes
14 October 2013 12
• Unlike TPI, where fraudulent claims are an issue for
whiplash there seems to be no evidence of fraudulent
claims being reported to the NHSLA
• “We have also strengthened our approach to claims
where claimants exaggerate their symptoms, to ensure
that payments are made only where it is appropriate and
only to those who are entitled to receive compensation.”
Source: NHSLA Annual Report 2012/2013

14/10/2013
7
Differences to other liability classes
14 October 2013 13
© NHSLA Annual Report 2012/2013
12.7% 14.2%12.3% 11.5% 10.6%
33.2%
41.0%39.2%
43.6% 44.3%45.9%
55.2%51.5%
55.1% 54.9%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
2008/09 2009/10 2010/11 2011/12 2012/13
Financial Year
Ratio of legal costs to damages for NHSLA clinical claims closed
% Defence Costs of damages
% Claimant costs of damages
% Total costs of damages
• Steep increase in claimant costs
as percentage of damages
• Defence costs as percentage of
damages
Differences to other liability classes
• Approximately 40% of all those claims received by the
NHS are resolved without a damages payment
• In 2012 around 70% of MDU medical cases were
resolved without a financial settlement with the claimant
• Motor TPI nil proportion – about 18%
14 October 2013 14
Source: NHSLA Annual Report 2012/2013

14/10/2013
8
Claims Reported Frequency
14 October 2013 15
Source: NHSLA, Third Party Motor Working Party, ONS
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
2005/2006 2006/2007 2007/2008 2008/2009 2009/2010 2010/2011 2011/2012
Reported Claims frequency Clinical Vs Motor Third Party Injury claims
NHS LA Claims Freq - LTPS exposure NHS LA Claims Freq - Population exposure
Motor TPI Claims Frequency Linear (NHS LA Claims Freq - LTPS exposure)
The average rate of inflation for the
reported claims frequency by LTPS
exposure is 10.8% shown by the dotted
line
Claims Reported Change Year on Year*
14 October 2013 16
Source: NHSLA, Third Party Motor Working Party, ONS
-40.00%
-30.00%
-20.00%
-10.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
2006/2007 2007/2008 2008/2009 2009/2010 2010/2011 2011/2012
Analysis of claims frequency YoY change
NHS LA Claims Freq - LTPS exposure Change YoY NHS LA Claims Freq - Population exposure Change YoY
Motor TPI Claims Frequency Change YoY

14/10/2013
9
Claims Severity
14 October 2013 17
Source: NHSLA
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
2005/2006 2006/2007 2007/2008 2008/2009 2009/2010 2010/2011 2011/2012
Co
sts
o
f cla
ims
Year
Average cost of paid claims
Total Damages Defence Costs Claimant Costs Linear (Total)
The average rate of inflation for total claim
severity is 10.6% shown by the dotted line
Claims Severity Change Year on Year
14 October 2013 18
Source: NHSLA
-30.00%
-20.00%
-10.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
2006/2007 2007/2008 2008/2009 2009/2010 2010/2011 2011/2012
Ch
an
ge in
c o
sts
o
f cla
ims
Year
Change in Average cost of paid claims (%)
Total YoY Damages YoY Defence Costs YoY Claimant Costs YoY

14/10/2013
10
Compare with Motor Third Party Injury
(TPI)
14 October 2013 19
Source: NHSLA, Third Party Motor and PPO Working Party
-
2,000
4,000
6,000
8,000
10,000
12,000
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
2007/2008 2008/2009 2009/2010 2010/2011 2011/2012 2012/2013
Mo
tor
TP
I
NH
S L
A
Average Cost Per Claim Clinical Vs Motor TPI
NHS LA Motor TPI
Compare with Motor TPI – indexed values
14 October 2013 20
Source: NHSLA, Third Party Motor Working Party
0.000
0.200
0.400
0.600
0.800
1.000
1.200
1.400
1.600
1.800
2.000
2007/2008 2008/2009 2009/2010 2010/2011 2011/2012 2012/2013
Indexed Average Cost Per Claim
NHS LA indexed Motor TPI indexed

14/10/2013
11
Workers’ Compensation – Top 10 US
States
14 October 2013 21
0
200
400
600
800
1,000
1,200
1,400
1,600
0
10,000
20,000
30,000
40,000
50,000
60,000
70,000
2004 2005 2006 2007 2008
Med
ical
On
ly (
$)
Lo
st
Tim
e (
$)
Average workers compensation claim costs – top 10 US states
Lost Time ($) Medical Only ($)
Source: Oliver Wyman “Examining Costs and Trends of Workers’ Compensation
Claims”
The average rate of inflation for medical
costs is 5.6%
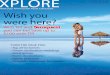
Motor TPI/TPD ratio vs CMC density
14 October 2013 22
Source: “The Isles of Wonder” ,Third Party Working Party GIRO 2012, reproduced with kind permission

14/10/2013
12
Number of clinical claims reported 2011/12
by Post Area by SHA
14 October 2013 23
Interpretation of NHSLA data
Exposure 2011/12
by Post Area by SHA
14 October 2013 24
Interpretation of NHSLA data

14/10/2013
13
Frequency of clinical claims 2011/12
by Post Area by SHA
14 October 2013 25
Interpretation of NHSLA data
Frequency of clinical claims – by SHA
including the number of births (2011/12)
14 October 2013 26
Number of births in
2011/12
Interpretation of NHSLA data

14/10/2013
14
Frequency of clinical claims – by Post
Area
2006/07 2011/12
14 October 2013 27
Interpretation of NHSLA data
Frequency of clinical claims – by
Strategic Health Authority
2006/07 2011/12
14 October 2013 28
Interpretation of NHSLA data

14/10/2013
15
Jackson Reform - background
14 October 2013 29
• Legal Aid, Sentencing and Punishment of Offenders Act
2012
• Aim
– controlling the rising costs of the civil litigation process
– speed up claims settlement
• Main changes
– Methods of funding
– Cost budgeting
Post Jackson comments
14 October 2013 30
Changes Effect Outcome
Success Fee – no longer recoverable
from losing party, cap at 25% of the
claimant’s damages
Lower defendant’s costs if they lose
and put some responsibility to
claimants to control their own legal
costs
Claimants may receive less damages
than before
Risk that lower value claims may no
longer be economic to pursue (is that
fair? )
ATE insurance premiums– no longer
recoverable from losing party except
for expert reports
Controlling the cost of litigation Claimant may have to pay the ATE
premiums up front or fund from their
own fund
10% increase in general damages Compensate for the claimant having
to pay success fee and ATE premium
out of their damages
Claimants may receive less damages
than before
Solicitors may not recover full fees as
before too
Qualified One-way Costs Shifting
(QOCS)
Claimant no need to pay defendant’s
costs if the claim is unsuccessful
No need for ATE premium except for
their own disbursement.
Defendant cannot recoup their legal
fees if they win
Part 36 offers Make both sides consider Part 36
seriously – hope to speed up claims
settlement
See more claimants part 36 offers?

14/10/2013
16
An International Perspective – Annual
Clinical Negligence Payouts
14 October 2013 31
USA
Annual Payout $3.6bn
Population 313.9m
Wales
Annual Payout £46m
Population 3.1m
New Zealand
Annual Payout NZD 106m
Population 4.4m
England
Annual Payout £1.26bn
Population 53.0m
Scotland
Annual Payout £55m
Population 5.3m
Italy
Annual Payout >€10 bn
Population 60.9m
MDU Research, 2013
Approaches Taken in Different
Jurisdictions
14 October 2013 32
• Tort reform: examples - United States and Australia
• No fault schemes: Sweden, New Zealand, FL, WV, under
active consideration in Scotland; has been considered for
UK in late 70s, 90s
• Arbitration: Germany (from 1970s) and France (Patients’
Rights law of 2002)
• NHS Redress Act 2006 sets framework for claims less
than £20,000 but no plans to bring into force in England.
A similar scheme is in force in Wales for claims up to
£25,000 (hospital claims only)

14/10/2013
17
What Could Happen in the UK?
14 October 2013 33
• Law Reform Personal Injuries Act 1948 (S2(4)) means awards
in the UK are made without regard to care that is available
through the NHS
• Tort reform: has reduced costs in US and Australia. Favoured
by the MDOs.
• Caps on damages for future care costs and caps on loss of
earnings?
• No fault schemes:
– effect on costs uncertain. NZ scheme does not look especially cheap; some level
proof still needed
– reduction in legal costs; more open culture
• Change to discount rate?
Summary
• NHSLA liabilities are large and growing
• Nature of future claims costs is uncertain, especially
effect of Jackson reforms
• Basing NHS liabilities on cost of private care per 1948 Act
may be unsustainable
14 October 2013 34

14/10/2013
18
14 October 2013 35
Expressions of individual views by members of the Institute and Faculty of Actuaries and its
staff are encouraged.
The information in this presentation is based on our understanding of current taxation law,
proposed legislation and HM Revenue & Customs practice, which may be subject to future
variation.
The views expressed in this presentation by Cherry Chan are those of the presenter.
Questions Comments