Embed Size (px)
Citation preview

Glycolysis Gluconeogenesis


Pentose phosphate pathway

Glycogen metabolism

Blood Glucose

Blood Glucose
• Fasting blood glucose concentration (blood plasma) (person who has not eaten in the past 3-4 hours)
3.9mmol/L – 6.1 mmol/L 70mg% – 110mg% mean: 90mg%
• It is tightly regulated as a part of metabolic homeostasis.

• Mean normal blood glucose levels in humans are about 90 mg/dl, equivalent to 5mmol/L.
• Glucose levels rise after meals for an hour or two and are usually lowest in the morning, before the first meal of the day.
• Transported via the bloodstream from the intestines or liver to body cells.
• Failure to maintain blood glucose in the normal range leads to conditions of persistently high (hyperglycemia) or low (hypoglycemia) blood sugar.
Blood Glucose

• If blood glucose levels fall below 3 mmol/L (hypoglycemia) this would lead to a loss of consciousness (coma).
• If level goes above 10 mmol/L (hyperglycaemia) glucose will appear in the urine, the pH of the blood would fall and this also leads to coma.
• If cells have inadequate amounts of glucose to catabolize, the cells immediately shift to the catabolism of fats for energy.
• In starvation, proteins are also used for energy after carbohydrate and fats are depleted.
Blood Glucose

Maintaining Glucose Homeostasis• Goal is to maintain blood glucose levels between 70 and 110 mg%.
• The levels of glucose in the blood are monitored by the cells in the pancreas's Islets of Langerhans.
• Two pancreas hormones play important roles in maintaining glucose homeostasis:– Insulin– Glucagon

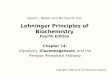
A: Pancreatic islet with exocrine cells. B: Confocal image of an isolated islet immunolabelled for insulin (red), glucagon (green) somatostatin (blue).
cells. (20%) secrete glucagon cells (75%) secrete insulin cells (5%) secrete somatostatin

If the blood glucose level falls to dangerous levels (as in very heavy exercise or lack of food for extended periods), the alpha cells of the pancreas release glucagon.
-- Convert glycogen into glucose (glycogenolysis).
-- Activates gluconeogenesis.
-- The glucose is released into the bloodstream, increasing blood sugar levels.
Glucagan
Glucagan

Proglucagon (158Aa) Glucagon (29Aa)

When levels of blood sugar rise, the pancreas released a different hormone insulin, from beta cells.
-- Causes the liver to convert more glucose into glycogen (glycogenesis).
-- Activates glycolysis but inhibits gluconeogenesis.
-- Bind to insulin receptor and force body cells to take up glucose from the blood through the glucose transporter.
-- Stimulates excess glucose to be converted into fat.
As a result, blood glucose levels drop.
Insulin

Proinsulin Insulin

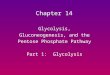
The insulin receptor is a combination of 4 subunits held together by disulfide linkages: two -subunits lying outside the cell membrane and two -subunits protruding into the cell cytoplasm.
Mechanism of Insulin Action

Mechanism of Insulin
• When insulin binds to the -subunit in target tissues, the -subunits in turn become activated.

• Activation of the -subunits triggers a series of reactions that draw the glucose transporter to the cell membrane or regulate metabolism of glucose.
• Cells (liver, muscle, adipose) are now able to increase their uptake of glucose (w/in seconds after insulin binds with its membrane) .
Mechanism of Action of Insulin

Regulating Blood Glucose Levels
• Blood glucose levels rise due to eating a carbohydrate containing meal
– In response, the pancreas releases insulin into the blood to decrease glucose level.
• After the meal is over and blood glucose level begins to fall to a low level:
– The pancreas decreases insulin secretion– Glycogen synthesis in liver is stopped– Glucose uptake by cells from blood is prevented
• If blood glucose levels continue to fall,– Glucagon will be released to increase the release of glucose from
the cells.

Hyperglycemia A condition in which an excessive amount of glucose circulates in the blood plasma (>10 mmol/L or 180 mg/dl),
• Temporary hyperglycemia is often benign and asymptomatic.
• Blood glucose levels can rise well above normal for short periods without producing any permanent effects or symptoms.
• However, chronic hyperglycemia at levels more than slightly above normal can produce a very wide variety of serious complications over a period of years, including kidney damage, neurological damage, cardiovascular damage, damage to the retina etc.

Hyperglycemia
• Exerts high osmotic pressure in extracellular fluid, causing cellular dehydration
• Excess of glucose begins to be lost from the body in the urine: GLYCOSURIA

The following symptoms may be associated with acute or chronic hyperglycemia,
• Polyphagia - frequent hunger, especially pronounced hunger
• Polydipsia - frequent thirst, especially excessive thirst
• Polyuria - frequent urination, especially excessive urination
• Blurred vision
• Fatigue
• Weight loss
• Poor wound healing (cuts, scrapes, etc.)
• Dry mouth
• Dry or itchy skin
• Impotence (male)
• Recurrent infections
• Cardiac arrhythmia
• Coma

Hypoglycemia
• Blood sugar less than 70mg% (3.9mmol/L)
• Symptoms include
– shaking
– sweating
– nervousness
– feeling irritable
– blurry vision or headache
– feeling tired
– Coma

Diabetes mellitus
Diabetes– Greek for siphon or fountain for the characteristic
frequent urination
Mellitus– Latin for sweet as honey. In 1679, a
physician tasted the urine of a person with diabetes and described as sweet
like honey.
A condition in which the body either does not produce enough, or does not properly respond to insulin or both. This causes glucose to accumulate in the blood, often leading to various complications.

Diabetes mellitus
Symptoms:
• Hyperglycemia (high blood glucose)
• Glucosuria (glucose in the urine)
• Polyuria (frequent urination)
• Polydipsia (drinking large amounts)
• Polyphagia (frequent hunger)
• Weight loss
• Acids and ketones in the blood from lipid breakdown (toxic if high)
• Coma if ketones build up
© 2008 Paul Billiet ODWS

Hyperglycemia > Glycosuria>Polyuria>Polydipsia
• Excessive glucose in the kidney filtrate acts as an osmotic diuretic, inhibiting water reabsorption resulting in POLYURIA: huge urine output >>> decreased blood volume and dehydration.
• Dehydration stimulates hypothalamic thirst centers, causing POLYDIPSIA: excessive thirst.

Polyphagia
• POLYPHAGIA: excessive hunger and food consumption, a sign that the person is “starving in the land of plenty.” That is, although plenty of glucose is available, it cannot be used, and the cells begin to starve.
• Without fuel, cells cannot produce energy >> fatigue and weight loss.
• POLYURIA, • POLYDIPSIA, • POLYPHAGIA = The 3 most important symptoms of diabetes
Poor with gold in home

Diabetes Mellitus
• Two main common forms:
– Type 1 diabetes
• Other names:
– “Juvenile” diabetes
– Insulin dependent diabetes mellitus (IDDM)
– Type 2 diabetes
• Other names:
– “Adult onset” diabetes
– Noninsulin dependent diabetes mellitus (NIDDM)

Incidence of Diabetes
• Type 1 Diabetes
– 5-10 % of diabetics
– Onset is generally before age 20
• Average age of onset ~12
• Type 2 Diabetes
– 90-95% of diabetics
– Onset is generally after age 40

Type 1 Diabetes
Results from the body's failure to produce insulin. The majority of type 1 diabetes is of the immune-mediated nature.
• Causes:– Immune-mediated destruction of ß cells
• Genetic component• Immune system destroys beta cells of pancreas
– May also be caused by a viral infection that damages the pancreas.
• Pancreas is unable to make/secrete insulin.– Glucose cannot enter cells– Blood glucose levels rise
• Glucose “spills” into the urine• Water moves into blood
– Frequent need to urinate– Thirsty

Type 1 Diabetes
– Cells use fats and proteins as an energy source, results in:
• Weight loss
• Ketones produced (due to “overuse” of fats for energy) potential for diabetic acidosis
Fat Fatty acids Acetyl-CoA Ketones:
acetoacetate; β-hydroxybutyrate; acetone
The increased ketones in the blood lower the pH of blood, resulting in a form of acidosis called KETOSIS, or ketoacidosis.If too high, ketones are excreted in the urine: KETONURIA.

Type 1 Diabetes
• Treatment
– Insulin shots or pump
– Highly regulate intake of carbohydrates
• Consistent pattern of moderate carbohydrate intake to minimize fluctuations in blood glucose
– Closely monitor blood glucose levels

Type 2 Diabetes
• Results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with relative insulin deficiency.
• Fewer insulin receptors on cells• More insulin is secreted to compensate• Eventually the islet cells cannot keep up with the demand• Less insulin binds to cells
– Glucose enters cells SLOWLY– Hungry– Eat more
• Blood glucose levels remain elevated• Glucose “spills” into the urine• Water moves into blood
– Frequent need to urinate– Thirsty

Type 2 DiabetesPancreas continues to make insulin
• Often in large amounts to compensate for the insulin resistance of cells
• May get to point where pancreas cannot keep up with the body’s needs and insulin is required.
Associated with obesity
• As gain weight, cells make fewer insulin receptors
• Insulin doesn’t bind as well to receptors

Type 2 Diabetes
• Recommendations
– Lose weight
• Even moderate weight loss can help
– Exercise
• Increases number of insulin receptors
• Improves binding of insulin to the receptors
• Helps with weight loss

CAUSES OF TYPE-2 DIABETES
• Two factors especially important in the development of type-2 diabetes:
1) Heredity: About a 5% risk of developing Type II diabetes if mother, father, or sibling has diabetes. Higher risk (up to 50%) if overweight.
2) Obesity: 80% of people w/ Type II diabetes are overweight when diagnosed and symptoms disappear in many of the obese patients when they lose weight.

Type I vs. Type II Diabetes
Type 1 (IDDM) Type 2 (NIDDM)
Age at onset Usually under 40 Usually over 40
Body weight Thin Usually overweight
Symptoms Appear suddenly Appear slowly
Insulin produced None or littler Relative deficiency
Insulin required Must take insulin May require insulin
Other names Juvenile onset diabetes
Adult onset diabetes