Embed Size (px)
DESCRIPTION
The Psychological Effects of Trauma: Implications for Working with Homeless Populations Brian E. Lozano, Ph.D. Contributing Collaborator: Peter Tuerk, Ph.D. Ralph H. Johnson VA Medical Center Homeless Outreach Meeting Columbia, SC July 23, 2014. Goals of Presentati on. - PowerPoint PPT Presentation
Citation preview

The Psychological Effects of Trauma: Implications for Working with
Homeless Populations
Brian E. Lozano, Ph.D.Contributing Collaborator: Peter Tuerk, Ph.D.
Ralph H. Johnson VA Medical Center
Homeless Outreach MeetingColumbia, SCJuly 23, 2014

Goals of Presentation
To facilitate trauma-informed care with homeless populations through better understanding of:
• Normal reactions to trauma
• Genesis and maintenance of PTSD
• Relation of trauma to homelessness
• Barriers to service utilization
• Approaches for overcoming barriers to service utilization
• Effective treatment of PTSD

Psychological Trauma
• What is your understanding of trauma and PTSD?
• Psychological trauma stems from potentially traumatic events that overwhelm the usual methods of coping that give people a sense of control, connection, and meaning.
• Exposure to trauma can severely change the way persons think about themselves and experience the world around them: safety, trust, benevolence, justice, sense of self.

NORMAL Post-Trauma Reactions (not pathological: 1-4 weeks)
• Most people will experience trauma-related symptoms following exposure to trauma or series of traumas. But most people will get better with simple support, obtained from family, friends, and community.
• Just because someone goes through something horrible doesn’t mean they need treatment.
• Treatment is appropriate for those who still have problems 4-12 weeks later.

Posttraumatic Stress Disorder (PTSD)
• PTSD is classified as an Anxiety Disorder in the DSM-IV.
• Exposure to traumatic event involving:
1. Real or perceived threat of life/injury to self/others
AND
2. Intense fear, horror, or hopelessness
• It is a complex disorder that can occur following extremely stressful or traumatic events (e.g., MVA, rape, natural disasters, combat exposure).

PTSD: DSM-IV
Exposure to trauma results in:
1. Re-experiencing symptoms (at least 1)• Recurring intrusive thoughts, images, nightmares of trauma event• Severe anxiety in response to reminders of the event • Flashbacks
2. Avoidance symptoms (at least 3)• Avoidance of thoughts, feelings, conversations, or reminders related to event • Inability to recall important aspects of the trauma event• Emotional numbing/detachment, isolation, decreased interest in activities
3. Hyperarousal symptoms (at least 2)• Physiological reactivity when exposed to trauma reminders • Irritability/angry outbursts, difficulty falling/staying asleep, difficulty concentrating,
exaggerated startle• Hypervigilance – constantly scanning people and surroundings

Prevalence of PTSD • General population
• Men: 2% current; 4% lifetime• Women: 5% current; 10% lifetime(Kessler et al., 2005 -National Comorbidity Survey-Replication)
• Veteran populations• US/Vietnam: 9% current; 19% lifetime (Dohrenwend, 2006)
• US/Gulf War: 3-16% (Sutker et al., 1993; Wolfe et al., 1999)
• US/Iraq & Afghanistan: 12-13% (Hoge et al., 2004)

Time Course of Post-trauma Reactions
Trauma
1month
3months
6months
20years
40years
Acute stress disorder
Acute PTSD
Chronic PTSD
Delayed-onset PTSD
Acute stress reactionAcute stress reaction

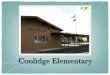
Rate of Recovery After Rape
W 3m 9m Years
94%
47%42%
25%-15%?% with PTSD
Symptoms
Data from Rothbaum et al., 1992
12m
30 %

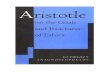
One Year Course: Type of Assault and PTSD
1 wk* 1 mo 2 mo 3 mo 6 mo 12 mo0
102030405060708090
100
Rape
Non-Sexual Assault
% w
ith P
TSD
Foa, Hembree, and Dancu (2003)*Month duration not met

Comorbidity with PTSD
Anxiety• Nervousness (racing heart, muscle tension)• GI upset & other Physical Problems• Impaired Concentration & Memory that imitate organic
problems• Sexual Dysfunction• Avoidance of previously enjoyable activities
Panic Disorder• 3-4x more likely among persons with PTSD (Kessler et al.,
1995)

Comorbidity with PTSD
Depression• Guilt / Self-Blame• Feelings of Worthlessness / low self-esteem• Loss of confidence • Problems with memory/concentration• Eating and Sleep Difficulties• Exacerbation of Physical Problems• Lack of Energy and Motivation• Isolation / withdrawal
Substance Abuse• Increased risk of alcohol and drug abuse/dependence• 2-4x more likely among persons with PTSD

Summary of Reactions to Trauma
• The majority of trauma victims recover with time.
• PTSD represents a failure of natural recovery.
• After one year, PTSD does not remit without treatment.
• PTSD is highly distressing and debilitating disorder.

Trauma, PTSD, and Homelessness
• Among veterans, presence of a mental health disorder is the strongest predictor of homelessness following military discharge (Department of Veterans Affairs Office of the Inspector General, 2012).
• PTSD was associated with 85% increased risk of recurrent homelessness among formerly homeless veterans (O’Connell et al., 2008).
• Among women, those who served in the military were 3x more likely to experience homelessness (Gamache et al., 2003).
• Homeless female veterans were 3x more likely to have received treatment for MST (Washington et al., 2011).

Trauma, PTSD, and Homelessness
• In general population, trauma exposure and subsequent development of PTSD often occurs prior to becoming homeless (Goodman et al., 1991; North & Smith, 1992).
• Homelessness presents increased risk of exposure to trauma (Perron et al., 2008; Williams & Hall, 2009).o Increased risk of criminal violence and nonviolent crimeo Detachment from support systems
• Along with comorbidity with substance use disorders there can be an increased tendency to engage in high-risk behaviors making one susceptible to trauma exposure (Fischer & Breakey, 1991).

Barriers to Service Utilization
• Lack of awareness of resources• Limited resources available• Limited understanding re: trauma• Not enough time to address trauma• Disagreement about target for
intervention• Difficulty coordinating across
services• Discomfort with assessment of
trauma
• Lack of awareness of resources• Overwhelmed by multiple
comorbidities • Limited insight re: symptoms• Hopeless that situation can improve• Disagreement about target for
intervention• Negative reporting experiences
(particularly for sexual assault)• Guilt, shame, mistrust• Minimization of symptoms• FEAR• Ambivalence
What are the most frequent barriers to service utilization that you have noticed?
Patient Barriers Provider / System Barriers

As health care providers, it is important for us to…
• Maintain awareness of and routinely screen for trauma and related symptoms
• Ensure privacy and confidentiality re: communications• Convey confidence in assessment and discussion re: trauma• Understand our own emotional state• Be able to tolerate emotional distress (within self and patients)• Focus on establishing positive rapport and trust• Be empathic and non-judgmental • Normalize reactions to trauma• Be mindful of physical space, body language, tone/volume of
voice, and potential trauma-related triggers
Overcoming Barriers to Service Utilization

As health care providers, it is important for us to…
• Actively elicit patient’s concerns and perspective on symptoms• Communicate understanding through reflective listening• Respect and promote patient autonomy• Align with and emphasize patient’s values and strengths• Recognize that avoidance is normal – it’s a symptom and therefore
expected!• Accept that repeated efforts at engagement will likely be needed• Communicate hope and confidence re: capacity to overcome
challenges through treatment• At the very least, we can keep the door open!
Overcoming Barriers to Service Utilization

Effective Therapy for PTSD
• Prolonged Exposure (PE; Foa et al., 2007) and Cognitive Processing Therapy (CPT; Resick & Schnicke, 1996) – identified as front-line treatments (VA/DoD, 2010).
• Institute of Medicine (2007) identifies exposure therapy as the only effective treatment for combat-related PTSD.
• Randomized controlled trials demonstrate slightly more favorable outcomes for veterans in PE as compared with CPT (Steenkamp & Litz (2013).

What is Prolonged Exposure Therapy?
Prolonged Exposure is a manualized, 90-min, weekly, treatment protocol that consists of the following major components:
• Education regarding common reactions to trauma & detailed rationale for treatment.
• Self-assessment of anxiety using subjective units of distress (SUDs).
• Repeated in vivo exposure to situations avoided due to distress.
• Repeated, prolonged imaginal exposure to traumatic memories followed by processing or discussion of the memories.

Clinical Outcomes: Prolonged Exposure for PTSD
PTSD Checklist (PCL) and Beck Depression Inventory-II (BDI) outcomes over the course of treatment (N = 65 OEF/OIF Veterans with PTSD).
Self-rated PTSD Symptoms Self-rated Depression Symptoms

Clinical Outcomes: Prolonged Exposure for PTSD
Self-rated PTSD Symptoms Self-rated Depression Symptoms
OEF/OIF Veterans

Clinical Outcomes: Prolonged Exposure for PTSD
A quarter (25%) of treatment completers used mental health services once or not at all in the year following treatment.
The need for mental health service utilization decreases by 50% for Veterans completing PE treatment (N=60)