Embed Size (px)
Citation preview

Health Care, Development and Fiscal Policy in Brazil
Pedro Jucá MacielBrazilian National Treasury – Ministry of Finance
Visiting Scholar at Stanford Center for Latin American Studies
April, 26 th 2010The opinions expressed and arguments employed herei n
do not necessarily reflect the official views of th e Brazilian National Treasury – Ministry of Finance

2Agenda
1. Motivation 1: Health and Development
2. Motivation 2: Health Care and Fiscal Policy Agenda
3. Brazilian Unified Health System (SUS)3. Brazilian Unified Health System (SUS)
4. Hospital Sector Performance
5. Policy Recommendations

3
Motivation 1: Health and DevelopmentDevelopment

4Motivation 1: What is the Importance of Health for Development?
1) “Health Promotion is the process of enabling people to increase their control over improvements in their environment to reach a state of complete physical, mental, and social well being.” [WHO (1986)].
2) Health market failures such as imperfect competition(pharmaceutical industry, health insurance and hospitals), externalitiesamong other development indicators or contagious diseases and informational asymmetryjustify public intervention in this sector (Most governments apply many regulations over private sector and have a key role in providing this public good).
3) World Bank (1999): “[Brazilian] health care system known for inefficiency and inequity, and a population that is exposed to a variety of endemic diseases.”
.
and a population that is exposed to a variety of endemic diseases.”
4) Health is the sector that pushes down Brazilian Human Development Index:
Life expectancy at birth (Health)
Adult literacy rate (Education)
Gross enrolment ratio (Education)
GDP per capita (Income)
(years) (% ages 15 and above) (%) (PPP US$)1. Norway (0.971) 1. Japan (82.7) 1. Georgia (100.0) 1. Australia (114.2)
1. Liechtenstein (85,382)
73. Dominica (0.814) 79. Latvia (72.3) 69. Viet Nam (90.3) 38. Germany (88.1) 77. Saint Lucia (9,786)74. Grenada (0.813) 80. Algeria (72.2) 70. Arab.Emirates (90.0)39. Poland (87.7) 78. South Africa (9,757)75. Brazil (0.813) 81. Brazil (72.2) 71. Brazil (90.0) 40. Brazil (87.2) 79. Brazil (9,567)76. Bosnia (0.812) 82. Mauritius (72.1) 72. Myanmar (89.9) 41. Liechtenstein (86.8) 80. Macedonia (9,096)77. Colombia (0.807) 83. Honduras (72.0) 73. Lebanon (89.6) 42. Japan (86.6) 81. Colombia (8,587)182. Niger (0.340) 176. Afghanistan (43.6) 151. Mali (26.2) 177. Djibouti (25.5) 181. Congo (298)
Table 1: Brazil’s Human Development Index 2007
Human Development Index
Source: Human Development Report 2009

5Motivation 1: What is the Importance of Health for Development?
.
• Health has a complex role over the development process due to its relationships (causality runs in both directions) with other sectors such as education, income (e.g. poverty) and environment (e.g. sanitation facilities).
Health EducationHealth Education
IncomeEnvironment
Development

6Motivation 1: What is the Importance of Health for Development?
.
[Todaro and Smith (2009)]
• Health is an important factor in school attendance.
• Healthier children are more successful in school and learn more efficiently.
• Deaths of school-age children increase the cost ofeducation per worker.
• Longer life raise return to investments in education.
• Healthier individuals are more able to productively
.1) Health Education
[Todaro and Smith (2009)]
• Many health programs rely on skills learned in school.
• Schools teach basic personal hygiene and sanitation.
• Education is needed for the formation and training ofhealth personnel.
1) Education Health
It is hard to measure!
• Healthier individuals are more able to productivelyuse education at any point in life.
2) Health Income
3) Health Environment
[Thomas et al (2006)]
• Healthier men are more likely: (i) working well(ii) sleep less, (iii) lose less work time due to illness, (iv) able to conduct physically arduous work, (v) psycho-social healthier is better
• Increase economic productivity.
• Definition of poverty is based on a basic consumption bundle (minimum daily calories).
• Wealthier individuals can enjoy a diversified food base and present a better nutritional standard.
• Income is a key issue to access promptly to: (i) better medical facilities; (ii) health personnel and (iii) medicines.
2) Income Health
3) Environment Health• Healthier societies reduce Ev. contaminations through bacterial, parasitic and virus diseases.
• Reduces chances of epidemic problems.
• Clean air, water and food are key elements for a better health standard.• Access to sanitations facilities reduces significantly health diseases.

7
.
• Most primary health indicators are showing significant improvements:
• Life Expectancy in Brazil rose 10.1 years in comparison to 1980.
• Average growth rate is 0.36 (year of life per year) and it has shown a constant behavior since 1980.
• Life expectancy of women is 7.6 years more than men. In 1980, it was 6 years. (This is a very good topic for the social security reform!)
Life Expectancy in Brazil (1980 - 2008)
60
65
70
75
80
Ano
s de
Vid
a
Brazilian Primary Health Indicators: Facts and Trends
Under-5 Mortality Rate (Deaths per 1000 live births )
• Under-5 mortality rate has declined considerably since 1990 from 47.1 per 1000 to 19.3.
• This fall comes mostly from the Northeast (the poorest region) which reduced its mortality to 1/3 of the 1990’s level.
• However, there is still a considerable regional inequality where the Northeast presents a mortality 2.1 times higher than the South.
55
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
Total Homem Mulher

8
.
• Most primary health indicators are showing significant improvements:
• Almost all one year olds in Brazil are covered by the immunization system.
• Meningococcal conjugate (MCV), three doses of diphtheria tetanus toxoid and pertussis (DTP3) and three doses of Haemophilus influenzae type B (Hib3) vaccines cover more than 98% of the kids.
• Three doses of Hepatitis B vaccine (HepB3) needs to increase 5% coverage to reach all population.
Prevalence of Undernourishment in Total Population
One-Year-Olds Immunization Coverage (%Total Kids) - Brazil
60%
65%
70%
75%
80%
85%
90%
95%
100%
Brazilian Primary Health Indicators: Facts and Trends
Source: FAO Database (2010)
• Prevalence of Undernourishment in the Brazilian population has reduced considerably in the last 10 years from 10% to 6%.
• Brazil performed better than Latin American Countries. In 2004-2006, the difference became 2% of total population.
• The situation in the Near East and North Africa is worst than in the last 26 years. Sub-Saharan Africa, which is the poorest region in the world, reduced its prevalence by 4% in the last 10 years.
Prevalence of Undernourishment in Total PopulationFAO Division Statistics
0
3
6
9
12
15
18
21
24
27
30
33
36
1990-1992 1995-1997 2000-2002 2004-2006
in P
erce
ntag
e
Asia and the Pacific Latin America and the Caribbean
Near East and North Africa Sub-Saharan Africa
Brazil
60%
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
MCV DTP3 HepB3 Hib3Source: WHO

9Brazilian Primary Health Indicators: Facts and Trends
.
• World Bank (1999) explains these improvements by: (i) increase in purchasing power, (ii) maternal education, (iii) access to health care, (iv) community infrastructure and (v) individual behavior.
• Average income of the poorer populations has increased in the last 5 years.
• Both the poverty and extreme poverty rates are declining sharply, leading to improvements in the population’s nutritional status and access to better housing facilities (sanitation).
• IPEA (2010) projects “the end of extreme poverty in Brazil” in 2014.
Poverty and Extreme Poverty in Brazil% of the Population (1980 - 2008)
15%20%25%30%35%40%45%50%
% P
opul
atio
n
Income Inequality in Brazil: Theil and Gini
Source: IPEAData
Source: IPEAData
• Reductions in poverty didn’t only come from an increase in national income, but also from a better division of its resources.
• Both Theil and Gini Indexes have fallen significantly since 2002.
0%5%
10%
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
Poverty Extreme Poverty
Income Inequality in Brazil: Theil and Gini Indexes (1980 - 2008)
0.5
0.55
0.6
0.65
0.7
0.75
0.8
0.85
0.9
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
Gini Index Theil Index

10Health and Development: There’s a lot left to do
.
• Although there have been improvements, Brazil’s historic lack of investments in human capital means there’s a lot left to do…
World Infant Mortality Rate (Deaths / 1000 live births)
Source: 2006 Revision of the UN World Population Prospects Report.

11
..
• Brazil still has a lower life expectancythan most Latin American countries.
• Nicaragua has a 1/4 of Brazilian GDP per capita and has a better indicator.
• Regional Inequality (2000):
MA: 63.9 yrs (white) and 61 yrs (black)
SP: 72.3 yrs (white) and 69 yrs (black)
• World comparison: Difference in life
Health and Development: There’s a lot left to doLife Expectation vs GDP per Capita in LA (2007)
COS CHI
HND
GUY
SUR
GTM
SALPAR
NICBRA
COLPERVEN
ECU
BLZ
ARGMEXPANURU
67
68
69
70
71
72
73
74
75
76
77
78
79
80
Yea
rs
Life Expectancy vs. GDP per Capita in LA (2007)
expectancy between Brazil and most developed countries is 10 years!
Source: World Bank
Source: OECD Brazil Outlook 2009
BOL65
66
0 2000 4000 6000 8000 10000 12000 14000 16000USD $ PPP

12
• According to the 2006 Human Development Report, half of the world's hospital beds are occupied by patients suffering diseases associated with inadequate provision of water and sanitation!!!
• Investments in water supply infrastructure can lead to savings in hospitals.
• Maranhao, Piaui and Acre provide just 62% of their population with access to drinking water.
Population with access to Drinking Water (%) – Brazil (2007)
Health and Development: There’s a lot left to do
Population with Access to Drinking Water (%) 1995 - 2007
• There was considerable improvement in the Access to Drinking Water indicator, mostly in the Northeast. However there is still a lot to do (1/4 of the population!)
• North Region shows a stable trend around 75% of the population.
• It seems that Southern States in Brazil almost completed population’s universal coverage.
1995 - 2007
50%
60%
70%
80%
90%
100%
1995 1996 1997 1998 1999 2001 2002 2003 2004 2005 2006 2007
Centro-oeste Norte Nordeste Sul Sudeste
Source IPEAData

13Population with Access to Sewerage System (%) – Brazil (2007)
Health and Development: There’s a lot left to doSanitation Facilities vs GDP per Capita in LA
(2006)
CHLURU
COS
ARG MEXSUR
SALECU
PAR
GUA
GUYBRA
COLPER
HON PAN
NICBOL
50
60
70
80
90
100
0 2000 4000 6000 8000 10000 12000 14000USD $ PPP
% U
rban
Pop
.
Source: World Bank
• Brazil has a lower percentage in the urban population with access to sanitation facilities than most Latin American countries.
• !There are 5 states with sewerage coverage for just 25% of the population!
• The sewage system seems to be one of the most important infrastructure challenges that Brazil must face in the medium run.
Source IPEAData
USD $ PPP
Population with Access to Sewerage System (%) 1995 - 2007
30%
40%
50%
60%
70%
80%
90%
100%
1995 1996 1997 1998 1999 2001 2002 2003 2004 2005 2006 2007
Centro-oeste Norte Nordeste Sul Sudeste
!!!!
Source IPEAData
Source: World Bank
Source IPEAData

14
.
Maternal Mortality Ration (100.000 live births) in 2005
Brazil, a Transition (Health) Economy: Risk Factors• Maternal Mortality in Brazil is higher than American regional average.
• Infant Mortality (<1yr): Infectious and parasitic di seases (under-development health indicator) have declined over last decade. Problems originated in the pregnancy period and congenital problems have increased their share.
Source: World Health Statistics 2009

15Brazil, a Transition (Health) Economy: Risk Factors
.
Mortality Indicator: Distribution of Death Causes i n Brazil (2005)
• Infections and parasitic diseases represented 4.6% of Brazilian mortality in 2005.
• Diseases associated with circulatory systemare the major cause of deaths in Brazil – 28.3% in 2005.
• Obesity replaced malnutrition as a health problem in Brazil. According to IBGE (2004), the Brazilian underweighted population reached 4% of total. The overweight counts for 40,6% of the population in which 11% are considered obese.
• Prevalence of current tobacco use among adults(>= 15 years) is 17.5% [PNAD (2008)]: prevalence in males represents 22% of total and in females 13%. According to Inca (2006), tobacco consumption is the most important isolated factor for deaths: 45% coronary heart diseases, 85% severe obstructive pulmonary diseases, 25% of brain stroke and 30% of cancers.

16Brazilian Health Care: Society and Violence
.• “External Cause” death is the 3rd major cause of death in Brazil. In average, Murder represents 41% of the “external causes” deaths.
• According to IBGE (2009), murders in Brazil offset partly the gains of infant mortality reduction(life expectancy) because it affects mostly youths.
• Rodrigues et al (2007) estimated the cost of violence to the Brazilian Health System in R$ 2.2 bi (USD 1.4 bi) in 2004. This value represented 15% of the federal investment in Education that year.
External Cause: Percentage of Murders in Total “External Cause” Deaths for Males(2000 and 2005)External Cause: Percentage of Murders in Total “External Cause” Deaths for Males
Source: Indicadores Sociodemograficos e de Saude do Brasil – IBGE (2009)

17Health Inequalities in Brazil
• Health inequality measures how health indicators vary among population groups by income distribution. Inequality remains high because the gain accrues disproportionally to those who already enjoy better health.• In Latin America, only Guyana and Ecuador present higher health disparities than Brazil. According to WHO (2000): “the objective of a good health [system] is really twofold: the best attainable average level – goodness – and the smallest feasible differences among individuals and groups – fairness. A gain in either one of these, with no change in the other, constitutes an improvement”.
Health Inequalities: 2000 World Health Report

18
Motivation 2: Health Care and Government’s Fiscal Policy
AgendaAgenda

19Public vs. Private Provision in the Health Care System1) Public Sector spends 48% of total resources allocated to health care on:
- Emergency Assistance and Hospitals– R$ 27.4 bi (FederalBudgetary Project 2010). - Prevention and Basic Services in Health– R$ 10.0 bi (Federal Budgetary Project 2010).- Drugs/Medicines Provision– R$ 4.9 bi (Federal Budgetary Project 2010).- Disease Surveillance and Control– R$ 2.7 bi (Federal Budgetary Project 2010).- Research and Development- R$ 0.4 bi (Federal Budgetary Project 2010).
2) Although the Private Sector represents 52% of total health care spending, the Public Sector plays a key role in regulating it.- Private Health Insurance (21% population): Agencia Nacional de Saude Suplementar (ANS)- Pharmaceutical Industry: Agencia de Vigilancia Sanitaria (ANVISA)- Food and Sanitary Guidelines: Agencia de Vigilancia Sanitaria (ANVISA)
Source: OECD Economic Survey: Brazil (2009)
Distribution of Brazilian Health Expenditure by Sou rce (2006)
Private, 52%
Public, 48%

20Brazilian Spending on Health: International Comparison• Brazil spent 7.5% of GDP in Health Care in 2006. This number is close to the average of OECD countries and higher than Latin American Countries which spend 7% of GDP.
• As other Latin American countries, the share of private sector in total spending is higher than OECD countries.
• Keep in mind: Brazilian society is younger than OECD countries.Health Care Sector will pressure public accounts as soon as Brazilian society becomes older. Ferraz (2006) estimates health spending, as a percentage of GDP, will increase to 12% in 2025, if the current level of health system inefficiency continues.
Source: OECD Economic Survey: Brazil (2009)

21In fact, Brazilian Demographic Profile is Changing Fast!
Source: IBGE – Projecao da Populacao 1980-2050 (2008 Review)

22Public Spending: Importance of Health Care in 20081) Health Care is the third largest sector of public spending in Brazil. It
accounted for 14% of the public sector budget in 2008.
2) Investments in sanitation (sewage/water) represent only 1% of the budget.
Brazilian Public Sector Expenditure (By Sectors)
Social Security, 30.9%Urbanism, 3.4%
Labor/Work, 2.4%
Defense, 2.2%
Others, 8.7%
Source: Secretariat of the National Treasury (2009)
30.9%
Education, 14.3%Administrative,
6.4%
Judiciary, 4.9%
Public Security, 4.0%
Transportation, 3.9%
Social Assistance, 3.7%
Health, 14.0%

23Who is Responsible for Health Care Provision?1) Total Public Sector spending on Health Care (functional classification) was 4.9% of
GDP in 2008.
2) Each Government Level has the same importance (in terms of resource managed) for health care provision.
3) After Federal Transferences, each Government Level manages almost the same amount of resources for the health sector: 1.7% of GDP.
4) Brazilian Health System is highly decentralized. Federal Government collects 50% of the health earmarking revenues and transfers the majority to states and municipalities.
Public Expenditure in Health All Levels
Source: Brazilian Department of the Treasury (2009)
Public Expenditure in Health All Levels 2008 (% GDP)
Municipalities, 1.7%
States, 1.6%
Federal, 1.7%
Total = 4.9% GDP

24Brazilian Primary Health Indicators: Facts and Trends
. • Sanitation infrastructure (Saneamento) and Health are complementary services. According to 2006 Human Development Report, half of the world's hospital beds are occupied by patients suffering diseases associated with inadequate provision of water and sanitation.
• Sanitation infrastructure spending represent less than 0.5% of GDP. This amount has shown stable trend during the last 6 years.
• Health spending (in relation to GDP) shows an upward trend. It increased from 3.7% (2002) to 4.8% GDP in 2008.
• Observed improvement in the access to health system is due to more public investment in this sector.
Expenditure in Health and Sanitation (sewerage/wate r) % GDP Brazilian Public Sector
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
5.5%
% G
DP
2008.
• Health care expenditure share increased from 12% in 2002 to 14% in 2004 due to the Emenda Constitucional (EC) n. 29 (2000) which requires Federal, State and Municipal Governments to reach a minimum allocation in the health sector before 2004.
• There are different interpretations for what is considered health expenditure in EC 29 regarding sanitation investments. Federal government doesn’t consider investment in Sanitation a health expenditure under EC 29. Some states do. This topic is still under discussion in the Congress. Source: STN (2009)
Source: STN (2009)
0.0%
0.5%
2000 2001 2002 2003 2004 2005 2006 2007 2008
Health Sanitation Total
Proportion of Health and Sanitation (sewerage/water ) Expenditure in Total Public Sector Expenditure (% Total)
0.0%1.0%2.0%3.0%4.0%5.0%6.0%7.0%8.0%9.0%
10.0%11.0%12.0%13.0%14.0%15.0%16.0%
2000 2001 2002 2003 2004 2005 2006 2007 2008
% T
otal
Exp
endi
ture
Health Sanitation Total

25
Fairness of Financial Contribution to Health Systems: 2000 World Health Report
• Fairness of financial contribution index is based on the fraction of household’s capacity to spend (income minus food expenditure) that goes to health care (including tax payments, social insurance, private insurance and out of pocket payments).
• Brazil is one of the least fair (financial) systems in the world! Poorer populations pay relatively more for health care services than higher income families.
Fairness of Financial Contribution to Health Care System

26• As an essential need, the poorest population - income less than two minimum wages (=<2 S.M.) – spends proportionally more in health services than the richer social classes.• Consequently, public provision of health care services can promote progressive impacts over income distribution.
Families Financial Contribution to Health Care System
25%
20%
Families Spending on Health Care by Income Distribution (2003)
Source: World Bank (2004)
Brazil North Northeast Southeast South Mid-West
15%
10%
5%
0%
Source: FUNSALUD (2007)

27• Regarding all health care spending categories, poorer populations spend proportionally more on drugs/medicine suggesting that Drugs Provision Programs (such as Farmacia Popular) potentially improve income distribution in Brazil.
100%
80%
60%
Families Spending on Health Care by Category and Income (2003)
Families Financial Contribution to Health Care System
40%
20%
0% Total =<2 SM 2-3 SM 3-5 SM >=30 SM
Drug/Medicine Insurance Emergency Hospitals OtherSource: FUNSALUD (2007)

28
Unify Health System(Sistema Unico de Saude – SUS)(Sistema Unico de Saude – SUS)

29Sistema Unico de Saude: a Historical Perspective 1930 to 1960 (Vargas’s Model):- Health care became part of Social Security System (Institutos de Aposentadorias e Pensoes - IPA) managed by work unions (only associated workers used to enjoy public health).
1960 to 1980 (Military Regime): - New Social Law unified all IPAs in a single regime for all formal workers (CLT), excluding rural workers and public servants. - For this sudden demand increase for public health care, Government hired private sector to provide this service. This is the period that private sector network raised sharply.
1980 to 1990 (Re-democratization and Constitution):- Establishment of the universal right to health care (SUS). Moreover, Government implemented policies towards institutional restructuring, decentralization to the state level and mechanisms for policies towards institutional restructuring, decentralization to the state level and mechanisms for social participation.
1990 to 1996 (Consolidation – SUS):- Consolidation of the unified system, municipalizationof services delivered, implementation of financial mechanisms through Federal Funds decentralization.
1996 to 2006 (Re-orientation):- Reorientation of health care model towards basic care, separate institutional roles, enact legal and regulatory changes.
Recent Policy “Pacto Pela Saude” (Act launched in 2006) :- Agreement between Federal and Subnational Governments towards: (i) clear definition of the responsibility of each level (municipalities became the final responsible for the health service provision); (ii) establishment of guidelines for decentralization, funding, regional unified planning, regulation and social participation.

30• SUS (Unified Health System): was created in 1988 by the Brazilian Constitution
which assured that health care is a universal right that should be provided by the Public Sector.
• Beneficiaries:
(i) 79% of Brazilians use regularly SUS.
(ii) 21% of the population (mostly high income families) has private insurance. However, in some occasions, they use SUS for procedures (usually complex) which private insurance doesn’t cover.
Sistema Unico de Saude: Understanding the System
• Social Participation: all states and municipalities must have “Health Councils” (represented by users, suppliers, health managers and professionals) which is responsible for the control of health polices in their jurisdiction.
• Roles:Federal government provides major funding source for the SUS and also formulates national policies. States and municipalities are responsible for the policy implementation.
• Decentralization(“Pacto pela Saude 2006”):municipalities are the final responsible for the health care provision in their jurisdiction. If a municipality doesn’t have all health services available, they are allowed to negotiate (consortium) with other municipalities in its region to provide this service.

31Sistema Unico de Saude: Understanding the System • Medicines Provision:(i) Basic: provided by the municipalities and states health secretariats;
(ii)Strategic(associated with a specific national program): provided by the Federal Government;
(iii)Exceptional(high cost or associated with continuous treatments): provided by the states and municipalities and reimbursed (80% in average) by the Federal Government.
• Funding: Constitutional Amendment n. 29 established a minimum expenditure value for health services:
(i) Federal: amount of the previous year plus increase based on the Nominal GDP growth rate.
(ii) States: 12% of total revenues.
(iii) Municipalities: 15% of total revenues.(iii) Municipalities: 15% of total revenues.
• Transferences from Federal Governmentare divided into 5 categories:(i) Basic Health System (Atencao Basica); (ii) Medium and High Complexity Coverage; (iii) Health Surveillance (Vigilancia em Saude); (iv) Pharmaceutics Provision; (v) SUS Management.
• Transference Criterions and Payment:• Basic Health: minimum amount (piso) based on the population of the jurisdiction. Federal
government provides more funding at the time that municipality joins/accepts Federal Programs such as Saude da Familia.
• Hospitals and Emergency Services:payments are based on the service provided by hospitals in SUS network (public or private). Ministry of Health defines the value ($) that will be paid for each service (schedule of payments). There is also a limit for payments in each region based on the population and epidemiolog profile and the health care network.

32• Pregnancy Care indicators:
• Brazil has the second highest Birth by Cesarean Section ratein the World (41.3%).
Brazilian Basic Health Care Coverage: Pregnancy
.Births Attended by skilled health
Personnel (%)Prenatal Care Coverage (%): at
least 1 visitNumbers of
Consultations2000 2003 2006 Growth Rate
2006/2000
None 4.93 3.21 2.18 -56%
From 1 to 3 11.56 10.12 8.59 -26%
From 4 to 6 37.47 35.59 33.85 -10%
More than 7 45.97 51.08 55.38 20%
SUS - Prenatal Care Consultation (1996-2006)
Source: Ministério da Saúde/SE/Datasus - Sistema de Informações Hospitalares do SUS
Cesarean Section ratein the World (41.3%). Much higher than high income countries average 26.8%. [WHO (2009)]
• Prenatal care system in Brazil is above average of American countries in both indicators: (i) births attended by skilled personnel and (ii) at least one prenatal consultation.
• SUS – Prenatal Care Consultation data reveals that 55% of pregnant women had more than 7 consultations in 2006. This number has improved throughout the decade.
Source: World Health Statistics 2009

33Brazilian Primary Health Care Coverage: Infectious Diseases
.
• Tuberculosis, Dengue and Malaria still need better policies.
Antiretroviral Therapy Coverage among people with advanced HIV infection (%)
Tuberculosis Treatment Success under DOTS (%)
• HIV policies in Brazil (treatment and pharmaceutical supply) have been successful.
• Malaria: according to WHO, there were 458,000 cases in Brazil in 2007. It is one of the world leaders.
• Tuberculosis: Brazilian treatment performance is below America’s average rate (72%).
• Dengue: since 2004 dengue incidence • Dengue: since 2004 dengue incidence has increased.
Dengue Incidence: Cases/100k inhabitants

34• Saude da Familia Program (PSF) aims to organize and orient Basic Health Care System in Brazil.
• PSF are composed of teams of Health Care Professionals who visit households and provide teams are composed of a physician, nurse, nurse auxiliary and six or more “community agents”.
• Since 2000, Oral Health teams have been included in the program composed of a surgeon dentist, dental hygienist and auxiliary.
• According to PNAD 2008, PSF covers 51% of Brazilian population (most in the poorest states).
Good Experience in Primary Health Care: Saude da Familia
Proportion of Households Registered in PSF- 2008
Brazilian population (most in the poorest states).
• PSF became the main entrance of the poorest population into the Brazilian Health System.
• PSF concentrates its efforts in the poorest households in Brazil, reducing health inequalities.
• Program covers 64% of the households with no or less than ¼ minimum wage and 16% of the richest category.
Brazil North Northeast Southeast South MidwestNo income to 1/4 Minimum Wage 64,2 54,0 72,8 50,5 58,0 55,7
Between 1/4 and 1/2 Minimum Wage 62,4 58,3 72,0 52,5 58,5 57,4
Between 1/2 and 1 Minimum Wage 54,6 51,8 66,6 45,0 58,2 56,3
Between 1 and 2 Minimum Wages 45,1 46,8 58,5 36,1 54,1 51,7
Between 2 and 3 Minimum Wages 35,3 44,1 46,8 27,9 44,5 41,5
Between 3 and 5 Minimum Wages 26,5 38,0 36,2 19,7 34,7 33,1
More than 5 Minimum Wages 16,3 34,1 23,6 11,3 21,4 19,8
Total 47,7 51,0 64,8 35,9 50,3 49,1
Proportion of Households Registered Programa Saude da Familia (PSF) in Relation to the Total Households of Each Income Category.
Programa Saude da Familia Coverage
Household Income Category

35Sistema Unico de Saude: Size and Coverage • SUS number of consultations reached 480 millions. Most are concentrated in the Southeast whose average consultations/inhabitants is 2.86.
• North region has less consult./inhab. 2.15, however this region has shown a higher growth rate (62% between 1995 and 2007).
• Between 2003 and 2007 many states had a decline of consult./inhabitants. Ministerio da Saude (2008) justifies this behavior due to the effects of the program Saude da Familia.Families are receiving their first health orientation through PSF team visits.
SUS - Consultation per Inhabitants (1995 - 2007)
1.2
1.4
1.6
1.8
2
2.2
2.4
2.6
2.8
3
Con
sulta
tion/
Inha
bita
nts
through PSF team visits.
• This a positive side effect of PSF on public accounts. It is cheaper to give first orientation (consultation) through PSF than in Hospitals.
Growth Rate 1995 / 2007
Region 1995 1999 2003 2007 1995 1999 2003 2007 North 14,893 18,720 25,181 33,013 1.33 1.54 1.83 2.15 62% Northeast 86,683 94,711 111,880 119,214 1.93 2.05 2.27 2.28 18% Southeast 172,134 187,700 216,981 230,841 2.6 2.69 2.88 2.86 10% South 48,105 50,664 62,023 68,143 2.08 2.07 2.38 2.47 19% Midwest 23,158 23,621 29,828 35,207 2.25 2.11 2.42 2.6 16% Brazil 344,974 375,417 445,893 486,418 2.21 2.29 2.52 2.57 16%
Source: Ministério da Saúde/SE/Datasus - Sistema de Informações Ambulatoriais do SUS (SIA/SUS)
Number Consultations (in Thousands) Consultations/Inhabitants
SUS - Consultation by Region (1995 - 2007)
1
1995 1999 2003 2007
North Northeast Southeast
South Midwest Brazil

36Health Care Sector: Hospitalization• Not only number of hospitalizations, but also beds/inhabitants indicator have declined over the last 12 years in Brazil (most from Private Sector).
• This fact can lead to re-arrangements in the number of hospitals within municipalities and regions to improve their scale economies (reducing average cost).
Growth Rate 1995 / 2007
Region 1995 1999 2003 2007 1995 1999 2003 2007 North 760 931 918 1,000 6.81 7.67 6.66 6.52 -4% Northeast 3,691 3,590 3,445 3,222 8.21 7.76 6.98 6.17 -25% Southeast 4,759 4,558 4,435 4,371 7.18 6.52 5.88 5.42 -25% South 1,887 1,995 1,884 1,842 8.16 8.16 7.24 6.67 -18% Midwest 725 876 953 894 7.06 7.81 7.74 6.62 -6%
SUS - Hospitalization by Region (1995 - 2007)
Number Hospitalizations (in Thousands) Hospitalization/1000 Inhabitants
Region
1999 2005 1999 2005 1999 2005
North 1.02 1.07 1.22 0.78 2.24 1.85
Northeast 1.07 1.03 1.66 1.24 2.74 2.27
Southeast 0.76 0.68 2.26 1.76 3.03 2.44
South 0.68 0.55 2.63 2.21 3.31 2.76
Midwest 0.99 0.96 2.48 1.66 3.46 2.62
Brazil 0.87 0.81 2.09 1.60 2.96 2.41
Hospital Beds p/1.000 Inhabitants by Region
Fonte: IBGE - Pesquisa Assistência Médico-Sanitária
Public Bed p/1.000 hab Private Bed p/1.000 hab Total Beds p/1.000 hab
Midwest 725 876 953 894 7.06 7.81 7.74 6.62 -6% Not Mentioned 824 - 3 - Brazil 12,646 11,951 11,638 11,330 8.12 7.29 6.58 5.98 -26%
Source: Ministério da Saúde/SE/Datasus - Sistema de Informações Ambulatoriais do SUS (SIA/SUS)

37Sistema Unico de Saude: Size and Coverage
Region Growth Rate 1995 / 2007
Growth Rate 1995 / 2007
1995 1999 2003 2007 1995 1999 2003 2007North 0.81 0.84 0.97 1.10 36% 0.07 0.10 0.14 0.16 129%Northeast 0.50 0.57 0.63 0.74 48% 0.08 0.09 0.09 0.11 38%Southeast 0.49 0.59 0.68 0.88 80% 0.11 0.13 0.13 0.15 36%South 0.46 0.55 0.61 0.73 59% 0.08 0.09 0.10 0.12 50%Midwest 0.50 0.61 0.71 0.81 62% 0.08 0.10 0.11 0.12 50%Brazil 0.50 0.59 0.68 0.84 68% 0.10 0.11 0.12 0.13 30%
Source: Ministério da Saúde/SE/Datasus - Sistema de Informações Ambulatoriais do SUS (SIA/SUS)
SUS - Diagnostic Procedures per Medical Consultation (1995 - 2007)
Pathological and Clinical Examinations/Consultation
Imaging Examinations/Consultation
• Examinations per consultations is one of the factors that affects the quality of hospital diagnoses in the Health Care System.
• Pathological and clinical examinations increased 68% in the last 12 years. South Region has the lowest indicator.
• DataSUS reveals an increase of 30% in imaging examinations between 1995 and 2007.
• Imaging indicator shows high inequality among regions. Southeast has 36% more imaging examinations per consultations than Northeast. This fact is partially justified by differences in the supply of imaging scanners across regions (next slide).

38SUS: Investments in Imaging Diagnostic Technology • Brazil has the lowest relative supply of imaging diagnostic technology of all OECD countries.
• Supply of X-ray, magnetic resonance and computed topographic scanners are less than the minimum requirement from Ministerio da Saude (MS) in NO and NE.
• Mammography and ultrasound scanner supplies are above MS recommendation.
• Private sector total
Ratio of Recommended vs. Available Scanners Supply
Source: IBGE Indicadores de Saude 2009
• Private sector total equipment supply (30,000) is larger than public 9,000.
• However, public sector has a higher investment growth rate 23% (2002/2005) than private sector 7.7%.
• Just 35% of private scanners are available for SUS

39Where the money is going: The Causes of Hospitalization.• Pregnancy and childbirth are the main causes of hospitalization.
• Respiratory and Circulatory Systems are important groups of diseases. Prevention policies such as blood pressure control and tobacco consumption discouragement may reduce their numbers.
• North and Northeast still presents high level of hospitalization due to sanitation problems (Infectious and Parasites). As long as water/sewage system expands, these hospitalizations numbers may decline.
• Cost of violence in the health sector is expressed in the “External Causes” category. SUS - Proportion Hospitalization by Region According to Group of Diseases (2007)
Groups of Diseases North Northeast Southeast South Midwest TotalInfectious and Parasites 12,89 11,67 5,20 6,10 7,93 8,08Neoplasms 3,57 4,82 6,26 7,12 5,00 5,65Mental 0,51 1,98 2,96 3,65 2,73 2,56Circulatory System 5,79 7,73 12,04 12,96 9,55 10,22Respiratory System 14,42 13,51 11,85 17,09 15,43 13,68Digestive System 8,32 8,30 9,16 9,09 8,68 8,79Genitourinary System 7,40 6,70 6,65 6,10 7,79 6,73Pregnancy and Child Birth 28,73 26,40 20,18 15,56 20,07 21,94External Causes 7,10 6,13 8,40 7,07 7,50 7,35Others 11,28 12,76 17,30 15,25 15,32 14,99
SUS - Proportion Hospitalization by Region According to Group of Diseases (2007)
Source: Ministério da Saúde/SE/Datasus - Sistema de Informações Hospitalares do SUS - SIH/SUS

40Health Care Sector: Labor Market• Many developing countries have a shortage of health care personnel. This doesn’t seem to be the case in Brazil.
• Brazil’s number of Health Sector Personnel/1000 Inhabitants is better than the average in higher middle income countries (except for physicians).
• There are studies identifying the low rate of nurses/physicianas a problem in the Brazilian Health labor market. Recent health care labor market data shows this is no longer a problem.
• Between 1997 and 2007, the numbers of nurses, nurse auxiliaries and nurse technicians increased 141%, 123% and 606%, respectively. This fact made possible technicians increased 141%, 123% and 606%, respectively. This fact made possible this indicator convergence to internationals standards.
Personnel / 1000 Inhabitants
PhysiciansNursing and Midwifery
Dentisty
Low Income Countries 0.4 1.0 0.1
Lower Middle Income C. 1.0 1.5 0.1
Higher Middle Income C. 2.2 4.2 0.6
BRAZIL* 1.7 6.6 1.2
High Income C. 2.7 8.6 1.0
International Health Labor Market
Source: World Health Statistics 2009 and Ministerio da Saude.* Based on Ministerio da Saude Data
Personnel / 1000 Inhabitants
1997 2002 2007Growth
Rate 2007/1997
Physicians 1.35 1.46 1.74 29%Dentists 0.64 0.93 1.16 81%Nurses 0.39 0.51 0.94 141%Nurse Technicians 0.35 0.70 2.47 606%Nurse Auxiliary 1.42 2.26 3.16 123%Nutricionists 0.15 0.15 0.20 33%Farmaceutics 0.35 n/a 0.55 57%
Health Care Labor Market (1997-2007)
Source: Ministério da Saúde/SGTES/DEGERTS/CONPROF - Conselhos

41Brazilian Health System: 2000 WHO Evaluation
Responsiveness of Health Systems: 2000 World Health Report
• Responsiveness includes two major components: (a) respect for individuals (including dignity, confidentiality and autonomy of individuals and families to decide about their own health) and (b) client orientation (including prompt attention, access to social support networks during care, quality of basic amenities and choice of provider).
• In 2000 (the last WHO evaluation), Brazil had the third lowest value in Latin America for the Responsiveness of Health System. We have improved, however there is still lots of for improvement…
Source: World Bank (2004)

42
Hospital Sector PerformanceHospital Sector Performance

43Importance of Studying Hospitals• According to La Fogia and Couttolenc (2008), hospitals are a critical part of the government’s budget, absorbing nearly 70% of public spending on Health.
• Many studies point to problems associated with the organization, cost and quality of hospital services.
• According to Ministerio da Saude (2004), there is significant unmet demand for medium and high complex services. This demand will pressure hospital’s available resources on the time that governments try to improve health care coverage.
• Brazilian Hospital Sector is complex in terms of ownership, size and funding.
• There are more private (57%) than public hospitals (42%). Most public hospitals are directly managed by Federal, State and Municipal governments (Adm. Direta). Regarding private hospitals, almost ½ are non-profit (highly dependent on SUS transferences).
Source: Ministerio da Saude (2004)

44Hospital Funding Network• Most hospitals in Brazil receive funding from diverse sources. National Health Fund is the main source in Brazil (directly or indirectly).
• About 70% of private hospitals receive public funding. SUS-contracted nonprofit hospitals operate under an arrangement that requires at least 60% of their beds for SUS patients.
Source: La Forgia and Couttolenc (2008)

45Problems in Hospital Sector: Management and Efficiency• La Fogia and Couttolenc (2008) state that organizational arrangements make significant differences in hospital performance in Brazil.
•Payment mechanisms create no incentives for quality improvements (future slide)
•Hospitals under direct administration display a rigid structure that limits managers to manage staff, reorganize departments or reconfigure services. Many managerial functions are centralized at higher administrative levels (Secretariats), combined with rigid public service rules and lack of information.
• Efficiency score measures the relationship between resources received (inputs) and services provided (output). Direct Administration Hospital has an average score less than 0.3!!! in a scale from 0 (inefficient) to 1 (most efficient in Brazil).
Source: La Forgia and Couttolenc (2008)
Efficiency Score (DEA) for Hospitals with more than 50 beds (Scale: 0 - 1) - 2002

46
Comparison of OSS and Direct Administration Hospitals: Quality and Efficiency Indicators Sao Paulo State (2003)
Problems in Hospital Sector: Management and Efficiency• The highest efficiency scores belong to Organizacoes Sociais de Saude (OSS), public hospital structure on experience in Sao Paulo (even better than Private Sector).
• La Forgia and Couttolenc (2008) suggests 5 key elements for the success of OSS: autonomy, flexible human resource management, strategic purchasing, contract enforcementand a robust information environment.
Source: Costa e Mendes (2005) in La Forgia and Couttolenc (2008)

47• SUS payments are based on “schedule payments” for a listed health procedures.
• SAS/MS (2004) recognizes that “the resource allocation model adopted [in Brazil] relies almost solely on production of services, overestimates high complexity over cognitiveprocedureswith no link toother aspects such as relevanceand qualityof the provided services”.
• International experience shows that there is no perfect health care provider payment mechanism (PPM), however, it is coming more often adjustpayments to diagnosesand for case severity(as in United States).
• Imbalance between SUS schedule payments and their costs results in overemphasis on few profitable services. According to La Forgia and Couttolenc (2008), SUS PPM is the main driver to (i) financial crisis in nonprofit hospitals sector; (ii) provide overlapping services or
Problems in Hospital Sector: Payment Mechanisms
driver to (i) financial crisis in nonprofit hospitals sector; (ii) provide overlapping services or submit fraudulent coding to raise revenues; (iii) specialize in lucrative treatments and (iv) seek lump-sum bailouts from local governments.
SUS Schedule Payments vs. Cost of Procedures (2002)
Source: Dias, Couttolenc and de Matos (2004) in La Forgia and Couttolenc (2008)

48• SUS financial allocation is based on population, epidemiologic profile and network coverage. Network coverage criteria carries historical spending patterns that not necessary revels the real need of the population and also maintains previous regional distortions.
• Ministerio da Saude (2004) recognizes an “incipient control over the hospitals services productions, in terms of quantity and quality, which doesn’t permit analysis of their adequacy in relation to the population needs…”.
• International experience shows a tendency of health care allocation oriented toward the population’s demand for services.
• Brazilian budgetary allocation creates no incentive to decrease excess capacity observed in small (and most inefficient) hospitals.
Problems in Hospital Sector: Budgetary Allocation
Hospital Spending by Line Item (2002)
Source: La Forgia and Couttolenc (2008)

49• We observe a positive relationship between hospital size and efficiency in Brazil.
• Most small hospitals face difficulties with (i) their own economic sustainability and (ii) their role in the health care system. Many hospitalizations are inadequate, unresolved and not necessary. Usually they duplicate hospitalizations in medium/large hospitals and/or compete with basic care programs. [Ministerio da Saude (2004)]
Problems in Hospital Sector: System Organization
Efficiency Score (DEA) for Hospitals by Bed Size
• Smaller hospitals are associated with lower quality services and higher mortality rates.
• However, they are still important for emergency assistance (especially in small municipalities).
Source: La Forgia and Couttolenc (2008) Source: Ministerio da Saude (2004)
Source: Couttolenc (2004) in La Forgia and Couttolenc (2008)
Coronary Bypass Surgery: Operations and Outputs by Hospital Size (1995)

50Problems in Hospital Sector: Quality of Services • A possible measurement of structural quality involves the state of buildings and infrastructure in hospitals. Facility inspections found disturbingly few facilities in compliance with licensing registration.• Accreditation programs are important instruments to develop and implement continuous quality improvements, however there are no incentives in Brazil to complete requirements for accreditation [La Fogia and Couttolenc (2008)].
Physical Conditions in Sao Paulo Hospitals (2003)
• Patient record keeping is a key organizational element for better attendance and to avoid duplicate diagnoses ($ savings). Only 20% of hospitals in SP have appropriate records!
Source: CREMESP (2004) in La Forgia and Couttolenc (2008)
Adequacy of Record Keeping in Hospitals in Sao Paul o
Source: CREMESP (2004) in La Forgia and Couttolenc (2008)

51• Information is a key element to evaluate hospital performance in Brazil. It seems that both public and private hospitals have problems related to this subject:
- IBGE 2002 Research points out that only 34.8% of non-profit hospitals (private) have an implemented cost system and only 23.2% control (regularly) their inventory.
- According to Ministerio da Saude (2004), there is no information available for public hospital performance evaluations.
• Information absence is clear picture of the poor managerial performance in Hospitals.
• The absence of systematic and reliable information on costs, volume, outcomes and patient characteristics impedes the design of robust hospital payment mechanisms and force policy makers to make key decisions about resource allocation without having even minimum data
Problems in Hospital Sector: Information
makers to make key decisions about resource allocation without having even minimum data [La Forgia and Couttolenc (2008)].
Source: La Forgia and Couttolenc (2008)
Financial Information Availability at Health Facili ties (2003)

52
Policy Recommendations

53Policy Recommendations: Primary Health Care
1. Increase investments in sanitation infrastructure.• Sewage system coverage needs special attention.• As Brazilian sanitation system is in the hands of local state owned enterprises, Federal
Government may need to provide funding options and supportive regulation to expand the system.• High externalities through reductions in diseases and hospitals visits (costs in health care) justify
subsidies for investments in this area.• Investment in sanitation infrastructure is health expenditure!Not considering sanitation
infrastructure as a health expenditure for mandatory expenditure limits purpose (EC 29) leads to underinvestment in this sector and overspending on health systems (as a consequence of the lack of sanitation coverage – vicious cycle).
2. Investments in early childhood development programs and for women education.2. Investments in early childhood development programs and for women education.• Early childhood not only became a very important issue for the education sector, but also for the
health system.• There are studies showing high returns of public investments in the early childhood period to avoid
latter diseases. Coordination between Education and Health Ministries can potentially bring goods results.
3. Improve treatment and control of infectious diseases. Brazilian performance is below regional average:
• Tuberculosis / Malaria / Dengue
4. Continue/Expand good practices in primary care, such as: • Saude da Familia (expanding Dental Care) / Farmacia Popular / Immunization Programs

54Policy Recommendations: Unified Health System (SUS)1. Policy Formulation• The idea of “Federal formulation and Local Governments implementation” seems effective.• Impacts of “Pacto pela Saude” in the organization of Brazilian health care need to be evaluated.
The idea of clear definition of responsibilities among government entities is important.
2. System Planning and Coordination• Develop and implement state-level master plans for care coordination and establishment of
regional network [La Forgia and Couttolenc (2008)].• Planning is a key element to:
(i) organize several public health policies (from different government levels) in their jurisdiction. Public policies should complement each other, not compete.(ii) improve allocative efficiency of the system through correct health services provision/allocation based on the local population’s demand.
• State Health Secretariats must be well prepared to face health care planning challenges. It includes a solid public servant career and a long-term vision for health care policy.
3. Design programs/campaign to reduce the most important mortality factors:• Circulatory System: Obesity/Blood Pressure Control• Respiratory System: Tobacco Consumption• External Causes: Violence (Multi-Sector Policy)
4. Invest in Imaging Diagnostic Technology in order to reduce regional disparities and increase the quality of diagnoses.
• Savings derived from “scale economy” by concentrating services in medium/large hospitals can provide funding for it.

55Policy Recommendations: Hospitals1. What is the real problem in Hospital Sector?• Considering the average efficiencyin hospitals under Direct Administration being less than 0.3(and 0.4in
others) compared to the most efficient hospital in Brazil (= 1), it doesn’t seem the major problem in the Brazilian hospital sector is insufficient funding.
• International data ranks Brazil’s total expenditure in health care close to the average of OECD countries, although Brazilian population is much younger.
2. Information• Information availability is a pre-conditionfor most important reforms in hospitals such as outcome
(production), cost, inventory, clinical and patient record.
• Develop an integrated IT system for different programs (possible data exchange). Saude da Familia (as an example) can provide helpful information about its beneficiaries to hospitals.
3. Organization/Management3. Organization/Management• OECD (2009) and La Forgia and Couttolenc (2008) recognize flexible institutional arrangements for
hospital administration and human-resource management are more efficient. Is it possible to migrate all Hospital Systems to OSS benchmark?
• Experiments and a gradual implementation agenda may be recommendable for these reforms.
4. Payment Mechanisms• Implement Global Budget Payment System linked with performance.
• Realign payments with costs in AIH/SIA system linked with better information provision (accountability) and reforms implementation.
5. Health Care Coordination and Hospitals• Brazil Outlook OECD (2009): “In decentralized setting, cost-effectiveness depends a great deal on the
ability of service deliverers to exploit economies of scale and scope”.
• Re-define the role of small hospitals in the health care system. They should concentrate efforts in emergency procedures and on patient transferences to medium/large hospitals.

56
Thank you!
Downloads:Downloads:
www.pedrojucamaciel.com
Contacts:

57
Backup Slides

5858Public Spending: Importance of Health Care in 2008States Expenditure (By Sectors)
Education, 22%
Social Security, 15%
Health, 15%Public
Administrative, 8%
Judiciary, 9%
Transportation, 6%
Legislative, 3%
Others, 10%
Municipals Expenditure (By Sectors)
Education, 26%
Health, 23%
Urbanism, 13%
Social Security, 6%
Administrat.,
Transport., 3%
Social Assistance, 3%
Sanitation, 3%Legislative, 3%
Others, 6%
Federal Expenditure (By Sectors)
Social Security, 51.1%
Health, 9.8%
Social Assistance,
5.7%
Education, 5.0%
Labor/Work, 4.5%
Defense, 4.4%
Administrat., 2.6%
Judiciary, 4.1%
Others, 9.1%Transport., 2.6%
Source: Secretariat of the National Treasury (2009)
Health, 15%Public Security, 11%
Administrat., 13%

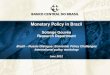
5959Importance of Health Care in Brazilian Families Budget• Health is the third largest families spending category.
• In average, Brazilian families spends 6% of their budget in health.
40%
35%
30%
25%
Families Expenditure Profile: Share in Total Income (2003)
Source: FUNSALUD (2007)
20%
15%
10%
5%
0%
Food Housing Transport. Health Education
Brazil North Northeast Southeast South Mid-West
Source: FUNSALUD (2007)

6060Demography and Risk Factors
Source: Ministerio da Saude (2009)
Região 2000 2005 2009Variação
2000-2009
Norte 79.416 76.172 62.046 -21,90%
Nordeste 249.057 214.865 159.036 -36,10%
Centro-Oeste 52.112 43.362 32.792 -37,00%
Sudeste 217.243 174.465 138.401 -36,30%
Sul 81.530 63.677 51.781 -36,50%

6161
2000
Good Experiences: Programa Saude da Familia
2005 Feb 2010

6262Brazilian Health System: performance indicator
Overall Performance of Health System: 2000 World Health Report
Source: World Health Report (2000)