Embed Size (px)
Citation preview

1
NAVIGATING HEALTH TECHNOLOGY ASSESSMENT
PROCESSES AROUND THE WORLD
ISPOR 13th Annual International MeetingToronto, Canada, May 2008
HTA – EBD Forum
2
Health Technology Assessment and Evidence-Based Decisions (HTA-EBD) Special Interest Group (SIG)
Working Groups (WG)
HTA & Good Research Practices for Reimbursement Decisions
HTA of Emerging New Technologies
Global HTA Used in Healthcare Reimbursement
ISPOR LiaisonNadia Naaman - Randa Eldessouki
3
Moderator
Jalpa A. Doshi, PhDPhiladelphia, PA, USA
NAVIGATING HEALTH TECHNOLOGY ASSESSMENT PROCESSES AROUND
THE WORLD
4
Speakers
NAVIGATING HEALTH TECHNOLOGY ASSESSMENT PROCESSES AROUND
THE WORLD
Jennifer StephensBethesda, MD, USA
Karl Matuszewski Chicago, IL, USA
Neil PalmerOttawa, Canada
Annie Chicoye Paris - France
Afdlsa;jfl;dsjfl
Global Survey to Assess Methods Used in HTA & Reimbursement
DecisionsHealth Technology
Assessment & Good Research Practices
for Reimbursement Decisions WG
6
Co-Chairs:Jalpa A. Doshi PhD, Research Assistant Professor of Medicine, General Internal MedicineUniversity of PennsylvaniaBonnie Handke RN, Director, Health Policy and Planning, Medtronic, Inc, Neuromodulation Jennifer Stephens PharmD, Clinical Director & Partner, Pharmerit North America LLC
Gisselle Gallego PhD, Research Fellow, Centre for Health Economics Research andEvaluation (CHERE) University of Sydney, AustraliaWim Goettsch PhD, Consultant Pharmacoeconomics Dutch Health Insurance BoardSeema Haider MSc, Director, Pfizer Inc, Global HE/ORFranz Hessel MD, MPH, Senior Manager, Sanofi-Aventis, Managed Markets / HEOR Tove Holm-Larsen MSc, University of DenmarkDeborah Lubeck PhD, Vice President Icon Clinical ResearchJohn O’Donnell PhD, Regional DirectorI, Astra-ZenecaDan Ollendorf MPH, Chief Review Officer, Institute for Clinical and Economic ReviewCarlos Gouveia Pinto PhD, Associate Professor of Health Economics, Technical University of Lisbon
Other Key Contributors:Isaac Foley, Pharmerit North America LLC; Howard Tag, Tag & Associates
HTA & Good Research Practices for Reimbursement Decisions WG
2
7
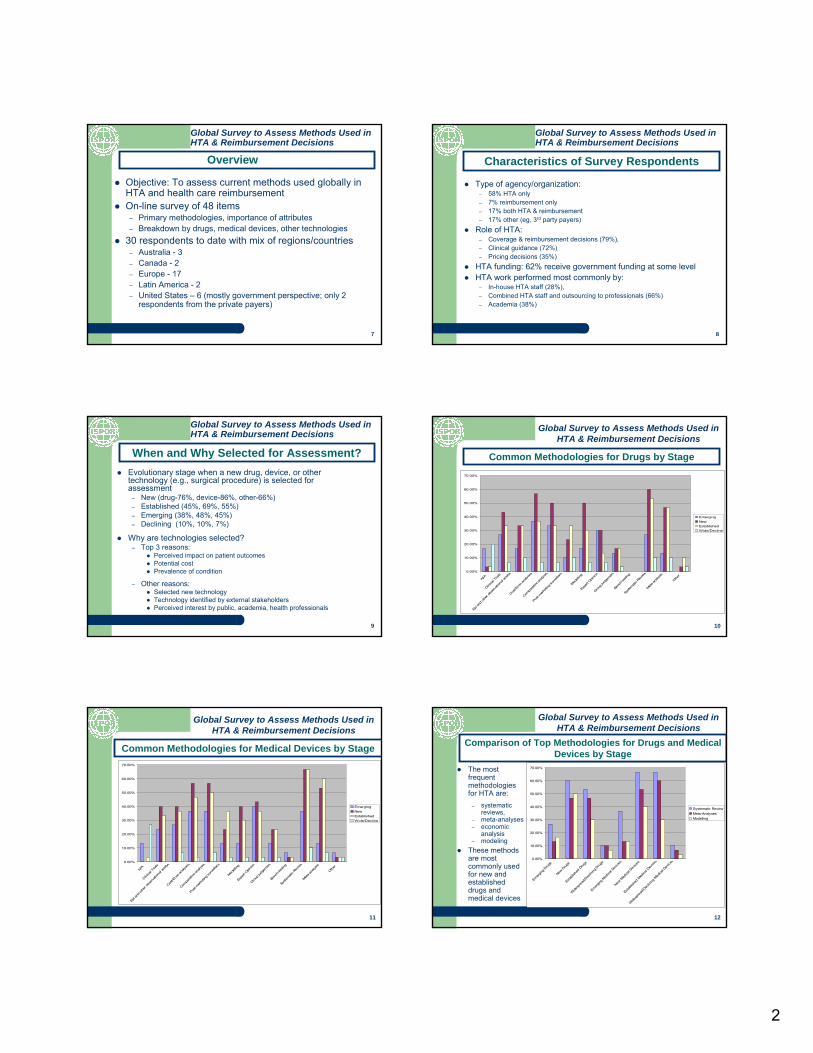
Objective: To assess current methods used globally in HTA and health care reimbursementOn-line survey of 48 items
– Primary methodologies, importance of attributes – Breakdown by drugs, medical devices, other technologies
30 respondents to date with mix of regions/countries– Australia - 3– Canada - 2– Europe - 17– Latin America - 2 – United States – 6 (mostly government perspective; only 2
respondents from the private payers)
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Overview
8
Type of agency/organization:– 58% HTA only – 7% reimbursement only – 17% both HTA & reimbursement – 17% other (eg, 3rd party payers)
Role of HTA:– Coverage & reimbursement decisions (79%), – Clinical guidance (72%)– Pricing decisions (35%)
HTA funding: 62% receive government funding at some levelHTA work performed most commonly by:
– In-house HTA staff (28%), – Combined HTA staff and outsourcing to professionals (66%) – Academia (38%)
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Characteristics of Survey Respondents
9
Evolutionary stage when a new drug, device, or other technology (e.g., surgical procedure) is selected for assessment
– New (drug-76%, device-86%, other-66%) – Established (45%, 69%, 55%)– Emerging (38%, 48%, 45%)– Declining (10%, 10%, 7%)
Why are technologies selected?– Top 3 reasons:
Perceived impact on patient outcomesPotential costPrevalence of condition
– Other reasons:Selected new technologyTechnology identified by external stakeholdersPerceived interest by public, academia, health professionals
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
When and Why Selected for Assessment?
10
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
N/A
Clinica
l Tria
ls
Epi a
nd othe
r obs
erva
tiona
l ana
lys
Cost/
Econ
ana
lyses
Compa
rativ
e ana
lyses
Post-
marke
ting s
urve
illanc
Modell
ing
Expe
rt Opin
ion
Group
judg
emen
t
Benc
h-testi
ng
Syste
matic R
eview
Meta-an
alysis
Other
EmergingNewEstablishedWide/Decline
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Methodologies for Drugs by Stage
11
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
N/A
Clinica
l Tria
ls
Epi a
nd ot
her o
bserva
tiona
l ana
lyse
Cost/E
con a
nalys
es
Compa
rativ
e ana
lyses
Post-
marke
ting s
urve
illanc
e
Modell
ing
Expe
rt Opin
ion
Group
judg
emen
t
Benc
h-tes
ting
Syste
matic R
eview
Meta-ana
lysis
Other
EmergingNewEstablishedWide/Decline
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Methodologies for Medical Devices by Stage
12
The most frequent methodologies for HTA are:
– systematic reviews,
– meta-analyses– economic
analysis– modeling
These methods are most commonly used for new and established drugs and medical devices
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Emer
ging D
rugs
New D
rugs
Establi
shed
Drug
s
Wide
spre
ad/D
eclin
ing D
rugs
Emergin
g Med
ical D
evice
s
New M
edica
l Dev
ices
Establi
shed
Med
ical D
evice
s
Wide
spre
ad/D
eclin
ing M
edica
l Dev
ices
Systematic ReviewMeta-AnalysesModelling
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Comparison of Top Methodologies for Drugs and Medical Devices by Stage
3
13
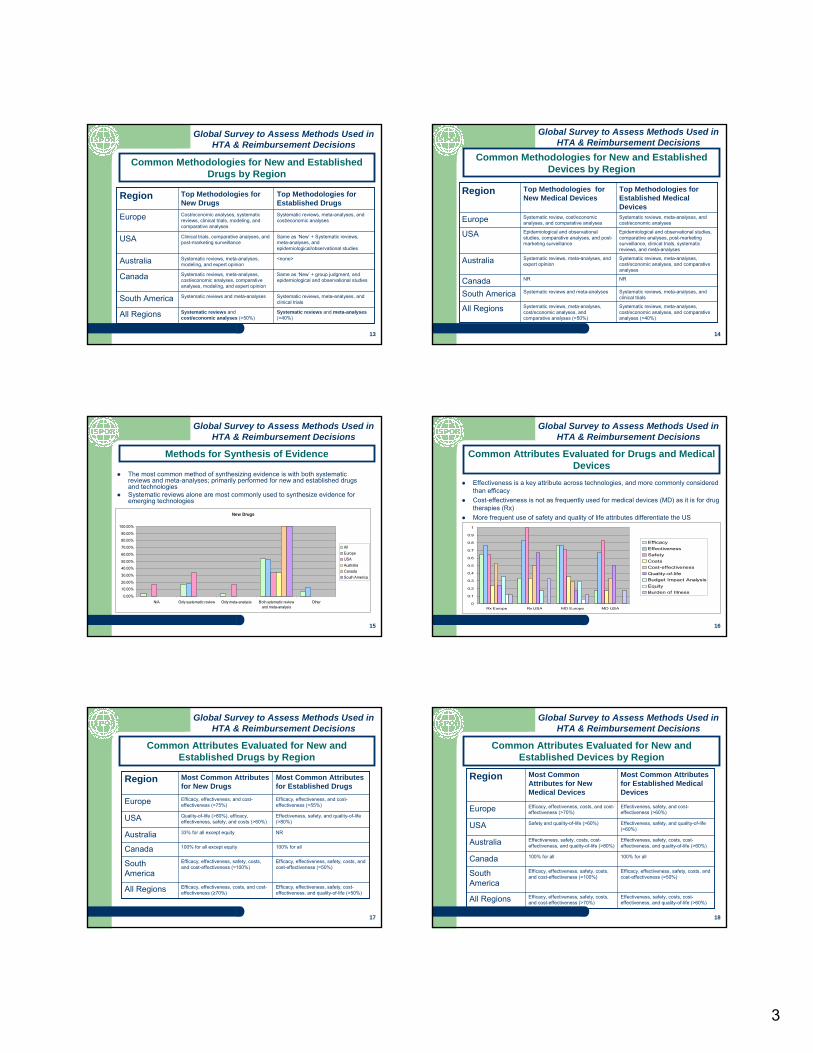
Systematic reviews and cost/economic analyses (>50%)
Systematic reviews and meta-analyses
Systematic reviews, meta-analyses, cost/economic analyses, comparative analyses, modeling, and expert opinion
Systematic reviews, meta-analyses, modeling, and expert opinion
Clinical trials, comparative analyses, and post-marketing surveillance
Cost/economic analyses, systematic reviews, clinical trials, modeling, and comparative analyses
Top Methodologies for New Drugs
Systematic reviews and meta-analyses(>40%)All Regions
Systematic reviews, meta-analyses, and clinical trialsSouth America
Same as ‘New’ + group judgment, and epidemiological and observational studiesCanada
<none>Australia
Same as ‘New’ + Systematic reviews, meta-analyses, and epidemiological/observational studies
USA
Systematic reviews, meta-analyses, and cost/economic analysesEurope
Top Methodologies for Established Drugs
Region
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Methodologies for New and Established Drugs by Region
14
Systematic reviews, meta-analyses, cost/economic analyses, and comparative analyses (>50%)
Systematic reviews and meta-analyses
NR
Systematic reviews, meta-analyses, and expert opinion
Epidemiological and observational studies, comparative analyses, and post-marketing surveillance
Systematic review, cost/economic analyses, and comparative analyses
Top Methodologies for New Medical Devices
Systematic reviews, meta-analyses, cost/economic analyses, and comparative analyses (>40%)
All Regions
Systematic reviews, meta-analyses, and clinical trialsSouth America
NRCanada
Systematic reviews, meta-analyses, cost/economic analyses, and comparative analyses
Australia
Epidemiological and observational studies, comparative analyses, post-marketing surveillance, clinical trials, systematic reviews, and meta-analyses
USA
Systematic reviews, meta-analyses, and cost/economic analysesEurope
Top Methodologies for Established Medical Devices
Region
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Methodologies for New and Established Devices by Region
15
The most common method of synthesizing evidence is with both systematic reviews and meta-analyses; primarily performed for new and established drugs and technologiesSystematic reviews alone are most commonly used to synthesize evidence for emerging technologies
New Drugs
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
N/A Only systematic review Only meta-analysis Both sytematic reviewand meta-analysis
Other
AllEuropeUSAAustraliaCanadaSouth America
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Methods for Synthesis of Evidence
16
Effectiveness is a key attribute across technologies, and more commonly considered than efficacyCost-effectiveness is not as frequently used for medical devices (MD) as it is for drug therapies (Rx)More frequent use of safety and quality of life attributes differentiate the US
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Rx Europe Rx USA MD Europe MD USA
EfficacyEffectivenessSafetyCostsCost-effectivenessQuality-of-lifeBudget Impact AnalysisEquityBurden of Illness
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Attributes Evaluated for Drugs and Medical Devices
17
Efficacy, effectiveness, costs, and cost-effectiveness (≥70%)
Efficacy, effectiveness, safety, costs, and cost-effectiveness (=100%)
100% for all except equity
33% for all except equity
Quality-of-life (>80%), efficacy, effectiveness, safety, and costs (>60%)
Efficacy, effectiveness, and cost-effectiveness (>75%)
Most Common Attributes for New Drugs
Efficacy, effectiveness, safety, cost-effectiveness, and quality-of-life (>50%)All Regions
Efficacy, effectiveness, safety, costs, and cost-effectiveness (=50%)South
America
100% for allCanada
NRAustralia
Effectiveness, safety, and quality-of-life (>80%)USA
Efficacy, effectiveness, and cost-effectiveness (>55%)Europe
Most Common Attributes for Established Drugs
Region
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Attributes Evaluated for New and Established Drugs by Region
18
Efficacy, effectiveness, safety, costs, and cost-effectiveness (>70%)
Efficacy, effectiveness, safety, costs, and cost-effectiveness (=100%)
100% for all
Effectiveness, safety, costs, cost-effectiveness, and quality-of-life (>80%)
Safety and quality-of-life (>60%)
Efficacy, effectiveness, costs, and cost-effectiveness (>70%)
Most Common Attributes for New Medical Devices
Effectiveness, safety, costs, cost-effectiveness, and quality-of-life (>60%)All Regions
Efficacy, effectiveness, safety, costs, and cost-effectiveness (=50%)South
America
100% for allCanada
Effectiveness, safety, costs, cost-effectiveness, and quality-of-life (>60%)Australia
Effectiveness, safety, and quality-of-life (>60%)USA
Effectiveness, safety, and cost-effectiveness (>60%)Europe
Most Common Attributes for Established Medical Devices
Region
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Common Attributes Evaluated for New and Established Devices by Region
4
19
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
Efficacy Effectiveness Safety Costs Cost-effectiveness
Quality-of-life Budget impactanalysis
Equity Burden of illness
DrugsMedical Devices
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
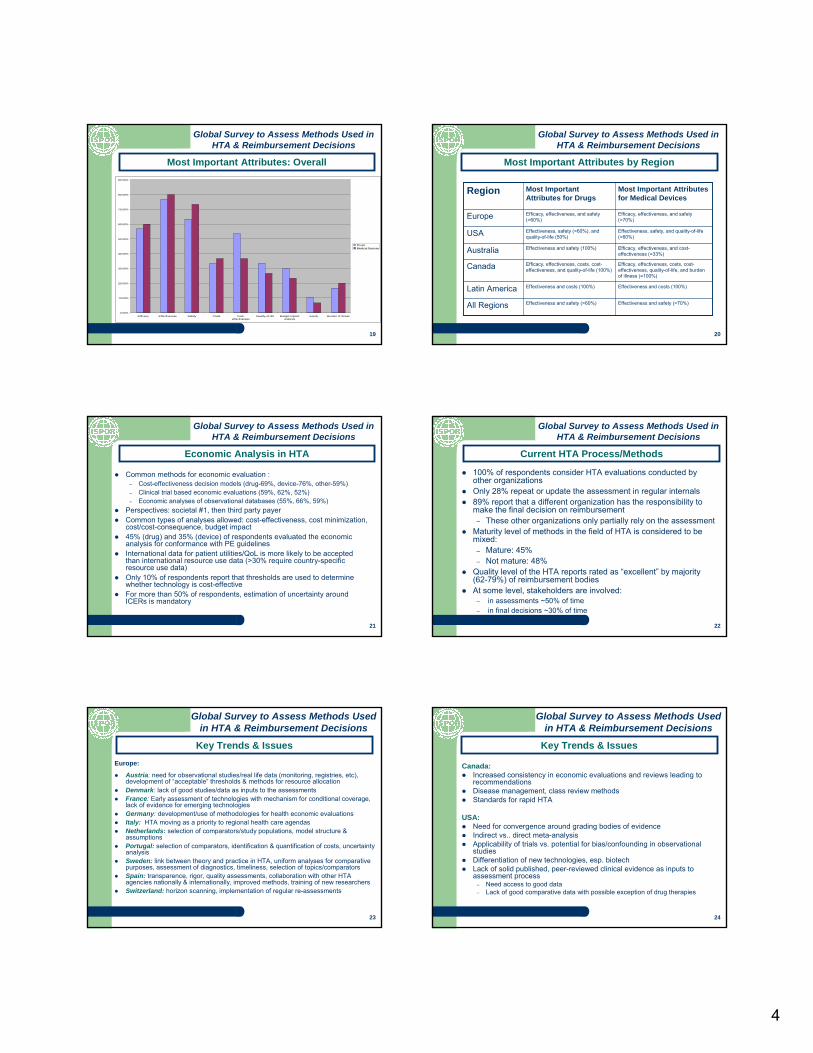
Most Important Attributes: Overall
20
Effectiveness and safety (>60%)
Effectiveness and costs (100%)
Efficacy, effectiveness, costs, cost-effectiveness, and quality-of-life (100%)
Effectiveness and safety (100%)
Effectiveness, safety (>60%), and quality-of-life (50%)
Efficacy, effectiveness, and safety (>60%)
Most Important Attributes for Drugs
Effectiveness and safety (>70%)All Regions
Effectiveness and costs (100%)Latin America
Efficacy, effectiveness, costs, cost-effectiveness, quality-of-life, and burden of illness (=100%)
Canada
Efficacy, effectiveness, and cost-effectiveness (=33%)Australia
Effectiveness, safety, and quality-of-life (>60%)USA
Efficacy, effectiveness, and safety (>70%)Europe
Most Important Attributes for Medical Devices
Region
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Most Important Attributes by Region
21
Common methods for economic evaluation :– Cost-effectiveness decision models (drug-69%, device-76%, other-59%)– Clinical trial based economic evaluations (59%, 62%, 52%)– Economic analyses of observational databases (55%, 66%, 59%)
Perspectives: societal #1, then third party payerCommon types of analyses allowed: cost-effectiveness, cost minimization, cost/cost-consequence, budget impact45% (drug) and 35% (device) of respondents evaluated the economic analysis for conformance with PE guidelinesInternational data for patient utilities/QoL is more likely to be accepted than international resource use data (>30% require country-specific resource use data)Only 10% of respondents report that thresholds are used to determine whether technology is cost-effectiveFor more than 50% of respondents, estimation of uncertainty around ICERs is mandatory
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Economic Analysis in HTA
22
100% of respondents consider HTA evaluations conducted by other organizationsOnly 28% repeat or update the assessment in regular internals89% report that a different organization has the responsibility to make the final decision on reimbursement
– These other organizations only partially rely on the assessmentMaturity level of methods in the field of HTA is considered to be mixed:
– Mature: 45%– Not mature: 48%
Quality level of the HTA reports rated as “excellent” by majority (62-79%) of reimbursement bodiesAt some level, stakeholders are involved:
– in assessments ~50% of time– in final decisions ~30% of time
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Current HTA Process/Methods
23
Europe:
Austria: need for observational studies/real life data (monitoring, registries, etc), development of “acceptable” thresholds & methods for resource allocationDenmark: lack of good studies/data as inputs to the assessmentsFrance: Early assessment of technologies with mechanism for conditional coverage, lack of evidence for emerging technologiesGermany: development/use of methodologies for health economic evaluationsItaly: HTA moving as a priority to regional health care agendasNetherlands: selection of comparators/study populations, model structure & assumptionsPortugal: selection of comparators, identification & quantification of costs, uncertainty analysisSweden: link between theory and practice in HTA, uniform analyses for comparative purposes, assessment of diagnostics, timeliness, selection of topics/comparatorsSpain: transparence, rigor, quality assessments, collaboration with other HTA agencies nationally & internationally, improved methods, training of new researchersSwitzerland: horizon scanning, implementation of regular re-assessments
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Key Trends & Issues
24
Canada:Increased consistency in economic evaluations and reviews leading to recommendationsDisease management, class review methodsStandards for rapid HTA
USA:Need for convergence around grading bodies of evidence Indirect vs.. direct meta-analysisApplicability of trials vs. potential for bias/confounding in observational studiesDifferentiation of new technologies, esp. biotechLack of solid published, peer-reviewed clinical evidence as inputs to assessment process
– Need access to good data– Lack of good comparative data with possible exception of drug therapies
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Key Trends & Issues
5
25
Australia:Timeliness, rapid review methodologies, prioritizing topics for reviewLack of evidence for some new & emerging technologies; small patient groupsIncreasing the use of economic analysisAssessment of diagnostic tests & use of linked evidenceSurrogate outcome validityValidity of combined endpointsAssessment of public health programs
Latin America:Burden of disease Microsimulation methodsEstablishment and validation of methodological guidelines for economic evaluation and systematic reviews
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Key Trends & Issues
26
Most HTA occurs at “new” or “established” stageTop methods used in HTA include systematic reviews, meta-analysis, cost-effectiveness analysis via modelingAttributes assessed and the importance of the attributes differ by country/regionKey issues & trends in HTA include standardizing methods for economic evaluations and grading of evidence, lack of evidence and data for emerging new technologiesPerception of maturity level of HTA methods varies
Global Survey to Assess Methods Used in HTA & Reimbursement Decisions
Summary
Decision-Makers & Health Technology Assessment Decision Making process
Health Technology Assessment of Emerging
New Technologies WG
28
HTA of Emerging New Technologies WG
Co-Chairs: Noreen Sullivan BS, President and CEO, Technology Assessment Evaluation Group LLC, Encinitas, CA, USASheryl Szeinbach BS, MS, PhD, RPh, Professor, College of Pharmacy, Ohio State University, Columbus, OH, USA
Amit Chhabra MD, MPH, Outcomes Research Reimbursement Manager, Medtronic, Europe Sarl, Tolochenaz, Switzerland Eric Faulkner, Sr. Director RTI Health Solutions, Director, Genomics Biotech Institute, National Association of Managed care Physicians, NC, USA Karl Matuszewski MS, PharmD, Senior Director, Clinical Knowledge Service, University HealthSystem Consortium, Oak Brook, IL, USA Dimitris Polygenis PharmD, Vice President, Consulting Clinical Services, McKesson Phase 4 Solutions, Toronto, ON, Canada Mayvis Rebeira MBA, MA, Health Economist/Policy Adviser, Ministry of Health, Toronto, ON, Canada Prabashni Reddy PharmD, MS, RPh, Director of the Center for Drug Policy Partners Healthcare, Charlestown, MA, USA Jose-Manuel Rodriguez Barrios PharmD, MPH, MSc, Health Economics Reimbursement Manager, Medtronic, Iberia, Madrid, Spain Enrique Seoane-Vazquez PhD, Assistant Professor Ohio State University, Columbus, OH, USA
29
Overview
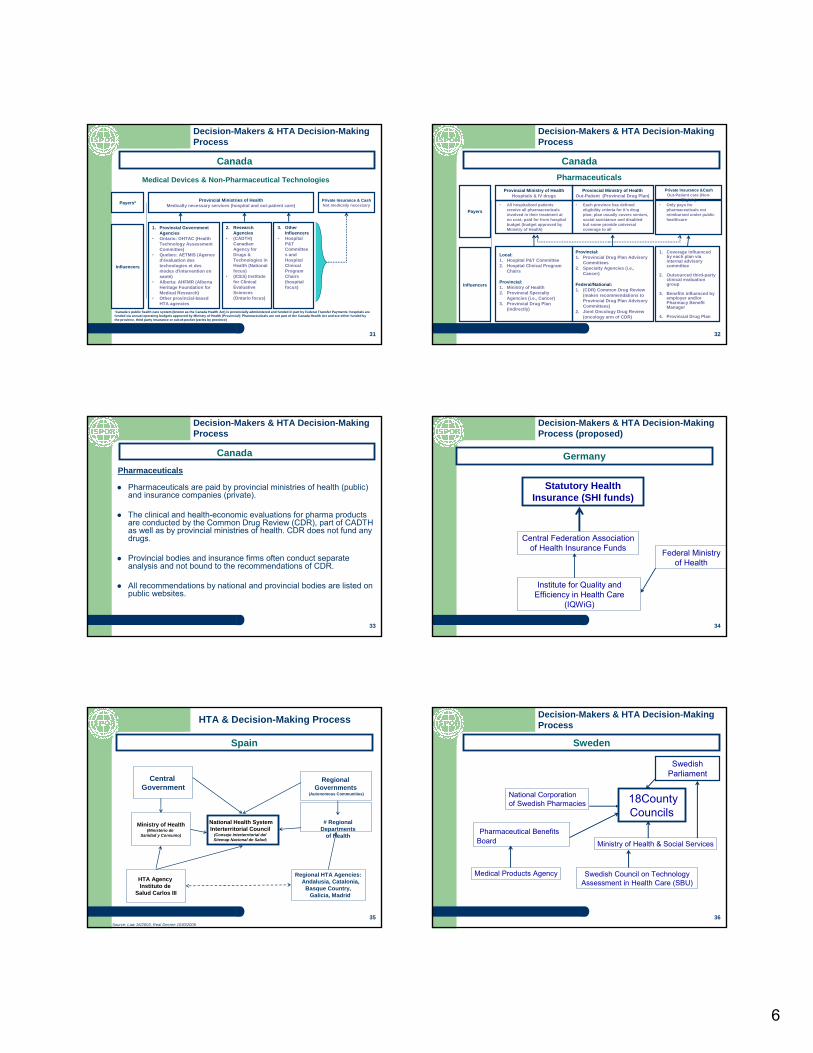
Countries Evaluated:Australia, Canada, Germany, Spain, Sweden, United Kingdom and United States
Decision-Maker (DM): Defined as the payer (person or organization) who makes final decisions for coverage and paymentof a product or technology.
Evaluator: Defined as a person or organization who provides inputinto the decision-making process via HTA development but does notmake final decision for coverage and payment.
Decision-Making Process: The HTA evaluation process, as defined in the public domain, for emerging new technologies (i.e. medical device, pharmaceutical, diagnostic) in consideration forcoverage and payment.
Decision-Makers & HTA Decision-Making Process
30
Pharmaceutical BenefitsAdvisory
Committee (PBAC)
Medical Services Advisory Committee
(MSAC) (21 specialists)
Ministry for Healthand Ageing -
Department ofHealth & Ageing
Australian Health Minister’s
Advisory Council (AHMAC)
Health Policy Advisory Committee
on Technology (Health PACT)
Decision-Makers & HTA Decision-Making Process
Australia
6
31
Medical Devices & Non-Pharmaceutical Technologies
Canada
Payers* Provincial Ministries of HealthMedically necessary services (hospital and out-patient care)
Private Insurance & CashNot medically necessary
3. Other Influencers
• Hospital P&T Committees and Hospital Clinical Program Chairs (hospital focus)
1. Provincial Government Agencies
• Ontario: OHTAC (Health Technology Assessment Committee)
• Quebec: AETMIS (Agence d'évaluation des technologies et des modes d'intervention en santé)
• Alberta: AHFMR (Alberta Heritage Foundation for Medical Research)
• Other provincial-based HTA agencies
2. Research Agencies
• (CADTH) Canadian Agency for Drugs & Technologies in Health (National focus)
• (ICES) Institute for Clinical Evaluative Sciences (Ontario focus)
Influencers
•Canada’s public health care system (known as the Canada Health Act) is provincially administered and funded in part by Federal Transfer Payments; hospitals are funded via annual operating budgets approved by Ministry of Health (Provincial); Pharmaceuticals are not part of the Canada Health Act and are either funded by the province, third party insurance or out-of-pocket (varies by province)
Decision-Makers & HTA Decision-Making Process
32
Pharmaceuticals
Canada
Payers
Provincial Ministry of HealthHospitals & IV drugs
Private Insurance &CashOut-Patient care (Non-
Eligible)
Provincial:1. Provincial Drug Plan Advisory
Committees2. Specialty Agencies (i.e.,
Cancer)
Federal/National:1. (CDR) Common Drug Review
(makes recommendations to Provincial Drug Plan Advisory Committees)
2. Joint Oncology Drug Review (oncology arm of CDR)
• All hospitalized patients receive all pharmaceuticals involved in their treatment at no cost; paid for from hospital budget (budget approved by Ministry of Health)
Influencers
Provincial Ministry of HealthOut-Patient (Provincial Drug Plan)
• Only pays for pharmaceuticals not reimbursed under public healthcare
Local:1. Hospital P&T Committee2. Hospital Clinical Program
Chairs
Provincial:1. Ministry of Health2. Provincial Specialty
Agencies (i.e., Cancer)3. Provincial Drug Plan
(indirectly)
1. Coverage influenced by each plan via internal advisory committee
2. Outsourced third-party clinical evaluation group
3. Benefits influenced by employer and/or Pharmacy Benefit Manager
4. Provincial Drug Plan
• Each province has defined eligibility criteria for it’s drug plan; plan usually covers seniors, social assistance and disabled but some provide universal coverage to all
Decision-Makers & HTA Decision-Making Process
33
Pharmaceuticals
Pharmaceuticals are paid by provincial ministries of health (public) and insurance companies (private).
The clinical and health-economic evaluations for pharma products are conducted by the Common Drug Review (CDR), part of CADTH as well as by provincial ministries of health. CDR does not fund any drugs.
Provincial bodies and insurance firms often conduct separate analysis and not bound to the recommendations of CDR.
All recommendations by national and provincial bodies are listed on public websites.
Canada
Decision-Makers & HTA Decision-Making Process
34
Statutory Health Insurance (SHI funds)
Central Federation Association of Health Insurance Funds
Institute for Quality and Efficiency in Health Care
(IQWiG)
Federal Ministry of Health
Germany
Decision-Makers & HTA Decision-Making Process (proposed)
35
Central Government
Ministry of Health(Ministerio de
Sanidad y Consumo)
Regional Governments
(Autonomous Communities)
Regional HTA Agencies:Andalusia, Catalonia,
Basque Country,Galicia, Madrid
National Health System Interterritorial Council
(Consejo Interterritorial del Sitemap Nacional de Salud)
HTA Agency Instituto de
Salud Carlos III
# Regional Departments
of Health
Source: Law 16/2003, Real Decree 1030/2006
Spain
HTA & Decision-Making Process
36
18County Councils
Swedish Council on Technology Assessment in Health Care (SBU)
Ministry of Health & Social Services
Medical Products Agency
Pharmaceutical Benefits Board
National Corporation of Swedish Pharmacies
Swedish Parliament
Sweden
Decision-Makers & HTA Decision-Making Process
7
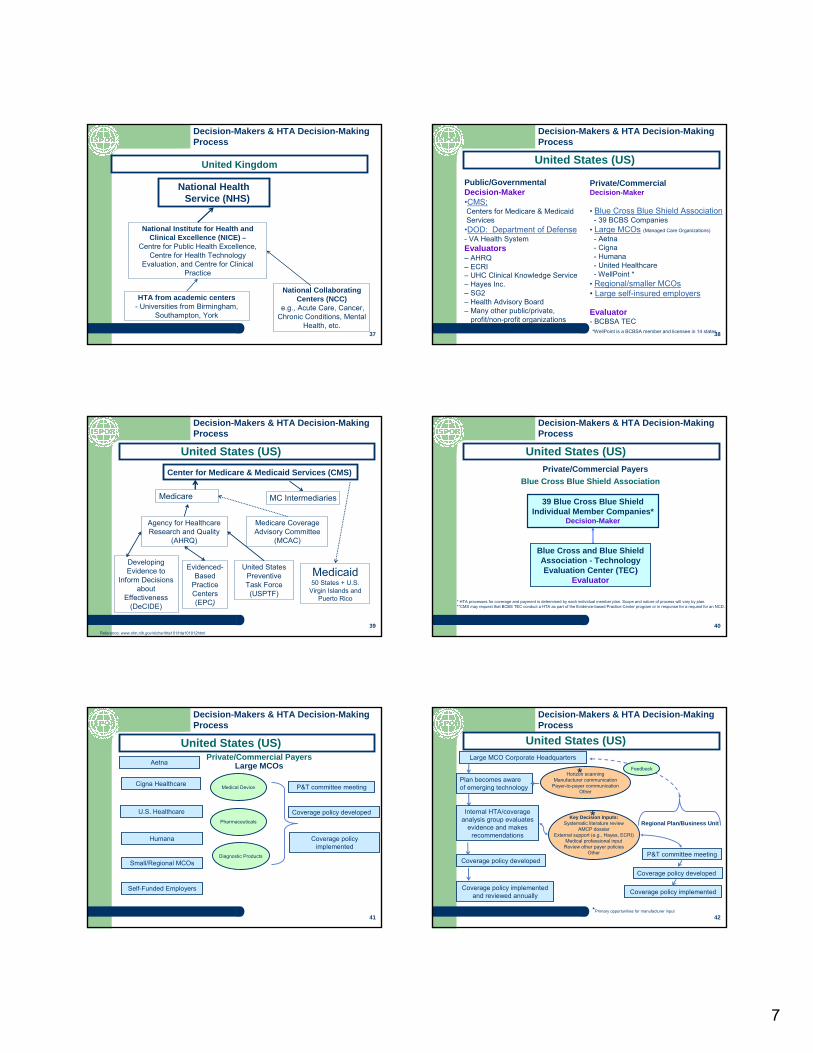
37
National Institute for Health and Clinical Excellence (NICE) –
Centre for Public Health Excellence, Centre for Health Technology
Evaluation, and Centre for Clinical Practice
HTA from academic centers- Universities from Birmingham,
Southampton, York
National Health Service (NHS)
National Collaborating Centers (NCC)
e.g., Acute Care, Cancer, Chronic Conditions, Mental
Health, etc.
United Kingdom
Decision-Makers & HTA Decision-Making Process
38
Private/Commercial Decision-Maker
• Blue Cross Blue Shield Association- 39 BCBS Companies
• Large MCOs (Managed Care Organizations)
- Aetna- Cigna- Humana- United Healthcare- WellPoint *
• Regional/smaller MCOs• Large self-insured employers
Evaluator- BCBSA TEC
Public/GovernmentalDecision-Maker•CMS:Centers for Medicare & MedicaidServices•DOD: Department of Defense- VA Health SystemEvaluators– AHRQ– ECRI– UHC Clinical Knowledge Service– Hayes Inc.– SG2– Health Advisory Board– Many other public/private,
profit/non-profit organizations*WellPoint is a BCBSA member and licensee in 14 states
United States (US)
Decision-Makers & HTA Decision-Making Process
39
Agency for Healthcare Research and Quality
(AHRQ)
Medicare Coverage Advisory Committee
(MCAC)
Developing Evidence to
Inform Decisions about
Effectiveness(DeCIDE)
Reference: www.nlm.nih.gov/nichsr/hta101/hta101012html
Evidenced-Based
Practice Centers (EPC)
United States Preventive Task Force (USPTF)
Medicare MC Intermediaries
Center for Medicare & Medicaid Services (CMS)
Medicaid50 States + U.S.
Virgin Islands and Puerto Rico
United States (US)
Decision-Makers & HTA Decision-Making Process
40
Blue Cross Blue Shield AssociationPrivate/Commercial Payers
39 Blue Cross Blue Shield Individual Member Companies*
Decision-Maker
* HTA processes for coverage and payment is determined by each individual member plan. Scope and nature of process will vary by plan.**CMS may request that BCBS TEC conduct a HTA as part of the Evidence-based Practice Center program or in response for a request for an NCD.
United States (US)
Decision-Makers & HTA Decision-Making Process
Blue Cross and Blue Shield Association - Technology Evaluation Center (TEC))
Evaluator
41
Private/Commercial PayersLarge MCOsAetna
Cigna Healthcare
U.S. Healthcare
Humana
Coverage policy developed
P&T committee meeting
Coverage policy implemented
Medical Device
Diagnostic Products
Pharmaceuticals
Small/Regional MCOs
Self-Funded Employers
United States (US)
Decision-Makers & HTA Decision-Making Process
42
Large MCO Corporate Headquarters
Plan becomes aware of emerging technology
Internal HTA/coverage analysis group evaluates
evidence and makes recommendations
Coverage policy developed
Coverage policy developed
P&T committee meeting
Coverage policy implemented and reviewed annually
Key Decision Inputs:Systematic literature review
AMCP dossierExternal support (e.g., Hayes, ECRI)
Medical professional inputReview other payer policies
Other
Horizon scanningManufacturer communication
Payer-to-payer communicationOther
Coverage policy implemented
Feedback
Regional Plan/Business Unit
*
*
*Primary opportunities for manufacturer input
United States (US)
Decision-Makers & HTA Decision-Making Process
8
43
Conclusion & Next Steps
To gain a better understanding of the HTA decision-makers and evaluators and the process used to determine coverage and payment for emerging new technologies.
Next Steps for Emerging New Technologies Special Interest Group:– Conduct 1-on-1 interviews with Decision-Makers
to further refine decision-making processes;– Publish results, i.e. manuscript(s) in Value in
Health, ISPOR website;– Timeline: Q3/Q4, 2008
Decision-Makers & HTA Decision-Making Process
ISPOR Global Health care Systems Road Map
Global Health Technology Assessment used in
Health Care Reimbursement WG
45
Co-Chairs: Stefan Holmstrom BSc, MSc, Director of Project Management, HE&OR, NicOx SA, Antipolis - cedex, France Kevin Mayo PhD, Director Health Outcomes Research, Daiichi Sankyo, Inc., Parsippany, NJ, USA
Lieven Annemans PhD, MSc, Ghent University, Faculty of Medicine, Meise, BelgiumAnnie Chicoye, Senior Principal Director Pricing & Market Access IMS Consulting, FranceShanlian Hu MD, MSc, Professor Training Center for Health Management School of PublicHealth Fu Dan UniversityChristine Huttin PhD, Health Scientist & Research Professor, ENDEPUSresearch and ENDEPResearch Group, Cambridge MA USAIsao Kamae MD, DrPH, Professor of Pharmacoeconomics, JPMA Research and EducationProject, Keio University of Tokyo, Fujisawa-City, Kanazawa, JapanProfessor Shu Chen Li, Chair, Discipline of Pharmacy , The University of Newcastle, Newcastle, AustraliaHans Middelhoven PhD, F. Hoffmann – La Roche Ltd., Basel, SwitzerlandMark Nuijten PhD, MD, MBA Eramus University, Rotterdam, The NetherlandsW. Neil Palmer, Vice-President, Pricing and Reimbursement, RTI Health Solutions, Ottawa, CanadaCarolyn Steeds BSc, Independent Consultant, Carolyn Steeds Consulting, Motherwell, ScotlandRebecca Townsend BSc, Project Director, Evidence Research Unit, Macclesfield, UKChristoph Vauth MSc PhD Student, University of Hannover / IVBL, Hanover, GermanyKonrad RB Wallerstein, Adelphi Focus, Doylestown, PA, USAFeng Zeng PhD, Health Economist, MedImpact Healthcare Systems, San Diego, CA
Global Health Technology Assessment used in Health Care Reimbursement WG
46
Objectives:– To develop a global review of available health
technology assessment information – To develop a roadmap of health technology
assessment information at the ISPOR website for health care decision-makers and payers.
Achievements:– The ISPOR Global Health Care Systems Road
Map
Global Health Technology Assessment used in Health Care Reimbursement WG
47
The Road Map provides an overview of country-specific health care delivery systems, reimbursement and pricing approval processes, reimbursement terminology and contact information for the most relevant HTA and other government organizations.
ISPOR Global Health care Systems Road Map
48
France
ISPOR Global Health care Systems Road Map
9
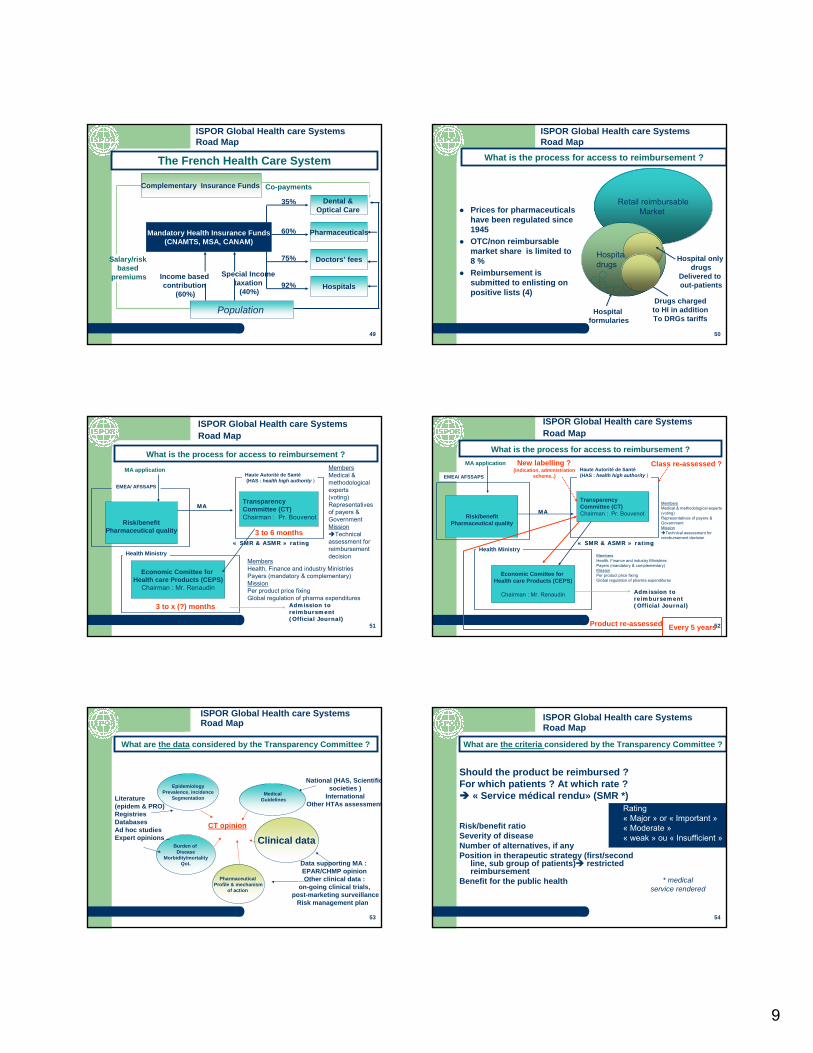
49
Mandatory Health Insurance Funds(CNAMTS, MSA, CANAM)
Population
Complementary Insurance Funds
Dental & Optical Care
Pharmaceuticals
Doctors’ fees
HospitalsIncome based contribution
(60%)
Special Income taxation
(40%)
Salary/risk based
premiums
Co-payments
35%
60%
75%
92%
The French Health Care System
ISPOR Global Health care Systems Road Map
50
Prices for pharmaceuticalshave been regulated since1945OTC/non reimbursablemarket share is limited to 8 % Reimbursement issubmitted to enlisting on positive lists (4)
Retail reimbursableMarket
Hospitaldrugs
Hospital onlydrugs
Delivered to out-patients
Drugs chargedto HI in addition To DRGs tariffs
Hospitalformularies
What is the process for access to reimbursement ?
ISPOR Global Health care Systems Road Map
51
TransparencyCommittee (CT) Chairman : Pr. Bouvenot
Economic Comittee for Health care Products (CEPS)
Chairman : Mr. Renaudin
Members Medical & methodological experts(voting) Representatives of payers & Government Mission
Technical assessment for reimbursement decision
Haute Autorité de Santé(HAS : health high authority )
Health MinistryMembersHealth, Finance and industry MinistriesPayers (mandatory & complementary) MissionPer product price fixing Global regulation of pharma expenditures
Risk/benefitPharmaceutical quality
EMEA/ AFSSAPS
MA application
MAMA
«« SMR & ASMRSMR & ASMR »» ratingrating
Admission to Admission to reimbursmentreimbursment(Official Journal)(Official Journal)
3 to 6 months
3 to x (?) months
What is the process for access to reimbursement ?
ISPOR Global Health care Systems Road Map
52
TransparencyCommittee (CT) Chairman : Pr. Bouvenot
Economic Comittee for Health care Products (CEPS)
Chairman : Mr. Renaudin
Members Medical & methodological experts(voting) Representatives of payers & Government Mission
Technical assessment for reimbursement decision
Haute Autorité de Santé(HAS : health high authority )
Health MinistryMembersHealth, Finance and industry MinistriesPayers (mandatory & complementary) MissionPer product price fixing Global regulation of pharma expenditures
Risk/benefitPharmaceutical quality
EMEA/ AFSSAPS
MA application
MAMA
«« SMR & ASMRSMR & ASMR »» ratingrating
Admission to Admission to reimbursementreimbursement(Official Journal)(Official Journal)
Every 5 years
New labelling ? (indication, administration
scheme..)
Class re-assessed ?
Product re-assessed
ISPOR Global Health care Systems Road Map
What is the process for access to reimbursement ?
53
EpidemiologyPrevalence, incidence
Segmentation
Burden of Disease
Morbidity/mortalityQoL
Clinical dataCT opinion
Data supporting MA : EPAR/CHMP opinion Other clinical data :
on-going clinical trials, post-marketing surveillance
Risk management plan
Pharmaceutical Profile & mechanism
of action
Literature(epidem & PRO) RegistriesDatabasesAd hoc studiesExpert opinions ..
MedicalGuidelines
ISPOR Global Health care Systems Road Map
What are the data considered by the Transparency Committee ?
National (HAS, Scientificsocieties )
InternationalOther HTAs assessment
54
Should the product be reimbursed ? For which patients ? At which rate ?
« Service médical rendu» (SMR *)
Risk/benefit ratioSeverity of diseaseNumber of alternatives, if anyPosition in therapeutic strategy (first/second
line, sub group of patients) restrictedreimbursement
Benefit for the public health
Rating « Major » or « Important »« Moderate »« weak » ou « Insufficient »
* medicalservice rendered
What are the criteria considered by the Transparency Committee ?
ISPOR Global Health care Systems Road Map
10
55
Should the product be priced at a premium price ? « Amélioration du Service médical rendu» (ASMR *)
Clinical studies versus reference product :– Cheapest, most prescribed, most recently
enlisted– Usual therapy eventually
Direct or indirect comparisons (meta-analysis, lit review, experts opinions)
Determined for each indication / sub-group of population
RRating versus determinedcomparatorGrade I: MajorGrade II: Important Grade III: ModerateGrade IV: MinorGrade V: no ASMR
* Improvement of medicalservice rendered
ISPOR Global Health care Systems Road Map
What are the criteria considered by the Transparency Committee ?
56
SMR Rating - 2006
0
50
100
150
200
250
300
350
Major/important moderate weak insufficient
SMR grade
Num
ber o
f pro
duct
s
First enlisting new indication
ASMR - 2006
050
100150200250300350400
I II III IV V
Comments
ASMR Rate
Num
ber
of
prod
ucts
/indi
catio
n
First enlisting New indication
SMR 2006: 87 % rated major / important 3 % rated unsufficient
Source HAS – report 2006
ASMR 2006 : 11 % rated I to III 4 % rated IV 87 % rated V
ISPOR Global Health care Systems Road Map
Not discriminant for SMR, but highly for ASMR
57
Economic negotiation with CEPS Technical assesement by CT
Reimbursement rate (100%, 65% 35%)SMR rate
EU price corridor Premium price versus competitor (I to III)
ASMR rate
Sales / volumes price agreementTarget population, position in therapeutic strategy, duration of treatment ..
Re-assessment of ASMR withprice/volume agreement consequences
Utilisation profile, real life effectiveness, new clinicalevidence
No pharmacoeconomics are required, although they can betaken into consideration
ISPOR Global Health care Systems Road Map
The CT assessessment is determinant for price negotiation
58
ISPOR Global Health care Systems Road Map
Canada
59
Federal Canada Health Act defines Canadian “Medicare”– Universal access – all Canadians covered– Publicly administered – Coverage is portable across provinces– Comprehensive – most medical necessary services are covered
(But not prescription drugs dispensed outside hospitals)– Publicly funded (funding shared between federal/provincial
governments)All provinces have established prescription drug benefit programs (no federal funding)
– Significant differences in coverage, eligibility between provincesFederal government has established drug benefit plans for:
– Veterans, Native Peoples, Federal Prisons, etc.
ISPOR Global Health care Systems Road Map
Canadian Heath Care System
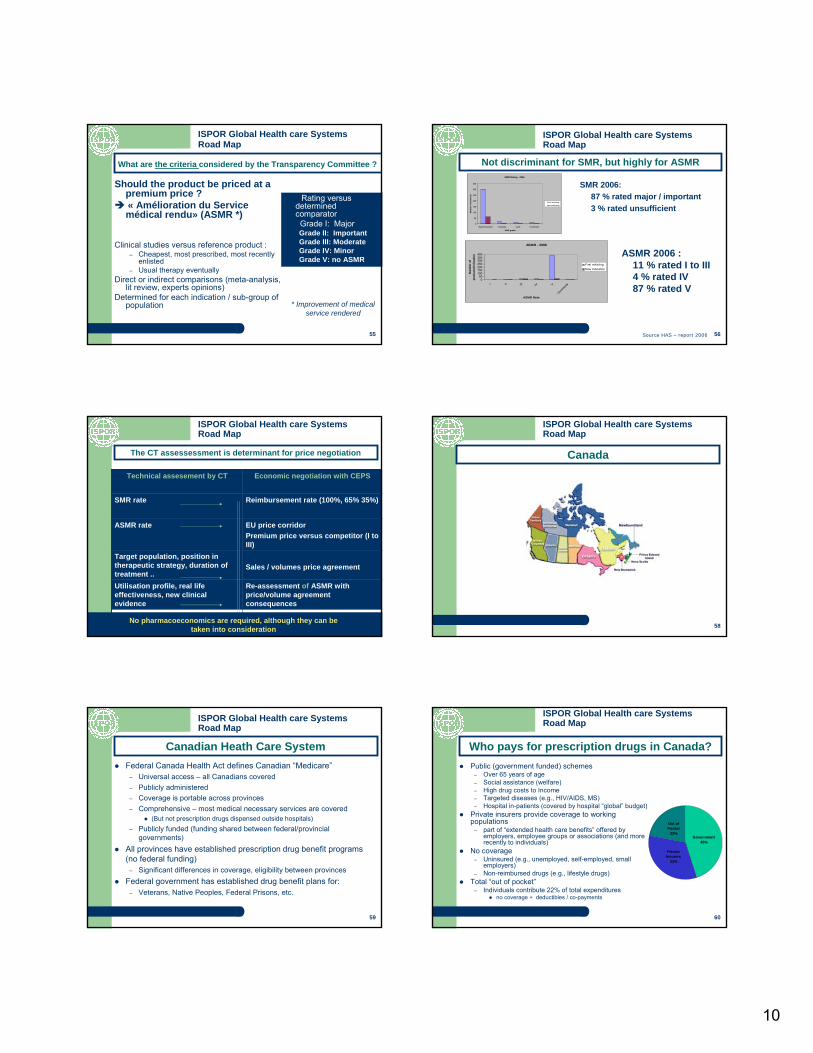
60
Public (government funded) schemes– Over 65 years of age– Social assistance (welfare)– High drug costs to Income– Targeted diseases (e.g., HIV/AIDS, MS)– Hospital in-patients (covered by hospital “global” budget)
Private insurers provide coverage to working populations
– part of “extended health care benefits” offered by employers, employee groups or associations (and more recently to individuals)
No coverage– Uninsured (e.g., unemployed, self-employed, small
employers)– Non-reimbursed drugs (e.g., lifestyle drugs)
Total “out of pocket”– Individuals contribute 22% of total expenditures
no coverage + deductibles / co-payments
Government45%
Private Insurers
33%
Out of Pocket
22%
ISPOR Global Health care Systems Road Map
Who pays for prescription drugs in Canada?
11
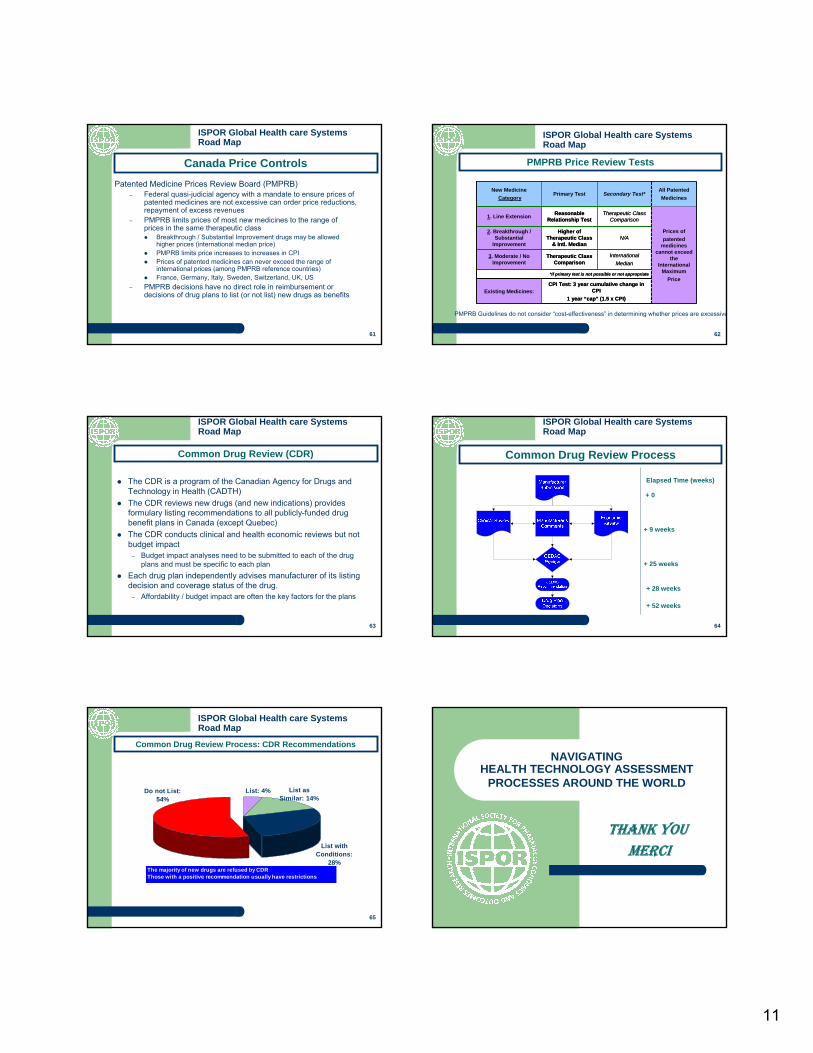
61
Patented Medicine Prices Review Board (PMPRB)– Federal quasi-judicial agency with a mandate to ensure prices of
patented medicines are not excessive can order price reductions,repayment of excess revenues
– PMPRB limits prices of most new medicines to the range of prices in the same therapeutic class
Breakthrough / Substantial Improvement drugs may be allowed higher prices (international median price)PMPRB limits price increases to increases in CPIPrices of patented medicines can never exceed the range of international prices (among PMPRB reference countries)France, Germany, Italy, Sweden, Switzerland, UK, US
– PMPRB decisions have no direct role in reimbursement or decisions of drug plans to list (or not list) new drugs as benefits
ISPOR Global Health care Systems Road Map
Canada Price Controls
62
PMPRB Guidelines do not consider “cost-effectiveness” in determining whether prices are excessive
*if primary test is not possible or not appropriate
CPI Test: 3 year cumulative change in CPI
1 year “cap” (1.5 x CPI)Existing Medicines:
International Median
Therapeutic Class Comparison
3. Moderate / No Improvement
N/AHigher of
Therapeutic Class & Intl. Median
2. Breakthrough / Substantial
Improvement
Prices ofpatented
medicines cannot exceed
the International
MaximumPrice
Therapeutic Class Comparison
Reasonable Relationship Test1. Line Extension
All PatentedMedicines
Secondary Test*Primary TestNew Medicine
Category
*if primary test is not possible or not appropriate
CPI Test: 3 year cumulative change in CPI
1 year “cap” (1.5 x CPI)Existing Medicines:
International Median
Therapeutic Class Comparison
3. Moderate / No Improvement
N/AHigher of
Therapeutic Class & Intl. Median
2. Breakthrough / Substantial
Improvement
Prices ofpatented
medicines cannot exceed
the International
MaximumPrice
Therapeutic Class Comparison
Reasonable Relationship Test1. Line Extension
All PatentedMedicines
Secondary Test*Primary TestNew Medicine
Category
ISPOR Global Health care Systems Road Map
PMPRB Price Review Tests
63
The CDR is a program of the Canadian Agency for Drugs and Technology in Health (CADTH)The CDR reviews new drugs (and new indications) provides formulary listing recommendations to all publicly-funded drug benefit plans in Canada (except Quebec)The CDR conducts clinical and health economic reviews but not budget impact
– Budget impact analyses need to be submitted to each of the drug plans and must be specific to each plan
Each drug plan independently advises manufacturer of its listingdecision and coverage status of the drug.
– Affordability / budget impact are often the key factors for the plans
ISPOR Global Health care Systems Road Map
Common Drug Review (CDR)
64
+ 9 weeks
+ 25 weeks
+ 0
Elapsed Time (weeks)
+ 28 weeks
+ 52 weeks
ISPOR Global Health care Systems Road Map
Common Drug Review Process
65
List: 4%
List with Conditions:
28%
Do not List: 54%
List as Similar: 14%
The majority of new drugs are refused by CDRThose with a positive recommendation usually have restrictions
ISPOR Global Health care Systems Road Map
Common Drug Review Process: CDR RecommendationsNAVIGATING
HEALTH TECHNOLOGY ASSESSMENT PROCESSES AROUND THE WORLD
THANK YOU MERCI