Embed Size (px)
Citation preview

Clin. RadioL (1967) 18, 74-82
H E P A T I C T U M O U R S I N C H I L D H O O D
P E T E R M c D O N A L D
From the Royal Children's Hospital, Melbourne*
The rad iographic findings in twelve children with p r imary mal ignan t hepat ic tumours are presented. The significance o f osteoporosis is discussed. The value o f var ious methods of invest igat ion is c o m p a r e d and the impor tance o f angiographic studies in the diagnosis and management is stressed.
PRIMARY hepa toma is a relat ively u n c o m m o n t u m o u r o f chi ldhood. The usual mode o f presenta- t ion is with a large abdomina l mass and anaemia . Repor t s of successful t rea tment by par t ia l hepa tec tomy indicate the need for accurate pa tho- logical and anatomical diagnosis. In addi t ion, the in t roduc t ion of more effective regimes of manage- ment for other ch i ldhood malignancies such as Wi lms ' t umour and neurob las toma makes desirable as accurate a pre-opera t ive diagnosis as is pract ic- able. I t is the purpose of this paper to demons t ra te how this m a y best be achieved.
The rad iographic features o f p r imary hepa toma have been reviewed previously by Margul is , Nice and Rigler (1956). More recently Bouchier and Lessof (1964) discussed the rad iograph ic diagnosis o f p r imary ca rc inoma o f the liver and Boijsen and A b r a m s (1965) descr ibed their findings in 11 adul ts with p r imary liver tumours and stressed the role o f ang iography in the diagnosis. Several o f the chi ldren in the present series have been subjected to a n g i o g r a p h y and the results are incorpora ted in this paper .
Var ious terms such as hepa toma, hepa tob las toma and embryona l ca rc inoma are used to classify these tumours . However , such great var ia t ion occurs in different par ts o f an indiv idual t umour tha t no real dis t inct ion is possible between them. The degree of mal ignancy cor responds roughly wi th the degree o f differentiation. A l l are g rouped here under the c o m m o n te rm of ' h epa toma ' .
Twelve patients , 8 boys and 4 girls, have presented at this hospi ta l wi th p r imary mal ignan t liver turnouts in the pas t 6 years. Their ages ranged between 6 months and 14 years. In all, the diagnosis was conf i rmed by b iopsy or a t autopsy. Ten pat ients presented wi th a b d o m i n a l masses, one with obstruct ive jaundice and anaemia , a n d one with xan thomatous deposi ts and spleno- megaly. A l l but one have d ied f rom their disease. The ma in clinical and rad iograph ic findings are summar i sed in Table 1.
ILLUSTRATIVE CASE HISTORIES Case 6.--S.T., a boy of 18 months, admitted with three
months anorexia, poor weight gain and abdominal disten- sion. During the previous six months he had sustained frac- tures of both legs from trivial injuries. A hard upper abdo- minal mass was present and he was anaelnic (Hb. 6.5 G. ~). A clinical diagnosis of neuroblastoma was made.
Radiological Findings.--A chest film showed the presence of several small pulmonary metastases. Skeletal survey revealed a marked and generalised osteoporosis (Fig. 1, A and B) and a healing fracture of the distal right femur. A plain film of the abdomen demonstrated a large, mainly right sided, upper abdominal mass with elevation of the diaphragm. An aortogram (Fig. 2) clearly revealed that the tumour was in the liver with enlargement and stretching of the branches of the hepatic artery, and that it contained a typical 'malignant' pattern of vessels. The inferior vena cava was obstructed very close to its origin, with all the contrast medium passing collaterally. The right kidney was displaced posteriorly and a little inferiorly.
Other Investigations.--The serum protein level was 8.6 g. per 100 ml. A liver biopsy obtained at laparotomy confirmed the tumour as a malignant hepatoma. Bone marrow exami- nation did not reveal any infiltration with tumour cells. Biopsy of the fracture site in the right femur showed no evidence of metastasis.
There was no response to a course of 5-fluoro-uracil. The child died two months after his initial admission. Post- morteln examination showed tumour involving both lobes of the liver, with secondary deposits in the lungs. No cause for the obstruction of the inferior vena cava was found and this was presumably related to the large size of the tumour. Skeletal metastasis were not found.
Case 7.--K.B., a boy of 14 years, admitted for investigation of obstructive jaundice. Transient jaundice had occurred 7 months previously. The liver was enlarged and a plain radiograph of the abdomen showed a small area of nodular calcification below the right hemi-diaphragm. At laparo- tomy, clotted blood was found in the biliary tree. A cho- langiogram showed normal filling of the bilim-y passages to the origin of the common hepatic duct but no filling could be obtained above this level. A liver biopsy revealed a pattern consistent with obstructive jaundice. A hepatic arteriogram was performed 3 months latex" and this demonstrated an area of abnormal vessels in the right lobe of the liver close to the porta hepatis. A splenic portal venogram demonstrated a block of the portal vein just beyond the junction of the splenic and superior mesenteric veins, and showed oesophageal varices. A further laparotomy and needle biopsy of the liver in the suspect area did not confirm the presence of a tumour. Four months after admission, the jaundice began to fade, but
* Address from March, 1967: c/o 21 Crieff Road, London, S.W.18
74

H E P A T I C T U M O U R S I N C H I L D H O O D 75
.o & oo
• ~ ~ ~ ~ ~ •
~ ~ 0 ~ 0
0
i m
. , n : A • N ~d ~: o ~ N ~ .
0 # 0 0 0 0 ~ o ~. . s~ ~ ~ ~ - o = ~ ~ = o ~ o~- o o ~ o
0 0 ~ 0
0 0 TM ~ • 0 ,~
• -~'n "~ "~ ~ o . ~ ' n ~ o . u > ~ "~ "~ ~ ' ~ o . : •
o . ~ # ~ ~ ' ~ " ~ " ~ ~'~ = ~ o ~ O o o ~ o ~ o ~ , . ~ , o o ~ o ~ #
,~,, ~ . ~ ~ . ~ . ~ . ~ = ~ ~ ~ : . ~
O o
• ~ ~ ~o ~ ~o ~ ~ ~ ~ ~ ~.° o= ~ ~ " - ~ ~ . ~ . ~ ~=~.~ ~ - ~ ~ ~'~ I :~ .~ . ~ ~ . - ,~ , ~ . n ~ -

76 CLINICAL RADIOLOGY
Fia. 2 Case 6. Aortogram. The liver is greatly enlarged with stretching of all the branches of the hepatic artery and abundant tumour vessels
mainly in the right lobe.
it did not clear completely and periodically it became more evident. Nine months after the first admission he was seen with an episode of haematemesis and melaena, with increased jaundice. A repeat hepatic arteriogram was performed but on this occasion no abnormal vessels were identified. Because of recurrent bleeding into the gut which was regarded as originating from the varices, a spleno-renal venous anasto- mosis was carried out. D u r i n g the subsequent months further episodes of gastro-intestinal haemorrhage occurred. The liver increased in size and he becanae more anaemic. Two years after his first admission he developed cutaneous nodules and enlarged axillary glands. Biopsy of a gland showed metastatic carcinoma, probably malignant hepatoma. Three months later he died with massive hepatomegaly and widespread cutaneous and lymph node metastases.
Post-mortem showed a fairly well differentiated hepatoma in the right lobe of the liver with a few nodules in the left
lobe. It had extended down the portal vein and into the splenic vein almost to the spleno-renal anastomosis. Metastases were present in the lungs, ribs and spine, lymph nodes and skin. Tumour cells also infiltrated the serosal lymphatics of the stomach.
Case 8.--F.J.E., a girl aged 9, was admitted for investi- gation of areas of yellow (xanthomatous) pigmentation in the skin creases. She was found to have moderate hepatic and splenic enlargement and a mild elevation of the serum bilirubin level. Bone marrow biopsy revealed numerous foana cells resembling those seen in Niemann Pick disease or in essential familial hyperlipaenqia, but specific stain for Niemann Pick disease were negative. The serum cholesterol was 1500 rag. per 100 ml. Liver biopsy showed gross fatty change in the liver cells. In spite of dietary modification, no improvement in the levels of lipids in the serum occurred. She remained reasonably well for several months but was later readmitted with left subcostal pain. Tuberous lesions had now appeared on the extensor surfaces of the elbows.
Her general condition deteriorated quickly, with the develop- ment of obstructive jaundice, marked abdominal distension and oedema. An inferior vena eavogram showed no obstruc- tion or displacement, but a portal venogram revealed com- plete blockage of the vein close to its origin from the splenic and superior mesenteric veins. She died 6 months after he," initial admission without the correct diagnosis having been established.
At post-mortem, the liver, which was markedly enlarged, was largely replaced by confluent masses of yellow tumour tissue. The radicles of the portal vein were distended with tumour tissue and this extended several centimetres down the portal vein below the liver. Histologically the tumour was a well differentiated hepatoma. Widespread intra- vascular tumour emboli were present in the lungs.
Case 12.--B.M., a girl of 9 months, was admitted for investigation of an abdominal mass present for one month.

H E P A T I C TUMOURS IN C H I L D H O O D 77
FIG. 3A; FIG. 3B
Case 12. Barium meal. The stomach is pushed upwards and forwards by a large mass beneath and behind it, with stretching of the proximal duodenum. This tumour was a pedunculated hepatoblastoma.
A rounded mobile lump was present in the mid-abdomen. The haemoglobin level was 9"3 g. per 100 nal.
Radiological Findings.--A chest radiograph and skeletal survey were normal. An intra-venous pyelogram demon- strated an 11 em. rounded mass lying in front of the left kidney which was displaced a little posteriorly. No calcifi- cation was present. A barium meal showed the body and pyluric end of the stomach to be lifted upwards and forwards (Fig. 3, A and B), with some stretching of the proximal duo- denum, but with the second part in a relatively normal position. The appearances were considered to indicate an intra-abdominal mass, possibly a mesenteric cyst or redupli- cation cyst.
At laparotomy a large vascular mass was found projecting from below the stomach, encapsulated and attached by a narrow pedicle to the liver just posterior to the porta hepatis. Large vessels passed to the tumour along its pedicle. The operative diagnosis was haemangioma of the liver. Histo- logical examination revealed the tumour to be a hepatoblas- toma. Removal was thought to be complete and the patient remains well during a brief follow-up period. A post-opera- tive selective coeliac axis arteriogram was performed (Fig. 4), but it revealed no evidence of other tumour in the liver.
in 4 patients. Calcification within the t umour could be seen in only one patient, the eldest, and was in the form of several small nodules.
Excretion pyelography was carried out in 9 patients. In 2 the appearances were normal . In the remainder there was posterior displacement of the relevant kidney, usually the right, indicating an in t ra-abdominal site for the mass. Associated
R A D I O G R A P H I C F E A T U R E S
Abdominal . - -Eleven patients had plain radio- graphs of the abdomen. I n all there was a mass present in the upper abdomen. In 10 it was mainly right sided, in one it was left sided bu t mobile and in one the spleen was also large. The diaphragm showed a localised deformity in 5 patients (Fig. 5, A and B) and in 4 there was only a generalised elevation. The lower margin of the mass had a characteristic undula t ing border (Margulis et al.)
Fro. 4 Case 12. Coeliac axis arteriogram. There is no evidence of residual tumour. The left hepatic artery has been occluded
and distal filling occurs via collaterals.

78 C L I N I C A L R A D I O L O G Y
F ~ . 5A Fro. 5B
Case 11. There is local elevation and deformity of the right hemi-diaphragm by the mass in the right lobe of the liver.
with this there was often some compression of the calyces and pelvis antero-posteriorly, and slight inferior displacement of the kidney (Fig. 6, A and B).
Barium studies of the upper gastro-intestinal tract was performed in only 3 patients. In 2 the stomach showed displacement inferiorly, posteriorly and to the left. In the other, Case 12, the pedun- culated tumour displaced the body and pyloric
end of the stomach upwards and anteriorly, with consequent stretching of the first part of the duodenum (Fig. 3, A and B). A similar pedun- culated malignant hepatoma was described by Pirie (1932) in a girl of 11 years. In 5 other patients displacement of the stomach to the left could be identified in plain films.
Two patients had trans-splenic portal venography performed. In both, cases 7 and 8, the diagnosis

H E P A T I C T U M O U R S I N C H I L D H O O D 79
FIG. 7 ,
Case 7. Por ta l venogram. The por ta l vein is obst ructed at its origin, wi th filling of col la teral pathways. The obs t ruc t ion is irregular, and was la ter shown to be due to t umour
extension down the por ta l vein.
was obscure and the mode of presentation unusual. Both showed blockage of the portal vein close to its commencement (Fig. 7) and no filling of the hepatic branches. An operative cholangiogram performed in Case 7 to elucidate his obstructive jaundice also revealed only a blockage of the common hepatic duct.
Inferior vena cavography was carried out in seven patients by percutaneous catheterisation of a femoral vein. In one no abnormality was shown. In 4, there was complete blockage of the vena cava between the second and fourth lumbar vertebral levels (Fig. 8, A and B). In a sixth patient there was an incomplete obstruction at the second lumbar level. The remaining patient showed only narrowing of the vena cava from side to side in its course through the hepatic groove. It was not possible to distinguish reliably between intrinsic involvement and obstruction from simple compres- sion by the mass, the latter being more usual.
The most informative diagnostic method was arteriography, and such studies were available in 5 patients. In every case in which it was employed an abnormality was present which enabled the correct diagnosis to be suggested. Depending on
80 C L I N I C A L R A D I O L O G Y
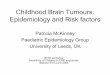
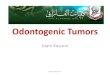
FIG. 9 F~G. 10
FIG. 9 Case 10. Aortogram. The coeliac axis is dislocated to the left, the branches of the right hepatic artery are stretched and a network of tnmour vessels is seen. FIG. I0 Case 11. Hepatic arteriogram. There is stretching of the branches of the right hepatic
artery, with tumour vessels visible in the lower part of the mass.
the size of the patient either aortography or selective arteriography via the coeliac axis (Hiller, 1966) was performed using the usual percutaneous .catheterisation technique via the femoral artery under basal sedation. Stretching of the appropriate branches of the hepatic artery was invariably seen, with a typical pathological circulation within the tumour mass (Figs. 2, 9 and 10). A further patient, Case 12, aged nine months, with the tumour recognised after laparotomy, had a selective ~coeliac axis arteriogram performed post-operatively, but:no further tumour mass was seen, though it was ~apparent that the left branch of the hepatic artery had been occluded at the time of the operation (Fig. 4).
Metastases.---In 2 patients, multiple small rounded metastases were present in the lungs at the time of their initial investigation. No special features were noted. Several other patients developed multiple pulmonary deposits during the course of their disease and one a massive malignant pericardial effusion. In one patient an osteolytic metastasis developed in the humerus. Localised bony metastasis is not usual i n hepatoma and its occurrence in adult patients has been reviewed by Carnahan (1950).
Other Features.--A striking degree of osteo- porosis was present in two patients (aged 10 and
18 months), with large tumours and with pulmon- ary metastases (Figs. 1, A and B, and 11, A and B). If affected the skeleton diffusely and was associated with only short periods of preceding ill health. Bone marrow examination did not reveal malignant infiltration, nor was this present at autopsy. Review of the other cases showed moderate osteoporosis, (especially spinal) in 3, and milder changes in 4 others. The severity of the condition tended to progress during the course of the disease.
DISCUSSION
Liver tumours in children fall, from a diagnostic viewpoint, into three main groups. (a) Those with a typical history and typical physical findings (e.g. Case 6), where the problem is to confirm the diagnosis and determine the extent of the tumour. (b) Those with unusual abdominal masses where the problem is that of establishing the site and nature of the lesion as well as its extent (e.g. Case 12). (c) Those where the clinical features are due to the metabolic disturbances associated with liver tumours, i.e. disturbances of protein and lipid metabolism (e.g. Case 8). However, hepatic enlarge-

H E P A T I C TUMOURS 1N C H I L D H O O D 81
ment is usually present and investigation of the cause of this may lead to the diagnosis.
The findings on plain radiography, barium study and excretion pyelography confirm the observations of Margulis et al. (1956) that these tumours can be clearly distinguished from the commoner retro- peritoneal masses of childhood. Tumour calcifica-
tion, however, was seen only once in the present 12 patients, whilst Margulis et al. identified it 3 times in their 11. The association between liver disease and osteoporosis was not discussed by these authors. In two of the present series it was sufficiently severe to cause vertebral collapse and in one there were femoral fractures after minor
FIG. 12A FIG. 12B
Case 6. Same patient as Fig. 1. The osteoporosis has become more severe in the intervening eight weeks. The pulmonary metastases are now obvious and the diaphragm is further elevated by the enlarging liver.

82 C L I N I C A L R A D I O L O G Y
trauma. Though both of these patients had pulmonary metastases, there was no evidence o f bone metastases. Osteoporosis in liver disease in children has been reviewed by Ching Tseng Teng, Doesclmer, Singleton, Rosenberg, Cole, Hill and Brennan (1963) and has been described previously by Hansen, Zeigler and McQuarnel (1940) and by Roberts and Sullivan (1955). The former authors described their findings in primary hepatic turnouts, glycogen storage disease and hepatic cirrhosis. Of 9 children with tumours, 6 showed osteoporosis and in 3 it was of severe degree. Such tumours are not always malignant and in one the changes regressed after treatment of the tumour by partial hepatectomy. They ascribed it to relative protein deficiency from loss of functioning fiver tissue and found the serum proteins to be low when osteo- porosis was present, though in Case 6 of the present series the total serum protein level of 8-6 G. per 100 ml. was within the normal range. The patient recorded by Hansen et al. (1940) with primary liver carcinoma showed osteoporosis in association with disturbed lipid metabolism characterised by hyperlipaemia and hypercholesterolaemia. Roberts and Sullivan (1955) described 2 patients, one with cirrhosis, possibly following hepatitis, and severe osteoporosis, and one with primary liver carcinoma in whom there was an episode of severe osteoporosis which cleared up and did not recur despite progres- sion of the disease. It is of interest that the patient in this series with disordered lipid metabolism, Case 8, showed only mild to moderate osteoporosis. Whatever the mechanism, it is clear that the signific- ance of osteoporosis is very different from that in other malignancies such as neuroblastoma, where it usually implies diffuse infiltration.
In this department the majority of children with abdominal tumours are subjected to arteriographic studies. It is believed that the information derived is of value both in diagnosis and management. Radiotherapy and chemotherapy are of little value in the treatment of hepatic tumours and the best hope for cure would at present seem to lie in earlier and more adequate surgery. The arterio- graphic demonstration of the anatomy of the turnout is of value in assessing tl~e feasibility of partial hepatectomy, as well as in disclosing the
cause of obscure hepatic enlargement. The material presented here confirms the value of this procedure in establishing the nature and extent of intra- hepatic masses, as shown in adults by Boijsen and Abrams (1965). Portal venography has been of little diagnostic help, though the present limited experience suggests that demonstration of a complete block of the vein indicates tumour extension down it. Inferior vena cavography has also proved of little help as complete obstruction is frequently due only to pressure from these often very large turnouts and actual invasion cannot be reliably differentiated.
CONCLUSIONS
1. Primary hepatic tumours in children can be accurately identified prior to laparotomy, so that their management may be planned.
2. Angiographic studies are of value in demonstrating the nature of a hepatic mass and in assessing the feasibility of its removal.
3. Osteoporosis is not uncommon in association with hepatic tumours and it may be of sufficiently severe degree to lead to vertebral collapse and fracture from minor trauma. It does not imply skeletal metastasis.
Aeknowledgements.--The author is indebted to the physi- cians and surgeons of The Royal Children's Hospital, Mel- bourne for access to the notes of their patients, and to the Photographic Department for the illustrations.
REFERENCES
BOIISEN, E. t~; ABRAMS, H. L. (1965). Acta radioL (Stockh.), 3, 257.
BOUCHIER, I. A. D. & LESSOE, L. (1964). Brit. J. RadioL, 37, 34.
CARNAUAN, D. S., Jnr. (1950). Radiology, 55, 844. HANSEN, A. E., ZIGLER, M. R., & McQUARNEL, L (1940).
J. Pediat., 17, 9. ]'IILL, L. L. t~ BRENNAN, J. C. (1961). J. Pediat., 59, 684. HILLER, H. G. (1966). In preparation. MARGULIS, A. R., NICE, C. M., & RIGLER, L. G. (1956).
Radiology, 66, 809. PINE, G. R. (1932). Canad. uted. Ass. J., 27, 401. ROBERTS, M. H. & SULLIVAN, C. (1955). a r. Amer. med. Ass.,
159, 1002. TENG, C. T., DOESCHNER, C. W., SINGLETON, E. B., ROSEN-
BERG, H. S., COLE, V. W., HILL, L. L., & BRENNAN, J. C. (1961). J. Pediat., 59, 684.