Embed Size (px)
Citation preview

Here is what Step 1 covers- did we get them all?
• Production/function granulocyte, NK cells and macrophages/DC• Production/function of T cells, TCR, cytokines/chemokines• Production/function of B cells and PC, Ig structure, classes, molecular
basis for specificity, receptors• Antigenicity/immunogenicity, host defenses(read Innate I),
primary/secondary responses, passive transfer of immunity(all ways)• In vitro complement, other diagnostic tests and antigen antibody
reactions• Mediators, complement, aa, histamine, NO and cytokines• MHC structure and function, RBC antigens. Transplantation• Vaccines, protective immunity, tumor immunity• Disease states like ID, HIV and pharmacological immunosuppression

INNATE IMMUNITY
• NOT ANTIGEN SPECIFIC
• HAS NO MEMORY
• MEDIATED BY
– NEUTROPHILS
– MACROPHAGES/MONOCYTES
– NATURAL KILLER CELLS
– EOSINOPHILS
– BASOPHILS/MAST CELLS
– MANNOSE BINDING PROTEIN AND COMPLEMENT
– PROSTAGLANDIN & KININ SYSTEMS
INDISCRIMINATE DESTRUCTION


PRO-INFLAMMATORY CYTOKINES
ADAPTIVE IMMUNITY
• ANTIGEN SPECIFIC
• CLONAL EXPANSION
• AMPLIFIES AN IMMUNE RESPONSE AFTER A SPECIFIC RECEPTOR INTERACTION
• INTEGRATES THE INNATE RESPONSE INTO THE REACTION
• MEMORY OF THE ENCOUNTER
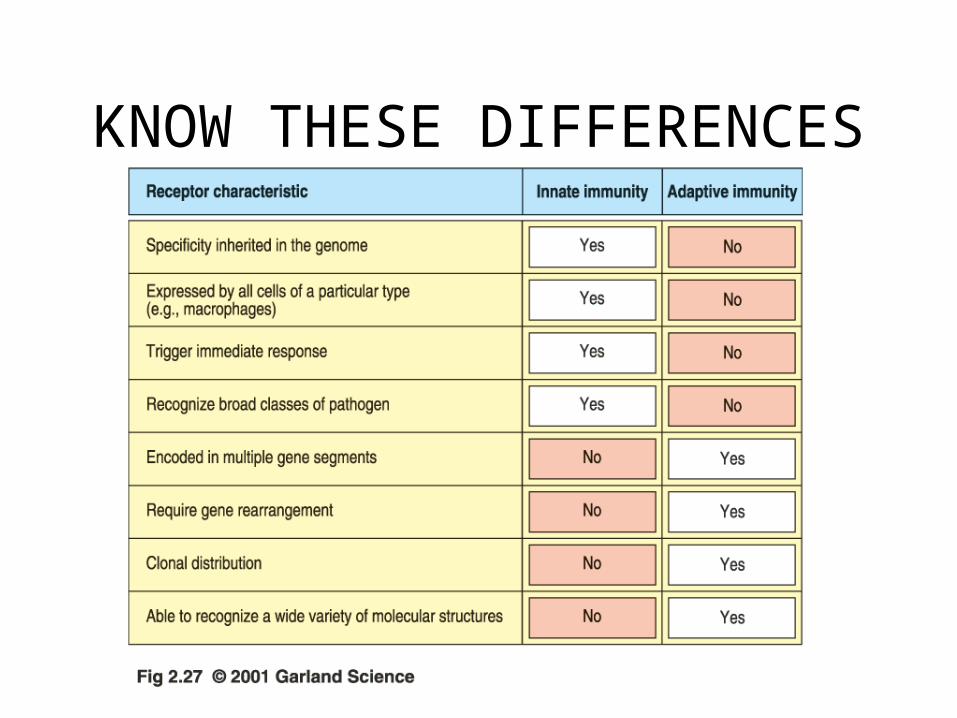
KNOW THESE DIFFERENCES

ANATOMY OF THE IMMUNE SYSTEM
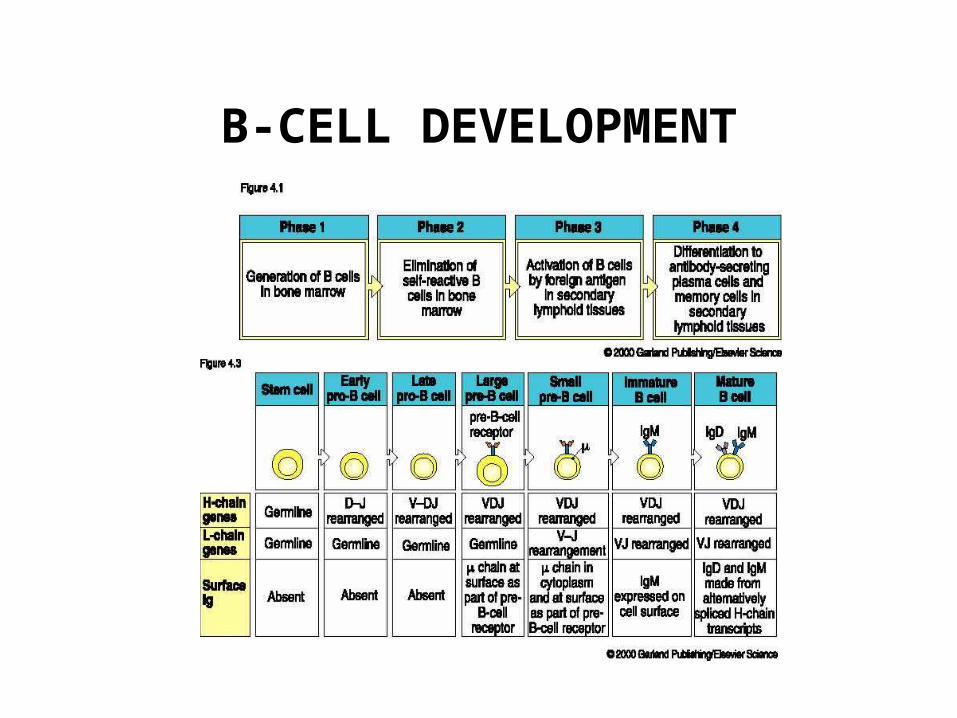
B-CELL DEVELOPMENT

ANTIBODY STRUCTURE

ANTIBODY FUNCTIONS

ANTIBODY FUNCTIONS

COMPLEMENT
• FLUID PHASE AMPLIFIER OF INNATE AND ANTIBODY MEDIATED RESPONSES
• THREE ARMS– ALTERNATE-BACTERIAL CELL WALLS
– MANNOSE BINDING-BACTERIAL CELL WALLS and MBP
– DIRECT(CLASSIC)-SPECIFIC Ag/Ab REACTIONS

COMPLEMENT
COMPLEMENT
• ENZYME ACTIVATED CASCADE WITH GENERATION OF INFLAMMATORY AND REGULATORY FRAGMENTS
• ACTIVATES INFLAMMATORY CELLS BY SPECIFIC RECEPTOR INTERACTIONS
• HAS IMPORTANT IMMUNOREGULATORY AND IMMUNE COMPLEX DISPOSAL ROLES
• Measured by serum C3 and C4, total hemolysis and individual components

COMPLEMENT-RELATED DISEASES
• Rare• C1esterase deficiency with angioneurotic
edema-• Deficiencies in the direct sequence associated
with IC diseases like SLE• Homozygous C3 is lethal• Deficiencies in the alternate path very rare• Individual component deficiency after C5
associated with Neisserial bacteremia

ANTIGEN PRESENTING CELLS

MHC

T-CELL DEVELOPMENT
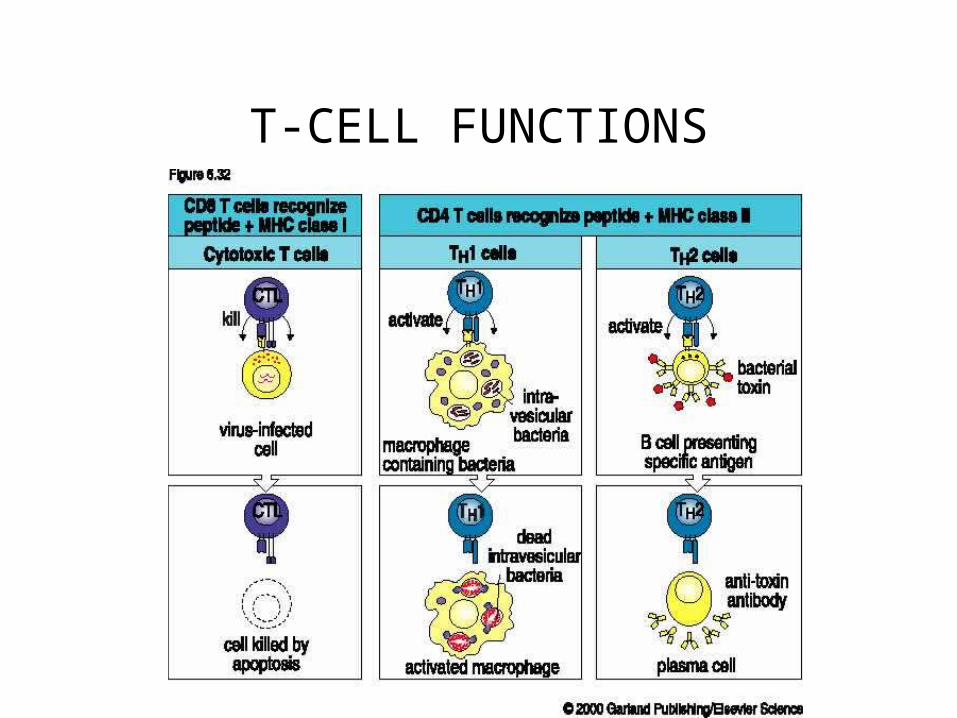
T-CELL FUNCTIONS
QUESTIONS
• From stem cell to T cell
• why the thymus
• CD4 versus CD8
• gamma delts versus alpha bets
• peripheral blood
• CDs to remember……….– 3,4,8,25,19,16,20,
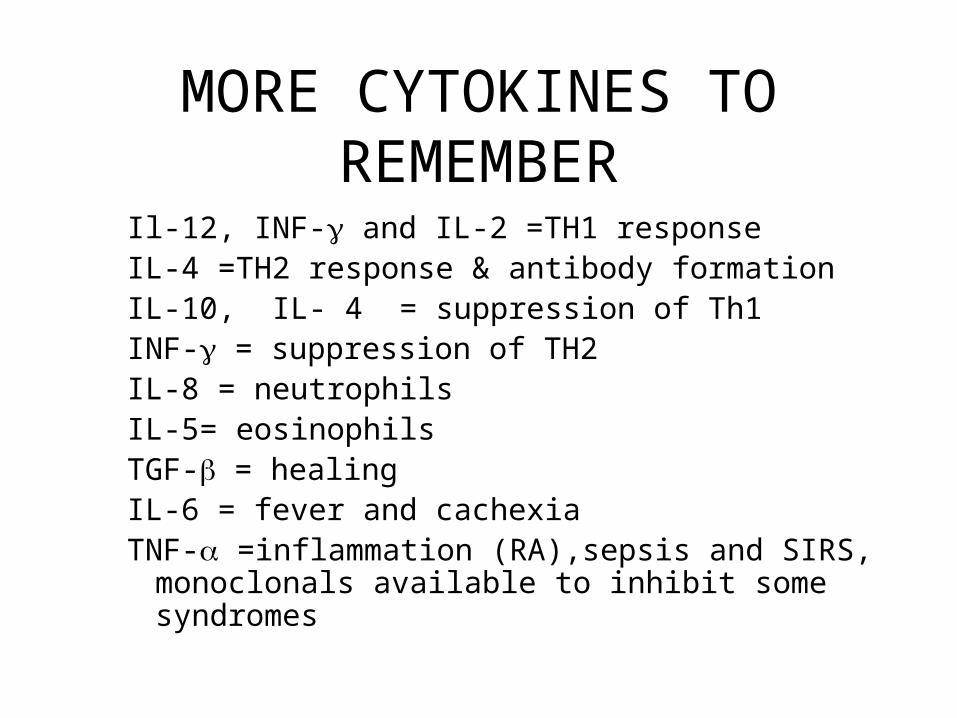
MORE CYTOKINES TO REMEMBER
Il-12, INF- and IL-2 =TH1 responseIL-4 =TH2 response & antibody formationIL-10, IL- 4 = suppression of Th1INF- = suppression of TH2IL-8 = neutrophilsIL-5= eosinophilsTGF- = healing IL-6 = fever and cachexiaTNF- =inflammation (RA),sepsis and SIRS,
monoclonals available to inhibit some syndromes

MHC
• Co-dominant alleles
• Present on Chromosome 6 in humans
• A,B,C loci are Class I
• D loci are class II and control immune responses and rejection

MLC

TRANSPLANT TYPES
• Autograft
• Isograft
• Allograft (also known as Homograft)
• Xenograft
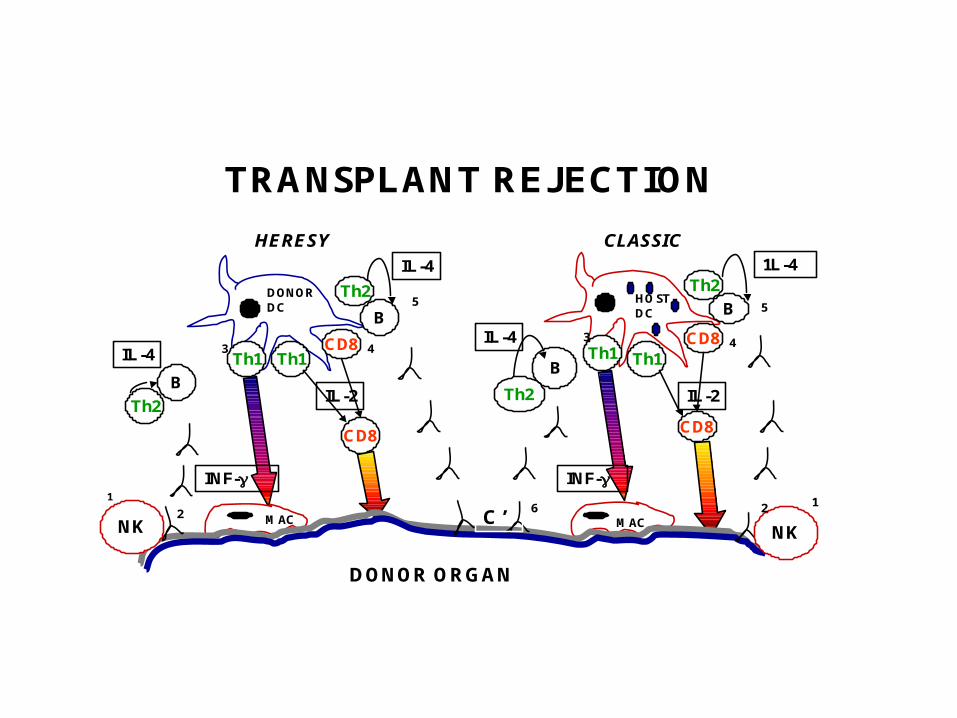
TRANSPLANT REJECTION
Th2 Th2
B B
CD8 CD8Th1 Th1
BB
DONORDC
HOSTDC
CLASSICHERESY
CD8
IL-2Th2
IL-4
IL-4
Th2
IL-4
1L-4
CD8
IL-2
Th1 Th1
C’NK NK
DONOR ORGAN
1
2 6
3 4
5
12
3 4
5
INF- INF-
MAC MAC

IMMUNOSUPPRESSION
• Corticosteroids-inhibit NFB
• Cyclosporine-inhibit T-cell activation
• Tacrolimus- inhibit T-cell activation
• Rapamycin- block IL-2 receptor activation
• Anti-cytokine/ligand monoclonals

PREDICT THE TYPE OF INFECTION
• Pure B cell…encapsulated bacteria and systemic spread of GI viruses..frequent after 6 mos of age
• “pure” T cell….TB, fungi, pneumocystis since helper function is lost…occurs at birth. B cell infections will not occur until maternal antibody gone-approx 6 mos
• B & T cell..at birth, severe and fatal if not transplanted
• CGD –neutrophil inability to kill bacterial that produce catalase..esp staph
• cytokine..IL-12, Interferon gamma, IL-4

DISEASES ASSOCIATED WITH T-CELL DEFICIENCY
• HIV/AIDS
• THYMIC APLASIA
• SENESCENCE
• BIRTH
• WISKOTT-ALDRICH
• ATAXIA-TELANGIECTASIA
• TREATMENT

DISEASES ASSOCIATED WITH B-CELL DEFICIENCY
• X-LINKED AGAMMAGLOBULINEMIA
• COMMON VARIABLE IMMUNODEFICIENCY
• SELECTIVE IgA DEFICIENCY• CLL• HYPER IgM SYNDROME• TREATMENT

DISEASES ASSOCIATED WITH T & B CELL DEFICIENCY
• SCID
• THERAPY:– STEM CELL TRANSPLANTS– BMT– GENE REPLACEMENT- recent problems with
the retroviral vector insertion has led to leukemia

TESTING IMMUNE FUNCTION
• B-CELLS– SERUM IG LEVELS– ELECTROPHORECTIC DETECTION OF
CLONALITY– ENUMERATION OF B-CELLS– DETECTION OF SPECIFIC ANTIBODIES– IMMUNOHISTOPATHOLOGIC

Know your Flow!

TESTING IMMUNE FUNCTION
• T-CELLS– IN VIVO SKIN TESTING- will not be valid in
patients with malnutrition, on steroids etc– ENUMERATION OF T-CELLS-can be
misleading because doesn’t reflect tissue distribution
– IMMUNOHISTOPATHOLOGIC– IN VITRO FUNCTIONS- rarely needed

HYPERSENSITIVITY REACTIONS
• TYPE I- Atopy, asthma & anaphylaxis
• TYPE II-Antibody to cell structures-immune thrombocytopenia, AIHA
• TYPE III- Immune complex diseases-SLE is prototype
• TYPE IV- Delayed hypersensitivity-sarcoidosis

AN ALLERGIC REACTION
MASTCELL
MASTCELL
Th2
B CELL
LATE
EARLYORACUTE
DENDRITIC CELL
EOS
IL-5
IL-5
IL-4
IL-4
IgE
VASOACTIVE MEDIATORS
ALLERGEN

ALLERGY MEDIATORS

ASTHMA

Asthma
• Limited early exposure to infections-so-called hygiene hypothesis
• Obesity
• Genes– Maternal 11 for IgE increase– T-bet gene abnormalitiesfor deficient INF-– IL-13
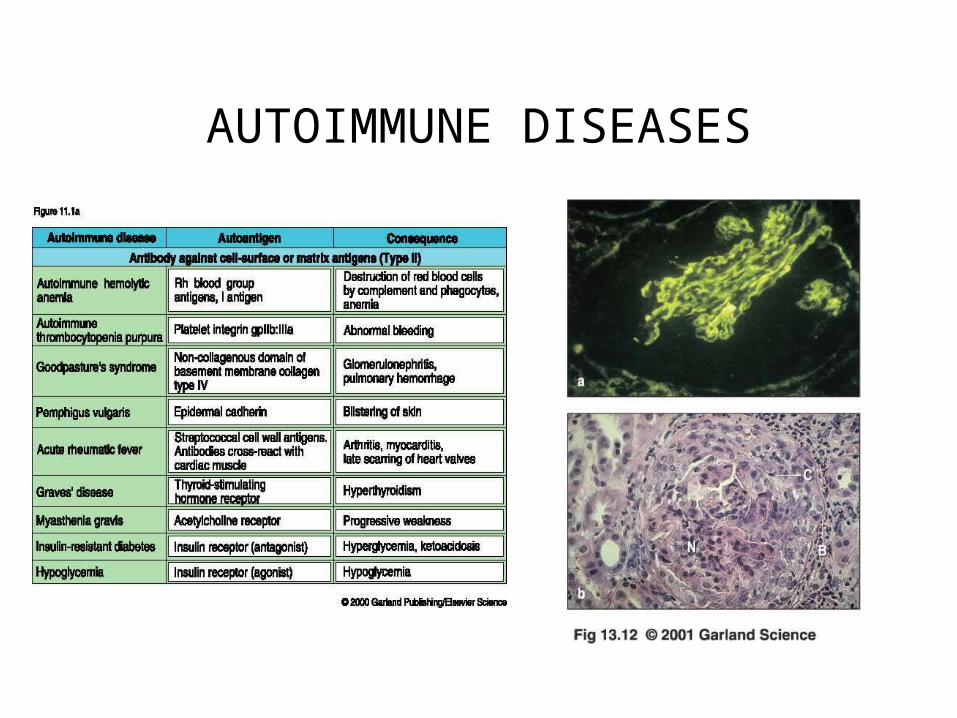
AUTOIMMUNE DISEASES
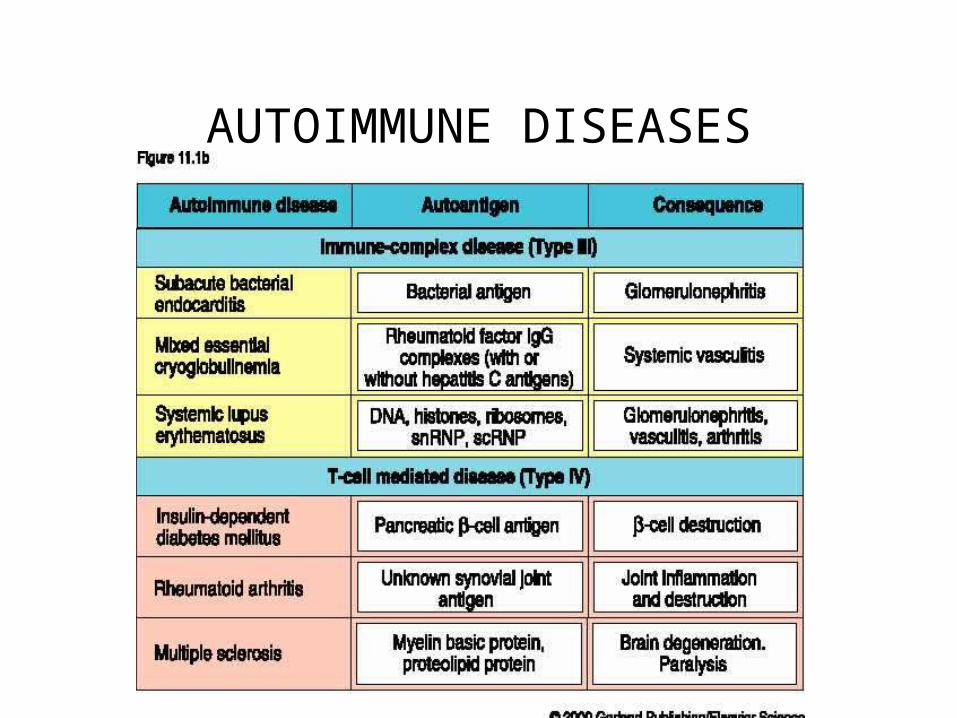
AUTOIMMUNE DISEASES

IMMUNE COMPLEX DISEASE-AKA SERUM
SICKNESS
AUTOANTOBODIES
• SLE- – ANA is a SCREENING TEST ONLY(HIGH
SENSITIVITY, LOW SPECIFICITY)– double stranded(ds/native) DNA correlates loosely with
renal disease, very specific – Sm very specific for SLE-low sensitivity– Histone- present in drug induced lupus but also SLE
and other diseases– Ribonucleoprotein (RNP)- associated with mixed
connective tissue disease

AUTOANTOBODIES
– ANCA• cANCA high specificity for Wegeners
Granulomatosus
• pANCA found in some glomerulonephritis, microscopic vasculitis and other vasculitis
Polymyositis/Dermatomyositis……anti-JO-1
SS-A(Ro)/SS-B(La)- Sjogren syndrome, congenital heart block

MORE AUTOANTIBODIES
• Scleroderma– SCL-70( aka anti-topoisomerase) specific but
very low sensitivity– Centromere-high sensitivity for CREST(limited
scleroderma) and codes for presence of pulmonary hypertension

Other Autoantibodies to remember
• AntiAcR- myasthenia
• Anti-endomysial- Sprue (anti gliadin)
• Rheumatoid factor- not specific for RA

Acute Phase reactants
• C-reactive Protein- • Most accurate indicator of an inflammatory reaction • Proxy for IL-6• May correlate independently of Lipids for CA• High likelihood something about CRP will be on
Boards!..especially as independent indicator of coronary artery disease
Transferrin, ceruloplasmin, C3, haptoglobin increase with infection, albumin and hemoglobin decrease

HLA ASSOCIATIONS WITH SPECIFIC DISEASES
• Ankylosing spondylitis-B27……………….90RR*
• Reactive Arthropathy-B27.………………...40
• Rheumatoid Arthritis-DR4.………………...4
• Behcet’s-B51.………………………………4
• SLE-DR3.…………………………………..6
• IDDM-DR3,4……………………………….6
• Dermatitis Herpetiformis-DR3.…………….16
• MS-DR2…………………………………….4
• Goodpastures-DR2…………………………16
• Birdshot Retinochoroidopathy-A29.……….109**– *…remember the caveats, ** …..for that extra point

TERMS TO REMEMBER
• ANTIGEN
• IMMUNOGEN
• EPITOPE
• HAPTEN
• ADJUVANT
• STEM CELLS
• PRIMARY AND SECONDARY IMMUNE RESPONSE

TERMS TO REMEMBER
• INNATE(AKA NATURAL)
• ADAPTIVE(SPECIFIC OR ACTIVE)
• CELL-MEDIATED IMMUNITY
• HUMORAL/ANTIBODY IMMUNITY
• PASSIVE IMMUNIZATION
• ACTIVE IMMUNIZATION
• ARTHUS REACTION

TERMS TO REMEMBER
• ISOTYPE
• IDIOTYPE
• MONOCLONAL
• SYNGENEIC
• ALLOGRAFT
• AUTOGRAFT
• ELISA & RIA

Here is what Step 1 covers- did we get them all?
• Production/function granulocyte, NK cells and macrophages/DC• Production/function of T cells, TCR, cytokines/chemokines• Production/function of B cells and PC, Ig structure, classes, molecular
basis for specificity, receptors• Antigenicity/immunogenicity, host defenses(read Innate I),
primary/secondary responses, passive transfer of immunity(all ways)• In vitro complement, other diagnostic tests and antigen antibody
reactions• Mediators, complement, aa, histamine, NO and cytokines• MHC structure and function, RBC antigens. Transplantation• Vaccines, protective immunity, tumor immunity• Disease states like ID, HIV and pharmacological immunosuppression
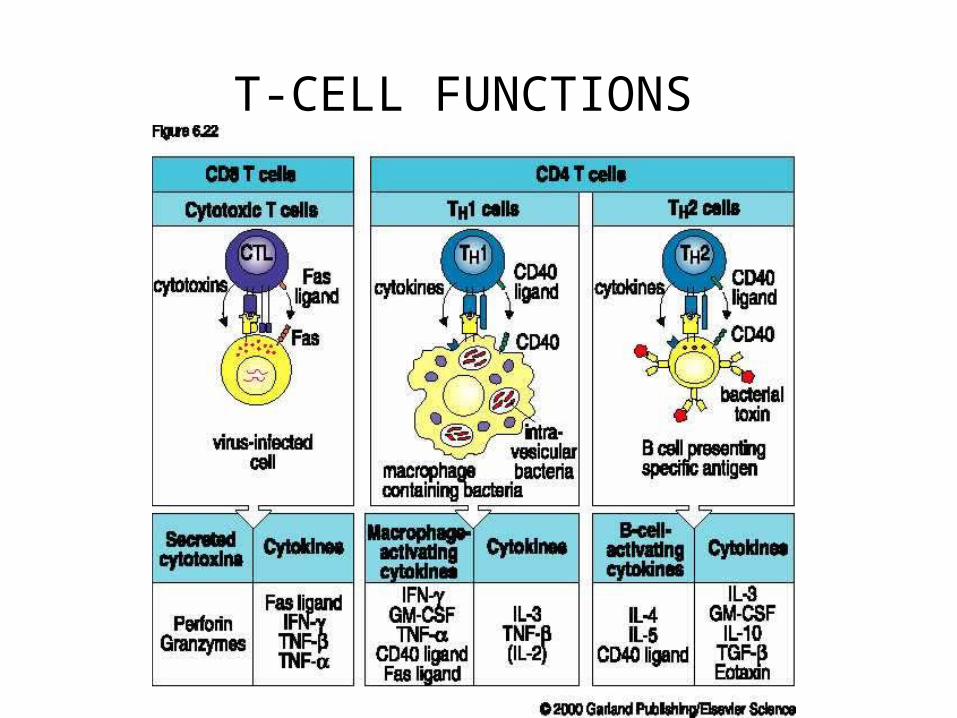
T-CELL FUNCTIONS

Isotype switching