Embed Size (px)
Citation preview

Hereditary gingival fibromatosis:Review of the literature and a case reportLarissa Perales Bittencourt, DDS, MDSWera Campos, DDS, MDSVLuiz Flávio Martins Moliterno, DDS, MDSVDanilo Passeado Branco Ribeiro, DDSVRenato Kobler Sampaio, DDS, MDS'
Hereditary gingival fibromatosis is a proliferatiue fibrous lesion of the gingival tissue thai causes estheticand functional problems. Both genGtically and pharmacologically induced forms of gingival fibromatosisexist. This paper reports a case of severe generalizGd hereditary gingival fibromatosis in a 5-year-old girl.Treatment consisted of surgical removal of the hyperplastic fibrous tissue in a series of conventional gin-givectomies. Postoperative examination 35 months after Ihe final procedure revealed no signs of recur-rence. (Quintessence Int 2000:31:415-418)
Key words: gingivectomy, hereditary gingival fibromatosis, idiopathic fibromatosis, primary dentition
T" Jereditary gingiva! fibromatosis, also known as idio-llpathic gingival fibromatosis,'~^ is defined as a rare,benign, asymptomatie, nonhemorrhagic, and nonexuda-tive proliferative fibrous lesion of the gingival tissue. Itoccurs equally among men and women, in both arches,varying in intensity in individuals within the same iam-i[y2,6-i7 Hereditary gingival fibromatosis is usually identi-fied as an autosomal-dominant condition,'•-•*''^'^'^'''=-'*although recessive forms are described in the litera-ture,'"''"'^'' Consanguinity seems to increase the risi< ofautosomal-dominant inheritance,^'"'*
Hereditary gingivai fibromatosis may appear as anisolated disorder, but in some cases it is associated withother alterations, such hypertrichosis and epilepsy. It issometimes associated with other syndromes, such asZimtnerman-Laband, Murray-Puretic-Drescher, Cow-den's, Cross, and prune-belly,*•'•"'• "'̂ '̂̂ ^ Oiifarinen andcolleagues,^" Bozzo and colleagues,'* and Grinspan'suggested that there may be a relationship betweengrowth hormone deficiency and gingival overgrowthwhere dental and skeletai alterations are present alongwith gingiva! fibroblasts.
The hyperpiastic gingiva usually is roseate, has afirm consistency, and has abundant stippling on theadjacent gingiva. This anomaly is classified in 2 typesaccording to its form. The first, the nodular form, is
''Private Practice, Rio de Janeiro, Brazil,
Reprint requests: Dr Larissa Perales Bitlencourt, Cruz Lima, 33/303,Flamergo, CEP 23030-010, Rio de Janeiro, Brazil. E-mail: mneto®buriti,com.br
characterized by the presence of multiple tumors inthe dentai papillae. The other form, the symmetricform, results in uniform enlargement of the gingivaand represents the most common type. Both formsvary in shape and volume and may cover the dentaicrowns. There may be a combination of the 2 types. Inmany cases, there is an exaggerated growth in thetuherosity region.'"
Gingival tissue enlargement usually begins witheruption of the permanent dentition but can developwith the eruption of the primary dentition. It is rareiypresent at birth,-'" According to a study of Brazilianpatients, gingival enlargement occurs mainly in themixed dentition and may worsen when girls have theirfirst menstrual period,* Enlargement seems to progresssuddenly during "active" tooth eruption and decreasewith the end of this stage,""' According to a number ofresearchers,'-^'''''^ hereditary gingival fibromatcsis isan atypical disease of infants,
Histologicaily, the fibrous connective tissue hasbundles of coarse collagenous fibers and a high degreeof differentiation with young fibroblasts and scarceblood vesseis. The epitheiium is dense with elongatedpapulae and hyperkeratosis. The more fihrohlasts thereare, the greater the chance of recurrence. '̂''̂ '"'=
The most common effects related to the lesion arediastemas, maipositioning of teeth, and prolongedretention of primary teeth. More severe lesions maycover the dental crowns. Hereditary gingival fibro-matosis results in both esthetic and functionalproblems,'-"'*'"''^'^'^''*'^'-^^ Although gingival hyper-plasia occurs, the alveolar hone is not alfected.̂ '̂ ''"'̂
Quintessence I niernational 415
• Bitlencourl el al
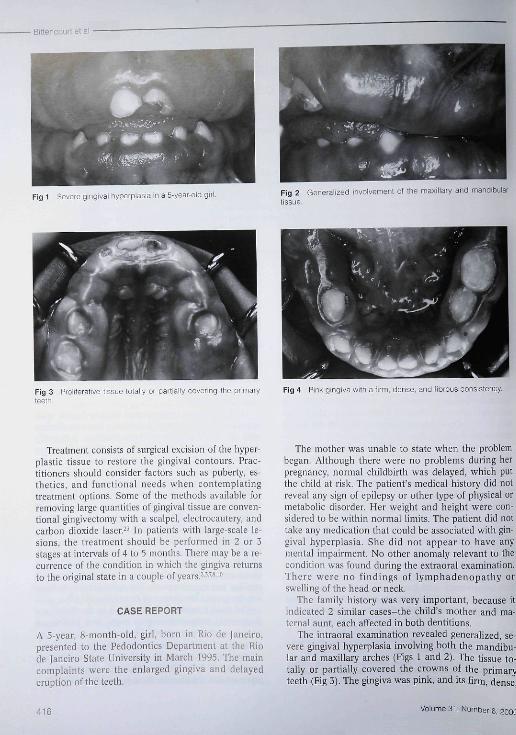
Fig 1 Severe gingival hypeiplasia in a 5-year-old girl. Fig 2 Generalized involvement of Lhe maxillary and mandibular[issue
Fig 3 Proliferative tissue totally or partially covering lhe primaryteeth.
Fig 4 Pink gingiva with a firm, dense, and fibrous consistency
Treatment t;onsists of surgical excision of the hyper-plastic tissue to restore the gingival contours. Prac-titioners should consider factors such as puberty, es-thetics, and functional needs when contemplatingtreatment options. Some of the methods availahle forremoving large quantities of gingivai tissue are conven-tional gingivectomy with a scalpel, electrocautery, andcarbon dioxide laser.̂ ^ In patients with large-scale le-sions, the treatment should be performed in 2 or 3stages at intervals of 4 to 5 months. There may be a re-currence of the condition in which the gingiva returnsto the original state in a couple of years,-'"'*'"
CASE REPORT
A 5-year, S-month-old, girl, horn in Rio de Janeiro,presented to the Pedodontics Department at the Riode (aneiro State University in March 1995, The maincomplaints were the enlarged gingiva and delayederuption of the teeth.
The mother was unahle to state when the problembegan. Although there were no problems during herpregnancy, normal childbirth was delayed, which putthe child at risk. The patient's medical history did notreveal any sign of epilepsy or other type of physical ormetabolic disorder. Her weight and height were con-sidered to be within normal iimits. The patient did nottake any medication that could be associated with gin-gival hyperplasia. She did not appear to have anymental impairment. No other anomaly relevant to thecondition was found during the extraoral examination.There were no findings of lymphadenopathy orswelling of the head or neek.
The family history was very important, because itindicated 2 similar cascs-the child's mother and ma-ternal aunt, each affected in both dentitions.
The intraoral examination revealed generalized, se-vere gingival hyperplasia involving both the mandibu-lar and maxillary arches (Figs 1 and 2), The tissue to-tally or partially covered the crowns of the primaryteeth (Fig 3). The gingiva was pink, and its firm, dense.
416 Volume 31, Number 6, 200C
• Bitten court et al
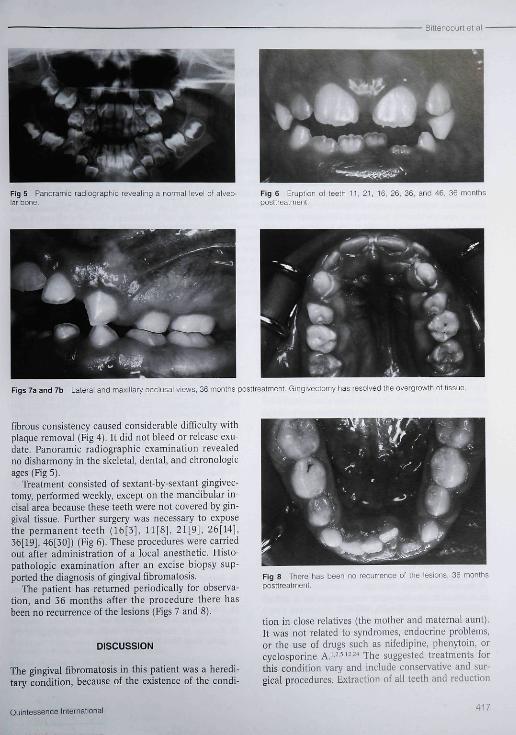
Fig 5 Panoramic radiographie revealing a normal level o' alveo-lar bone.
Fig 6 Eruption ol teeth 11, 21, 16, 26, 36, ano 46, 36 monthsposttreatment
Figs 7a and 7b Lateral and maxillary occlusal views, 36 months posttreatment. Gingivectomy has resolved the overgrowth of tissue.
fibrous consistency caused considerable difficulty withplaque removal (Fig 4), It did not bleed or release exú-date, Panoramie radiographie examination revealedno disharmony in the skeletal, dental, and ehronologicages (Fig 5),
Treatment consisted of sextant-by-sextant gingivec-tomy, performed weekly, except on the mandibular in-cisal area because these teeth were not eovered by gin-gival tissue. Further surgery was necessary to exposethe permanent teeth (16[3J, 11[S], 21[9j, 26[14],36[19J, 46[30]) (Fig 6), These procedures were carriedout after administration of a loeal anesthetic, Histo-pathologic examination after an excise biopsy sup-ported the diagnosis of gingival fibromatosis.
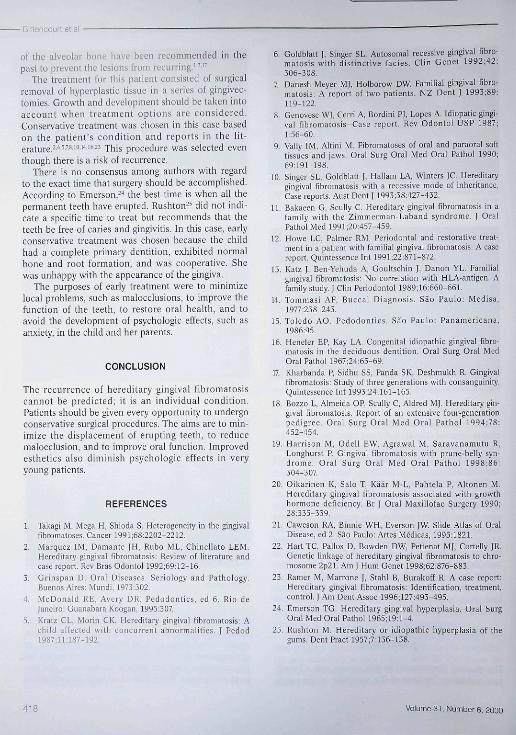
The patient has returned periodically for observa-tion, and 36 months after the procedure there hasbeen no recurrence of the lesions (Figs 7 and 8),
DISCUSSION
The gingival fibromatosis in this pafient was a heredi-tary condition, because of the existence of the condi-
Fig 8 There has been no recurrence ot the lesions, 36 monthsposttreatment.
tion in close relatives (the mother and maternal aunt).It was not related to syndromes, endocrine problems,or the use of drugs such as nifedipine, phenytoin, orcyclosporine A,^'^''^'^'' The suggested treatments forthis condition vary and include conservative and sur-gical procedures. Extraction of all feeth and reduction
Quintessenoelnternational 417
Bittencourt et ai
of tbe alveolar bone bave been recommended in thepast to prevent tbe iesions frotn recurring,'^"
Tbe treatment for this patient consisted of surgicairemoval of hyperplastic tissue in a series of gingivec-tomies. Growth and development should be taken intoaccount when treatment options are considered.Conservative treatment was cbosen in tbis case basedon tbe patient's condition and reports in the lit-erature,"5'.^'">'-'i"5 jh¡y procedure was selected eventbough there is a risk of recurrence.
There is no consensus among authors with regardto the exact time that surgery sbould he accomplisbed.According to Emerson,--' the best time is when all tbepermanent teeth have erupted. Rusiiton-' did not indi-cate a specific time to treat but recommends that theteeth be free of caries and gitigivitis. In this case, eariyconservative treatment was chosen because tbe cbildhad a compiete primary dentition, exhihited normalbone and root formation, and was cooperative. Sbewas unhappy with the appearance of the gingiva.
The purposes of early treatment were to minimizeiocal problems, sucb as rnaiocclusions, to improve tbefunction of tbe teetb, to restore orai heaith, and toavoid the devciopment of psychologic effects, such asanxiety, in the child and ber parents.
CONCLUSION
The recurrence of hereditary gingival fibromatosiscatinot be predicted; it is an individuai condition.Patients sbould be given every opportunity to undergoconservative surgical procedures. The aims are to min-imize the displacement of erupting teetb. to reducemalocclusion, and to improve oral function. Improvedestbetics also diminish psychologic effects in veryyoung patients.
REFERENCES
1. Takagi M, Mega H, Shioda S. Heterogeneity in the gingivalfibromatoses. Cancer 1991;68:2202-2212.
2. Marquez IM, Damante JH, Rubo ML, Chineilato LEM.Hereditary gingival fibromatosis; Review of literature andcase report. Rev Bras Odontol 1992 ;69:12-15.
3. Grinspan D. Oral Diseases. Seriology and Pathology.Buenos Aires' Mundi, 1973:302.
4. McDonald RE, Avery DR, Pedodonties. ed 6. Rio deJaneiro. Guanabara tioogan, 1995:307.
5. Kratz CL, Morin CK. Hereditary gingival fibrotnatosis: Achild affected with concurrent abnormalities, J Pedod1987:11:187-192,
6. Goldblatt |, Singer SL. Autosomal récessive gingival fibro-niatasis with distinctive tacies. Clin Genet 1992;42:306-308.
7. Danesh-Meyer MJ, Holborow DW. Familial gingival fibro-matosis: A report of two patients. NZ Dent J 1993;89:U9-122,
8. Genovese WJ, Cerri A, Bordini PJ, Lopes A, Idiopatic gingi-val fibromatosis-Case report. Rev Odontol USP 1987;1:56-60.
9. Vally IM, Altini M. Pibromatoses of oral and paraoral softtissues and iaws. Oral Surg Oral Mod Oral Pathol 1990;69:191-198.
10. Singer SL, Goldblatt J, Hallam LA, Winters JC, Hereditarygingival fibromatosis with a recessive mode of inheritance.Case reports. Aust Dent J I993;38:427-432,
11. Bakaeen G. Scully C. Hereditary gingival fibromatosis in afamily with the Zimincrman-Laband syndrome. J OralPathol Med 1991;20:457-459.
12. Howe LC, Palmer RM. Periodontal and restorative treat-ment in a patient with familial gingival fibromatosis: A easereport. Quintessence Int 1991;22:871-872.
13. Katz J, Ben-Yehuda A, Goultschin J, Danon YL. Familialgingival fibromatosis: No correlation with HLA-antigen. Afamily study, ] Clin Periodontol 19S9;16:660-661.
14. Tommasi AF, Buccal Diagnosis. Sao Paulo. Medisa,1977:238-243.
15. Toledo AC Pedodontics. Sao Paulo: Panamerieana,1986.95,
16. Henefer EP, Kay LA. Congenital idiopathic gingival fibro-matosis in the deciduous dentition. Oral Surg Oral MedOral Pathol 1967;24:65-69.
17 Kharbanda P, Sidhu SS, Panda SK, Deshmukh R. Gingivalfibrumatosis: Study of three generations with consanguinity.Quintessence Int 1993;24:161-165,
18. Rozzo L, Almeida OP, Scully C, Aldred MJ. Hereditary gin-gival fibromatosis. Report of an extensive four-gen er ationpedigree. Oral Surg Oral Med Oral Patbol 1994;78;452-454
19. Harrison M, Odell EW, Agrawal M. Saravanamittu R,Longhurst P. Gingival fibromatosis with prune-belly syn-drome. Oral Surg Oral Med Oral Pathol 1998;86:304-307.
20. Oikarinen K, Salo T, Kääv M-L, Pahtela P, Altonen M,Hereditary gingival fibromatosis associated with growthhormone deficiency, Br J Oral Maxillofac Surgery 1990;28335-339.
21. Caweson RA, Binnit: WH, Everson JW. Slide Atlas of OralDisease, ed 2. Sau Paulo: Artes Médicas, 1995:1821.
22. Hart TC, Pallos D, Bowden DW, Petlenat M], Cortelly JR.Genetic linkage of hereditary gingival fibromatosis to chro-mosome 2p21. Am J Hum Genet 1998;62:876-883.
23. Ramer M, Marrone J, Stahl B, Burakoff R. A case report;Hereditary gingival fibromatosis: Identification, treatment,control. J Am Dent Assoc 1996;127:493-495.
24. Emerson TG. Hereditary gingival hyperplasia. Oral SurgOral Med Oral Pathol 1965;19:l-4,
25. Rushton M, Hereditary or idiopathic hyperplasia of thegums. Dent Pract 1957;7;136-138.
418 Volume 31. Number 6, 2000





























