Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, 2064–2067
Herniation of the brain after conservative treatment of alarge congenital skull defect in an infant withAdams-Oliver syndromeRalf-Bodo Tröbs a,⁎, Karin Barenberg a, Michael Hemminghaus a,Martin Günther b, Matthias Neid c
aDepartment of Pediatric Surgery, Catholic Foundation Marienhospital Herne, Ruhr-University of Bochum,Widumer Str 8, D-44627 Herne, GermanybDepartment of Pediatrics and Adolescent Medicine, Marienhospital Bottrop, Bottrop, Joseph-Albers-Str 70,D-46236 Bottrop, GermanycDepartment of Pathology, BG-Kliniken Bergmannsheil, Bürkle-de-la-Camp-Platz 1, D-44789 Bochum, Germany
Received 29 November 2009; revised 22 May 2010; accepted 13 June 2010
4
rakmm(M
0d
Key words:Aplasia cutis congenita;Congenital skull defect;Adams-Oliver syndrome;Brain herniation
Abstract We report the case of a newborn baby with a large congenital skull defect owing to Adams-Oliver syndrome. An initial attempt at conservative treatment failed and led to disruption of theleptomeningeal membrane and prolapse of the brain. After local debridement, delayed and stepwisesurgical closure was complicated by cerebrospinal fluid leakage, which required the insertion of acerebrospinal fluid shunt. This case report highlights the potential serious risks of nonsurgicalmanagement of largely extended congenital skull defects.© 2010 Elsevier Inc. All rights reserved.
Aplasia cutis congenita (ACC) of the head is a rarecongenital malformation first described by Campbell in 1826[1]. It is defined by the congenital absence of skin,subcutaneous tissue, and even the calvaria [2]. Theprevalence of large ACC has been estimated at 1 per10,000 live births. Aplasia cutis congenita may present as an
⁎ Corresponding author. Tel.: +49 2323 4992451; fax: +49 2323992451.E-mail addresses: [email protected],
[email protected] (R.-B. Tröbs),[email protected] (K. Barenberg),[email protected] (M. Hemminghaus),[email protected] (M. Günther), [email protected]. Neid).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2010.06.029
isolated condition or may be associated with othermalformations, indicating the presence of a genetic syn-drome. Adams-Oliver syndrome (AOS) is mainly character-ized by the presence of ACC of the scalp in combination withvariable degrees of terminal transverse limb defects [3]. Themanagement of large skull defects resulting from ACCremains controversial. Recently, conservative treatment hasbeen described as the preferred initial treatment, even forlarge defects involving both scalp and bone [4,5].
In this article, we report surgical problems in themanagement of a newborn with extended ACC of thescalp. In this case report, conservative treatment resulted inlocal infection, necrosis, delayed wound closure, andcerebrospinal fluid (CSF) leakage.

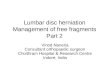
Fig. 2 Mainly right-sided protrusion of the uncovered brain at theage of 3 weeks.
2065Risks of conservative treatment of congenital skull defects
1. Case report
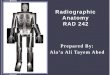
The boy was delivered spontaneously after 36 weeks ofgestation with a birth weight of 1,640 g, a body length of 41cm, and a head circumference of 29 cm (all less than the fifthpercentile). He was the third child of first-degree consanguinehealthy young parents. Antenatal ultrasound revealedoligohydramnios, developmental retardation of the fetus,and a single umbilical artery. The baby was born with a 7 × 4-cm asymmetrical defect of the neurocranium involving thescalp and bone of the midline and the right parietotemporalregion (Fig. 1). In addition, an area of dysplastic and atrophicscalp with 3 × 4-cm extension occipitally to the bony defectwas present. The surface of the open brain was covered by athin translucent and intact membrane. Furthermore, 2separated skin defects of the upper anterior abdominal wallwere present, each measuring 1 cm in diameter. Bilateralhypoplasia and partial syndactyly of the toes and a glandulartype of hypospadia indicated the presence of AOS. Accordingto recommendations from the recent literature [4], aconservative treatment approach was taken. Sterile moisturegauze dressings were changed daily. Isotonic sodiumchloride solution alternating with the disinfectant Octenisept(Schülke undMayr GmbH, D-22840 Norderstedt, Germany),a nonalcoholic solution of octenidine hydrochloride andphenoxyethanol, was applied. A reduced general condition,hypothermia, and elevated leukocyte counts and C-reactiveprotein, however, indicated systemic bacterial infection after1 week. Antibiotic therapy was started but could not preventdisruption of the leptomeninges after 18 days, which led tothe protrusion of large unprotected parts of the brain. Thebaby was transferred to the pediatric surgery unit (Fig. 2).Surgical treatment was started with local debridement,including the removal of necrotic material around the superiorsagittal sinus and temporary covering of the brain surfacewith a pericardium patch (Tutopatch; Tutogen MedicalGmbH, Industriestrasse 6, D-91077 Neunkirchen a Br,Germany). Biopsy of the brain confirmed severe purulentleptomeningitis (Fig. 3). At the age of 5 weeks, aggressive
Fig. 1 Magnetic resonance imaging at the second day of
mobilization of the entire scalp in a complex pattern ofpedicle flaps (Fig. 4) allowed closure of the defect with theexception of a poorly vascularized small residual defect of 1.5cm on the vertex. This area was temporarily covered with asmall piece of soft foam dressing (Syspur-derm; PaulHartmann AG, D-89522 Heidenheim, Germany), whichwas later replaced with a full-thickness skin graft. Healingoccurred; however, intermittent subdural fluid collected at theformer defect, with CSF leakage (Fig. 5). In addition,moderate dilation of the side ventricles indicated increasedintracranial pressure and disturbed CSF circulation. Asubduroperitoneal CSF shunt with a low-pressure Mietke(Christoph Miethke GmbH, Ulanenweg 2, D-14469 Pots-dam, Germany) valve (4/24 mm Hg) was inserted. Afterinsertion of the shunt, the CSF leakage disappeared. The babywas in stable condition over a follow-up of 6 months. Anoxycephalic appearance of the head resulted, however; andbony remodeling of the calvaria did not occur. Furthermore,moderate neurologic impairment of the baby resulted.
life shows a thin membrane at the defect (asterisks).

Fig. 3 High-grade florid and fibrinous inflammation of theleptomeninges (biopsy, ×125, hematoxylin-eosin).
Fig. 5 Protrusion of the scalp owing to CSF collection (magneticresonance imaging).
2066 R.-B. Tröbs et al.
2. Discussion
Aplasia cutis congenita of the scalp occurs morecommonly on the vertex than the parietal and temporalregion [6]. We observed a mainly right-sided parietotem-poral pathology. The defects may be of different sizes andcan extend to variable depths to involve the skull or both theskull and the dura [2]. The mortality of large extended anddeep ACC is as high as 20% to 55% of cases [7].
The pathogenesis of ACC still remains unclear. Thereexist 4 main theories: (1) early fetal vascular disruption, (2)embryonic developmental error such as incomplete closureof the outermost ectodermal portion of the neural tube, (3)amniotic adhesions, and (4) intrauterine external compres-sion. None of these causes, except heredity, in patients withAOS, however, has been proven to be the etiologic factor[4-6]. Screening of the affected family has been recom-
Fig. 4 Extensive mobilization of the scalp and creation of pedicleflaps. The arrows show extension of the defect.
mended to identify familial forms of the disease withautosomal-dominant genetic transmission [7].
The management of ACC has been a subject ofcontroversy in the literature. Small and superficial defectswithout exposure of vital structures heal spontaneously orcan be closed surgically. For larger scalp and skull defects,however, the treatment may be challenging. The depth of thetissue defect makes a difference. Cases with an uncoveredbrain are at high risk of developing meningitis, thrombo-phlebitis, and thrombosis or hemorrhage of the superiorsinus. For the management of large skull defects, bothsurgical closure and conservative treatment have beenfavored by different authors. Conservative treatment hasbeen advocated in a recent meta-analysis, even for largedefects [4]. Controlled healing is based on a strong tendencyfor spontaneous closure of the defect and the osteogenicpotential of the intact leptomeningeal covering. This processmay be time consuming, and complete osseous regenerationmay take 1 year. De Olivera et al (2006) [4] recommendeddaily dressings with silver sulfadiazine or bacitracin cream toreduce the rate of infection and to dehydrate the wound.Povidone-iodine dressings should be avoided because theycan lead to exsiccation and denaturation of the wound surface.
Serious complications and death following attemptedconservative treatment have been reported and includemassive sinus hemorrhage, sinus thrombosis, and leptome-ningitis [1,2,8]. In our patient, disruption of the leptome-ninges allowed herniation of the brain, resulting in infectionand superficial necrosis of the protruded mass. Furthermore,extension of the defect, protrusion, and local soft tissueinflammation required a staged closure.
Early surgical closure, especially of large and deepdefects, may prevent these life-threatening complications[7,8]. However, surgical closure of a large defect in small

2067Risks of conservative treatment of congenital skull defects
neonates may be a serious undertaking with potential risks ofhemorrhage, impaired wound healing, and donor sitemorbidity [5,6,9]. In our patient, we used a complex patternof skin flaps in combination with a temporary skin substitute,which was later replaced by a full-thickness skin graft.Furthermore, insertion of a CSF shunt was required to drainfluid that collected below the surgically created scalp.
The reported case highlights the serious surgical and long-term consequences of a failed conservative treatmentapproach to large open congenital skull defects.
References
[1] Campbell W. Case of congenital ulcer on the cranium of a fetus,terminating in fatal hemorrhage, on 18th day after birth. J Med Sci(Edinburgh) 1826;2:82-4.
[2] Piatt JH. Congenital defects of the scalp and skull. In: Albright AL,Pollack IF, Adelson PD, editors. Principles and practice of pediatricneurosurgery. 2nd ed. Thieme, New York: Stuttgart; 2008. p. 254-64.
[3] Jones KL. Smith's recognizable patterns of human malformation.6th ed. Philadelphia: Elsevier Saunders; 2006. p. 356-7.
[4] De Oliveira RS, Juca CEB, Lins-Neto AL, et al. Aplasia cutis congenitalof the scalp: is there a better treatment strategy? Childs Nerv Syst2006;22:1072-9.
[5] Rhee ST, Colville C, Buchman SR. Complete osseous regeneration of alarge skull defect in a patient with cutis aplasia: a conservativeapproach. J Craniofac Surg 2002;13:497-500.
[6] Kruk-Jeromin J, Janik J, Rykala J. Aplasia cutis congenita of the scalp.Dermatol Surg 1998;24:549-53.
[7] Casanova D, Amar E, Bardot J, et al. Aplasia cutis congenital. Eur JPediatr Surg 2001;11:280-4.
[8] Kim CS, Tatum SA, Rodziewicz G. Scalp aplasia cutis congenitapresenting with sagittal sinus hemorrhage. Arch Otolaryngol Head NeckSurg 2001;127:71-4.
[9] Yang JY, Yang WG. Large scalp and skull defect in aplasia cutiscongenital. Br J Plast Surg 2000;53:619-22.









![A systematic approach in the diagnosis of paediatric skull ... systemati… · neurological symptoms, a conservative approach with a six-month observation period is advised [13,14]](https://img.pdfslide.net/doc/110x75/5ea78942aab2327dff2e4f4d/a-systematic-approach-in-the-diagnosis-of-paediatric-skull-systemati-neurological.jpg)