Embed Size (px)
Citation preview

Hiperprogresores e hiperrespondedores.
Bases biologicas y como detectarlos
Antonio CallesServicio de Oncología Médica
Unidad de Tumores Torácicos y Unidad de Fases 1
Hospital General Universitario Gregorio Marañón
Instituto Investigación Sanitaria HGUGM
Universidad Complutense de Madrid
Madrid, España

Conflicts of interest
• Honoraria: AstraZeneca, Boehringer-Ingelheim, Pfizer, Roche, Novartis, Merck
Sharp & Dohme, and Bristol-Myers Squibb.
• Consulting or advisory role: AstraZeneca, Boehringer-Ingelheim, Pfizer,
Roche/Genentech, Eli Lilly and Company, Novartis, Merck Sharp & Dohme,
and Bristol-Myers Squibb.
• Travel financial support: Roche, Boehringer-Ingelheim, Merck Sharp &
Dohme, and Bristol-Myers Squibb.

Hiperprogresión Hiperrespondedores

Borcoman et al. Ann Oncol 2019
Champiat et al. Nat. Rev. Cancer 2018
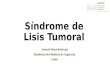
Patrones de respuesta a la inmunoterapia

Ferrara R. et al. JAMA Oncol. 2019
Concepto de “Hyperprogressive Disease” (HPD)

La definición de “Hyperprogressive Disease” (HPD) se basa en análisis retrospectivos
Champiat et al CCR 2017

Los pacientes que desarrollan HPD tienen peor supervivencia
NSCLC Mesothelioma
Ferrara R. et al. JAMA Oncol. 2019
Zalcman et al. ESMO 2019

0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
CR/P
R SD
PD
Pse
udoPD
HPD
19%
39%42%
5%
14%
0%
10%
20%
30%
40%
50%
60%
CR/PR SD PD
PseudoPD HP
D
10%
59%
31%
5%0%
Ferrara R. et al. WCLC 17; JAMA Oncol. 2018
Inmunoterapia Quimioterapia
La HPD también está descrita con la quimioterapia

Las muertes precoces en los ensayos clínicos podrían corresponder a HPD
Borghaei. et al. N Engl J Med 2015
Champiat et al. Nat. Rev. Cancer 2018

Hipotesis biologicas de HPD en pacientes tratados con ICI
Champiat et al. Nat. Rev. Cancer 2018

Hacia una definición de HPD: Intregración del tratamiento previo
Champiat et al. Nat. Rev. Cancer 2018

Fórmulas para el cálculo de HPD
Tumor Growth Rate (TGR) (Champiat et al. 2016; Ferrara R. et al. 2018)
(assumes exponential tumor growth: Vpost= V0 (expTG x time)
Tumor Growth Kinetics (TGK) (Saada-Bouzid E. et al. 2017)
(assumes linear tumor growth)
Ferté C. et al. Clin. Cancer Res. 2014;
Champiat S. et al. Clin. Cancer Research 2016
Saasa-Bouzid E. et al. Ann. Oncol. 2017
Ferrara R. et al. JAMA Oncol. 2018

Criterios habitualmente utilizados en la definición de HPD
• Progresión por RECIST en primera revaluación (8 semanas)
• >50% incremento en carga tumoral
• Incremento TGR > 2x entre el tratamiento PREVIO y el ACTUAL
• Incremento TGK ratio > 2
• Nuevas lesiones (en mismo órgano y/o nuevos órganos)
• Deterioro de PS a ECOG 2
• Muerte precoz (< 3 meses)
Ferté C. et al. Clin. Cancer Res. 2014;; Champiat S. et al. Clin. Cancer Res 2016; Saasa-Bouzid E. et al. Ann. Oncol. 2017; Ferrara R. et al.
JAMA Oncol. 2018; Kanjanapan et al. Cancer 2019; Kato et al. Clin Cancer Res 2017; Lo Russo et al. Clin Cancer Res 2019

Matos et al. Clin Cancer Res Published OnlineFirst November 22, 2019
Criterios de HPD utilizando RECIST 1.1

Garassino. AACR 2019
Estudios que evalúan HPD en tumores sólidos tratados con ICI

No hay características clínicas asociadas a HPD con ICI
Kanjanapan et al. Cancer 2019
Progresión por RECIST en primera revaluación (8 semanas)
+
Incremento TGR > 2x entre el tratamiento PREVIO y el ACTUAL HPD 7%
n=182 solid tumors

Alteraciones genéticas asociadas a HPD
Factors associated with HPDOdds ratio (95% CI)
multivariate
P value
multivariate
MDM2/4 amplification 10.8 (1-88-infinity) 0.001
EGFR alteration 8.36 (1.28-98.5) 0.004
Progresión antes de 2 meses
+
>50% incremento en carga tumoral respecto al basal
+
Incremento TGR > 2x entre el tratamiento PREVIO y el ACTUAL
Kato et al. Clin Cancer Res 2017
Análisis retrospectivo de 155 pacientes tratados con ICI
en los que se realizó NGS en MDACC

Rate of change in growth pattern in four cases with MDM2
amplification that progressed rapidly while on immunotherapy.
MDM2 pathway
La amplificacion de MDM2 es un posible marcador de HPD
Kato et al. Clin Cancer Res 2017 MDM2 amplification tumors included bladder (n=1), TNBC (n=1),
endometrial stromal sarcoma (n-=1), LUAC (n=2), HNSCC (n=1)

STK11/LKB1 mutations are a genomic determinant of resistance to anti-P1
blockade in NSCLC
Skoulidis et al. Cancer Discov 2018

La HPD podría ser más frecuente en presencia de mutaciones driver
Ferrara – JAMA Oncol 18
N = 406
Hyperprogression : 14%
Necesidad de encontrar un racional

Análisis de cfDNA para monitorización precoz de respuesta
Jensen et al. Mol Cancer Ther 2019
Borcoman et al. Ann Oncol 2019

Antibody-Fc/FcR Interaction on Macrophages as a Mechanism for Hyperprogressive
Disease in Non-small Cell Lung Cancer Subsequent to PD-1/PD-L1 Blockade
Lo Russo et al. Clin Cancer Res 2019
TAM reprogrammingM2-like CD163+CD33+PD-L1+

Radiomica para la identificacion de HPD
En el modelo final utiliza:• 4 variables radiómicas
• 4 covariantes clínicas : Presencia de metástasis hepáticas y
óseas, líneas de tratamientos previos y ratio neutrofilo-
linfocito (NLR)
• AUROC 0.804 (S=63.43%, E= 83.46%, P=73.41%)
Tunaly et al. Lung Cancer 2019

Hiper-respondedoresMás allá de la expresión de PD-L1
Estados de hiper-mutación
POLE-POL D1/APOBEC signatures
MSI-H/dMMR
HRD
TMB
Variabilidad individual
Clonalidad
HLA
TCR
Situación inflamatoria del tumor y del individuo
“Hot vs. cold tumors” (GEP, IFN-ɣ)
dLNR, LDH
Factores modificadores del individuo
Antibióticos, corticoides, IBPs
Microbioma

2
5
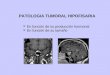
Landmark analysis of OS by response category status at 6 months*Pooled Checkmate 017/ 057 survival analysis
*In all randomized patients from Checkmate 017 and 057 studies alive at the 6-month landmark; 65.6% and 61.8% patients in the nivolumab and docetaxel treatment arms, respectively, were included in this analysis.
Antonia SJ et al. Lancet Oncol. 2019:doi: 10.1016/S1470-2045(19)30407-3..
CheckMate 017/057 4-Year Survival Outcomes
CR/PR
Nivo
93%
81%
63% 61%
100
0
40
60
80
20
0 126 18 24 30 4236 48 54 60 66
58%
Nivo
58%
80%
35%
24%
100
0
40
60
80
20
0 126 18 24 30 4236 48 54 60 66
19%
Nivo
60%
40%
13%
8%
100
0
40
60
80
20
0 126 18 24 30 4236 48 54 60 66
4%Docetaxel
88%
62%
38%
26%
12%18%
Docetaxel
62%
35%
7%2%
Docetaxel
41%
22%
12%8%
5%
70 5765 52 44 42 3739 24 7 0 0 66 3853 29 23 18 1315 10 2 0 0 144 5587 32 17 10 510 3 0 0 0
34 2130 15 13 10 79 4 0 0 0 102 3563 24 17 11 47 2 0 0 0 128 2852 18 15 13 810 5 1 0 0
Months from landmark analysis Months from landmark analysis Months from landmark analysis
OS
(%
)
OS
(%
)
OS
(%
)
Nivolumab
Docetaxel
No. at risk
Nivo(n=70)
Docetaxel(n=34)
Median OS(95% CI), mo
NR(25.6, NR)
17.1(11.1, 28.7)
HR (95% CI), vs PD
0.18(0.12, 0.27)
0.43(0.29, 0.65)
Nivo(n=66)
Docetaxel(n=102)
Median OS(95% CI), mo
16.1(10.2, 23.5)
8.0(6.6, 10.4)
HR (95% CI), vs PD
0.52(0.37, 0.71)
0.80(0.61, 1.04)
Nivo(n=144)
Docetaxel(n=128)
Median OS(95% CI), mo
9.1(6.2, 11.4)
4.8(3.4, 5.9)
HR (95% CI), vs PD
- -
SD PD

Beyond PD-L1 Expression: Tumour–Immune Classification
Teng et al. Cancer Res 2015
Cold Hot
Immune-ignored Immune-excluded

Multiplexed immunofluorescence
KeyPD-L1 PD-
1 CD8FOXP3CD68
Tumor DAPI
Post-treatment
Forde et al NEJM 2018
Calles et al JTO 2016
Conde et al. Hystopathology, 2017
PD-1
200μm
PD-L1 PD-L2
CD8
200μm 200μm
200μm

Bensch F et al. Nat Med 2018
89Zr-atezolizumab Immune-PET

The Tumor Immunogenicity – Inflammation Pathway
Mismatch
Repair
Defect
Micro-
Satellilte
Inestability
High
Mutation
Burden
POLE & D1
Mutations
Enviromental
Factors
Homologous
Recombination
Deficency
High
Tumor
Immuno-
genicity
Tumor
Inflammation
PD-L1
Positive
Clinically Validated Biomarkers
Adaptive
Response
Investigational Biomarkers

Microsatellite Instability as a Biomarker for PD-1 Blockade
Dudley J, et al. Clin Cancer Res 2016
Xiao and Freeman. Cancer Discov 2015

First tissue-agnostic FDA approval: Pembrolizumab for the treatment of
microsatellite instability-high solid tumors
Dung T. Le et al. Science 2017;357:409-413
+12 tumor types

The Tumor Immunogenicity – Inflammation Pathway
Mismatch
Repair
Defect
Micro-
Satellilte
Inestability
High
Mutation
Burden
POLE & D1
Mutations
Enviromental
Factors
Homologous
Recombination
Deficency
High
Tumor
Immuno-
genicity
Tumor
Inflammation
PD-L1
Positive
Clinically Validated Biomarkers
Adaptive
Response
Investigational Biomarkers

No Association Between TMB and PD-L1 Expression
Peters AACR 2017
Gandara ASCO 2018
PD-L1 (% Tumor Expression)a
High TMB
7550
1000
316
100
32
10
0 25 100
TM
B (N
o. o
f M
issen
se M
uta
tio
ns
)
Low/medium TMB
243

Tumor mutational load predicts survival after immunotherapy across
multiple cancer types
Samstein RM, et al. Nature Genetics 2019
MSK-IMPACT
N=1662 pts treated with ICI
Different TMB cutpoints by cancer type

The Tumor Immunogenicity – Inflammation Pathway
Mismatch
Repair
Defect
Micro-
Satellilte
Inestability
High
Mutation
Burden
POLE & D1
Mutations
Enviromental
Factors
Homologous
Recombination
Deficency
High
Tumor
Immuno-
genicity
Tumor
Inflammation
PD-L1
Positive
Clinically Validated Biomarkers
Adaptive
Response
Investigational Biomarkers

Neoantigen-based prediction: quantity, heterogeneity and quality
Havel, et al. Nat Rew Cancer 2019
DAI
Differential agretopicity index
Neoantigen fitness model:
- Tumour clonality
- DAI
- Microbial epitope homology
>> TMB to predict ICI benefit

Patient HLA class I genotype influences cancer response to checkpoint
blockade immunotherapy
Chowell et al. Science 2018;359:582-587

Individual Levels of Clonality of Immune Repertoire
Langerak et al. J Immunol 2017

The Tumor Immunogenicity – Inflammation Pathway
Mismatch
Repair
Defect
Micro-
Satellilte
Inestability
High
Mutation
Burden
POLE & D1
Mutations
Enviromental
Factors
Homologous
Recombination
Deficency
High
Tumor
Immuno-
genicity
Tumor
Inflammation
PD-L1
Positive
Clinically Validated Biomarkers
Adaptive
Response
Investigational Biomarkers

Immune signatures as biomarkers of response and mechanisms of
resistance to ICI
Ayers et al. Clin Cancer Res 2019
Ock et al. Nat Commun 2017
Chen et al. Cancer Discov 2016
IFN-gamma

Immune signatures as biomarkers of response and mechanisms of
resistance to ICI
Reck M et al. Impower 150 PFS analysis
Teff Gene Signature
PDL1
IFNG
CXCL9
Pre-existing
immunity
PD-L1 expression
on TC and IC
Teff Gene Signature vs PD-L1 IHC (SP142)a
36%14% 20%
Teff
≥ median
TC1/2/3
or IC1/2/3b
N = 753
0,25
Population n (%)a
ITT (including EGFR/ALK mutant +) 800 (100%)
EGFR/ALK mutant + onlyb 108 (14%)
ITT-WT 692 (87%)
Teff-high (WT) 284 (43%)
Teff-low (WT) 374 (57%)
PD-L1 IHC TC2/3 or IC2/3 (WT) 244 (35%)
PD-L1 IHC TC1/2/3 or IC1/2/3 (WT) 354 (51%)
PD-L1 IHC TC0 and IC0 (WT) 338 (49%)
PD-L1 IHC TC3 or IC3 (WT) 135 (20%)
PD-L1 IHC TC0/1/2 or IC0/1/2 (WT) 557 (80%)
Median PFS, mo
1.0
In favour of Arm C:
bev + CP
Hazard Ratioc
In favour of Arm B:
atezo + bev + CP
0.6
10.5
9
0.7
6
0.4
80.5
0 0.7
7
0.5
1
0.6
2
1.25
0.3
9 0.6
8
Arm B Arm C
8.3 6.8
9.7 6.1
8.3 6.8
11.3 6.8
7.3 7.0
11.1 6.8
11.0 6.8
7.1 6.9
12.6 6.8
8.0 6.8

Tumor and Immune Biomarkers Being Evaluated to Predict Better
Outcomes to Immuno-Oncology Therapy
• Biomarkers indicative of
hypermutation & neoantigens may
predict response to IO treatment
Examples:
‒ TMB, MSI-high, neoantigens
Tumor Antigens
• Biomarkers that identify tumor
immune system evasion beyond
PD-1/CTLA-4 to inform new IO
targets and rational combinations
Examples:
‒ Tregs, MDSCs, IDO, LAG-3
Tumor Immune
Suppression
• Biomarkers (intra- or peri-tumoral) indicative of an inflamed phenotype may predict response to IO treatment
Examples:
‒ PD-L1, inflammatory signatures
Inflamed Tumor
Microenvironment
• Biomarkers which characterize the
host environment, beyond tumor
microenvironment, may predict
response to IO treatment
Examples:
‒ Microbiome, germline genetics
Host Environment
Tumor
Antigens
Tumor Immune
Suppression
Inflamed
Tumor
IDO = indoleamine-2,3 dioxygenase; LAG-3 = lymphocyte activation gene-3; MDSCs = myeloid-derived suppressor cells; MSI-high = microsatellite instability high; TMB = tumor mutational burden. Adapted from Blank C.U. et al. Science 2016;352:658–660.

Mezquita et al JAMA Oncol. 2018;4(3):351-357. doi:10.1001/jamaoncol.2017.4771
Lung Immune Prognostic Index (LIPI)
dNLR greater than 3 and LDH
Neutrophil to Lymphocyte Ratio
0 factors = good
1 factor = intermediate
2 factors = poor

Impact of Baseline Steroids on Efficacy of PD-1 and PD-L1 blockade
Arbour et al JCO 2018 Oct 1
Prednisone ≥ 10 mg or equivalent
Steroids are powerful immune
-suppresants

Gut microbes shape response to cancer immunotherapy

Proton pump inhibitors negatively impact survival of PD-1/PD-L1 inhibitors
Mukherjee S, et al. J Oncol Pharm Practice 2018
Homicsko K, et al. CheckMate 069 ESMO-IO 2018
Chalabi M, et al. OAK & POPLAR ESMO-IO 2018


J-C Soria AACR 2019

HiperrespondedoresHiperprogresión
❑ Efecto real vs. historia natural de la enfermedad
❑ Infrecuente: <10%
❑ No hay una definición globalmente aceptada
❑ Supervivencia muy limitada
❑ No hay claros biomarcadores
❑ Definición de nuevos largos supervivientes
❑ Infrecuentes: <20%
❑ Múltiples mecanismos potenciales identificados
❑ Muchos factores de confusión
❑ No es posible identificar pacientes a priori
Conclusiones
2 fenómenos extremos observados con el tratamiento con ICI que comparten similitudes