Embed Size (px)
Citation preview
1456 Case Reports / Journal of Clinical Neuroscience 19 (2012) 1456–1458
Histiocytic sarcoma of the brain
Spinderjeet Gill-Samra a,⇑, Thomas Ng a,g, Mark Dexter b, Mark Wong c, Najmun Nahar d,Katherine Allsopp e, Rose A. Boadle f, Winny Varikatt a,g
a Department of Tissue Pathology, Level 3, ICPMR, Westmead Hospital, Hawkesbury Rd, Westmead, New South Wales 2145, Australiab Department of Neurosurgery, Westmead Hospital, New South Wales, Australiac Department of Medical Oncology, Westmead Hospital, New South Wales, Australiad Department of Radiation Oncology, Westmead Hospital, New South Wales, Australiae Department of Palliative Care, Westmead Hospital, New South Wales, Australiaf Department of Tissue Pathology, Electron Microscope Laboratory, Westmead Hospital, New South Wales, Australiag School of Medicine, University of Western Sydney, New South Wales, Australia
a r t i c l e i n f o
Article history:Received 25 June 2011Accepted 9 October 2011
Keywords:BrainHistiocytic sarcomaLympho-hematopoieticMalignant tumour
a b s t r a c t
Histiocytic sarcoma is a rare malignant neoplasm of the lympho-hematopoietic system that usuallyoccurs in the skin, lymph nodes and intestinal tract. We present a 36-year-old woman with a rare histio-cytic sarcoma with isolated central nervous system (CNS) involvement of multifocal circumscribedlesions. Biopsy of the brain lesions showed diffuse proliferation of pleomorphic histiocytes that wereimmunopositive for CD45, CD68 and CD163. Various cytokeratins and markers of lymphoma, melanoma,germ cell tumours and primary CNS tumours were negative. Examination of bone marrow trephine and awhole-body positron emission tomography scan showed no evidence of involvement of any other organsystems, thus establishing the primary nature of the lesion. The neoplastic cells uniquely showed eosin-ophilic globules within the cytoplasm, which were positive for CD68. These globules were shown by elec-tron microscopy to be collections of lysosomes. A thorough discussion of the differential diagnosis andliterature review is included.
� 2012 Elsevier Ltd. All rights reserved.
1. Introduction
Histiocytic sarcoma (HS), formerly designated as true histiocyticlymphoma, is a rare hematopoietic neoplasm, representing 1% ofall non-Hodgkin’s lymphomas (NHL).1 Difficulties in identifyingthe histiocytic derivation of HS contribute to their under diagnosisand these lesions have often been mistakenly diagnosed asanaplastic large cell lymphoma or malignant lymphomas withabundant reactive macrophages.2
HS is a disease of adults, with a peak incidence in the fifth dec-ade. It usually arises in lymph nodes and skin, but extranodal pre-sentation is frequent and the course is generally aggressive.3–5
There are only a few reports in the literature of involvement ofgastrointestinal tract,6 spleen,7 brain,8,9 thyroid10 and heart.11 Wepresent a patient with this rare tumour with primary, butmultifocal, presentation in the brain, without any other organinvolvement.
2. Case report
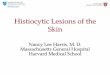
A 38-year-old woman of Chinese descent presented with aone-to-two month history of headaches associated with nausea,vomiting and dizziness. A brain MRI revealed multiple supratento-rial lesions of heterogeneous signal intensity, which enhancedfollowing gadolinium administration. The largest lesion (50 mmdiameter) was located in the left posterior temporal lobe, with evi-dence of central necrosis, mass effect and adjacent white matteroedema (Fig. 1). F-18 fluorodeoxyglucose–positron emissiontomography (FDG–PET) imaging demonstrated multiple hyper-metabolic lesions within the brain, but no evidence of any lesionoutside the central nervous system (CNS). Similarly, whole-bodyCT scans did not reveal any evidence of malignancy outside ofthe CNS. A stereotactic left temporal craniotomy for removal of
⇑ Corresponding author. Tel.: +61 2 98456222; fax: +61 2 96872330.E-mail address: [email protected] (S. Gill-Samra).
the largest lesion was performed, with a clinical diagnosis of pri-mary or metastatic malignancy, or less likely, an infective lesion.
Fig. 1. Axial T1-weighted, contrast-enhanced MRI showing a 50-mm lesion locatedin the left posterior temporal lobe, with evidence of central necrosis, mass effectand adjacent white matter oedema.
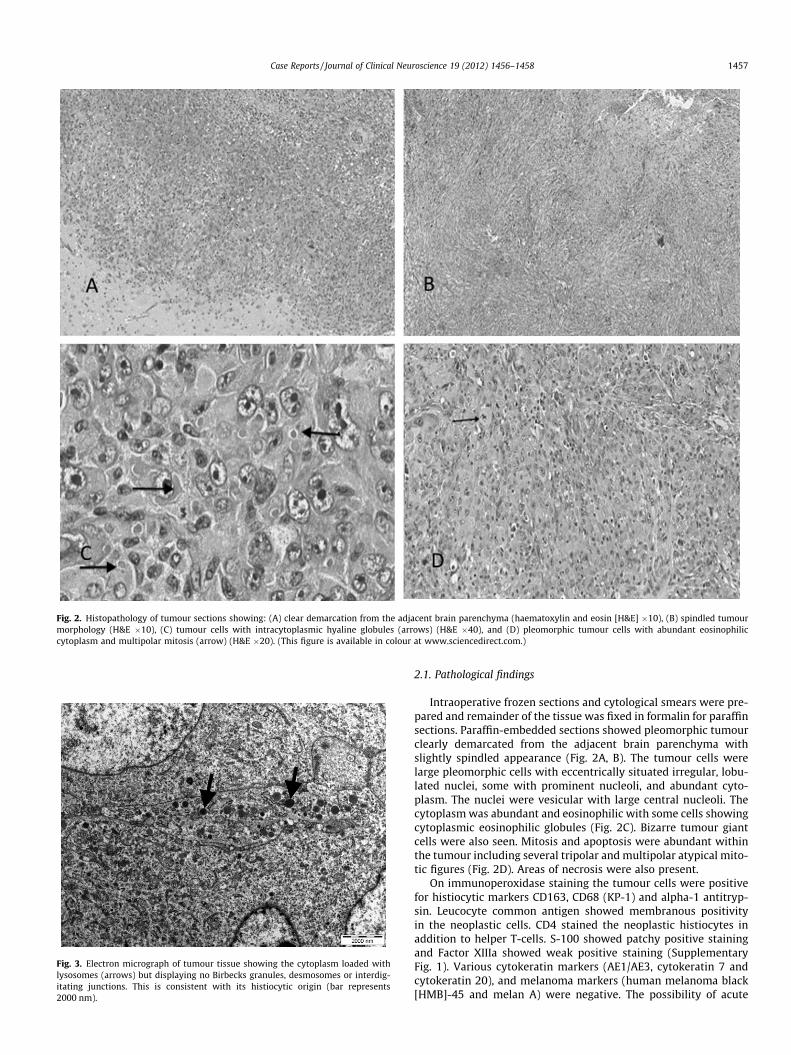
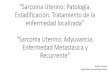
Fig. 2. Histopathology of tumour sections showing: (A) clear demarcation from the adjacent brain parenchyma (haematoxylin and eosin [H&E] �10), (B) spindled tumourmorphology (H&E �10), (C) tumour cells with intracytoplasmic hyaline globules (arrows) (H&E �40), and (D) pleomorphic tumour cells with abundant eosinophiliccytoplasm and multipolar mitosis (arrow) (H&E �20). (This figure is available in colour at www.sciencedirect.com.)
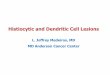
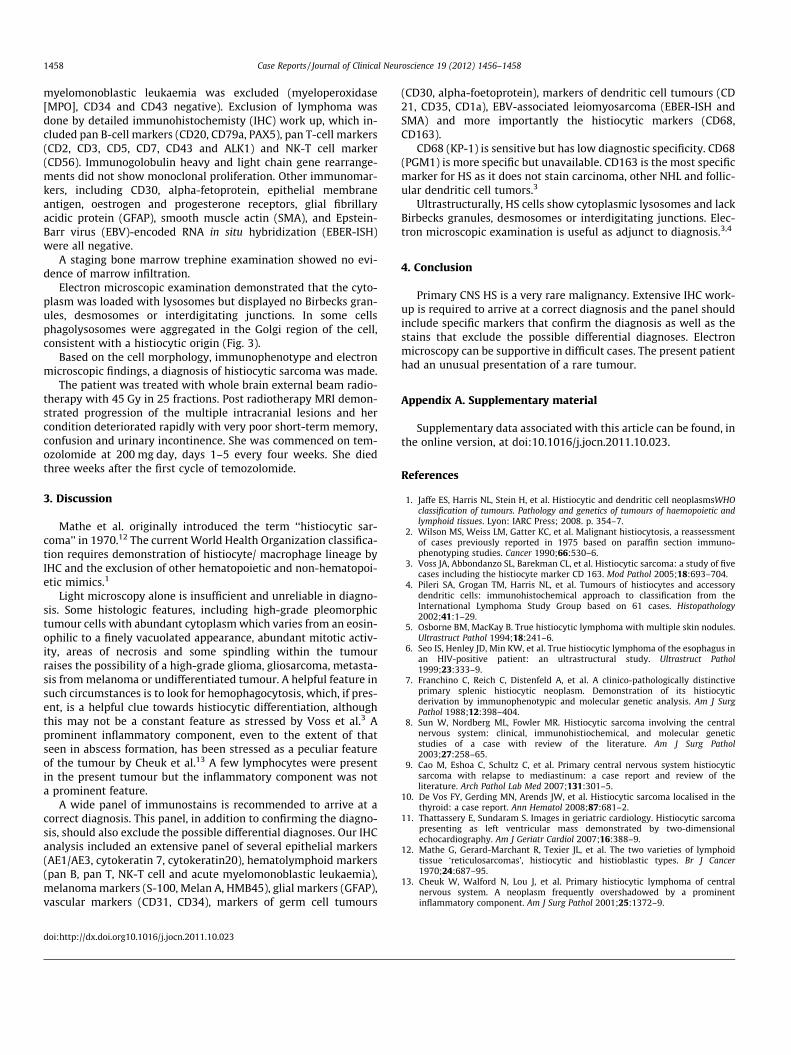
Fig. 3. Electron micrograph of tumour tissue showing the cytoplasm loaded withlysosomes (arrows) but displaying no Birbecks granules, desmosomes or interdig-itating junctions. This is consistent with its histiocytic origin (bar represents2000 nm).
Case Reports / Journal of Clinical Neuroscience 19 (2012) 1456–1458 1457
2.1. Pathological findings
Intraoperative frozen sections and cytological smears were pre-pared and remainder of the tissue was fixed in formalin for paraffinsections. Paraffin-embedded sections showed pleomorphic tumourclearly demarcated from the adjacent brain parenchyma withslightly spindled appearance (Fig. 2A, B). The tumour cells werelarge pleomorphic cells with eccentrically situated irregular, lobu-lated nuclei, some with prominent nucleoli, and abundant cyto-plasm. The nuclei were vesicular with large central nucleoli. Thecytoplasm was abundant and eosinophilic with some cells showingcytoplasmic eosinophilic globules (Fig. 2C). Bizarre tumour giantcells were also seen. Mitosis and apoptosis were abundant withinthe tumour including several tripolar and multipolar atypical mito-tic figures (Fig. 2D). Areas of necrosis were also present.
On immunoperoxidase staining the tumour cells were positivefor histiocytic markers CD163, CD68 (KP-1) and alpha-1 antitryp-sin. Leucocyte common antigen showed membranous positivityin the neoplastic cells. CD4 stained the neoplastic histiocytes inaddition to helper T-cells. S-100 showed patchy positive stainingand Factor XIIIa showed weak positive staining (SupplementaryFig. 1). Various cytokeratin markers (AE1/AE3, cytokeratin 7 andcytokeratin 20), and melanoma markers (human melanoma black[HMB]-45 and melan A) were negative. The possibility of acute
1458 Case Reports / Journal of Clinical Neuroscience 19 (2012) 1456–1458
myelomonoblastic leukaemia was excluded (myeloperoxidase[MPO], CD34 and CD43 negative). Exclusion of lymphoma wasdone by detailed immunohistochemisty (IHC) work up, which in-cluded pan B-cell markers (CD20, CD79a, PAX5), pan T-cell markers(CD2, CD3, CD5, CD7, CD43 and ALK1) and NK-T cell marker(CD56). Immunogolobulin heavy and light chain gene rearrange-ments did not show monoclonal proliferation. Other immunomar-kers, including CD30, alpha-fetoprotein, epithelial membraneantigen, oestrogen and progesterone receptors, glial fibrillaryacidic protein (GFAP), smooth muscle actin (SMA), and Epstein-Barr virus (EBV)-encoded RNA in situ hybridization (EBER-ISH)were all negative.
A staging bone marrow trephine examination showed no evi-dence of marrow infiltration.
Electron microscopic examination demonstrated that the cyto-plasm was loaded with lysosomes but displayed no Birbecks gran-ules, desmosomes or interdigitating junctions. In some cellsphagolysosomes were aggregated in the Golgi region of the cell,consistent with a histiocytic origin (Fig. 3).
Based on the cell morphology, immunophenotype and electronmicroscopic findings, a diagnosis of histiocytic sarcoma was made.
The patient was treated with whole brain external beam radio-therapy with 45 Gy in 25 fractions. Post radiotherapy MRI demon-strated progression of the multiple intracranial lesions and hercondition deteriorated rapidly with very poor short-term memory,confusion and urinary incontinence. She was commenced on tem-ozolomide at 200 mg day, days 1–5 every four weeks. She diedthree weeks after the first cycle of temozolomide.
3. Discussion
Mathe et al. originally introduced the term ‘‘histiocytic sar-coma’’ in 1970.12 The current World Health Organization classifica-tion requires demonstration of histiocyte/ macrophage lineage byIHC and the exclusion of other hematopoietic and non-hematopoi-etic mimics.1
Light microscopy alone is insufficient and unreliable in diagno-sis. Some histologic features, including high-grade pleomorphictumour cells with abundant cytoplasm which varies from an eosin-ophilic to a finely vacuolated appearance, abundant mitotic activ-ity, areas of necrosis and some spindling within the tumourraises the possibility of a high-grade glioma, gliosarcoma, metasta-sis from melanoma or undifferentiated tumour. A helpful feature insuch circumstances is to look for hemophagocytosis, which, if pres-ent, is a helpful clue towards histiocytic differentiation, althoughthis may not be a constant feature as stressed by Voss et al.3 Aprominent inflammatory component, even to the extent of thatseen in abscess formation, has been stressed as a peculiar featureof the tumour by Cheuk et al.13 A few lymphocytes were presentin the present tumour but the inflammatory component was nota prominent feature.
A wide panel of immunostains is recommended to arrive at acorrect diagnosis. This panel, in addition to confirming the diagno-sis, should also exclude the possible differential diagnoses. Our IHCanalysis included an extensive panel of several epithelial markers(AE1/AE3, cytokeratin 7, cytokeratin20), hematolymphoid markers(pan B, pan T, NK-T cell and acute myelomonoblastic leukaemia),melanoma markers (S-100, Melan A, HMB45), glial markers (GFAP),vascular markers (CD31, CD34), markers of germ cell tumours
doi:http://dx.doi.org10.1016/j.jocn.2011.10.023
(CD30, alpha-foetoprotein), markers of dendritic cell tumours (CD21, CD35, CD1a), EBV-associated leiomyosarcoma (EBER-ISH andSMA) and more importantly the histiocytic markers (CD68,CD163).
CD68 (KP-1) is sensitive but has low diagnostic specificity. CD68(PGM1) is more specific but unavailable. CD163 is the most specificmarker for HS as it does not stain carcinoma, other NHL and follic-ular dendritic cell tumors.3
Ultrastructurally, HS cells show cytoplasmic lysosomes and lackBirbecks granules, desmosomes or interdigitating junctions. Elec-tron microscopic examination is useful as adjunct to diagnosis.3,4
4. Conclusion
Primary CNS HS is a very rare malignancy. Extensive IHC work-up is required to arrive at a correct diagnosis and the panel shouldinclude specific markers that confirm the diagnosis as well as thestains that exclude the possible differential diagnoses. Electronmicroscopy can be supportive in difficult cases. The present patienthad an unusual presentation of a rare tumour.
Appendix A. Supplementary material
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.jocn.2011.10.023.
References
1. Jaffe ES, Harris NL, Stein H, et al. Histiocytic and dendritic cell neoplasmsWHOclassification of tumours. Pathology and genetics of tumours of haemopoietic andlymphoid tissues. Lyon: IARC Press; 2008. p. 354–7.
2. Wilson MS, Weiss LM, Gatter KC, et al. Malignant histiocytosis, a reassessmentof cases previously reported in 1975 based on paraffin section immuno-phenotyping studies. Cancer 1990;66:530–6.
3. Voss JA, Abbondanzo SL, Barekman CL, et al. Histiocytic sarcoma: a study of fivecases including the histiocyte marker CD 163. Mod Pathol 2005;18:693–704.
4. Pileri SA, Grogan TM, Harris NL, et al. Tumours of histiocytes and accessorydendritic cells: immunohistochemical approach to classification from theInternational Lymphoma Study Group based on 61 cases. Histopathology2002;41:1–29.
5. Osborne BM, MacKay B. True histiocytic lymphoma with multiple skin nodules.Ultrastruct Pathol 1994;18:241–6.
6. Seo IS, Henley JD, Min KW, et al. True histiocytic lymphoma of the esophagus inan HIV-positive patient: an ultrastructural study. Ultrastruct Pathol1999;23:333–9.
7. Franchino C, Reich C, Distenfeld A, et al. A clinico-pathologically distinctiveprimary splenic histiocytic neoplasm. Demonstration of its histiocyticderivation by immunophenotypic and molecular genetic analysis. Am J SurgPathol 1988;12:398–404.
8. Sun W, Nordberg ML, Fowler MR. Histiocytic sarcoma involving the centralnervous system: clinical, immunohistiochemical, and molecular geneticstudies of a case with review of the literature. Am J Surg Pathol2003;27:258–65.
9. Cao M, Eshoa C, Schultz C, et al. Primary central nervous system histiocyticsarcoma with relapse to mediastinum: a case report and review of theliterature. Arch Pathol Lab Med 2007;131:301–5.
10. De Vos FY, Gerding MN, Arends JW, et al. Histiocytic sarcoma localised in thethyroid: a case report. Ann Hematol 2008;87:681–2.
11. Thattassery E, Sundaram S. Images in geriatric cardiology. Histiocytic sarcomapresenting as left ventricular mass demonstrated by two-dimensionalechocardiography. Am J Geriatr Cardiol 2007;16:388–9.
12. Mathe G, Gerard-Marchant R, Texier JL, et al. The two varieties of lymphoidtissue ‘reticulosarcomas’, histiocytic and histioblastic types. Br J Cancer1970;24:687–95.
13. Cheuk W, Walford N, Lou J, et al. Primary histiocytic lymphoma of centralnervous system. A neoplasm frequently overshadowed by a prominentinflammatory component. Am J Surg Pathol 2001;25:1372–9.