Embed Size (px)
Citation preview

JCN 2014, Vol 28, No 5 33
WOUND CARE
Over the past five years both the incidence and the severity of pressure ulcers
has been scrutinised more closely by the NHS and Department of Health (DH) (Calkin, 2013), with trusts facing financial penalties if the number of pressure ulcers is not reduced. There is now a greater awareness among NHS staff and the public that a high overall incidence of pressure ulcers (particularly when
How to accurately identify and record pressure ulceration
accompanied by the presence of severe pressure damage), may reflect poor standards of care within a health setting, whether in hospital or the community (Pinkney et al, 2014).
NHS England has identified the prevention of pressure ulcers as a priority under domain 5 of the NHS outcomes framework for 2014/2015 (DH, 2013). This has raised the importance of identifying and classifying pressure damage still higher, both in the eyes of care commissioning groups (CCGs), healthcare providers and the public.
Key performance indicators, such as targets for reductions in the number of pressure ulcers, are now set by CCGs when commissioning care from healthcare providers.
All of this attention increases the pressure on community nurses to accurately grade pressure ulcers.
However, this is not always a straightforward procedure and is complicated by several factors.
EDUCATION AND TRAINING
Clinicians of all professional groups, not solely nurses, require regular education and training in the prevention and management of pressure ulcers (NICE, 2014a). However, it is not sufficient to simply provide education by describing pressure ulcer grades — additional training is required, including: Group work Studying photographs Patient scenarios Bedside training (although this
requires patient consent).
It is vital that tissue viability nurses (TVNs) work with generalist nurses to improve their skills rather
Pauline Beldon is a retired tissue viability nurse consultant, Epsom and St Helier University Hospitals NHS Trust, Surrey
The accurate grading or staging (henceforth referred to as grading in this article) of pressure ulcers has become increasingly important over the past five years as healthcare organisations insist on each wound being accurately documented (National Institute for Health and Care Excellence [NICE], 2014a, b). The impetus to capture improved data on pressure ulcers has been driven both by the need to reduce the impact of these debilitating wounds on patients, but also to bring down the spiralling costs to the NHS associated with their treatment. However it is not always easy to grade a pressure ulcer and the accuracy of any conclusions can be affected by multiple factors such as the presence of necrotic tissue, the colour of the individual’s skin and the skill of the clinician, whether nurse, therapist, doctor, podiatrist or healthcare assistant. This article examines the basic principles of grading pressure ulcers, particularly where there may be conflicting signs and indications, and also investigates so-called ‘ungradeable’ pressure damage and how community nurses might reasonably interpret the guidelines on this.
KEYWORDS:Wound care Unstageable pressure ulcers Eschar Key performance indicators
Pauline Beldon
THE SCIENCE — PRESSURE ULCERS
Pressure ulcers are defined as localised injuries to the skin as well as underlying tissue.
They usually occur over bony prominences and involve pressure, or pressure in combination with shear. Pressure ulcers most commonly occur on the sacrum and heel, but can be found over any bony prominence and, although more prevalent in the elderly, can affect patients of any age, in any care setting (EPUAP/NPUAP/PPPIA, 2014).
Cre
dit:
Esse
nt@
wik
icom
mon
s
© 2014
Wou
nd C
are P
eople
Ltd
34 JCN 2014, Vol 28, No 5
However, an additional category in the updated 2009/2014 guidance — unstageable or unclassified pressure damage — has caused some consternation in the UK, mainly because, although it does assist the clinician in classifying the presence of a serious ulcer of more than full dermal thickness, it does not help to define the actual grade. Similarly, many clinicians are either unwilling to use the term ‘ungradeable’ or feel under pressure from their healthcare organisation to state a definitive grade for a pressure ulcer. The EPUAP/NPUAP/ PPPIA (2014) additional criteria of ‘unstageable’ pressure damage clearly states that:
‘Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown or black) in the wound bed. Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and, therefore, category/stage, cannot be determined.’
Clearly, it is difficult for any community nurse to accurately grade pressure damage until
WOUND CARE
— they might report being trapped in the same position for an extended period after a fall, for example, or complain of pain in specific areas overlying bony prominences.
In these situations, the community nurse should be doubly vigilant and in the author’s opinion can reasonably prepare for the potential development of pressure damage, which may not yet have fully presented.
A full assessment requires the community nurse to gather as much evidence as possible, including the patient’s medical background, especially if they are insensate and unable to feel or detect discomfort (Clarke, 2010). Similarly, if an older person, for example, has an underlying painful comorbidity (i.e. a joint affected by rheumatoid arthritis), she may not be able to determine whether any discomfort originates from pressure damage or the pre-existing medical problem.
GRADING
Before 2003, there were a number of different pressure ulcer grading scales used in the UK, for example, the Scottish Pressure Sore Severity Scale (SPSSS) (Reid and Morrison, 1994) and the Torrance Scale (Torrance, 1983). This not only resulted in a lack of consensus regarding the severity of pressure ulcers, it also meant that any data collected internally had little relevance outside a particular healthcare organisation. Similarly, it was impossible to compare data between trusts or with centres in other countries (Bell, 2005).
In 2003, the European Pressure Ulcer Advisory Panel (EPUAP), published guidance on pressure ulcer classification, which finally provided a standardised grading system. This guidance was updated in 2009 in collaboration with the US National Pressure Ulcer Advisory Panel (NPUAP) and again recently in collaboration with the Pan Pacific Pressure Injury Alliance (EPUAP/NPUAP/PPPIA, 2014). This guidance has now been adopted throughout the UK (Table 1).
than holding the responsibility of pressure ulcer grading themselves.
In the author’s opinion, it is also unrealistic for any organisation to expect community nurses to determine pressure ulcer grading without explicit education and training. Each organisation needs to be robust in providing this.
ACCURATE ASSESSMENT
It is imperative that community nurses are able to perform a robust pressure ulcer risk assessment (NICE, 2014a). This includes the patient’s home/personal circumstances and any recent events such as falls or changes in equipment, i.e. a new wheelchair, that might have contributed to any pressure damage.
Perhaps the most reliable witnesses are patients themselves
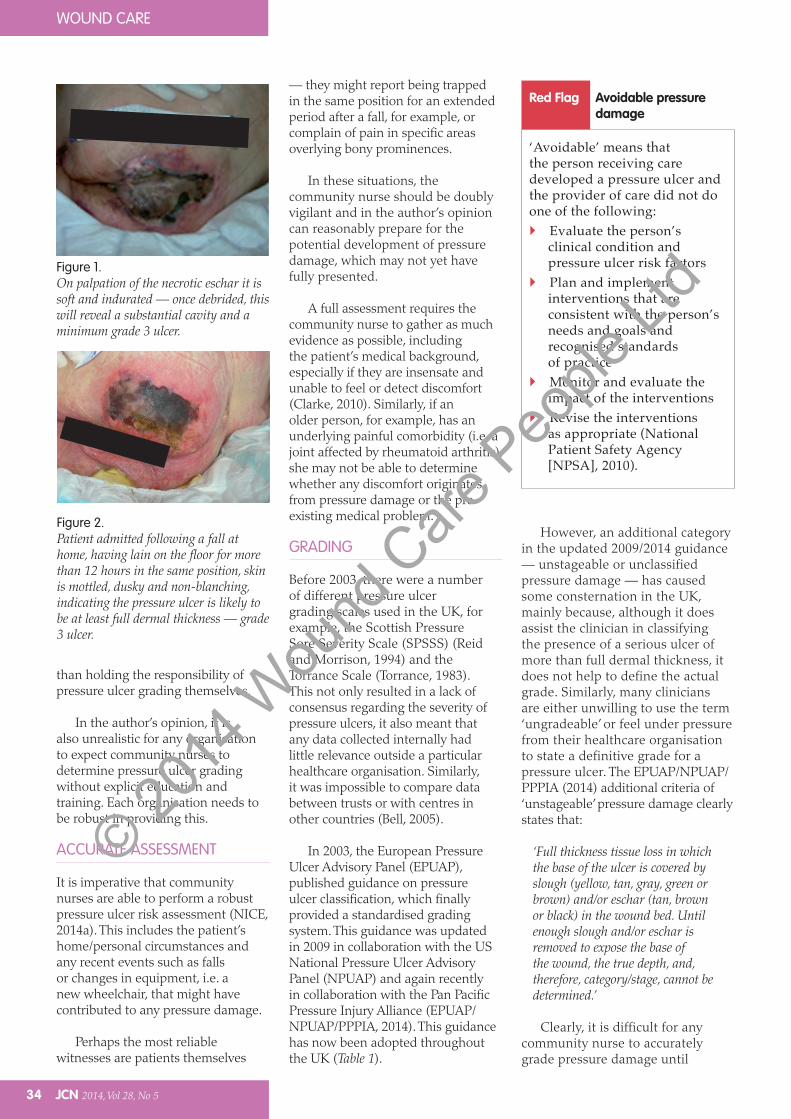
Figure 1.On palpation of the necrotic eschar it is soft and indurated — once debrided, this will reveal a substantial cavity and a minimum grade 3 ulcer.
Figure 2.Patient admitted following a fall at home, having lain on the floor for more than 12 hours in the same position, skin is mottled, dusky and non-blanching, indicating the pressure ulcer is likely to be at least full dermal thickness — grade 3 ulcer.
Red Flag Avoidable pressure damage
‘Avoidable’ means that the person receiving care developed a pressure ulcer and the provider of care did not do one of the following: Evaluate the person’s
clinical condition and pressure ulcer risk factors
Plan and implement interventions that are consistent with the person’s needs and goals and recognised standards of practice
Monitor and evaluate the impact of the interventions
Revise the interventions as appropriate (National Patient Safety Agency [NPSA], 2010).
© 2014
Wou
nd C
are P
eople
Ltd
Dedicated to Exudate Management
Crawford Healthcare Ltd | King Edward Court | King Edward Road | Knutsford
Cheshire | WA16 0BE | UK | Tel +44 (0)1565 654920 | Email [email protected]
KerraMax & KerraMax Care are trade marks of Crawford Woundcare Ltd | © Copyright Crawford Healthcare Ltd, 2014.
You’ve seen the suffering that chronic wounds can cause.
The exudate can be relentless.
The pain can be unbearable.
His granddaughter won’t visit because of the smell.
Then, one day, you try KerraMax Care.™
It removes the wetness, and in doing so, helps control infection.
And then, you’ve turned a corner.
Daily dressing changes aren’t needed.
With the pain gone, appetite is recovered.
His confidence returns.
And a relationship between grandparent and
child begins all over again.
He has a life because you made a choice.
EFFECTIVENESS OF CARE
PATIENTSAFETYPATIENT
EXPERIENCE
Better careSafer productsHappier patients
That’s our domain
NEW adhesive
border now
available
© 2014
Wou
nd C
are P
eople
Ltd
36 JCN 2014, Vol 28, No 5
that they have developed pressure damage, even though there may not be any clear early signs. On examination, the skin may be mottled and have a bruised appearance, but appear level with the surrounding skin with non-blanching erythema.
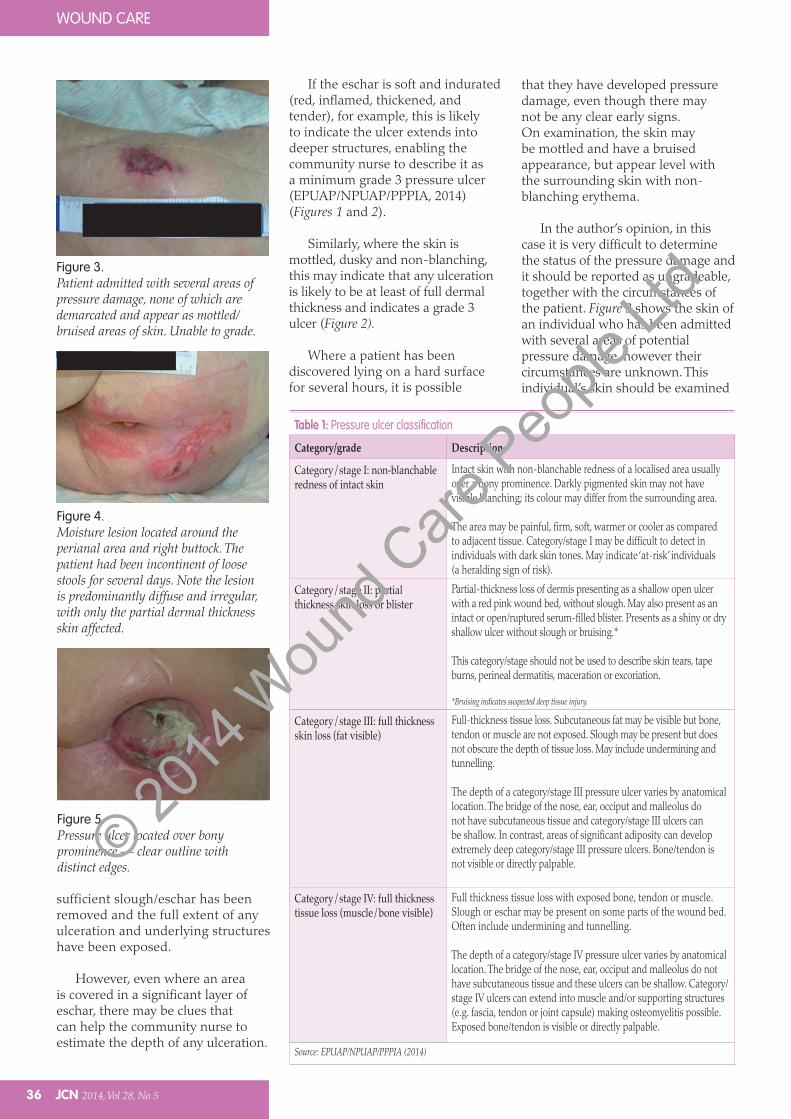
In the author’s opinion, in this case it is very difficult to determine the status of the pressure damage and it should be reported as ungradeable, together with the circumstances of the patient. Figure 3 shows the skin of an individual who has been admitted with several areas of potential pressure damage, however their circumstances are unknown. This individual’s skin should be examined
sufficient slough/eschar has been removed and the full extent of any ulceration and underlying structures have been exposed.
However, even where an area is covered in a significant layer of eschar, there may be clues that can help the community nurse to estimate the depth of any ulceration.
If the eschar is soft and indurated (red, inflamed, thickened, and tender), for example, this is likely to indicate the ulcer extends into deeper structures, enabling the community nurse to describe it as a minimum grade 3 pressure ulcer (EPUAP/NPUAP/PPPIA, 2014) (Figures 1 and 2).
Similarly, where the skin is mottled, dusky and non-blanching, this may indicate that any ulceration is likely to be at least of full dermal thickness and indicates a grade 3 ulcer (Figure 2).
Where a patient has been discovered lying on a hard surface for several hours, it is possible
WOUND CARE
Figure 3.Patient admitted with several areas of pressure damage, none of which are demarcated and appear as mottled/bruised areas of skin. Unable to grade.
Figure 4.Moisture lesion located around the perianal area and right buttock. The patient had been incontinent of loose stools for several days. Note the lesion is predominantly diffuse and irregular, with only the partial dermal thickness skin affected.
Figure 5.Pressure ulcer located over bony prominence — clear outline with distinct edges.
Table 1: Pressure ulcer classification
Category/grade Description
Category/stage I: non-blanchable redness of intact skin
Intact skin with non-blanchable redness of a localised area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its colour may differ from the surrounding area.
The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Category/stage I may be difficult to detect in individuals with dark skin tones. May indicate ‘at-risk’ individuals (a heralding sign of risk).
Category/stage II: partial thickness skin loss or blister
Partial-thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled blister. Presents as a shiny or dry shallow ulcer without slough or bruising.*
This category/stage should not be used to describe skin tears, tape burns, perineal dermatitis, maceration or excoriation.
*Bruising indicates suspected deep tissue injury.
Category/stage III: full thickness skin loss (fat visible)
Full-thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunnelling.
The depth of a category/stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and category/stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep category/stage III pressure ulcers. Bone/tendon is not visible or directly palpable.
Category/stage IV: full thickness tissue loss (muscle/bone visible)
Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunnelling.
The depth of a category/stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow. Category/stage IV ulcers can extend into muscle and/or supporting structures (e.g. fascia, tendon or joint capsule) making osteomyelitis possible. Exposed bone/tendon is visible or directly palpable.
Source: EPUAP/NPUAP/PPPIA (2014)
© 2014
Wou
nd C
are P
eople
Ltd
Advancis Medical
@AdvancisMedical
+44 (0)1623 751500
MAR382
References (references relate to Advancis Manuka honey)* taken from ‘International consensus: Appropriate use of silver dressings in wounds’ - Wounds International 2012
Effective exudate management1
Maintains a moist wound healing enviroment
Optimum Moisture Vapour Transfer Rate1
Unique range of sizes
The use of
Activon Manuka Honey®
and Eclypse®
Viral and bacterial backing barrier
Strike-through barrier1
Up to 7 days wear time
The perfect combination
© 2014
Wou
nd C
are P
eople
Ltd
38 JCN 2014, Vol 28, No 5
WOUND CARE
regularly during the day and on first appearance of damage, which should be clearly documented.
It is also important for clinicians to remember that they should not reverse the grading as a pressure ulcer begins to heal, i.e. assume that as the wound becomes shallower a grade 3 ulcer will become a grade 2 ulcer, etc. On healing, the ulcer cavity fills with granulation tissue, which contracts, covering the cavity with epithelial tissue and gradually forming avascular scar tissue.
PRESSURE ULCERS AND MOISTURE LESIONS
The continuous presence of moisture against the skin — as a result of incontinence or sweat, for example — increases a patient’s susceptibility to pressure damage, hence the inclusion of moist skin as a risk factor in many pressure ulcer risk assessment tools (Norton et al, 1962; Bergstrom et al, 1987; Waterlow, 1987).
However, moisture, particularly in the perianal area, can also cause skin damage that is not related exclusively to pressure or shear, especially where enzymes contained in faeces and urine begin to break down the skin.
Wounds that develop due to the persistent presence of moisture, including faeces, urine, sweat and wound exudate, are known as moisture lesions (although moisture-associated skin damage [MASD] is becoming known as an umbrella term for the different
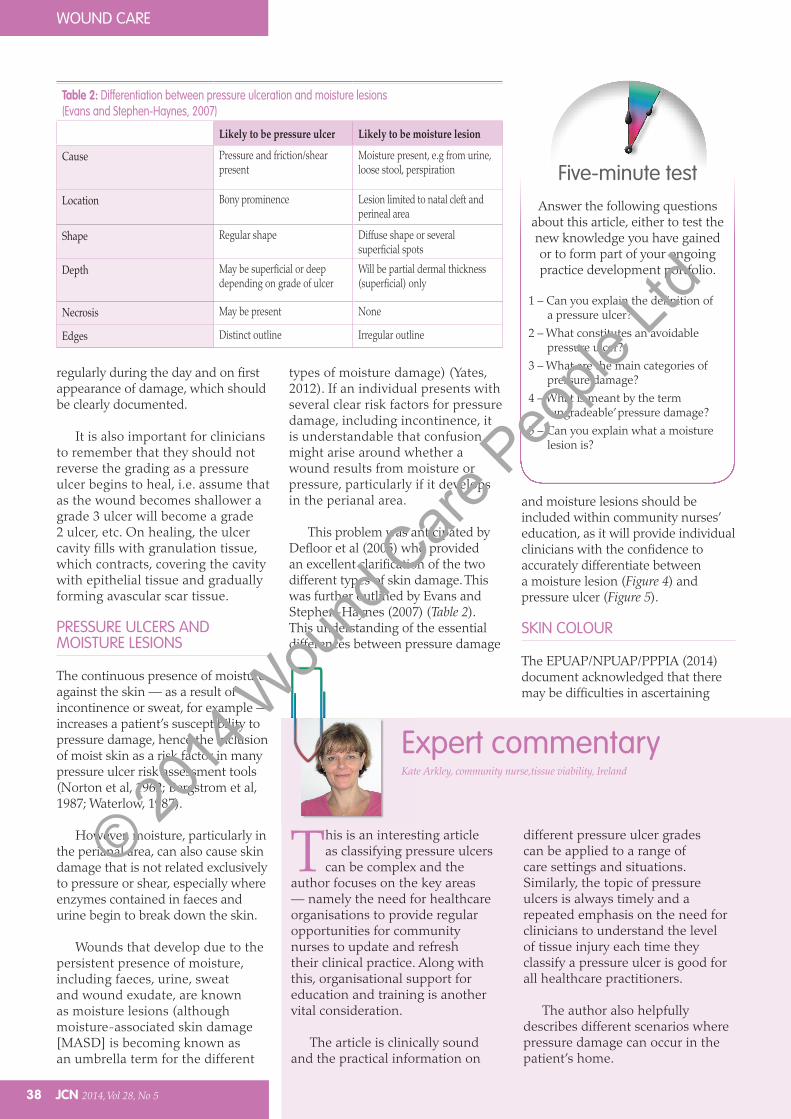
and moisture lesions should be included within community nurses’ education, as it will provide individual clinicians with the confidence to accurately differentiate between a moisture lesion (Figure 4) and pressure ulcer (Figure 5).
SKIN COLOUR
The EPUAP/NPUAP/PPPIA (2014) document acknowledged that there may be difficulties in ascertaining
types of moisture damage) (Yates, 2012). If an individual presents with several clear risk factors for pressure damage, including incontinence, it is understandable that confusion might arise around whether a wound results from moisture or pressure, particularly if it develops in the perianal area.
This problem was anticipated by Defloor et al (2005) who provided an excellent clarification of the two different types of skin damage. This was further outlined by Evans and Stephen-Haynes (2007) (Table 2). This understanding of the essential differences between pressure damage
Answer the following questions about this article, either to test the new knowledge you have gained or to form part of your ongoing practice development portfolio.
1 – Can you explain the definition of a pressure ulcer?
2 – What constitutes an avoidable pressure ulcer?
3 – What are the main categories of pressure damage?
4 – What is meant by the term ‘ungradeable’ pressure damage?
5 – Can you explain what a moisture lesion is?
Five-minute test
This is an interesting article as classifying pressure ulcers can be complex and the
author focuses on the key areas — namely the need for healthcare organisations to provide regular opportunities for community nurses to update and refresh their clinical practice. Along with this, organisational support for education and training is another vital consideration.
The article is clinically sound and the practical information on
different pressure ulcer grades can be applied to a range of care settings and situations. Similarly, the topic of pressure ulcers is always timely and a repeated emphasis on the need for clinicians to understand the level of tissue injury each time they classify a pressure ulcer is good for all healthcare practitioners.
The author also helpfully describes different scenarios where pressure damage can occur in the patient’s home.
Expert commentaryKate Arkley, community nurse,tissue viability, Ireland
Table 2: Differentiation between pressure ulceration and moisture lesions (Evans and Stephen-Haynes, 2007)
Likely to be pressure ulcer Likely to be moisture lesion
Cause Pressure and friction/shear present
Moisture present, e.g from urine, loose stool, perspiration
Location Bony prominence Lesion limited to natal cleft and perineal area
Shape Regular shape Diffuse shape or several superficial spots
Depth May be superficial or deep depending on grade of ulcer
Will be partial dermal thickness (superficial) only
Necrosis May be present None
Edges Distinct outline Irregular outline
© 2014
Wou
nd C
are P
eople
Ltd
Read JCN’s newoptimised versionfor tablets and smartphones
JCN has been around for a while,but read it now 21st century style,via tablets and smart phones,online and in print
Visit: www.jcn.co.uk
© 2014
Wou
nd C
are P
eople
Ltd
40 JCN 2014, Vol 28, No 5
WOUND CARE
whether an individual with dark skin tone has blanching or non-blanching erythema. Similarly, if an individual with dark skin tone has been identified as at risk of pressure damage, there may be initial difficulties in determining whether pressure damage has actually occurred.
One clue to potential pressure damage in a person with a darker skin tone is where the skin in the affected area appears darker than the surrounding skin or has a blue/purple hue (EPUAP/NPUAP/PPPIA, 2014).
The community nurse should also check for localised changes in the texture and temperature of the skin and early signs of damage may include induration and increased warmth at the injury site (Sommers, 2011). Community nurses should acknowledge the difference in skin colour and adjust patient assessment where necessary to ensure a comprehensive skin assessment is performed — it is important to be aware that different signs may exist in darker-skinned persons.
It is important for all community nurses to recognise that the risk assessment of pressure damage is not a ‘one-off’ assessment, but rather a continuous and regular exercise, especially if the patient’s health deteriorates or circumstances change, i.e. different equipment, such as a new wheelchair cushion is used.
CONCLUSION
While it may be difficult at times to grade suspected pressure damage, it is a skill that is expected of community nurses, particularly where the pressure ulcer is clearly presented and without obscuring factors, such as a covering of slough.
It is important that community nurses and healthcare organisations acknowledge the need for education and training to enable nurses to better identify and classify pressure damage.
However, it is also important to acknowledge that there will be occasions where the extent of a
patient’s pressure damage is not immediately apparent, but that the possibility of deep pressure damage exists.
In these cases, the phrase ‘unable to determine; the ulcer is ungradeable at this time’ should be employed and clearly documented in the patient’s records. JCN
REFERENCES
Bell J (2005) Are pressure ulcer grading and risk assessment tools useful? Wounds UK 1(2): 62–9
Bergstrom N, Braden BJ, Laguzza A, Holman V (1987) The Braden Scale for predicting pressure sore risk. Nurs Res 36(4): 205–10
Calkin S (2013) Nurses face new focus on reducing pressure ulcers. Nurs Times Available at: www.nursingtimes.net/nursing-practice/specialisms/wound-care/nurses-face-new-focus-on-reducing-pressure-ulcers/5053787.article (accessed 15 August, 2014)
Clark M (2010) Skin assessment in dark pigmented skin; a challenge in pressure ulcer prevention. Nurs Times 106(30): 16–17
Defloor T, Schoonhoven L, Fletcher J, et al (2005) Statement of the European Pressure Ulcer Advisory Panel. Pressure Ulcer Classification: differentiation between pressure ulcers and moisture lesions. J Wound Ostomy Continence Nurs 32(5): 302–6
DH (2013) NHS Outcomes Framework for 2014/2015. Available at: www.gov.uk/government/uploads/system/uploads/attachment_data/file/256456/NHS_outcomes.pdf (accessed 15 August, 2014)
EPUAP/NPUAP/PPPIA (2014) Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Available at: http://www.epuap.org/wp-content/uploads/2010/10/Quick-Reference-Guide-DIGITAL-NPUAP-EPUAP-PPPIA-Oct2014.pdf (accessed 9 October, 2014)
Evans J, Stephen-Haynes J (2007) Identification of superficial pressure ulcers. J Wound Care 16(2): 54–6
NPSA (2010) Defining Avoidable and Unavoidable Pressure Ulcers. Available at: www.patientsafetyfirst.nhs.uk/ashx/Asset.ashx?path=/PressureUlcers/Defining%20avoidable%20and%20unavoidable%20pressure%20ulcers.pdf (accessed 27 June, 2014)
NICE (2014a) CG179 Pressure ulcers: the prevention and management of pressure ulcers. Available at: www.nice.org.uk/guidance/cg179/resources/guidance-pressure-ulcers-prevention-and-management-of-pressure-ulcers-pdf (accessed 15 August, 2014)
NICE (2014b) Costing Statement: pressure ulcers. Implementing the NICE guideline on pressure ulcers (CG179). Available at: www.nice.org.uk/guidance/cg179/resources/cg179-pressure-ulcers-costing-statement2 (accessed 15 August, 2014)
Norton D, McLaren R, Exton-Smith AN (1962) An Investigation of Geriatric Nursing Problems in Hospital. National Corporation for the Care of Old People, London
Reid K, Morrison M (1994) Towards a consensus: classification of pressure sores. J Wound Care 3(3): 157–60
Pinkney L, Nixon J, Wilson L (2014) Why do patients develop severe pressure ulcers? A retrospective case study. Br Med J Open Available at: http://bmjopen.bmj.com/content/4/1/e004303.full (accessed 15 August, 2014)
Sommers MS (2011) Colour awareness: a must for patient assessment. Am Nurs Today 6(1): 8
Torrance C (1983) Pressure Sores: aetiology, treatment and prevention. Groom Helm, London
Waterlow J (1987) Calculating the risk. Nurs Times 83(39): 58–60
Yates S (2012) Differentiating between pressure ulcers and moisture lesions. Wound Essentials 2: 16–22
KEY POINTS While it may be difficult to grade
suspected pressure damage it is a skill that is expected of community nurses.
It is also important to acknowledge that sometimes the extent of pressure damage is not immediately apparent, but that the possibility of deep pressure damage exists.
In these cases, the phrase ‘unable to determine; the ulcer is ungradeable at this time’ should be employed.
Clinicians should not reverse the grading as a pressure ulcer begins to heal.
© 2014
Wou
nd C
are P
eople
Ltd





























