-
he ophthalmoscope (Figure 1), which was in-vented in 1850 by
Hermann von Helmholtz,1
allowed for the clinical correlation of retinalfindings with
many systemic diseases, such as
diabetes mellitus, hypertension, hyperlipidemia, thy-roid
disease, vascular disease, and systemic infections.Although ocular
signs are not necessarily disease specif-ic (eg, signs seen in
hypertensive patients also appearin diabetic patients), early
recognition of these signscan help prevent unnecessary vision
loss.2 Additionally,these signs in combination can help the
physiciandetermine which systemic disease is responsible for
thepatients retinopathy. A comprehensive discussion ofall systemic
diseases with ocular manifestations is be-yond the scope of this
article. Hence, this review focus-es on retinal findings associated
with two of the mostcommon diseases seen in primary care: diabetes
melli-tus and hypertension. A brief review of the techniquefor
ocular examination with the ophthalmoscope alsois included.
OCULAR EXAMINATION
A systematic routine should be used when examin-ing the eyes and
surrounding tissues.2,3 Generally, it isbest to examine the eyes in
the following sequence:visual acuity, extraocular muscle function,
visual fieldtesting, and then finally ophthalmoscopy.4,5 For
opti-mum retinal examination, a mydriatic agent is used todilate
the pupil.2 Both tropicamide 1% (Mydriacyl) andphenylephrine
hydrochloride 2.5% (Mydfrin) dilatethe pupils in approximately 30
minutes. Once the pa-tients eyes are dilated, the ophthalmoscope is
heldapproximately 12 to 15 cm away from the patients eye.For
examining the patients right eye, the examinerholds the
ophthalmoscope in close proximity to his orher own right eye using
the right hand. For examiningthe patients left eye, the examiner
uses the left handand left eye. The examiner then moves in closer
to thepatients eye while adjusting the lens settings for opti-
mal focus. The physician also should keep his or hernonexamining
eye open during this procedure.
DIABETES MELLITUS
Diabetes mellitus is the leading cause of new cases ofblindness
in middle-aged Americans.6,7 Timely detec-tion and treatment of
diabetic retinopathy can substan-tially reduce the likelihood of
blindness. Approximatelyhalf of adult diabetics in the United
States, however, donot receive yearly eye examinations.8
Type 2 diabetes mellitus is more common than type 1diabetes, and
the prevalence of type 2 diabetes increaseswith age. Type 2
diabetes may remain undetected for along time. It has been
estimated that 5 to 10 years of sus-tained hyperglycemia are needed
to develop retinalmanifestations.6 A high degree of correlation
existsbetween glycemic control as measured by
glycosylatedhemoglobin levels and presence of early
retinopathic
T
Dr. Gunderson is as Assistant Professor of Medicine and Director
ofPediatric Ophthalmology and Adult Strabismus, University of
TexasMedical Branch, Galveston, TX. Dr. Karnath is an Assistant
Professorof Internal Medicine, University of Texas Medical
Branch.
www.turner-white.com Hospital Physician November 2003 15
R e v i e w o f C l i n i c a l S i g n s
Series Editor: Bernard Karnath, MD
Retinal Manifestations of Diabetes Mellitus and Hypertension
Charlise A. Gunderson, MDBernard Karnath, MD
RETINAL SIGNS OF DIABETES AND HYPERTENSION
Microaneurysms Dot and blot hemorrhagesHard exudates Macular
edema Cotton-wool spotsNeovascularization Retinal edema Optic disc
edema
-
changes. As a rule, retinopathy precedes nephropathy.Therefore,
early detection of the ocular manifestationsof diabetes (Table 1)
is important.9
The initial stage of retinal changes in the diabeticpatient is
called nonproliferative diabetic retinopathy9,10
and includes the appearance of dot and blot hemor-rhages (which
are caused by intraretinal blood) and/ormicroaneurysms (Figure 2).
Microaneurysms are seenas scattered red spots in the retina caused
by weakenedarterioles and capillaries leading to outpouching of
thevessel walls. Dot and blot hemorrhages represent bloodin the
retina. The differentiation between a micro-aneurysm and a dot and
a blot hemorrhage is basedon size and is somewhat subjective.
Distinguishing be-tween a dot and blot hemorrhage and
microaneurysmon direct ophthalmoscopy may be difficult.
Several years may pass before other lesions, such asretinal
hemorrhages and exudates, develop.10,11 Hardexudates caused by
leakage of proteins and lipids fromthe damaged arterioles appear as
small white or yellowareas with sharp margins, often with a
glistening ap-pearance on the retina (Figure 3). As the disease
pro-gresses further, retinal changes occur, including macularedema
and cotton-wool spots (Figure 4). Cotton-woolspots result from
microinfarctions of nerve fibers causedby focal ischemia after
occlusion of terminal retinal arte-rioles occurs. These spots
appear as white fluffy spots onthe retina. Macular edema is the
principal mechanismof visual loss in nonproliferative retinopathy.
Macularedema results from leakage from microaneurysms.
Proliferative diabetic retinopathy is a late stage ofdisease and
is characterized by neovascularization (ie,new blood vessel
formation), which is a response tocontinued retinal ischemia.9
Neovascularization resultsin vision loss due to vitreous
hemorrhages and retinaldetachment.
16 Hospital Physician November 2003 www.turner-white.com
G u n d e r s o n & K a r n a t h : R e t i n a l M a n i f
e s t a t i o n s : p p . 1 5 1 8
Figure 1. A drawing of Hermann von Helmholtzs
originalophthalmoscope. (Reprinted with permission from Ravin
JG.Sesquicentennial of the ophthalmoscope. Arch
Ophthalmol1999;117:1636.)
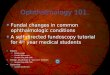
Figure 2. The arrow indicates dot and blot hemorrhages.Hard
exudates also are visible.
Figure 3. The arrow indicates hard exudates. Dot and
blothemorrhages also are visible.
Table 1. Subdivisions and Characteristic Lesions ofDiabetic
Retinopathy
Nonproliferative retinopathy
Microaneurysms
Hemorrhages
Hard exudates
Cotton-wool spots
Macular edema
Proliferative retinopathy
Neovascularization
-
HYPERTENSION
The funduscopic changes in the eye noted withhypertension were
first described in 1898.12 Since thattime, little has changed in
the terminology describingthese characteristic retinal
abnormalities. These char-acteristic retinal changes included
arteriolar narrow-ing, arteriovenous crossing changes, alterations
of lightreflexes on arterioles, cotton-wool spots, micro-aneurysms,
retinal hemorrhages, retinal edema, andblurred disc margins.13
The first and most widely used grading system forhypertensive
retinopathy was proposed by Keith et al.14
The classification system consists of 4 grades as follows:
Grade I: mild narrowing of the retinal arterioles
Grade II: arteriovenous nicking (ie, venous com-pression at
arteriovenous crossings) (Figure 5)
Grade III: cotton-wool spots, hemorrhages (Fig-ure 6), retinal
edema
Grade IV: optic disc edema (Figure 7)
A newer more simplified grading system was recent-ly proposed
and divides the features, according to
G u n d e r s o n & K a r n a t h : R e t i n a l M a n i f
e s t a t i o n s : p p . 1 5 1 8
www.turner-white.com Hospital Physician November 2003 17
Figure 4. The arrow indicates a cotton-wool spot.
Figure 5. Hypertensive retinopathy showing arteriovenousnicking
(arrow). (Reprinted with permission from BradfordCA. Basic
ophthalmology for medical students and primarycare residents. 7th
ed. San Francisco: American Academy ofOphthalmology; 1999:135.)
Figure 6. The arrow indicates retinal hemorrhages. Hardexudates
also are visible.
Figure 7. Malignant hypertension showing optic disc edema.Also
seen are flame-shaped hemorrhage, hard exudates, arte-rial
constriction, and cotton-wool spots. (Reprinted with per-mission
from Bradford CA. Basic ophthalmology for medicalstudents and
primary care residents. 7th ed. San Francisco:American Academy of
Ophthalmology; 1999:135.)
-
prognosis, into 2 categories: nonmalignant and malig-nant
hypertension.15 Nonmalignant findings includearteriolar narrowing
and arteriovenous nicking; malig-nant findings consist of
hemorrhages, hard exudates,cotton-wool spots, and optic disc edema.
Hard exu-dates in the macula would suggest diabetic
retinopathyversus hypertensive retinopathy in which the hard
exu-dates would more likely appear in the peripheral reti-nal
around a macroaneurysm. Optic disc edema canbe caused by other
conditions (eg, increased intracra-nial pressure); however, the
presence of cotton-woolspots is highly suggestive of malignant
hypertension asthe etiology of disc edema.16,17 In the case of
malignanthypertension, optic disc edema is caused by ischemicoptic
neuropathy.16 Papilledema develops within daysto weeks of increased
blood pressure and resolves with-in weeks to months following
lowering of blood pres-sure.
Retinal vascular abnormalities, such as arteriolarnarrowing and
arteriovenous nicking, are irreversiblelong-term markers of
hypertension. These nonmalig-nant hypertensive retinal vascular
changes persist longterm even after successful antihypertensive
therapy.18
Retinal vascular abnormalities are useful risk indicatorsfor
cerebrovascular disease and stroke.19
Early detection of malignant hypertension is essen-tial in
reducing the likelihood of permanent visualdamage.20 Malignant
hypertensive retinal changes suchas papilledema, cotton-wool spots,
and hemorrhagesresolve if blood pressure is well controlled.18
Malignanthypertensive retinal changes are likely findings
inpatients in hypertensive crisis, which is an abrupt eleva-tion in
blood pressure with a systolic blood pressure ofgreater than 210 mm
Hg and a diastolic blood pressureof more than 120 mm Hg.
Ischemic optic neuropathy is a common cause ofvisual loss.
Hypertension is the most frequently report-ed underlying disease.
Ischemic optic neuropathy is adirect complication of hypertension,
which affects thesmall arterioles supplying the anterior part of
the opticnerve. Patients with ischemic optic neuropathy fre-quently
report blurred vision, and funduscopic exami-nation reveals optic
disc edema.
CONCLUSION
Hypertension and diabetes are commonly encount-ered systemic
diseases in primary care. A thorough eyeexamination can uncover
retinal manifestations ofthese disease processes and thus prevent
further dam-age leading to visual impairment. A basic
understand-ing of these common retinal manifestations is
essentialin primary care. HP
REFERENCES1. Ravin JG. Sesquicentennial of the
ophthalmoscope.
Arch Ophthalmol 1999;117:16348.2. Bradford CA. Basic
ophthalmology for medical students
and primary care residents. 7th ed. San Francisco: Amer-ican
Academy of Ophthalmology; 1999.
3. Frith P, Gray R, Maclennan S, Ambler P. The eye in clini-cal
practice. 2nd ed. Malden (MA): Blackwell Science;2001.
4. Seidel HM, Ball JW, Dains JE, Benedict GW. Mosbys guideto
physical examination. 4th ed. St. Louis: Mosby; 1999.
5. Bickley LS. Bates guide to physical examination and his-tory
taking. 7th ed. Philadelphia: Lippincott, Williams &Wilkins;
1999.
6. Aschner P. Current concepts of diabetes mellitus.
IntOphthalmol Clin 1998;38:110.
7. Brechner RJ, Cowie CC, Howie LJ, et al. Ophthalmicexamination
among adults with diagnosed diabetes mel-litus. JAMA
1993;270:17148.
8. Javitt JC, Aiello LP. Cost-effectiveness of detecting
andtreating diabetic retinopathy. Ann Intern Med 1996;124(1 Pt
2):1649.
9. DAmico DJ. Diseases of the retina. N Engl J Med
1994;331:95106.
10. Feman SS. The natural history of the first clinically
visiblefeatures of diabetic retinopathy. Trans Am OphthalmolSoc
1994;92:74573.
11. Doft BH, Kingsley LA, Orchard TJ, et al. The
associationbetween long-term diabetic control and early
retinopa-thy. Ophthalmology 1984;91:7639.
12. Walsh JB. Hypertensive retinopathy. Description,
classifi-cation, and prognosis. Ophthalmology 1982;89:112731.
13. Wagener HP, Clay GE, Gipner JF. Classification of
retinallesions in the presence of vascular hypertension.
Oph-thalmol Trans Am Sci 1947;45:5773.
14. Keith NM, Wagener HP, Barker NW. Some differenttypes of
essential hypertension: their course and progno-sis. Am J Med Sci
1939;197:33243.
15. Dodson PM, Lip GY, Eames SM, et al. Hypertensiveretinopathy:
a review of existing classification systemsand a suggestion for a
simplified grading system. J HumHypertens 1996;10:938.
16. Wall M. Optic disk edema with cotton-wool spot.
SurvOphthalmol 1995;39:5028.
17. Lee AG, Beaver HA. Acute bilateral optic disk edemawith a
macular star figure in a 12-year-old girl. Surv Op-thalmol
2002;47:429.
18. Bock KD. Regression of retinal vascular changes by
anti-hypertensive therapy. Hypertension 1984;6(6 Pt
2):III15862.
19. Wong TY, Klein R, Couper DJ, et al. Retinal microvascu-lar
abnormalities and incident stroke: the AtherosclerosisRisk in
Communities Study. Lancet 2001;358:113440.
20. Browning AC, Mengher LS, Gregson RM, Amoaku WM.Visual
outcome of malignant hypertension in youngpeople. Arch Dis Child
2001;85:4013.
18 Hospital Physician November 2003 www.turner-white.com
G u n d e r s o n & K a r n a t h : R e t i n a l M a n i f
e s t a t i o n s : p p . 1 5 1 8
Copyright 2003 by Turner White Communications Inc., Wayne, PA.
All rights reserved.