Embed Size (px)
Citation preview

Why Find Disease Genes?
Acceleratedby finding
the disease gene

•Virtually all diseases result from a combination of genes and environmental factors
•We have no systematic ways to discover environmental risk factors
•We do have systematic ways discover disease genes
•Discovery of disease genes will provide clues to pathogenic mechanisms, new
approaches to treatment, inference of environmental risk factors, and ultimately disease prevention•Personalized medicine ( = “Precision Medicine”)
Why Find Disease Genes?
The Holy Grail

Personalized/Precision Medicine Paradigm
• Discover risk genes for common diseases, specific risk variants, high-risk combinations
• Carry out accurate DNA-based predictive diagnostics of disease susceptibilities based on individualized genetic risks
• Apply optimized individualized treatment or prevention based on genetic diagnosis of disease susceptibilities and pharmacogenetic
• analysis of optimized drug efficacy/specificity• This is why there was a Human Genome Project

Personalized/Precision Medicine Paradigm--Problems
•For most common complex traits, individual genes/variants confer low odds ratio OR = Risk of disease having a given gene variant / Risk of disease not having variant Population/study wide; no meaning at level of individual
•We do not yet know how to do “combinatorial” complex trait risk prediction Genetic risk scores
•For most complex diseases it has been hard to account for much of the ‘heritability’ of the trait H2 = (Var G) / (Var P)
•Low positive predictive value of genetic tests for complex traits significant non-genetic component late onset

Hunting for Disease Genes
1. In a “Mendelian”, single-gene trait, one gene is sufficient to cause (most of) the disease phenotype2. In a polygenic/multifactorial, “complex” trait, no one gene is sufficient to cause the disease phenotype

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome

Disease Gene Identification—“Functional Cloning” vs. “Positional Cloning”

Positional Cloning: Determine a Disease Gene’s Genomic Position, and then
Identify the GeneObviated by
Human Genome Project

• You can only track/measure differences between people and through families
• Polymorphic DNA markers constitute any scorable differences at known genomic positions
• Surrogates for disease mutations; some polymorphisms cause disease; most don’t
• Most commonly used marker types:– microsatellites– single-nucleotide polymorphisms (SNPs)– copy-number variations (CNVs)
Gene Mapping Technology Polymorphic DNA Markers

The First Goal of the HGP was to Assemble a High-Density Genome Map
of Polymorphic Markers

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome
Most hypotheses wrong!

Genetic Linkage Studies
•Studies families•Search for regions of genome that are systematically co-inherited along with disease on passage through families•Requires families with multiple affected relatives (multiplex families)•Best at detecting genes with Mendelian effects (uncommon alleles with strong effects)•Unit of genetic linkage is LOD (“Log of the Odds) score (>3)

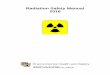
Principle of genetic linkage—Loci close by on a chromosome tend not to be separated by recombination vs. loci far apart
Loci on the same chromosome Loci on different chromosomes Very close Nearby Far Apart
Freq. of crossover Rare Some Frequent - between 2 loci
Linkage Tight Some Absent Absent
Recombination 0% 1-49% 50% 50%
• Unit of genetic “distance” is centiMorgan (cM) = 1% recombination/meiosis; ~ 1 Mb

Genetic Linkage Analysis
• Statistical measure is LOD (log of odds) score
• Significance level: LOD >3.0 for Mendelian trait LOD >3.3 for Polygenic
trait
Likelihood of data if loci unlinked
Likelihood of data if loci linked at LOD = Log10

Restriction Fragment Length Polymorphism (RFLP)
EcoRI
Allele 1 AGAGCCTCAACTTGAATTCGTTTAGTAA
Allele 2 AGAGCCTCAACTTGAATTTGTTTAGTAA
Restriction enzyme EcoRI cuts at sequence
5’-GAATTC-3’
Allele 1 has an EcoRI cut site; Allele 2 does not• This RFLP is assaying a SNP


“Genetic linkage analysis”Co-segregation of disease gene in “multiplex
families” with alleles of polymorphic DNA “markers” (initially RFLPs)

“Microsatellites” (SSLPs; STRPs, SSRs) [multi-allelic; ~ 1/30,000 bp; mostly used for
linkage analysis, forensics]
ggctgcacacacacacacacacacacacatgctt
ggctgcacacacacacacacacacacatgctt
ggctgcacacacacacacacacacatgctt
ggctgcacacacacacacacacatgctt
ggctgcacacacacacacacatgctt

Can follow “segregation” of ancestral “haplotypes” of linked marker alleles along a chromosome through families

Recombination events prune marker haplotypes, defining “genetic interval” that
must contain the disease gene

Single-Nucleotide Polymorphisms (SNPs) [bi-allelic; ~1/50-300 bp; mostly used for
association analysis]SNP1 Allele 1 CCGAGATCCAGAAATCCTGAACATAA
SNP1 Allele 2 CTGAGATCCAGAAATCCTGAACATAA
SNP2 Allele 1 CCGAGATCCAGAAATCCTGAACATAA
SNP2 Allele 2 CCGAGATCCAGAAAGCCTGAACATAA
• Occurrence/allele frequencies differ in different ethic groups/populations
• Can be in genes (~4,000,000) on not (~8,000,000), can result in amino acid substitutions or not
• Each occurs in local context (haplotype) of surrounding SNPs (in example above, SNP2 is on background of SNP1 C allele)

Haplotype Map of Human GenomeInternational HapMAP Project
•Recombination breaks macro-patterns of polymorphic genotypes on the same chromosome into haplotypes
•Recombination is not truly random, so very close polymorphism genotypes on the same chromosome cluster into ~10-50 kb haplotype blocks in which SNP alleles are in linkage disequilibrium (marker alleles within blocks tend to be co-inherited, because recombination within blocks is uncommon)
•Blocks smaller in African than Caucasian or Asian pops. because African pop. is more ancient
•HapMap genotyped SNPs in different populations to characterize haplotype block distributions

Copy-Number Variants (CNVs) [bi-allelic]
Basically are common genomic deletions, hundreds to tens of thousands of nucleotides in size
May be detected by LD with local SNP patterns:
Allele --1---1---1----1---2----1----2----1-----1----2----1----1----1----1---Allele --2---2---2----1---1----2----2----1-----1----2----2----2----1----2---CNV Allele --1---1—[ ]--1----2---
• Tens of thousands known• Like SNPS, occurrence/allele frequencies differ in different
ethic groups/populations• Individually most are rare (< 1%), collectively common• Can be in genes or not, can include genes• NOT commonly definitively causal for human disease

1000 Genomes Project, UK10K Project International projects to sequence 1000/10000
genomes from different ethnic groups
• Catalog human genetic variations (particularly SNPs, indels)– ~60,000,000 SNPs now known– Essential for sequence-based analysis of rare variants that may be causal for
common diseases

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome
Most hypotheses wrong!

Common, Complex Diseases
• Asthma• Autism• Obesity• Preterm birth• Cleft lip/palate• IBD• Diabetes• Cancers• Common traits like height

Common, Complex DiseasesUtility of Experimental Approaches
CommonCommon
RISK ALLELE RISK ALLELE FREQUENCYFREQUENCY
RareRare
SmallSmall LargeLargeEFFECT SIZE (OR)EFFECT SIZE (OR)
GWASGWAS
LinkageLinkageRe-SequencingRe-Sequencing

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome

Hypothesis-Driven Approaches
Candidate genes Depends on:
biological hypothesis (biological candidate) positional hypothesis / information (positional
candidate)
Sometimes successful in Mendelian disorders Low yield in polygenic, multifactorial
(“complex”) disorders—pathogenic sequence variants not obvious, often present in normal individuals
Most hypotheses wrong!

Candidate Gene Association Study
Concept:Causal disease variation in gene suggested by known biology ‘tagged’ by nearby polymorphic DNA markers; test for co-occurrence.Because:DNA sequence variations very close together on the same piece of DNA will tend to not be separated by recombination over long periods, and so will be non-randomly co-inherited even on a populationbasis (“linkage disequilibrium”).Most hypotheses wrong!

Candidate Gene Association Studies Compares SNP allele frequencies in cases
versus controls (“case-control” study design) Easy statistics (Fisher exact test, Chi-square) Must Bonferroni correct for multiple-testing Must ethnically match cases and controls Easy, cheap Most powerful for common risk alleles Can detect common alleles with small allele-
specific effects (i.e. “complex”, polygenic traits)
Most common published type of “genetic study”
Most hypotheses wrong! Most (~96%) such published studies wrong!!

Three Fatal Flaws in Gene-by-Gene Case-Control Design
• Must apply multiple-testing correction; true denominator often not known
• Must ethnically match cases & controls; otherwise, differences in allele frequencies may reflect different genetic backgrounds of cases vs. controls
• Positive studies result in publication bias

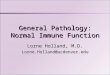
“Population stratification” and false-positive case-control genetic association studies
Population 1 Population 2
Admixed Study Population 1/2
Cases Controls
Disease
blue/green just indicates overall genetic background
Prof. Wizard’s Prof. Wizard’s Case-Control Case-Control
StudyStudy
Eureka!

Hypothesis-Free Approaches Genome-Wide Association Studies (GWAS)
Relatively recent approach (>300 published):
•Genotype hundreds of thousands to millions of SNPs across genome using microarrays; extremely expensive•Case-control or family-based (trio) design•Requires no hypotheses about pathogenesis; can discover new genes•Can discover common alleles with small effects•Can provide very fine localization

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome

Hypothesis-free approachesGenome-wide association studies (GWAS)
• Study self-contained; can apply appropriate multiple testing correction
- “Genomewide significance” P < 5 x 10-8
• Still requires ethnic matching of cases and controls- Can correct for population stratification by
“Principal components” analysis- Can correct for residual “Genomic inflation
factor” by “genomic control”• Can discover new, unknown genes; power similar to
candidate gene case-control study• Case-control “associations” require independent
confirmation

The Genomewide Association Study (GWAS)
Manolio TA. N Engl J Med 2010;363:166-176.

Meta-Analysis of Multiple Genomewide Association Studies

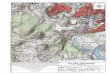
Genome-Wide Association Studies“Manhattan plot”
Per-SNP -log(P values)across genomefor association ofSNP allele freq.differences between patientswith generalizedvitiligo versuscontrols (all Caucasian)

Genome-Wide Association Studies
• Very large number of SNPs tested (500,000 – 2,000,000) presents huge multiple-testing problem; requires at least ~1000 cases and ~1000 controls• Many SNPs in linkage disequilibrium (i.e. correlated); simple Bonferroni correction too strict (assumes independence)•“Significant” associations require confirmation by independent follow-up association study of specific SNPs to reduce multiple-testing complexity

Personalized MedicineThe case of the ‘missing heritability’
• Disease risk genes found by GWAS account for only a small fraction of genetic risk >Type 1 diabetes-- ~100 genes, ~70% of genetic risk 50% of risk due to HLA class II
• Are there a virtually unlimited number of additional genes, each conferring small additional risk?
>Maybe• Have we under-estimated fraction of genetic risk already
accounted for?>Maybe. GWAS misses rare risk alleles
• Have we over-estimated total genetic component of risk? >Maybe, but not ten-fold

Hypotheses of Common, “Complex” Disease
• Common disease, common variant hypothesis (Reich & Lander, 2001)
versus
• Rare variant hypothesis (Pritchard, 2001; Prixhard and Cox, 2002)

Complex DiseasesUtility of Experimental Approaches
CommonCommon
RISK ALLELE RISK ALLELE FREQUENCYFREQUENCY
RareRare
SmallSmall LargeLargeEFFECT SIZE (OR)EFFECT SIZE (OR)
GWASGWAS
LinkageLinkageRe-SequencingRe-Sequencing

Combined hypothesis-based and hypothesis-free approaches
Deep re-sequencing
• High-throughput DNA sequencing• Biological candidate genes • GWAS signals (specific genes or genes
within regions)• Must distinguish potentially causal variants
from non-pathological variation (1000 Genomes Project data will help)
• Prioritize for follow-up functional analyses

How Do You Find Disease Genes?
I. Hypothesis-driven approachesCandidate gene associationCandidate gene sequencing
II. Hypothesis-free approachesGenomewide linkageGenomewide association(Genomewide expression)Genomewide sequencing
ExomeFull-genome

Hypothesis-free approach
Exome/Genome sequencing
• High-throughput DNA sequencing- Genome- Exome (1% of genome)
• Must distinguish potentially causal variants from non-pathological variation (1000 Genomes Project data will help)
- Predict based on Mendelian inheritance- Compare across unrelated families
• Prioritize for follow-up functional analyses

Exome Sequencing in Mendelian DiseasesMethod
E
Exome = Gene coding regions; ~ 3 Mb (1% of genome)

How Do You Find Disease Genes?Exome/Genome Sequencing in Mendelian Diseases
There is a lot of genomic ‘noise’
E
There is a lotof noise!!

Variant Filtering in Exome/Genome Sequencing
• Missense (non-synonymous) substitutions- Most rare (<1%) missense may be deleterious
• Nonsense, frameshift mutations• Splice junction mutations• Exonic splice enhancer mutations• INDELs, CNVs, translocations• Regulatory Feature variants

How Do You Find Disease Genes?Exome/Genome Sequencing in Mendelian Diseases
Filtering Schemes
E

How Do You Find Disease Genes?Exome/Genome Sequencing in Mendelian Diseases
Exome sequencing is rapidly becoming a fairly routine clinical test, costing ~$1000, ordered in lieu of tens of thousands of dollars worth of functional clinical tests in a patient one believes might have a genetic (principally single-gene Mendelian) cause for their disorder.
Who will do the interpretation of the data, how will “variants of unknown significance” (VUS) be addressed, and what will that cost?