Embed Size (px)
Citation preview

CIRCULATORY EFFECTS OF CHRONICHYPERVOLEMIA IN POLYCYTHEMIA VERA
Leonard A. Cobb, … , Robert J. Kramer, Clement A. Finch
J Clin Invest. 1960;39(11):1722-1728. https://doi.org/10.1172/JCI104194.
Research Article
Find the latest version:
http://jci.me/104194/pdf

CIRCULATORYEFFECTS OF CHRONICHYPERVOLEMIAINPOLYCYTHEMIAVERA*
By LEONARDA. COBB, ROBERTJ. KRAMERAND CLEMENTA. FINCH
(From the Department of Medicine, School of Medicine, University of Washington,Seattle, Wash.)
(Submitted for publication May 11, 1960; accepted July 21, 1960)
In this study the relationship of cardiac outputto oxygen supply on the one hand and to bloodvolume on the other is examined in patients withpolycythemia vera.
Oxygen supply is a function of the cardiac out-put and the oxygen content of arterial blood.There is good evidence that cardiac output maybe altered by changes in either tissue oxygen re-quirements or oxygen content. Thus, with in-creased physical activity or hyperthyroidism, car-diac output is elevated. Likewise, in severe ane-mia or with the hypoxia of high altitude, cardiacoutput rises. The relationship between cardiacoutput and arterial oxygen content was well il-lustrated by Richardson and Guyton in dogs whosehematocrits were rapidly altered by blood ex-change without blood volume change (1). Car-diac output fell with polycythemia and rose withanemia; maximal oxygen delivery occurred at anormal hematocrit. From the above considera-tions it would seem reasonable to postulate thatcardiac output is regulated in some manner by tis-sue oxygen requirements and blood oxygen con-centration.
The influence of blood volume as a cardiac regu-latory mechanism has been demonstrated in dogsas well as in man (24). Such observations fol-lowing the acute manipulation of blood volumehave shown an augmentation of cardiac outputand stroke volume in hypervolemia. The effectsof chronic hypervolemia in cardiovascular regu-lation have not been reported.
Polycythemia vera presents an interesting situ-ation in which the above factors may be examined.There is a long-standing surplus of hemoglobinand blood oxygen without a proportionate in-
* These studies have been supported in part by grantsfrom the United States Public Health Service (H-908-C8and H-2994), the Washington State Heart Association,and State of Washington Initiative 171 Funds for Re-search in Biology and Medicine.
crease in tissue oxygen requirements; further-more, blood volume is increased in polycythemiavera. The increased arterial oxygen content andblood viscosity might be expected to decreasecardiac output, whereas chronic hypervolemiamight have the opposite effect. Our studies weredesigned to evaluate these possibilities.
MATERIAL AND METHODS
Three types of subjects were selected for study. GroupIa consisted of 6 subjects with incidental illness not con-sidered to affect erythropoiesis or cardiac function.These individuals were ambulatory and asymptomatic:they had hematocrits between 40 and 50 per cent andnormal blood volumes. There was no recognizable cardiacor pulmonary disease. Electrocardiograms were all nor-mal, and heart size by X-ray was not enlarged. Grouplb consisted of 4 subjects with hematocrits of 50 to 55per cent and with normal or only slightly enlarged bloodvolumes. These subjects also had no evidence of cardiacor pulmonary disease. X-rays showed normal sizedhearts and, except for isolated left axis deviation in D.G.,electrocardiograms were normal.
Group II consisted of 10 patients with polycythemiavera, 5 of whom had symptoms of approximately 1month's duration. The other 5 had been previouslytreated, but were all polycythemic and hypervolemic atthe time of initial studies. The spleen was palpable inall subjects except S.Ta., S.Tu. and B.P. Electrocardio-grams were normal, except for left ventricular hypertrophyin Patient S.Ta. and right bundle branch block in B.P.Patient A.L. had a previous history of paroxysmal auricu-lar fibrillation. Cardiac enlargement of 25, 20 and 25per cent was present in Patients S.Ta., G.S. and A.L.,but was normal in the other subjects (± 10 per cent).Pertinent clinical data on the 20 subjects studied aresummarized in Tables I and II.
Single studies were performed in Groups Ia and lb. In7 patients with polycythemia vera, studies were repeatedafter phlebotomy. The patients were in the supine posi-tion when the hemodynamic measurements were made1 to 3 hours after a light nonfat breakfast. No premedi-cation was given. Intravascular pressures were re-corded on a Sanborn polygraph using Statham P23Dstrain gage transducers. Heart rate was measured fromthe electrocardiogram obtained during the determinationof cardiac output. Cardiac output was measured by the
1722

1723CIRCULATORYEFFECTS OF CHRONICHYPERVOLEMIA
TABLE I
Clinical and laboratory summary of normovolemic subjects
Arterial oxygenMean %saturation
brachialarterial Arterial 100 %
Patient Age Sex Weight pressure hematocrit Air Oxygen
yrs kg mmHg %Ia Normal hematocrit
A.R. 42 M 59.5 82 0.43 95.2D.B. 49 M 86.4 103 0.48 95.8W.S. 50 M 82.6 103 0.41C.H. 71 F 69.0 99 0.49 97.3Z.B. 52 F 64.8 100 0.44 96.5O.W. 42 F 66.6 104 0.40 95.3
lb Elevated hematocritG.A. 47 M 86.5 82 0.53 98.9 100-D.G. 73 F 55.7 116 0.53 96.0 100+C.D. 44 M 70.5 94 0.53 94.2 99.2F.B. 65 M 57.5 90 0.55
direct Fick principle in one patient (S.Tu.) and with in- Indicator dilution curves were constructed on semi-dicator dilution curves in the others. Mixed venous logarithmic paper from the plasma concentration ofblood was sampled from the pulmonary artery and ar- T-1824. Cardiac output and mean transit time were cal-terial blood from the brachial artery. Oxygen consump- culated by mathematically extrapolating the downslopetion was measured with a 9 L Collins respirometer while of the dye curve to zero concentration as described bythe subjects were breathing 100 per cent oxygen. Oxy- Lilienfield and Kovach (7). Stroke volume was obtainedgen content of blood was determined by the Van Slyke- by dividing cardiac output by heart rate. Arterial he-Neill method. matocrits were read in Wintrobe tubes after centrifu-
Indicator dilution curves were obtained while the sub- gation at 2,260 G for 30 minutes. Red cell volume wasjects were breathing 100 per cent oxygen from the Col- measured by the dilution of Cr51-labeled red cells as de-lins respirometer. Thirteen to 19 mg of Evans blue dye scribed previously (8). In calculating plasma volumewas rapidly injected from a calibrated syringe into the from the Cr51 cell determinations, the total body hemato-main pulmonary artery in 3 patients (D.G., G.S. and A.L.) crit was assumed to be 0.92 times the large vessel hemato-and into an antecubital vein, with prompt elevation of crit (8, 9). Direct measurement from T-1824 concen-the subject's arm, in the remaining 17. Using a rotating trations after 10 minutes of equilibration gave similarmultiple-sampling device which was adjusted to collect plasma volume measurements. The blood volume datasamples at 2-second intervals, brachial arterial blood was recorded in Table III are those derived from the Cr`collected through a no. 17-T Cournand needle and a short method.polyethylene tube, in tubes containing a few particles of RESULTSpowdered heparin. The arterial blood was centrifuged, . . .sand the optical density of the undiluted plasma was read Data obtained in individual subjects are sum-twice with a Beckman DU spectrophotometer at 620 mg. marized in Table III. Oxygen consumption ap-
TABLE II
Clinical and laboratory summary of subjects with chronic hypervolemia (polycythemia vera)
Arterial oxygenMean %saturation
Duration Previous brachialof treat- Arterial arterial 100%
Patient Age Sex Weight symptoms ment Hct. pressure WBC Platelets Air Oxygen
yrs kg mos % mmHg 103/cu mmS.Ta. 76 F 45.3 1 0 0.65 110 10.9 186 95.0 100+G.S. 65 F 51.4 1 0 0.65 120 16.8 850 93.0 99.5A.L. 61 M 71.8 1 0 0.56 120 15.3 830 94.1 98.7F.Y. 42 M 67.3 1 0 0.60 97 22.9 1,315 94.0 97.4T.S. 68 M 58.0 1 0 0.65 128 18.0 510 93.3 100+H.W. 68 M 63.6 12 P32* 0.59 99 10.3 220 93.7 99.5R.S. 55 M 69.0 12 P32* 0.56 108 13.3 330 97.0 100+S.Tu. 33 F 58.0 156 * 0.57 81 8.4 220 99.5 100+J.F. 33 M 75.9 60 p32* 0.64 100 22.8 258 96.9 99.0B.P. 65 M 66.9 84 P32* 0.56 100 10.8 184 91.6 100+
* One or more phlebotomies.

LEONARDA. COBB, ROBERTJ. KRAMERAND CLEMENTA. FINCH
0> :nG~~~~~~~ CN U) - N -o
00- ei e - v
>~~~~~~~~~~~~~~~~~~~~IAc m C
E~~~~ V ~0 C1 -I 00%NC4 - V' -!t00 "14 00 m cq C4 M 'tjU0 00o0000 .. ) t U0 0'-o%0U) 04-0a v.)
N'aU-v) C'00
- --- ~~~CN14 C'4
4- -I--~~~~~~~~~~~~~4 444)~ 00 kn0 m't 'IC t"-U0%0% 0e4 I- C00\V00 MI)- VU)k00 00
e4 - -4 eq -4v Osoe nenoo4 urci <C4 C4C' o-O-
' 0 a,0 O.N C0 e4)0 00'ON ,f2'-00 1'1'4e00 C
cd4 m a, enON tn - 0 I"0 t- '-4 0 0 C.,CJ0 - C4 00 r--00o2 >d C 0000 -0 00 00 0000 '-a00 t- 0%0%tr- \ - \.-VU)No t-= v
) )
00 e-4 e14 r-00 00 Ur) -
N4 00 V'\
t U) 00 V0
00 - 0% O
O r4- t-No +4Uo6 r :o6 6
C'lC^S4 -4 Co
0%oV, 0, 00 00
--Obe
. .
0.oxr-oNe o_
f s o o
00
to0% -4U
U)ea
\-6 o6u-r
o o o
-U)
sN
,
0Nf)
0 '00 CN U') U) 00- CU) C4. m U)
0N 0N CN \ 0 It 00 0 c4 t-
m in ro0\ C\ o4-t t rC o i00 -tt 000 -I m
u)00 to to Vc 0 00 %oVo Ut t-
\' -Rt -ti V0 1' inU) U) V\
C0%0000%N(N 0ON000%4'-0\00 00 00 4t'-. . . . . . . .6 .4 ; . .:: . . .
C'-VU)0~'-~C'UU) m m0U 000
OOOOOCOOOOOOOOOOO
0 \ O °°U)00 0000 In°e°O ,,
t -1' 1.' 00 0 00 V0\ CV
o C'sCo CZ CO.I CId 0 C C
CZ
0
C0E(A
CZ
CZCZ
0
E.
2)
0
0
I. -
0)
.0
0
CZ.-0.
-Q
¢)4.
0).-
...
D
1724
4)124
0
E
.4
0-
O.v
bo
I.)
qJ
Ir
- s:
_0
0
,4a- o
m 4
04
24
m 0
A4
" 02/2-

CIRCULATORYEFFECTS OF CHRONICHYPERVOLEMIA
peared to be similar between the subjects in GroupsI and II. The average for the former was 148 mlper m2 per minute, and in subjects with polycythe-mia vera, 155 ml per m2 per minute. The meanarterial oxygen saturations were 96, 96 and 95 percent in Groups Ia, lb and II. Oxygen content ofblood differed; Group Ia had an average arterialoxygen content of 17.83; Group Ib, 20.81; GroupII, 22.04 volumes per cent.
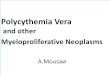
The average cardiac output of 3.65 L per min-uite per m2 in the normovolemic subjects with nor-mal hematocrit (Group Ia) was similar to that of3.50 L per minute per m2 in Group lb with ele-vated hematocrits but normal blood volume. Inthe polycythemia group (II), output was 32 percent higher, i.e., 4.81 L per minute per M2. Whenboth arterial oxygen content and cardiac output areconsidered, the total oxygen available to the tissuesper unit of time was greater by 19 per cent inGroup lb and by 70 per cent in Group II, com-lared with Group Ia.
Blood volume measurements indicated an aver-age red cell mass of 24 nil per kg in Group Ia, 34mil per kg in Group Ib, and 53 ml per kg inGroup II. Plasma volumes were 36, 34 and 42;total blood volumes were 60. 68 and 95 il per kg.The body hematocrit correction factor 1 was 0.87,0.92, and 0.91 in Groups Ia, Ill, and IT. Thesesimilar values would seem to exclude any signifi-cant blood vessel distributional difference amongthe three groups. Five of the 10 hypervolemicpatients with polycythemia vera had high cardiacoutputs (Figure 1). Comparing those with highand normal output, the former had an averageblood volume of 102 ml per kg versus 89 ml perkg in the latter. There was no apparent differ-ence between the five subjects with normal outputand the five with high output when evaluated fromthe standpoint of duration of illness, splenomegaly.hematocrit level, oxygen consumption or age.Pulse rate was greater in the subjects with a highoutput (95 versus 69 beats per minute). Therewas a high degree of correlation (R = + 0.94) be-tween blood volume and resting stroke volume inall subjects studied. The output per beat per M2
Where mean body hematocrit correction factorred cell volume (Cr11) x
red cell volume (Cr51) + plasma volume T-1824i
arterial hematocrit'
FIG. 1. RESTING CARDIAC OUTPUTEXPRESSEDAS CARDIACINDEX IN CONTROLSAND POLYCYTHEMICSUBJECTS.
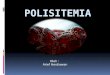
exceeded normal values in all of the polycythemiapatients, and the correlation coefficient betweenblood volume and stroke volume corrected for bodysurface area was + 0.91 (Figure 2). Similarly.cardiac index correlated well with blood volumeper M2 (R = + 0.76). The mean transit time(antecuibital vein to brachial artery) of 21.1 sec-onds in the hypervolemic patients was slightlygreater than the average value of 17.6 seconds inthe normovolenmic subjects.
These results suggested a relationship betweenthe increased blood volume and elevated strokeoutput. In order to evaluate this relationshipand the significance of the other measurements,seven patients with polycythemia vera were re-studied following phlebotomy. Between 500
70
4 60
j 50
('5
40
*- Polycythemia Vera* - Normovolemic
00 o
0 0rz 0.91
1 2 3 4Total Blood Volume (L /M2)
5
FIG. 2. THE RELATIONSHIP BETWEENTOTAL BLOODVOL-UMEAND RESTING STROKE INDEX IN NORMOVOLEMICANDPOLYCYTITEMIC SUBJECTS.
1725
.
.

LEONARDA. COBB. ROBERTJ. KRAMERAND CLEMENTA. FINCH
2000 3100 1500 1000 2400 1500 500 removed
50
10JrmOvolemir
subjectsK - -_;91 m.
-~~~~~~~~25~~~~~~~~~~~~ControlAfterPhle-botomny
L.LFY.T._S. TO
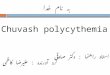
FIG. 3. THE EFFECT OF BLOODREMOVALON STROKE INDEXIN POLYCYTHEMIAVERA.
and 3,100 ml of blood was removed from the pa-tients over time intervals of up to 62 days. Inthe six subjects studied two to, eight weeks post-phlebotomy (excluding the one instance whenmeasurements were made immediately after bleed-ing), the average hematocrit was reduced from0.62 to 0.45. Blood volume fell from 100.2 to86.3 ml per kg. Cardiac index was reduced from4.8 to 4.1 L per minute per in2, and stroke indexfell correspondingly from 61 to 53 ml per beat perII2. The decreases, while not of great magnitude,were significant in that they occurred in each pa-tient subjected to phlebotomy (Figure 3).
In the instances of intracardiac pressures meas-ured in polycythemia vera (S.Ta., G.S. and A.L.),mean right atrial pressures were 1, 3 and 3; meanpulmonary artery, 12, 13 and 25; and pulmonary"capillary," 9, 9 and 11 mmHg.
In the patients with polycythemia there was asignificant correlation of total blood volume andoxygen consumption per M2; the coefficient of cor-relation between these parameters prior to phle-botomy was 0.89 (p < 0.001). Oxygen consump-tion in the normovolemic subjects, however,showed no such relationship, although there wasconsiderable overlap in oxygen consumption be-tween the two groups. Red cell mass in the poly-cythemic subjects was similarly related to oxygenuptake.
DISCUSSION
Previous estimates of cardiac output in poly-cythemia vera have been limited and have beenperformed by the indirect Fick principle. Alt-schule, Volk and Henstell, employing the ethyliodide method of measurement, reported normaloutput in three patients (10). Brooks also re-
ported a normal cardiac index in one patient ( 1 1 ).Several others have agreed that retardation ofperipheral blood flow is a prominent feature ofpolycythemia vera (12). Goldsmith, estimatingoutput by the acetylene method, reported increasedoutput in one of four patients studied (13). Thesereports are so limited in number as well as inmethods that conclusions can not be drawn.
The present studies show a normal or elevatedcardiac output and a consistently increased strokevolume in polycythemia vera. This is oppositeto the experimental results obtained by Richard-son and Guyton (1) in acutely induced normo-volemic polycythemia.
The explanation for the elevated stroke indexwould appear to relate to the altered blood volumein polycythemia vera. That hypervolemia exertsits effect through increased central blood volumeand enhanced diastolic filling seems logical (14).It is possible that the increased cardiac output ob-served in five of the ten subjects was in part de-pendent upon increased venous return, similar tothe transient effects described with acute hyper-volemia in dogs (15). From other studies thereis evidence that acute hypervolemia achieved by theinfusion of dextran and other blood volume ex-panders increases output (2, 4, 6, 16). Thesetechniques also produce a decrease in hematocritas a complicating feature. The present study in-dicates that high output occurs with hypervolemiaeven in the presence of an elevated hematocrit.These observations in the chronic hypervolemiaof polycythemia vera may be compared with thestudies of Kjellberg, Rudhe and Sjdstrand inwhich an augmentation of blood volume and workcapacity per heart beat were observed in trainedathletes (17). The possible relationship betweenincreased output observed with high altitude poly-cythemia (18) and altered blood volume wouldseem to merit study.
Although blood volume correlated with bothstroke volume and cardiac output in this study,the question should be raised whether hypervole-mia was a causal factor or whether this correlationwas incidental. The fall in cardiac output andstroke volume after blood volume was reduced byphlebotomy suggests that the hyperkinemia doesindeed causally relate to chronic hypervolemia orsome feature thereof. Recent observations onnormal subjects show that acute bleeding results
1726

CIRCULATORYEFFECTS OF CHRONICHYPERVOLEMIA
in a decreased stroke volume which is correlatedwith the reduction in "central blood volume" (19).It was of some interest also that the effect of theincreased cardiac output was to maintain a normalplasma flow in the patients (Figure 4). Althoughbody tissues may have plasma flow requirementsthat influence cardiac regulation, such considera-tions at present remain conjectural.
Under the conditions of this study there is anotable lack of correlation between oxygen re-quirement, as reflected by oxygen consumption,and oxygen supply, as measured by hemoglobinconcentration and cardiac output. In looking fur-ther into possible correlations, it is equally ap-parent that poor correlation exists between oxygenconsumption, which presents similar average val-ues in the three groups of subjects, and the bloodvolume, which is considerably elevated in the poly-cythemia vera group. There is, however, an im-pressive correlation between blood volume andoxygen consumption among the individuals ofthe polycythemia vera group (R = + 0.89). Onemight suggest that increased blood volume per secould affect cardiac work and perhaps metabolicactivity of other tissues. There was some corre-lation between oxygen consumption and cardiacwork (R = + 0.69) and stroke volume (R = +0.78), but not with heart rate or arterial bloodpressure. However, post-phlebotomy studies ap-pear to negate this reasoning, since a reduction inblood volume was associated with no change, orperhaps with a slight increase in oxygen consump-tion. A second explanation would seem to be the
Normovolemia PolycythemiaVera
a I
FIG. 4. PLASMAFLOW IN NORMOVOLEMICAND POLY-
CYTHEMICSUBJECTS.
possible contribution of enhanced hematopoieticactivity to the general body metabolic rate. Thusthe increased red cell mass or blood volume andthe enhanced metabolic activity would both bemanifestations of the marrow disturbance. Theexplanation for this association awaits furtherstudies, but two additional features might be men-tioned: 1) that while Bliss (20) reported a tend-ency for increased metabolic rate in polycythemiavera, our average oxygen consumption is not abovethat of the two other groups studied; and 2)while there is a correlation between oxygen con-sumption and total blood volume or red bloodcell mass, there is no correlation between oxygenconsumption and hematocrit levels in the poly-cythemia vera patients.
SUMMARYANDCONCLUSIONS
Resting hemodynamic studies were performedin 10 patients with expanded blood volumes due topolycythemia vera. In comparison with compara-ble groups of normovolemic subjects, the patientswith polycythemia showed a consistently elevatedstroke index (39 per cent) as well as a significantbut less uniform increase in cardiac index (34 percent) .
The augmentation of stroke volume described inthese patients was closely related to the increasein total blood volume. There was excellent cor-relation between resting stroke index and totalblood volume per m2 in the 20 patients studied(R = + 0.91).
Phlebotomies, performed in seven patients, werefollowed by a reduction in stroke volume andcardiac output in all instances.
The rate of plasma flow was found to be normalin polycythemia vera.
In patients with polycythemia there was a sig-nificant correlation between oxygen consumptionand total blood volume.
ACKNOWLEDGMENTS
The authors are grateful to Doctors Daniel H. Cole-man, Quin B. DeMarsh, Harold E. Laws and AlexanderR. Stevens, Jr., for affording us the opportunity to studytheir patients.
REFERENCES
1. Richardson, T. Q., and Guyton, A. C. Effects ofpolycythemia and anemia on cardiac output andother circulatory factors. Amer. J. Physiol. 1959,197, 1167.
1727
Zt 3-R:
e0
1
it 0
-11. 2-4.C3 - Ic-
I-Sjk

LEONARDA. COBB, ROBERTJ. KRAMERAND CLEMENTA. FINCH
2. Withanm, A. C., Fleming, J. W., and Bloom, W. L.The effect of the intravenous administration ofdextran on cardiac output and other circulatorydynamics. J. clin. Invest. 1951, 30, 897.
3. Ferguson, T. B., Shadle, 0. W., and Gregg, D. E.Effect of blood and saline infusion on ventricularand diastolic pressure, stroke work, stroke volumeand cardiac output in the open and closed chestdog. Circulat. Res. 1953, 1, 62.
4. Gowdey, C. WV., Hatcher, J. D., and Sunahara, F. A.Cardiovascular responses in dogs to large intra-venous infusions. Canad. J. Biochem. 1954, 32,282.
5. Holt, J. P. Effect of plethora and hemorrhage on
left ventricular volume and pressure. Circulat.Res. 1957, 5, 273.
6. Schnabel, T. G., Jr., Eliasch, H., Thomasson, B.,and Werk6, L. The effect of experimentally in-duced hypervolemia on cardiac function in normalsubjects and patients with mitral stenosis. J. clin.Invest. 1959, 38, 117.
7. Lilienfield, L. S., and Kovach, R. D. Simplifiedmethod for calculating flow, mean circulation timeand downslope from indicator-dilution curves.
Proc. Soc. exp. Biol. (N. Y.) 1956, 91, 595.8. Donohue, D. M., Motulsky, A. G., Giblett, E. R.,
Pirzio-Biroli, G., Viranuvatti, V., and Finch, C. A.The use of chromium as a red-cell tag. Brit. J.
Haemat. 1955, 1, 249.9. Chaplin, H., Jr., Mollison, P. L., and Vetter, H.
The body/venous hematocrit ratio: Its constancyover a wide hematocrit range. J. clin. Invest. 1953,32, 1309.
10. Altschule, M. D., Volk, M. C., and Henstell, H.Cardiac and respiratory function at rest in patients
with uncomplicated polycythemia vera. Amer. J.mcd. Sci. 1940, 200, 478.
11. Brooks, WV. D. Circulatory adjustments in poly-cythemia rubra vera. Proc. roy. Soc. Med. 1936,29, 1379.
12. Lawrence, J. H. Polycythemia. New York, Gruneand Stratton, 1955, p. 8.
13. Goldsmith, G. Cardiac output in polycythaemia vera.
Arch. intern. Med. 1936, 58, 1041.14. Sjdstrand, T. Volume and distribution of blood and
their significance in regulating the circulation.Physiol. Rev. 1953, 33, 202.
15. Guyton, A. C., Lindsey, A. XV., Kaufmann, B. N.,and Abernathy, J. B. Effect of blood transfusionand hemorrhage on cardiac output and on the ve-
nous return curve. Amer. J. Physiol. 1958, 194,263.
16. Fowler, N. O., Franch, R. H., and Bloom, WV. L.Hemodynamic effects of anemia with and withoutplasma volume expansion. Circulat. Res. 1956, 4,319.
17. Kjellberg, S. R., Rudhe, U., and Sjbstrand, T. In-crease of the amount of hemoglobin and blood vol-ume in connection with physical training. Actaphysiol. scand. 1949, 19, 146.
18. Theilen, E. O., Gregg, D. E., and Rotta, A. Ex-ercise and cardiac work response at high altitude.Circulation 1955, 12, 383.
19. Ralston, L. A., Cobb, L. A., and Bruce, R. A. Therole of blood volume in regulation of cardiac out-put, the effects of arterial bleeding in normal sub-jects. Clin. Res. 1960, 8, 124.
20. Bliss, T. L. Basal metabolism in polycythemia vera.
Ann. intern. Med. 1929, 2, 1155.
1728