Embed Size (px)
Citation preview
Develop. Mecl. Child Neitrol. 1961, 9, 430-447
Idiopathic Hypoglycaemia and Children of Low Birth-Weight
Murguret Cox Henry G. Dunn
of hypoglycaemia in childhood still present many aetiological problems. At times, ii clear-cut primary hepatic, endocrine or metabolic disorder is found to be responsible, or the child is severely malnourished, or a chemical agent like insulin or a sulphonylurea may have been administered, but in about two-thirds of all cases the basic causation is obscure (Mc- Quarrie 1954, Ulstrom 1964). The hypo- glycaemia is then referred to as ‘idiopathic’. This condition is reported to be commoner in males and is sometimes familial (McQuarrie 1954, Haworth and Coodin 1960). Inareview ofthe literature, Haworth and Coodin (1960) found that 90 per cent of the reported instances of idiopathic hypoglycaemia in children under 15 years of age hiid their onset at under 2 years, and 60 per cent had become evident before the age of 6 months. Among the latter group, about half the affected children sub- sequently had neurological disabilities, part ic LI I ;ir I y W h i le thcse disabilities ;ire usually attributable to brain damage caused by the hypoglycacniia, it has been rccognised that, conversely, cerebral defects o r injuries may sometimes be the primary C;ILISC of hypoglycnenia (Dorrow 1930, Hal-tmann and Jaudon
mental re t ardn t i o n ,
1937, Conn and Seltzer 1955, Cornblath et a/. 1959, Haworth and Coodin 1960, Etheridge and Millichap 1964).
At present it seems that idiopathic hypo- glycaemia is not a single clinical entity and may have a variable pathogenesis. First, an rxcc.ssive secretion of insulin may be responsible. Adenomata of the islets of Langerhans are quite rare in small children, but hyperplasia of the islets was found in 9 out of 29 patients who had a laparotomy (Haworth and Coodin 1960). Excessive insulin release may also occur without demonstrable anatomical abnormality. The causes of such hyperinsulinism are prob- ably multiple. In some cases excessive sensitivity to leucine has been demon- strated (Cochrane et al. 1956), and in the majority of these the administration of L-leucine leads to ii marked rise in the level of plasma insulin (Grumbach and Kaplan 1960, Mnbry (’1 u/. 1960). I t now seems that this is probably a marked exaggeration of a normal physiological phenomenon (Faijans (it a/. 1962, Floyd et a/. 1963). However, thcse patients are also liable t o have severe hypoglycnemia in the fasting state and may secrete insulin a t an abnormally low threshold of blood glucose (Roscnthal (’ I r r / . 1964). Other children

MARGARET COX HENRY G. DUNN
develop hypoglycaemia in association with keto.sis. It has long been k n o w n t h a t starvation and infection may precipitate hypoglycaemia, usually preceded by ketosis. Colle and Ulstrom (1964) have demon- strated that a low-calorie ketogenic diet will induce symptoms and hypoglycaemia within 12-24 hours in this group of patients, who are not sensitive to leucine. How ketosis leads to hypoglycaemia in these children is not clear, but animal experiments suggest that its action is indirect by stimulation of pancreatic beta cells and consequent release of insulin (Madison et al. 1964). I n yet other patients, hyperinsiilinism causing hypoglycaemia may be the precursor of clinical diabetes mellitus (Bessman 1960, Lloyd 1964). Secondly, there may be reduucedsrcretioii q/’ substances niuintaining tlw blood sugur level. In some cases of idiopathic hypo- glycaemia there appears to be an inability to secrete adrenaline i n response to it low blood-sugar level (Kinsbourne and Woolf 1959, Broberger et al. 1959). Broberger and Zetterstrom (1961) postulated this mechanism in seven affected infants who had a low excretion rate of urinary catecholamines after the injection of insulin, and Bruiljes et al. (1963) also found this phenomenon in seven out of eight affected children. Both groups of authors noted the absence of ‘epinephrine symp- toms’, such as sweating and palpitations, in their patients. In some cases there may well be reduced secretion of other substances keeping up the blood-sugar level-e.g., glucagon (McQuarrie 1954, Grollman et al. 1964) or corticotrophin (Woeber and Arky 1965); this may explain the marked hyper- sensitivity to insulin sometimes found in such patients (Van Creveld et al. 1965). Finally, other nwchunisms, such as abnor- malities of intermediary carbohydrate metabolism, may sometimes be responsible, as has been postulated for the hypo-
glycaemia caused by alcohol (Freinkel et ul. 1965).
Idiopathic hypoglycttemiu in the new- born presents even more problems. In the differential diagnosis we have to consider not only primary diseases of the infant but also metabolic and endocrine disturbances caused by disease of the mother, and particularly maternal diabetes mellitus, which may be overt, subclinical or even in the pre-diabetic phase. Again, the idio- pathic form is almost certainly not a single entity (Haworth and Coodin 1960), and in its causation the interplay of hormonal agents is complicated by their different rates of ‘maturation’, the availability of fetal carbohydrate stores (particularly glycogen), and the variable demands made on them in extrauterine life according to the expenditure of energy in respiration (t>.g., in respiratory distress), maintenance of body temperature (e.g., in chilling) and muscular activity. The amount and com- position of food, and the presence of ketosis or infection may also play a role, as they do in older children.
I t has been known for many years that the blood-sugar level in newborn infants is normally lower than in later months, and it is now considered that levels of blood glucose should only be considered ab- normal below 30 mg. per 100 ml. in full- term infants and below 20 mg. per 100 ml. in prematures (Hartmann and Jaudon 1936, Cornblath and Reisner 1965). After the first 72 hours of life blood-glucose levels below 40-50 mg. per 100 ml. may be considered hypoglycaemic in full-size in- fants (Cornblath and Reisner 1965). Even at these low levels neonates may not have any symptoms, and in past years the clinical significance of neonatal hypo- glycaemia was doubtful. Since 1959 these doubts have been dispelled (Cornblath er al. 1959, Haworth et al. 1963, Brown and Wallis 1963, Neligan et ul. 1963). The
43 1

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1967, 9
commonest symptoms of neonatal hypo- glycaemia are episodes of apnoea with cyanosis (Brown and Wallis 1963). Other findings include tremors (‘jitters’), irrit- ability, limpness, lethargy, a weak or high- pitched cry, feeding difficulties, disappear- ance of sucking and postural responses (Haworth et al. 1963), rolling of the eyes, and hypothermia (Brown and Wallis 1963). Convulsions are a serious and late manifestation. Head retraction has also been described (Tynan and Haas 1963). The fact that these symptoms and signs are due to hypoglycaemia can often be demon- strated by their prompt disappearance after intravenous injection of glucose. They may start at any time from 2 t hours to 7 days after birth but most commonly on the 2nd or 3rd days (Cornblath et al. 1964).
Recent reports have indicated the follow- ing further features of idiopathic hypo- glycaemia in the newborn :
1. As in older infants and children it occurs more commonly in males; the pro- portion of males to females in the total reported cases is about 3:1 (Cornblath er al. 1964) but has varied considerably in different series.
2. It occurs much more commonly in infants of low birth-weight than in those of normal weight, and most of the affected infants are ‘dysmature’*-Le., of low weight for their length of gestation-rather than strictly premature-i.e., of low weight in accordance with short gestation (Corn- blath et al. 1959, Baens et al. 1963, Brown and Wallis 1963, Neligan 1963). Accord- ingly, maternal toxaemia is often associated and had occurred in about half of the total reported cases (Cornblath et al. 1964). ‘Placental insufficiency’ was noted in 12
* We agree with Gruenwald (1963) that the term ‘dysmature’ is not ideal, since it is the infant’s nutrition rather than the maturity which is defec- tive, but semantically ‘dysmaturity’ stands in simple contrast to prematurity and is easier to use than ‘fetal malnutrition.’
out of 13 cases in one series (Tynan and Haas 1963).
3. Malnourished (dysmature) infants of low birth-weight generally tend to have a lower blood-sugar level than well-nourished infants of the same gestational age (Neligan ef al. 1963).
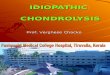
4. When a dysmatui-e twin is over 25 per cent lighter than the other, he runs a particularly high risk of hypoglycaemia (Reisner et al. 1965).
5. Injury or congenital defect of the CNS may be a primary cause of hypo- glycaemia in the newborn, as at later ages; this was thought to be a factor in 5 out of 24 cases reported by Cornblath et al. (1964).
6. The proportion of children who exhibit brain damage after neonatal hypo- glycaemia has varied considerably in reported series. On the whole, such damage has been demonstrated in about half of the survivors who had had symptoms in the newborn period (Brown and Wallis 1963, Cornblath ef al. 1964, Haworth and McRae 1965), whereas the outlook was much better when the neonatal hypo- glycaemia had been asymptomatic (Haworth and McRae 1965). Obviously the incidence of such sequelae will depend on the duration of follow-up and the care taken in testing.
7. Most authors have found little tend- ency for the hypoglycaemia to recur after the first 2 months (Haworth et al. 1963, Cornblath et al. 1964), but isolated instances of later recurrence have been reported (Neligan et al. 1963, Cornblath et al. 1964, Haworth and McRae 1965). Conversely, Broberger and Zetterstrom (1961) noted that 6 out of 7 cases of spontaneous recurrent hypoglycaemia in later childhood had rated very low on the weight-maturity scale at birth, and Neligan (Neligan et al. 1963, Neligan 1964) has warned that such poor fetal nutrition may be an important warning sign of possible
432

MARGARET COX HENRY G. DUNN
long-term endocrine abnormality, a t least in regard to the regulation of carbohydrate metabolism.
We have been involved in a long-term prospective follow-up study of infants with low birth-weight since September 1958. Most of these babies were private patients and were observed but not treated by our study group, and blood-sugar levels were not determined routinely. Nevertheless it seemed of interest to review our experience with the diagnosis of idiopathic hypo- glycaemia and with the follow-up of the affected children. I n addition, we decided to collect information on all the children admitted to the Vancouver General Hospital with idiopathic hypoglycaemia after the neonatal period in 1958-1964 and to study their birth and subsequent course retrospectively.
Material and Methods In the Premature Nursery of the Van-
couver General Hospital, 500 infants with a birth-weight of 44 Ib. (2,040 g.) or less have been examined. The intake of new babies into the survey ceased in May 1965. 418 have survived the neonatal period, and 82 died, 20 of them in the fii’st 48 hours of life. Follow-up has been main- tained on 342 survivors. They have been re-examined in their homes by ;I Research Fellow at 3, 6, 12 and 18 months, and the older ones have been visited further by a Research Fellow and ;I psychologist at 21, and 4 years and-so far only in 50 cases--- at 6) years. Children suspected of any neurological or opht1i;ilmological defect have been referred for neuropiiediatric consultation (to H.G.D.). Examinations for eye defects have been carried o u t by 3 staff ophthalmologists in the newborn nursery and again at 4 years; speci;tl tests for hearing have been performed a t I and 4 years and for language development at 4 years. Electroencephnlography was carried out on most of the infants before their
discharge from the nursery and again a t about 1 year, and in some cases a t 64 years.
When hypoglycaemia has been sus- pected by the attending physicians o r residents, blood-sugar estimations have been carried out by a micro technique modelled on Harding’s modification of the Nelson-Somogyi method for ‘true’ blood sugar (see Wootton 1964). Blood samples were obtained by heel puncture, using 50 pl. per test in duplicate. These samples were mixed with isotonic sodium sulphate- copper sulphate solution a t the cribside, thus preventing glycolysis, and the pro- cedure was then completed in the labora- tory by the standard technique.
For comparative analysis we perused the hospital charts of patients admitted with idiopathic hypoglycaemia to the Health Centre for Children, Vancouvei- General Hospital, in 1958-1964. In this gl-oup, a ‘true’ blood-sugar level of under 50 mg. per 100 ml. was considered essential for the diagnosis. When the patients were not in the follow-up study, an inquiry con- cerning their subsequent course was directed to the attendant physician.
Results A . Idiopathic h j pg lvcuet i I iu it1 prospective survt>j. of’infants uiith Ion, hirth-uvighr
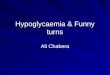
Nine infarits with a birth-weight of 4 t Ib. (2,010 8.) or less in our follow-up study were diagnosed by their medical attendants as having neonatal hypoglycaemia. They are listed in Table I . Of these 9 infants, 5 were males. Six were singletons and three were twins. Four were dysmature--i.e., below the 10th percentile in weight for their gestntional age (Lubchenco P / a/. 1963, Naeye ct NI. 1966), and one binovular twin (J.P.) was borderline i n this respect, since his birth-weight was only just above the 10th percentile ( s w Figs. I and 2), while the birth-weight of the others was more in keeping with the duration of pregnancy. Maternal toxaemia was known
433

TA
BL
E I
EL
~~
LK
Nin
e L
ow
Bir
th-w
eigh
t B
abi
--
-~
.~
._
_ ~
,
F 3
.3
31
No
-
(la6’
I ~
-.
-
-,
F
3.3
40
Y
es
Mul
tipl
e (1
446)
pl
acen
tal
mic
ro-
infa
rcts
with
in
terv
illou
s fi
brin
dep
ositi
on
__--.--.-.
with
Neo
nata
l Id
iopa
thic
Hyp
ogly
caer
nia
No
Yes
Fam
ily h
isto
ry
of e
pile
psy
Uni
vovu
lar t
win
(o
ther
wei
ghed
3
:b.
10 oz.
(1.6
44 9
.)
3.4
( 1
474)
--
34
Srm
pto
ms
and
signs
EE
G
Lat
esf
veur
olox
icc
sfat
us
Bir
th-
wei
gh
f W
eek 01
Ib. o
z.
gest
alio
n D
JJS
- m
afu
re
Cor
nrne
nf
Pof
ieni
F
ollo
w-u
p
In n
urs
rry
Lat
er
Slow
and
mon
o-
rhyt
hmic
at
11 m
os.
Nor
mal
T
wit
chin
g 4
yr.-s
mal
l st
atur
e an
d hy
poto
nia.
B
inet
IQ
86
~_
__
.
Nor
mal
-
15
4 20
’
5 3
yr.-r
epor
ted
wel
l (ou
t oft
own)
G
riff
iths
DQ
102
at
1 y
r.
Apn
oea,
cya
nosi
s,
irri
tabi
lity,
h y
pert
onic
ity.
exce
ssiv
e cr
ying
Slee
p SD
indl
es
mos
t pr
omin
ent
post
erio
rly
at
1 yr
.
Nor
mal
09
I2
12
I2
14
MJ
1 M
2.14
38
Y
es
Mat
erna
l (I
304)
al
coho
lism
7
4 0
4
Lou
d cr
ies,
tr
emor
s.
conv
ulsi
on
Min
or
asym
met
ry in
am
plit
ude
Asy
mm
etry
of
ampl
itud
e an
d fr
eque
ncy
at
8 m
as.
3 yr
.-mul
tiple
co
ngen
ital
an
omal
ies.
M
enta
l re
tard
a-
tion
and
sig
nifi
- ca
ntly
sm
all
head
, pre
sum
- ab
ly d
ue to
con-
ge
nita
l cer
ebra
l de
fect
. G
riff
iths
DQ 4
5 at
2) y
r.
Abn
orm
a
-. -
20
I-, ~.~
-._
___
M
3.4
33
Bor
der-
B
inov
ular
twin
(1
474)
lin
e (o
ther
sti
llbo
rn).
M
ater
nal
tnxa
emia
JP
DW
~
DT
h
.~
LD
Nor
mal
3
yr.-n
o gr
oss
neur
olog
ical
ab
norm
alit
y (t
houg
h hy
per-
re
flex
ic a
nd
trem
ulou
s to
I)
yr.)
Bin
et 1
0 86
Que
stio
n-
able
0 I
-
4 5 2 2
Nor
mal
at
11 m
os.
Tre
mor
s, h
igh-
pi
tche
d cr
y I5
-
17
I5
-
0 19
~. N
o 1s
t tw
in (
othe
r of
sam
e w
eigh
t di
ed on
2nd
day:
~
Low
-am
plit
ude
min
or v
olta
ge
asym
met
ry
~ 24 y
r.-sp
astic
qu
adri
pleg
ia.
men
tal r
etar
da-
tion
and
hea
ring
de
fect
. G
riff
iths
DQ 4
1
Slow
for
age
at
10 m
os.
Apn
oea
cyan
osis
tw
itchi
&
arch
in;
Abn
orm
a
M
3.13
37
(I
729
) Y
es
Mat
erna
l to
xaem
ia
Mul
tifk
al sh
arp
wav
es, s
pike
s an(
as
ymm
etri
cal
slow
wav
es a
t 2
wk.
~
Nor
mal
at 9
an
d 20
rno
s.
~ 2) y
r.-no
gr
oss
neur
olog
ical
ab
norm
alit
y.
Gri
ffith
s D
Q 9
8 at
I&
yr.
~
Nor
mal
A
pnoe
a, c
yano
sis,
tw
itchi
ng a
nd
conv
ulsi
ons
- ,~
.L
II
M
3.13
31
(I
729
) 19
0
Tre
mor
s T
wo
bord
erli
ne
reco
rds
with
ra
re s
harp
wav
es
and
spik
es f
rom
ri
ght h
emis
pher
e
Nor
mal
at
12 m
os.
1 ) y
r.-no
gr
oss
neur
olog
ical
ab
norm
alit
y.
Gri
ffith
s DO 9
0
Que
stio
n-
able
KIM
-.
__
I4
0
twin
’s
33)
1 T
rem
ors,
ex
cess
ive
cryi
ng,
sett
ing sun
sign
Nor
mal
at
1 w
k.
Nor
mal
at
13
mos
apa
rt f
rom
on
e (7
) ab
orti
ve
spik
e-w
ave
disc
harg
e w
hen
drow
sy
1 yr
.-no
gros
s ne
urol
ogic
al
abno
rmal
ity.
G
riff
iths DQ 1
01
Nor
mal
9 3
--
Apn
oea,
cya
nosi
s,
trem
ors
and
hype
rton
us
Low
-am
plit
ude
at 8
wk.
N
orm
al a
t 9
mos
. 1
yr.-s
past
ic
dipl
egia
. G
riff
iths DO 82
at 6 m
os.
Abn
orm
al
-

MARGARET COX HENRY G. DUNN
BIRTH WEIGHT OF SINGLETON CHILDREN WITH IDIOPATHIC HYPOGLYCAEMIA
( S H O W N ON L U B C H E N C O FOETAL G R O W T H CURVE)
* 4000 -
- 3600 -
- 3200 -
- 2800 -
- 2400 -
- 2033 -
- 1600 -
- 1200 -
- 800 -
-
M A L E S
FEMALES
* PERCENTILES
............. CURVE FOR
.....
90
75
50
25
10
400 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1
24 26 28 30 32 34 36 38 40 42 WEEKS OF G E S T A T I O N
0 0 Survey i n f a n t s wi th l o w b i r t h w e i g h t a n d n e o n a t a l
h y p o g l y c a e m i a ( T a b l e I ) . S u r v e y c h i l d r e n wi th l o w b i r t h w e i g h t a d m i t t e d l a t e r
wi th h y p o g l y c a e m i a ( T a b l e 1 1 )
0 0 N o n - s u r v e y c h i l d r e n a d m i t t e d w i t h h y p a g l y c a e m i a
( T a b l e I l l )
on fetal growth curve designed by Lubchenco et ul. (1963). Fig. 1. Birth-weight of singleton children with idiopathic hypoglycaemia shown
to have been present in 2 cases and placental infarction of unknown cause in another. At ages varying from 1 to 4 years, 3 of these 9 children are already known to have neurological abnormalities, and 3 are of questionabIe neurological status. One abnormal boy (M.J.) has multiple con- genital defects, and his brain may well be malformed. Of the other two abnormal
children, one has spastic quadriplegia with deafness and the other spastic diplegia. Of the children with questionable abnormality, B.L. and J.P. have minor abnormal signs and low-normal IQ, while L.D. has a suspicious EEG and a family history of epilepsy. Admittedly the distinction be- tween normal and questionable neuro- logical status is somewhat arbitrary. I t is,
43 5
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1967, 9
BIRTH WEIGHT OF TWINS WITH IDIOPATHIC HYPOGLYCAEMIA [SHOWN O N NAEYE FOETAL GROWTH CURVE)
DlCHORlONlC TWINS MONOCHORIONIC TWINS
3600 3 2 0 0 5
2800
2400
9nnn / percentiles
90% * 75% 50% 25%
10%
1 1 1 1 1 1 I I 24 26 28 30 32 34 36 38 40 32 34 36 38 40
WEEK OF GESTATION WEEK OF GESTATION
0 0 Survey infants with low birth weight and neonata l hypoglycaemia (Table I1
0 ' Survey children with low birth weight admitted later with hypoglycaemia [Table 111
0 Non-survey child admitted w i t h hypoglycoernio {Toble I l l )
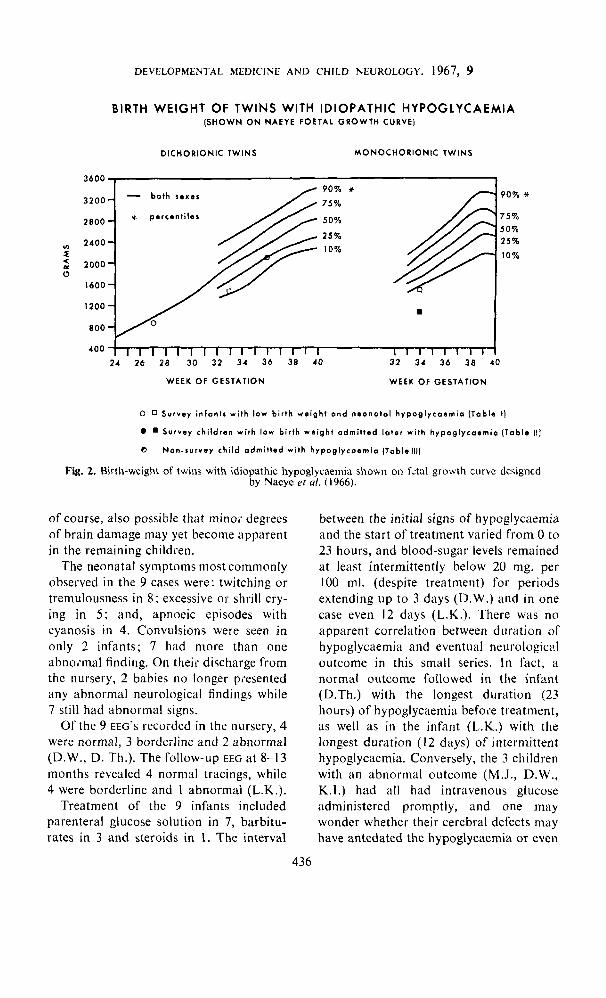
Fig. 2. Birth-weight of twins with idiopathic hypoglycaemia shown on fetal growth cwvc dcsigned by Naeye et ul. (1966).
of course, also possible that minor degrees of brain damage may yet become apparent in the remaining children.
The neonatal symptoms most commonly observed in the 9 cases were: twitching or tremulousness in 8; excessive or shrill cry- ing in 5; and, apnoeic episodes with cyanosis in 4. Convulsions were seen in only 2 infants; 7 had more than one abnoimal finding. On their discharge from the nursery, 2 babies no longer piesented any abnormal neurological findings while 7 still had abnormal signs.
Of the 9 EEG'S recoided in the nursery, 4 were normal, 3 borderline and 2 abnormal (D.W., D. Th.). The follow-up EEG a t 8-13 months revealed 4 normal tracings, while 4 were borderline and 1 abnormal (L.K.).
Treatment of the 9 infants included parenteral glucose solution in 7, barbitu- rates in 3 and steroids in 1. The interval
between the initial signs of hypoglycaemia and the start of treatment varied from 0 to 23 hours, and blood-sugar levels remained at least intermittently below 20 mg. per 100 ml. (despite treatment) for periods extending up to 3 days (D.W.) and in one case even 12 days (L.K.). There was no apparent correlation between duration of hypoglycaemia and eventual neurologicd outcome in this small series. In fact, a normal outcome followed in the infant (D.Th.) with the longest duration (23 hours) of hypoglycaernia before treatment, as well as in the infant (L.K.) with the longest duration (12 days) of intermittent hypoglycaemia. Conversely, the 3 children with an abnormal outcome (M.J., D.W., K.I.) had all had intravenous glucose administered promptly, and one may wonder whether their cerebral defects may have antedated the hypoglycaemia or even
436

MARGARET COX HENRY G. DUNN
caused it. None of these 9 patients have bilateral extensor plantar and Chaddock responses. D.S. was delivered by Caesarean section a t 36 relapsed so far. weeks’ gestation, because the mother had toxaemia
In addition to these 9 children, there are and marked idiopathic kyphoscoliosis with res- piratory insufficiency. There was difficulty in
Others i n the survey group Of infants of extracting the head from the uterus, and the low birth-weight who were diagnosed as placenta was sectioned during delivery. The baby
was limp, pale and oedematous after birth,with having idiopathic hypoglycaemia later bruises on the head and petechiae on the trunk (Table 11). Two of the 3 were males. Two but had fairly good air entry despite irregular
respirations. He weighed 3 Ib. 9 oz. ( I ,616 g.). At had been dysmature and one was only just 3 days, he became tremulous, with poor sucking above the 10th percentile in birth-weight. and depressed asymmetrical Moro response. He
also had kyphosis and moderate bilateral talipes Two have abnormalities on follow-up, equinovarus. The blood-sugar level was not while the third is of questionable neuro- checked. On discharge home at 55 days he had
mild left ptosis and still showed depressed postural logical status. responses. At 17 months he was admitted for ‘blank spells’ in which he stared and appeared
S.W., the girl in this group. was trenlulous and tremulous. These were found to be due to idio- had a depressed Moro response on the second to pathic hYPoglYcaemia. He was also significantly fifth days after birth, with Some peripheral cyanosis sniall for his age, still with left ptosis and dorsal and mild jaundice attributed to ABO incompati- kYPhosk and had a DQ of 91 on the Griffiths bility. However, after receiving incubator care for scale. At 23 months he was again admitted for 3 weeks she did quite well. Her blood-sugar level hYPoglYcaemia. Apart from the Ptosis, he then was not checked in the neonatal period. Subse- Presented no gross neurological abnormality, but quently she was admitted to hospital with charac- the possibility of some cerebral dysfunction teristic attacks of idiopathic hypoglycaeniia at 23 remains.
months and 3+ years. When last seen at 6 years 9 months she was well but had only just managed to pass Grade I , with a Wechsler (wrsc) full-scale B. Idiopathic / ~ . ~ ~ ~ o ~ ~ ~ ~ . c ~ I L ~ J I I ~ u hi other rQ of 93, and presented evidence of mild cerebral dysfunction-viz., absence of left-right distinction, poor control of fine movements, immature ex- Table I I I lists another 14 patients, in pressive language, difficulty with arithmetic, poor
line EEG with minimal spike activity in the posterior admitted to the Health Centre for Children head regions during drowsiness. She also had with idiopathic hypog~ycaemia during intermittent right esotropia, overactivity and a short attention span, and crossed laterality. 1958-1964. They are arranged in order of
R.B. is a uniovular ‘runt’ twin who was born increasing age at onset of symptoms. one first and weighed only 2 Ib. 8 oz. (1,134 g.), whereas his brother weighed 4 Ib. 5 OZ. (1,956 g.). is a femele twin (C.Z.) whose mother had R.B. did not breathe spontaneously for I minute toxaemia. l-his i n f a n t weighed 4 Ib. 1 I oz. after birth but then cried well. He required oxygen in the incubator for 24 weeks and was (2,126 8.) at birth after 36 weeks’ gestation, abnormally hypotonic during that time. He had and her non-identical t w i n sister weighed twitchings on the 6th to 8th days and was noted to be apnoeic in some of these. At 7 days his little more (5 Ib.). Among the 13 singletons,
was having intramuscular hydrocortisone and an interstitial infusion of glucose solution at that and these were all dysmature. They were time. On discharge home at I I + weeks he still not in our follow-up survey of infants had depressed postural responses (poor Moro, absent stepping and placing reflexes), but an EEG low birth-weight because they weighed 2 weeks earlier had shown a normal sleep trace. than 43 Ib., were not born at our At 8 months he had mild twitchings and rolling of the eyes during febrile episodes. At 18 months hospital, or were born before the survey he had Some unexplained tantrums. At 4 years, he began. s~~~~~~~ started in these 14 was admitted to hospital with a hypoglycaemic convulsion, preceded by confusion and limpness. children at ages varying from 3 months to When the hypoglycaemia had been corrected, an 8 years but at or before 2 years in 1 1 cases. EFG again proved normal. When last seen at 44 years he had a Stanford-Bjnei 1 0 of only 78, with The neonatal records of the 4 ex- a Vineland SQ of 102, and the Graham-Ernhart dysmature children showed that all had Block Sort Test was suggestive of ’organic brain damage’. He was also overactive and impulsive, had signs possibly due to hypoglycaemia, with mood swings and brief attention span, and but had had blood-sugar measure- had a significantly small head for his age and height, immature speech, poor co-ordination and ments. In the case of both K.L. and L.F. a
c17ildre,, ac/i77irted tO hos,,iral
tactile appreciation of block shapes, and a border- addition to the just described, who were
blood-sugar level was 106 mg. Per 100 nd.. but he 4 had a birth-weight below 5 3 Ib. (2,500 g.),
43 7

TA
BL
E I
1 l’
hree
Lo
w B
irth-
wei
ght C
hild
ren
Adm
itted
with
Hyp
ogly
caem
ia L
ater
-
Oat
ieni
-
Dys
- m
atur
e
-
Bor
der-
lin
e*
-
Min.
bloo
d-
suga
r :m
g. %
-
-
42
27
-
Age
2-5
days
23
mos.
3)
yr.
6t
yr.
~ -
6-8
days
9 wk.
8
mos
. I
yr.
18
mos.
4 yr
.
-
3 da
ys
13
mos
. 17
m
os.
23
mos
. -
-
Wk of
gest
atio
n
35
Neu
rolo
gic
al
sfar
us
16. 0
2.
(g.)
C
omm
ent
Fol
low
-up
Sym
ptom
s an
d si
gns
EEG
sw
-
RB
~
6)
yr.-F
ree
of s
eizu
res
sinc
e 31
yr.
Mild
cer
ebra
l dy
sfun
ctio
n. W
.I.S.
C.
full-
scal
e IQ
93
at 6
6 yr
.
Abn
orm
al
Tre
mor
s,
depr
esse
d M
oro
resp
onse
L
imp,
con
fuse
d
Con
vuls
ion
pre-
ce
ded
by c
onfu
sion
(A
sym
ptom
atic
)
3.12
(1
701)
Mul
tiple
spi
ke a
nd s
low
- w
ave
activ
ity in
sle
ep
Nor
mal
in n
on-h
ypo-
gl
ycae
mic
stat
e B
orde
rlin
e: m
inim
al
spik
e ac
tivity
in p
oste
rior
re
gion
s du
ring
dro
wsi
ness
Abn
orm
al
2.8
(I
134)
34
Y
es
‘Run
t’ t
win
(o
ther
wei
ghed
4
Ib.
5 02
. (1
956
g.)
Plac
enta
m
onoc
hori
onic
lO6t
8 -
-
33
2
Tw
itchi
ng,
apno
eic
epis
odes
? Fe
brile
co
nvul
sion
Tan
trum
s
Con
vuls
ion
pre-
ce
ded
by
conf
us-
ion
and
limpn
ess
-
-
44 y
r.-c
ereb
ral
dysf
unct
ion,
‘or
gani
c bc
havi
our
synd
rom
e’,
smal
l hea
d.
Bin
ct IQ
78
Nor
mal
sle
ep tr
ace
(asl
eep
thro
ugho
ut)
Nor
mal
-
-
Nor
mal
with
blo
od-s
ugar
59
mg.
per
cen
t
DS
3.9
(1
616)
36
- Y
es - M
ater
nal
toxa
emia
and
ky
phos
colio
sis
(mot
her
had
fata
l re
spir
ator
y fa
ilure
18
mos
. la
ter)
C
aesa
rean
se
ctio
n
Tre
mor
s, h
igh-
pi
tche
d cr
y,
depr
esse
d M
oro
resp
onse
‘Bla
nk s
pells
’ w
ith t
rem
or (
mild
ot
itis
med
ia)
Let
harg
y an
d se
mi-
com
a (u
pper
res
pira
tory
in
fect
ion)
-
Normal a
t 2 w
eeks
. 23
mos
.-no
gros
s ne
urol
ogic
al a
bnor
mal
ity.
Con
geni
tal
kyph
osis
. pt
osis
- and
talip
es. G
riff
itt
oq
91
at
It yr
.
Que
stio
nabl
e
Nor
mal
-
Nor
mal
with
blo
od-s
ugar
59
mg.
per
cen
t
SW’s
bir
th-w
eigh
t fal
ls ju
st a
bove
the
10th
per
cent
ile f
or g
esta
tiona
l ag
e ac
cord
ing
to L
ubch
enco
(19
63).
t RR’. h
lnod
-rup
ar of 1
06 m
p.
oer
eent
was
rec
orde
d w
hile
he
was
rec
eivi
ng in
tram
uscu
lar h
ydro
cort
ison
e an
d in
ters
titi
al g
luco
se in
fusi
on.

TA
BL
E 1
11
Four
teen
Non
-Sur
vey
Chi
ldre
n A
dmitt
ed w
ith I
diop
athi
c H
ypog
lyca
emia
co
ntin
ued
over
leof
-
Wk
. of
gesr
atio
n
-
DYS
- na
ture
'a
lien
t
I_
AS
__
EP
Bir
rh-w
r.
(g.1
S
ex
1 Ib. 0:.
M
inim
um
bl
ood-
suga
r m
p.
per
cent
Age
-ran
ge
o/ s
ymp
rom
s C
om
men
t F
ollo
w-u
p
8 m
os.-s
ubto
tal
panc
reat
ecto
my
2 yr
s.-h
ealth
y
EEG
--
M
1 7.1
(3
203)
N
o 8*
, 10
. 15
, 27
34
to
7 m
os.
Tw
itchi
ng a
nd
star
ing
spel
ls 3
times
3f m
os.-m
ildly
sl
ow f
or
7 m
os.-n
orm
al
age
40
36
_-
F 1 5.15 (2
693)
No
Mot
her
has
Adi
e's
synd
rom
e
5 rnos. t
o 9
yrs.
R
ecur
rent
sei
zure
s 6
and 7
mos
.-nor
mal
1 I
mos
.-mor
e sl
ow a
ctiv
ity
and
one
burs
t of
(?)
sha
rp
wav
es o
n r
ight
sid
e 25
mos.
and
3 yr
s-bo
rder
- lin
e re
cord
; m
onor
hyth
mic
an
d sl
ow
7 yr
s-pa
roxy
smal
bi
late
ral
high
-vol
tage
sh
arp
wav
es a
nd s
pike
s
9 yn
.+rg
anic
co
nvul
sive
dis
orde
r.
In r
esid
entia
l sc
hool
fo
r ret
arde
d ch
ildre
n.
Fast
ing
bloo
d-su
gar
norm
al
Abn
orm
al
37.4
7
1
(181
4)
I 4'0
41
Yes
M
ater
nal
toxa
emia
; sm
all u
lace
n
25,
367,
14
8 m
os.
to 7
yrs
. G
ener
aliz
ed c
on-
vuls
ions
, ni
ght,
or
earl
y m
orni
ng
34 y
r.-no
rmal
4&
sh
arp yr.-b
orde
rline
; w
aves
dur
ing
(?)
slee
p,
and
spik
e-an
d-sl
ow
activ
ity w
hen
drow
sy
wav
es
5 yr
.-spi
ke-a
nd-s
low
w
hen
drow
sy,
with
bloo
d-su
gar
48 m
g. %
84 y
r. -n
o
seiz
ures
in
pas
t ye
ar.
In
spec
ial c
lass
aft
er
faili
ng G
rade
I.
Hyp
erac
tive
Abn
orm
al
I LL
__
vc
~
SJ
38
___ 40
Yes
__
N
o
Mat
erna
l to
xaem
ia;
fam
ily h
isto
i of
epi
leps
y
24:
9 m
os. t
o 5
yr.
44 y
r.-fa
stin
g bl
ood-
su
gar
96 m
g. %
6
yr.-n
o co
nvul
- si
ons
in p
ast y
ear.
M
ild
cere
bral
dys
- fu
ncti
on. W
echs
ler
(WIS
C).
Ful
l Sca
le
IQ 8
4 (v
erba
l IQ
74,
pe
rfor
man
ce I
Q 9
9)
Abn
orm
al
wav
e 11
yr.-
bord
erlin
e;
dysr
hyth
mia
slow
2-2b
yr.-
bord
erlin
e;
exC
ess
shar
p w
aves
dur
ing
spin
dle
phas
e of
sle
ep
2-2t
w
aves
yr.-a
borti
ve
duri
ng b
ypog
lyca
emic
sh
arp
slee
p. c
lear
ed a
fter
glu
cose
6f
yr:-
irreg
ular
sp
ike
and
slow
wav
e ac
tivity
bi
sync
hron
ousl
y
14 m
os.-n
orm
al
15 m
os.-
diff
usel
v sl
ow.
prob
ably
due
to
h ypo
glyc
aem
ia
6 neur
olog
ical
yr
.-no
gros
s
abno
rmal
ity.
A
v. i
ntel
ligen
ce.
Smal
l sta
ture
18#,
39
11-1
5 m
os.
Tan
trum
s. c
onvu
l-
sion
. to
nic
seiz
ures
with
br
eath
-hol
ding
Nor
mal
40
No
Fam
ily h
istc
of
epi
leps
y 34
14
rnos. t
o 2
yr.
Tan
trum
and
st
arin
g sp
ells
2 yr
.-nor
mal
tw
ice
-abn
orm
al
once
w
ith r
ando
m s
pike
-and
- sl
ow w
aves
bila
tera
lly
5 yr
.-'bl
ank
spel
ls'
and
emot
iona
lly
labi
le a
t 3
yr.
Que
stio
nabl
c
MB
40
No
Fam
ily h
istc
of
epi
leps
y 3
yr.-n
o gr
oss
neur
olog
ical
ab
norm
alit
y
Nor
mal
16
mos.
only
Sy
ncop
e af
ter
fast
ing
17 rnos. to
3 y
r. C
oma
and
conv
ulsi
ons
36 0
25, 5
1 F
G -
40
- No
-
17 m
os.-
only
fas
t-w
ave
dysr
hyth
mia
rela
ted
to
barb
itur
ates
. Unc
hang
ed
at 2
and
3 y
r.
5 yr
.--c
onvu
lsiv
e di
sord
er w
ith m
enta
l re
tard
atio
n
Abn
orm
al

TA
BL
E I
llL
anti
nu
ed
Four
teen
Non
-Sur
vey
Chi
ldre
n A
dmin
ed w
ith I
diop
athi
c H
ypog
lyca
emia
- co
ntin
ued
EE
G
! A
ze-r
ang
e 01 s?
mpf
onrs
F
ollo
w-u
p
~~~
19 m
os.
only
C
onvu
lsio
n 19
mos
.-no
rmal
4
yr.-n
o gr
oss
neur
olog
ical
ab
norm
alit
y
20 m
os. o
nly
20 m
as.-
bo
rder
line;
do
ubtf
ul le
ft-s
ided
sl
ow-w
avz
abno
rmal
ity
7 yr
.-no
gros
s ne
urol
ogic
al
abno
rmal
ity
8 yr
. on
ly
Ear
ly m
orni
ng a
nd
la
te a
fter
noon
w
eakn
ess.
Poo
r sc
hool
rec
ord
-
10 y
r.-sc
hool
pr
ogre
ss p
oor.
IQ
91
-
D, 5
-
mat
ure
No
-
-
Yes
-
Yes
,Veu
rolo
,qir
al
srar
us
Bir
rh-w
r.
M.k
, pr
srnr
ion
Com
nwrt
bl
ood-
ruqa
r (m
a. p
er c
errr
)
.-qT
(334
5)
Nor
mal
-T
Nor
mal
M
ater
nal
toxa
emia
: si
ster
hy
pogl
ycae
mic
.q--
z-
(238
1 J
~
2 to
I2
yr.
Ear
ly m
orni
ng
com
a an
d se
mi-
com
as
3 yr
.-no
rmal
I2
yr.-
no
gros
s ne
urol
ogic
al
abno
rmal
ity.
R
epor
ted
wel
l. S
choo
l pr
ogre
ss
acce
ptab
le
Nor
mal
7ij
-G-
(382
9)
WR
I
F
No
F
amil
y hi
stor
y 49
of
dia
bete
s m
elli
tus
34 y
r.-n
orm
al
4 yr
.-no
gros
s ne
urol
ogic
al
abno
rmal
ity
Nor
mal
31
yr.
onl
y.
Syn
cope
aft
er
2 ea
rly
mor
ning
se
mi-
com
as.
Hea
dach
e, n
ause
a,
pall
or,
fati
gue
and
ab
dom
inal
pai
n T
Tq
-7
7
(294
8)
~-
~~
-
5-10
! I2
yr.
-bor
derl
ine:
pa
roxy
smal
hig
h-am
plit
ude
slow
-wav
e re
spun
% t
o hy
perv
enti
lati
on
-~
61 y
r.-s
ynco
pal
atta
cks.
obe
si1.
y.
abdo
min
al p
ain.
G
oo
d s
choo
l pr
ogre
ss
Que
stio
nabl
l No
of d
iabe
tes
mel
litu
s
(212
6) t B
inov
ular
tw
in
(tw
in 5
Ib.
or
2.26
8 g.
). T
Mat
erna
l
Que
stio
nabl
i N
o
-
I to
xaem
ia
* + +
$
0
0 0
**
AS
- B
lood
-sug
ar b
elow
50
mg.
per
cen
t o
n 1
2 se
para
te d
ays,
duri
ng in
itia
l adm
issi
on.
JB - C
ereb
rosp
inal
flu
id s
ugar
leve
l 33
mg.
per
cen
t at
this
tim
e.
LL
- C
ereb
rosp
inal
flu
id s
ugar
15
mg.
per
cen
t at
18
mos
., an
d 2
3 m
g. p
er c
ent
at 2
-2/1
2 yr
. V
C - B
lood
-sug
ar h
elow
50
mg.
per
cen
t o
n 8
sep
arat
e da
ys a
t 14
mos
., an
d o
n 3
sep
arat
e da
ys a
t 15
mos
. M
B - C
ereb
rosp
inal
flu
id s
ugar
42 mg.
per
cent
. L
F - B
lood
-sug
ar b
elow
50
mg.
per
cen
t o
n 4
sep
arat
e da
ys.
Cer
ebro
spin
al f
luid
sug
ar 1
3 m
g. p
er c
ent.
K
L - C
ereb
rosp
inal
flu
id s
ugar
21
mg.
per
cen
t.

MARGARET COX HENRY G. DUNN
C. Further analysis oj'jndings The 7 children listed in Tables I 1 and 111
who were originally dysmature or border- line and were admitted with hypoglycaemia later were not investigated systematically. Glucose-tolerance tests were performed in all 7 children (intravenously in 2, orally in 4, and by both routes in 1). The results were within normal limits during the first 24 hours in all children except D.S., who had abnormally low fasting levels (33 and 47 mg. per 100 ml.) on two occasions. However, in 5 cases the test was carried on for 5 hours, and in 3 of these (L.F., L.L. and S.W.) the blood-sugar level dropped below 50 mg. per 100 ml. at 3 hours (to 44,44 and 49 mg.). I n 2 of these it then rose again at 4 and 5 hours, but in
younger sibling was also dysmature (4 lb. 14 oz. or 2,211 g. at 41 weeks, and 4 Ib. 10 oz. or 2,098 g. a t 40 weeks, respectively), and K.L. had a neonatal convulsion while L.F. had 'weak spells' a t 2-23 years.
Information on the subsequent course of these 14 children is based on corres- pondence with their physicians and the hospital records of their further admissions. Three of the children have subnormal intelligence at 5-9 years, but E.P. and F.G. have an organic convulsive disorder which may be the primary abnormality. L.L. has mild cerebral dysfunction and a paroxys- mal abnormality of the EEG. Three others have questionable neurological status at 5-10 years. The remaining 7 children are normal at 2-12 years, though the youngest required a subtotal pancreatectomy at 8 months and the oldest has had one relapse of hypoglycaemia at 11 years. Of the 12 patients who have had one or more EEG studies, E.W., K.L. and W.R. had normal records and A S . and V.C. showed only slowing due to the hypoglycaemia itself; L.F. and L.M. had borderline records, and only 5 had definite EEG abnormalities.
: I
44 1
L.F. the level continued to fall from 44 mg. at 3 hours to 31 mg. per 100 ml. at 5 hours. Insulin-tolerance tests in 3, adrenaline- tolerance tests in 4, and leucine-tolerance tests in 6 of these formerly dysmature children all gave normal results.
Thus essentially the limited biochemical investigations of these ex-dysmature child- ren showed no abnormality apart from terminal hypoglycaemia after 3 hours in 3 out of 5 patients in whom the glucose- tolerance tests were carried on for 5 hours. This terminal hypoglycaemia would be in keeping with the possibility of inadequate secretion of catecholamine when the blood- sugar level falls in response to endogenous insulin. However, no measurements of catecholamine excretion and its response to insulin were performed.
When we add the borderline dysmature children (J.P. in Table I and S.W. in Table 11) to all those who had fetal malnutrition (dysmaturity) and developed hypoglycae- mia either in the neonatal period or later, we obtain a total of 12 cases. Of these, 5 have significant neurological abnormalities on follow-up, and 2 are of questionable status, while the remaining 5 have no gross dysfunction of the nervous system. On the whole, this outcome seems similar to the ultimate neurological status in the remaining 14 children, which was abnormal in 4, questionable in 5 and normal in 5.
The birth-weights of all 26 patients with idiopathic hypoglycaemia are shown in relation to normal fetal growth curves for singletons and twins in Figs. 1 and 2. These show that the frequency of some degree of intrauterine malnutrition is probably greater than one would calculate from the incidence of dysmaturity accord- ing to our strict criterion of a birth-weight at or below (or only just above) the 10th percentile. While only 12 of the 26 children were strictly dysmature and 2 were borderline with a birth-weight just

DEVELOPMENTAL MEDICINE A N D CHILD NEUROLOGY. 1967, 9
above the 10th percentile, the Figures show that 21 of the 26 had a birth-weight below the 50th percentile and one was at the percentile itself, leaving only 4 with an above-average birth-weight in relation to their length of gestation. All the 5 twins in this series had birth-weights below the 50th percentile.
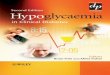
Finally, the 14 hypoglycaemic children with a birth-weight below 4-5 Ib. in Tables I, TI and I l l (8 dysmature, 2 borderline and 4 premature) were compared with a control group without apparent hypoglycaemia. The control cases were obtained from the records of our prospective survey of infants with low birth-weight by taking the next- born baby matched in sex, plurality and birth-weight category, within ranges of f Ib. (Table IV). Of the 14 hypoglycaemic children, I 1 were neurologically abnormal or questionable, whereas only 4 of the 14 controls were subsequently abnormal or questionable. This difference is statistically significant (x' L; 4.517 at p << 0.05 with Yates' correction).
Discussion It is well-recognised that neonatal idio-
pathic hypoglycaemia can be relieved by the early administration of intravenous glucose solution, which may have to be supplemented by steroids. If untreated, the disease may cause irreparable brain dam- age. Therefore, it should be considered a medical emergency (Brown and Wallis 1963), and early diagnosis is vital. The diagnostic difficulty lies in the non- specificity of the symptoms and signs in neonates, particularly in infants of low birth-weight who commonly have cyanotic and apnoeic episodes, irritability or drowsi- ness, depressed postural responses and even tremulousness. The only way to avoid missing the diagnosis is to bear it in mind and check the blood-sugar level. When lumbar puncture is performed, the spinal fluid sugar level may also be helpful. The
recent finding that neonatal hypoglycaemia is particularly common in dysmature infants of low birth-weight with relatively long gestation (fetal malnutrition), and in the smaller of twins with discordant birth- weight, may also be helpful in diagnosis and is confirmed in the present study. Maternal toxaemia is a useful diagnostic pointer in many cases, and the placenta may be small or infarcted.
The frequency of neonatal idiopathic hypoglycaemia is not yet certain. Neligan and his colleagues (1963) detected 12 cases with symptoms among approximately 6,000 babies born in hospital--i.e., about 2 per 1,000 live births. Farquhar (1963) considered the condition rarer in his local experience in Scotland and wondered whether the incidence might vary with socio-economic status, the proportion of complicated deliveries, and the use of drugs influencing carbohydrate metabol- ism. On the other hand, Wybregt et al. ( 1964), from routine blood-glucose deter- minations found that 6 per cent of 128 babies in a nursery for premature infants in Chicago had significant hypoglycaemia and symptoms. That group included many non-white and indigent infants and also about 18 per cent of extramural origin. However, if one accepts that group of infants as a characteristic sample of 'pre- matures' and presumes that the incidence of low birth-weight is about 7 per cent of all births, then the infants of low birth- weight alone would bring the incidence of neonatal idiopathic hypoglycaemia to at least 4 per 1,000 live births. It is also note- worthy that all the cases of idiopathic hypoglycaemia detected by Wybregt and her colleagues occurred among the 77 per cent with a birth-weight of under 2,000 g., so that the incidence of hypoglycaemia in that weight-group was nearly 8 per cent. I n comparison, the finding of only 9 such cases (about 2 per cent) among 480 infants with a birth-weight of 44 Ib. (2,040 8.) or
442

P
P
H Y
PO
GL
YC
AE
MIA
N
O A
PP
AR
EN
T H
YP
OC
LY
CA
EM
IA
__
__
._
__
_.
DQ
Pari
rnt
Sex
B
irth
-wt.
Wk.
of
L at
esf
neur
olog
ical
or
(g.)
grs
tari
on
st
atus
IQ
1.61
6 38
Q
uest
iona
ble
at 2
4 yr
. 79
_
__
JB
at
M
1,24
7 28
N
orm
al a
t 24
yr.
83
5 ;a
RH
M
2,
013
38
Nor
mal
at
It y
r. I1
8
0
>
9
m -1
c,
Lrrr
est n
euro
logi
cal
SfR
lYS
Pa
tient
B
arh-
wr.
Wk.
o/
(g.)
ges
tatio
n
-
LK
F 1.
446
40
Nor
mal
at
3 yr
.
MJ
M
1.30
4 38
A
bnor
mal
at
3 yr
.
DT
h
sw
F
1.70
1 35
A
bnor
mal
at
6( y
r. KF
F
1,92
8 37
N
orm
al a
t 6f
yr.
I05
1,72
9 37
N
orm
al a
t 24
yr.
-_
__
M
-_
_
RB
**
M
1.13
4 34
A
bnor
mal
at
44 y
r. M
I .
446
28
Nor
mal
at 2
t yr
. 10
0
DS
M
1.
616
36
Que
stio
nabl
e at
2 y
r. 1,
701
36
Nor
mal
at
24 y
r. 9
1
JB
LL
F
1,446
~~
__
_
M
1.81
4 41
A
bnor
mal
at
8f y
r.
M
1,58
8 37
N
orm
al a
t 64
yr.
115
1.38
9 34
N
orm
al a
t 6
f yr
. 91
5
Nor
mal
at
4 yr
. 9
2
m F
38
Abn
orm
al a
t 6
yr.
2
.e
BL
F
1,44
6 31
Q
uest
iona
ble
at 4
yr.
JP**
M
1,
474
33
Que
stio
nabl
e at
2t y
r. 1,
389
29
Abn
orm
al a
t 15
yr.
71
F
850
27
Abn
orm
al a
t 2
t yr
. A
R**
F
1.
219
28
Que
stio
nabl
e at
I yr
. 71
D
W**
LD
M
1.
729
31
Que
stio
nabl
e at
It y
r. JM
cI
M
1,84
3 32
N
orm
al a
t I &
yr.
96
KI
F 1,
332
31
Abn
orm
al a
t I y
r.
DT
u**
M
1,
474
34
Nor
mal
at
I yr
. 1,
389
28
Que
stio
nabl
e at
I!
yr.
69
Ave
rage
1.461
34.7
A
vera
ge
1.53
3 32
.4
--
8 _
__
__
z
F
1.24
7 29
N
orm
al a
t 1
yr.
91
z
-_
-
-
__-_
-
DEVELOPMENTAL MEDICINE AND
less, surviving the second day of life in our series, probably indicates that they have not been diagnosed adequately on clinical grounds. This may be particularly true in such conditions as cerebral anoxia, respira- tory distress syndrome and chilling, which can cause similar symptoms on their own but may also predispose the infant to h ypogl ycaemia.
The present study further confirms Neligan’s (1963, 1964) view that fetal mal- nutrition may be a warning sign of a possible long-term abnormality of carbo- hydrate metabolism, at least in the pre- school years. Few of the cases of neonatal hypoglycaemia relapse after the first 2 months but the ‘ex-dysmature’ babies evidently make a siz,eable contribution to the cases of idiopathic hypoglycaemia later-7* out of 17 such cases in our experience (Tables TI and 111). The signific- ance of fetal malnutrition is also suggested by the fact that the birth-weight of 13 of the 17 children was below the 50th per- centile. This peculiar association between malnutrition in ulero and idiopathic hypo- glycaemia later, even after the neonatal period, is still unexplained and has aetio- logical implications. Recent work, particu- larly by Cornblath and his group (1964), shows that idiopathic neonatal hypo- glycaemia is probably not explained by excessive secretion of insulin, abnormal sensitivity to insulin or ingested leucine,
* Including the borderline dysmature S.W. in Table 11.
CHILD NEUROLOGY. 1967, 9
lack of enzymes concerned in mobilising liver glycogen or converting galactose and fructose to glucose, or inability to use amino-acids and fats as glucose-sparers in muscle (Neligan 1964, Haworth 1965). It does seem that fasting lowers the blood- sugar level more readily after the first 36 hours of life than earlier (Kaye et al. 1961) and that dysmature infants have low hepatic glycogen reserves (Shelley 1964). It might therefore be concluded that such infants become hypoglycaemic because their hepatic glycogen stores are exhausted, and Cornblath and his colleagues (1964) have suggested that the metabolic needs of the relatively large brain in these babies may exceed the capacity of the liver to produce glucose, particularly on fasting and with the increased glucose require- ments of muscle in respiratory distress. However, the continued liability of ‘ex- dysmature’ children to become hypo- glycaemic later in childhood indicates that they have some more basic and permanent abnormality in their carbohydrate meta- bolism.
Acknowledgements: We are grateful to Dr. T. K. Oliver, Dr. S. Israels, Dr. J. A. Birkbeck and Dr. A. R. M. Cairns for encouragement and criticism, to Dr. N. L. Auckland for help in interpreting the EEGS, to Miss H . Mowat, R.N., for assistance with the tabulation of data, and to the Department of Medical Illustration, University of British Colum- bia, for help with the illustrations. We are also indebted to many colleagues for permission to study their patients and for information on the subsequent course of those listed in Table 111.
The study was assisted by funds provided by Public Health Grant No. 609-7-115 of the National Health Grants Programme, Canada.
SUM MARY Of 500 infants with a birth-weight of 4 t Ib .(2,040 g.) or less, born between September
1958 and May 1965, 480 survived the first 2 days and 9 were diagnosed by their medical attendants as having idiopathic neonatal hypoglycaemia. Of these 9, 4 were ‘dysmature’- i . ~ . , below the 10th percentile in weight for their gestational age-and a fifth had a birth- weight only just above that percentile.
Among 342 surviving infants in this group with low birth-weight, who have been followed prospectively, 3 others have been diagnosed as having idiopathic hypoglycaemia later at ages from 17 months to 4 years. Two of these were dysmature and the third had a birth- weight only just above the 10th percentile.
444

MARGARET COX HENRY G . DUNN
In addition to these 3 children in the follow-up study, 14 others with idiopathic hypo- glycaemia were admitted to the Vancouver General Hospital in 1958-1964. Among the 13 singletons in this group, 4 had had a birth-weight below 2,500 g., and thcse had all been malnourished. Thus, out of 17 children with idiopathic hypoglycaemia after the neonatal period, 7 had been dysmature (or borderline) at birth.
Adding the 2 borderline cases to the 10 children with hypoglycaemia who had been dysmature we find that the neurological status at the time of the last examination was abnormal in 5, questionable in 2 and normal in 5. The incidence of ultimate neurological dysfunction in this small group does not seem markedly different from that in the 14 other children with hypoglycaernia, in whom the latest neurological status was abnormal in 4, questionable in 5 and normal in 5. On the other hand, the outcome in the 14 children with a birth-weight below 4$ lb. (2,040 g.) who had hypoglycaemia is significantly more abnormal than in 14 controls of low birth-weight without hypoglycaemia from the prospective study.
Parmi 500 enfants d’un poids de naissance de 2040 g. ou moins nCs entre Septembre 1958 et mai 1965, 480 ont survCcu les deux premiers jours et chez 9 I’hypoglycCmie idio- pathique neonatale a etP. diagnostiquke par le mtdecin en charge. De ces 9 enfants, 4 Ctaient ‘dysmatures’-c’est-a-dire au-dessous de 10 pour cent en poids pour leur Ige gestationnel- et un cinquiime avait un poids de naissance juste au-dessus de ce 10 pour cent.
Parmi les 342 enfants survivants dans ce groupe A poids de naissance faible, qui ont C t i suivis par la suite on a diagnostiqut chez 3 autres I’hypoglycemie idiopathique plus tard B des %ges variant entre 17 mois et 4 ans. Deux de ceux-ci etaient dysmatures et le troisierne avait un poids de naissance juste au-dessus du 10 pour cent.
En plus de ces 3 enfants suivis dans le cadie de cette Ctude, 14 autres atteints d’hypoglycemie idiopathique ont t t e admis a I’h8pital general de Vancouver en 1958-1964. Parmi les 13 singletons de ce groupe, 4 avaient eu des poids de naissance au-dessous de 2500 g., et ceux-ci avaient CtC tous ma1 nourris. Ainsi siir 17 enfants atteints d’hypo- glyctrnie idiopathique apres la ptriode nkonatale 7 avaient ete dysmatures (ou presque) a la naissance.
En ajoutant ces 2 cas limitrophes aux 10 enfants atteints d’hypoglycemie qui avaient CtC dysmatures, nous trouvons que I’Ctat neurologique au moment dn dernicr examen Ctait: anormal chez 5, questionnable chez 2 et normal chez 5. L’incidence d u n dysfonctlonnement neurologique definitif dans ce petit groupe ne semble pas vraiment diffirente de celle parmi les 14 autres enfants atteints dhypoglycemie, chez lesquels I’etat neurologique recent etait anormal chez 4, questionnable chez 5 et normal chez 5. D’un autre cote, le resultat chez les 14 enfants avec un poids de naissance au-dessous de 2040 g. qui avaient de l’hypo- glyckmie B une periode quelconque est plus anormal de facon significative que chez 14 cas-tCmoins de poids de naissance faible sans hypoglycemie Ctudies dans le cadre de ces recherches.
ZUSA M MENFASSUNG Von 500 Sauglingen mit einem Geburtsgewicht von 4’, Ib. (2040 g.) oder weniger, die
zwischen September 1958 und Mai 1965 geboren wurden, uberlebten 480 die ersten zwei Tage und bei neun wurde von ihren medizinischen Pflegern die Diagnose von idiopathischer neonataler Hypoglykamie gestellt. Vier von diesen neun waren ‘unreif’ d. h . unter dem 10. Prozentsatz an Gewicht fur ihre Schwangerschaftsdauer und ein funfter hatte ein Geburts- gewicht etwas uber diesem Prozentsatz.
Unter 342 uberlebenden Sauglingen in dieser Gruppe mit niederem Geburtsgewicht, deren
RESUME
445

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1967, 9
Falle nach Moglichkeit verfolgt wurden, wurden bei drei, im spateren Alter, das von 17 Monaten bis zu 4 Jahren variierte, eine Diagnose von idiopathischer Hypoglykamie gestellt. Zwei von diesen waren unreif und der dritte hatte ein Geburtsgewicht nur etwas uber dem 10. Prozentsatz.
Zusatzlich zu diesen drei Kindern in der Fortsetzungs-Studie wurden vierzehn andere mit idiopathischer Hypoglykamie in das Vancouver General Hospital wahrend der Jahre 1958-1964 aufgenommen. Von den dreizehn einzigen Kindern in dieser Gruppe hatten vier ein Geburtsgewicht unter 2500 g. und diese waren alle unterernahrt. Demnach waren insgesamt sieben aus siebzehn Kindern mit idiopathischer Hypoglykamie nach der neo- natalen Periode ursprunglich unreif (oder an der Grenze von unreif) bei Geburt.
Wenn man die beiden Grenzfalle zu den 10 Kindern mit Hypoglykamie die unreif waren, hinzufugt, findet man, dass der neurologische Stand zur Zeit der letzten Unter- suchung in funf abnorm, in zwei fraglich und in funf normal waren. Die Haufigkeitsquote der letztlichen neurologischen Dysfunktion in dieser kleinen Gruppe scheint nicht bedeutend von der bei den vierzehn anderen Kindern mit Hypoglykamie zu differieren, bei denen der letzte neurologische Stand in 4 abnorm,in 5 fraglich und in 5 normal waren. Andererseits ist das Ergebnis bei den vierzehn Kindern rnit einem Geburtsgewicht unter 43 Ib. (2040 g,), die wahrend der einen oder anderen Zeit Hypoglykamie hatten, bedeutend abnormer als bei vierzehn Kontrollfallen init niederem Geburtsgewicht ohne Hypoglykamie, von der prospektiven Studie. RESUMEN
Sobre hipoglicemia idiophtica, con referencia especial a recikn nacidos de peso bajo Entre 500 reciCn nacidos que pesaron al nacer menos de 4+ libras (2040 g.), y que nacieron
entre el mes de Septiembre 1958 y el mes de mayo de 1965, 480 sobrevivieron a 10s dos primeros dias, y en 9 se diagnostic0 hipoglicemia idiopatica neonatal. Cuatro de esos 9 eran 'desmaturos', es decir, pesaron menos de la dCcima percentila para su edad gestacional; y otro peso muy poco mas de la dCcima percentila.
Entre 10s 342 nifios sobrevivientes en este grupo de peso bajo, a quienes se ha continuado a observar, se ha diagnosticado la hipoglicemia idiopatica en 3 otros, entre 10s 17 meses y 10s 4 aiios. Dos de estos eran desmaturos, y el tercero peso poco mas de la decima percentila.
Ademas de estos 3 niiios bajo observacion, 14 otros afectos de hipoglicemia idiopatica ingresaron a1 Hospital General de Vancouver durante 10s aiios 1958-1964. Entre 10s 13 hijos unicos en este grupo, 4 pesaron al nacer menos de 2500 g., y todos 10s 4 habian sido desnutridos. Asi se ve que 7 de 17 nifios afectos de hipoglicemia idiopatica despuCs del period0 neonatal habian sido desmaturos (0 casi desmaturos) a1 nacer.
Entre 10s 10 niiios afectos de hipoglicemia que habian sido desmaturos, y 10s dos casi desmaturos, el estado neurologico al examen mas reciente estaba anormal en 5, dudoso en 2, y normal en 5. La incidencia de disfuncion neurologica ultima en este grupo pequeiio no parece muy diferente de la de 10s otros 14 nifios afectos de hipoglicemia, cuyo estado neurologico a1 examen mas reciente estaba anormal en 4 casos, dudoso en 5, y normal en 5. Sin embargo, es claro que las consecuencias en 10s 14 niiios que pesaron menos de 43 libras (2040 g.) al nacer y que fueron afectos a un tiempo u otro de hipoglicemia, son mas anormales que en otros 14 nifios de entre 10s 342 bajo observacion, de peso bajo pero no afectos de hipoglicemia. REFERENCES Baens, G . S., Lundeen, E., Cornblath, M. (1963) 'Studies of carbohydrate metabolism in the newborn
Bessrnan. S. P. (1960) 'Diabetes mellitus: observations, theoretical and practical.' J . Pediar., 56, 191. Broberger, U., Jungner, I . , Zetterstrom, R. (1959) 'Studies in spontaneous hypoglycemia in childhood.'
446
infant. VI. Levels of glucose in blood in premature infants.' Pediatrics, 31, 580.
1. Peditrl.. 55, 71 3 .
MARGARET COX HENRY C . DUNN
- Zetterstrom, R. (1961) ‘Hypoglycemia with an inability to increase the epinephrine secretion in insulin-
Brown, R. J. K., Wallis, P. G. (1963) ‘Hypoglycaemia in the newborn infant.’ Lancet, i , 1278. Brunjes, S., Hodgman, J., Nowack, J., Johns, V. L. (1963) ‘Adrenal medullary function in idiopathic
Cochrane, W. A., Payne, W. W., Simpkiss, M. J., Woolf, L. 1. (1956) ‘Familial hypoglycemia precipitated
Colle, E., Ulstrom, R. A. (1964) ‘Ketotic hypogIycemia.’J. Pediat., 64, 632. Conn, J. W., Seltzer, H. S. (1955) ‘Spontaneous hypoglycemia.’ Amer. J. Med., 19, 460. Cornblath, M., Odell, G. B., Levin, E. Y. (1959) ‘Symptomatic neonatal hypoglycemia associated with
toxemia of pregnancy.’J. Pediat., 55, 545. - Reisner, S. H. (1965) ‘Blood glucose in the neonate and its clinical significance.’ New Engl. J. Med.,
273, 378. - Wybregt, S. H., Baens, G. S., Klein, R. I. (1964) ‘Symptomatic neonatal hypoglycemia: studies of
carbohydrate metabolism in the newborn infant. VIII.’ Pediatrics, 33, 388. Darrow, D. C. (1936) ‘Mental deterioration associated with convulsions and hypoglycemia.’ Amer. J. Dis.
Child., 51, 575. Etheridge, J. E., Millichap, J. G. (1964) ‘Hypoglycemia and seizures in childhood: the etiologic significance
of primary cerebral lesions.’ Neurology (Minneap.), 14, 397. Fajans, S. S., Knopf, R. F., Floyd, J. C., Conn, J. W. (1962) ‘On the physiologic significance of leucine
hypoglycemia in healthy subjects.’J. Lab. clin. Med., 60, 873. Farquhar, J. W. (1963) ‘Neonatal hypoglycaemia.’ Lancet, ii, 941. Floyd, J. C., Fajans, S. S., Knopf, R. F., Conn, J. W. (1963) ‘Evidence that insulin release is the mechanism
for experimentally induced leucine hypoglycemia in man.’ J. din. Invest., 42, 1714. Freinkel, N., Arky, R. A., Singer, D. L., Cohen, A. K., Bleicher, S. J., Anderson, J. B., Silbert, C. K.,
Foster, A. E. (1965) ‘Alcohol hypoglycemia. IV: Current concepts of its pathogenesis.’ Diabetes, 14, 350; Grollman, A., McCaleb, W. E., White, F. N. (1964) ‘Glucagon deficiency as a cause of hypoglycemia.
Metabolism, 13, 686. Gruenwald, P. (1963) ‘Chronic fetal distress and placental insufficiency.’ Biol. Neonat., 5, 215. Grumbach, M. M., Kaplan, S. L. (1960) ‘Amino acid and alpha-keto acid-induced hyperinsulinism in the
leucine-sensitive type of infantile and childhood hypoglycemia.’ J. Pediat., 57, 346. Hartmann, A. F., Jaudon, J. C. (1937) ‘Hypoglycemia.’ J . Pediat., 11, I . Haworth, J. C. (1965) ‘Carbohydrate metabolism idthe fetus and newborn.’ Pediar. Clin. N. Amer., 12, 573. - Coodin, F. J. (1960) ‘Idiopathic spontaneous hypoglycemia in children: report of 7 cases and review
of the literature.’ Pediatrics, 25, 748. - - Finkel, K. C., Weidman, M. L. (1963) ‘Hypoglycemia associated with symptoms in the newborn
period.’ Canad. med. Ass. J., 88, 23. - McRae, K. N. (1965) ‘The neurological and developmental effects of neonatal hypoglycemia: a follow-
up of 22 cases.’ Canad. med. Ass. J., 92, 861. Kaye, R., Davidson, M. H., Williams, M. L., Kumagai, M., Picou, D. M. (1961) ‘The response of blood
glucose, ketones and plasma non-esterified fatty acids to fasting and epinephrine injection in infants
induced diabetes.’ 1. Pediat., 59, 215.
spontaneous hypoglycemia of infancy and childhood.’ Amer. J. Med., 34, 168.
by amino acids.’ J. din. Invest., 35, 411.
and children.’ J. Pediat., 59, 836.
Soc. Med.. 57. 1061.
Kinsbourne, M., Woolf, L. I. (1959) ‘Idiopathic infantile hypoglycemia.’ Arch. Dis. Childh., 34, 166. Lloyd, J. K. (1964) ‘Diabetes mellitus presenting as spontaneous hypoglycemia in childhood.’ Proc. roy.
Lubchenco, L., Hansman, C., Dressler, M., Boyd, E. (1963) ‘Intrauterine growth as estimated from live- born birth-weight data at 24 to 42 wczks of gestation.’ Pediatrics, 32, 793.
Mabry, C. C., DiGeorge, A. M., Auerbach, V. H. (1960) ‘Leucine-induced hypogIycemia.’J. Pediat., 57,539. Madison, L. L., Mebane, D., Unger, R. H., Lochner, A. (1964) ‘The hypoglycemic action of ketones.
11. Evidence for a stimulatory feedback of ketones on the pancreatic beta cells.’ J. clin. Invest., 43, 408. McQuarrie, I . (1954) ‘Idiopathic spontaneously occurring hypoglycemia in infants.’ Amer. J. Dis. Child.,
87, 399. Naeye, R. L., Benirschke, K., Hagstrom, J. W. C., Marcus, C. C. (1966) ‘Intrauterine growth of twins as
estimated from liveborn birth-weight data.’ Pediatrics, 37, 409. Neligan, G. A. (1964) ‘Hypoglycaemia in the newborn.’ Proc. roy. Soc. Med., 57, 1059. - Robson, E., Watson, J. (1963) ‘Hypoglycaemia in the newborn.’ Lancet, i, 1282. Reisner, S. H., Forbes, A. E., Cornblath, M. (1965) ‘The smaller of twins and hypoglycaemia.’ Lnrrcef,
Rosenthal, T. M., Metz, R., Pirani, C. (1964) ‘Congenital leucine-sensitive hypoglycemia.’ Amer. J. Dis.
Shelley, H. J. (1964) ‘Carbohydrate reserves in the newborn infant.’ Brit. med. J., i , 273. Tynan, M . J . , Haas, L. (1963) ‘Hypoglycemia in the newborn.’ Lancet, i i , 90. Ulstrom, R. A. (1964) ‘Hypoglycemia.’ Lecture at seminar, American Academy of Neurology, Minneapolis. Van Creveld, S., Bouman, P. R., DeLeeuw, R., Oie, T. L. (1965) ‘Idiopathic hypoglycemia.’ Ann. paediur.
Woeber, K. A,, Arky, R. (1965) ‘Hypoglycaemia as the result of isolated corticotrophin-deficiency.’ Brit.
Wootton, I . D. P. (1964) Micro-analysis in Medical Biochemistry. 4th ed. London: Churchill. 93. Wybregt, S. H., Reisner, S. H., Patel, R. K., Nellhaus, G., Cornblath. M . (1964) ‘The incidence of neonatal
447
i, 524.
Child., 107, 343.
(Ba.rle), 205, 12.
med. J. , i i , 857.
hypoglycemia in a nursery for premature infants.’ J. Pediot.. 64. 796.