Embed Size (px)
Citation preview

CONSTIPATION IN CHILDREN
DR. HOSSAIN IBRAHIM AGEEL PEDIATRIC GASTROENTEROLOGIST
PEDIATRIC DEPARTMENT KFCH – JAZAN
1

PREVALENCE • Common problem in childhood. • The worldwide prevalence rates 1% -‐ 30%. • 3 to 5 percent of all visits to pediatricians. • 25 percent of pediatric GI consults.
2

Defini=on • Infrequent bowel movements. • Hard stool consistency. • Large stool size. Painful defecaHon
3

“NASPGHAN” defini=on a delay or difficulty in defecaHon, present for two weeks or more, and sufficient to cause significant distress to the paHent.
4

5

q Normal stool frequency • The iniHal bowel movement is within the first 24 hours of birth in 90 percent of normal newborns.
• Approximately 4 stools per day in the 1st week of life . • Gradually changes to 1-‐2 stools per day by the age of 4 years with range of 3 per day to 3 per week.
• BreasRed infants can stool with each feeding or only once every 7 to 10 days.
6

q Bowel control • Many children achieve voluntary bowel control between18 months and 2 years of age.
• Majority of children (98%) are toilet trained by 4 years of age.
• Girls achieve toilet training slightly earlier than boys.
7

ANATOMY OF ANORECTAL REGION
l Major structures include: ¡ External anal sphincter ¡ Puborectalis muscle ¡ Internal anal sphincter ¡ Rectum
8

NORMAL DEFECATION MECHANICS
9

10

E=ology of cons=pa=on
q Func=onal cons=pa=on: – ConsHpaHon without objecHve evidence of a pathological condiHon.
– Accounts for > 95% of all consHpated children. q Organic causes:
– Disease enHHes. – Accounts for less than 5% of all consHpaHon.
11

ORGANIC CAUSES OF CONSTIPATION Imperforated anus Anal stenosis Anteriorly displaced anus
Anatomic malformaHon
Hypothyroidism Hypokalemia Hypercalcemia Celiac disease CysHc fibrosis
Metabolic causes
Cerebral palsy Spina bifida Tethered cord Spinal cord trauma/tumor Neurofibromatosis
Neuropathic condiHons
12

ORGANIC CAUSES OF CONSTIPATION Hirschsprung disease IntesHnal Neuronal Dysplasia IntesHnal pseudo-‐obstrucHon Gastroschisis
IntesHnal nerve or muscle disorders
Opiates Phenobarbital AnH-‐cholinergics AnH-‐depressants ChemotherapeuHc agents Sucralfate Antacids Lead toxicity
Drugs/Toxins induced
13

Painful stool Voluntary withholding of feces
Prolonged fecal stasis with fluids
resorp=on
Larger and harder stool
Rectal dila=on
Urge to defecate disappears
PATHOGENESIS OF FUNCTIONAL CONSTIPATION
14

Causes of painful stools : • Difficult or stressful toilet training.
• Changes in rouHne or diet. • Stressful events. • Illness causing dehydraHon. • Unavailability of toilets. • Withholding while busy or playing.
Func=onal Cons=pa=on
15

Func=onal Cons=pa=on
Withholding behaviors : • Squaeng. • Crossing ankles. • SHffening of the body. • Holding onto furniture or mother.
• Flushing, sweaHng and crying.
• Hiding during defecaHon in a corner.
16

l Functional constipation presents most commonly at three age periods:
¡ Introduction of cereals and solid foods. ¡ Toilet training. ¡ The start of school.
Presenta=on when?
17

Diagnosis of func=onal cons=pa=on
ROME III criteria
18

q Infants and toddlers less than 4 years of age
Must include 1 months of at least two of the followings: • Two or fewer defecaHons per week. • At least one episode per week of inconHnence ager the
acquisiHon of toilet skills. • History of excessive stool retenHon. • History of painful or hard bowel movements. • Presence of a large fecal mass in the rectum. • History of large diameter stools that may obstruct the toilet.
19

q Older children or adolescents more than 4 years of age
Must include 2 months of two or more of the followings occurring at least once per week : • Two or fewer stools in the toilet per week. • At least one episode of fecal inconHnence per week . • History of retenHve posturing or excessive voliHonal stool
retenHon. • History of painful or hard bowel movements. • Presence of a large fecal mass in the rectum. • History of large diameter stools that may obstruct the toilet.
20

Associated symptoms Toilet habit Intes=nal : • Abdominal pain • Abdominal disten=on • Vomi=ng • Anorexia • weight loss or poor wt gain Extra-‐intes=nal • Urinary tract symptoms such
as frequency, enuresis, and infec=on.
History of chief complaint: • Age of onset of cons=pa=on • Stool frequency • Stool consistency • Stool size • Painful defeca=on • Blood in the stool • Withholding symptoms • History of encopresis • Time of 1st bowel movement
CLINICAL APPROACH -‐ HISTORY
21

Other important points in the history to address Including neonatal GI complica=ons such as NEC and prior surgeries
Past medical and surgical history
Fluid intake, milk consump=on, fiber content of food stuffs
Dietary
Cons=pa=on, celiac disease, cys=c fibrosis, etc.
Family
Household structure, stressors, temperament, toilet habits at school
Psychosocial
Toilet training history, Development Developmental Laxa=ves used and their results, drugs known to cause cons=pa=on
Medica=on
Atopic history, food allergy Allergy 22

“RED FLAG” HISTORY FINDINGS
• Delayed passage of meconium. • Onset in neonatal period or very early infancy. • Significant weight loss or poor weight gain. • Passage of blood . • Delayed developmental milestone especially motor.
• Abdominal distension with vomiHng.
23

Perineum, perianal, Digital rectal exams: • PosiHon of anus • Fissures or fistulas • Perianal erythema • Presence of soiling • Perianal sensaHon • Presence of anal wink • Anal sphincter tone • Size of rectal vault,
presence of polyps • Presence , size and
consistency of stool within the rectum
General examina=on • Vital signs • Growth parameters • Skin : Café au lait spots
Physical examina=on
Abdominal examina=on • Distension • Tenderness • Fecal masses • Bowel sounds
Back • PigmentaHon • Sacral dimples or pits • Tugs of hair • Mass (cysHc or solid)
Neuro examina=on • Lower extremity tone • Strength • Deep tendon reflexes • Cremasteric reflex
All systems should be Examined carefully
24

“RED FLAG” PHYSICAL EXAMS FINDINGS • Failure to thrive. • Abdominal distension. • Finding of spinal dysraphism. • PigmentaHon, dimples, or tugs of hair over lumbo-‐sacral
region . • Ano-‐rectal malformaHon. • Anteriorly displaced anus. • Patulous anus. • Absent cremasteric reflex. • Absent anal wink. • No stool is felt in the rectal vault with gush of stool ager
rectal exams. • Sensory or motor defects of the lower extremiHes.
25

Red flags Specialist referral FuncHonal
consHpaHon
ImpacHon
DisimpacHon EducaHon, MedicaHon, Diet, Behavioral modificaHon
Blood tests
EffecHve Not effecHve
Maintenance therapy Regular follow-‐up
Pediatric gastroenterologist
Appropriate treatment
Specialist referral
ConsHpaHon
Normal Abnormal
TherapeuHc approach to consHpaHon in children
26

MANAGEMENT 1. Educa=on 2. Disimpac=on 3. Maintenance therapy 4. Close follow-‐up
27

I. EDUCATION Educate pa=ent and family : • Explain pathophysiology. • Remove the negaHve alribuHons with soiling. • Promote consistent, posiHve supporHve aetudes with treatment.
• Advise parents that treatment can be prolonged and difficult, with relapses common.
• PaHent should not stop treatment abruptly, as this may lead to relapse.
28

2. DISIMPACTION
• Determine if fecal impacHon is present § Hard mass in lower abdomen (abdominal exam) § Dilated rectum filled with large amount of stool (rectal exam).
§ Excessive stool in the colon (KUB).
• Treat the impacHon if present: oral and/or rectal approach may be used .
29

30

DOSAGES MEDICATIONS ORAL ROUTE ADMINISTRATION -‐ (OVER 1-‐2 DAYS)
25 ml/kg/hour, up to 500 ml/hour unHl fecal effluent is clear
Polyethylene glycol with electrolyte soluHon
ORAL ROUTE ADMINISTRATION -‐ (OVER SEVERAL DAYS) 2 ml/kg twice per day for 7 days 3 ml/kg twice per day for 7 days 2 ml/kg twice per day for 7 days 1.5 g/kg/day for 3 days
Milk of magnesia Mineral oil Lactulose or Sorbitol Polyetylene glycol 3350 (PEG)
RECTAL ROUTE ADMINISTRATION 1 suppository for infants & toddlers 6 ml/kg, up to 135 ml for > 2 years
Glycerine suppositories Phosphate enema
FECAL DISIMPACTION REGIMEN
31

3. MAINTENANCE THERAPY
• Dietary interven=ons • Behavioral modifica=on • Laxa=ve therapy
Ø Goal is to pass one to two sog stools daily. Ø Allow rectal vault to approach normal size. Ø May take several months to years. Ø Includes:
32

Dietary interven=ons
• Increase fluid intake. • Small amounts of absorbable carbohydrates (e.g. sorbitol in prune, pear, and apple juice).
• Increase dietary fibers including whole grains, fruits and vegetables. Children older than 2 years of age should consume dietary fibers = age in ys + 5 g/day.
• EliminaHon of cow milk protein from diet may be helpful in some paHent with intractable consHpaHon in parHcular those with atopic disease.
33

BEHAVIORAL MODIFICATION q Establish a toilet-‐sieng schedules: • Unhurried Hme on toilet – 30 minutes ager meals in order to work with peristalHc contracHons.
• Regular toilet visits: 2-‐3 Hmes per day for 10-‐15 minutes in order to uHlize the gastro-‐colic reflex.
q Appropriate toilet hygiene: Sit up straight, thighs parallel to ground, good foot support, valsalva maneuver and no distracHons.
q PosiHve reinforcement: keep diaries of stool frequency combined with a reward system.
q Consider referral to mental health care provider if behavioral problems interfere with treatment.
34

LAXATIVE THERAPY
Divided into three major types : • OsmoHc agents: Absorb water in the intesHnal lumen and make stools sog.
• Lubricant agents: Facilitate the passage of stools through the colon.
• SHmulant agents: Induce colonic contracHons and expel stools.
35

SIDE EFFECTS DOSAGES MEDICATIONS OSMOTIC LAXATIVES
Mg, PO4, Ca BloaHng, cramps, Diarrhea Diarrhea, Flatulence, mild abdominal pain
1-‐3 ml/kg/day 1-‐3 ml/kg/day 0.8 g/kg/day
Magnesium hydroxide Lactulose Polyethylene glycol 3350 (PEG)
LUBRICANT LAXATIVES Risk of lipoid pneumonia 1-‐3 ml/kg/day Mineral oil
STIMULANT LAXATIVES Melanosis coli, HepaHHs, Abdomin Pain, arthropathy Hypokalemia, Urolithiasis Abdominal pain
2.5-‐15 ml/day 5-‐15 mg/day
Senna Bisacodyl
COMMONLY USED LAXATIVES IN CHILDREN
36

4. Close follow-‐up and prognosis
• 60% of children with funcHonal consHpaHon respond to convenHonal therapy by one year.
• 30-‐50% of children treated persist to have severe symptoms ager 5 years of follow-‐up.
• Nonresponse to convenHonal therapy caused commonly by unrecognized disease, poor compliance or associated behavioral problems.
37

Tests to consider if consHpaHon is refractory to medical management
• Thyroid funcHon tests. • Serum calcium and potassium level. • Serum lead level. • TTG IgA, serum IgA level. • Sweat test if clinically indicated . • MRI of lumbosacral spine if clinically indicated. • Barium enema. • Rectal biopsy. • Anorectal or colonic manometry (more advanced)
38

• History : Infant with significant consHpaHon from neonatal period, especially with delayed passage of meconium.
• Physical exam : Empty rectal vault on rectal exam with gush of stool.
HIRSCHSPRUNG DISEASE
• Unprepped barium enema • Rectal biopsy
39

HIRSCHSPRUNG DISEASE Motor disorder of the colon caused by the failure of neural crest cells (precursors of colonic Ganglion cells) to migrate completely during colonic development so affected colonic segment fails to relax causing a func=onal obstruc=on
40

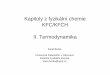
HIRSCHSPRUNG DISEASE
Barium enema: Contracted distal colon, abrupt transiHon to a dilated proximal colon 41

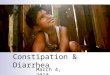
HIRSCHSPRUNG DISEASE Submucosa
Myenteric
Rectal biopsy: absence of ganglion cells 42

History and physical examinaHon showed: • Spinal dysraphism. • PigmentaHon, dimples, or tugs of hair over lumbosacral region.
• Neurological impairment of perianal area such as patulous anus, absent cremasteric reflex, absent anal wink.
• Sensory or motor defects of the lower extremiHes.
Plain film of lumbosacral spine MRI of spine
43

Mechanism of cons=pa=on • Spas=c colon • Loss of rectal tone and sensa=on
• Colonic hypomo=lity and dilata=on
• Laxity of external anal sphincter.
• Poor reinforcement of evacua=on
SPINA BIFIDA
44

SPINA BIFIDA
45

TETHERED SPINAL CORD
Common causes : • Lipoma • Split cord malformaHon • Dermal sinus tract • Faly or Hght filum • Myelomeningocele
46

TETHERED SPINAL CORD
47

NEUROFIBROMATOSIS • Autosomal dominant • Cardinal features: 1-‐ mulHple neurofibromas 2-‐ café au lait spots 3-‐ axillary & inguinal freckling 4-‐ pigmented iris hamartomas • Cons=pa=on is due to intes=nal neurofibromas which lead to intes=nal obstruc=on.
48

ANAL FISSURE
49

STREPTOCOCCAL DERMATITIS
50

Imperforate anus
51

ANTERIOR DISPLACED ANUS
52

Anogenital index:
Distance in cenHmeters: from the vagina or scrotum to the anus from the vagina or scrotum to the coccyx. Females: 0.39 ± 0.09 Males: 0.56 ± 0.2
53

CELIAC DISEASE
q Unhappy child q Slender limbs q Wasted bufocks q Prominent abdomen
54

CONGENITAL HYPOTHYROIDISM
q Coarse facial features q Macroglossia q Large fontanel q Umbilical hernia q Molled, cool, dry skin q Developmental delay
Ø ConsHpaHon due to hypotonia of the abdominal or intesHnal structures
55