-
IMAGING OF BLUNTABDOMINAL TRAUMA, PART II
Ruedi F. Thoeni, M. D.University of California, San
Francisco
IMAGING OF BLUNTIMAGING OF BLUNTABDOMINAL TRAUMA, PART
IIABDOMINAL TRAUMA, PART II
Ruedi F. Thoeni, M. DRuedi F. Thoeni, M. D..University of
California, San FranciscoUniversity of California, San
Francisco
SCBT-MR Summer Practicum, Williamsburg, 2009SCBTSCBT--MR Summer
Practicum, Williamsburg, 2009MR Summer Practicum, Williamsburg,
2009
-
Learning Objectives for blunt abd. TraumaLearning Objectives for
blunt abd. Trauma
• MDCT Trauma Protocol
• Incidence of bowel and mesenteric injuries
• Specific signs of bowel/mesenteric injuries
• Nonspecific findings of bowel/mesenteric injuries
• Plan in patients with nonspecific signs
•• MDCT Trauma Protocol MDCT Trauma Protocol
•• Incidence of bowel and mesenteric injuriesIncidence of bowel
and mesenteric injuries
•• Specific signs of bowel/mesenteric injuriesSpecific signs of
bowel/mesenteric injuries
•• Nonspecific findings of bowel/mesenteric injuries Nonspecific
findings of bowel/mesenteric injuries
•• Plan in patients with nonspecific signsPlan in patients with
nonspecific signs
-
ABD. TRAUMA (16 or 64) MDCTABD. TRAUMA (16 or 64) MDCT
• Contrast Materials:– Oral contrast (if possible): 3 cups of
450 ml of
2.2% Gastrografin (10 mL/450 of water)– Rectal contrast (if
possible: shear force):
40 cc of Conray 60% in 1000 mL normal saline: use 500-1000 mL as
tolerated
– IV contrast: 3 mL/sec for 150 ml• Important:
– Clamp bladder catheter to achieve full distention of
bladder
•• Contrast Materials:Contrast Materials:–– Oral contrast (if
possible):Oral contrast (if possible): 3 cups of 450 ml of 3 cups
of 450 ml of
2.2% Gastrografin (10 mL/450 of water)2.2% Gastrografin (10
mL/450 of water)–– Rectal contrastRectal contrast (if possible:
shear force):(if possible: shear force):
40 cc of Conray 60% in 1000 mL normal saline: 40 cc of Conray
60% in 1000 mL normal saline: use 500use 500--1000 mL as
tolerated1000 mL as tolerated
–– IV contrast:IV contrast: 3 mL/sec for 150 ml3 mL/sec for 150
ml•• Important:Important:
–– Clamp bladder catheter to achieve full Clamp bladder catheter
to achieve full distention of bladderdistention of bladder
-
ABD. TRAUMA (16 or 64) MDCT ABD. TRAUMA (16 or 64) MDCT
• MDCT Technique:- Detector config: 16 (64) x 1.25 mm, mode
1.375:1- Reconstruction thickness: axial: 1.25 mm & 5 mm-
ALWAYS use coronal and sagittal MPRs (3mm)
• Scan delay:- 70-80 sec or smart prep- 3 minute delay-
Diaphragm to ischial tuberosity
•• MDCT Technique:MDCT Technique:-- Detector config: 16 (64) x
1.25 mm, mode 1.375:1Detector config: 16 (64) x 1.25 mm, mode
1.375:1-- Reconstruction thickness: axial: 1.25 mm & 5
mmReconstruction thickness: axial: 1.25 mm & 5 mm--
ALWAYSALWAYS use coronal and sagittal MPRs (3mm)use coronal and
sagittal MPRs (3mm)
•• Scan delay:Scan delay:-- 7070--80 sec or smart prep80 sec or
smart prep-- 3 minute delay3 minute delay-- Diaphragm to ischial
tuberosityDiaphragm to ischial tuberosity
-
ABD. TRAUMA (16 or 64) MDCT ABD. TRAUMA (16 or 64) MDCT
• Important:• Single acquisition: “total body” trauma CT
scan:
head, cervical spine, chest, abdomen & pelvis• Delayed scans
(3 min) optional: parenchymal organs,
excretory system incl. bladder, vasc. extravasation• CT
cystogram for bladder injury: 300-400 cc of
20 cc of 60% contrast/500 cc of sterile saline
• • Important:Important:•• Single acquisitionSingle acquisition:
: ““total bodytotal body”” trauma CT scan: trauma CT scan:
head, cervical spine, chest, abdomen & pelvishead, cervical
spine, chest, abdomen & pelvis•• Delayed scans (3 min)
optionalDelayed scans (3 min) optional: parenchymal organs, :
parenchymal organs,
excretory system incl. bladder, vasc. extravasationexcretory
system incl. bladder, vasc. extravasation•• CT cystogram for
bladder injuryCT cystogram for bladder injury: 300: 300--400 cc of
400 cc of
20 cc of 60% contrast/500 cc of sterile saline20 cc of 60%
contrast/500 cc of sterile saline
-
CT IN BLUNT TRAUMA: BOWEL + MESENTERYCT IN BLUNT TRAUMA: BOWEL +
MESENTERY
• Bowel & mesenteric injuries are seen in 5% of blunt
abdominal trauma at laparoscopy
• Third most common type of injury
• Mechanism: • Direct force crushes GI tract
• Rapid deceleration -> shearing force between fixed and
mobile portions of GI tract
• Sudden increase in intraluminal pressure -> bursting
•• Bowel & mesenteric injuries are seen in 5% of Bowel &
mesenteric injuries are seen in 5% of blunt abdominal trauma at
laparoscopyblunt abdominal trauma at laparoscopy
•• Third most common type of injuryThird most common type of
injury
•• Mechanism:Mechanism: • • Direct force crushes GI tractDirect
force crushes GI tract
•• Rapid deceleration Rapid deceleration --> shearing force
between > shearing force between fixed and mobile portions of GI
tractfixed and mobile portions of GI tract
•• Sudden increase in intraluminal pressure Sudden increase in
intraluminal pressure --> > burstingburstingHughes Tm, Elton
C. The pathophysiology and management of bowel and mesenteric
injuries due to blunt trauma. Injury 2002; 33: 295-302.
-
COMMON SITES OF INJURY TO SBCOMMON SITES OF INJURY TO SB
• Proximal jejunum near ligament of Treitz• Distal ileum near
ileocecal valve• Mobile and fixed portions -> shear force
•• Proximal jejunum near ligament of TreitzProximal jejunum near
ligament of Treitz•• Distal ileum near ileocecal valveDistal ileum
near ileocecal valve•• Mobile and fixed portions Mobile and fixed
portions --> shear force> shear force
Hawkins AE, Mirvis SE. Evaluation of bowel and mesenteric
injury: role of multidetector CT. Abdominal Imaging 2003; 28:
505-514.
-
DX OF BOWEL & MESENTERIC INJURYDX OF BOWEL & MESENTERIC
INJURY
• Increased morbidity and mortality if dx delayed• Caused by
hemorrhage & peritonitis• Symptoms often nonspecific: pain•
With head + cord injuries: symptoms unreliable• Clinical assessment
alone: 40% negative lap.• Tests: peritoneal lavage, US and CT
•• Increased morbidity and mortality Increased morbidity and
mortality if dx delayedif dx delayed•• Caused by hemorrhage &
peritonitisCaused by hemorrhage & peritonitis•• Symptoms often
nonspecific: painSymptoms often nonspecific: pain•• With head +
cord injuries: symptoms unreliableWith head + cord injuries:
symptoms unreliable•• Clinical assessment alone: 40% negative
lap.Clinical assessment alone: 40% negative lap.•• Tests:
peritoneal lavage, US and CTTests: peritoneal lavage, US and CT
Fryer JP, Graham TL, Fong HM, Burns CM. Diagnostic peritoneal
lavage as an indicator for therapeutic surgery. Can J Surg 1991;
34: 471-46.7
-
TESTS FOR ABDOMINAL INJURIESTESTS FOR ABDOMINAL INJURIES
Talton DS, Craig MH, Hauser CJ, Poole GV. Major gastroenteric
injuries from blunt trauma. Ann Surg 1995: 61: 69-73. Dohlich
MOMcKenney MG, Varela JE, Compton RP, McKenney KL, Cohn SM. 2,576
ultrasounds for blunt abdominal trauma. J Trauma 2001;50: 108-112.
Liu A, et al. A computer-based simulator for peritoneal
lavage.Studies in Health Technology and Informatics. IOS Press,
2001;
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Peritoneal lavage:- 90% sensitivity for hemoperitoneum-
Insensitive for retroperitoneum- Perforation missed in up to 10%
(early)- Can compromise results with CT
Peritoneal lavage:Peritoneal lavage:-- 90% sensitivity for
hemoperitoneum90% sensitivity for hemoperitoneum-- Insensitive for
retroperitoneumInsensitive for retroperitoneum-- Perforation missed
in up to 10% (early)Perforation missed in up to 10% (early)-- Can
compromise results with CTCan compromise results with CT
-
TESTS FOR ABDOMINAL INJURIESTESTS FOR ABDOMINAL INJURIES
Talton DS, Craig MH, Hauser CJ, Poole GV. Major gastroenteric
injuries from blunt trauma. Ann Surg 1995: 61: 69-73.Dohlich MO,
McKenney MG, Varela JE, Compton RP, McKenney KL, Cohn SM. 2,576
ultrasounds for blunt abdominal trauma. J Trauma 2001; 50: 108-112.
Weekes AJ, Alteveer JG, Stahmer S. Emergency Us in trauma.
PowerPoint
Presentation.http://www.google.com/search?hl=en&q=ultrasound+in+emergency+room%2C+FAST%2C+images&btnG=Search&aq=f&oq=&aqi=
Ultrasound: FAST:- 86% sensitivity for free intra-abd. fluid-
98% specificity for free intra-abd. fluid- Nonspecific for organ
injury
Ultrasound: FAST:Ultrasound: FAST:-- 86% sensitivity for free
intra86% sensitivity for free intra--abd. fluidabd. fluid-- 98%
specificity for free intra98% specificity for free intra--abd.
fluidabd. fluid-- Nonspecific for organ injuryNonspecific for organ
injury
-
TESTS FOR ABDOMINAL INJURIESTESTS FOR ABDOMINAL INJURIES
• MDCT:- 69-95% sensitivity for bowel & mesenteric inj.-
94-100% specificity for bowel & mesenteric inj.- Time to
diagnosis significantly reduced- Less motion artifacts- Best
assessment of organs and vessels
Most important CT function: distinction between injuries that
require surgery from those treated conservatively
•• MDCT:MDCT:-- 6969--95% sensitivity for bowel & mesenteric
inj.95% sensitivity for bowel & mesenteric inj.-- 9494--100%
specificity for bowel & mesenteric inj.100% specificity for
bowel & mesenteric inj.-- Time to diagnosis significantly
reducedTime to diagnosis significantly reduced-- Less motion
artifactsLess motion artifacts-- Best assessment of organs and
vesselsBest assessment of organs and vessels
Most important CT function: Most important CT function:
distinctiondistinction between injuries between injuries that
require surgerythat require surgery from those from those treated
conservativelytreated conservatively
Scaglione M, Castelguidone EL, Scialpi M, et al. Blunt trauma to
the gastrointestinal tract and mesentery: is there a role for
helical CT? Eur J Radiol 2004: 50: 67-73.
! !! !
-
MDCT OFMDCT OF ABDOMINAL TRAUMA:ABDOMINAL TRAUMA:
MULTISYSTEMMULTISYSTEM
-
SIGNIFICANTSIGNIFICANT BOWEL/MESENTERIC INJURIESBOWEL/MESENTERIC
INJURIES
• Bowel Injuries:- Complete tear of bowel wall- Incomplete tear
that involves serosa and
muscularis but not mucosa
• Mesenteric Injuries:- Active mesenteric bleed- Disruption of
the mesentery- Mesenteric injury with bowel injury (ischemia)
•• Bowel Injuries:Bowel Injuries:-- Complete tear of bowel
wallComplete tear of bowel wall-- Incomplete tear that involves
serosa and Incomplete tear that involves serosa and
muscularis but not mucosamuscularis but not mucosa
•• Mesenteric Injuries:Mesenteric Injuries:-- Active mesenteric
bleedActive mesenteric bleed-- Disruption of the
mesenteryDisruption of the mesentery-- Mesenteric injury with bowel
injury (ischemia)Mesenteric injury with bowel injury (ischemia)
-
NONSIGNIFICANTNONSIGNIFICANT BOWEL/MESENTERIC
INJURIESBOWEL/MESENTERIC INJURIES
• Bowel Injuries:- Hematoma- Tear that involves serosa only
• Mesenteric Injuries:- Isolated mesenteric hematoma
•• Bowel Injuries:Bowel Injuries:-- HematomaHematoma-- Tear that
involves serosa onlyTear that involves serosa only
•• Mesenteric Injuries:Mesenteric Injuries:-- Isolated
mesenteric hematomaIsolated mesenteric hematoma
-
LOCATION OF BOWEL INJURIESLOCATION OF BOWEL INJURIES
• Stomach injury 5%• Duodenal injuries 11%• Jejunal injuries
25%• Cecum/ascending colon 7%• Transverse colon 11%• Descending
colon 2%• Sigmoid colon 5%• Multiple sites 34%
•• Stomach injuryStomach injury 5%5%•• Duodenal injuriesDuodenal
injuries 11%11%•• Jejunal injuriesJejunal injuries 25%25%••
Cecum/ascending colonCecum/ascending colon 7%7%•• Transverse
colonTransverse colon 11%11%•• Descending colonDescending colon
2%2%•• Sigmoid colonSigmoid colon 5%5%•• Multiple sitesMultiple
sites 34%34%Brofman N, Atri M, Epid D, Hanson JM, Grinblat L,
Chughtai T, Brenneman F. Evaluation of bowel and mesenteric blunt
trauma with MDCT. RadioGraphics 2006; 26: 1119-1131.
-
FINDINGS SPECIFIC TO BOWEL INJURYFINDINGS SPECIFIC TO BOWEL
INJURY
• Bowel discontinuity: 7% (4/54)• Extraluminal contrast
material: 6% (3/54)• Extraluminal air: 20% (11/54), high spec.•
Associated mesenteric features • Mesenteric foci of fluid or blood*
(interloop, triangular) • Fat stranding due to bowel injury
(streaky mesentery) • Retroperitoneal air (duodenum: air &
fluid/contrast
in anterior pararenal space); asc. & desc. colon)
•• Bowel discontinuityBowel discontinuity: 7% (4/54): 7%
(4/54)•• Extraluminal contrast material: 6% (3/54)Extraluminal
contrast material: 6% (3/54)•• Extraluminal air: 20% (11/54), high
spec.Extraluminal air: 20% (11/54), high spec.•• Associated
mesenteric featuresAssociated mesenteric features •• Mesenteric
foci of fluid or bloodMesenteric foci of fluid or blood**
(interloop, triangular)(interloop, triangular) •• Fat stranding due
to bowel injury (streaky mesentery)Fat stranding due to bowel
injury (streaky mesentery) •• Retroperitoneal air (duodenum: air
& fluid/contrast Retroperitoneal air (duodenum: air &
fluid/contrast
in anterior pararenal space); asc. & desc. colon) in
anterior pararenal space); asc. & desc. colon) Sentinel
clot!Sentinel clot!
-
SENTINEL CLOT SIGN FOR VISCERAL INJURYSENTINEL CLOT SIGN FOR
VISCERAL INJURY
SENSITIVITY 84%; 3 FP; sentinel clot the only sign in
14%SENSITIVITY 84%; 3 FP; sentinel clot the only sign in
14%SENSITIVITY 84%; 3 FP; sentinel clot the only sign in 14%Orwig
D, Federle MP. Localized clotted blood as evidence off visceral
trauma on CT: the sentinel clot sign. AJR 1989; 153-747-749.
-
• Mechanical ventilation• Pulmonary barotrauma• Peritoneal
lavage• Pneumothorax• Chest injury• Entry of air through fallopian
tubes• Intraperitoneal laceration of bladder (trauma or
due to cystography)• Pseudoperitoneum in abdominal wall
•• Mechanical ventilationMechanical ventilation•• Pulmonary
barotraumaPulmonary barotrauma•• Peritoneal lavagePeritoneal
lavage•• PneumothoraxPneumothorax•• Chest injuryChest injury••
Entry of air through fallopian tubesEntry of air through fallopian
tubes•• Intraperitoneal laceration of bladder (trauma or
Intraperitoneal laceration of bladder (trauma or
due to cystography)due to cystography)•• Pseudoperitoneum in
abdominal wallPseudoperitoneum in abdominal wallKane NM, Francis
IR, Burney RE, Wheatley MJ, Ellis JH, Korobkin Kane NM, Francis IR,
Burney RE, Wheatley MJ, Ellis JH, Korobkin M. Traumatic
pneumoperitoneum.M. Traumatic pneumoperitoneum.Implications of
computed tomography diagnosis. Invest Radiol 199Implications of
computed tomography diagnosis. Invest Radiol 1991; 26: 5741; 26:
574--578.578.
OTHER CAUSES: INTRAPERITONEAL AIR (78%)OTHER CAUSES:
INTRAPERITONEAL AIR (78%)
-
DUODENAL TRAUMADUODENAL TRAUMA
• Uncommon: only 1% of abdominal trauma• Direct compression of
duodenum against spine• Duodenal rupture (perf.) vs. intramural
hematoma • Rupture requires emergency surgery • Hematoma usually
treated conservatively
• Concomitant injuries may involve liver, pancreas, colon,
stomach and small bowel
•• UncommonUncommon: only 1% of abdominal trauma: only 1% of
abdominal trauma•• Direct compression of duodenum against
spineDirect compression of duodenum against spine•• Duodenal
rupture (perf.) vs. intramural hematomaDuodenal rupture (perf.) vs.
intramural hematoma •• Rupture requires emergency surgeryRupture
requires emergency surgery •• Hematoma usually treated
conservativelyHematoma usually treated conservatively
•• Concomitant injuries may involve liver, pancreas, Concomitant
injuries may involve liver, pancreas, colon, stomach and small
bowelcolon, stomach and small bowel
-
CT OF DUODENAL TRAUMACT OF DUODENAL TRAUMA
• Duodenal rupture: • Gas, water-density fluid, blood or
extravasated oral contrast in right anterior pararenal space•
Duodenal hematoma • Mass in duodenal wall due to a hematoma •
Obstructive symptoms within 48 hours of injury
• Both conditions • Duodenal wall thickening • Right anterior
space fluid or hemorrhage• Important to distinguish as management
differs!
•• Duodenal rupture:Duodenal rupture: •• Gas, waterGas,
water--density fluid, blood or extravasated oraldensity fluid,
blood or extravasated oral contrast in right anterior pararenal
spacecontrast in right anterior pararenal space•• Duodenal
hematomaDuodenal hematoma •• Mass in duodenal wall due to a
hematomaMass in duodenal wall due to a hematoma •• Obstructive
symptoms within 48 hours of injuryObstructive symptoms within 48
hours of injury
•• Both conditionsBoth conditions •• Duodenal wall
thickeningDuodenal wall thickening •• Right anterior space fluid or
hemorrhageRight anterior space fluid or hemorrhage•• Important to
distinguish as management differs!Important to distinguish as
management differs!
-
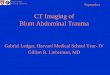
DUODENAL RUPTUREDUODENAL RUPTURE
Blood and water-density fluid in anterior pararenal space and
thick-walled duodenum (contusion)
Blood and waterBlood and water--density fluid in anterior
pararenal density fluid in anterior pararenal space space and
thickand thick--walled duodenum (contusion)walled duodenum
(contusion)
-
DUODENAL HEMATOMADUODENAL HEMATOMA
SENSITIVITY
-
FLUID IN INTRAFLUID IN INTRA-- OR EXTRAPERITONEAL SPACESOR
EXTRAPERITONEAL SPACES
• Hemorrhage• Leakage of bowel contents• Leakage of urine•
Pancreatic juice• Residual from peritoneal lavage
•• HemorrhageHemorrhage•• Leakage of bowel contentsLeakage of
bowel contents•• Leakage of urineLeakage of urine•• Pancreatic
juicePancreatic juice•• Residual from peritoneal lavageResidual
from peritoneal lavage
-
FINDINGS SPECIFIC TO MESENTERIC INJURYFINDINGS SPECIFIC TO
MESENTERIC INJURY
• Mesenteric extravasation• Specificity of 100%• Seen in 17%
(9/54)• Indication for urgent laparotomy
• Mesenteric vascular beading• Indicative of vascular injury•
Seen in 39% (21/54)
• Termination of mesenteric vessels• Abrupt termination of
mesenteric art.or veins• Seen in 35% (19/54), highly specific (1
FP)
•• Mesenteric extravasationMesenteric extravasation••
Specificity of 100%Specificity of 100%•• Seen in Seen in 17%17%
(9/54)(9/54)•• Indication for urgent laparotomyIndication for
urgent laparotomy
•• Mesenteric vascular beadingMesenteric vascular beading••
Indicative of vascular injuryIndicative of vascular injury•• Seen
in Seen in 39%39% (21/54)(21/54)
•• Termination of mesenteric vesselsTermination of mesenteric
vessels•• Abrupt termination of mesenteric art.or veinsAbrupt
termination of mesenteric art.or veins•• Seen in Seen in 35%35%
(19/54), highly specific (1 FP)(19/54), highly specific (1 FP)
-
FINDINGS LESS SPECIFIC TO BOWEL FINDINGS LESS SPECIFIC TO BOWEL
AND MESENTERIC INJURYAND MESENTERIC INJURY
• Bowel:• Bowel wall thickening:
- focal wall contusion- diffuse: overhydration or shock
bowel
• Abnormal bowel wall enhancement: - patchy or irregular
suggestive of full thickness injury
- absent or decreased -> ischemic bowel
•• Bowel:Bowel:•• Bowel wall thickeningBowel wall thickening:
:
-- focal wall contusionfocal wall contusion-- diffuse:
overhydration or shock boweldiffuse: overhydration or shock
bowel
•• Abnormal bowel wall enhancementAbnormal bowel wall
enhancement: : -- patchy or irregular suggestive of full patchy or
irregular suggestive of full thickness injurythickness injury
-- absent or decreased absent or decreased --> ischemic
bowel> ischemic bowel
-
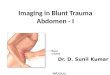
OVERHYDRATION & SHOCK BOWELOVERHYDRATION & SHOCK
BOWEL
OverhydrationOverhydrationOverhydration Shock bowel with liver
lacShock bowel with liver lacShock bowel with liver lac
-
FINDINGS LESS SPECIFIC TO BOWEL FINDINGS LESS SPECIFIC TO BOWEL
AND MESENTERIC INJURYAND MESENTERIC INJURY
• Mesentery• Mesenteric infiltration:
- Mesenteric injury with or without bowel injury; high
sensitivity; seen in 69%
- DDx: mesenteritis• Mesenteric hematoma:
- Laceration of mesenteric vessel- May not need surgery, if not
active bleed
• Bowel features (wall thickening & abnl. enh.) - Secondary
to mesenteric injury indicative
of vascular compromise; may be delayed!
•• MesenteryMesentery•• Mesenteric infiltration: Mesenteric
infiltration:
-- Mesenteric injury with or without bowel Mesenteric injury
with or without bowel injury; high sensitivity; seen in 69% injury;
high sensitivity; seen in 69%
-- DDx: mesenteritisDDx: mesenteritis•• Mesenteric hematoma:
Mesenteric hematoma:
-- Laceration of mesenteric vesselLaceration of mesenteric
vessel-- May not need surgery, if not active bleedMay not need
surgery, if not active bleed
•• Bowel features (wall thickening & abnl. enh.) Bowel
features (wall thickening & abnl. enh.) -- Secondary to
mesenteric injury indicative Secondary to mesenteric injury
indicative
of vascular compromise; may be delayed! of vascular compromise;
may be delayed!
-
COMMON FEATURES: BOWEL/MESENT. INJURIESCOMMON FEATURES:
BOWEL/MESENT. INJURIES
• Intraperitoneal & Extraperitoneal Fluid:- Intraperitoneal
fluid associated with
bowel/mesenteric injuries common (93%, 50/54)- Specificity low
because of other concomitant
injuries or pre-existing disease- Location:
- Retroperitoneal fluid -> retroperitoneal segmentof
bowel
- Retroperitoneal blood -> close to site of injury-
Hemoperitoneum + no parenchymal organ injury
= bowel or mesenteric injury
•• Intraperitoneal & Extraperitoneal Fluid:Intraperitoneal
& Extraperitoneal Fluid:-- Intraperitoneal fluid associated
with Intraperitoneal fluid associated with
bowel/mesenteric injuries common (93%, 50/54)bowel/mesenteric
injuries common (93%, 50/54)-- Specificity low because of other
concomitant Specificity low because of other concomitant
injuries or preinjuries or pre--existing diseaseexisting
disease-- Location: Location:
-- Retroperitoneal fluid Retroperitoneal fluid -->
retroperitoneal > retroperitoneal segmentsegmentof bowelof
bowel
-- Retroperitoneal blood Retroperitoneal blood --> close to
site of injury> close to site of injury
-- Hemoperitoneum + no parenchymal organ injury Hemoperitoneum +
no parenchymal organ injury = bowel or mesenteric injury= bowel or
mesenteric injury
-
COMMON FEATURES: BOWEL/MESENT. INJURIESCOMMON FEATURES:
BOWEL/MESENT. INJURIES
• Abdominal Wall Injury:
- Abdominal wall injury (e. g., seat belt injury = soft tissue
stranding, tear, hematoma) associated with
- Bowel or mesenteric injuries in 17% (9/54)
•• Abdominal Wall Injury:Abdominal Wall Injury:
-- Abdominal wall injury Abdominal wall injury (e. g., seat belt
(e. g., seat belt injury = soft tissue stranding, tear, injury =
soft tissue stranding, tear, hematoma) associated withhematoma)
associated with
-- Bowel or mesenteric injuries in 17% Bowel or mesenteric
injuries in 17% (9/54)(9/54)
-
DIAGNOSTIC PITFALLSDIAGNOSTIC PITFALLS
• Multiple injuries incl. liver/spleen• Large size of patients•
Metallic monitoring devices• Arms in imaging field• Chaotic scene
at imaging site
•• Multiple injuries incl. liver/spleenMultiple injuries incl.
liver/spleen•• Large size of patientsLarge size of patients••
Metallic monitoring devicesMetallic monitoring devices•• Arms in
imaging fieldArms in imaging field•• Chaotic scene at imaging
siteChaotic scene at imaging site
-
SENSITIVITY & SPECIFICITY IN DIAGNOSING SENSITIVITY &
SPECIFICITY IN DIAGNOSING SURGICALLY SURGICALLY IMPORTANT
BOWEL/MESENTERIC INJURYIMPORTANT BOWEL/MESENTERIC INJURY
Bowel wall defect 11 100 *Extraluminal contrast 8 100
*Intraperitoneal air 24 95Thick large bowel wall 18 97 *Thick small
bowel wall 45 76Retroperitoneal air 5 98Abnormal bowel enhanc. 8
90Positive (negative) Likelihood ratio useful * *
Bowel wall defectBowel wall defect 1111 100 100 **Extraluminal
contrastExtraluminal contrast 88 100 100 **Intraperitoneal
airIntraperitoneal air 2424 9595Thick large bowel wallThick large
bowel wall 1818 97 97 **Thick small bowel wallThick small bowel
wall 4545 7676Retroperitoneal airRetroperitoneal air 55
9898Abnormal bowel enhanc.Abnormal bowel enhanc. 88 9090Positive
(Positive (negativenegative) Likelihood ratio useful * ) Likelihood
ratio useful * **
Atri M, et al. Surgically important bowel and/or mesenteric
injury in blunt trauma: accuracy of MDCT for evaluation.Radiology
2008; 249: 524-533.
SignSign Sensitivity (%) Specificity (%)Sensitivity (%)
Specificity (%)
-
SENSITIVITY & SPECIFICITY IN DIAGNOSING SENSITIVITY &
SPECIFICITY IN DIAGNOSING SURGICALLY SURGICALLY IMPORTANT
BOWEL/MESENTERIC INJURYIMPORTANT BOWEL/MESENTERIC INJURY
Retroperitoneal fluid 37 52Mesenteric vessel beading 50 95
*Abrupt mes. vessel term. 45 93 *Mesenteric vessel extrav. 26 100
*Focal mesenteric hematoma 45 90Mesenteric air 21 95Intraperitoneal
fluid 100 26 *Mesenteric fluid +/or strand. 84 66
Retroperitoneal fluidRetroperitoneal fluid 3737 5252Mesenteric
vessel beadingMesenteric vessel beading 5050 95 95 **Abrupt mes.
vessel term.Abrupt mes. vessel term. 4545 93 93 **Mesenteric vessel
extrav.Mesenteric vessel extrav. 2626 100 100 **Focal mesenteric
hematomaFocal mesenteric hematoma 4545 9090Mesenteric airMesenteric
air 2121 9595Intraperitoneal fluidIntraperitoneal fluid 100100 26
26 **Mesenteric fluid +/or strand.Mesenteric fluid +/or strand.
8484 6666
Atri M, et al. Surgically important bowel and/or mesenteric
injury in blunt trauma: accuracy of MDCT for evaluation.Radiology
2008; 249: 524-533.
SignSign Sensitivity (%) Specificity (%)Sensitivity (%)
Specificity (%)
-
CONCLUSIONS: BOWEL/MESENTERIC INJURYCONCLUSIONS:
BOWEL/MESENTERIC INJURY
• Recognize significant bowel/mesenteric injuries• CT signs of
significant injuries: • Bowel wall defect • Free air
(intraperitoneal, retroperitoneal or mesenteric) • Intraperitoneal
bowel contrast material • Extravasation of contrast from mesenteric
vessels • Evidence of bowel infarct
• CT signs: high specificity, low sensitivity!
•• Recognize significant bowel/mesenteric injuriesRecognize
significant bowel/mesenteric injuries•• CT signs of CT signs of
significant injuriessignificant injuries:: •• Bowel wall
defectBowel wall defect •• Free air (intraperitoneal,
retroperitoneal or mesenteric)Free air (intraperitoneal,
retroperitoneal or mesenteric) •• Intraperitoneal bowel contrast
material Intraperitoneal bowel contrast material •• Extravasation
of contrast from mesenteric vesselsExtravasation of contrast from
mesenteric vessels •• Evidence of bowel infarctEvidence of bowel
infarct
•• CT signs: CT signs: high specificity, low sensitivity!high
specificity, low sensitivity!
-
CONCLUSIONS: BOWEL/MESENTERIC INJURYCONCLUSIONS:
BOWEL/MESENTERIC INJURY
Signs for injury needing surgery:
• Mesenteric hematoma combined with bowel thickening
• Significant amount of free fluid without solid organ
injury
Signs for injury needing surgery:Signs for injury needing
surgery:
•• Mesenteric hematoma combined with bowel Mesenteric hematoma
combined with bowel thickeningthickening
•• Significant amount of free fluid without solid Significant
amount of free fluid without solid organ injuryorgan injury
-
CONCLUSIONS: MESENTERIC INJURYCONCLUSIONS: MESENTERIC INJURY
• Two additional useful signs for mesenteric injury:• Mesenteric
vascular beading• Abrupt termination of mesenteric vessels
• Both with high specificity and more frequently seen than
mesenteric extravasation
•• Two additional useful signs for mesenteric injury:Two
additional useful signs for mesenteric injury:•• Mesenteric
vascular beadingMesenteric vascular beading•• Abrupt termination of
mesenteric vesselsAbrupt termination of mesenteric vessels
•• Both with high specificity and more frequently Both with high
specificity and more frequently seen than mesenteric
extravasationseen than mesenteric extravasation
-
CONCLUSIONS: BOWEL/MESENTERIC INJURYCONCLUSIONS:
BOWEL/MESENTERIC INJURY
• Nonspecific features of significant bowel or mesenteric
injury:
• Decision for surgery depends on clinical judgment• Reevaluate
with CT within 6-8 hours
• MDCT negative for bowel and/or mesenteric injury -> CT
screening tool to discharge a patient
•• Nonspecific features of significant bowel or Nonspecific
features of significant bowel or mesenteric injury:mesenteric
injury:
•• Decision for surgery depends on clinical judgmentDecision for
surgery depends on clinical judgment•• Reevaluate with CT within
6Reevaluate with CT within 6--8 hours8 hours
•• MDCT negative for bowel and/or mesenteric MDCT negative for
bowel and/or mesenteric injury injury --> CT screening tool to
discharge a patient> CT screening tool to discharge a
patient