Embed Size (px)
Citation preview

Improving breastfeeding rates in Neonatal Abstinence Syndrome
infants in the NICU
Donna Garey MD MPH
Lisa Stellwagen MD
UC San Diego Medical Center
Division of Neonatology
January 2015

FACULTY DISCLOSURE INFORMATION
Lisa Stellwagen MD
I have a relevant financial relationship to disclose:
Medela, Inc: speaker
Donna Garey MD MPH
I have a relevant financial relationship to disclose:
none

Objectives
• Identify current evidence based reasons to encourage
breastfeeding of the Neonatal Abstinence Syndrome
(NAS) infant
• Identify what concrete steps can be implemented to
improve breastfeeding rates at discharge in the NAS
infant
• Learn the what is currently known about the effects of
Marijuana during pregnancy and lactation, and then be
able to accurately counsel mothers on this issue

Neonatal Abstinence Syndrome
(NAS)
• Due to abrupt discontinuation of
chronic exposure to opioids in utero
• Generalized multi-system disorder
• Incidence of NAS increasing around
the US

Date of download: 1/27/2015 Copyright © 2015 American Medical
Association. All rights reserved.
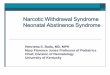
From: Neonatal Abstinence Syndrome and Associated Health Care Expenditures: United States, 2000-2009
JAMA. 2012;307(18):1934-1940. doi:10.1001/jama.2012.3951
Error bars indicate 95% CI. P for trend < .001 over the study period. The unweighted sample sizes for mothers diagnosed with and
without antepartum opiate use are 987 and 833 494 in 2000; 1058 and 849 133 in 2003; 2160 and 879 910 in 2006; and 4563 and
816 554 in 2009; respectively.
Figure Legend:

Date of download: 1/27/2015 Copyright © 2015 American Medical
Association. All rights reserved.
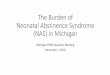
From: Neonatal Abstinence Syndrome and Associated Health Care Expenditures: United States, 2000-2009
JAMA. 2012;307(18):1934-1940. doi:10.1001/jama.2012.3951
NAS indicates neonatal abstinence syndrome. Error bars indicate 95% CI. P for trend < .001 over the study period. The unweighted
sample sizes for rates of NAS and for all other US hospital births are 2920 and 784 191 in 2000; 3761 and 890 582 in 2003; 5200
and 1 000 203 in 2006; and 9674 and 1 113 123 in 2009; respectively.
Figure Legend:

NAS Timeline
NAS. Pediatrics. Kocherlakota. 2014

Opiates
• Mimic natural endogenous endorphins at and receptors on the neuronal cell membrane
• Block transmission of noxious stimuli from the periphery to the spinal cord
• Develop tolerance to analgesia, sedation, and euphoria
• Cross the placenta – Lipophilic, low molecular
weight compounds

Heroin • -opioid receptor agonist
• Approx 40-80% of infants have NAS
• Earlier onset and shorter withdrawal
– Onset of withdrawal symptoms at 24 to 48
hours
– Duration of withdrawal is 8-10 days

Prescription Narcotics
• Long-Acting Opioids – Fentanyl Transdermal Patch
– Oxymorphone or Oxycodone
hydrochloride extended-release
– Morphine sulfate extended-release
• Short-Acting Opioids – Hydrocodone
– Oxycodone
– Tramadol
– Fentanyl (IV) or Morphine (IV)
– Codeine
– Hydromorphone
• Frequency of NAS
depends on amount
and duration of
maternal use
• Onset and duration of
withdrawal depends on
half-life of the drug
• Approx 5-20%
experience NAS

Treatment for opioid addiction
Methadone
• -opioid receptor agonist
• Half Life 23-48 hours
• Typical dose is 20 to 120
mg per day
• Mean hospital stay for NAS
– 17.5 days
• Later onset and longer
withdrawal
Buprenorphine
• partial -opioid agonist
• Half-life 26-34 hours
• Mean hospital stay for NAS
– 10 days
• Later onset and longer
withdrawal
Minimal relationship between maternal
opioid dose and NAS.

Buprenorphine +/- Naloxone • Synthetic opioid receptor agonist
• Prescribed in a doctor’s office by qualified MD
• Available formulations:
– Tablets - 2 and 8 mg tablets
– Sublingual film - 2-4-8-12 mg
– Patch form for chronic pain
• Less respiratory depression than other narcotics
– Can cause coma/death if combined with benzos, alcohol, other respiratory
depressants
• Shorter duration of NAS

Onset, Duration, and Frequency of NAS
Opioids Onset
(hours)
Frequency
(%)
Duration
(days)
Heroin 24-48 40-80 8-10
Prescription
Opioids
36-72 5-20 10-30
Buprenorphine 36-60 22-67 Up to 28 or
more
Methadone 48-72 13-94 Up to 30 or
more

Infants Admitted for Observation for Neonatal Abstinence Syndrome
Admit to NICU:
NAS (Finnegan score) q 4 hr.
Implement non-pharmacologic
therapies
Observation and Monitoring:
NAS < 8 continue to monitor until safe for
discharge
NAS >8 times 2 implement therapy
Observation Period:
• Short acting prescription narcotics: 4 days
• Benzo + opiates: 4-7 days
• Heroin/methadone: 5-7 days
• Suboxone: 5-6 days

Why treat maternal drug abuse and neonatal withdrawal?
• Decreases illicit drug use
• When combined with good obstetrical care improves fetal
outcomes
• Avoids complications of NAS such as seizures and
dehydration due to poor feeding, vomiting, and diarrhea.
• Allows infant to have normal feeding and infant
interactions.

Risk Factors for Increased Severity/Intensity of NAS
• Term
• Polydrug abuse
• Combination with benzodiazepines
• Specific gene polymorphisms of the -opioid receptor
(OPRM1) and catechol-O-methyltransferase (COMT)
• Smoking
• Methadone
• Combination with SSRIs

Withdrawal in Preterm Infants
• Decreased intensity and severity
– Decreased cumulative exposure
– Decreased transmission across placenta in
early gestation
– Decreased receptor development and
sensitivity
– Decreased fatty tissues
• Methadone accumulates in fatty tissues

Modified Finnegan
Zimmerman-Baer U, et al. Addiction. 2010.

Infants Admitted for Observation for Neonatal Abstinence Syndrome
Admit to NICU:
NAS (Finnegan score) q 4 hr.
Implement non-pharmacologic therapies
Observation and Monitoring:
NAS < 8 continue to monitor until
safe for discharge
NAS >8 times 2 implement therapy
Observation Period:
• Short acting prescription narcotics: 4 days
• Benzo + opiates: 4-7 days
• Heroin/methadone: 5-7 days
• Suboxone: 5-6 days

CNS Signs and Symptoms

Excessive High Pitched Cry
Scored infants 30 – 60
minutes after a feed.
If the infant requires rocking
to quiet during this time.
Their cry is considered
prolonged.
If infant’s cry is high
pitched at its peak even
though it is not prolonged –
score 2.
If cry is high pitched
throughout, or if crying is
prolonged, even if not high
pitched – score 3.

Increased muscle tone
Score if excessive or
above-normal muscle
tone.
For instance: no head lag
when being pulled to a
sitting position or tight
flexion of the infant’s
arms and legs.

Moro Reflex
If the infant exhibits
pronounced jitteriness
(rhythmic tremors that are
symmetrical and involuntary) of
the hands during or at the end
of a Moro reflex – score 2.
If jitteriness and clonus
(repetitive involuntary jerks) of
the hands and/or arms are
present during or after a Moro
– score 3.

Myoclonic jerks
Score if involuntary muscular
contractions which are
irregular and exceedingly
abrupt (usually involving a
single muscle group) are
observed.

Tremors
Mild, Moderate, and Severe
Disturbed or Undisturbed
Undisturbed means that the
baby is either sleeping or at
rest in its bed.

Seizures
Most commonly seen as tonic
extensions of all limbs.
Unusual limb movements may
accompany a seizure. In the
upper limbs these often
resemble swimming or rowing
in the lower limbs, they
resemble pedaling or bicycling.
Other subtle signs may include
staring, rapid involuntary eye
movement, chewing, back
arching, and fist clenching.
Occurs in 2-11% of infants with NAS

Gastrointestinal Signs and Symptoms

Excessive Sucking
Score if hyperactive or
disorganized sucking,
increased rooting reflex.

Loose/watery stools
Score if loose (curds/seedy
appearance) or watery stools
(water ring on nappy around
stool) are observed.
Score if at least one episode
of regurgitation is observed.
Vomiting

Poor Feeding
Score if the infant
demonstrates excessive
sucking prior to feeding,
yet sucks infrequently
during a feeding, taking a
small amount; and/or
demonstrates an
uncoordinated sucking
reflex.

Respiratory and Vasomotor Signs and Symptoms

Respiratory Rate
Score 1 only if respirations
are >60/min in the
absence of lung or airway
disease.
Score 2 only if respirations
are >60/min and
retractions are present in
the absence of lung or
airway disease

Nasal Stuffiness
Score if the infant sounds
congested; mucous may
be visible
Score if more than three
sneezes are noted within
the scoring interval
Sneezing

Yawning
Score if more than 3
yawns are observed within
the scoring interval.

Sweating
Score if sweating is
spontaneous and not due to
excessive clothing or high
room temperature.

Hyperthermia
Temperature should be
taken per axilla.
Mild pyrexia is an early
indication of heat
produced by increased
muscle tone and tremors.
Usually less than 102
Frequent low grade temp

Mottling
Score if mottling is
present on the infant’s
chest, trunk, arms, or
legs.

Non-pharmacologic Adjunct Therapy
• Swaddling
• Settling
• Rocking
• Decrease outside
stimulation/white noise
• Massage
• Relaxation Baths
• Pacifiers

Pharmacologic Treatment
Half-life
(hours)
Advantages Disadvantages
Morphine 9 Shorter weaning
course
Frequent doses
Constipation
Methadone 26 Long half-life Longer weaning
course
Phenobarbital 45-100 Long half-life Sedation
Possible
apoptosis
Clonidine 44-72 No sedation Hypotension,
Rebound
hypertension

Adjunct Pharmacotherapy
• Phenobarbital
– Binds to the GABA receptor, improving the effect of GABA by extending GABA-mediated chloride channel openings which permits an increasing flow of chloride ions across the membrane, causing neuronal hyperpolarization (e.g., membrane inhibition to depolarization).
– Does not treat gastrointestinal symptoms
• Clonidine
– Central acting alpha-adrenergic receptor agonist
– Stimulates presynaptic adrenergic receptor thus inhibiting CNS sympathetic outflow and reducing norepinephrine
– Treats autonomic over activity - tachycardia, hypertension, restlessness, and diarrhea, sweating

Previous Pharmacologic Therapies
• Tincture of opium
– Very concentrated - small error in dosing leads to significant
overdose
– Contains 19% ethanol
– Does not control diarrhea
– No longer recommended
• Paregoric
– Contains anhydrous morphine
– Also contains camphor, 44% ethanol, anise oil, benzoic acid, and
glycerin
– No longer recommended due to other toxic ingredients

Neonatal Abstinence Syndrome
(NAS): Standardizing Management,
Promoting Breastfeeding, and
Improving Communication University of California San Diego
NICU Quality Improvement Team
Donna Garey, MD, MPH
Lisa Stellwagen, MD
Mary Ekno, BSN, RNC-NIC
Alicia Somers, PharmD
Poster Session and Podium Presentation

Specific Aims
• Decrease median LOS for infants with NAS
from 95 days to 30 days by September 2014
• Increase any human milk exposure in infants (with no
contraindications)
from 50% to 75% by December 2014
• Increase human milk at discharge
from 0% to 25% by December 2014

Settings and Methods
• Level III regional NICU
– 2,500 deliveries and 700 admissions per year
– Infants requiring NAS treatment are admitted to the NICU
• Chart review of infants treated for NAS
– May to July 2012 (before internal QI project)
– Sept to Nov 2013 (VON Day Quality Audit 1)
– June to Sept 2014 (VON Day Quality Audit 2)
• Data collected
– Based on the VON Day Quality Audits
– Additional data on Breastfeeding (BF)

Interventions/PDSA Cycles • Optimizing Care Team
– Hospitalist Service
• Coordination with maternal outpatient providers
– 2:1 Nursing ratios
– Finnegan nursing superusers
• Provider education
– VON iNICQ Core Webinars
• Revised policy/algorithm on Initial Management at risk for NAS
– Included initial breastfeeding management
• Monthly QI Task Force meetings
– Multidisciplinary involvement

In Utero Exposures
Risk for Neonatal Abstinence Syndrome
Exposure to long-acting
narcotics (see list below)
Admit to NICU
Exposure to multiple agents such as short-acting
narcotics in addition to benzodiazepines,
antipsychotics, nicotine, etc.
Admit to NICU
Not at risk/low risk for Neonatal Abstinence Syndrome
Exposure to methamphetamines
or THC
Admit to couplet care*
Exposure to short-acting narcotics without
multiple exposures
Admit to couplet care and observe for 4 days.
(No NAS Scoring by nursing) Call MD to assess if concern
for opioid withdrawal.
Exposure to antipsychotics, antidepressants (ie SSRIs), and
other medications.
Admit to couplet
care
*A positive maternal toxicology screen for THC and/or amphetamines can’t be used as an indication to legally
separate a mother from her well newborn. These infants can only be separated from mother after a CPS hold has
been placed.
Breastfeeding
Permitted for almost all mothers/infants at admission to FMCC or NICU.
Continued breastfeeding will be determined by medical team.
Contraindications to breastfeeding are positive HIV status, medications that are
Category L5, or confirmed on-going illegal drug use.
Long-Acting Opioids Fentanyl Transdermal Patch
Methadone Buprenorphine (Butrans, Subutex)
Oxymorphone hydrochloride extended-release (Opana) Oxycodone hydrochloride controlled-release (Oxycontin) Morphine sulfate extended-release (Oramorph, Kadian)
Short-Acting Opiods
Hydrocodone and Hydrocodone+APAP (Vicodin, Norco) Oxycodone+APAP (Percocet) or oyycodone IR
Tramadol Fentanyl (IV) or Morphine (IV)
Codeine Hydromorphone (Dilaudid)

Infants Admitted for Observation for Neonatal Abstinence Syndrome
Admit to NICU:
NAS (Finnegan score) q 4 hr.
Implement non-pharmacologic therapies
Observation and Monitoring:
NAS < 8 continue to monitor until safe for
discharge
NAS >8 times 2 implement therapy
Observation Period:
• Short acting prescription narcotics: 4 days
• Benzo + opiates: 4-7 days
• Heroin/methadone: 5-7 days
• Suboxone: 5-6 days

NAS Patient Characteristics and Outcomes
NAS Patient
Characteristics and Outcomes
2012 (May-July) n=4
2013 (Sept-Nov) n=6
2014 (June-Sept) n=6
Length of Stay(days) Median
94.5 31.5 32
DC on Meds 100% 67% 40%
Any BM 50% 67% 67%
BM at discharge 0% 17% 50%
Reason no BM at dc In treatment,
counseled to stop(3)
HIV positive (1)
Incarcerated (3)
In treatment,
relapse (2)
Incarcerated (2) Not provided (1)

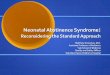
Any Breastmilk(%) by Month Admitted
Breastmilk at Discharge (%) by Month Admitted
Median
Goal
0
10
20
30
40
50
60
70
80
90
100
Ma
y-
12
Jul-1
2
Se
p-
13
Nov-
13
Ma
y-
14
Au
g-
14
%

Summary/Key to Success
• Multidisciplinary involvement – Nursing and SW champions
– Updating policy to standardize initial management in L&D, couplet care, and NICU
• Continuity of care – Hospitalist service
– Coordination with outpatient maternal treatment providers
• Monthly QI task force meetings – Kept leadership informed and involved

Breastfeeding in the NAS infant
• BF benefits of specific
interest to NAS infant
• Review narcotic
transfer in MBM
• What had we tried?
• What worked this
time?

Benefits of breastmilk for the newborn that may be of specific significance to the NAS infant
• Reduction in SIDS
• Significant reduction in infections in
childhood
• Improved maternal-child bonding
• Decreased risk of neglect
• Modified NAS symptoms/ length of
hospital stay

Dose response for beneficial effects of breastfeeding
AAP Breastfeeding and the use of human milk. Pediatrics 2012
Condition Lower risk
Otitis Media 50%
Pneumonia 77%
Asthma 27%
RSV bronchiolitis 74%
NEC 77%
Eczema 27%
Gastroenteritis 64%
Inflammatory bowel
disease
31%
Obesity 24%
Celiac disease 52%
Type 1 diabetes 30%
Type 2 diabetes 40%
SIDS 73%

Does breastfeeding protect against substantiated child abuse and neglect? A 15-year cohort study.
• 5890 Australian mother-infant pairs followed for 15 yrs
• 512 children with maltreatment reports
• 4.3% had >1 episode of maternal maltreatment
• Assessed no BF (21%), < 4 mos (39%), > 4mos (40%)
• No association with BF and non-maternal maltreatment
• 2.6 times higher risk of maternal maltreatment for non-BF children
• Maternal neglect was the only type of maltreatment associated with
BF duration
• Their conclusions: ‘among other factors, breastfeeding may help to
protect agains maternally perpetrated child maltreatment, particularly
child neglect’
Strathearn et al. Pediatrics 2009

Breastfeeding reduces the need for withdrawal treatment in opioid-exposed infants
• 124 women in narcotic treatment (methadone and
buprenorphine) and their infants (in Norway)
• High rates of BF 77%, but also high rates of early weaning
• Breastfed infants exposed to methadone prenatally had
less need for opioid treatment (53% vs 80%)
• This effect was not significant for buprenorphine (64% vs
44%)
• For those that were treated, length of treatment was
shorter for those who were breastfeed (27 d vs 47 d)
Welle-Strand et al. Acta Paediatrica 2013

What national metrics are there to support BF in the NAS population?
• ABM
• AAP
• VON network
• LactMed
• MotherRisk
• Thomas Hale

Thomas Hale, Medications and Mother’s Milk 2014
PEDIATRICS Vol. 132 2013 pp. e796 -e809
RID: relative infant dose =
Dose: infant mg/kg/day
____________________
Dose: mother mg/kg/day
If RID <10% considered safe for baby

U.S. National Library of Medicine TOXNET Data Network: LactMed 2015 Methadone
• Mother on methadone maintenance has about 1-3 % of
her weight adjusted methadone in her milk (safe level <
10%)
• Highest levels are about 1/3 baby treatment dose
• Peak levels occur 4-6 hours after maternal dose
• BF may reduce NAS symptoms and LOS in baby
• Abrupt weaning may lead to symptom increase in baby
• ‘Women who received methadone maintenance during
pregnancy and are stable should be encouraged to
breastfeed their infants postpartum’

U.S. National Library of Medicine TOXNET Data Network: LactMed 2015 Buprenorphine
• Achieves low levels in breastmilk about 1.4-2.4% maternal
weight adjusted dose
• Poor oral absorption by infant
• Low infant blood levels
• Infant dose unlikely to aide in NAS symptoms
• However infants have developed NAS with rapid BF
cessation
• ‘women who received buprenorphine for opiate abuse
during pregnancy and are stable should be encouraged to
breastfeed their infants postpartum’

Breastfeeding and the use of human milk AAP Policy Statement 2012
Maternal substance abuse is not a categorical
contraindication to breastfeeding. Adequately nourished
narcotic-dependent mothers can be encouraged to
breastfeed if they are enrolled in a supervised methadone
maintenance program and have negative screening for HIV
and illicit drugs.96
PEDIATRICS Vol. 129 2012 pp. e827 -e841

From the American Academy of Pediatrics Clinical Report
The Transfer of Drugs and Therapeutics Into Human Breast Milk: An Update
on Selected Topics
• Potential adverse effects on breastfeeding infants from methadone (according
to product labeling) and buprenorphine include lethargy, respiratory difficulty,
and poor weight gain.52 The long-term effects of methadone in humans are
unknown. Nonetheless, methadone levels in human milk are low, with
calculated infant exposures less than 3% of the maternal weight-adjusted
dose.53,54 Plasma concentrations in infants are also low (less than 3% of
maternal trough concentrations) during the neonatal period and up to 6 months
postpartum.55,56 For these reasons, guidelines from the Academy of
Breastfeeding Medicine encourage breastfeeding for women treated with
methadone who are enrolled in methadone-maintenance programs.48
• Transferred amounts of methadone or buprenorphine are insufficient to prevent
symptoms of neonatal abstinence syndrome.49,60 Neonatal abstinence
syndrome can occur after abrupt discontinuation of methadone.51,61 Thus,
breastfeeding should not be stopped abruptly, and gradual weaning is advised
if a decision is made to discontinue breastfeeding.
PEDIATRICS Vol. 132 2013 pp. e796 -e809

Academy of Breastfeeding Medicine 2009 ABM Clinical Protocol #21: Guidelines for breastfeeding and the drug-dependent woman
• Women engaged in substance abuse treatment who have provided their
consent to discuss progress in treatment and plans for postpartum treatment
with substance abuse treatment counselor
• Women whose counselors endorse that she has been able to achieve and
maintain sobriety prenatally; counselor approves of client’s plan for
breastfeeding
• Women who plan to continue in substance abuse treatment in the postpartum
period
• Women who have been abstinent from illicit drug use or licit drug abuse for 90
days prior to delivery and have demonstrated the ability to maintain sobriety in
an outpatient setting
• Women who have a negative maternal urine toxicology testing at delivery
except for prescribed medications
• Women who received consistent prenatal care
• Stable methadone-maintained women wishing to breastfeed should be
encouraged to do so regardless of maternal methadone dose.

MotherRisk website (Dr Gideon Koren)
• Heroin toxicity has been observed in infants breastfed by mothers
abusing heroin, but at therapeutic doses, most opioids, such as
morphine, meperidine, methadone, and codeine, are excreted into
milk in only minimal amounts18,19 and are compatible with
breastfeeding.
http://www.motherisk.org

Medications and Mother’s Milk 2014 Thomas W Hale, PhD & Hilary E Rowe PharmD
• Buprenorphine: L2 ‘no evidence that the use of this drug
will have an adverse effect in the breastfed infant’
• Buprenorphine + Naloxone: L3 ‘probably compatible with
breastfeeding’
• Methadone: L2 ‘averages 2.8% of the maternal dose…the
amount in milk is insufficient to prevent neonatal
withdrawal syndrome’

UCSD breastmilk and maternal medication policy 2011
• Despite being Baby Friendly since 2006 with BF rates of 95%...
• We were not consistent about who could and could not BF
• Different rules for NICU and well baby unit
• OB and Peds not on the same page
• Policy written and maternal handouts made
• Party line was to be: anything taken in pregnancy is safe for early
breastfeeding
• All mothers encouraged to BF (except HIV+, very few contraindicated
medications/combinations)
• Pediatric medical team would sort out feeding plan after birth
• But policy not adhered to
• Methadone mothers in particular were told not to BF

1
UCSD Medical Center: WOMEN & INFANT SERVICES
POLICY/PROCEDURE TITLE:
BREASTMILK: DRUGS OF ABUSE, NARCOTICS AND USE OF HUMAN MILK
RELATED TO:
Medical Center Policy (MCP) Nursing Practice Stds.
JCAHO Patient Care Stds.
QA Other
Title 22
ADMINISTRATIVE CLINICAL PAGE 1 OF _
Effective date: 1/11 Revision date:
Review date:
Unit/Department of Origin: ISCC, FMCC Other Approval: Newborn Management, ISCC Core Group &
Perinatal Practices 1/11
KEY ELEMENTS:
1. Drugs of abuse are known to have potential for risk to the young or premature infant
2. Infants gain benefit from early exposure to their mother’s milk
3. Most medications used by mothers result in very low levels of drug exposure in human milk
4. Straightforward unit policy will help to extend human milk benefits to all infants and clarify to mothers their role in the health of their infant
5. Support of the mother/infant couplet at risk for substance abuse is a priority in our unit
POLICY STATEMENT:
1. All mothers will be asked about medication use in pregnancy 2. Mothers that use narcotics under a physicians order for chronic pain are, in general, allowed
to breastfeed
3. Mothers with known or suspected street drug or alcohol use will be given the benefit of the
doubt, educated about providing safe milk for their infant, and followed closely 4. There is no need to discard milk, test the milk, or have the mother refrain from
breastfeeding
PROVIDER:
RN, NP, MD
EQUIPMENT:
PROCEDURE:
1. The pediatric medical team will review mother’s history, consult with pharmacy and standard tertiary references (e.g. LactMed, Medications and Mother's Milk), to make an assessment
of the breastfeeding safety of a mother’s medications
2. Maternal chart will be reviewed for history of drug use, recent toxicology screening, and time of last positive toxicology test
3. NICU/FMCC social worker will evaluate mothers with a drug or alcohol history re: willingness
to abstain from substance abuse and to provide expressed breastmilk or breastfeed the infant
4. Mothers with known or suspected drug or alcohol history will be given handout on ‘Providing
safe milk for your baby’



Why were we non-compliant with our own policy?
• Policy in place, but not followed
• Consultant for NAS infants told mothers not to BF
• Staff believed
– methadone in milk made baby hard to wean
– most mothers were not staying clean
– that rapid discontinuation of breastfeeding could precipitate significant risk
for baby
– that maternal dose over 90 mg of methadone made breastfeeding
dangerous
• Mothers are tested weekly during pregnancy, but not routinely after delivery
• We had no information about mother’s compliance with her methadone clinic
• We did not weight the benefits to baby of human milk against the risks of not
breastfeeding

As we worked to improve our NAS policy, we incorporated new BF guidelines
• Neonatologists all agreed on new guidelines
• Reaffirmed our policy
• Clarified the tiny amount of methadone in mother’s milk
• Additional rules to address concerns
• Arranged MD-to-MD contact with mother’s methadone clinic
• Clinic asked to test mother every week and call us if tox+
• Encouraged staff to consider the great benefit to the baby of breastmilk
• Presented BF as part of our treatment of baby.
• Encouraged parents to stay with baby, do skin to skin and breastfeed as part of non-pharmacologic management of NAS

Complicating factors:
• A high number of these mothers smoke cigarettes which
can make withdrawal more difficult and add risk to infant
(of SIDS, otitis media)
• Mothers who are incarcerated have much difficulty in
pumping and getting their milk to baby
• Mothers with narcotic addiction may relapse
• Mothers who are not clean often will not provide
breastmilk- this was the first sign of relapse.

New version of NAS policy regarding breastmilk The role of breastfeeding in the setting of neonatal abstinence syndrome is controversial. For mothers on a stable maintenance methadone regimen, breastfeeding may reduce length of stay, though care must be taken in weaning from mother’s own milk. Recommendation regarding which women should be allowed to breastfeed in this scenario from the Academy of Breastfeeding Medicine (2009):
•Women engaged in substance abuse treatment who have provided their consent to discuss progress in treatment and plans for postpartum treatment with substance abuse counselors
•Women whose counselors endorse that she has been able to achieve and maintain sobriety prenatally; counselor approves of client’s plan for breastfeeding
•Women who plan to continue in substance abuse treatment in the postpartum period
•Women who have been abstinent from illicit drug use or licit drug abuse for 90 days prior to delivery and have demonstrated the ability to maintain sobriety in an outpatient setting
•Women who have a negative maternal toxicology testing at delivery except for prescribed medications
•Women who received consistent prenatal care
•Women who do not have HIV or other contraindications to breastfeeding
•Women who are not taking a psychiatric medication that is contraindicated in lactation
•Stable methadone-maintained women wishing to breastfeed should be encouraged to do so regardless of maternal methadone dose
•Women and their partners should be fully informed about the risk of rapid weaning from the breast or exposure to street drugs during lactation

In Utero Exposures
Risk for Neonatal Abstinence Syndrome
Exposure to long-acting
narcotics (see list below)
Admit to NICU
Exposure to multiple agents such as short-acting
narcotics in addition to benzodiazepines,
antipsychotics, nicotine, etc.
Admit to NICU
Not at risk/low risk for Neonatal Abstinence Syndrome
Exposure to methamphetamine
s or THC
Admit to couplet care*
Exposure to short-acting narcotics without multiple
exposures
Admit to couplet care and observe for 4 days.
(No NAS Scoring by nursing) Call MD to assess if concern
for opiod withdrawal.
Exposure to antipsychotics, antidepressants (ie SSRIs), and
other medications.
Admit to couplet
care
*A positive maternal toxicology screen for THC and/or amphetamines can’t be used as an indication to legally
separate a mother from her well newborn. These infants can only be separated from mother after a CPS hold has
been placed.
Breastfeeding
Permitted for almost all mothers/infants at admission to FMCC or NICU.
Continued breastfeeding will be determined by medical team.
Contraindications to breastfeeding are positive HIV status, medications that are
Category L5, or confirmed on-going illegal drug use.
Long-Acting Opioids Fentanyl Transdermal Patch
Methadone Buprenorphine (Butrans, Subutex)
Oxymorphone hydrochloride extended-release (Opana) Oxycodone hydrochloride controlled-release (Oxycontin) Morphine sulfate extended-release (Oramorph, Kadian)
Short-Acting Opiods
Hydrocodone and Hydrocodone+APAP (Vicodin, Norco) Oxycodone+APAP (Percocet) or oyycodone IR
Tramadol Fentanyl (IV) or Morphine (IV)
Codeine Hydromorphone (Dilaudid)

Benefits we have seen since our policy change
• We have a clear message- less
frustration
• Mothers feel needed- and
welcome
• Less adversarial relationship
• Mother has a role no one else
can fill
• Fathers or family empowered to
help her visit and breastfeed, or
ferry milk
• For the compliant NAS mother, it
can be a success and an early
positive experience as a mother

Thank you! Questions?

Marijuana and Milk…
what to do?
Donna Garey MD MPH
Lisa Stellwagen MD
UC San Diego Medical Center
Division of Neonatology
http://ideatransfuser.wordpress.com/2013/11/12/marijuana-legalization-is-not-a-free-for-all-good-times-smoke-fest-bonanza/

Emerging Public Health Problem
• Legalization of marijuana in Washington and Colorado
• Decriminalized in many states
– Including California, Oregon, Nevada, Nebraska…
• Medical Marijuana
– 19 states (Oregon, Nevada, Arizona, New Mexico, Montana…)
• Increasing Potency (data from seized samples)
– 1985 – THC content 2.8%
– 1993 – THC content 3.4%
– 2008 –THC content 5.8 to 9.3%

Emerging Public Health Problem
• States responding to new concerns
– Focusing on education regarding the negative effects on the fetus
and infants
• Colorado formed health advisory committee

Marijuana and THC
• Marijuana: leaves and flowers of Cannabis sativa
• ∆-90-tetrahydrocannabinol is the psychoactive ingredient
– Highly lipophilic
– Half life of 20-36 hours (slow excretion)
– Excreted well into breastmilk (because it is fat soluble)
– Crosses the placenta
• Like smoking it can increased carboxyhemoglobin levels
– May impair fetal oxygenation and growth
Djulus J et al. Marijuana and breastfeeding. Can Fam Physician 2005

What do we know about the effects of THC on the
baby via the placenta/breastmilk?
Pregnancy • Complicated by other exposures
• Baby may have mild withdrawal
• There may be long term neuro-
behavioral deficits for the child
• No increased risk of SIDS for
maternal use (+ for paternal use)
Lactation • THC does pass into milk
• Infant effects unclear due to
prenatal exposure as well in
almost all cases
• Theoretical risk milk supply in
mother-but no decrease in
duration of lactation
• Concern about maternal
intoxication and infant care
• No data on infant effects
Jaques SC et al. J of Perinatology 2014 LactMed 2014

Marijuana Use in Pregnancy
• Most commonly used illicit drug in
women of reproductive age
• Self-reported use of 2.9% during
pregnancy

THC in pregnancy
• No known “safe” threshold for use in pregnancy
• Endogenous cannabinoids involved in development of the
nervous system
– Role is progenitor cell commitment and survival
– Five receptors identified
• CB1 –predominant CNS – Involved in neuronal proliferation, migration, and synaptogenesis
• Estimated dose to fetus unclear
– Human studies THC level 3 to 6 times lower in cord blood than
maternal blood

Early Neurologic Disturbances
Withdrawal symptoms
• Tremors
• Exaggerated startle
response
• Increased hand to mouth
behavior
• High pitched cry
• Sleep cycle disturbance
• No reports of withdrawal
requiring treatment
• Described as “mild narcotic
withdrawal”

Neurodevelopment and Growth Effects
Fetal Development
• Mixed BW effects –
depends on exposure and
population
– Decreased growth and BW
after 2nd trimester exposure
– Decreased length after first
trimester exposure
• Decreased gestational age
• No definitive link to
congenital anomalies
Neonatal Development
• Increased tremors and
startles
• Differences in sleep
recordings

Neurodevelopment and Behavior
Infant/Toddler
• Mixed results – some show
no difference
• 18 months: more
inattention and aggression
• 36 months: decreased
short-term memory
function and verbal
reasoning
Child
• 6 years: increased
impulsivity and
hyperactivity
• 10 years: decreased
abstract and visual
reasoning, decreased
attention
• 9-12 years: impaired visuo-
perceptual functioning
More effects with heavy use

What is known about THC levels in MBM?
• Review past & current statements
• Many references are based on opinion
and not study
• THC is confounded with other illicit
drugs and cigarette smoking
• THC use only during BF has not been
well studied
• Legal issues are rapidly changing
• Child Welfare Services in SD does not
act on THC issues
• We should balance what is really known
with risks of not BF

Committee on Nutritional Status during Pregnancy and Lactation, Institute of Medicine 1990
• “despite the relatively high prevalence of marijuana use
during pregnancy, no conclusive data are available on the
effect of marijuana on the developing fetus. There is,
however, suggestive evidence that marijuana use during
pregnancy may impair fetal growth”

Breastfeeding and the use of human milk AAP Policy Statement 2012
“Street drugs such as PCP (phencyclidine), cocaine, and
cannabis can be detected in human milk, and their use by
breastfeeding mothers is of concern, particularly with regard
to the infant’s long-term neurobehavioral development and
thus are contraindicated.97
Section on breastfeeding vol 129 PP e827 2012

Reference 97: cannabis and breastfeeding Garry et al. Journal of toxicology 2009
• “There are a few studies about the effects of cannabis consumption
during lactation on infant health and development. More attention has
been directed towards adverse effects of prenatal cannabis
exposure.”
• “Cannabis consumption during breastfeeding is contraindicated
according to Hale and the American Academy of Pediatrics in
Breastfeeding Mothers. If the mother regularly uses cannabis,
breastfeeding is contraindicated”
• “In conclusion, clinical and pharmacokinetic data indicate that
cannabis use is dangerous during breastfeeding for the child.
Observed effects in breastfed infant like sedation or reduced muscular
tonus could be due to, not only cannabis, but also other drugs or
medicines (psychotropic, antiepileptic, etc.) that mothers are likely to
take.”

Medications and Mother’s Milk 2014 Thomas W Hale, PhD & Hilary E Rowe PharmD
• Marijuana: L5 ‘studies concerning the use of cannabis in
pregnant women appear to be inconsistent in their results.
Cannabis should not be used during pregnancy or
breastfeeding’
• ‘this drug should not be used by nursing mothers’
• ‘while the data on neurobehavioral effects of cannabis on
infants from breastfeeding mothers is limited, cannabis
use in breastfeeding mothers should be strongly
discouraged. For daily continued use, mothers should be
advised not to breastfeed’

MotherRisk
• Despite abundant recreational use of cannabinoids by women of reproductive age, very little
is known about marijuana use and lactation.
• The passage of THC into breast milk has not been extensively studied. A study by Perez-Reyes and
Wall in 1982 suggested that THC is excreted into human breast milk in moderate amounts.8 Based
on their findings, 0.8% of the weight-adjusted maternal intake of one joint would be ingested by an
infant in one feeding7. In heavy users, the milk-to-plasma ratio (ie, levels in milk vs levels in maternal
blood) was as high as 8:1.8 Animal studies suggest that marijuana can decrease the amount of milk
produced by suppressing prolactin production and possibly through a direct effect on the mammary
glands. There are no human data to corroborate these observations.
• In 1990, a study by Astley and Little suggested that exposure to THC through breast milk in the first
month of life could result in decreased motor development at 1 year old.9 No studies have
adequately addressed the effects on long-term neurodevelopment. Lethargy, less frequent feeding,
and shorter feeding times are other observations reported after babies’ exposure to THC through
breast milk.10 A mother’s ability to nurse and care for her child might be compromised because
marijuana can affect mood and judgment.
• With chronic use, THC can accumulate in human breast milk to high concentrations.8 Because a
baby’s brain is still forming, THC could theoretically affect brain development. It is also important to
avoid environmental exposure to maternal marijuana smoke. Nursing mothers should be referred to
appropriate services for counseling.
http://www.motherisk.org/prof/updatesDetail.jsp?content_id=724

Academy of Breastfeeding Medicine 2009 ABM Clinical Protocol #21: Guidelines for breastfeeding and the drug-dependent woman
• D9-Tetrahydrocannabinol (THC) is present in human milk, and
metabolites not found in human milk are found in infant feces,
indicating that THC is absorbed and metabolized by the infant. There
may or may not be long-term effects on infant development from
perinatal THC exposure.
Pertinent THC references all from 1980’s

Presence of Δ9-tetrahydrocannabinol in human milk
Perez-Reyes M and Wall ME. NEJM 1982
• This was a correspondence; not peer reviewed
• 2 mothers who self reported smoking marijuana brought in
milk samples and infant urine samples
• Mother 1 milk: 105 ng/ml
• Mother 2 milk: 340 ng/ml
• Neither urine was positive for THC
• Mother 2 declined to stop using THC and agreed to have
her blood and milk and baby’s stool tested again
– Milk was tested at 1 hour after smoking (peak level) (estimated
0.8% of weight adjusted dose now frequently quoted)
– Infant 1 stool had THC metabolites

U.S. National Library of Medicine TOXNET Data Network: LactMed 2015
• Although published data are limited, it appears that active components of marijuana are
excreted into breastmilk in small quantities. Data are from random breastmilk screening
rather than controlled studies because of ethical considerations in administering
marijuana to nursing mothers. Concern has been expressed regarding marijuana's
possible effects on neurotransmitters, nervous system development and
endocannabinoid-related functions.[1][2] One long-term study found that daily or near
daily use might retard the breastfed infant's motor development, but not growth or
intellectual development.[3] This and another study[4] found that occasional
maternal marijuana use during breastfeeding did not have any discernable
effects on breastfed infants, but the studies were inadequate to rule out all long-
term harm.
• Marijuana use should be minimized or avoided by nursing mothers because it
may impair their judgment and child care abilities. Some evidence indicates that
paternal marijuana use increases the risk of sudden infant death syndrome in breastfed
infants. Marijuana should not be smoked by anyone in the vicinity of infants because
the infants may be exposed by inhaling the smoke. Because breastfeeding can mitigate
some of the effects of smoking and little evidence of serious infant harm has been
seen, it appears preferable to encourage mothers who use marijuana to continue
breastfeeding while minimizing infant exposure to marijuana smoke and reducing
marijuana use.[5]

Does THC exposure increase risk of SIDS?
• 239 SIDS cases and matched
controls (SoCal)
• Parents interviewed
• THC, Methamphetamine, cocaine,
LSD (mostly during pregnancy not
BF)
• After adjusting for risk factors no
association with SIDS for maternal
recreational drug use
• Paternal use of marijuana was
associated with SIDS (x2)
Klonoff-Cohen et al. Arch Pediatr Adolesc Med 2001

How to separate all the effects of THC use in lactating mothers?
Low milk supply
Altered maternal caregiver
Socio-economic factors
Other toxin exposures
Prenatal THC exposure
Prematurity
Breastfed vs formula fed
Growth restriction
Paternal use of THC

How to separate all the effects of THC use in lactating mothers? And balance that with the risk of not receiving breastmilk?
Low milk supply
Altered maternal caregiver
Socio-economic factors
Other toxin exposures
Prenatal THC exposure
Prematurity
Breastfed vs formula fed
Growth restriction
Risk of obesity
Altered maternal child bonding
Lack of developmental benefits of mother’s milk
Increased risk of infections Increased risk of SIDS
Paternal use of THC

So what should we tell mothers?
• THC gets transmitted to fetus and
breastfed infant
• Placenta and fetal brain are full of THC
receptors
• Long term effects of THC use in pregnancy
are not clear; but may include
abnormalities in development and school
performance
• Long term effects of THC use while
breastfeeding are not clear
• Breastfeeding however, is protective for
baby whether or not mother uses THC
• Is there a safe way to pump and dump with
THC for occasional use?


Next steps at UCSD…
• For select compliant mothers in
treatment:
– Improve pre-delivery
counseling
– Parent handout about our
policies
– Mom and baby stay together
in couplet care for 5 days
– Baby to NICU if starts to
withdraw
• MJ + BF handout to be given out
prenatally and after delivery for
women known to use THC

Urinary Drug Screening and Duration of Detection in Neonate
• Opioids
– Heroin, morphine, codeine
• 1-2 days
– Hydromorphone,
oxycodone
• 2- 4 days
– Methadone
• 2-3 days
– Methadone metabolites
• up to 6 days
– Buprenorphine
• 2-3 days
• Marijuana
– Single Use
• 1- 3 days
– Moderate Use
• 5-7 days
– Heavy Use
• up to 10 days
– Chronic Heavy Use
• up to 30 days

Meconium Drug Screening in Neonate
• More sensitive than urine screening
• Longer window of detection
– From 20 weeks gestation

References
• Brown MS, Hayes MJ et al. Methadone versus morphine for treatment of neonatal abstinence
syndrome: a prospective randomized clinical trial. J Perinatol. 2014 (epub ahead of print)
• Hall ES et al. A multicenter cohort study of treatments and hospital outcomes in neonatal abstinence
syndrome. Pediatrics. 2014;134(2):e527-34
• Hudak ML et al, committee on drugs: committee on fetus and newborn, American Academy of
Pediatrics. Neonatal drug withdrawal. Pediatrics. 2012;129(2):e540-60
• Huizink AC, et al. Maternal smoking, drinking or cannabis use during pregnancy and
neurobehavioral and cognitive functioning in human offspring. Neuroscience and Behavioral
Reviews. 2006; 30: 24-41.
• Huizink AC. Prenatal cannabis exposure and infant outcomes: Overview of studies. Progress in
Neuro-Psychopharmacology and Bilogical Psychiatry. 2014; 52: 45-52.
• Jaques SC et al. Cannabis, the pregnant woman and her child: weeding out the myths. J Perinatol.
2014;34:417-24
• Jones H, et al. Neonatal Abstinence Syndrome after Methadone and Buprenorphine Exposure.
NEJM. 2010; 363(24): 2320-2331.
• Kocherlakota P. Neonatal Abstinence Syndrome. Pediatrics 2014;134:e547–e561
• Hill M, Reed K. Pregnancy, breastfeeding, and marijuana: a review article. Ob and Gyn survey.
2013:69(10):710-8
• Stratherarn L, et al. Does breastfeeding protect against substantiated child abuse and neglect? A 15-
year cohort study. Pediatrics. 2009:123(2):483-93
• Klonoff-Cohen H, Lam-Kruglick P. Maternal and paternal recreational drug use and sudden infant
death syndrome. Arch Pediatr Adolesc Med. 2001;155:765-770

Thank you! Questions?



![UC Davis Neonatal Abstinence Syndrome.pptx [Read-Only] Davis... · 19/4/2017 · Neonatal Abstinence Syndrome ... sensory neurons, intestinal tract ... and autonomic functioning)](https://img.pdfslide.net/doc/110x75/5ad501df7f8b9a48398d07fd/uc-davis-neonatal-abstinence-read-only-davis1942017neonatal-abstinence-syndrome.jpg)