Embed Size (px)
Citation preview

Incontinentia pigmenti (Bloch-Sulzberger syndrome) A case report
Joseph Vogt, CDR, DC, USN,” and John Matheson, CAPT, DC, USN,b Portsmouth, Va.
PORTSMOUTH NAVAL HOSPITAL
lncontinentia pigmenti is a rare genodermatosis with multiple manifestations affecting the skeletal, ocular, dental, and other tissues. More than 95% of reported cases occur in females, and more than 60% of reported cases involve some dental abnormality. A brief review of the literature and a case in a 7-year-old
girl with the disease are presented. (ORAL SURC ORAL MED ORAL PATHOL 1991;71:454-6)
I ncontinentia pigmenti (IP) is an uncommon hered- itary disorder with significant manifestations affect- ing the neuroectodermal, ocular, and musculoskeletal tissues. It initially presents within 2 weeks of birth as a vesiculobullous eruption scattered on the trunk and extremities. These lesions may persist for months and do not correspond to any known dermatome.’ The second, or verrucous, phase is characterized by pap- illomatous, hypertrophic, or pruritic erythematous growths on one or more of the extremities. This stage is usually resolved by 1 year of age, although it may persist longer.* The third, or hyperpigmented, phase is typified by irregular whorls, macules, and streaks of brown or blue-gray pigmentation similar in distribu- tion to the vesiculobullous eruptions. These derma- toses may resolve by puberty or be retained into adulthood. All three stages may overlap and even be evident at birth.
Ocular abnormalities are observed in up to 30% of patients, including strabismus, cataracts, optic atro- phy, retinal dysfunction, blue sclera, nystagmus, and blindness. Dental abnormalities include pegged inci- sors, partial or complete anodontia, and delayed eruption of deciduous and succedaneous dentition.3 Carney4 reported the incidence of dental abnormali- ties at 64.7%, with partial anodontia the most com- mon (43.3%). More than half of all patients with IP exhibit neurologic deficits, including seizure disor- ders, mental retardation, spastic paralysis, ataxia, and
aResident, Oral and Maxillofacial Surgery. bDirector, Oral and Maxillofacial Surgery, and Head, Dental De- partment. 7/13/20614
454
motor dysfunction.5 Cardiac abnormalities and mus- culoskeletal malformations including microcephaly, syndactyly, spina bifida, cleft lip, cleft palate, and dwarfism have all been reported.‘, 6 Additional ecto- dermal dysplasias include patchy alopecia and thin, spoon-shaped fingernails and toenails.
Each stage of the disorder has a typical histopatho- logic appearance. The vesiculobullous phase is char- acterized by an epithelial spongiosis with inflamma- tory and eosinophilic infiltrate. The verrucous phase characteristically shows dyskeratosis, acanthosis, and hyperkeratosis. In the pigmentation phase, numerous melanophages are interspersed in the upper dermis with vacuolization of basal cells3, 6
IP is primarily found in females, who comprise more than 95% of all reported cases. The etiology is unknown; however, various authors have postulated viral or infectious causes during pregnancy as possi- ble factors. No clear correlation has been demon- strated, because the majority of pregnancies have been uncomplicated.4 Transmission is thought to be autosomal dominant with expression in females or a lethal X-chromosome linkage in males. Many cases have occurred with no family history of IP, suggest- ing a high mutation rate. The disease appears to have a predilection for Caucasians, but cases have been re- ported in Mongoloids, Negroes, Dravidians, Indo- Polynesians, and South Americans.
Incontinentia pigmenti achromians, or hypomel- anosis of Ito, is a separate but closely related disease entity. The typical cutaneous lesions appear as “neg- ative images” of IP lesions, and some appear de- pressed in side lighting. The three stages and cutane- ous anomalies of IP are not observed. The depig- mented patches are usually present at birth. There

Volume 7 I Number 4
Incontinentia pigmenti 455
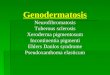
Fig. 1. Peg-shaped lower incisors, hypodontia of upper incisors, and delayed eruption of permanent mo- lars.
appears to be a high correlation of incontinentia pig- menti achromians with mental and motor retardation and seizure disorders.7
CASE REPORT
A 7-year-old white girl was brought by her parents to the oral surgery department at Portsmouth Naval Hospital for evaluation of her carious dentition. The parents were con- cerned about her having had repeated episodes of gingival swelling and pain. Her previous medical history was signif- icant for IP, which manifested at birth by what the parents described as “red welts” on her body. These changed to brown lesions after several days and then faded during the course of succeeding years. She presently manifests only a few mildly pigmented macules on the torso. Hydrocephalus was diagnosed in the child, and a ventriculoperitoneal shunt was placed when she was 1 month of age. She had a seizure disorder, status asthmaticus, spastic paraplegia, and clonus of the extremities. Her ocular defects included strabismus, blue sclera, and nystagmus. She was severely mentally re- tarded, with an inability to speak and an understanding of only a few words. Her diet consisted of pureed and baby foods, and bottle feedings.
Examination of the dentition revealed peg-shaped lower incisors, hypodontia of upper anteriors, and delayed erup- tion of the permanent molars (Fig. 1). Several posterior de- ciduous molars were grossly decayed. The patient’s mother stated that the child commonly had several episodes of pneumonia each year. One week before presentation the patient had undergone spinal fusion for correction of scoli- osis. Medications included phenytoin (Dilantin), 50 mg twice daily; phenobarbital, 48 mg/day; theophylline (Ac- cubron), 75 mg three times daily; and metaproterenol (Metaprel), 4 ml four times daily. The patient had no known drug allergies.
Consultation was obtained with the parents, pediatrician, and orthopedic surgeon. It was decided that extraction of
the remaining dentition would help preclude secondary in- fection, a significant risk because of the presence of the ventriculoperitoneal shunt and because of a history of fre- quent pneumonitis.
The leukocyte count was 9400/mm3; erythrocyte count, 3.95 X 106/mm3; hemoglobin level, 12.0 gm/dl; hematocrit, 36.3%; and platelet count, 37 X 103/mm3. The differential was within normal limits. Blood levels for phenytoin, theo- phylline, and phenobarbital were measured preoperatively and the preoperative medication dosages adjusted accord- ingly. Because of the child’s mental and physical disabili- ties, radiographs were not obtainable until perioperatively.
The patient was taken to the main operating room, and with the patient under general nasoendotracheal anesthesia, all 12 erupted deciduous teeth (A, C, G, H, I, J, M, N, 0, P, Q, R) were extracted without complication. The patient’s recovery was unremarkable, and she was discharged the same evening in good condition.
DlSCUSSlON
IP, although rarely seen in clinical practice, never- theless presents a diagnostic and therapeutic chal- lenge. Carney,4 in his extensive study of the disorder, cites 198 of 306 patients (64.7%) as having some ma- jor dental deformity, with partial anodontia the most common (43.1%). The majority of patients with IP generally have other significant neurologic or skeletal deficits that complicate the treatment plan. The den- tist may be consulted regarding actual or potential problems resulting from dental disease that impinge on management of this condition.
REFERENCES
1. Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KI, eds. Dermatology in general medicine. New York: McGraw- Hill, 1987:856-S.

456 Vogt and Matheson
2. O’Brien JE, Feingold M. Incontinentia pigmenti: a longitudi- nal study. Am J Dis Child 1985;139:71 l-2.
3. Rook A, Wilkinson DS, Ebling FJG. Textbook of dermatology; vol 2. London: Blackwell Scientific Publications, 1986: 1559- 61.
4. Carney RG. Incontinentia pigmenti: a world statistical anal- ysis. Arch Dermatol 1976;112:535-42.
5. Larsen R, Ashwal S, Peckham N. Incontinentia pigmenti: as- sociation with anterior horn cell degeneration. Neurology 1987;37:446-50.
6. Moschella SL, Hurley HJ. Dermatology. Philadelphia: WB Saunders, 1985:1286-7.
ORAL SURC ORAL MED ORAL PATHOL April 1991
7. Fitzpatrick TB, Eisen AZ, Wolff K, Freedberg IM, Austen KI, eds. Dermatology in general medicine. New York: McGraw- Hill, 1987:827-8.
Reprint requests to: Joseph A. Vogt, DDS Department of Oral and Maxillofacial Surgery Portsmouth Naval Hospital Portsmouth, VA 23708
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of ORAL SURGERY, ORAL MEDICINE, AND ORAL PATHOLOGY are available to subscribers (only) for the 1991 issues from the Publisher, at a cost of $45.00 for domestic, $60.15 for Canadian, and $57.00 for international, for Vol. 71 (January-June) and Vol. 72 (July-December). Shipping charges are included. Each bound volume contains a subject and author index and all advertising is removed. Copies are shipped within 60 days after publication of the last issue in the volume. The binding is durable buck- ram with the journal name, volume number, and year stamped in gold on the spine. Poymrnt must ac- company all orders. Contact Mosby-Year Book, Inc., Subscription Services, 11830 Westline Industrial Drive, St. Louis, MO 63146-3318, USA; phone (800)325-4177, ext. 4351. ~ppvstbeinforce to qualify. Bound volumes are not available in place of a regular journal subscr+tion.