Embed Size (px)
Citation preview

Incontinentia pigmenti in male patients
Theresa R. Pacheco, MD,b Moise Levy, MD,c James C. Collyer, MD,a,b Nelida Pizzi de Parra, MD,d
Cristobal A. Parra, MD,d Marisel Garay, MD,d Gabriela Aprea, MD,d Silvia Moreno, MD,d
Anthony J. Mancini, MD,a and Amy S. Paller, MDa
Chicago, Illinois; Denver, Colorado; Houston, Texas; and Mendoza, Argentina
Background: Incontinentia pigmenti (IP) is a rare X-linked dominant genodermatosis that is typified bydistinctive cutaneous findings and often by abnormalities of teeth, hair, nails, eyes, musculoskeletal system,and central nervous system. The gene that is mutated in patients with IP has been mapped to Xq28 andencodes the NF-kB essential modulator, NEMO. Female patients with IP show functional mosaicism andcutaneous manifestations follow Blaschko’s lines of ectodermal embryologic development. The conditionis generally considered to be lethal in utero in male fetuses, suggesting that having some normal geneexpression is critical for survival.
Observations: We observed 9 boys with IP. All had normal karotypes and no apparent family historyof IP. In 8 of these 9 patients, lesions were localized to one extremity at presentation. The diagnosis wasconfirmed by histopathologic examination that showed eosinophils within intraepidermal, multiloculatedvesicles. One of the boys later developed dental and neurologic abnormalities.
Limitations: The case series was small and the workup for these patients from different sites was notuniform.
Conclusions: Male individuals may show cutaneous and noncutaneous features of IP in a limited dis-tribution that allows survival. Postzygotic mutation/somatic mosaicism is the likely mechanism. Given thepotential sequelae associated with this condition, continuing follow-up of these patients is recommended.( J Am Acad Dermatol 2006;55:251-5.)
Incontinentia pigmenti (IP) (MIM 308300) isan X-linked dominant disorder and, therefore,primarily manifests in female patients. The con-
dition is characterized by typical cutaneous lesionsand, in many patients, by abnormalities of the centralnervous system and the eyes. Central nervous systemabnormalities may include seizures, mental retarda-tion, spasticity, hemiparesis, and encephalopathy.Ocular findings include retinal vascular abnormali-ties, cataracts, uveitis, strabismus, and nystagmus.
From the Departments of Dermatology and Pediatrics, Northwest-
ern’s Feinberg School of Medicine, Chicagoa; Department of
Dermatology, University of Colorado Health Sciences Centerb;
Departments of Dermatology and Pediatrics, Baylor Medical
College, Houstonc; and Children’s Hospital, University of Cuyo,
Mendoza.d
Funding sources: None.
Conflicts of interest: None identified.
Accepted for publication December 6, 2005.
Reprints not available from the authors.
Correspondence to: Amy S. Paller, MD, Northwestern University
Medical School, 645 N Michigan Ave, Suite 520, Chicago, IL
60611. E-mail: [email protected].
Published online May 16, 2006.
0190-9622/$32.00
ª 2006 by the American Academy of Dermatology, Inc.
doi:10.1016/j.jaad.2005.12.015
Other ectodermal abnormalities may involve thehair (alopecia), nails (variable dystrophy), and teeth(missing or small teeth, conical or peg teeth, delayederuption).
The skin findings of IP tend to be patterned alongBlaschko’s lines of ectodermal cell embryologicdevelopment. They have been characterized asvesiculopustular, verrucous, hyperpigmented, andhypopigmented/atrophic. These morphologic pat-terns are often sequential, but may overlap and occurat different sites, providing evidence that the se-quence is not an evolution.1 The first 3 stagestypically appear during the first 6 months of life,and tend to be distributed on the torso and usuallymore than one extremity. The hyperpigmentedstreaks and whorls often persist for years, clearinglater in childhood or after puberty. Of patients, 28%and 14% show atrophic and hypopigmented lesions,respectively; these lesions may be subtle and only
Abbreviations used:
ED: ectodermal dysplasiaID: immunodeficiencyIP: incontinentia pigmenti
251

J AM ACAD DERMATOL
AUGUST 2006
252 Pacheco et al
visible with a Wood’s lamp or with darkening ofsurrounding skin.2
The gene that is mutated in patients with IP hasbeen mapped to Xq28 and encodes the NF-kBessential modulator, NEMO.3 NEMO is the regulatorycomponent of IKKg, the central activator of theNF-kB signaling pathway. NEMO mutations disruptNF-kB activity and inhibit activation of downstreamgenes, including those responsible for the produc-tion of chemokines, adhesion molecules, and cyto-kines, leading to increased cellular sensitivity toapoptosis.4 IKKg knockout male mice die in utero,whereas female mice develop transient skin mani-festations similar to IP. At birth IKKg 1/� newbornfemale mice are indistinguishable from wild-typecounterparts. A few days after birth, the IKKg 1/�female mice develop inflammatory skin changescharacterized initially by red, blistered skin that isreplaced by hyperkeratotic lesions that eventuallydesquamate. Patchy pigmentation then occurs.5,6
Of IP cases, 90% are caused by the same genomicdeletion in NEMO.7 Despite identical mutations andnearly complete X-linked dominant penetrance,phenotypic expressivity is variable. The markedfemale preponderance and frequency of spontane-ous abortions of male fetuses of affected motherssuggest an X-linked dominant inheritance patternwith lethality in males. However, rare cases of IPhave occurred in male patients who survive. Wedescribe 9 additional male patients with limited IPand stress the possibility that noncutaneous mani-festations may develop after infancy.
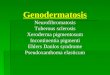
Fig 1. Linear collection of vesicles on left lower leg ofpatient 1.
REPRESENTATIVE CASE REPORTSPatient 1
A 2-week-old boy developed an eruption at3 days of age that initially appeared on the left ankleand extended to the back aspect of the left leg ina linear pattern. The patient was adopted, with noknown family history of IP.
Pustules, vesicles, and crusts extended in a linearpattern from the left lateral malleolus to the leftpopliteal fossa (Fig 1). No other cutaneous lesionswere noted, including lack of nail dystrophy orscalp lesions. Complete neurologic, ophthalmologic,and musculoskeletal examinations revealed normalfindings.
Histologic examination of a vesicle revealedeosinophils within intraepidermal, multiloculatedvesicles. Chromosomal analysis from peripheralblood leukocytes showed a normal male karyotype.Chromosomal studies of cultured fibroblasts fromskin of an affected site (left leg) versus a clinicallynormal site (left forearm) showed no difference andwere reported to be normal.
At 8 weeks of age, the vesicles and pustulesresolved spontaneously. At 2 years of age, no othercutaneous or systemic abnormalities had developed.At 7 years of age, partial seizures were diagnosed.Brain magnetic resonance imaging showed no ab-normalities. At 14 years of age, hypomelanosis in alinear distribution became apparent on the left lowerextremity (Fig 2). The patient has had a variety of
Fig 2. At age 13 years patient 1 first noted discontinuoushypopigmented streak on left lower leg in distributionof linear collection of vesicles during neonatal and earlyinfantile period.

J AM ACAD DERMATOL
VOLUME 55, NUMBER 2
Pacheco et al 253
dental abnormalities, including a midline supernu-merary tooth (mesiodens), late exfoliation, and extracusps and roots (Fig 3). Seizures remain controlledwith carbamazepine and phenytoin, and his eyeexaminations have revealed normal findings.
Patient 2A 6-day-old boy had a 3-day history of vesicles
on left medial thigh and leg, and a 2-day history ofsimilar lesions in the left inguinal area. There was nofamily history of IP. Physical examination revealeda linearly arranged collection of clustered vesicleson an erythematous base on his left inguinal area,medial thigh, lower leg, and foot (Fig 4). No othercutaneous lesions were noted, including lack of naildystrophy or scalp lesions. Complete neurologic,ophthalmologic, and musculoskeletal examinationsproduced normal results. The mother’s cutaneousexamination failed to reveal stigmata of IP.
Histologic examination revealed an intraepider-mal blister with inflammatory cells and eosinophilsconsistent with IP. His peripheral blood showed9% eosinophils. Chromosomal analysis from periph-eral blood leukocytes showed a normal male karyo-type. Fibroblast chromosomal studies were notperformed.
By 3 months of age, the vesicular lesions hadcleared. No verrucous, dyspigmented, or atrophiclesions developed. At last follow-up at 8 years of age,his skin was normal and he had no other medicalproblems.
Patients 3 to 9Seven other male patients with IP were seen at 3
medical centers. Their presentations and courses arediscussed in Table I. All showed linearly distributedlesions along lines of Blaschko and had a history ofvesiculopustular lesions. All who were tested hadmild peripheral eosinophilia. None had a knownfamily history of IP.
Fig 3. Eruption of teeth was delayed in patient 1. At 14years of age, he shows mesiodens and abnormally spacedteeth that first became apparent at 7 years of age.
DISCUSSIONIP is considered an X-linked dominant disorder,
which is usually lethal in males. We describe 9 malepatients with IP. In 8 of these 9 patients, lesionswere localized to one extremity at presentation; inthe ninth (patient 6), lesions involved more thanone extremity, but were localized to one side ofthe body.
The diagnosis in each patient was confirmedhistologically. In 8 of the 9 patients, the histologicexamination of a vesicle revealed eosinophils withinintraepidermal, multiloculated vesicles. The ninthpatient (patient 4) with verrucous lesions showedhistologically irregular epidermal acanthosis, mildhyperkeratosis, and occasional dyskeratotic kerati-nocytes with scattered melanin pigment in the pap-illary dermis. At birth and in the first year of life,evidence of other stigmata of IP were not noted;however, one of these patients (patient 1) latershowed manifestations consistent with IP (hypopig-mented streak, dental abnormalities, and seizures).There was no family history of IP and examinationof the mothers failed to reveal signs of IP. None ofthe 9 boys had evidence of a 47, XXY karyotype orperipheral leukocyte gross chromosomal mosaicism(Table I).
A total of 64 previously published cases of IPin male patients have been described.8-12 Threepotential mechanisms have been proposed to ex-plain the survival of male patients with IP carryingthe NEMO mutation: (1) abnormal karyotypes; (2)hypomorphic mutations; and (3) mosaicism.10,13
Of the 64 cases, 5 patients had abnormal karyo-types consistent with Klinefelter’s syndrome (47,XXY).10,14-18 One of these patients continues to befollowed up by us,14,16 and shows only cutaneousand dental manifestations. Analysis of the NEMOgene in one patient with Klinefelter’s syndromeshowed the common deletion mutation in thematernal X chromosome, which was randomly
Fig 4. Linearly arranged collection of clustered vesicles onerythematous base on left inguinal area, medial thigh,lower leg, and foot of patient 2 at 6 days of age.

J AM ACAD DERMATOL
AUGUST 2006
254 Pacheco et al
Table I. Incontinentia pigmenti in male patients
Patient
no. Skin findings Onset Other findings Follow-up Karyotype
Other
laboratory
Family
history
1 L leg: linear papulovesicleshypopigmented linearstreaks
7 d 13 y Nl eye examination,development
Partial seizures,dental abnormalitiesby age 7 y
14 y 46, XY Nl fibroblastchromosomes
Adopted
2 L inner groin, thigh, calf,medial ankle: lineararrangement ofvesicles
3 d Nl eye examination,development; mildspeech delay;hearing Nl
8 y 46, XY 9% Eosinophils None
3 R medial thigh, lower leg:linear papulovesicles linearhyperpigmented streaks
and verrucous papuleslinear atrophic
hyperpigmented streaks
2 d 4 mo13 mo
Nl eye examination,development
10 y 46, XY ND None
4 R flank, axilla, leg: linearerythemateous papules
linear hyperpigmentedstreaks
linear hyperpigmentedstreaks and verrucouspapules
7 d 2 mo5 mo
Nl eye examination 3 mo 46, XY 9% Eosinophils None
5 R lower leg: linearpapulovesicles
5 d 33-wk gestationalage triplet
15 y 46, XY ND None
6 R and L extremities, groin,trunk, face, and scalp:linear papulovesicles
Birth Nl eye examination 11.5 y 46, XY 5% Eosinophils None
7 L medial thigh: linearpapulovesicles
1 d Nl eye examination 6 y 46, XY 8% Eosinophils None
8 L lower leg: linearpapulovesicles
1 d Nl eye examination 5 y 46, XY 6% Eosinophils None
9 L extremities, face,and scalp: linearpapulovesicles
1 d Nl eye examination 3 y 46, XY 9% Eosinophils None
L, Left; ND, no data; Nl, normal; R, right.
inactivated in cells, presumably allowing survival.10
The presence of a 47, XXY karyotype in approxi-mately 7% of male patients now described with IPhighlights the importance of karyotyping any malepatient with suggested IP.
Hypomorphic mutations may result in milderphenotypes but are an unlikely explanation for IPin a male patient. Hypomorphic mutations of theNEMO gene differ from the characteristic deletion ofexons 4 to 10 on the NEMO gene (seen in 80%-90%of patients with IP) by generally being duplicationmutations of a cytosine tract in exon 10.18 Boys withthe hypomorphic mutations usually have a pheno-type of ectodermal dysplasia (ED) and immuno-deficiency (ID).19-21 However, a boy with ED ID wasborn of a mother with IP,22 and patients have beendescribed with features of both IP and ED ID.19-22
These observations suggest that the hypomorphicmutations are capable of producing the phenotypeof IP, even without manifestations of ID or ED.23
The most likely explanation for manifestationsof IP in male patients is somatic mosaicism, a con-cept that is increasingly being recognized as anexplanation for skin conditions. Somatic mosaicismresults from a postzygotic mutation that occursduring the blastocyst stage of embryogenesis. De-pending on the timing of the occurrence of thismutation, the manifestations of somatic mosaicismcan be extensive or quite limited.24 Evidence ofmosaicism in genomic DNA from peripheral bloodcells may be difficult to demonstrate unless thepatient exhibits sufficient mesodermal involvement,given the mesodermal origin of leukocytes. IP seemsto primarily manifest in cells of neuroectodermal

J AM ACAD DERMATOL
VOLUME 55, NUMBER 2
Pacheco et al 255
lineage; thus, demonstration of somatic mosaicismmay require examination for NEMO gene abnormal-ities of affected cells of ectodermal origin, particu-larly keratinocytes. The finding of mutations inkeratin 10 or keratin 1 in cultured keratinocytesfrom lesional skin of patients with epidermal neviof the epidermolytic hyperkeratotic type, but notnecessarily from underlying fibroblasts or leukocyteDNA,19 emphasizes the need to examine affectedneuroectodermal cells from boys with potential mo-saicism for NEMO gene mutations and may explainthe failure to show the molecular basis of mosaicismin IP in cultured fibroblasts.10 The clearance of earlyskin lesions presumably occurs through keratinocyteapoptosis and replacement by surrounding cells witha normal genotype. Thus, one potential pitfall indemonstrating mosaicism through use of culturedkeratinocytes from the lesional skin of a boy with IP isthe likelihood that cells that express the abnormalNEMO gene product have a selective survival disad-vantage and greater tendency to become apoptotic.As a result, cultures of keratinocytes taken fromlesional tissue may show only the normal NEMOgene if both normal and abnormal keratinocytes arecaptured in the original biopsy section.
Clinical and histologic studies suggest the diag-nosis of mosaic IP in the 9 male patients reportedherein. The development of dental and neurologicabnormalities in one of these boys after infancyemphasizes the need for continuing evaluation.In the future early acquisition of affected skin mayallow for genetic analysis that proves the mechanismof postzygotic mosaicism in these boys with IP andlimited involvement.
REFERENCES
1. Mayer EJ, Shuttleworth GN, Greenhalgh KL, Sansom JE, Grey
RHB, Kenwrick S. Novel corneal features in two males with
incontinentia pigmenti. Br J Ophthalmol 2003;87:554-6.
2. Berlin AL, Paller AS, Chan LS. Incontinentia pigmenti: a review
and update on the molecular basis of pathophysiology. J Am
Acad Dermatol 2002;47:169-87.
3. Smahi A, Courtois G, Vabres P, Yamoka S, Heuertz S, Munnich
A, et al. Genomic rearrangement in NEMO impairs NF-kappa B
activation and is a cause of incontinentia pigmenti: the
international incontinentia pigmenti (IP) consortium. Nature
2000;405:466-72.
4. Greaves S. The consequences of incontinentia pigmenti. Nat
Cell Biol 2000;2:E144.
5. Makris C, Godfrey VL, Krahn-Senftleben G, Takahashi T,
Roberts JL, Schwarz T, et al. Female mice heterozygous for
IKK gamma/NEMO deficiencies develop a dermatopathy similar
to the human X-linked disorder incontinentia pigmenti. Mol
Cell 2000;5:969-79.
6. Schmidt-Supprian M, Bloch W, Courtois G, Addicks K, Israel A,
Rajewsky K, et al. NEMO/IKK gamma-deficient mice model
incontinentia pigmenti. Mol Cell 2000;5:981-92.
7. Aradhya S, Woffendin H, Jakins T, Bardaro T, Esposito T, Smashi
A, et al. A recurrent deletion in the ubiquitously expressed
NEMO (IKK-gamma) gene accounts for the vast majority of
incontinentia pigmenti mutations. Hum Mol Genet 2001;10:
2171-9.
8. Scheuerle AE. Male cases of incontinentia pigmenti: case
report and review. Am J Med Genet 1998;77:201-18.
9. Mansour S, Woffendin H, Mitton S, Jeffery I, Jakins T, Kenwrick
S, et al. Incontinentia pigmenti in a surviving male is accom-
panied by hypohidrotic ectodermal dysplasia and recurrent
infection. Am J Med Genet 2001;99:172-7.
10. Kenwrick S. Survival of male patients with incontinentia
pigmenti carrying a lethal mutation can be explained
by somatic mosaicism or Klinefelter syndrome: the inter-
national IP consortium. Am J Hum Genet 2001;69:1210-7.
11. Hadj-Rabia S, Froidevaux D, Bodak N, Hamel-Teillac D, Smashi
A, Touil Y, et al. Clinical study of 40 cases of incontinentia
pigmenti. Arch Dermatol 2003;139:1163-70.
12. Cho SY, Lee CK, Drummond BK. Surviving male with inconti-
nentia pigmenti: a case report. Int J Paediatr Dent 2004;14:
69-72.
13. Fowell SM, Greenwald MJ, Prendiville JS, Jampol LM. Ocular
findings of incontinentia pigmenti in a male infant with
Klinefelter syndrome. J Pediatr Ophthalmol Strabismus 1992;
29:180-4.
14. Garcia-Dorado J, de Unamuno P, Fernandez-Lopez E, Salazar
Veloz J, Armijo M. Incontinentia pigmenti: XXY male with a
family history. Clin Genet 1990;38:128-38.
15. Prendiville JS, Gorski JL, Stein CK, Esterly NB. Incontinentia
pigmenti in a male infant with Klinefelter syndrome. J Am
Acad Dermatol 1989;20:937-40.
16. Ormerod AD, White MI, McKay E, Johnston AW. Incontinentia
pigmenti in a boy with Klinefelter’s syndrome. J Med Genet
1987;24:439-41.
17. Kunze J, Frenzel UH, Huttig E, Grosse FR, Wiedemann HR.
Klinefelter’s syndrome and incontinentia pigmenti Bloch-
Sulzberger. Hum Genet 1977;35:237-40.
18. Aradhya S, Courtois G, Rajkovic A, Lewis RA, Levy M, Israel A,
et al. Atypical forms of incontinentia pigmenti in male
individuals result from mutations of a cytosine tract in exon
10 of NEMO (IKK-gamma). Am J Hum Genet 2001;68:765-71.
19. Zonana J, Elder ME, Schneider LC, Orlow SJ, Moss C, Golabi M,
et al. A novel X-linked disorder of immune deficiency and
hypohidrotic ectodermal dysplasia is allelic to incontinentia
pigmenti and due to mutations in IKK-gamma (NEMO). Am J
Hum Genet 2000;67:1555-62.
20. Jain A, Ma CA, Liu S, Brown M, Cohen J, Strober W. Specific
missense mutations in NEMO result in hyper-IgM syndrome
with hypohydrotic ectodermal dysplasia. Nat Immunol 2001;
2:223-8.
21. Doffinger R, Smahi A, Bessia C, Geismann F, Feinberg J,
Durandy A, et al. X-linked anhidrotic ectodermal dysplasia
with immunodeficiency is caused by impaired NF-kappaB
signaling. Nat Genet 2001;27:277-85.
22. Dupuis-Girod S, Corradini N, Hadj-Rabia S, Fournet JC, Faivre L,
Le Deist F, et al. Osteopetrosis, lymphedema, anhidrotic
ectodermal dysplasia, and immunodeficiency in a boy and
incontinentia pigmenti in his mother. Pediatrics 2002;109:
97-102.
23. Erickson RP. Somatic gene mutation and human disease other
than cancer. Mutat Res 2003;543:125-36.
24. Paller AS, Syder AJ, Chan YM, Yu QC, Hutton E, Tadini G, et al.
Genetic and clinical mosaicism in a type of epidermal nevus.
N Engl J Med 1994;331:1408-15.