Embed Size (px)
Citation preview

European Neuropsychopharmacology (]]]]) ], ]]]–]]]
0924-977X/$ - see frohttp://dx.doi.org/1
nCorrespondence tUniversity of TuebinTel.: +49 7071 29 82
E-mail address: A(A.J. Fallgatter).
1Both authors con
Please cite this artof cognitive respon
www.elsevier.com/locate/euroneuro
Influence of a Latrophilin 3 (LPHN3) risk haplotypeon event-related potential measures of cognitiveresponse control in attention-deficit hyperactivitydisorder (ADHD)
Andreas J. Fallgattera,b,n,1, Ann-Christine Ehlisa,b,1, Thomas Dreslera,b,Andreas Reifb, Christian P. Jacobb, Mauricio Arcos-Burgosc,Maximilian Muenkec, Klaus-Peter LeschbaDepartment of Psychiatry and Psychotherapy, University of Tuebingen, GermanybDepartment of Psychiatry, Psychosomatics and Psychotherapy, University Hospital Wuerzburg, GermanycTranslational Medicine Department ,ANU College of Medicine, Biology and Environment, John Curtin School of MedicalResearch, The Australian National University, Canberra, Australia
Received 12 April 2012; received in revised form 16 October 2012; accepted 3 November 2012
KEYWORDSLatrophilin 3 (LPHN3);Attention-deficithyperactivity disorder(ADHD);Prefrontal cortex;Go–NoGo;Imaging genetics
nt matter & 20120.1016/j.euroneur
o: Department ofgen Calwerstr. 24,300; fax: +49 7071
ndreas.Fallgatter
tributed equally t
icle as: Fallgatter,se.... European N
AbstractCurrent research strategies have made great efforts to further elucidate the complex geneticarchitecture of attention-deficit hyperactivity disorder (ADHD). The present study examined theimpact of an LPHN3 haplotype that has recently been associated with ADHD (Arcos-Burgos et al.,2010) on neural activity in a visual Go-NoGo task. Two hundred sixteen adult ADHD patientscompleted a Continuous Performance Test (CPT) while the ongoing EEG was simultaneouslyrecorded. Results showed that patients carrying two copies of the LPHN3 risk haplotype (n=114)made more omission errors and had a more anterior Go-centroid of the P300 than patientscarrying at least one LPHN3 non-risk haplotype (n=102). Accordingly, the NoGo-Anteriorization(NGA; topographical ERP difference of the Go- and NoGo-condition), a neurophysiological markerof prefrontal functioning, was reduced in the LPHN3 high risk group. However, in the NoGo-condition itself no marked differences attributable to the LPHN3 haplotype could be found. Ourfindings indicate that, within a sample of ADHD patients, the LPHN3 gene impacts behavioral andneurophysiological measures of cognitive response control. The results of our study furtherstrengthen the concept of an LPHN3 risk haplotype for ADHD and support the usefulness of theendophenotype approach in psychiatric and psychological research.& 2012 Published by Elsevier B.V.
Published by Elsevier B.V.o.2012.11.001
Psychiatry and Psychotherapy,72076 Tuebingen, Germany.29 5379.
@med.uni-tuebingen.de
o this work.
A.J., et al., Influence of a Latropeuropsychopharmacology (2012),
1. Introduction
Attention-deficit hyperactivity disorder (ADHD) is a commonpsychiatric childhood disorder that frequently persists into
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

2Ratio of N-acetylaspartate to creatine (assessed via protonmagnetic resonance spectroscopy), which provides an index ofneuronal number or viability.
A.J. Fallgatter et al.2
adulthood (Barkley, 1998) and is accompanied by a wealthof socio-economic problems (Kessler et al., 2006). Coresymptoms comprise inattention, hyperactivity and impulsivity,and comorbid conditions are common (Biederman, 2005;Polanczyk et al., 2007; Skounti et al., 2007). While mostchildren display all symptoms, subtypes emphasizing inat-tention or hyperactivity-impulsivity have been defined (Saßet al., 2003). Overall, ADHD puts children at higher risk forprospective disadvantage (Mannuzza et al., 1993) andplaces a substantial economic burden on patients, families,and society (Birnbaum et al., 2005; Matza et al., 2005).
One well-elaborated neuropsychological model assumesADHD to be based on a core deficit in behavioral inhibition(Barkley, 1997, 1998; Dopfner and Lehmkuhl, 2006), subse-quently affecting related executive functions. More recentconcepts stress the importance of other response controlaspects in pathogenesis, particularly higher-order con-trolled motor (dys-) functioning as well as deficient atten-tional control and mental flexibility (Slaats-Willemse,2003). In his dual-pathway model, Sonuga-Barke (2003)proposed—in addition to the mentioned inhibition deficit(executive circuit)—a second mechanism potentially under-lying ADHD symptoms in at least part of the patients, whichis associated with an increased delay aversion and relatedto reward circuitry dysfunction (motivational subtype).Currently a triple-pathway model is under debate (withadditional temporal processing deficits), which, however,still needs to be empirically replicated (Sonuga-Barke et al.,2010). The concept of ADHD-related deficits in responseinhibition, motor control, and general executive processes(i.e. the executive circuit according to Sonuga-Barke) hasbeen supported by numerous neuropsychological studies(e.g., Barkley et al., 1992; Borger and van der Meere,2000; Hanisch et al., 2006; Losier et al., 1996; Martel et al.,2007; Nigg, 1999; Uebel et al., 2010). Accordingly, brainimaging studies found reduced activity in prefrontal areasduring performance of response inhibition/higher ordermotor control paradigms (Rubia et al., 1999; Rubia et al.,2005) and other executive processes (Bush et al., 1999;Schweitzer et al., 2000).
There is evidence for substantial genetic influences onthe etiology and pathogenesis of ADHD (Biederman, 2005;Faraone and Doyle, 2000; Faraone et al., 2005; Frankeet al., 2012; Gizer et al., 2009; Martin et al., 2002).Especially variations in genes of the dopaminergic, but alsothe noradrenergic and the serotonergic system have beenexamined in association and linkage studies. Potentialcandidate genes include the dopamine transporter (DAT)gene, the dopamine receptor D4 (DRD4) gene, the dopamineß hydroxylase (DBH) gene, and the serotonin transporter(5-HTT) gene. Despite the high heritability of ADHD shown intwin studies (Faraone and Doyle, 2000; Levy et al., 1997),results from molecular genetic studies indicate a complexgenetic architecture with many genes of small effectmediating the genetic vulnerability (Faraone et al., 2005).Linkage analyses found markers at diverse loci on differentchromosomes (Arcos-Burgos et al., 2004) that are related tothe diagnosis of ADHD. Recently, common variants of theLatrophilin 3 (LPHN3) gene located on chromosome 4 werefound to increase the susceptibility for ADHD in severalpopulations (Arcos-Burgos et al., 2010). LPHN3, the mostbrain-specific latrophilin (Ichtchenko et al., 1998; Sugita
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
et al., 1998), is a member of the LPHN subfamily ofG-protein coupled receptors (GPCRs). LPHN3 mRNA showedsignificant expression in human amygdala, caudate nucleus,cerebellum, and cerebral cortex, and individuals carryingthe LPHN3 susceptibility haplotype exhibited a significantlydecreased NAA/Cr ratio2 in the left lateral and medialthalamus as well as the right striatum (Arcos-Burgoset al., 2010). As LPHN3 is particularly expressed in meso-limbic regions of the brain that have been implicated inADHD (Krain and Castellanos, 2006), a functional relationwith ADHD symptomatology is quite plausible. Recently,Domene et al. (2011) could show that the susceptibilityhaplotype was not associated with significant coding regionchanges or canonical splice site alterations, which indicatesnon-coding variations to be likely contributors for ADHD.
Genetic approaches are hampered as the relation ofspecific genes and discrete disorders is often not as closeas twin studies suggest. The endophenotype concept(cf. Almasy and Blangero, 2001; for more recent conceptualconsiderations see also Kendler and Neale, 2010) aims atidentifying markers that are more directly connected to theunderlying psychopathology than the clinical diagnosesthemselves, and therefore much ‘‘closer’’ to etiologicalfactors (e.g., genes, environment). Besides measuring psy-chological constructs (Zobel and Maier, 2004), assessingbrain function is one means of characterizing such endo-phenotypes (Ehlis et al., 2007; Hariri et al., 2002; Hariri andWeinberger, 2003). By combining neuroimaging with geneticanalyses, associations of genetic variants (e.g., singlenucleotid polymorphisms; SNPs) with measures of brainfunction can be examined. The first imaging genetic studydescribed an effect of the 5-HTT genotype on the topogra-phy of event-related potentials during a response inhibitiontask (Fallgatter et al., 1999). Hence, it is possible tomeasure gene-related differences in neural activity thatare not necessarily apparent on a behavioral level(Bookheimer et al., 2000; Dresler et al., 2010; Eganet al., 2001; Ehlis et al., 2007).
Among the different endophenotypes that have beenproposed for ADHD, dysfunctions in response inhibition aswell as in attentional control and motor control processesplay a particularly important role (Slaats-Willemse, 2003).A cognitive paradigm that comprises all of these functions isthe Continuous Performance Test (CPT; Rosvold et al.,1956), a Go–NoGo task that requires both the executionand the inhibition of primed motor responses. The CPT caneasily be applied and has been used several times to studybehavioral inhibition and related neurophysiological mar-kers in ADHD (e.g., Dhar et al., 2010; Losier et al., 1996;Spronk et al., 2008). For this paradigm, a reliable electro-physiological marker presumably capturing prefrontal func-tioning, the so-called NoGo-Anteriorization (NGA), has beenidentified and established (Fallgatter et al., 1997, 2002b;Fallgatter and Strik, 1999). In line with conventional P300single electrode data, indicating increased P300 amplitudesover fronto-central electrode positions under inhibitory(NoGo) conditions, the NGA quantitatively describes theamount of anteriorization of the positive brain electrical
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

3Latrophilin 3 and response control processes in ADHD
field during the inhibition (NoGo-condition) relative to theexecution (Go-condition) of a primed motor response andhas been suggested as a topographical ERP marker ofcognitive response control (see, e.g., Fallgatter et al.,1997). Neuroanatomically, the phenomenon of the NGAseems to reflect an increased activation of prefrontal areasduring motor inhibition (Fallgatter et al., 2002b). The NGA,as well as the underlying Go- and NoGo-centroids, wereshown to have an excellent short- (Fallgatter et al., 2001)and long-term test-retest reliability (Fallgatter et al.,2002a). Adult ADHD patients were characterized by reducedNGA values (Fallgatter et al., 2005), indicating that thisparameter might be an adequate endophenotypic markerfor prefrontal dysfunction during processes of responsecontrol in ADHD. Moreover, an impact of dopaminergic(Dresler et al., 2010; Ehlis et al., 2007), glutamatergic(Fallgatter et al., 2006) and serotonergic (Baehne et al.,2009) genetic polymorphisms on the NGA has been shown,indicating that the NGA constitutes a suitable functionalparameter for imaging genetic studies.
In the present study, we examined if variants of theLPHN3 gene are associated with altered neural activity, i.e.differences in the NGA, in adult ADHD patients. Because ofthe expression of LPHN3 in ADHD relevant brain regions, andbecause of the prominent executive/inhibitory dysfunctionsassociated with the disorder, we hypothesize an influence ofLPHN3 on this measure of prefrontal functioning in an adultADHD sample. Although there is a plethora of findings onERP parameters in ADHD assessing various cognitive pro-cesses (e.g. Doehnert et al., in press; Marzinzik et al.,2012), we focus on a specific response execution/responseinhibition parameter that has proven to be well-suited forour purpose.
2. Materials and methods
2.1. Participants
Two hundred sixteen adult in- and outpatients of the Department ofPsychiatry, Psychosomatics and Psychotherapy of the University ofWuerzburg participated in the study, all fulfilling the diagnosticcriteria for ADHD (according to DSM-IV). Patients gave their writteninformed consent after complete description of the study. Exclusioncriteria were age below 18 and above 60 years, current medicationwith methylphenidate3 or other psychotropic compounds, as well assevere somatic or neurological disorders. Patients were stratifiedaccording to their LPHN3 genotype and grouped into patients witheither two copies of the Latrophilin risk haplotype (‘‘high riskgroup’’, n=114) or a maximum of one copy of the risk haplotype(heterozygous genotype [n=85] or homozygous non-risk haplotype
3Methylphenidate (MPH) acts as an indirect dopamine agonistwith a putative site of action within the prefrontal cortex(cf., Berridge et al., 2006; Spencer et al., 2012; Vaidya et al.,1998). As previous genetic findings could show an impact ofdopaminergic risk alleles on the NGA and CPT-related neurophysiol-ogy (Dresler et al., 2010; Heinzel et al., in press) and the prefrontalcortex is strongly involved in the phenomenon of the NGA(Fallgatter et al., 2002b), we chose to exclude patients treatedwith MPH to avoid confounding effects of this medication. Also, thestrong link of LPHN3 to dopaminergic pathways (see above)contributed to our decision to exclude this potential confound fromour analyses.
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
carriers [n=17]; ‘‘low risk group’’, n=102; cf. Arcos-Burgos et al.,2010). Sample characteristics are given in Table 1. These two groupswere comparable in age, gender distribution, distribution ofhandedness, mean WURS-k score (German short version of theWender Utah Rating Scale; Retz-Junginger et al., 2002)4 and meanverbal IQ estimated according to the MWT-B, a measure of crystal-lized intelligence5. 64 patients of the whole sample belonged to theinattentive subtype of ADHD, 13 to the hyperactive-impulsivesubtype and 139 to the combined subtype. Subtype compositiondid not significantly differ between genotype groups. All patientswere of Caucasian origin. Regarding psychiatric comorbidities, 45out of the 216 ADHD patients (20.8) had a comorbidity with anotheraxis I disorder as assessed via the Structured Clinical Interview forthe DSM-IV (SCID-I). Details regarding comorbidities and medicationcan be found in Table 1.
The study was reviewed and approved by the Ethics Committeeof the University of Wuerzburg, and the procedures involved were inaccordance with the latest version of the Declaration of Helsinki.
2.2. LPHN3 genotyping
For LPHN3 genotyping, we selected four single nucleotide polymorph-isms (SNPs) defining the ADHD-associated at-risk haplotype in thestudy by Arcos-Burgos and associates (Arcos-Burgos et al., 2010):rs2305339, rs734644, rs1397547, and rs1397548. DNA was extractedfrom venous blood using a routine de-salting method. SNPs weregenotyped according to the manufacturer’s instructions by using theSequenom MassArray system (Sequenom, San Diego, CA) coupled to aBruker Autoflex mass spectrometer (Bruker Daltonics, Bremen,Germany). PCR was performed using iPlex chemistry along themanufacturer’s recommendations as found in the MassArray iPlexstandard operation procedure. Primer sequences can be obtained onrequest. All genotyped SNPs were in Hardy–Weinberg equilibrium.Subsequent to genotyping, individual haplotypes were constructedusing the famhap software package (Becker and Knapp, 2004; Heroldand Becker, 2009). Likelihood weight was above 0.96 in every case(means, 0.997). rs2305339—rs734644—rs1397547—rs1397548 AGCCwas defined as the ADHD-risk haplotype H1, whereas all otherhaplotypes were grouped together and designated as No-H1. Indivi-duals carrying two H1 copies were considered as a LPHN3 high riskgroup, while all other subjects were grouped together forming theLPHN3 low risk group.
2.3. Electrophysiological investigation
Patients performed an OX-version of the Continuous PerformanceTest (Rosvold et al., 1956) during registration of the ongoing EEG.The measurement took place in a dimly lit, sound-attenuated andelectrically shielded room. Letters were presented sequentially ona computer screen (viewing distance: 80 cm) in pseudo-randomizedorder. The stimuli were approximately 30 mm high and 20 mm wide,resulting in a visual angle of 2.151 vertically and 1.431 horizontally.Patients were instructed to press a response button only when theletter O was directly followed by the letter X. Speed and accuracywere emphasized equally during explanation of the test. A shorttraining session was performed to ensure correct understanding ofthe instructions. The complete stimulus set consisted of 400 letters
4The WURS-k assesses the severity of earlier childhood ADHDsymptoms by investigating adults retrospectively. The WURS-k scorethus reflects severity of childhood ADHD symptoms for eachparticipant. For a total of 7 patients no WURS-k score was availabledue to single items missing.
5For a total of 7 patients no IQ data were available.
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

Table 1 Sample characteristics.
High-risk (n=114) Low-risk (n=102) Statistics
Age 34.85710.43 34.9279.36 t214=0.052, p=0.96Male/female 58/56 52/50 �2=0.99, p=0.55Right-/left-handed 105/9 95/7 �2=0.77, p=0.49WURS-k score 34.69714.27 36.00713.39 t207=0.68, p=0.50verbal IQ 112.08713.23 110.65713.21 t207=0.78, p=0.43
Subgroup composition (combined/inattentive/hyperactive-impulsive)
74/34/6 65/ 30/ 7 �2=0.24, p=0.89
Comorbidities 22 23 �2=0.35, p=0.56Alcohol dependence 3 3Depressive episode 9 5Agoraphobia 1 2Social phobia 4 4Panic disorder 0 1Generalized anxiety disorder 2 2Obsessive-compulsive disorder 1 3Hypochondriac disorder 0 1Bulimia 2 2
MedicationSSRI 6 9Tricyclic antidepressants 3 2Benzodiazepines 0 2
For a total of 7 patients no WURS-k score was available due to single items missing. For a total of 7 patients no IQ data were available.
A.J. Fallgatter et al.4
(114 letters O=primer condition, 57 X following an O=Go-condition,57 other letters following an O=NoGo-condition, and 172 letters notfollowing an O=distractors) with a stimulus-onset asynchrony (SOA)of 1850 ms and a stimulus presentation time of 200 ms. The wholeCPT procedure lasted about 15 min.
The current version of the CPT allows for an examination of Goand NoGo processes at the same time (both of which also contributeto the calculation of the NGA; see above). Since the P300 isparticularly sensitive to stimulus probability, both conditions canbe directly compared only with an equal probability of Go and NoGotrials. In order to provoke response preparation and thereby motorinhibition in NoGo trials, we—therefore—chose not to manipulatethe Go:NoGo ratio (which would be one way to ensure heightenedinhibitory control in NoGo trials, if for example an 80:20 ratio ofGo:NoGo trials was chosen), instead including a primer (‘‘cuedCPT’’) which preceded both Go and NoGo trials thus provokingresponse preparation in either case. That way, prepared motorresponses had to be suppressed in the NoGo condition, hopefullyinvolving about the same amount of inhibitory control that wouldalso have been provoked by unequal stimulus probabilities (e.g.Eimer, 1993). Beyond that, as we were not only interested ininhibition processes but also in general cognitive and motor control,respectively, an equal probability of Go and NoGo trials seemed themost suited.
During performance of the task, the EEG was recorded from 21 scalpelectrodes placed according to the International 10/20-System (Jasper,1958). Three additional electrodes were attached at the outer canthi ofboth eyes and below the right eye for registration of eye movements.The technical equipment consisted of a 32-channel DC-amplifierand the recording software Vision Recorder (Brain Products,Munich, Germany). The hardware filter was set to a bandpass from
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
0.1–100 Hz; A/D rate was 1000 Hz. The recording reference was placedbetween Fz and Cz, the ground electrode between Fpz and Fz.All electrode impedances were kept below 5 k.
2.4. Data analysis
Electrophysiological data were processed using the Vision Analyzersoftware (Brain Products, Munich, Germany). As a first step, data werefiltered offline with a bandpass from 0.1 to 70 Hz and re-referenced toan average reference. They were corrected for ocular artifacts usingthe standard algorithm implemented in the software (Gratton andColes, 1989). After a computerized artifact rejection (only amplitudeso70 V were allowed in all EEG-channels within 100 ms before and700 ms after stimulus presentation), the artifact-free epochs aftercorrect responses were segmented and individually averaged to oneGo- and one NoGo- event-related potential (ERP). For the NoGo-ERP,the time point of the most positive peak at electrode position Czwithin a P300 time-window (277–434 ms) (Fallgatter et al., 1997) wasused to calculate the two-dimensional topography by means of thecentroid method (Lehmann, 1987), whereas the respective peak atelectrode position Pz was used for the Go-condition. The location ofeach individual centroid on an anterior-posterior axis was determinedby numbers from 1 (level of electrode position Fpz) to 5 (level of Oz)as illustrated in Figure 1 (locations somewhere in between twoelectrode positions were expressed by respective decimal numbers).Smaller values of centroid-locations indicate a more anterior localiza-tion. For a more detailed description of the centroid-method,please confer the work of Lehmann (Lehmann, 1987) and ourprevious publications (e.g., Fallgatter et al., 1997). The individual
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

0
0.2
0.4
0.6
0.8
high risk low risk
NGA
*
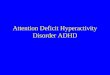
Figure 1 Grand average curves for the CPT Go (blue; Pz) and NoGo condition (red; Cz) in patients with no copy (n=17) or one copy(n=85) of the LPHN3 risk haplotype (low risk group; A) vs. patients homozygous for the risk haplotype (n=114; high risk group; B).Maps above the curves display the brain electrical field at the time-point of the P300 peak at Pz (Go condition; left map of a pair)and Cz (NoGo condition; right map of a pair), respectively. The difference map for the comparison of the two haplotype groups withrespect to the Go-centroid (high minus low risk group) is depicted in the left part of the figure (C). Right panel depicts the mainresult of a reduced NoGo-Anteriorization in LPHN3 high risk carriers (vertical bars represent the standard error of the mean) (D).(For interpretation of references to color in this figure legend, the reader is referred to the web version of this article.)
5Latrophilin 3 and response control processes in ADHD
NoGo-Anteriorization (NGA) was calculated as the difference betweenthe Go- and NoGo-centroid on the anterior–posterior axis.
2.5. Statistical analysis
All statistical analyses were performed with the software SPSS forWindows (version 14.0). For the P300 centroids, a 2� 2 analysis ofvariance (ANOVA) was conducted, comprising the between subjectfactor ‘‘genotype’’ and the within-subject factor ‘‘CPT condition’’(Go vs. NoGo). Post-hoc analyses were calculated by means of two-tailed t-tests for independent samples for between-group compar-isons of the Go- and NoGo-centroid as well as the NGA. T-tests werealso used to compare mean Go reaction times between the twogenotype groups. Equality of variances was tested by means ofLevene’s test and corrections for unequality were performed whennecessary. Since none of the CPT error data (number of commissionerrors after NoGo stimuli; commission errors after primers ordistractors; number of omission errors) was normally distributedaccording to Kolmogorov–Smirnov’s Z-statistic (all p-valueso0.001), Mann–Whitney U-tests were used for between-groupcomparisons of these variables. The significance level was set topo0.05. We derived our hypotheses for the risk haplotype from therecently published literature and intended to test these in a firststudy on the functional impact of the LPHN3 risk haplotype onspecific parameters of brain function in ADHD. For this first,exploratory analysis we think that our methodological approach offoregoing a strict correction for multiple testing is warranted.
2.6. sLORETA source localization analyses
Source localization of between-group differences in topographicalERP data was carried out using standardized low resolution brain
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
electromagnetic tomography (sLORETA) (Fuchs et al., 2002; Jurcaket al., 2007; Pascual-Marqui, 2002). sLORETA is a weighted mini-mum norm inverse solution for EEG/MEG data used to computestatistical maps from scalp potentials indicating the location ofunderlying neural sources with small error. Briefly, sLORETA calcu-lates the standardized current density at 6239 Gy matter voxels inthe cortex, ACC and hippocampus of the MNI-reference brain underthe assumption that neighboring voxels should have a maximallysimilar electrical activity. The inverse solution was computedseparately per condition and subject. In order to detect sourcesfor between-group differences, comparison of LPHN3 groups wasconducted for each voxel using the non-parametric method imple-mented in the software, performing randomization (5000 permuta-tions) and correcting for multiple comparisons (Pascual-Marqui,2002). Specifically, voxel-based sLORETA images were comparedbetween genotype groups for the time-point of the mean Golatency of the P300 across the whole study sample (350 ms; low-risk group, n=102: 344749 ms; high-risk group, n=114:353741 ms). Log of ratio of averages was used and consideredwith a 5 level of significance.
3. Results
3.1. Behavioral data
The two genotype groups did not differ significantly regardingtheir mean reaction times to Go-stimuli (low risk group:511.447117.58 ms vs. high risk group: 490.527115.34 ms;t214=1.32, p=0.19). Mann–Whitney U-tests also indicated asimilar number of commission errors after NoGo stimuli andafter primers/ distractors (U=5647.0 and 5408.5, respectively;
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

0.5-0.5 0.25-0.25 0Log of ratio of averages
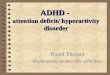
Figure 2 Source localization of the difference in P300 data between genotype groups for the Go conditions of the CPT; sLORETAimage displays the maximum difference, which was found in Brodman Area 10 (middle frontal gyrus) where patients of the LPHN3low risk group (n=102) tended to exhibited stronger activation values than patients of the high risk group (n=114; p=0.1).
Figure 3 Analysis of potential gene-dose effects for omission errors (left panel) and the NGA (right panel).
A.J. Fallgatter et al.6
Z=�0.61 and �0.94; p40.35), however, patients with a highrisk genotype made significantly more omission errors thanpatients of the low risk group (U=4796.0, Z=�2.29, p=0.02).Reaction time variability was comparable between the twogenotype groups (t214=0.169, p=0.866).
6Due to the left-lateralized finding, we repeated the analysis forright-handers only, in order to exclude the possibility of a con-founding influence of patients’ handedness. This analysis confirmedthe reported finding with overall stronger effects (minimalp=0.042) and a significant impact of LPHN3 genotype on left-frontal structures (BA 10 and 46; left middle frontal gyrus as well asleft inferior and superior frontal gyrus).
3.2. ERP data
The grand average ERPs and mean centroids of bothgenotype groups are shown in Figure 1, along with aschematic illustration of the quantification of the NGA asthe geometrical distance between the Go- and NoGo-centroid. The 2� 2 ANOVA for the centroids revealed asignificant main effect ‘‘CPT condition’’ (F1, 214=471.10,po0.001) as well as a significant interaction ‘‘CPT conditionx genotype’’ (F1, 214=3.96, po0.05). No significant maineffect ‘‘genotype’’ occurred (F1, 214=2.08, p=0.15). Post-hoc analyses revealed that the two genotype groups did notdiffer significantly regarding their NoGo-centroids (high riskgroup: 3.0370.40 vs. low risk group: 3.0470.41; t214=0.15,p=0.88), however, patients of the high risk group displayedGo-centroids that were located significantly more anterior
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
(3.6270.43) than Go-centroids of the low risk group(3.7570.39; t214=2.26, p=0.025). This topographical ERPfinding was accompanied by a statistical trend for reducedactivation within the left middle frontal gyrus (BA 10; MNIcoordinates according to sLORETA software: �40, 45, 25;p=0.1) in LPHN3 high risk carriers (see Figure 2)6. Thedifferential impact of LPHN3 genotype on Go- and NoGo-centroids resulted in a significantly reduced mean NGA inpatients of the high risk (0.5970.46) as compared to thelow risk group (0.7170.42; t214=1.99; po0.05). The maineffect ‘‘CPT condition’’ indicated that NoGo-centroids werelocated significantly more anterior than Go-centroids acrossthe whole sample of ADHD patients (mean Go-centroid:3.6870.42; mean NoGo-centroid: 3.0370.40), which reflectsthe well known finding of the NoGo-Anteriorization (NGA).
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

7Latrophilin 3 and response control processes in ADHD
Neither the NGA nor the centroids were significantly corre-lated with WURS-k scores (�0.05oro0.06; p40.4). P300latencies for Go- and NoGo-trials did not differ significantlybetween the haplotype groups (t214o1.53, p40.13). Theelectrophysiological data did not correlate with the beha-vioral data. Results remained virtually unchanged, whenpatients with a current tricyclic medication were excludedfrom the analysis. Adjusting the analyses for effects of ageand sex did not change the results.
We split the sample into three separate groups (0 [n=17]vs. 1 [n=85] vs. 2 risk haplotypes [n=114]) and checked inan additional analysis whether there were any gene-doseeffects. For the omission errors there was a significantlinear trend (F1, 213=5.244, p=0.023); however, this effectwas mainly driven by the group with 2 risk haplotypes, i.e.the groups with 0 and 1 risk haplotype did not substantiallydiffer (see Figure 3). The same was found for the NGA (seeFigure 3). The linear trend test revealed a marginallysignificant effect (F1, 213=3.336, p=0.069), but this wasalso due to the group with 2 risk haplotypes withoutdifferences between the other two groups. This analysis ofthe gene-dosage model suggests a recessive rather than anadditive effect of LPHN3.
4. Discussion
In the present EEG study we investigated if LPHN3, ahaplotype presumably conveying susceptibility for ADHD(Arcos-Burgos et al., 2004), is associated with a neuralmarker of cognitive response control that has been found tobe aberrant in adult ADHD patients (the so-called ‘‘NoGo-Anteriorization’’ or NGA; Fallgatter et al., 2005). To thisend, we compared two groups of adult ADHD patients, onebeing homozygous for the risk haplotype (high risk group)and the other one carrying at least one copy of the non-riskhaplotype (low risk group), regarding their behavioral andERP responses during a primed Go-NoGo task (ContinuousPerformance Test, CPT) which has been shown to representa suitable paradigm for endophenotype research in ADHD(Uebel et al., 2010). In previous CPT studies with controlpopulations, the general behavioral and ERP findings can besummarized as follows (Fallgatter et al., 2004, 2005;Baehne et al., 2009; Dresler et al., 2010): Controls showan increased frontalization of the brain electrical (P300)field during NoGo trials (as indexed by the topographicalERP parameter of the NGA) as compared to childhood andadult ADHD populations. They also generally make lessomission and commission errors, show reduced reactiontimes and also a significantly reduced reaction time varia-bility. NoGo-related ACC function has been shown to bereduced in ADHD patients compared to controls.
In line with our hypotheses, we found a significant impactof LPHN3 haplotype on ERPs evoked by the CPT, with asignificantly reduced NGA in the high risk group of patients.Remarkably, this effect was solely carried by differences inthe Go-centroid (brain electrical distribution of the P300during Go-trials), which showed a significantly more anteriorlocation in the high risk as compared to the low risk group,with a tendency for reduced activation within the middlefrontal gyrus (BA 10) according to sLORETA source localiza-tion. The NoGo-centroid however, which has primarily been
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
associated with processes of inhibitory control, was verysimilar for both groups of patients. These findings are inremarkable accordance with the results of Fallgatter et al.(2005), who found a significantly reduced mean NGA in adultpatients with a probable childhood ADHD that was mainlyattributable to a significantly more anterior location of theGo-centroid in patients as compared to healthy and psychia-tric controls. In line with our electrophysiological findings,analyses of the behavioral data showed that patients of thehigh risk LPHN3 group made more omission errors (i.e. noresponse to a Go-stimulus) than patients of the low riskgroup, whereas reaction times and commission errors (i.e.button presses following NoGo, primer, or distractor stimuli)were comparable for both haplotypes. Behavioral data,therefore, confirmed abnormalities in the high risk group ofADHD patients during the execution of primed motorresponses, without indicating a specific influence of LPHN3on processes of inhibitory control. Given the attentionalnature of many ADHD symptoms, it should also be consideredthat differences in omission errors may indicate differencesin inattention between genotype groups without beingspecifically related to processes of response or motor control.
Taken together, these findings show that a functionalhaplotype recently associated with the diagnosis of ADHD(Arcos-Burgos et al., 2010) is also related to basic neuralactivity and processes of cognitive response control (andpossibly attention in general) in these patients. The haplo-type group more susceptible for ADHD (the high risk group)showed an altered pattern of neural activation, as well asbehavioral deficits, during the execution of prepared motorresponses. Since impaired processes of attentional andmotor control have been proposed to be specifically relatedto (the genetic vulnerability for) ADHD (compare Slaats-Willemse, 2003), this finding nicely links a putative geneticrisk factor (LPHN3 risk haplotype) to an endophenotypicmarker of the disease. Since both haplotype groups werecomparable with respect to various possible confounds,including the distribution of ADHD subtype diagnoses (seeSection 2), the above described differences cannot simplybe explained by differences in any of the registeredconfounding factors.
The underlying neurobiological mechanisms of LPHN3 andits endogenous function in vertebrates are far from beingunderstood. Currently, it is discussed if LPHN3 mutations mayimpact the development of synaptic circuits: fibronectinleucine-rich repeat transmembrane (FLRT) proteins havebeen found to act as endogenous LPHN3 ligands and in-vitrofindings indicate an involvement of the FLRT3–LPHN3 com-plex in glutamatergic synapse development (O’Sullivan et al.,2012). Such developmental pathways may alter general task-dependent circuit activity by modifying glutamatergic-GABAergic balance in subcortical and cortical brain areas.A possible relationship of FLRT3 copy number variations withADHD (Lionel et al., 2011) hints at a putative mechanismmediating the development of ADHD symptoms. As LPHN3 isexpressed in brain structures belonging to the nigrostriatal,the mesolimbic, and the mesocortical dopaminergic systems(Martinez et al., 2011), interaction with prefrontal cortexactivity is quite likely and may explain differences in theinvestigated neurophysiological marker. However, these pre-liminary findings—without further support from in-vitro andin-vivo studies—have yet to be considered with caution.
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

A.J. Fallgatter et al.8
In our study, several limitations need to be considered.First, the statistical effects—though existent—are rathersmall (po0.05), indicating small haplotype effects onbehavioral and neurophysiological measures of cognitiveresponse control in ADHD. Thus, results may also representfalse positive errors. However, as we had explicit hypoth-eses derived from recent literature regarding the directionof effects, and genetic effects were not expected to belarge, we deem our results meaningful in a way that theyadd to the existing knowledge about the complex geneticinfluences in psychiatric disorders such as ADHD. Theconvergence of an association on a categorical level(Arcos-Burgos et al., 2010) and our support for an associa-tion on an endophenotypic supports a contribution of LPHN3to ADHD pathogenesis. Second, about 20 of the investigatedsample had psychiatric comorbidities that might haveaffected the present findings, even if these comorbiditiesare commonly associated with ADHD (Jacob et al., 2007).However, since comorbidity distribution across genotypegroups was rather even and ADHD was always the primarydiagnosis, we consider our sample to be representative forthe ADHD population. Third, a control sample stratified forthe respective haplotype is missing in our analyses. There-fore, our results—though hypothesis-driven—have to beconsidered preliminary and explorative. Nonetheless, anendophenotypic effect of the same LPHN3 haplotype pre-viously associated with ADHD (Arcos-Burgos et al., 2010)further supports the assumed involvement of LPHN3 in ADHDpathogenesis. Fourth, although we investigated a ratherlarge sample for an imaging genetic study, it is relativelysmall as compared to genetic association studies which mayprevent detecting genetic influences that—as singlegenes—actually only share a small proportion on the overalllarge hereditary influences in genetically complex disorderssuch as ADHD. Fifth, the sLORETA results have to beconsidered with caution as the (limited) number of electro-des prevents a more precise localization, which might havebeen most critical for localizing deeper structures such asthe hippocampus or ACC. Adding to that, effects wedetected were rather weak on a statistical level. Therefore,the sLORETA analysis should be considered preliminary.What increases our confidence in the findings is the factthat a prefrontal structure plausibly involved in processes ofcognitive response control (the middle frontal gyrus) wasdetected as the source of our topographical ERP findings andthat the results of the source localization were exactlyreplicated (with increased statistical significance) in asubgroup of patients including only right-handers (withseveral neighboring voxels showing the same effect).
Recently, theoretical and conceptual aspects of theendophenotype concept have been considered in the scien-tific community stressing the importance of differentiatingbetween mediational (i.e. the endophenotype mediates therelation from gene to disorder) and liability-index models(i.e. the endophenotype is risk-indicating and may only bean epiphenomenon) and of considering bidirectional rela-tionships of endophenotype and disorder (Kendler andNeale, 2010). Beyond that, relationships may be morecomplex with endophenotypes also reflecting environmentalinfluences, and some genetic influences may only affect theendophenotype while others only affect the clinical symp-toms. This indicates that with our investigation we can only
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
cover a part of the gene-disorder-relationship, and addi-tional prospective studies using multivariate analyses areneeded to further elucidate the complex aetiopathologyof mental disorders. As genetic influences may changeover the life course (Dresler et al., 2010; Franke et al.,2010), it also has to be mentioned that our results onlyapply to adult ADHD patients as there is no data availablefor children.
To our best knowledge, our study is the first to show aninfluence of the LPHN3 susceptibility haplotype on beha-vioral and neurophysiological responses of adult ADHDpatients in an executive function task. The results of ourstudy further strengthen the concept of an LPHN3 riskhaplotype for ADHD, and seem to implicate that motorcontrol processes might be a basic cognitive mechanismmediating a respective genetic influence on overt behavior(symptomatology). The significant (behavioral and neuro-physiological) differences between both haplotype groupswithin a clinical group of ADHD patients might furthermoreindicate that the LPHN3 risk haplotype is related to aspecific subtype of the disorder, going beyond the subtypesdefined by DSM-IV. Since the LPHN3 risk haplotype isassociated with a significantly decreased NAA/Cr ratio inbrain regions also associated with ADHD pathology (seeintroduction, Arcos-Burgos et al., 2010; Krain and Cas-tellanos, 2006), we propose that a pathologically alteredfunction (i.e. neuronal loss or damage) in these brainregions underlies the impact of LPHN3 on cognitiveresponse control and, thereby, ADHD symptomatology.In summary, our findings support a link between LPHN3and behavioral and neurophysiological measures of cog-nitive response control in ADHD patients, and once againemphasize the usefulness of the endophenotypeapproach in psychiatric and psychological research toelucidate putative etiological pathways.
Role of funding source
This study was supported by the Deutsche Forschungsgemeinschaft(KFO 125-1/2 to A.J.F., C.P.J., A.R. and K.P.L.; SFB/TRR 58 to A.J.F.,A.R., K.P.L. and A.C.E.). The Deutsche Forschungsgemeinschaft hadno further role in study design; in the collection, analysis andinterpretation of data; in the writing of the report; and in thedecision to submit the paper for publication.
Contributors
Authors A.J.F, K.P.L., A.C.E., M.A.B. and M.M. designed the studyand wrote the protocol. Authors A.C.E., T.D. and C.P.J. managedthe literature searches and analyses. Authors A.C.E. and T.D.undertook the statistical analysis and A.J.F., A.C.E. and T.D. wrotethe first draft of the manuscript. Authors A.R. and K.P.L. performedgenetic analyses and together with M.A.B. and M.M. wrote thegenetics part of the manuscript. All authors contributed to and haveapproved the final version of the manuscript.
Conflict of interest
The authors declare that they have no conflicts of interest.
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

9Latrophilin 3 and response control processes in ADHD
Acknowledgments
We would like to thank Andrea Boreatti-Hummer and Monika Heinefor the help in diagnosing patients and Christina G. Bahne, IngeGrobner and Melanie Harder for the help in data collection.
References
Almasy, L., Blangero, J., 2001. Endophenotypes as quantitative riskfactors for psychiatric disease: rationale and study design. Am.J. Med. Genet. 105, 42–44.
Arcos-Burgos, M., Castellanos, F.X., Pineda, D., Lopera, F., Palacio, J.D.,Palacio, L.G., Rapoport, J.L., Berg, K., Bailey-Wilson, J.E., Muenke,M., 2004. Attention-deficit/hyperactivity disorder in a populationisolate: linkage to loci at 4q13.2, 5q33.3, 11q22, and 17p11. Am. J.Hum. Genet. 75, 998–1014.
Arcos-Burgos, M., Jain, M., Acosta, M.T., Shively, S., Stanescu, H.,Wallis, D., Domene, S., Velez, J.I., Karkera, J.D., Balog, J.,Berg, K., Kleta, R., Gahl, W.A., Roessler, E., Long, R., Lie, J.,Pineda, D., Londono, A.C., Palacio, J.D., Arbelaez, A., Lopera, F.,Elia, J., Hakonarson, H., Johansson, S., Knappskog, P.M.,Haavik, J., Ribases, M., Cormand, B., Bayes, M., Casas, M.,Ramos-Quiroga, J.A., Hervas, A., Maher, B.S., Faraone, S.V.,Seitz, C., Freitag, C.M., Palmason, H., Meyer, J., Romanos, M.,Walitza, S., Hemminger, U., Warnke, A., Romanos, J., Renner, T.,Jacob, C., Lesch, K.P., Swanson, J., Vortmeyer, A., Bailey-Wilson, J.E., Castellanos, F.X., Muenke, M., 2010. A commonvariant of the latrophilin 3 gene, LPHN3, confers susceptibility toADHD and predicts effectiveness of stimulant medication. Mol.Psychiatry 15, 1053–1066.
Baehne, C.G., Ehlis, A.C., Plichta, M.M., Conzelmann, A., Pauli, P.,Jacob, C., Gutknecht, L., Lesch, K.P., Fallgatter, A.J., 2009.Tph2 gene variants modulate response control processes in adultADHD patients and healthy individuals. Mol. Psychiatry 14,1032–1039.
Barkley, R., 1998. Attention-deficit hyperactivity disorder: A Hand-book for Diagnosis and Treatment, 2nd edition Guilford, NewYork.
Barkley, R.A., 1997. Behavioral inhibition, sustained attention, andexecutive functions: constructing a unifying theory of ADHD.Psychol. Bull. 121, 65–94.
Barkley, R.A., Grodzinsky, G., DuPaul, G.J., 1992. Frontal lobefunctions in attention deficit disorder with and without hyper-activity: a review and research report. J. Abnorm. Child Psychol.20, 163–188.
Becker, T., Knapp, M., 2004. Maximum-likelihood estimation ofhaplotype frequencies in nuclear families. Genet. Epidemiol.27, 21–32.
Berridge, C.W., Devilbiss, D.M., Andrzejewski, M.E., Arnsten, A.F.,Kelley, A.E., Schmeichel, B., Hamilton, C., Spencer, R.C., 2006.Methylphenidate preferentially increases catecholamine neuro-transmission within the prefrontal cortex at low doses thatenhance cognitive function. Biol. Psychiatry 60, 1111–1120.
Biederman, J., 2005. Attention-deficit/hyperactivity disorder: aselective overview. Biol. Psychiatry 57, 1215–1220.
Birnbaum, H.G., Kessler, R.C., Lowe, S.W., Secnik, K., Greenberg, P.E.,Leong, S.A., Swensen, A.R., 2005. Costs of attention deficit-hyperactivity disorder (ADHD) in the US: excess costs of personswith ADHD and their family members in 2000. Curr. Med. Res.Opin. 21, 195–206.
Bookheimer, S.Y., Strojwas, M.H., Cohen, M.S., Saunders, A.M.,Pericak-Vance, M.A., Mazziotta, J.C., Small, G.W., 2000. Pat-terns of brain activation in people at risk for Alzheimer’sdisease. N. Engl. J. Med. 343, 450–456.
Borger, N., van der Meere, J., 2000. Motor control and stateregulation in children with ADHD: a cardiac response study. Biol.Psychol 51, 247–267.
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
Bush, G., Frazier, J.A., Rauch, S.L., Seidman, L.J., Whalen, P.J.,Jenike, M.A., Rosen, B.R., Biederman, J., 1999. Anteriorcingulate cortex dysfunction in attention-deficit/hyperactivitydisorder revealed by fMRI and the counting stroop. Biol.Psychiatry 45, 1542–1552.
Dhar, M., Been, P.H., Minderaa, R.B., Althaus, M., 2010. Informationprocessing differences and similarities in adults with dyslexiaand adults with attention deficit hyperactivity disorder during acontinuous performance test: a study of cortical potentials.Neuropsychologia 48 (10), 3045–3056.
Doehnert, M., Brandeis, D., Schneider, G., Drechsler, R., Steinhausen,H.C. A neurophysiological marker of impaired preparation in an11-year follow-up study of attention-deficit/hyperactivity disorder(ADHD). J. Child Psychol. Psychiatry 10.1111/j.1469-7610.2012.02572.x, in press.
Domene, S., Stanescu, H., Wallis, D., Tinloy, B., Pineda, D.E., Kleta, R.,Arcos-Burgos, M., Roessler, E., Muenke, M., 2011. Screening ofhuman LPHN3 for variants with a potential impact on ADHDsusceptibility. Am. J. Med. Genet. B 156B, 11–18.
Dopfner, M., Lehmkuhl, G., 2006. Aufmerksamkeitsdefizit-/Hyper-aktivitatsstorung — Neuropsychologie. In: Forstl, H., Hautzinger, M.,Roth, G. (Eds.), Neurobiologie psychischer Storungen. SpringerMedizin Verlag, Heidelberg, pp. 671–689.
Dresler, T., Ehlis, A.C., Heinzel, S., Renner, T.J., Reif, A., Baehne, C.G.,Heine, M., Boreatti-Hummer, A., Jacob, C.P., Lesch, K.P., Fallgatter,A.J., 2010. Dopamine transporter (SLC6A3) genotype impactsneurophysiological correlates of cognitive response control in anadult sample of patients with ADHD. Neuropsychopharmacology 35,2193–2202.
Egan, M.F., Goldberg, T.E., Kolachana, B.S., Callicott, J.H.,Mazzanti, C.M., Straub, R.E., Goldman, D., Weinberger, D.R.,2001. Effect of COMT Val108/158 Met genotype on frontal lobefunction and risk for schizophrenia. Proc. Natl. Acad. Sci. USA98, 6917–6922.
Ehlis, A.C., Reif, A., Herrmann, M.J., Lesch, K.P., Fallgatter, A.J.,2007. Impact of catechol-O-methyltransferase on prefrontalbrain functioning in schizophrenia spectrum disorders. Neurop-sychopharmacology 32, 162–170.
Eimer, M., 1993. Effects of attention and stimulus probability onERPs in a Go/Nogo task. Biol. Psychol. 35, 123–138.
Fallgatter, A.J., Aranda, D.R., Bartsch, A.J., Herrmann, M.J.,2002a. Long-term reliability of electrophysiologic response con-trol parameters. J Clin. Neurophysiol. 19, 61–66.
Fallgatter, A.J., Bartsch, A.J., Herrmann, M.J., 2002b. Electrophy-siological measurements of anterior cingulate function.J. Neural Transm. 109, 977–988.
Fallgatter, A.J., Bartsch, A.J., Strik, W.K., Mueller, T.J., Eisenack, S.S.,Neuhauser, B., Aranda, D., Herrmann, M.J., 2001. Test-retestreliability of electrophysiological parameters related to cognitivemotor control. Clin. Neurophysiol. 112, 198–204.
Fallgatter, A.J., Brandeis, D., Strik, W.K., 1997. A robust assess-ment of the NoGo-anteriorisation of P300 microstates in a cuedcontinuous performance test. Brain Topogr. 9, 295–302.
Fallgatter, A.J., Ehlis, A.C., Rosler, M., Strik, W.K., Blocher, D.,Herrmann, M.J., 2005. Diminished prefrontal brain function inadults with psychopathology in childhood related to attentiondeficit hyperactivity disorder. Psychiatry Res. 138, 157–169.
Fallgatter, A.J., Herrmann, M.J., Hohoff, C., Ehlis, A.C., Jarczok, T.A.,Freitag, C.M., Deckert, J., 2006. DTNBP1 (dysbindin) gene variantsmodulate prefrontal brain function in healthy individuals. Neurop-sychopharmacology 31, 2002–2010.
Fallgatter, A.J., Jatzke, S., Bartsch, A.J., Hamelbeck, B., Lesch, K.P.,1999. Serotonin transporter promoter polymorphism influencestopography of inhibitory motor control. Int. J. Neuropsychophar-macol. 2, 115–120.
Fallgatter, A.J., Strik, W.K., 1999. The NoGo-anteriorization as aneurophysiological standard-index for cognitive response con-trol. Int. J. Psychophysiol. 32, 233–238.
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

A.J. Fallgatter et al.10
Faraone, S.V., Doyle, A.E., 2000. Genetic influences on attentiondeficit hyperactivity disorder. Curr. Psychiatry Rep. 2, 143–146.
Faraone, S.V., Perlis, R.H., Doyle, A.E., Smoller, J.W., Goralnick, J.J.,Holmgren, M.A., Sklar, P., 2005. Molecular genetics of attention-deficit/hyperactivity disorder. Biol. Psychiatry 57, 1313–1323.
Franke, B., Arias Vasquez, A., Johansson, S., Hoogman, M.,Romanos, J., Boreatti-Huemmer, A., et al., 2010.Meta-analysisof the SLC6A3/DAT1 VNTR haplotype in adult ADHD suggestsdifferential involvement of the gene in adult and childhoodADHD. Neuropsychopharmacology 35, 656–664.
Franke, B., Faraone, S.V., Asherson, P., Buitelaar, J., Bau, C.H.,Ramos-Quiroga, J.A., Mick, E., Grevet, E.H., Johansson, S.,Haavik, J., Lesch, K.P., Cormand, B., Reif, A., 2012. Thegenetics of attention deficit/hyperactivity disorder in adults, areview. Mol. Psychiatry 17/10, 1476–5578.
Fuchs, M., Kastner, J., Wagner, M., Hawes, S., Ebersole, J.S., 2002.A standardized boundary element method volume conductormodel. Clin. Neurophysiol. 113, 702–712.
Gizer, I.R., Ficks, C., Waldman, I.D., 2009. Candidate gene studiesof ADHD: a meta-analytic review. Hum. Genet. 126, 51–90.
Gratton, G., Coles, M.G.H., 1989. Generalization and evaluation ofeye-movement correction procedures. J. Psychophysiol. 3, 1–50.
Hanisch, C., Radach, R., Holtkamp, K., Herpertz-Dahlmann, B.,Konrad, K., 2006. Oculomotor inhibition in children withand without attention-deficit hyperactivity disorder (ADHD).J. Neural Transm. 113, 671–684.
Hariri, A.R., Mattay, V.S., Tessitore, A., Kolachana, B., Fera, F.,Goldman, D., Egan, M.F., Weinberger, D.R., 2002. Serotonintransporter genetic variation and the response of the humanamygdala. Science 297, 400–403.
Hariri, A.R., Weinberger, D.R., 2003. Imaging genomics. Br. Med.Bull. 65, 259–270.
Heinzel, S., Dresler, T., Baehne, C.G., Heine, M., Boreatti-Hummer, A.,Jacob, C.P., Renner, T.J., Reif, A., Lesch, K.P., Fallgatter, A.J.,Ehlis, A.C.. COMT x DRD4 epistasis impacts prefrontalcortex function underlying response control. Cerebral Cortex,10.1093/cercor/bhs132, in press.
Herold, C., Becker, T., 2009. Genetic association analysis withFAMHAP: a major program update. Bioinformatics 1, 134–136.
Ichtchenko, K., Khvotchev, M., Kiyatkin, N., Simpson, L., Sugita, S.,Sudhof, T.C., 1998. Alpha-latrotoxin action probed with recom-binant toxin: receptors recruit alpha-latrotoxin but do nottransduce an exocytotic signal. EMBO J. 17, 6188–6199.
Jacob, C.P., Romanos, J., Dempfle, A., Heine, M., Windemuth-Kieselbach, C., Kruse, A., Reif, A., Walitza, S., Romanos, M.,Strobel, A., Brocke, B., Schafer, H., Schmidtke, A., Boning, J.,Lesch, K.P., 2007. Co-morbidity of adult attention-deficit/hyperactivity disorder with focus on personality traits andrelated disorders in a tertiary referral center. Eur. Arch.Psychiatry Clin. Neurosci. 257, 309–317.
Jasper, H., 1958. Report of committee on methods of clinical examin EEG. Electroencephalogr Clin. Neurophysiol. 10, 370–375.
Jurcak, V., Tsuzuki, D., Dan, I., 2007. 10/20, 10/10, and 10/5systems revisited: their validity as relative head-surface-basedpositioning systems. Neuroimage 34, 1600–1611.
Kendler, K.S., Neale, M.C., 2010. Endophenotype: a conceptualanalysis. Mol. Psychiatry 15, 789–797.
Kessler, R.C., Adler, L., Barkley, R., Biederman, J., Conners, C.K.,Demler, O., Faraone, S.V., Greenhill, L.L., Howes, M.J., Secnik, K.,Spencer, T., Ustun, T.B., Walters, E.E., Zaslavsky, A.M., 2006. Theprevalence and correlates of adult ADHD in the United States:results from the National Comorbidity Survey Replication. Am. J.Psychiatry 163, 716–723.
Krain, A.L., Castellanos, F.X., 2006. Brain development and ADHD.Clin. Psychol. Rev. 26, 433–444.
Lehmann, D., 1987. Principles of spatial analysis. In: Gevins, A.,Remond, A. (Eds.), Handbook of Electroencephalographyand Clinical NeurophysiologyMethods of Analysis of Brain
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
Electrical and Magnetic Signals, vol. 1. Elsevier, Amsterdam,pp. 309–354.
Levy, F., Hay, D.A., McStephen, M., Wood, C., Waldman, I., 1997.Attention-deficit hyperactivity disorder: a category or a con-tinuum? Genetic analysis of a large-scale twin study. J. Am.Acad. Child Psychiatry 36, 737–744.
Lionel, A.C., Crosbie, J., Barbosa, N., Goodale, T., Thiruvahin-drapuram, B., Rickaby, J., Gazzellone, M., Carson, A.R.,Howe, J.L., Wang, Z., et al., 2011.Rare copy number varia-tion discovery and cross-disorder comparisons identify riskgenes for ADHD. Sci. Translational Med. 3, 95ra75.
Losier, B.J., McGrath, P.J., Klein, R.M., 1996. Error patterns on thecontinuous performance test in non-medicated and medicatedsamples of children with and without ADHD: a meta-analyticreview. J. Child Psychol. Psychiatry 37, 971–987.
Mannuzza, S., Klein, R.G., Bessler, A., Malloy, P., LaPadula, M.,1993. Adult outcome of hyperactive boys. Educational achieve-ment, occupational rank, and psychiatric status. Arch. Gen.Psychiatry 50, 565–576.
Martel, M., Nikolas, M., Nigg, J.T., 2007. Executive function inadolescents with ADHD. J. Am. Acad. Child Psychiatry 46,1437–1444.
Martin, N., Scourfield, J., McGuffin, P., 2002. Observer effects andheritability of childhood attention-deficit hyperactivity disordersymptoms. Br. J. Psychiatry 180, 260–265.
Martinez, A.F., Muenke, M., Arcos-Burgos, M., 2011. From the blackwidow spider to human behavior: Latrophilins, a relativelyunknown class of G protein-coupled receptors, are implicatedin psychiatric disorders. Am. J. Med. Genet. B: Neuropsychiatr.Genet. 156, 1–10.
Marzinzik, F., Wahl, M., Kruger, D., Gentschow, L., Colla, M.,Klostermann, F., 2012. Abnormal distracter processing in adults withattention-deficit-hyperactivity disorder. PLoS One 7 (3), e33691.
Matza, L.S., Paramore, C., Prasad, M., 2005. A review of theeconomic burden of ADHD. Cost effect. Res. Allocation 3, 5.
Nigg, J.T., 1999. The ADHD response-inhibition deficit as measured bythe stop task: replication with DSM-IV combined type, extension, andqualification. J. Abnorm. Child. Psychiatry 27, 393–402.
O’Sullivan, M.L., de Wit, J., Savas, J.N., Comoletti, D., Otto-Hitt,S., Yates III, J.R., Ghosh, A., 2012. FLRT proteins are endogen-ous latrophilin ligands and regulate excitatory synapse develop-ment. Neuron 73, 903–910.
Pascual-Marqui, R.D., 2002. Standardized low-resolution brainelectromagnetic tomography (sLORETA): technical details.Methods Find Exp. Clin. Pharmacol. 24 (Suppl. D), 5–12.
Polanczyk, G., de Lima, M.S., Horta, B.L., Biederman, J., Rohde, L.A.,2007. The worldwide prevalence of ADHD: a systematic review andmetaregression analysis. Am. J. Psychiatry 164, 942–948.
Retz-Junginger, P., Retz, W., Blocher, D., Weijers, H.G., Trott, G.E.,Wender, P.H., Rossler, M., 2002. Wender Utah rating scale. Theshort-version for the assessment of the attention-deficit hyper-activity disorder in adults. Nervenarzt 73, 830–838.
Rosvold, H.E., Mirsky, A., Sarason, I., Bransome, E.D., Beck, L.H.,1956. A continuous performance test of brain damage. J. Consult.Psychol. 20, 343–350.
Rubia, K., Overmeyer, S., Taylor, E., Brammer, M., Williams, S.C.,Simmons, A., Bullmore, E.T., 1999. Hypofrontality in atten-tion deficit hyperactivity disorder during higher-order motorcontrol: a study with functional MRI. Am. J. Psychiatry 156,891–896.
Rubia, K., Smith, A.B., Brammer, M.J., Toone, B., Taylor, E., 2005.Abnormal brain activation during inhibition and error detectionin medication-naive adolescents with ADHD. Am. J. Psychiatry162, 1067–1075.
Saß, H., Wittchen, H., Zaudig, M., 2003. Diagnostische Kriterien(DSM-IV-TR). Hogrefe, Gottingen.
Schweitzer, J.B., Faber, T.L., Grafton, S.T., Tune, L.E., Hoffman, J.M.,Kilts, C.D., 2000. Alterations in the functional anatomy of working
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001

11Latrophilin 3 and response control processes in ADHD
memory in adult attention deficit hyperactivity disorder. Am. J.Psychiatry 157, 278–280.
Skounti, M., Philalithis, A., Galanakis, E., 2007. Variations inprevalence of attention deficit hyperactivity disorder world-wide. Eur. J. Pediatr. 166, 117–123.
Slaats-Willemse, D.I.E., 2003. Cognitive Endophenotypes of ADHD.Ponsen & Looijen BV, Wageningen.
Sonuga-Barke, E.J., 2003. The dual pathway model of AD/HD: anelaboration of neuro-developmental characteristics. Neurosci.Biobehav. Rev. 27, 593–604.
Sonuga-Barke, E., Bitsakou, P., Thompson, M., 2010. Beyond thedual pathway model: evidence for the dissociation of timing,inhibitory, and delay-related impairments in attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolescent Psychiatry49, 345–355.
Spencer, R.C., Klein, R.M., Berridge, C.W., 2012. Psychostimulantsact within the prefrontal cortex to improve cognitive function.Biol. Psychiatry 72, 221–227.
Spronk, M., Jonkman, L.M., Kemner, C., 2008. Response inhibitionand attention processing in 5- to 7-year-old children with andwithout symptoms of ADHD: An ERP study. Clin. Neurophysiol.119, 2738–2752.
Please cite this article as: Fallgatter, A.J., et al., Influence of a Latropof cognitive response.... European Neuropsychopharmacology (2012),
Sugita, S., Ichtchenko, K., Khvotchev, M., Sudhof, T.C., 1998.Alpha-Latrotoxin receptor CIRL/latrophilin 1 (CL1) definesan unusual family of ubiquitous G-protein-linked receptors.G-protein coupling not required for triggering exocytosis. J. Biol.Chem. 273, 32715–32724.
Uebel, H., Albrecht, B., Asherson, P., Borger, N.A., Butler, L., Chen, W.,Christiansen, H., Heise, A., Kuntsi, J., Schafer, U., Andreou, P.,Manor, I., Marco, R., Miranda, A., Mulligan, A., Oades, R.D., van derMeere, J., Faraone, S.V., Rothenberger, A., Banaschewski, T., 2010.Performance variability, impulsivity errors and the impactof incentives as gender-independent endophenotypes for ADHD.J. Child Psychol. Psychiatry 37, 201–218.
Vaidya, C.J., Austin, G., Kirkorian, G., Ridlehuber, H.W., Desmond, J.E.,Glover, G.H., Gabrieli, J.D., 1998. Selective effects ofmethylphenidate in attention deficit hyperactivity disorder:a functional magnetic resonance study. Proc. Natl. Acad. Sci.USA 95, 14494–14499.
Zobel, A., Maier, W., 2004. Endophanotypen—ein neues Konzept zurbiologischen Charakterisierung psychischer Storungen (Endopheno-type—a new concept for biological characterization of psychiatricdisorders). Nervenarzt 75, 205–214.
hilin 3 (LPHN3) risk haplotype on event-related potential measureshttp://dx.doi.org/10.1016/j.euroneuro.2012.11.001