Embed Size (px)
Citation preview

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 3
ORIGINAL RESEARCH
INFLUENCE OF APICECTOMY MODALITIES
ON APICAL SEAL OF RESIN-OBTURATED
ROOT CANALS
Mohamed I. Elshinawy1
Corresponding author email: [email protected]
Contributor:
1Assistant professor of Endodontics
Department of Endodontics, Faculty
of Dentistry, Tanta University, Egypt
and Department of Restorative
Dental Sciences, College of
Dentistry, King Khalid University, Abha, Saudi Arabia
ABSTRACT
Background: Apical seal helps preventing apical leakage following apicectomy.
Aim: To investigate the influence of apicectomy modalities on apical seal of root
canals obturated with resin-based system. Materials and Methods: Root canals of
60 extracted premolars were prepared and obturated in 6 groups using RealsealSE
sealer-points system. The teeth were divided into 6 equal groups according to
apicectomy procedures. Group1 (obturation, immediate apicectomy, glass-ionomer
retro-filling), Group2 (obturation, apicectomy after 24 hours, no retro-filling),
Group3 (obturation, immediate apicectomy, light-curing of the sealer at the cut-
surface), Group4 (obturation, immediate apicectomy, no apical-sealer light-curing),
Group5 (apicectomy, obturation, apical-sealer light-curing), Group6 (apicectomy,
obturation, light-curing of apical sealer coat). Specimens in all groups were
subjected to dye leakage and longitudinal sectioning test. The collected data were
statistically analyzed. Results: Both G1 (control) and G6 recorded comparable
leakage possibility that was the lowest among test groups. Leakage values of groups
3 and 5 were also comparable and lower than groups 2 and 4. Leakage values of
group 4 were the worse among all groups. Conclusion: Apical sealing with a self-
etch adhesive sealer coat is an acceptable alternative to retrograde filling in resin-
obturated canals. Light-curing of the sealer exposed following apicectomy might improve the apical seal.
Key words: apicectomy, adhesive sealers, leakage, retrograde filling
INTRODUCTION:
Management of the resected root end during
periradicular surgery is critical to a successful
outcome.(1) The goal of periradicular surgery is to
access the affected area, remove the diseased tissue,
and place a biocompatible seal. This sealing material
should stimulate cementum deposition and re-
establishment of periodontal attachment as a desired
healing response. (2) Resection of the root end results
in an exposed dentinal root face surrounded
peripherally by cementum with a root canal in the
middle. Favorable healing response is characterized by
a biological seal formed by cementum fill from the
circumference of the resected root-end to the center
added to the physical seal of the root end filling
forming a double seal. (3)
An ideal root-end filling material should promote
periradicular tissue healing through its tolerability and
adherence to retrograde cavity walls. (4, 5)
Too many solid and plastic filling materials have been
used for retro-grade cavity filling. Solid fillings
include silver, tin and titanium posts, amalgam and
gallium alloys. Plastic fillings include sealers such as
calcium hydroxide and epoxy resin sealers and
cements such as zinc phosphate, polycarboxylate,
ZOE, IRM, Super EBA, MTA, calcium phosphate,

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 4
bone cements and gutta-percha. Composite resin is
also commonly used as a retro-filling material.
Ceramic inlays, teflon, a mixture of sulfathiazole and
powdered dentin, cyanoacrylates, citric acid
demineralization and laser are less commonly used
alternatives.(6- 11) Glass ionomer showed good
marginal sealing capacity in vitro, and has been found
to offer excellent biocompatibility.(12,13) Compomers
has been proved to have better biocompatibility than
ordinary glass ionomer cements and MTA and was
suggested as the material of choice in root resorption,
perforations, and root-end filling.(14)
There has long been a debate on whether a root-end
filling should always be placed to achieve a better
apical seal. (15-18) So, this in vitro study was conducted
to investigate the influence of different apicectomy
modalities on the apical seal of root canals obturated
with Realseal SE sealer-points system
Materials and Methods
Sixty single-canaled human mandibular premolars
with straight root canals, freshly extracted from
persons with age group 20 to 45 years old were
selected for this study. Teeth were radiographed to
ensure root integrity and canal patency and then stored
at room temperature in physiological saline solution.
Teeth with immature apices, cracks, and caries were
excluded from the study. Soft tissue remnants and
calculus were removed using ultrasonic scalers. The
teeth were decoronated using a diamond disc (Edenta
AG, AU/SG, Switzerland) under water cooling to
standardize the remaining root length to 16 mm. The
working length was established using #15 K-file
(Dentsply, Maillefer, Ballaigues, Switzerland). The
file was introduced through root canals until its tip was
visible at the apical foramen. The actual working
length was then determined to be 1mm shorter than the
length of the used file.
All root canals were prepared with a series of k-files
using step back technique. The apical preparation was
standardized to master apical file # 40 and the stepping
back procedure was continued till K-file # 60. The
coronal flaring was done using gates glidden drills
(Union Broach, New York, NY) size 1,2&3. During
root canal preparation, 2ml. of 2.5% sodium
hypochlorite solution was used for irrigation after each
file. After canal preparation, the root canals were
conditioned with 10 ml of 17% EDTA (Canal +,
Septodont, France) for 60 seconds for smear layer
removal, followed by washing using 10 ml of 5.25%
NaOCl. Finally root canals were flushed with 10 ml
saline solution and dried with paper points (Dentsply-
Maillefer, Ballaigues, Switzerland).(19)
Grouping
The prepared roots were thereafter randomly divided
into 6 groups (n=10) according to the modality of
apicectomy procedures.
G.1 (control) - G.4: Realseal Self-Etch sealer /
Realseal point obturation was done first followed by
resection of the apical 3mm of the roots.
Size 40 master Realseal point (0.02 taper) was
seated to check the tug-back into the prepared canal
and confirmed with periapical radiograph. To
standardize the consistency of the sealer,
predetermined amount, 1cm long, of the self-etching
adhesive Realseal SE sealer (SybronEndo, Basicweg ,
Amersfoort, The Netherlands) was thoroughly mixed
with one drop of thinning liquid on a graduated mixing
pad. The master cone was used to apply the mixed
sealer against the prepared canal walls using slight
pumping motion twice before seating the cone to the
full working length. Lateral condensation was carried
out using a finger spreader (Dentsply, Maillefer,
Ballaigues, Switzerland). The rest of the canal space
was filled with laterally condensed auxiliary Realseal
points. The excess points were cut off using a heated
hand plugger (Dentsply, Maillefer, Ballaigues,
Switzerland) followed by vertical condensation.
Excess sealer was removed with alcohol-soaked
cotton pellet. A check radiograph was then taken to
ensure complete canal filling and the coronal surface
of the obturation was light cured using a curing light
(Hilux LED 550; Benlioglu Dental, Ankara, Turkey)
with an output of 1000 mW/cm2 for 40 seconds to
create an immediate coronal seal. After root canal
obturation, their apical 3mm were resected using a
high-speed handpiece with water coolant and a fissure
bur (Dentsply/Maillefer). The resected root-ends were
smoothed with a double-sided carborundum disk
(Dentorium Export Ltd, New York, NY, USA).(20 , 21)
and received different kinds of treatments as follows:
G.1(control): the root resection was done immediately
after obturation followed by preparation of a small
cavity at the apical end of the root canal by a rotating
# 4 slow speed round bur (Dentsply/Maillefer) to 2mm
depth into the canal followed by filling this cavity with
compoglass F (Ivoclar Vivadent AG,
Schaan/Liechtenstein).(22) (Fig. 1,2)
G.2: obturation, apicectomy after 24 hours, no further
apical treatment.
G.3: obturation, immediate apicectomy, light-curing
of the sealer exposed at the cut-surface.
G.4: obturation, immediate apicectomy, no further
apical treatment.
G.5 & G.6: surgical resection of the apical 3mm of
the root was done first followed by RealSeal Self-
Etch sealer / Realseal point obturation using the

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 5
same technique with the only exception that the
extruded realseal points through the resected
apices were cut off using a hot hand plugger.
In G.5: the sealer exposed at the cut root surfaces was
thereafter light-cured.
In G.6: a thin sealer coat was thereafter rubbed over
the cut root surface using a small brush followed by
light curing (Fig. 3).
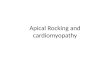
Fig. 1: Digital radiograph showing resected root apices(a), retrograde cavity depth(b) & root end filling(c)
Fig. 2: Retrograde Cavity Before & After Filling
Fig.3 Resected root with apical sealer coating
Fig 4: Removal of root canal filling (a) & root canal and root end filling (b)
Leakage testing
Root surfaces were coated with two layers of nail
varnish except the apical 2 mm. The apex of each
resected root was subsequently immersed uprightly in
freshly prepared 2% methylene blue dye solution for
72 hours at 37 ˚C. (23)
Teeth were then rinsed in tap water to remove
excess dye, nail varnish was removed with scalpel
blade and two longitudinal grooves were prepared on
the lingual and buccal surfaces of each root with a
diamond disc under water-cooling. Each root was then
split longitudinally into two halves using a chisel and
hammer. The teeth were then dried, coded and the root
fillings were removed to detect the maximum coronal
linear dye penetration from the apical cut end in both
halves of each split root (Fig.4). (24) Maximum linear
dye penetration was measured in mm using a
graduated ruler and a magnifying lens.
Statistical analysis: The mean values of apical leakage of experimental
groups with the standard deviation were calculated and
analyzed statistically using 1-way analysis of variance
(ANOVA). Sceffe’s test was performed to pick up the
site of statistical significance at α =0.05. Furthermore,
Tukey’s comparisons at α =0.05 was done to stand on
the significance of differences between test groups.
RESULTS
The mean leakage measurements and their statistical
values were shown in tables 1 and 2. One-way
ANOVA test indicated some differences in the leakage
parameter between the test groups (p= 6.24E-22).
Additionally, Tukey’s comparisons indicated that both
G1 (control) and G6 recorded comparable leakage
possibility (p=0.4332). The leakage values of both
groups were proved to be the lowest in comparison to
other test groups. The leakage values of groups 3 and
5 were also comparable (p=0.4332) and lower than

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 6
groups 2 and 4. Leakage values of group 4 were the
worse among all groups.
DISCUSSION The purpose of retrograde sealing after
apicectomy is to establish an effective barrier between
the root canal and the periapical tissues.(25)
In the current study, all the root canal preparation and
obturation procedures were standardized and done by
the same operator to decrease variability. Sodium
hypochlorite was used as a canal irrigant because of its
lubricant, antimicrobial, organic tissue dissolving
properties (26) but was not used as the final rinse as it
may affect the sealer-dentin bond strength.(27) Smear
layer was removed to allow deeper resin sealer
penetration into dentinal tubules thus improving the
adhesion.(28) Root canals were obturated with realseal
points/realseal SE sealer (SybronEndo, Basicweg ,
Amersfoort, The Netherlands) that was previously
marketed as Resilon-epiphany SE system (Pentron
Clinical Technologies LLC, Wallingford, CT) which
is a resinous material claimed to give monoblock
obturation. Some in vitro and in vivo studies (29, 30)
proved an acceptable resistance of Epiphany sealer to
bacterial leakage. It was also reported that this material
can reinforce the obturated roots minimizing the
chances of vertical root fracture.(31)
Realseal SE has been tried as an apical seal in
group 6 of the current study based on the finding that
adhesives are usually used over composite retro-
fillings for better sealability.(32) The self-etch
adhesives were also found less time consuming and
TABLE (1): The mean and standard deviation for different groups
Group 1 2 3 4 5 6
1 0.000145* 0.0003* 0.000145* 0.000145* 0.4332
2 14.82 0.000155* 0.000145* 0.006293* 0.000145*
3 6.891 7.93 0.000145* 0.4332 0.04583*
4 24.36 9.535 17.46 0.000145* 0.000145*
5 9.535 5.287 2.643 14.82 0.0003*
6 2.643 12.18 4.248 21.71 6.891
* Significant (sig.) difference at P ≤ 0.05
less technique sensitive with better sealability.(33) In
addition, Maltezos, et al., 2006(34) observed good
sealing results for Resilon and concluded that it might
be used as retrograde filling material.
Compoglass F retro-filling was used as a control
in this study as it has been proved to have better
biocompatibility than ordinary glass ionomer
cements and MTA and was suggested as the
material of choice in root resorption,
perforations, and root-end filling. (14)
Root resection of 3 mm from root tip was done
perpendicular to its long axis of the tooth as this
reduces the apical ramification and lateral canals, thus
decreasing the number of open dentinal tubules and
leakage at the resected root end. (35- 38) The retro-cavity
was prepared 2mm in depth to ensure effective light-
curing of compoglass retrofilling.(39)
Methylene blue dye linear penetration &
Longitudinal sectioning of roots were performed for
measurement of microleakage in this study as it
enables the direct observation of the dye penetration
and its penetration pattern. (40) Also Methylene blue
has a comparable molecular size to those small
bacterial metabolic products, rapidly detected under
visible light, water soluble, diffusible and hard tissue
non-reactive. (41-43) The recommended times of
exposure to dyes in leakage studies have ranged from
2 hours to 30 days. (40) In our investigation the teeth
were left in the dye solution for 72 hours.(23)
Groups Mean ± SD
G.1 obturation - Immediate apicectomy - compoglass retrograde filling 1.5± 0.43
G.2 obturation - apicectomy after 24hrs- no further treatment 3.2± 0.39
G.3 obturation-Immediate apicectomy - apical light curing of exposed sealer 2.3± 0.38
G.4 obturation - Immediate apicectomy- no further treatment 4.3± 0.36
G.5 apicectomy – obturation - curing of the exposed sealer at the cut surface 2.6± 0.29
G.6 apicectomy - obturation + cut surface coating with SE sealer - curing 1.75± 0.18
Table 2: Tukey’s pair wise comparisons:

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 7
The results of this study showed comparable
sealability for both G.1 (obturation, immediate
apicectomy and compoglass retrograde filling) and
G.6 (apicectomy, obturation and coating the cut
surface with SE sealer). These results were supported
by findings of some previous studies which showed
that, the direct application of a retrograde root seal
may eliminate the need for preparing a retrograde
cavity that might be difficult to prepare due to the
limited access to the surgical field.(44) Also it has been
shown that preparing and filling a small concavity on
the resected root face with composite resin and dentin
bonding agent (26) or light cure glass ionomer cement (45,46) gave acceptable (44) and even better (45,46) sealing
ability than retrograde filled cavities. In addition, open
dentinal tubules at the beveled root surface of
apicectomized teeth may invite leakage and the
authors advocated complete coverage of the resected
surface with an adhesive retro-seal regardless the
angle and extent of the bevel thus blocking these
dentinal tubules.(47) Moreover, Tanomaru-Filho et al.,
(48) had come to a conclusion that, Epiphany may be an
alternative as a retro-filling material.
The results also showed that both of G.3
(obturation, immediate apicectomy and apical light
curing of exposed sealer) & G.5 (apicectomy,
obturation and curing of the exposed sealer at the cut
surface) are comparable to each other. This might be
referred to the fact that each of them has a good chance
for good condensation of realseal points and hence less
sealer exposure at the apex and also get the benefit of
light curing at the periapical area which accelerates the
polymerization and sealer bonding to both the realseal
points and the root dentin.
The better results for both G3 and G5 (light
curing was done to the sealer at the exposed apical root
end) compared to both G2 and G4 (no light curing to
the sealer at the exposed apical root end) may be
referred to the fact that the light curing improve the
sealing through the formation of hybrid layer at the
dentin-resin sealer interface. This is supported by the
results of a study done by Hashimoto et al (49) who
concluded a superior dentin sealing of a self-etch
adhesive resin due to the retained hybridized smear
plugs within the tubules. (50)
G.2 (obturation, apicectomy after 24hrs with no
further treatment) showed less than expected sealing
ability because of some suggested reasons. The first is
that this dual-cure resin sealer depends mainly on its
chemical-cure components for polymerization in the
apical region and the second is that the cutting stresses
at the apex might have interrupted the apical bond
between the sealer and the dentin wall resulting in
more leakage.
This is supported by previous findings that
proved that mechanical interruption of the
sealer/realseal point /root dentin bond with a rotating
cutting instrument might affect their apical seal.(51)
Additionally, despite the hybridization of resin-filling
materials, a tight seal is difficult to achieve because of
the complex anatomy and mechanical challenges such
as polymerization shrinkage and unfavorable C-factor
inside the root canals.(52)
The least leak-proof results was for G.4
(obturation, immediate apicectomy with no further
treatment) which might be due to the obvious fact that,
the chemical curing reaction takes too much time
compared to light activated cure giving a chance for
sealer degradation and more leakage and this was
confirmed by a study of Beriat et al, 2009(53) who
came to a conclusion that, the amount of conversion of
Epiphany was approximately 50% after photo-
activation and improved by approximately 10% after
15 days. These results indicated weak polymerization
of uncured Epiphany which supports our results.
From the previous studies, it is clear that further in
vivo histologic and microleakage studies are needed to
assess the healing pattern(s) of the periapical tissue
following the application of different treatment
modalities suggested by the current study.
Conclusion:
Under the circumstances of this study we can conclude
that, apical sealing with a self-etch adhesive sealer
coat is an acceptable alternative to retrograde cavity
filling in apicectomized roots obturated with resin-
based system. Light-curing of the sealer exposed
following apicectomy might improve the apical seal.
Conflict of interest
The author declares no conflict of interest
References:
1. Gutmann JL, Pitt Ford TR. Management of the
resected root end: a clinical review. Int Endod J. 1993;
233: 272–283.
2. Andreasen JO. Cementum repair after apicoectomy
in humans. Acta Odontol Scand. 1973; 31: 211–221.
3. Regan JD, Gutmann JL,Witherspoon DE.
Comparison of Diaket and MTA when used as root-
end filling materials to support regeneration of the
periradicular tissues. Int Endod J 2002; 35: 840–847.

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 8
4. Trope M, Lost C, Schmitz HJ, Friedman S. Healing
of apical periodontitis in dogs after apicoectomy and
retrofilling with various filling materials. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod.
1996;81:221-228.
5. Adamo HL. A comparison of MTA, Super-EBA,
composite and amalgam as root end filling materials
using a bacterial microleakage model. Int Endod J
1999;32:197-203.
6. Vasudev SK, Goel BR, Tyagi S: Root end filling
materials — A review. Endodontology 2003;15:12-
18.
7. Chong BS, Pitt Ford TR. Root-end filling materials:
rationale and tissue response. Endod Topics
2005;11:114-130.
8. Payal Saxena P., Gupta SK, Newaskar V.
Biocompatibility of root-end filling materials: recent
update. Restor Dent Endod; 2013;38:119-127.
9. Dammaschke T. Root-end filling with a new
bioactive cement. Inside Dentistry.2012; 8(3).
10.Xavier CB, Weismann R, deOliveira MG,
Demarco FF, Pozza DH.Root-end filling materials:
apical microleakage and marginal adaptation. J Endod.
2005 Jul;3:539-542.
11. Tanomaru-Filho M, Tanomaru JM., Barros DB.,
Watanabe E., Ito IY. In vitro antimicrobial activity of
endodontic sealers, MTA-based cements and Portland
cement. J. Oral Sci. 2007; 49: 41-45.
12. Blackman R, Gross M, Seltzer S. An evaluation of
the biocompatibility of a glass ionomer-silver cement
in rat connective tissue. J Endod. 1989;15:76-9.
13. Jesslen P, Zetterqvist L, Heimdahl A. Long-term
results of amalgam versus glass ionomer cement as
apical sealant after apicectomy. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod. 1995;79:101-3.
14.Gupta SK, Saxena P., Pant VA, Pant AB.
Adhesion and biologic behavior of human
periodontal fibroblast cells to resin ionomer
Geristore: a comparative analysis. Dental
Traumatology 2013;29:389–393.
15. Friedman S. Retrograde approaches in endodontic
therapy. Endod Dent Traumatol 1991; 7: 97–107.
16. Johnson BR. Considerations in the selection of a
rootend filling material. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod. 1999; 87: 398–404.
17. Theodosopoulou JN, Niederman R. A systematic
review of in vitro retrograde obturation materials. J
Endod. 2005; 31: 341–349.
18. Stefopoulos S, Tzanetakis G., Kontakiotis E. Non-
Surgical Retreatment of a Failed Apicoectomy without
Retrofilling Using White Mineral Trioxide Aggregate
as an Apical Barrier. Braz Dent J .2012; 23:167-171.
19. Kocak MM, Ozgur ER, BC, Yaman Sis. Apical
Leakage of Epiphany Root Canal Sealer Combined
with Different Master Cones. Eur. J Dent 2008; 2:91-
95.
20. Claudio Hideki KUBO CH, Ana Paula Martins
GOMES AP, MANCINI MN. In Vitro Evaluation of
Apical Sealing in Root Apex Treated with
Demineralization Agents and Retrofiled with Mineral
Trioxide Aggregate Through Marginal Dye Leakage.
Braz Dent J 2005;16:187-191.
21. Pop I. Oral surgery: part 2. Endodontic surgery.
Braz Dent J. 2013;215:279-286.
22. Winik R, Araki AT, Negrão JA, Bello-Silva MS,
Lage-Marques JI. Sealer Penetration and Marginal
Permeability after Apicoectomy Varying Retrocavity
Preparation and Retrofilling Material. Braz Dent
J.2006;17:323-327.
23. El Aasser M. Diab A. and El Bagdady Y. A
Comparative Study of the Sealing Ability of Different
Root End-Filling Materials: An in vitro study. Cairo
Dental Journal 2009;25: 353:359.
24.Barthel CR, Losche GM, Zimmer S, and Roulet
JF: Dye penetration in root canals filled with AH26 in
different consistencies. J. Endod. 1985;11:176-78.
25. Lamb EL, Loushine RJ, Weller RN, Kimbrough
WF, Pashley DH. Effect of root resection on the apical
sealing ability of mineral trioxide aggregate. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 2003;
95:732-5.26. Bolanos OR., Jensen JR: Scanning
electron microscope comparisons of the efficacy of
various methods of root canal preparation. J. Endod.
1980;6:815-22.
27. Wachlarowicz AJ, Joyce AP, Roberts S. Effect of
Endodontic Irrigants on the Shear Bond Strength of
Epiphany Sealer to Dentin. J. Endod. 2007;33:151-
155.
28. Johnson WT, Gutmann JL. “Obturation of the
cleaned and shaped root canal system” in Pathways
of the Pulp. Cohen S. Hargreaves KM. 9th ed. St
Louis, Mosby Elsevier. 2005; pp. 358–99.
29.Shipper, G., Ørstavik, D., Teixeira, F.B. and Trope,
M. An evaluation of microbial leakage in roots filled
with a thermoplastic synthetic polymer-based root
canal filling material (Resilon). J. Endod. 2004;
30:342- 347.
30.Shipper, G., Teixeira, F.B., Arnold, R.R. and
Trope, M. Periapical inflammation after coronal
microbial inoculation of dogs roots filled with gutta-
percha or resilon. J. Endod. 2005; 31:91-96.
31.Teixeira, F.B., Teixeira, E.C.N., Thompson, J.Y.
and Trope, M. Fracture resistance of roots
endodontically treated with a new resin filling
material. JADA. 2004l;135:646-652.
32. Yazdi1 PM, Schou S, Jensen SS, Stoltze K, Kenrad
B & Sewerin I. Dentine-bonded resin composite
(Retroplast) for root-end filling: a prospective clinical
and radiographic study with a mean follow-up period
of 8 years. Int Endod J. 2007;40: 493–503.

Journal of Dental & Oro-facial Research Vol 12 Issue 1 Jan 2016 JDOR
MSRUAS 9
33. Abdal AK, Retief DH, and Jamison HC: The apical
seal via the retrosurgical approach. An evaluation of
retrofilling material. Oral surg Oral Med Oral Pathol
Oral Radiol Endod 1982;54:213-8.
34.Maltezos C, Glickman GN, Ezzo P, He J.
Comparison of Resilon, Pro Root MTA, and Super
EBA as root-end filling materials: a bacterial leakage
study. J Endod. 2006; 32:324-7.
35. Erkut S, Tanyel RC, KeklikogluN, Yildirim S,
Katiboglu AB. A com-parative study of retrograde
filling ma-terials. Turk J Med Sci. 2006; 36:113-120.
36. Kim S, Kratchman S. Modernendodontic surgery
concepts and practice: a review. J Endod. 2006;
32:601-623.
37.Pereira CL, Cenci MS, Demarco FF. Sealing ability
of MTA, Super-EBA, Vitremer and amalgam as root-
end filling materials. Braz Oral Res 2004; 18:317-321.
38. Tsesis I, Rosen E, Schwartz-Arad D, Fuss Z.
Retrospective evaluation of surgical endodontic
treatment: traditional versus modern technique. J
Endod. 2006; 32:412-416.
39. Soh MS1, Yap AU, Siow KS. The effectiveness of
cure of LED and halogen curing lights at varying
cavity depths. Oper Dent. 2003; 28:707-15.
40. De Moor RJ, De Boever JG. The sealing ability of
an epoxy resin root canal sealer used with five Gutta-
Percha obturation techniques. Endod. Dent. Traumatol
2000;16:291–7.
41. De-Deus G, Coutinho-Filho T, Reis C, Murad C,
Paciornik S. Polymicrobial leakage of four root canal
sealers at two different thicknesses. J. Endod. 2006;
32:998-1001.
42. Kennedy WA, Walker III WA, Gough RW: Smear
layer removal effects on apical leakage. J. Endod.
1986, 12: 21-27.
43. Matloff IR., Jensen JR., Singer L., Tabibi A:
Comparison of methods used in root canal sealability
studies. Oral Surg. 1982; 53: 203-8.
44.Rud J, E.C.Munksgaard J.O.Andreason.Retrograde
root filling with composite and a dentin bonding
agent.1. Endod Dent Traumatol 1991;7:118-125.
45. Chong B.S., Pittford T.R., Watson T.F. Light cured
glass ionomer cement as a retrograde root seal. IEJ
1993; 26:218-224.
46. Mc Donald N.J. and T.C.Dumsha. An evaluation
of the retrograde apical seal using dentin bonding
materials. IEJ 1990; 23;156-162.
47. Vertucci F.J., Beatty R.G. Apical leakage
associated with retrofilling techniques;a dye study. J.
Endod. 1986;12:231-236.
48.Tanomaru-Filho M, Saçaki JN, Faleiros FB,
Guerreiro-Tanomaru JM. pH and calcium ion release
evaluation of pure and calcium hydroxide-containing
Epiphany for use in retrograde filling. J Appl Oral Sci.
2011;19:1-5.
49.Hashimoto M, Ito S, Tay FR, Et al. Fluid
movement across the resin-dentin interface during and
after bonding. J Dent. Res 2004; 83:843-848.
50.Yuan Y, Shimada Y, Ichinose S, Tagami J.
Qualitative analysis of adhesive interface nanoleakage
using FE-SEM/EDS. Dent.Mater. 2007; 23:561-569.
51. Othman HI, Elshinawy MI, Abdelaziz KM,
Retention of fiber posts to the optimally and over-
prepared dowel spaces. J Adv Prosthodont 2013; 5:16-
20.
52. Perdigao, J., Lopes M.M.,Gomes G.: Interfacial
adaptation of adhesive materials to root canal dentin.
J. Endod. 2007; 33: 259-263.
53. Beriat NC, Ertan A, Zafer C., Cehreli ZC, Kamran
Gulshai K.: Time-dependent conversion of a
Methacrylate-based Sealer polymerized with Different
Light-curing Units. J.Endod. 2009; 35:110-112.