Embed Size (px)
Citation preview

Information for healthcare providers in the Tri-state Region
MEDLINK NEWS
8
Also in this issue:Hematology/oncologyoutreach in Boscobel
Echocardiographyreaccreditation
Medical Educationp. 2
Avoid amputationswith early PAD diagnosesp. 3
Peds hematology/oncology offered close to home
Headache Clinic helps teens p. 4
Multiple options fromUterine Fibroid Clinic p. 5
New PracticesNew TelemedicineServicesp. 7
NeoNET delivers prompt video support to providers managingnewborns in crisisThe birth of a critically ill newborn is stressful. You need to determinethe best method of treating the infant quickly. Gundersen Health System now offers the live video expertise of its neonatologists andLevel 3 NICU through a new program called NeoNET.
NeoNET provides tri-state area hospitals with immediate access toGundersen’s neonatal specialty services and Newborn EmergencyTelemedicine. This comprehensive program includes:
• A telemedicine unit installed at your hospital with real-time visualand auditory conference capability 24 /7 with a neonatologist
• MedLink telephone consultations with a neonatologist• Continuing education at your facility and a job shadow
opportunity in our Level 3 NICU • Ground or air transport of an infant by our special Neonatal
Transport Team
“The NeoNET program gives regional family practice physicians additional tools, training opportunities and a higher level of consultation for newborns in crisis. Because our neonatologists are set up with telemedicine from their own homes, this is truly a 24/7 service,” says Kimberly Hable, RN, Gundersen Regional Services.
Ngozi Nduka, MDGundersen Neonataology
continued on page 6
1900 South AvenueLa Crosse, WI 54601www.gundersenhealth.org
Non-ProfitOrganizationU.S. Postage
P A I DLa Crosse, WI
Permit No. 395
Gundersen Lutheran Medical Center, Inc. | Gundersen Clinic, Ltd.Gundersen Boscobel Area Hospital and ClinicsGundersen St. Joseph’s Hospital and ClinicsGundersen Tri-County Hospital and Clinics9550-10_0515
May 2015
Endovascular treatment improvesoutcomes for stroke patientsA once-controversial question of whether endovascular treatment forstroke is effective has now been definitively put to rest.
“A number of recent studies* have shown that using endovascularclot retrieval (thrombectomy) in addition to clot busting medicinerTPA (thrombolysis) for patients with an acute ischemic stroke withlarge vessel occlusion works far better than just using the clot busting medicine alone,” reports Gundersen neurointerventionalistMouhammed Kabbani, MD. Mouhammed
Kabbani, MDGundersen Neurosurgery
continued on page 8
Kimberly HableGundersen Regional Services
According to Dr. Kabbani, the benefits of endovasculartreatment include:
• More time—treatment can be provided up to sixhours after a stroke versus the four-and-a-half-hourwindow for tPA.
• It offers a potential treatment option for patients whoare not eligible for tPA.
• There was no increase in mortality or intracerebralhemorrhage. In one study, mortality was actually reduced by 50 percent.
• There’s a clinically significant increase in functional independence. In the studies, many patients had amodified Rankin Scale (mRS) score of 2 or lower when assessed 90 days after stroke.
So why the difference in results of these recent studiescompared with earlier studies? “The primary reasonseems to be the development of stent retrievers—they were not available in the earlier studies. Also, the endovascular treatments were delivered more quicklyand large artery occlusion was confirmed using CT angiography or other imaging modalities,” Dr. Kabbani explains.
The sooner a stroke patient receives treatment, the betterthe potential outcomes. Stroke patients suspected of
having a major artery occlusion need to be stabilized andurgently transported to a hospital with comprehensivestroke care, such as Gundersen Health System, wherethere are appropriate facilities, protocols and staff inplace including a neurointerventionalist.
To get your patient the best and fastest care possible,Gundersen also offers telestroke services to many regional emergency rooms as well as critical ground and air transport.
Endovascular intervention isn’t for all stroke patients and there are some risks including downstream embolization, vessel dissections and perforations. But in the studies, the occurrences were very small and the benefits outweigh the risks.
With careful patient selection using CT, fast treatmentand use of retrieval devices, there is an overwhelmingclinical benefit to clot removal in conjunction with standard treatment. “It’s just a matter of time before this becomes the new standard of care,” concludes Dr. Kabbani.
*MR CLEAN, ESCAPE, EXTEND-IA and SWIFT PRIME, all presented at the 2015 International Stroke Conference.
Endovascular treatment improves outcomes for stroke patients - continued
Hematology and medical oncology outreach available in Boscobel
Gundersen Health System’scommitment to quality careclose to home is being enhanced with the Center forCancer & Blood Disorder’s newoutreach in Boscobel, Wis. Gundersen hematologist andmedical oncologist DavidMarinier, MD, FACP, now seespatients at Gundersen BoscobelArea Hospital and Clinics.
By traveling to Boscobel on thesecond and fourth Thursday of
every month, Dr. Marinier is helping relieve the burden ofa 130-mile round-trip drive to La Crosse for area patients.He provides consults for newly referred hematology andmedical oncology patients, and routine follow-up care forexisting patients. Oral and intravenous chemotherapytreatments are also available in Boscobel.
“I’m pleased to provide patients in the Boscobel area whoare battling cancer or blood disorders with a treatmentoption close to home,” comments Dr. Marinier who hasmedical interests in genitourinary malignancies,melanoma, myelodysplastic syndromes and medical education. “When cancer affects individuals and theirfamilies, coming to ‘their home’ is the least we can do.”
Dr. Marinier also sees patients by telemedicine in Boscobel. Gundersen Boscobel Area Hospital and Clinicsis just one of many locations throughout the Tri-state Region in which Gundersen provides cancer outreachand/or telemedicine services. Other locations includeBlack River Falls, Blair, Calmar, Decorah, Harmony, Hillsboro, Independence, Postville, Prairie du Chien, Richland Center, Sparta, Tomah, Viroqua, Waukon, West Union and Whitehall.
To schedule an outreach appointment for your patient,call the MedLink scheduling specialist at (800) 336-5465.In La Crosse, call (608) 775-5465.
David Marinier, MD, FACPGundersen Hematology & Oncology
New Telemedicine ServicesTo schedule a telemedicine appointment for your patient, call MedLink at (800) 336-5465 or in La Crosse call 775-5465.
Diabetic Education Holly Burrichter, RN, RDLocations: Gundersen Tri County Hospital and Clinics,Whitehall, Wis and Gundersen Harmony Clinic, Minn.
Medical OncologyDavid Marinier, MDLocations: Gundersen Boscobel Area Hospital and Clinics, Boscobel, Wis.
Palliative CareCarrie Lapham, clinical nurse specialist and Marcia Kendall, palliative care specialistLocations: In Wisconsin at Gundersen Clinics in Prairie du Chien and Tomah, GundersenTri-County Hospital and Clinics – Whitehall, Gundersen St. Joseph’s Hospital and Clinics,Hillsboro and Viroqua Medical Office Building; in Minnesota at Gundersen HarmonyClinic; and in Iowa at Gundersen Clinics in Calmar, Decorah, Waukon and West Union.
Gundersen Echocardiography receives reaccreditation Among the advanced diagnostic tools frequently used toevaluate heart structure and function is a noninvasiveechocardiogram. The skill of the technologist performingthe exam, equipment used, knowledge of the interpreting doctor and quality measures are all critical to quality patient testing.
Gundersen in La Crosse, has been granted three-yearreaccreditation in pediatric and adult transthoracicechocardiography by the Intersocietal Accreditation Commission (IAC). Gundersen has held accreditation continuously since 2006. To receive accreditation,
Gundersen Echocardiography Laboratory has undergonea thorough review of its operational and technical components by a panel of experts—confirmation thatyou and your patients can rely on.
Echocardiography accreditation is required in some statesand regions by the Centers for Medicare and MedicaidServices (CMS) and by some private insurers. Make certain your patients’ echocardiography procedures areperformed within accredited facilities, because, for many organizations, accreditation is voluntary.
7
Medical Education 2015 Ethics and Boundaries—Risk Management Tips for Mental Health ProfessionalsMay 18, Rasmus Center, Gundersen Healthy System, La Crosse
2015 Pharmacology ConferenceSept. 25, Lunda Center, Western Technical College, La Crosse
For more information and/or register visit gundersenhealth.org/seminars
2
Palliative CareAllison Harbour, MDLocation: Gundersen St. Joseph’s Hospital and Clinics – Hillsboro, Wis.
Radiation OncologyColin Driscoll, MDLocation: Gundersen Prairie du Chien Clinic, Wis.
TelestrokeClare Braun Hashemi, MD; Gregory Fischer, MD; Mary Goodsett, MD; John-Peter Temple, MD; Ragasri Kumar, MD; and Concepcion Santillan, MDEmergency Departments in these Wis. locations: Black River Memorial Hospital; Gundersen Boscobel Area Hospital and Clinics, Boscobel; Gundersen St. Joseph’s Hospital and Clinics, Hillsboro; Tomah Memorial Hospital; Vernon Memorial Hospital, Viroqua; and Gundersen Tri County Hospital and Clinics, Whitehall
New Practices
Charles Clark, MDFamily MedicineGundersen Onalaska Clinic
Kate O'Rourke, DOFamily MedicineGundersen St.Joseph’s Hospitaland Clinics – Hillsboro
Laurie Polubinsky, MDBehavioralHealthGundersen La Crosse Clinic
6
Take steps early to diagnose PAD, avoid amputationsPAD affects an estimated 18 to 23 percent of people age55 and over. “Yet PAD is still oneof the most under-recognizedand under-treated diseases inour country,” reports Gundersenvascular surgeon IrinaShakhnovich, MD. “Withoutearly intervention, PAD can leadto ulcers, infections, gangrene,amputation, poor quality of lifeand early death.”
Researchers, using data fromthe Centers for Medicare and Medicaid Services (CMS) for2000 through 2008, looked at PAD and amputations. Ofthe roughly 3 million patients hospitalized for PAD, about6-7 percent underwent lower extremity amputations as a result.
But, there’s promising news. The number of PAD-relatedamputations has declined in the last 10 years because of:
• Early recognition• Medical management when caught early• Improved revascularization techniques
“With PAD, healthcare providers need to look at intermittent claudication and critical limb ischemia, butalso be aware that fewer than half of patients with PADare symptomatic. That’s why it’s so important to screenpatients for PAD and look at co-morbidities such as diabetes, renal disease and coronary/carotid artery disease,” suggests Dr. Shakhnovich.
“Patients who have had diabetes for a decade or morehave a 23 times greater risk of ulcerations,” she adds. “So if your patient has diabetes and foot ulcerations, consider a referral to a vascular specialist right away. The earlier your patient sees a specialist, the better the chance of successful revascularization and preventing amputation.”
Dr. Shakhnovich also suggests, “If you have a patient with PAD symptoms, you should perform an ankle-brachial index (ABI) to establish PAD. ABI shouldalso be performed as part of annual physicals for patients who are:
• Older than age 70• Age 50-69 with other risk factors like diabetes or
smoking• Experiencing exertional leg pain
But note that an ABI in diabetic patients can result infalsely elevated numbers secondary to severe calcification. Above 1.4, the patient needs further studies such as toe pressure or angiogram which can be done at Gundersen.
Treatment of PAD is mainly medical, not surgical. If treated early, most patients can avoid percutaneous or surgical intervention. First-line treatment should include:
• Smoking cessation• Diabetes management• Antiplatelets like aspirin• Lipid reduction generally using statins• Structured walking program • Patient education and monitoring
But if that fails after a few months, or there’s life-limitingclaudication, surgery may be needed. Dr. Shakhnovich explains, “Your patients may be a candidate for revascularization if there are ulcerations on the feet, pain in the calf or toe at rest and/or critical limb is-chemia—all symptoms that put the patient at higher risk of amputation.”
Gundersen Vascular Medicine takes a multidisciplinaryapproach for the diagnosis, treatment, secondary treatment and vascular rehabilitation of patients. Thosewith intermittent claudication are generally seen by aVascular Medicine physician, but if patients have more serious symptoms, they are seen by a vascular surgeryand/or interventionalist to expedite the process.
For questions or a referral, contact Gundersen VascularMedicine via MedLink at (800)336-5465 or 775-5465 in La Crosse.
Irina Shakhnovich, MDGundersen Vascular Surgery
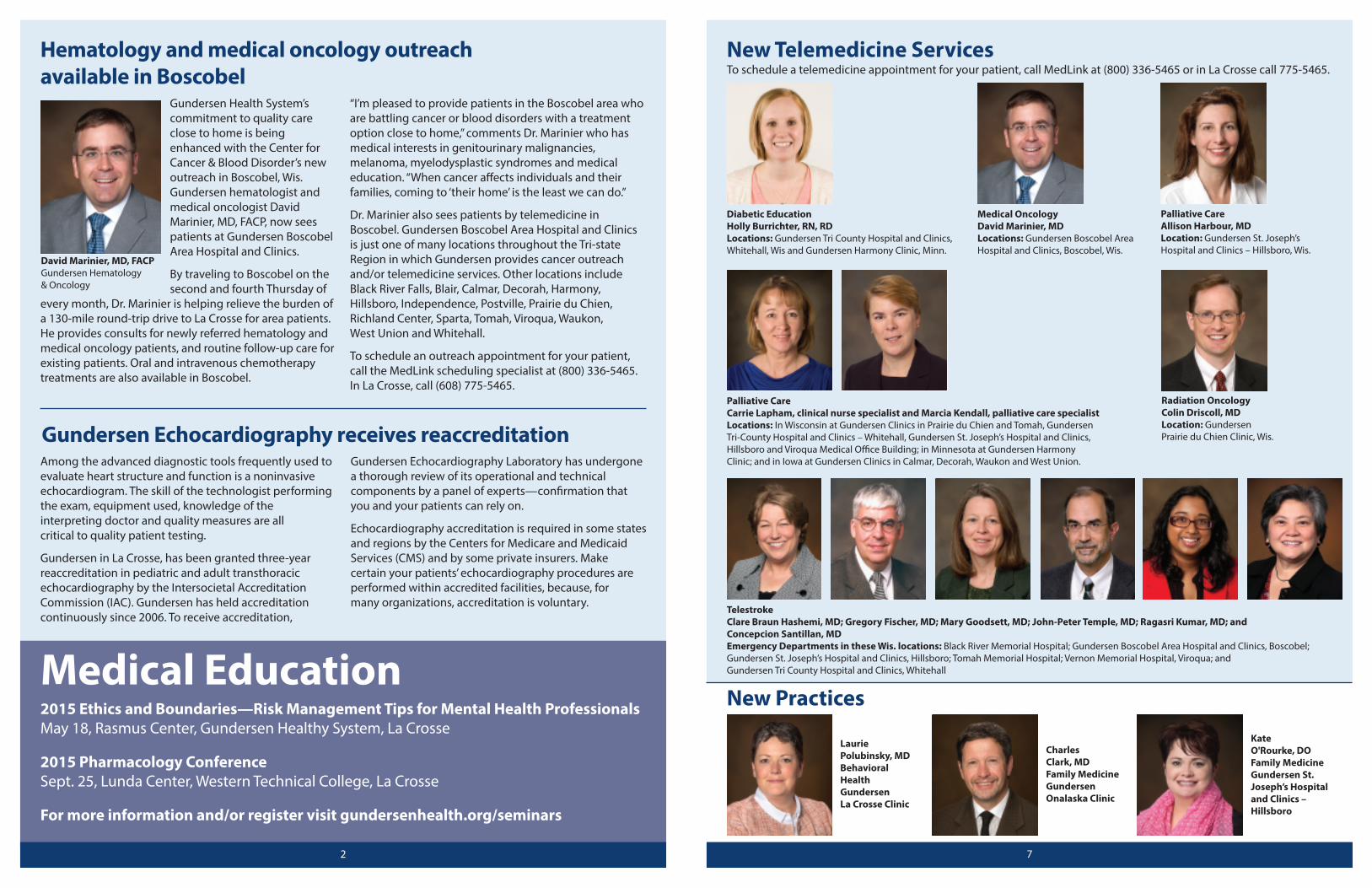
Seeing a baby in real timewhile consulting with a physician has definite advantages, according to neonatologist Ngozi Nduka,MD. “With a telemedicineunit, I can listen to the baby’s heart rate with a stethoscope and talk to the provider while examining the color of thebaby, its movement, alertness and any signs ofrespiratory distress. It helpsus make a better decisionabout whether the babyneeds to be transferred or if we can work with theprovider to treat the infant,” explains Dr. Nduka.
NeoNET was not establishedto encourage the transfer ofbabies to Gundersen’s NICU.“It’s always beneficial to havemom and baby stay in their hometown hospital whenpossible. Telemedicine provides families access to aneonatologist who can work collaboratively with theprovider to decide if transfer is necessary,” says Kim.
If a transfer is necessary, telemedicine can help stabilizethe baby. “The first hour is often critical for premature infants who require respiratory support. With telemedicine, we can advise how much c-pap to give and keep babies going without intubation until ourNeonatal Transport Team arrives,” explains Dr. Nduka.“Telemedicine also prepares the team for the condition of the infant prior to arrival. We appreciate the chance to collaborate as soon as possible when a critical situation presents itself.”
Winneshiek Medical Center in Decorah, Iowa, and
Tomah Memorial Hospital in Tomah, Wis., are the first touse Gundersen’s neonatal telemedicine services. FamilyMedicine providers at the Gundersen Decorah Clinic usetelemedicine services for the babies they deliver who require a neonatology consult at Winneshiek MedicalCenter. They’ve been very pleased with the collaborationswith Gundersen neonatologists. Six additional sites areexpected to go live with NeoNET this year.
For more information about NeoNET, to consult with aneonatologist or to arrange a transport, call Gundersen’sMedLink at (800) 336-5465. If you have questions on howto set up a telemedicine program in your newborn nursery, contact Kimberly Hable, RN, Regional Services, at (608) 799-6548.
NeoNET delivers prompt video support to providers managing newborns in crisis - continued
Examining a newborn via the telemedicine unit at Gundersen Health System are (L-R) Mary Kuffel,MD, Ob/Gyn, vice president, Regional System, and Kate Richmond, MD, neonatologist and medicaldirector of Gundersen’s NICU.
who want to become pregnant. Gundersen offers othereffective treatments, including:
• Medications to slow or stop fibroid growth• Laparoscopic or robotic myomectomy• Vaginal, laparoscopic or robotic hysterectomy—the
only procedure to guarantee an end to fibroids
“The Uterine Fibroid Clinic is here to help educate patients about all of their options, refer them to the appropriate specialist(s), and ultimately, help them selecta treatment that best fits their needs,” says Dr. Benden.
To refer a patient or for more information, contact theUterine Fibroid Clinic via MedLink at (800) 336-5465. In La Crosse, call (608) 775-5465.
Uterine Fibroid Clinic outlines all treatment options for patients - continued
Email version of MedLink News availableIf you are receiving this newsletter by mail,please help us with our goal to reduce the production costs of the printed version and lessen the impact on the environment by providing us with your email address. Youremail will not be shared outside of GundersenHealth System under any circumstances.
You can sign up for the electronic version of MedLink New at gundersenhealth.org/MedLink.
3
54
Headache Clinic offers teen patients easy accessto multiple specialists
An estimated half of allteenagers, ages 13-18, getchronic headaches—migraines,tension/stress headaches orboth. Often these are frequentheadaches which lead to missing a lot of school, extracurricular activities, social life and family life.
“Many times, headaches and migraines can be treated in theprimary care setting, but if acase is complicated, difficult to
manage and the headaches are interfering with quality oflife, it may be time to refer your patient to Gundersen’sChild and Adolescent Headache Clinic,” reports pediatric neurologist John-Peter Temple, MD.
In a single visit in Neurosciences on the Gundersen La Crosse Campus, the patient meets with members ofthe multidisciplinary team, including:
• Dr. Temple or a Pediatric Neurology nurse practitionerwho takes a history and performs an examination
• Pediatric behavioral health therapist Erin Millard, PsyD, for an evaluation of emotional causes or resultsof the headaches
Pediatric hematology and oncology offered close to homeArea children with cancer orblood disorders do not have totravel hundreds of miles to receive cutting-edge treatmentsand personalized care. Gundersen Health System in La Crosse has a Pediatric Cancer& Blood Disorders team dedicated to providing multidisciplinary care to children.
“We treat infants, children andyoung adults with a wide variety
of medical issues, ranging from bleeding disorders to malignancy. We also see patients with benign hematology issues—the most common being anemiaand evaluation for Von Willebrand disease and thrombophilia,” states Jennifer Orozco, MD, fellowshiptrained pediatric hematologist/oncologist and board certified pediatrician.
A native of Hartland, Wis., Dr. Orozco joined GundersenPediatric Cancer & Blood Disorders in October 2014. “I was impressed with the department’s model of carethat is focused on keeping children and their familiesclose to home and within their support networks,” she says.
For patients living in rural communities, lab work can be done at their local primary care clinic, saving them a trip to La Crosse. Patients also have access to cutting-edge clinical trials sponsored by the Children's Oncology
Group (COG), the world’s largest pediatric and adolescent cancer clinical trials organization. ThroughCOG, Gundersen collaborates with other institutions, such as MD Anderson and St. Jude Children’s ResearchHospital, to identify the most effective cancer treatment methods.
Childhood cancer definitely affects the child, but has anobvious impact on the parents, siblings and extendedfamily. “For this reason, we not only treat the child but thewhole family.” The team works collaboratively with ChildLife, Social Work, Spiritual Care, Behavioral Health, Nutrition Therapy, Music and Pet Therapy, and PalliativeCare to ensure all of the family’s needs are met. “And because we’re a small program, we can spend extra time with the children and families, or make classroomvisits for age-appropriate discussion of the child’s diagnosis,” she adds.
In addition to focusing on the needs of the family, communication with the child’s primary care team is alsokey. “We notify the primary care clinician of the patient’sdiagnosis or admission within 24 hours of seeing the patient. During the treatment of cancer, children are often not seen as frequently in their primary care clinic.Therefore, we provide regular updates on the child’s status to smooth the transition back to the primary carephysician once the child is in remission,” states Dr. Orozco.
To refer a patient to Pediatric Cancer & Blood Disorders,call the MedLink scheduling specialist at (800) 336-5465.In La Crosse, call (608) 775-5465. To learn more, go to gundersenhealth.org/kidscancer.
Jennifer Orozco, MDGundersen Pediatric Hematology & Oncology
John-Peter Temple, MDGundersen Pediatric Neurology
• Registered dietitian Valerie Pampuch, RD, to reviewthe importance of good nutrition and hydration, andavoiding headache triggers such as caffeine and concentrated sweets
• A pediatric neurology nurse to discuss the impact ofexercise, sleep habits, activities and screen time, andreview the team’s assessment and plan
Depending on the findings, further testing may be required, including an MRI or blood tests. Treatment may include medications to prevent headaches or to take when headaches occur; diet, sleep and other lifestyle modifications; and counseling.
Your teenage patient may also be a candidate for a special five-week group program. The group meetsweekly to discuss headache causes and prevention, peer support, relationships and stress management tohelp manage headaches.
“After the first visit, a member of our team will follow up with a phone call. We recommend a follow-up clinicvisit in six to eight weeks to see if we are on the righttreatment path and to make adjustments if needed,” explains Dr. Temple. “The patient is seen again at threemonths and then every three to six months.”
According to Dr. Temple, “Sometimes headaches are so ingrained it can take a while to turn things around. Wemay need to try different medications or treatment options. But once a treatment plan is in place and working well, we generally send the patient back to theprimary care provider for ongoing management. Butwe’re always available for consultation or another referral appointment, if needed.”
Gundersen also offers a pediatric Traumatic BrainInjury/Concussion Clinic and First Seizure Clinic. For a referral or consultation to any of these specialty clinics,call Pediatric Neurology via MedLink at (800) 336-5465 or 775-5465 in La Crosse.
Uterine Fibroid Clinic outlines all treatmentoptions for patients
Nearly one third of women willdevelop uterine fibroids by thetime they reach age 35, andabout 70-80 percent of womenwill do so by age 50. Now, patients seeking minimally invasive treatment for problematic fibroids can learnabout all of their options atGundersen Health System’s new Uterine Fibroid Clinic.
“Thirty years ago, medicationsor total abdominal hysterectomy would have been the only choices for patients with fibroids. Today,there are several minimally invasive treatments which canlead to quicker recovery,” saysGundersen obstetrician/gynecologist Dana Benden, MD,who together with interventional radiologist Ezana Azene, MD, PhD, developed the Uterine FibroidClinic at Gundersen.
The comprehensive clinic is designed to be a startingpoint for patients where all therapy options can be discussed. This includes uterine fibroid embolization(UFE, pronounced “you-fee”), an effective non-surgicalprocedure that is underutilized in our region.
Performed by an interventional radiologist, UFE is a minimally invasive, image-guided procedure that blocksblood flow to fibroids in the uterus. “UFE has been extensively studied in multiple trials, all of which supportit as a safe, effective therapy for symptomatic fibroids inappropriately selected women. The strength of this dataled the American College of Obstetrics and Gynecologyto give UFE a ‘Level A’ recommendation as an alternativeto hysterectomy in the management of fibroids,” explains Dr. Azene
Hundreds of thousands of women in the U.S. and aroundthe world have had UFE. Advantages of UFE include fewercomplications than surgery, faster recovery, it’s an outpatient procedure, it treats the entire uterus, there’sno abdominal scar and it may be repeated if necessary.
Although UFE is very safe with an extremely low risk ofside effects, it’s not right for all women, especially those
Dana Benden, MDGundersen Obstetrics & Gynecology
Ezana Azene, MD, PhDInterventional Radiology
continued on page 6