Embed Size (px)
Citation preview

Author Disclosure
Drs Palma, Van Eaton, and Longhurst
have disclosed no financial
relationships relevant to this article.
This commentary does not contain a
discussion of an unapproved/
investigative use of a commercial
product/device.
Information Technology to SupportHandoffs in Neonatal CareJonathan P. Palma, MD,*† Erik G. Van Eaton, MD,§ Christopher A. Longhurst, MD, MS†‡
AbstractCommunication failures during physician handoffs represent a significantsource of preventable adverse events. Computerized sign-out tools linkedto hospital electronic medical record (EMR) systems and customized forneonatal care can facilitate standardization of the handoff process andaccess to clinical information, thereby improving communication andreducing adverse events. It is important to note, however, that adoption oftechnological tools alone is not sufficient to remedy flawed communica-tion processes.
Objectives After completing this article, readers should be able to:
1. Identify key elements of a computerized sign-out tool.2. Describe how an electronic tool might be customized for neonatal care.3. Appreciate that technological tools are only one component of the handoff
process they are designed to facilitate.
IntroductionCommunication errors are a leadingunderlying cause of adverse events andpatient harm, and handoffs in patientcare represent one source of such er-rors. (1)(2)(3) The quantity and com-plexity of handoff information is in-creased in the intensive careenvironment, escalating the potentialfor errors in a process already describedas a haphazard “precarious exchange.”(4)(5)(6) The problem is exacerbatedin the academic setting for two rea-sons: 1) residency work hour restric-tions necessitate more frequent hand-offs, increasing the risk of anincomplete or incorrect transfer of in-
formation, (7)(8)(9) and 2) handoffsare conducted most commonly be-tween junior trainees who frequentlyhave not been given a formal structureor training for this process. (10)
The communication issues im-plicated as a root cause in greaterthan 80% of reported sentinel eventsrepresent an opportunity for the de-velopment of technological toolsdesigned to improve the exchangeof information. (2)(11)(12) Specifi-cally, computerized sign-out toolscan facilitate standardization of thehandoff process and access to clinicaldata. (13)(14) Such electronic sign-out applications have the potentialto improve communication and re-duce preventable adverse events.(15) The benefits of using computer-ized sign-out tools to facilitate thehandoff process have been demon-strated in various medical disciplines,(16)(17)(18) including pediatrics(19)(20) and the neonatal intensivecare unit (NICU). (21)
*Division of Neonatal and Developmental Medicine,Department of Pediatrics, Stanford University Schoolof Medicine, Stanford, CA.†Department of Clinical Informatics, Lucile PackardChildren’s Hospital, Palo Alto, CA.§Department of Surgery, University of WashingtonSchool of Medicine, Seattle, WA.‡Division of Systems Medicine, Department ofPediatrics, Stanford University School of Medicine,Stanford, CA.
topics in neonatal informatics
e560 NeoReviews Vol.12 No.10 October 2011
by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from

Electronic Sign-out ToolsElectronic sign-out tools can take sev-eral forms, including word processoror database manager documents, web-based systems, and tools integratedwithin a hospital’s EMR. Regardless ofthe sign-out system used, certain es-sential information should be in-cluded. Patient demographics (name,medical record number, and location)are required for patient tracking. Infor-mation such as weight, medications,allergies, pertinent laboratory data,and clinician-entered patient details(eg, a prioritized problem list, briefnarrative comments) are needed tosummarize a patient’s clinical statusand management. Information classi-
fied as either a “to do” or an anticipa-tory guidance item is more likely to becommunicated effectively, (8) so thesecategories should be included as well.Finally, instructions to covering col-leagues and shorthand commentarythat suggest methods to adapt thecare plan are not typically included inprogress notes and are more accessi-ble to covering clinicians when ag-gregated in a sign-out system.
Although standalone sign-outsystems such as manually updatedword processor documents may im-prove workflow over paper processes,they can contain troublesome inac-curacies due to the significant effortrequired to transcribe and manually
update information that often isavailable electronically. It is benefi-cial, therefore, to combine clinician-entered clinical information withdata automatically populated fromthe EMR. (5)(22) Frank and col-leagues (19) at the Alfred I. DuPontHospital for Children demonstratedthat integration of a sign-out toolwithin the hospital’s EMR to auto-mate the retrieval of demographicand clinical information improvedefficiency and accuracy. In additionto using data already present withinthe EMR, an EMR-integrated ap-proach allows recording of clinician-entered sign-out information in theEMR. Improved access to sign-outinformation has been shown to ben-efit communication by allowing theasynchronous transfer of informationbetween members of the care team.(23) Another potential benefit ofEMR integration is the developmentof automated checklists that provideclinical decision support using spe-cific patient information to promoteadherence to best practice guidelinesor other protocols.
Customization forNeonatal CareWhen an EMR-integrated sign-outtool adopted in the medical and sur-gical wards at Lucile Packard Chil-dren’s Hospital at Stanford failed togain usage in the NICU, (20) Palmaand associates (21) documented the
Figure 1. Neonatology team at Lucile Packard Children’s Hospital using an EMR-integrated sign-out document to facilitate communication.
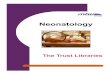
Figure 2. Sample of an EMR-integrated neonatal sign-out document.
topics in neonatal informatics
NeoReviews Vol.12 No.10 October 2011 e561 by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from

development and acceptance of asign-out tool specific to neonatalcare (Fig. 1, Fig. 2). Following itsintroduction, the neonatal EMR-integrated sign-out tool was adoptedrapidly, and clinician satisfactionand perceptions of sign-out accur-acy were improved compared withthe NICU’s previous standalonesign-out tool, a Microsoft Access™database.
The experience at Lucile PackardChildren’s Hospital underscores howthe handoff process varies acrossdifferent clinical settings. (24) Tosupport communication in a particu-lar setting, an electronic tool mustbe tailored to the needs of thatarea. A primary reason that thepreviously cited EMR-integratedmedical/surgical sign-out documentwas not adopted in the NICU wasits length: each page of the printeddocument contained 2 to 3 patients,making the complete documentcumbersome for rapid informationretrieval in the 40-bed NICU. Theneonatal sign-out tool was designedfor each page to include up to 10patients. Despite modification ofthe document’s layout, the represen-tation of clinician-entered sign-outinformation within the EMR is con-sistent with that of the medical/surgical sign-out. Because the infor-mation is patient-centric, whenNICU patients are transferred toother units, their sign-out informa-tion automatically populates thesign-out document used in the re-ceiving unit.
Electronic sign-out tools provideflexible layouts and alternative dataviews that permit powerful customiza-tion of the contained information. Thesame system used throughout an insti-tution can be adapted to fill the special-ized needs of a neonatology service. Inaddition to standard demographic in-formation, a neonatal sign-out toolshould include an infant’s estimated
gestational age. During the first severaldays following birth, inclusion of thetime of birth may aid in managementdecisions such as the treatment of hy-perbilirubinemia. The birthweight alsoshould be part of the sign-out docu-ment because it is often used for med-ication dosing and fluid calculationsduring the first 1 to 2 weeks after birth.Laboratory data (eg, total bilirubin)included on the sign-out could be an-notated with the patient’s age in hourswhen clinically appropriate. At somepoint, perhaps at 1 week after birth,automating the calculation of post-menstrual age lends context to an in-fant’s clinical status. Whereas the med-ical data in sign-out systems aretypically the patient’s own data, in-cluding key medical details about themother may be useful for the purposesof neonatal care.
Beyond TechnologyAlthough this review focuses ontechnological approaches to improv-ing communication, nontechnicalmethods must be employed to ad-dress flawed handoff processes; com-puterization alone is not sufficient toimprove communication in the set-ting of a poor process. (5)(25) Theprocess itself must be examined forcommunication failures, which de-fine the steps required for improve-ment. (24) Several authors have de-scribed methodologies for refiningthe handoff process, (26)(27) one ofwhich evaluates handoffs in nonmed-ical settings with high consequencesfor failure, such as nuclear powerplants and the NASA Johnson SpaceCenter. (28) Only after the handoffprocess has been defined can a com-puterized tool be designed to sup-port it effectively.
References1. Arora V, Johnson J, Lovinger D, Hum-phrey HJ, Meltzer DO. Communication
failures in patient sign-out and suggestionsfor improvement: a critical incident analysis.Qual Saf Health Care. 2005;14:401–4072. Streitenberger K, Breen-Reid K, HarrisC. Handoffs in care: can we make themsafer? Pediatr Clin North Am. 2006;53:1185–11953. Wilson RM, Runciman WB, GibberdRW, Harrison BT, Newby L, Hamilton JD.The Quality in Australian Health CareStudy. Med J Aust. 1995;163:458–4714. Mukherjee S. A precarious exchange.N Engl J Med. 2004;351:1822–18245. Van Eaton EG, Horvath KD, Lober WB,Pellegrini CA. Organizing the transfer ofpatient care information: the developmentof a computerized resident sign-out system.Surgery. 2004;136:5–136. Gray JE, Davis DA, Pursley DWM,Smallcomb JE, Geva A, Chawla NV. Net-work analysis of team structure in the neo-natal intensive care unit. Pediatrics. 2010;125:e14607. Cull W, Mulvey H, Jewett E, ZalneraitisE, Allen C, Pan R. Pediatric residency dutyhours before and after limitations. Pediat-rics. 2006;118:e1805–e18118. Chang VY, Arora VM, Lev-Ari S, D’ArcyM, Keysar B. Interns overestimate the effec-tiveness of their hand-off communication.Pediatrics. 2010;125:4919. Petersen LA, Brennan TA, O’Neil AC,Cook EF, Lee TH. Does housestaff discon-tinuity of care increase the risk for prevent-able adverse events? Ann Intern Med. 1994;121:866–87210. Horwitz LI, Krumholz HM, GreenML, Huot SJ. Transfers of patient care be-tween house staff on internal medicinewards: a national survey. Arch Intern Med.2006;166:1173–117711. The Joint Commission. Sentinel EventData - Root Causes by Event Type. 2011.Accessed July 2011 at: http://www.jointcommission.org/Sentinel_Event_Statistics/12. Kim GR, Lehmann CU, TechnologyCoCI. Pediatric aspects of inpatient healthinformation technology systems. Pediatrics.2008;122:e1287–e129613. Bates DW, Gawande AA. Improvingsafety with information technology. N EnglJ Med. 2003;348:2526–253414. Solet DJ, Norvell JM, Rutan GH,Frankel RM. Lost in translation: challengesand opportunities in physician-to-physiciancommunication during patient handoffs.Acad Med. 2005;80:1094–109915. Kilbridge P, Classen D. The informat-ics opportunities at the intersection of pa-tient safety and clinical informatics. J AmMed Inform Assoc. 2008;15:397–407
topics in neonatal informatics
e562 NeoReviews Vol.12 No.10 October 2011
by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from

16. Van Eaton EG, McDonough K, LoberWB, Johnson EA, Pellegrini CA, HorvathKD. Safety of using a computerizedrounding and sign-out system to reduceresident duty hours. Acad Med. 2010;85:1189–119517. Flanagan ME, Patterson ES, FrankelRM, Doebbeling BN. Evaluation of a phy-sician informatics tool to improve patienthandoffs. J Am Med Inform Assoc. 2009;16:509–51518. Petersen LA, Orav EJ, Teich JM,O’Neil AC, Brennan TA. Using a comput-erized sign-out program to improve conti-nuity of inpatient care and prevent adverseevents. Jt Comm J Qual Improv. 1998;24:77–8719. Frank G, Lawless ST, Steinberg TH.Improving physician communicationthrough an automated, integrated sign-
out system. J Healthc Inf Manag. 2005;19:68–7420. Bernstein JA, Imler DL, Sharek PJ,Longhurst CA. Improved physician workflow after integrating sign-out notes intothe electronic medical record. Jt Comm JQual Patient Saf. 2010;36:72–7821. Palma JP, Sharek PJ, Longhurst CA.Impact of electronic medical record integra-tion of a handoff tool on sign-out in a new-born intensive care unit. J Perinatol. 2011;31:311–31722. Sarkar U, Carter JT, Omachi TA, et al.SynopSIS: integrating physician sign-outwith the electronic medical record. J HospMed. 2007;2:336–34223. Sidlow R, Katz-Sidlow RJ. Using acomputerized sign-out system to improvephysician-nurse communication. Jt Comm JQual Patient Saf. 2006;32:32–3624. Van Eaton E. Handoff improvement:
we need to understand what we are tryingto fix. Jt Comm J Qual Patient Saf. 2010;36:5125. Coiera E. When conversation is betterthan computation. J Am Med Inform Assoc.2000;7:27726. Arora V, Johnson J. A model forbuilding a standardized hand-off protocol.Jt Comm J Qual Patient Saf. 2006;32:646–65527. Williams RG, Silverman R, Schwind C,et al. Surgeon information transfer andcommunication: factors affecting qualityand efficiency of inpatient care. Ann Surg.2007;245:159–16928. Patterson ES, Roth EM, Woods DD,Chow R, Gomes JO. Handoff strategies insettings with high consequences for failure:lessons for health care operations. Int J QualHealth C. 2004;16:125
topics in neonatal informatics
NeoReviews Vol.12 No.10 October 2011 e563 by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.12-10-e5602011;12;e560NeoReviews
Jonathan P. Palma, Erik G. Van Eaton and Christopher A. LonghurstNeonatal Care
Topics In Neonatal Informatics: Information Technology to Support Handoffs in
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/12/10/e560including high resolution figures, can be found at:
References
-1http://neoreviews.aappublications.org/content/12/10/e560.full#ref-listThis article cites 27 articles, 5 of which you can access for free at:
Subspecialty Collections
medicine_subhttp://classic.neoreviews.aappublications.org/cgi/collection/hospital_Hospital Medicineformation_technology_subhttp://classic.neoreviews.aappublications.org/cgi/collection/health_inHealth Information Technologyy_of_care_transition_-_discharge_planning_subhttp://classic.neoreviews.aappublications.org/cgi/collection/continuitContinuity of Care Transition & Discharge Planningfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.neoreviews.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.12-10-e5602011;12;e560NeoReviews
Jonathan P. Palma, Erik G. Van Eaton and Christopher A. LonghurstNeonatal Care
Topics In Neonatal Informatics: Information Technology to Support Handoffs in
http://neoreviews.aappublications.org/content/12/10/e560located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. Neoreviews is owned, published, and trademarked Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by guest on July 27, 2020http://neoreviews.aappublications.org/Downloaded from