-
8/10/2019 Inmunologia de Preeclampsia
1/11
-
8/10/2019 Inmunologia de Preeclampsia
2/11
ulated by the release of necrotic and/or apoptotic
syncytiotro-
phoblast cells into the maternal circulation [10]. As the
first
stage of preeclampsia mostly accounts for its origins, this
re-
view will discuss the second stage, as it is when the
maternal-
inflammatory response takes place, and most pathophysiologi-
cal processes occur. The second stage of preeclampsia may
also involve poor fetal growth and can be associated
indepen-dently with the development of intrauterine growth
restriction
[11]. However, not all babies from preeclamptic mothers are
born SGA, and intrauterine growth restriction may be more
frequent in early-onset preeclampsia than in late-onset pre-
eclampsia [12].
Some components of the innate and adaptive immune sys-
tem that may participate in the physiopathology of
preeclamp-
sia will be described here, as they produce certain
cytokines,
they modulate immune responses, or they have shown a modi-
fied function that may lead to the symptoms of this disease.
The pathophysiology of preeclampsia also involves altered
lev-
els of angiogenic factors, AT2-R autoantibodies [1315], and
the presence of different miRNAs [16, 17].
THE ROLE OF ANGIOGENIC/ANTIANGIOGENIC FACTORS AND
THEIRINTERACTION WITH THE IMMUNESYSTEM IN PREECLAMPSIA
The persistence of low-oxygen tensions or altered
oxygen-sens-
ing mechanisms in preeclampsia promotes placental overex-
pression of HIF-1[7, 18]. Later, an imbalance between pro-
and antiangiogenic factors can be observed in this syndrome.
Proangiogenic factors include the VEGF and PlGF, whereas
antiangiogenic factors that can be present in preeclamptic
pa-
tients are the sENG [19] and the sVEGF-R1 [20, 21] and
itsgeneric splice variant, known as sFlt1 [21]. sFlt1 inhibits
VEGF
and PlGF by binding to these factors in the maternal
circula-
tion and blocking their angiogenic effects [22]. Whereas
sFlt1
levels are relatively low early in normal pregnancy [23], in
the
presence of hypoxic conditions, sENG and sFlt1 are released
by the placenta [18, 24]. HIF-1 increases VEGF, ENG [25],
and sFlt1 expression [18]. sFlt1, which may be produced by
different cells, including endothelial cells [26] and the
hy-
poxic villous trophoblast, participates in the clearing of
free-
maternal VEGF [27]. Two isoforms of sVEGF-R1 have been
described: sFlt1, which is generic, and sFlt1-14, which is
hu-
man specific [21]. sFlt1-14, the most common VEGF inhibitor
produced by the human placenta in preeclampsia, is a C-termi-nal
variant isoform of sFlt1, and it is also known as sFlt1-e15a
[28]. Under hypoxic conditions, sFlt1-14 can accumulate in
the maternal circulation, neutralizing VEGF in distant
organs
and extending the consequences of preeclampsia [15]. High
levels of sFlt1 and low levels of PlGF may predict the
subse-
quent development of preeclampsia, as it may be detected 5
weeks before its onset [29].
sFlt1 levels differ in early- and late-onset preeclampsia.
sFlt1
levels are higher in early-onset preeclampsia, making sFlt1
a
possible biomarker for the early-onset form of this syndrome
[30]. As sFlt1 is secreted under hypoxic conditions, the
differ-
ences in sFlt1 levels in women that develop the disease
earlier
or later in pregnancy may be reflecting different oxygen
con-
centrations in preeclamptic patients.
Components of the immune system, especially cytokines,
may be interacting with angiogenic and antiangiogenic
factors
in preeclampsia. As sENG is increased in preeclampsia, and
it
binds TGF-, compromising its function and/or bioavailability
[23], it may be possible that sENG could affect the levels
ofTGF-required for iTreg. On the other hand, the levels of
TNF-present in preeclamptic patients can also promote the
release of sFlt1 [13], especially under chronic hypoxic
condi-
tions [31]. Likewise, the binding of AT1-AA, which will be
described later in the manuscript, can promote the secre-
tion of sENG and sFlt1 through TNF--mediated mecha-
nisms [32, 33].
THE ROLE OF miRNAs INPREECLAMPSIA
miRNAs are nonprotein-coding RNAs that regulate gene ex-
pression and may play a role in the pathogenesis of
pre-eclampsia, also serving as possible biomarkers for this
disease
[34]. Several miRNAs have been found elevated in placentas
with preeclampsia. For example, in severe preeclampsia, miR-
16, miR-29b, miR-195, miR-26b, miR-181a, miR-335, and miR-
222 are increased significantly in the placenta [35].
Placentas
with preeclampsia and preeclampsia complicated with SGA
newborns express miR-182 and miR-210, which are not present
in placentas related to SGA alone, SGA hypertension, or in
normal placentas [36]. miR-182 has been related T cell
clonal
expansion [37], to cell cycle, and to apoptosis pathways
[38].
miR-182 is present in placentas with severe preeclampsia, it
may regulate angiogenesis via VEGF, and it is also acknowl-
edged as a regulator of the transcript variants 1 and 2 of the
Bcell lymphoma 2-like gene [16]. On the other hand, miR-210
is a potent miRNA up-regulated by hypoxia [17] that can in-
hibit the migration and invasion ability of trophoblast
cells
[39]. Another miRNA overexpressed in preeclampsia that may
contribute to its development by down-regulating the angio-
genic-regulating factor CYR61 is miR-155 [40]. miRNAs may
not only be key players in the pathophysiology of preeclamp-
sia, but they may also help differentiate pathologic aspects
in
placentas affected by preeclampsia, preeclampsia complicated
with SGA, and SGA alone.
IMMUNE SYSTEM CELLS AND STBMs
In normal pregnancies, STBMs present in the maternal circu-
lation may stimulate the production of several cytokines by
peripheral monocytes [41]. The recognition of STBMs by pe-
ripheral mononuclear leukocytes has been related to inhibi-
tion of IFN-production and to decreased levels of IP-10 in
the first trimester of normal pregnancies [42]. These
changes
promote a shift toward type 2 T cell responses that is
essential
for gestation [43]. In preeclampsia, however, significantly
higher levels of sSTBMs are present compared with normal
pregnancies [44]; suppression of IFN-production by NK cells
and other lymphocytes that were stimulated with STBMs does
2 Journal of Leukocyte Biology Volume 94, July 2013
www.jleukbio.org
-
8/10/2019 Inmunologia de Preeclampsia
3/11
not occur; and these cells continue to secrete IFN-, IL-18,
TNF-, and IL-12 [42]. STBMs bind predominantly to recep-
tors on monocytes and some B cells, inducing phagocytosis
[43]. The receptors that participate in STBM recognition
have
not been identified clearly but may include RAGE and TLRs
[41]. Higher amounts of STBMs released by the placenta may
play a role in promoting a more robust inflammatory response[41]
in pregnant women. However, the conditions under
which the trophoblast microparticles are released may also
be
relevant, as microparticles derived from a hypoxic
trophoblast
induce higher concentrations of IL-6 and TNF- from PBMCs
that recognize STBMs than do particles derived from a normal
trophoblast [45]. Furthermore, STBMs from preeclamptic pla-
centas exacerbate LPS responses in PBMCs [46]. This may
help to explain the increased production of cytokines in
pre-
eclampsia, in which the placenta can be hypoxic, and may
also
be related to the generation of DAMPs under these hypoxic
environments.
In addition to cytokines derived from activated peripheral
granulocytes and monocytes, lymphocyte-derived cytokines
areprobably secondary to the activation of endothelial cells by
STBMs and may be involved in the pathophysiology of pre-
eclampsia [47].
THE INNATE IMMUNE SYSTEM IN THEPATHOPHYSIOLOGY OF
PREECLAMPSIA
TLRs in preeclampsiaAccording to the danger model [48], hypoxia
can lead to a
persistent inflammatory response, and this may occur in pre-
eclamptic patients. A key inflammatory factor in
preeclampsia
is the recognition of DAMPs that can result from endothelialcell
dysfunction, changes in glucose metabolism, hypoxia, or
oxidative stress [49]. In hypoxic microenvironments, DAMPs
may not be oxidized and denatured and thus, may promote
inflammation [50] through ligation of receptors, such as
RAGE, TLR2, and TLR4, which are expressed in immune sys-
tem cells [51]. S100 and HMGB1 are proteins that behave as
DAMPs [51, 52]. High cytoplasmic expression of HMGB1 oc-
curs in decidual cells of preeclamptic patients [53], and
S100B
is increased in amniotic fluid during preeclamptic
pregnancies
[54] in direct relation to oxidative stress [55].
Furthermore,
expression of TLR4 [56], TLR2, TLR3, and TLR9 is increased
in trophoblasts of preeclamptic patients [57]. The
expression
of TLRs and RAGE receptors by the placenta shows its poten-tial
ability to respond to DAMPs, although the role of the pla-
centa in this matter remains unknown [53]. In mice, TLR3
activation can increase systolic blood pressure and
endothelial
dysfunction, especially in the absence of IL-10 [58].
Although
this alteration has not been proven in humans, the findings
may be relevant, as preeclamptic women have decreased levels
of IL-10 [59]. Moreover, placentas of preeclamptic women
have increased expression of TLR3, TLR7, and TLR8 com-
pared with those of normal human pregnancies, and the acti-
vation of TLR3, -7, and -8 by dsRNAs and ssRNAs promotes
pregnancy-dependent, proteinuric hypertension and endothe-
lial dysfunction in mice [60]. Likewise, the binding of
circulat-
ing fetal DNA to TLR9 in mice can activate an inflammatory
response, leading to IL-6 secretion [61]. This may be
particu-
larly crucial in human preeclampsia, in which high levels of
circulating fetal DNA may be present [62]. Fetal DNA can
bind TLR9 promoting inflammation, and TLR9 signaling may
represent a potential therapeutic pathway, as it may be
blocked by pharmacological agents, such as chloroquine
[61].Maternal infections, especially urinary infections and
peri-
odontal disease, have been associated with an increased risk
of
preeclampsia [63]. As many pathogens are recognized by TLRs
[64], pathogens may also be increasing TLR activation in
this
syndrome. Thus, in preeclampsia, STBMs, pathogens, and
DAMPs may participate as important activators of inflamma-
tory processes. These mechanisms involve binding to TLRs,
making these receptors possible therapeutic targets for pre-
eclampsia.
Transcription factors, NF-B and TLRs, inpreeclampsia
It has been proposed that transcription factors may help usgain
insight into the pathophysiology of preeclampsia. On this
matter, microarray studies have shown a higher prevalence of
E-47, sterol regulatory element-binding protein, and NF-Bp50
transcription factor-binding sites in placentas complicated
with
preeclampsia [65]. NF-B is a regulator of inflammatory gene
expression, it promotes the production of proinflammatory
cytokines, and is highly activated in some inflammatory dis-
eases [66]. In patients with preeclampsia, increased
transloca-
tion of nuclear NF-B has been found in peripheral blood-
activated leukocytes [67]. Whereas the activation of NF-B
may
be associated to the presence of increased oxidative stress
in
preeclampsia [68], it is possible that TLRs may also be pro-
moting an increase of NF-B in this syndrome, as all TLR
sig-naling pathways culminate in the activation of this
transcrip-
tion factor [69].
Regarding possible therapeutic strategies affecting NF-B
pathways, 5-deoxy-(12,14)-PGJ(2) has been proposed as a
therapeutic alternative to modulate NF-B signaling in preg-
nancy, as it may decrease IFN-and TNF- production
through inhibition of NF-B in PBMCs of pregnant
women [70].
Monocytes promoting inflammatory conditions inpreeclampsia
Leukocytes from the nonspecific or innate immune system
areimportant in normal pregnancy, as they promote successful
implantation and participate in several events at the
feto-ma-
ternal interface [71]. These cells may, however, also be in-
volved in the pathophysiology of pregnancy disorders [72].
Activated monocytes and neutrophils are present in the fetal
and placental circulation under hypoxic conditions and may
contribute to the increased vascular resistance and
morbidity
of the fetus observed in preeclampsia [9].
Trophoblast cells under hypoxic conditions, such as those in
preeclampsia, produce high concentrations of IL-6 and IL-8
and low IL-10 levels [73]. Nevertheless, the placenta is not
the
only contributor to the production of inflammatory cytokines
Laresgoiti-Servitje The immune system in the pathophysiology of
preeclampsia
www.jleukbio.org Volume 94, July 2013 Journal of Leukocyte
Biology 3
-
8/10/2019 Inmunologia de Preeclampsia
4/11
in preeclampsia [74]. Monocytes may represent an important
source of proinflammatory cytokines in preeclampsia, as
monocytes from preeclamptic patients secrete high levels of
IL-1, IL-6, and IL-8 [75]. These cells have been classified
into
three subsets, according to their expression of CD14 (LPS
re-
ceptor) and CD16 (FCRIII). Classical monocytes are
CD14
CD16
, intermediate monocytes are CD14
CD16
,and nonclassical monocytes are CD14CD16 [76]. Women
with normal pregnancies have low percentages of classical
monocytes and higher percentages of nonclassical/intermedi-
ate monocytes compared with nonpregnant women [77]. Non-
classical and intermediate monocytes are even higher in pre-
eclampsia than in normal pregnancies [77, 78], and they show
up-regulated expression of TLR4 [78], reflecting the impor-
tance of TLRs and TLR ligands in this syndrome. The exact
function of the different subsets of monocytes in pregnancy
and preeclampsia is unknown. In nonpregnant humans, inter-
mediate monocytes are predisposed toward antigen presenta-
tion. They secrete inflammatory cytokines and ROS and may
participate in angiogenesis [79]. In contrast,
nonclassicalmonocytes may exhibit DC characteristics and produce
IL-12
and IL-8 [80].
During pregnancy, TNF-, IL-6, and other proinflammatory
cytokines derived from monocytes can activate the RAS, pro-
mote oxidative stress, and may lead to an increase in
endothe-
lium-derived vascular contracting molecules to diminish the
bioavailability of vascular-relaxing factors derived from the
en-
dothelium [81, 82]. Furthermore, elevated TNF- levels corre-
late with the activity of AT1-R autoantibodies and an
increase
in sFLT-1 and sENG levels through AT1-R-mediated TNF-induction
[33].
Neutrophils and oxidative stress in preeclampsiaNeutrophils are
activated in the peripheral blood [83, 84] andin the decidua of
preeclamptic patients, and elastase produced
by these cells may contribute to vascular damage [85]. In
fact,
neutrophils are strongly associated with vascular dysfunction
in
preeclamptic women, as they adhere to the endothelium in
high densities [86]. Increased expression of IL-8 and ICAM-1
in vessels of preeclamptic women contributes to the
infiltra-
tion of neutrophils into the maternal systemic vasculature
[86]. Later, neutrophil adhesion to endothelial cells is
linked
to increased expression of CD11b, and neutrophil adhesion
may be promoted by overproduction of superoxides and hy-
drogen peroxide [87]. Moreover, oxidants generated by acti-
vated neutrophil NADPH oxidase may react with different tar-gets
to form toxic metabolites that are products of lipid per-
oxidation, such as 4-hydroxynonenal, which contributes to
microbial death and the damage induced by neutrophils [88].
Lipid peroxidation is elevated before and after childbirth
(and
delivery of the placenta) in women with preeclampsia,
suggest-
ing that these patients are under persistent oxidative
stress
that contributes to an inflammatory response [89]. Neutro-
phils may be carriers of cellular oxidative stress from the
pla-
centa to the vascular environment of the mother [90].
Neutrophil activation results from exposure to hypoxic or
inflammatory conditions [89]. Placental microparticles, such
as
STBMs, may act as inflammatory agents, as in preeclampsia,
the release of STBMs can activate neutrophils and promote
formation of NETs [91]. NETs are extracellular structures
composed of chromatin and granular proteins released during
the death process, which occurs upon neutrophil stimulation.
In this process, euchromatin and heterochromatin are homog-
enized, the nuclear and granular membranes disintegrate, and
these components combine to create the NET. The NET isliberated
when the cellular membrane breaks; it then binds to
and kills microorganisms [92]. In the preeclamptic placenta,
many NETs are induced in the intervillous space as a result
of
stimulation of neutrophils by STBMs and IL-8 [91]. As NETs
participate in the pathogenesis of inflammatory disorders
and
autoimmunity [93], they may also contribute to the pathogen-
esis of preeclampsia, playing a role in the deficient
placental
perfusion associated with this disease [94]. In epithelial
and
endothelial cells, NETs can induce cytotoxicity, which is
mostly
mediated by histones and MPO [95]. The death process that
initiates NET formation, called NETosis, is different from
ne-
crosis and apoptosis and depends on autophagy [96], genera-
tion of ROS, and NADPH oxidase [92], which is required
toincrease neutrophil adhesion to the endothelium.
Besides oxidative stress-induced inflammation and endothe-
lial dysfunction, preeclamptic patients also have increased
lev-
els of MPO. This enzyme is produced by activated monocytes
and neutrophils and may contribute to placental and endothe-
lial oxidative damage and the dysfunction of endothelial
cells
reported in these patients [97].
NK cellsPlacental NK cells, designated as uNK cells, play an
important
role in the acceptance and rejection of the fetus, as they are
in
direct contact with the trophoblasts [98]. uNK cells produce
decidual IFN-in early human pregnancy, during which theymay
inhibit the invasion of the extravillous trophoblast [99]
and probably promote a CD4 Th1 cytokine profile in pre-
eclamptic women. Their participation may be more relevant
during the origins of preeclampsia. Peripheral NK cells from
preeclamptic women express lower intracellular VEGF levels
than those from normal pregnant women [100], a finding that
may link these cells with the endothelial dysfunction seen
in
this syndrome. Moreover, as NK cells express functional TLR3
and TLR9, they can recognize RNA and CpG DNA, which pro-
motes their activation, especially in the presence of IL-8
[101].
Components of STBMs are also ligands for the NK cell recep-
tor NKG2D [102]. Thus, STBMs or fetal DNA may interact
with NK cells in patients with preeclampsia.
NK cells also express several components of the RAS, such
as renin, angiotensinogen, angiotensin-converting enzyme,
and
AT1-R and AT2-R, making NK cells responsive to AT2 levels
[103]. Considering that preeclampsia may be related to dys-
regulation of the RAS [104], the presence of AT1-R and
AT2-R in NK cells could be relevant in this syndrome.
DCsBesides B cells and macrophages, DCs function as APCs
dur-
ing pregnancy and can modulate immune responses [105].
DCs are the link between the innate and adaptive immune
4 Journal of Leukocyte Biology Volume 94, July 2013
www.jleukbio.org
-
8/10/2019 Inmunologia de Preeclampsia
5/11
system, as they can respond to a variety of stimuli, such as
TLR
ligands, cytokines, and immune complexes [106]. These cells
are particularly relevant during pregnancy, as they may
modu-
late immune responses, depending on their activation through
different TLRs or depending on the cytokine microenviron-
ments in which their activation occurs [107].
Decidual CD14
DC-SIGN
DCs may play an important rolein iTreg induction, and in
preeclampsia, CD14DC-SIGN
and CD14DC-SIGN decidual DCs induce iTreg cells poorly
[108]. Regarding peripheral blood DCs, human myeloid DCs
(DC-1) are CD4CD11chighCD123lowCD45ROBDCA-1,
and plasmacytoid (lymphoid) DCs (DC-2) in peripheral blood
are CD4CD11cCD123highCD45RABDCA-2 [109]. The
percentage of BDCA-2 lymphoid DCs is significantly lower in
the blood of preeclamptic patients compared with women in
the third trimester with normal pregnancies [110]. Consider-
ing that CD11c (BDCA-1) myeloid DCs produce IL-12 and
may modulate toward Th1 responses [111] and that lymphoid
CD303 (BDCA-2) DCs can promote a shift toward Th2 re-
sponses [112], the decreased number of lymphoid DCs inblood of
preeclamptic women is noteworthy. Furthermore,
suppression of Th1 responses by DCs may be associated with
expression of serpin in myeloid APCs, which is a plasminogen
activator inhibitor [113] that is decreased in preeclamptic
women [114]. Myeloid and plasmacytoid DCs respond to TLR
ligands, depending on their TLR expression. Myeloid DCs ex-
press TLR16 and TLR8, whereas plasmacytoid DCs strongly
express TLR7 and TLR9 and have a low expression of TLR4
and TLR2 [115]. TLRs may represent a possible therapeutic
target in this syndrome, as DCs in women with preeclampsia
also show increased expression of basal TLR3, TLR4, and
TLR9 and secrete higher levels of IFN-, TNF-, IL-1, and
IL-12 [116].
Because of changes in expression of TLRs in DCs in pre-
eclampsia, it may be relevant to evaluate to what extent
TLR9
ligands, such as oligodeoxynucleotides containing unmethyl-
ated CpG motifs, or TLR7 ligands, such as RNA [117], may
participate in the overproduction of IFNs and the modulation
of the immune response in preeclamptic patients.
Until recently, the stage of DC maturation was considered to
be essential for their ability to induce Tregs or activate
inflam-
matory T cell responses, but the developmental stage is no
longer considered a key factor that differentiates between
tolerogenic versus immunogenic DCs [118]. It is not the
matu-
ration state but the inflammatory factors or cytokines
presentduring DC maturation that may influence the ability of DCs
to
induce different T cell responses [119]. The role of DCs in
preeclampsia requires further investigation. Factors
promoting
the polarization of lymphoid versus myeloid DCs and the fac-
tors present during their maturation in preeclampsia remain
unclear. The participation of TLRs and their ligands in DCs
may help broaden our perspective regarding the role of these
cells in the pathophysiology of preeclampsia.
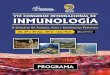
Figure 1 shows possible ligands for TLRs and their roles in
preeclampsia. The activation of innate immune system cells
that participate in the pathophysiology of preeclampsia is
also
described.
THE ADAPTIVE IMMUNE SYSTEM
In preeclampsia, the Th1/Th2 paradigm has been used to
explain T cell behavior, as a shift from a Th1 to a Th2 phe-
notype at the fetal-maternal interface may not occur in this
syndrome. Whereas Th1 cytokines, including IL-1, IL-2, and
IFN-, are predominant in preeclampsia, the production of
Th2 cytokines, including IL-10 and IL-5, can be decreased[120].
The changes in cytokine microenvironments, includ-
ing elevated IFN- levels [121123], occur during the first
weeks of pregnancy and promote a CD4 Th1 lymphocyte
cytokine profile that can persist further into the
preeclamp-
tic pregnancy. The presence of low IL-10 levels in pre-
eclampsia is also relevant [59], as IL-10 protects the fetus
from rejection during normal pregnancy via activation of
HLA-G expression in trophoblasts and monocytes at the fe-
tal-maternal interface [124]. Although many women with
preeclampsia present a shift toward Th1 cytokines, the
Th1/Th2 paradigm does not respond to all of the questions
regarding immune regulation in preeclampsia. The sole use
of this paradigm to explain immunological aspects partici-pating
in the pathophysiology of this syndrome could be
oversimplifying the mechanisms involved, as patients with
preeclampsia can have changes in other T lymphocyte sub-
sets. The alterations in numbers and function of Th17 cells
and Tregs may help us understand more clearly the role of
lymphocytes in the pathophysiology of preeclampsia.
T lymphocyte subsetsOne CD4 lymphocyte subset that may be
involved in the
pathophysiology of preeclampsia is the CD4CD25FoxP3
Treg (FoxP3 is a Treg transcription factor) [125]. Some re-
searchers have found no differences in Treg numbers
betweenhealthy and preeclamptic pregnancies [126]. Others have
re-
ported reduced numbers of Tregs in preeclampsia compared
with normal pregnancies [127, 128]. CD4CD25FoxP3 Treg
function is reduced in preeclampsia, which may be related to
the presence of inflammatory conditions [129]. Moreover, the
Treg pool in preeclamptic patients consists mostly of
CD4CD25FoxP3HLA-DRCD45RA cells. Although these
cells express HLA-DR, which is related to suppression activ-
ity, they exhibit reduced regulatory capacity [125]. Thus,
Tregs and Treg subsets seem to play a role in the patho-
physiology of preeclampsia, but their role remains unclear.
The presence of increased levels of sENG, a protein
thought to impair TGF- binding to receptors, could beblocking
TGF- signals required for Treg functions and may
participate in changes in this cell population in preeclamp-
sia [130].
In addition to Tregs, CD4 IL-17-producing T cells (Th17)
may participate in preeclampsia. Preeclamptic patients have
a
lower ratio of Tregs:Th17 cells [131]. T cell polarization is
re-
lated to an imbalance of T cell transcription factors in
PBMCs
and in the decidua of preeclamptic patients. Decreased mRNA
levels of FoxP3 and increased levels of the Th17
transcription
factor RORc and the Th1 transcription factor T-bet are pres-
ent in preeclamptic women compared with healthy pregnant
women [132]. The predominance of Th17 cells in pre-
Laresgoiti-Servitje The immune system in the pathophysiology of
preeclampsia
www.jleukbio.org Volume 94, July 2013 Journal of Leukocyte
Biology 5
-
8/10/2019 Inmunologia de Preeclampsia
6/11
eclampsia, accompanied by decreased Treg function and an
altered balance in the Th17:Treg ratio [129], may be a re-
sult of altered levels of cytokines, including IL-6 and
IL-1,
that promote differentiation of these cells from progenitor
cells [133]. However, CD8 lymphocytes and NK cells also
secrete IL-17 and may contribute to inflammation in this
syndrome [134].
T lymphocytes also possess functional RAS elements, able to
produce AT2 at inflammatory sites. As AT2 can promote che-
motaxis of NK cells and T cells by binding to AT1-R, a RAS-
mediated inflammatory pathway may also be involved in
pre-eclampsia [103].
The role of B lymphocytes and antibodies inpreeclampsiaA CD19
CD5 B cell population, which is able to produce
AT1-AAs, has been identified in the placenta of preeclamptic
patients [135]. These human CD19 CD5 B cells share phe-
notypic properties with murine B-1a lymphocytes [136]. In
mice, B-1a cells have been involved in the generation of
auto-
antibodies [137]. Likewise, human CD19 CD5 B cells may
become autoreactive [138], as they are able to activate
somatic
hypermutation mechanisms that can promote mutations in the
variable regions of the BCR [139]. This is a reason why
human
peripheral blood and spleen CD5 B cells may produce poly-
specific, autoreactive antibodies [140]. The identification
of
CD19 CD5 B cells that can produce AT1-AAs [135] repre-
sents an important step in the understanding of the patho-
physiology of preeclampsia. However, the mechanisms promot-
ing the development of AT1-R autoantibodies have not been
described yet.
AT1-AAs of the IgG isotype [141] are present in 70 95% of
preeclamptic patients [30, 142], they bind to receptors in
hu-
man trophoblast and vascular cells [143], and their
bindinginduces sFlt1 and sENG production by human villous
explants
through TNF-pathways [32, 33]. Binding of AT1-AA in-
creases TNF- signaling in human placental villous explants,
which then promotes IL-6 production that induces endothe-
lin-1 production [144]. AT1-AAs, by ligating to the AT1-R on
vascular smooth muscle cells, may also promote vasoconstric-
tion [145] and can mediate hypertension by promoting pla-
cental oxidative stress [14, 146]. High levels of AT1-AAs
are
associated with the presence of hypertension, proteinuria,
and
sFlt1 and may correlate with the severity of the disease
[142]. Moreover, AT1-AAs may be a possible biomarker for
late-onset preeclampsia [30]. As AT1-AAs can cross the pla-
Figure 1. In normal pregnancy, low levels of STBMs contribute to
the inhibition of IFN-production and a shift toward Th2 responses.
In pre-eclampsia, however, persistent hypoxia, the presence of free
fetal DNA, and the shedding of high amounts of STBMs into the
maternal cir-culation promote inflammatory conditions, in which
neutrophils (NTs), monocytes (MNs), NK cells, endothelial cells
(ECs), and DCs arestimulated. Neutrophil stimulation results in the
activation of elastases and the production of superoxides and
hydrogen peroxide viaNADPH and MPO activation, respectively. Direct
stimulation of neutrophils by STBMs may also result in damage
through NET formation.Superoxides also promote neutrophil adhesion
to the endothelium and NET formation at this level. Consequently,
neutrophil activation re-sults in vascular damage and dysfunction.
In contrast, the nonclassical and intermediate monocytes in the
presence of up-regulated TLR4secrete cytokines and may contribute
to the persistent inflammatory conditions. Plasmacytoid and myeloid
DCs (pDCs and mDCs, respec-tively) also respond to TLR ligands and
can modulate T cell responses. NK cells may play a role in the
production of IFN- and the shifttoward Th1 responses and may also
respond to TLR ligands.
6 Journal of Leukocyte Biology Volume 94, July 2013
www.jleukbio.org
-
8/10/2019 Inmunologia de Preeclampsia
7/11
cental barrier [104], these antibodies may also contribute
to
intrauterine growth restriction in some patients with pre-
eclampsia, directly by activating AT1-R on the surface of
fe-
tal organs and indirectly by induction of apoptosis in the
placenta [147]. AT1-AAs do not disappear completely after
childbirth [148].
AT1-AAs are not the only autoantibodies that have been
de-scribed in preeclamptic patients. The presence of
autoantibod-
ies against1, 2, and 1 adrenoreceptors has been demon-
strated in patients with severe preeclampsia and may
increase
the risk of neonatal morbidity and mortality [149]. Further
studies are needed to identify the factors triggering their
pro-
duction and plausible mechanisms by which these antibodies
may promote severe preeclampsia.
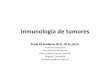
The participation of B cells and different T cell subsets
and
the possible mechanisms that modulate their activity are de-
scribed inFig. 2.
CONCLUSIONS
Persistent hypoxia, alterations in oxygen-sensing mecha-
nisms at the placental level, and increased levels of sSTBMs
from the placenta are important factors that can contribute
to the pathophysiology of preeclampsia. The increased shed-
ding of STBMs from the placenta during preeclampsia may
promote endothelial cell dysfunction and activation of ma-
ternal leukocytes, such as monocytes, neutrophils, NK cells,
and DCs. Whereas monocytes are involved in the secretion
of proinflammatory cytokines and may be promoting persis-
tent inflammatory conditions in the preeclamptic patient,
neutrophils play an important role in the vascular damage
seen in preeclampsia. Neutrophils can be activated by in-
flammatory conditions caused by STBMs and persistent hyp-oxia.
They may harm the endothelium through NET forma-
tion, elastase activation, or superoxide-related damage,
pro-
moting vascular dysfunction that results in increased
vascular resistance. On the other hand, changes in DC sub-
types may also participate in preeclampsia. Lower levels of
lymphoid BDCA-2 DCs in preeclampsia could promote
Th1-type responses in this syndrome, and they may be regu-
lated by TLR3 and TLR9 ligands.
As TLRs can act as receptors for STBMs, fetal DNA, andDAMPs,
TLRs may play a key role in maintaining inflamma-
tory conditions in preeclampsia. Moreover, TLRs may repre-
sent important therapeutic targets in this syndrome. Further
research is needed regarding the role of TLRs in the recog-
nition of STBMs and DAMPs in preeclampsia and their pos-
sible relationship with the modulation of DCs and T cell
subsets.
CD19CD5 B cells, by producing AT1-AAs, are important
contributors to the pathophysiology of preeclampsia and have
rendered preeclampsia as a syndrome with autoimmune char-
acteristics. This concept is also supported by the presence
of
autoantibodies against adrenoreceptors in patients with
severe
preeclampsia. However, the factors promoting the production
of adrenoreceptor autoantibodies and the mechanisms by
which these antibodies participate in preeclampsia still need
to
be explored. Many questions remain regarding the interaction
between angiogenic/antiangiogenic factors with immune sys-
tem cells and the possible participation of miRNAs in immune
system regulation in preeclampsia.
The immune system plays an important role in many patho-
physiological processes occurring in preeclamptic patients.
This review aimed to examine the participation of several
com-
ponents of the immune system in the pathophysiology of pre-
eclampsia. However, it has its limitations, as because of
the
great amount of cells and molecules that may be implicated, itis
not possible to give a comprehensive overview of all of the
interactions involved in this syndrome.
Figure 2. Although changes in T cell subsets maybe present at
the origin of preeclampsia, thepersistence of inflammatory
conditions pro-moted by hypoxia, increased STBMs, or freefetal DNA
via activation of the innate immunesystem cells may affect the
generation of differ-ent T cell responses. Preeclamptic women
havelower mRNA levels of FoxP3, increased numbersof Th17, increased
RORc mRNA, and increasedTh1 T-bet mRNA. High IFN-concentrations
maypromote the development of Th1 lymphocytes,whereas IL-1, IL-6,
and IL-7 may promote the gen-eration of Th17 lymphocytes in
preeclampticwomen. These changes can result in a reducedregulatory
capacity of Tregs in preeclampsia and alow Treg:Th17 ratio. High
levels of sENG could beaffecting TGF-signaling required for
iTreg.CD19 CD5 B cells participate in the patho-physiology of
preeclampsia by producing AT1-AAs.Factors promoting the development
of these anti-bodies have not been described yet.
Laresgoiti-Servitje The immune system in the pathophysiology of
preeclampsia
www.jleukbio.org Volume 94, July 2013 Journal of Leukocyte
Biology 7
-
8/10/2019 Inmunologia de Preeclampsia
8/11
DISCLOSURES
The author declares no conflicts of interest.
REFERENCES
1. Davey, D., Macgillivray, I., James, M. R., Richard, J. L.
(1989) Classifica-tion of hypertensive disorders in pregnancy.
Lancet334, 112113.
2. Chappell, L. C., Enye, S., Seed, P., Briley, A. L., Poston,
L., Shennan,A. H. (2008) Adverse perinatal outcomes and risk
factors for pre-eclampsia in women with chronic hypertension: a
prospective study.Hypertension51, 10021009.
3. James, J. L., Stone, P. R., Chamley, L. W. (2005)
Cytotrophoblast differ-entiation in the first trimester of
pregnancy: evidence for separate pro-genitors of extravillous
trophoblasts and syncytiotrophoblast. Reproduc-tion130, 95103.
4. Roberts, J. M., Gammill, H. S. (2005) Preeclampsia: recent
insights.Hypertension46, 12431249.
5. Kaufmann, P., Black, S., Huppertz, B. (2003) Endovascular
trophoblastinvasion: implications for the pathogenesis of
intrauterine growth retar-dation and preeclampsia. Biol. Reprod.69,
17.
6. Odegard, R. A., Vatten, L. J., Nilsen, S. T., Salvesen, K.
A., Austgulen,R. (2000) Preeclampsia and fetal growth. Obstet.
Gynecol. 96, 950955.
7. Rolfo, A., Many, A., Racano, A., Tal, R., Tagliaferro, A.,
Ietta, F., Wang,J., Post, M., Caniggia, I. (2010) Abnormalities in
oxygen sensing defineearly and late onset preeclampsia as distinct
pathologies. PLoS ONE5,e13288.
8. Laresgoiti-Servitje, E., Gmez-Lpez, N., Olson, D. M. (2010)
An im-munological insight into the origins of pre-eclampsia. Hum.
Reprod. Up-date16, 510524.
9. Mellembakken, J. R., Aukrust, P., Hestdal, K., Ueland, T.,
Abyholm, T.,Videm, V. (2001) Chemokines and leukocyte activation in
the fetal cir-culation during preeclampsia. Hypertension38,
394398.
10. Sargent, I. L., Borzychowski, A. M., Redman, C. W. G. (2006)
Immuno-regulation in normal pregnancy and pre-eclampsia: an
overview. Rep.BioMed. Online13, 680686.
11. Srinivas, S. K., Edlow, A. G., Neff, P. M., Sammel, M. D.,
Andrela,C. M., Elovitz, M. A. (2009) Rethinking IUGR in
preeclampsia: depen-dent or independent of maternal hypertension?
J. Perinatol.29, 680684.
12. Van der Merwe, J. L., Hall, D. R., Wright, C., Schubert, P.,
Grov, D.(2010) Are early and late preeclampsia distinct subclasses
of the dis-easewhat does the placenta reveal? Hypertens.
Pregnancy29, 457467.
13. Parrish, M. R., Murphy, S. R., Rutland, S., Wallace, K.,
Wenzel, K., Wal-lukat, G., Keiser, S., Ray, L. F., Dechend, R.,
Martin, J. N., Granger,J. P., LaMarca, B. (2010) The effect of
immune factors, tumor necrosis
factor-, and agonistic autoantibodies to the angiotensin II type
I re-ceptor on soluble fms-like tyrosine-1 and soluble endoglin
productionin response to hypertension during pregnancy. Am. J.
Hypertens. 23,911916.
14. Parrish, M. R., Wallace, K., Tam Tam, K. B., Herse, F.,
Weimer, A.,Wenzel, K., Wallukat, G., Ray, L. F., Arany, M.,
Cockrell, K., Martin,J. N., Dechend, R., LaMarca, B. (2011)
Hypertension in response toAT1-AA: role of reactive oxygen species
in pregnancy-induced hyper-tension. Am. J. Hypertens. 24,
835840.
15. Sela, S., Itin, A., Natanson-Yaron, S., Greenfield, C.,
Goldman-Wohl, D.,Yagel, S., Keshet, E. (2008) A novel
human-specific soluble vascularendothelial growth factor receptor
1: cell type-specific splicing and im-plications to vascular
endothelial growth factor homeostasis and pre-eclampsia.Circ.
Res.102, 1566 1574.
16. Noack, F., Ribbat-Idel, J., Thorns, C., Chiriac, A.,
Axt-Fliedner, R.,Diedrich, K., Feller, A. C. (2011) miRNA
expression profiling in forma-lin-fixed and paraffin-embedded
placental tissue samples from preg-nancies with severe
preeclampsia. J. Perinat. Med. 39, 267271.
17. Zhang, Z., Sun, H., Dai, H., Walsh, R., Imakura, M.,
Schelter, J., Bur-
chard, J., Dai, X., Chang, A. N., Diaz, R. L., Marszalek, J. R.,
Bartz,S. R., Carleton, M., Cleary, M. A., Linsley, P. S., Grandori,
C. (2009)MicroRNA miR-210 modulates cellular response to hypoxia
throughthe MYC antagonist MNT. Cell Cycle8, 2756 2768.
18. Nevo, O., Soleymanlou, N., Wu, Y., Xu, J., Kingdom, J.,
Many, A., Za-mudio, S., Caniggia, I. (2006) Increased expression of
sFlt-1 in in vivoand in vitro models of human placental hypoxia is
mediated by HIF-1.Am. J. Physiol. 291, R1085R1093.
19. Levine, R. J., Lam, C., Qian, C., Yu, K. F., Maynard, S. E.,
Sachs, B. P.,Sibai, B. M., Epstein, F. H., Romero, R., Thadhani,
R., Karumanchi,S. A., CPEP Study Group (2006) Soluble endoglin and
other circulat-ing antiangiogenic factors in preeclampsia. N. Engl.
J. Med. 355, 9921005.
20. Gould, P. S., Gu, M., Liao, J., Ahmad, S., Cudmore, M. J.,
Ahmed, A.,Vatish, M. (2010) Upregulation of urotensin II receptor
in preeclamp-sia causes in vitro placental release of soluble
vascular endothelialgrowth factor receptor 1 in
hypoxia.Hypertension56, 172178.
21. Sela, S., Natanson-Yaron, S., Zcharia, E., Vlodavsky, I.,
Yagel, S., Keshet,E. (2011) Local retention versus systemic release
of soluble VEGF re-
ceptor-1 are mediated by heparin-binding and regulated by
hepara-nase. Circ. Res.108, 10631070.
22. Maynard, S. E., Min, J-Y., Merchan, J., Lim, K-H., Li, J.,
Mondal, S.,Libermann, T. A., Morgan, J. P., Sellke, F. W.,
Stillman, I. E., Epstein,F. H., Sukhatme, V. P., Karumanchi, S. A.
(2003) Excess placental solu-ble fms-like tyrosine kinase 1 (sFlt1)
may contribute to endothelial dys-function, hypertension, and
proteinuria in preeclampsia. J. Clin. Invest.111, 649658.
23. Wang, A., Rana, S., Karumanchi, S. A. (2009) Preeclampsia:
the role of
angiogenic factors in its pathogenesis. Physiology24, 147158.24.
Gu, Y., Lewis, D. F., Wang, Y. (2008) Placental productions and
expres-sions of soluble endoglin, soluble fms-like tyrosine kinase
receptor-1,and placental growth factor in normal and preeclamptic
pregnancies.
J. Clin. Endocrinol. Metab.93, 260266.25. Fujita, D., Tanabe,
A., Sekijima, T., Soen, H., Narahara, K., Yamashita,
Y., Terai, Y., Kamegai, H., Ohmichi, M. (2010) Role of
extracellularsignal-regulated kinase and AKT cascades in regulating
hypoxia-in-duced angiogenic factors produced by a
trophoblast-derived cell line. J.
Endocrinol.206, 131140.26. Jung, J-J., Tiwari, A., Inamdar, S.
M., Thomas, C. P., Goel, A., Choud-
hury, A. (2012) Secretion of soluble vascular endothelial growth
factorreceptor 1 (sVEGFR1/sFlt1) requires Arf1, Arf6, and Rab11
GTPases.PLoS ONE7, e44572.
27. Munaut, C., Lorquet, S., Pequeux, C., Blacher, S., Berndt,
S., Fran-kenne, F., Foidart, J-M. (2008) Hypoxia is responsible for
soluble vascu-lar endothelial growth factor receptor-1 (VEGFR-1)
but not for solubleendoglin induction in villous trophoblast. Hum.
Reprod. 23, 14071415.
28. Thomas, C. P., Andrews, J. I., Raikwar, N. S., Kelley, E.
A., Herse, F.,
Dechend, R., Golos, T. G., Liu, K. Z. (2009) A recently evolved
noveltrophoblast-enriched secreted form of fms-Like tyrosine
kinase-1 vari-ant is up-regulated in hypoxia and preeclampsia. J.
Clin. Endocrinol.Metab.94, 2524 2530.
29. Levine, R. J., Maynard, S. E., Qian, C., Lim, K-H., England,
L. J., Yu,K. F., Schisterman, E. F., Thadhani, R., Sachs, B. P.,
Epstein, F. H.,Sibai, B. M., Sukhatme, V. P., Karumanchi, S. A.
(2004) Circulatingangiogenic factors and the risk of preeclampsia.
N. Engl. J. Med. 350,672683.
30. Herse, F., Verlohren, S., Wenzel, K., Pape, J., Muller, D.
N., Modrow,S., Wallukat, G., Luft, F. C., Redman, C. W. G.,
Dechend, R. (2009)Prevalence of agonistic autoantibodies against
the angiotensin II type 1receptor and soluble fms-like tyrosine
kinase 1 in a gestational age-matched case study. Hypertension53,
393398.
31. Murphy, S. R., Lamarca, B. B., Parrish, M., Cockrell, K.,
Granger, J. P.(2013) Control of soluble fms-like tyrosine-1
(sFlt-1) production re-sponse to placental ischemia/hypoxia: role
of tumor necrosis factor-.Am. J. Physiol. 304, R130 R135.
32. Zhou, C. C., Ahmad, S., Mi, T., Abbasi, S., Xia, L., Day,
M-C., Ramin,
S. M., Ahmed, A., Kellems, R. E., Xia, Y. (2008) Autoantibody
fromwomen with preeclampsia induces soluble Fms-Like tyrosine
kinase-1production via angiotensin type 1 receptor and
calcineurin/nuclearfactor of activated T-cells signaling.
Hypertension51, 1010 1019.
33. Irani, R. A., Zhang, Y., Zhou, C. C., Blackwell, S. C.,
Hicks, M. J.,Ramin, S. M., Kellems, R. E., Xia, Y. (2010)
Autoantibody-mediatedangiotensin receptor activation contributes to
preeclampsia throughtumor necrosis factor-signaling.
Hypertension55, 1246 1253.
34. Gilad, S., Meiri, E., Yogev, Y., Benjamin, S., Lebanony, D.,
Yerushalmi,N., Benjamin, H., Kushnir, M., Cholakh, H., Melamed, N.,
Bentwich,Z., Hod, M., Goren, Y., Chajut, A. (2008) Serum microRNAs
are prom-ising novel biomarkers. PLoS ONE3, e3148.
35. Hu, Y., Li, P., Hao, S., Liu, L., Zhao, J., Hou, Y. (2009)
Differential ex-pression of microRNAs in the placentae of Chinese
patients with severepre-eclampsia.Clin. Chem. Lab. Med. 47,
923929.
36. Pineles, B. L., Romero, R., Montenegro, D., Tarca, A. L.,
Han, Y. M.,Kim, Y. M., Draghici, S., Espinoza, J., Kusanovic, J.
P., Mittal, P., Has-san, S. S., Kim, C. J. (2007) Distinct subsets
of microRNAs are ex-pressed differentially in the human placentas
of patients with pre-eclampsia.Am. J. Obstet. Gynecol. 196, 261
e261e266.
37. ONeill, L. A. J. (2010) Outfoxing Foxo1 with miR-182.Nat.
Immunol.11, 983984.
38. Tang, T., Wong, H. K., Gu, W., Yu, M. Y., To, K. F., Wang,
C. C.,Wong, Y. F., Cheun g, T. H., Chung, T. K., Choy, K. W.
(2013)MicroRNA-182 plays an onco-miRNA role in cervical cancer.
Gynecol.Oncol.129, 199208.
39. Zhang, Y., Fei, M., Xue, G., Zhou, Q., Jia, Y., Li, L., Xin,
H., Sun, S.(2012) Elevated levels of hypoxia-inducible microRNA-210
in pre-ec-lampsia: new insights into molecular mechanisms for the
disease. J.Cell. Mol. Med.16, 249259.
40. Zhang, Y., Diao, Z., Su, L., Sun, H., Li, R., Cui, H., Hu,
Y. (2010)MicroRNA-155 contributes to preeclampsia by
down-regulating CYR61.Am. J. Obstet. Gynecol. 202,
466.e1466.e7.
41. Messerli, M., May, K., Hansson, S. R., Schneider, H.,
Holzgreve, W.,Hahn, S., Rusterholz, C. (2010) Feto-maternal
interactions in pregnan-cies: placental microparticles activate
peripheral blood monocytes. Pla-centa31, 106112.
8 Journal of Leukocyte Biology Volume 94, July 2013
www.jleukbio.org
-
8/10/2019 Inmunologia de Preeclampsia
9/11
42. Germain, S. J., Sacks, G. P., Soorana, S. R., Sargent, I.
L., Redman,C. W. (2007) Systemic inflammatory priming in normal
pregnancy andpreeclampsia: the role of circulating
syncytiotrophoblast microparticles.
J. Immunol.178, 5949 5956.43. Southcombe, J., Tannetta, D.,
Redman, C., Sargent, I. (2011) The im-
munomodulatory role of syncytiotrophoblast microvesicles. PLoS
ONE6, e20245.
44. Guller, S., Tang, Z., Ma, Y. Y., Di Santo, S., Sager, R.,
Schneider, H.(2011) Protein composition of microparticles shed from
human pla-
centa during placental perfusion: potential role in angiogenesis
andfibrinolysis in preeclampsia. Placenta32, 6369.45. Lee, S. M.,
Romero, R., Lee, Y. J., Park, I. S., Park, C-W., Yoon, B. H.
(2012) Systemic inflammatory stimulation by microparticles
derivedfrom hypoxic trophoblast as a model for inflammatory
response in pre-eclampsia.Am. J. Obstet. Gynecol. 207,
337.e1337.e8.
46. Holder, B. S., Tower, C. L., Jones, C. J. P., Aplin, J. D.,
Abrahams,V. M. (2012) Heightened pr o-inflammatory effect of
preeclamptic pla-cental microvesicles on peripheral blood immune
cells in humans. Biol.Reprod.86, 103, 101107.
47. Von Dadelszen, P., Hurst, G., Redman, C. W. G. (1999)
Supernatantsfrom co-cultured endothelial cells and
syncytiotrophoblast microvillousmembranes activate peripheral blood
leukocytes in vitro. Hum. Reprod.14, 919924.
48. Matzinger, P. (2002) The danger model: a renewed sense of
self.Sci-ence296, 301305.
49. Bonney, E. A. (2007) Preeclampsia: a view through the danger
model.J. Reprod. Immunol. 76, 6874.
50. Lotze, M. T., Deisseroth, A., Rubartelli, A. (2007) Damage
associated
molecular pattern molecules. Clin. Immunol.124, 14.51. Yang, H.,
Wang, H., Czura, C. J., Tracey, K. J. (2005) The cytokine ac-tivity
of HMGB1. J. Leukoc. Biol.78, 18.
52. Schmidt, A. P., Tort, A. B. L., Amaral, O. B., Schmidt, A.
P., Walz, R.,Vettorazzi-Stuckzynski, J., Martins-Costa, S. H.,
Ramos, J. G. L., Souza,D. O., Portela, L. V. C. (2004) Serum S100B
in pregnancy-related hy-pertensive disorders: a case-control study.
Clin. Chem.50, 435438.
53. Holmlund, U., Whmaa, H., Bachmayer, N., Bremme, K.,
Sverremark-Ekstrm, E., Palmblad, K. (2007) The novel inflammatory
cytokinehigh mobility group box protein 1 (HMGB1) is expressed by
humanterm placenta. Immunology122, 430437.
54. Tskitishvili, E., Komoto, Y., Temma-Asano, K., Hayashi, S.,
Kinugasa, Y.,Tsubouchi, H., Song, M., Kanagawa, T., Shimoya, K.,
Murata, Y. (2006)S100B protein expression in the amnion and
amniotic fluid in preg-nancies complicated by pre-eclampsia. Mol.
Hum. Reprod. 12, 755761.
55. Tskitishvili, E., Sharentuya, N., Temma-Asano, K., Mimura,
K., Kinu-gasa-Taniguchi, Y., Kanagawa, T., Fukuda, H., Kimura, T.,
Tomimatsu,T., Shimoya, K. (2010) Oxidative stress-induced S100B
protein fromplacenta and amnion affects soluble endoglin release
from endothelial
cells.Mol. Hum. Reprod. 16, 188199.56. Kim, Y. M., Romero, R.,
Oh, S. Y., Kim, C. J., Kilburn, B. A., Armant,
D. R., Nien, J. K., Gomez, R., Mazor, M., Saito, S., Abrahams,
V. M.,Mor, G. (2005) Toll-like receptor 4: a potential link between
dangersignals, the innate immune system, and preeclampsia? Am. J.
Obstet.Gynecol.193, 921927.
57. Pineda, A., Verdin-Teran, S. L., Camacho, A.,
Moreno-Fierros, L.(2011) Expression of Toll-like receptor TLR-2,
TLR-3, TLR-4 andTLR-9 is increased in placentas from patients with
preeclampsia. Arch.Med. Res. 42, 382391.
58. Chatterjee, P., Chiasson, V. L., Kopriva, S. E., Young, K.
J., Chatterjee,V., Jones, K. A., Mitchell, B. M. (2011) Interleukin
10 deficiency exac-erbates Toll-like receptor 3-induced
preeclampsia-like symptoms inmice.Hypertension58, 489496.
59. Hennessy, A., Pilmore, H. L., Simmons, L. A., Painter, D. M.
(1999) Adeficiency of placental IL-10 in preeclampsia. J. Immunol.
163, 34913495.
60. Chatterjee, P., Weaver, L. E., Doersch, K. M., Kopriva, S.
E., Chiasson,V. L., Allen, S. J., Narayanan, A. M., Young, K. J.,
Jones, K. A., Kuehl,T. J., Mitchell, B. M. (2012) Placental
Toll-like receptor 3 and Toll-likereceptor 7/8 activation
contributes to preeclampsia in humans andmice.PLoS ONE7,
e41884e41884.
61. Scharfe-Nugent, A., Corr, S. C., Carpenter, S. B., Keogh,
L., Doyle, B.,Martin, C., Fitzgerald, K. A., Daly, S., OLeary, J.
J., ONeill, L. A. J.(2012) TLR9 provokes inflammation in response
to fetal DNA: mecha-nism for fetal loss in preterm birth and
preeclampsia. J. Immunol. 188,57065712.
62. Leung, T. N., Zhang, J., Lau, T. K., Chan, L. Y. S., Lo, Y.
M. D. (2001)Increased maternal plasma fetal DNA concentrations in
women whoeventually develop preeclampsia. Clin. Chem.47,
137139.
63. Conde-Agudelo, A., Villar, J., Lindheimer, M. (2008)
Maternal infec-tion and risk of preeclampsia: systematic review and
metaanalysis. Am.
J. Obstet. Gynecol. 198, 722.64. Kawai, T., Akira, S. (2009) The
roles of TLRs, RLRs and NLRs in
pathogen recognition. Int. Immunol. 21, 317337.65. Vsrhelyi, B.,
Cseh, A., Kocsis, I., Treszl, A., Gyrffy, B., Rig Jr., J.
(2006) Three mechanisms in the pathogenesis of pre-eclampsia
sug-
gested by over-represented transcription factor-binding sites
detectedwith comparative promoter analysis.Mol. Hum. Reprod. 12,
3134.
66. Li, Q., Verma, I. M. (2002) NF-B regulation in the immune
system.Nat. Rev. Immunol. 2, 725734.
67. Luppi, P., Tse, H., Lain, K. Y., Markovic, N., Piganelli, J.
D., DeLoia,J. A. (2006) Preeclampsia activates circulating immune
cells with en-gagement of the NF-B pathway. Am. J. Reprod. Immunol.
56, 135144.
68. Vaughan, J. E., Walsh, S. W. (2012) Activation of NF-B in
placentas ofwomen with preeclampsia.Hypertens. Pregnancy31,
243251.
69. Kawai, T., Akira, S. (2007) Signaling to NF-B by Toll-like
receptors.Trends Mol. Med. 13, 460469.70. Sykes, L., MacIntyre, D.
A., Yap, X. J., Ponnampalam, S., Teoh, T. G.,
Bennett, P. R. (2012) Changes in the Th1: Th2 cytokine bias in
preg-nancy and the effects of the anti-inflammatory cyclopentenone
prosta-glandin 15-deoxy-(12,14)-prostaglandin J2. Mediators
Inflamm. 2012,416739.
71. Gomez-Lopez, N., Guilbert, L. J., Olson, D. M. (2010)
Invasion of theleukocytes into the fetal-maternal interface during
pregnancy. J. Leukoc.Biol.88, 625633.
72. Abrahams, V. M., Visintin, I., Aldo, P. B., Guller, S.,
Romero, R., Mor,G. (2005) A role for TLRs in the regulation of
immune cell migrationby first trimester trophoblast cells. J.
Immunol. 175, 8096 8104.
73. Bowen, R. S., Gu, Y., Zhang, Y., Lewis, D. F., Wang, Y.
(2005) Hypoxiapromotes interleukin-6 and -8 but reduces
interleukin-10 production byplacental trophoblast cells from
preeclamptic pregnancies. J. Soc. Gyne-col. Investig. 12,
428432.
74. Benyo, D. F., Smarason, A., Redman, C. W. G., Sims, C.,
Conrad, K. P.(2001) Expression of inflammatory cytokines in
placentas from women
with preeclampsia. J. Clin. Endocrinol. Metab. 86, 25052512.75.
Luppi, P., DeLoia, J. A. (2006) Monocytes of preeclamptic women
spontaneously synthesize pro-inflammatory cytokines. Clin.
Immunol.118, 268275.
76. Ziegler-Heitbrock, L., Ancuta, P., Crowe, S., Dalod, M.,
Grau, V., Hart,D. N., Leenen, P. J. M., Liu, Y-J., MacPherson, G.,
Randolph, G. J.,Scherberich, J., Schmitz, J., Shortman, K.,
Sozzani, S., Strobl, H., Zem-bala, M., Austyn, J. M., Lutz, M. B.
(2010) Nomenclature of monocytesand dendritic cells in blood.
Blood116, e74e80.
77. Melgert, B. N., Spaans, F., Borghuis, T., Klok, P. A.,
Groen, B., Bolt, A.,de Vos, P., van Pampus, M. G., Wong, T. Y., van
Goor, H., Bakker,W. W., Faas, M. M. (2012) Pregnancy and
preeclampsia affect mono-cyte subsets in humans and rats. PLoS
ONE7, e45229.
78. Al-Ofi, E., Coffelt, S. B., Anumba, D. O. (2012) Monocyte
subpopula-tions from pre-eclamptic patients are abnormally skewed
and exhibitexaggerated responses to Toll-like receptor ligands.
PLoS ONE7,e42217.
79. Zawada, A. M., Rogacev, K. S., Rotter, B., Winter, P.,
Marell, R-R.,
Fliser, D., Heine, G. H. (2011) SuperSAGE evidence forCD14CD16
monocytes as a third monocyte subset.Blood118,e50e61.
80. Ancuta, P., Weiss, L., Haeffner-Cavaillon, N. (2000)
CD14CD16cells derived in vitro from peripheral blood monocytes
exhibit pheno-typic and functional dendritic cell-like
characteristics. Eur. J. Immunol.30, 18721883.
81. Khalil, R. A., Granger, J. P. (2002) Vascular mechanisms of
increasedarterial pressure in preeclampsia: lessons from animal
models. Am. J.Physiol.283, R29R45.
82. Vila, E., Salaices, M. (2005) Cytokines and vascular
reactivity in resis-tance arteries. Am. J. Physiol. Heart Circ.
Physiol. 288, H1016H1021.
83. Greer, I., Haddad, N., Dawes, J., Johnstone, F., Calder, A.
(1989) Neu-trophil activation in pregnancy-induced hypertension.
Br. J. Obstet.Gynaecol.96, 978982.
84. Greer, I., Dawes, J., Johnston, T., Calder, A. (1991)
Neutrophil activa-tion is confined to the maternal circulation in
pregnancy-induced hy-pertension. Obstet. Gynecol. 78, 2832.
85. Butterworth, B., Greer, I., Liston, W., Haddad, N.,
Johnston, T. (1991)
Immunocytochemical localization of neutrophil elastase in term
pla-centa decidua and myometrium in pregnancy-induced
hypertension.Br. J. Obstet. Gynaecol. 98, 929933.
86. Cadden, K., Walsh, S. (2008) Neutrophils, but not
lymphocytes ormonocytes, infiltrate maternal systemic vasculature
in women with pre-eclampsia.Hypertens. Pregnancy27, 396405.
87. Tsukimori, K., Tsushima, A., Fukushima, K., Nakano, H.,
Wake, N.(2008) Neutrophil-derived reactive oxygen species can
modulate neu-trophil adhesion to endothelial cells in preeclampsia.
Am. J. Hypertens.21, 587591.
88. Quinn, M., Linner, J., Siemsen, D., Dratz, E., Buescher, E.,
Jesaitis, A.(1995) Immunocytochemical detection of lipid
peroxidation in phago-somes of human neutrophils: correlation with
expression of flavocyto-chrome b. J. Leukoc. Biol. 57, 415421.
89. Barden, A., Ritchie, J., Walters, B., Michael, C., Rivera,
J., Mori, T.,Croft, K., Beilin, L. (2001) Study of plasma factors
associated with neu-trophil activation and lipid peroxidation in
preeclampsia. Hypertension38, 803808.
Laresgoiti-Servitje The immune system in the pathophysiology of
preeclampsia
www.jleukbio.org Volume 94, July 2013 Journal of Leukocyte
Biology 9
-
8/10/2019 Inmunologia de Preeclampsia
10/11
90. Leik, C. E., Walsh, S. W. (2004) Neutrophils infiltrate
resistance-sizedvessels of subcutaneous fat in women with
preeclampsia.Hypertension44, 7277.
91. Gupta, A., Hasler, P., Holzgreve, W., Gebhardt, S., Hahn, S.
(2005) In-duction of neutrophil extracellular DNA lattices by
placental micropar-ticles and IL-8 and their presence in
preeclampsia. Hum. Immunol.66,11461154.
92. Fuchs, T. A., Abed, U., Goosmann, C., Hurwitz, R., Schulze,
I., Wahn,V., Weinrauch, Y., Brinkmann, V., Zychlinsky, A. (2007)
Novel celldeath program leads to neutrophil extracellular
traps.
J. Cell Biol.176,
231241.93. Kaplan, M. J., Radic, M. (2012) Neutrophil
extracellular traps: double-
edged swords of innate immunity. J. Immunol. 189, 2689 2695.94.
Gupta, A., Hasler, P., Holzgreve, W., Hahn, S. (2007)
Neutrophil
NETs: a novel contributor to preeclampsia-associated placental
hyp-oxia?Semin. Immunopathol.29, 163167.
95. Saffarzadeh, M., Juenemann, C., Queisser, M. A., Lochnit,
G., Barreto,G., Galuska, S. P., Lohmeyer, J., Preissner, K. T.
(2012) Neutrophil ex-tracellular traps directly induce epithelial
and endothelial cell death: apredominant role of histones. PLoS
ONE7, e32366.
96. Remijsen, Q., Kuijpers, T. W., Wirawan, E., Lippens, S.,
Vandenabeele,P., Vanden Berghe, T. (2011) Dying for a cause:
NETosis, mechanismsbehind an antimicrobial cell death modality.
Cell Death Differ. 18, 581588.
97. Gandley, R. E., Rohland, J., Zhou, Y., Shibata, E., Harger,
G. F., Raja-kumar, A., Kagan, V. E., Markovic, N., Hubel, C. A.
(2008) Increasedmyeloperoxidase in the placenta and circulation of
women with pre-eclampsia.Hypertension52, 387393.
98. Guleria, I., Sayegh, M. H. (2007) Maternal acceptance of the
fetus:true human tolerance. J. Immunol. 178, 33453351.99. Lash, G.
E., Otun, H. A., Innes, B. A., Kirkley, M., De Oliveira, L.,
Searle, R. F., Robson, S. C., Bulmer, J. N. (2006)
Interferon-inhibitsextravillous trophoblast cell invasion by a
mechanism that involvesboth changes in apoptosis and protease
levels. FASEB J. 20, 25122518.
100. Molvarec, A., Ito, M., Shima, T., Yoneda, S., Toldi, G.,
Stenczer, B.,Vasarh elyi, B., Rigo Jr., J., Saito, S. (2010) Decrea
sed propo rtion ofperipheral blood vascular endothelial growth
factor-expressing Tand natural killer cells in preeclampsia. Am. J.
Obstet. Gynecol. 203,567.e1567.e8.
101. Sivori, S., Falco, M., Chiesa, M. D., Carlomagno, S.,
Vitale, M., Moretta,L., Moretta, A. (2004) CpG and double-stranded
RNA trigger humanNK cells by Toll-like receptors: induction of
cytokine release and cyto-toxicity against tumors and dendritic
cells. Proc. Natl. Acad. Sci. USA101, 1011610121.
102. Hedlund, M., Stenqvist, A-C., Nagaeva, O., Kjellberg, L.,
Wulff, M.,Baranov, V., Mincheva-Nilsson, L. (2009) Human placenta
expressesand secretes NKG2D ligands via exosomes that down-modulate
the cog-
nate receptor expression: evidence for immunosuppressive
function. J.Immunol.183, 340351.103. Jurewicz, M., McDermott, D.
H., Sechler, J. M., Tinckam, K., Takakura,
A., Carpenter, C. B., Milford, E., Abdi, R. (2007) Human T and
natu-ral killer cells possess a functional renin-angiotensin
system: furthermechanisms of angiotensin II-induced inflammation.
J. Am. Soc. Neph-rol.18, 10931102.
104. Herse, F., Dechend, R., Harsem, N. K., Wallukat, G., Janke,
J., Qadri,F., Hering, L., Muller, D. N., Luft, F. C., Staff, A. C.
(2007) Dysregula-tion of the circulating and tissue-based
renin-angiotensin system in pre-eclampsia.Hypertension49,
604611.
105. Blois, S. M., Kammerer, U., Alba Soto, C., Tometten, M. C.,
Shaikly, V.,Barrientos, G., Jurd, R., Rukavina, D., Thomson, A. W.,
Klapp, B. F.,Fernndez, N., Arck, P. C. (2007) Dendritic cells: key
to fetal toler-ance?Biol. Reprod.77, 590598.
106. Steinman, R. M., Hemmi, H. (2006) Dendritic cells:
translating innateto adaptive immunity. Curr. Top. Microbiol.
Immunol.311, 1758.
107. Blois, S., Tometten, M., Kandil, J., Hagen, E., Klapp, B.
F., Margni,R. A., Arck, P. C. (2005) Intercellular adhesion
molecule-1/LFA-1 cross
talk is a proximate mediator capable of disrupting immune
integrationand tolerance mechanism at the feto-maternal interface
in murinepregnancies. J. Immunol. 174, 1820 1829.
108. Hsu, P., Santner-Nanan, B., Dahlstrom, J. E., Fadia, M.,
Chandra, A.,Peek, M., Nanan, R. (2012) Altered decidual DC-SIGN
antigen-pre-senting cells and impaired regulatory T-cell induction
in preeclampsia.Am. J. Pathol. 181, 2149 2160.
109. Kludka-Sternik, M., Serafin, A., Darmochwal-Kolarz, D.,
Radej, S., Ro-linski, J., Leszczynska-Gorzelak, B., Oleszczuk, J.
(2010) The expressionof B7-H1 and B7-H4 molecules on immature
myeloid and lymphoiddendritic cells in cord blood of healthy
neonates. Folia Histochem. Cyto-biol.48, 658662.
110. Darmochwal-Kolarz, D., Rolinski, J., Tabarkiewicz, J.,
Leszczynska-Gorzelak, B., Buczkowski, J., Wojas, K., Oleszczuk, J.
(2003) Myeloidand lymphoid dendritic cells in normal pregnancy and
pre-eclampsia.Clin. Exp. Immunol.132, 339344.
111. Leslie, D. S., Vincent, M. S., Spada, F. M., Das, H.,
Sugita, M., Morita,C. T., Brenner, M. B. (2002) CD1-mediated / T
cell maturation ofdendritic cells. J. Exp. Med. 196, 15751584.
112. Banchereau, J., Briere, F., Caux, C., Davoust, J.,
Lebecque, S., Liu, Y. J.,Pulendran, B., Palucka, K. (2000)
Immunobiology of dendritic cells.Annu. Rev. Immunol. 18,
767811.
113. Schroder, W. A., Le, T. T., Major, L., Street, S., Gardner,
J., Lambley,E., Markey, K., MacDonald, K. P., Fish, R. J., Thomas,
R., Suhrbier, A.(2010) A physiological function of
inflammation-associated SerpinB2 isregulation of adaptive immunity.
J. Immunol. 184, 26632670.
114. Ohkuchi, A., Minakami, H., Aoya, T., Haga, T., Kimura, H.,
Suzuki, M.,Sato, I. (2001) Expansion of the fraction of Th1 cells
in women with
preeclampsia: inverse correlation between the percentage of Th1
cellsand the plasma level of PAI-2. Am. J. Reprod. Immunol.46,
252259.115. Jarrossay, D., Napolitani, G., Colonna, M., Sallusto,
F., Lanzavecchia, A.
(2001) Specialization and complementarity in microbial molecule
rec-ognition by human myeloid and plasmacytoid dendritic cells.
Eur. J.Immunol.31, 3388 3393.
116. Panda, B., Panda, A., Ueda, I., Abrahams, V. M., Norwitz,
E. R., Stanic,A. K., Young, B. C., Ecker, J. L., Altfeld, M., Shaw,
A. C., Rueda, B. R.(2012) Dendritic cells in the circulation of
women with preeclampsiademonstrate a pro-inflammatory bias
secondary to dysregulation ofTLR receptors. J. Reprod. Immunol. 94,
210215.
117. Berghfer, B., Haley, G., Frommer, T., Bein, G., Hackstein,
H. (2007)Natural and synthetic TLR7 ligands inhibit CpG-A- and
CpG-C-oligode-oxynucleotide-induced IFN- production. J.
Immunol.178, 40724079.
118. Rutella, S., Danese, S., Leone, G. (2006) Tolerogenic
dendritic cells:cytokine modulation comes of age. Blood108,
14351440.
119. Muthuswamy, R., Urban, J., Lee, J. J., Reinhart, T. A.,
Bartlett, D., Ka-linski, P. (2008) Ability of mature dendritic
cells to interact with regu-latory T cells is imprinted during
maturation. Cancer Res. 68, 5972
5978.120. Verlohren, S., Muller, D. N., Luft, F. C., Dechend, R.
(2009) Immunol-ogy in hypertension, preeclampsia, and target-organ
damage. Hyperten-sion54, 439443.
121. Banerjee, S., Smallwood, A., Moorhead, J., Chambers, A. E.,
Papa-georghiou, A., Campbell, S., Nicolaides, K. (2005) Placental
expressionof interferon-(IFN-) and its receptor IFN-R2 fail to
switch fromearly hypoxic to late normotensive development in
preeclampsia. J.Clin. Endocrinol. Metab.90, 944952.
122. Arriaga-Pizano, L., Jimenez-Zamudio, L., Vadillo-Ortega,
F., Martinez-Flores, A., Herrerias-Canedo, T., Hernandez-Guerrero,
C. (2005) Thepredominant Th1 cytokine profile in maternal plasma of
preeclampticwomen is not reflected in the choriodecidual and fetal
compartments.J. Soc. Gynecol. Invest. 12, 335342.
123. Murphy, S. P., Tayade, C., Ashkar, A. A., Hatta, K., Zhang,
J., Croy,B. A. (2009) Interferon in successful pregnancies. Biol.
Reprod.80,848859.
124. Moreau, P., Adrian-Cabestre, F., Menier, C., Guiard, V.,
Gourand, L.,Dausset, J., Carosella, E. D., Paul, P. (1999) IL-10
selectively induces
HLA-G expression in human trophoblasts and monocytes. Int.
Immunol.11, 803811.125. Steinborn, A., Schmitt, E., Kisielewicz,
A., Rechenberg, S., Seissler, N.,
Mahnke, K., Schaier, M., Zeier, M., Sohn, C. (2012)
Pregnancy-associ-ated diseases are characterized by the composition
of the systemic reg-ulatory T cell (Treg) pool with distinct
subsets of Tregs. Clin. Exp. Im-munol.167, 8498.
126. Paeschke, S., Chen, F., Horn, N., Fotopoulou, C.,
Zambon-Bertoja, A.,Sollwedel, A., Zenclussen, M. L., Casalis, P.
A., Dudenhausen, J. W.,Volk, H-D., Zenclussen, A. C. (2005)
Pre-eclampsia is not associatedwith changes in the levels of
regulatory T cells in peripheral blood.Am. J. Reprod. Immunol. 54,
384389.
127. Steinborn, A., Haensch, G., Mahnke, K., Schmitt, E.,
Toermer, A.,Meuer, S., Sohn, C. (2008) Distinct subsets of
regulatory T cells duringpregnancy: is the imbalance of these
subsets involved in the pathogen-esis of preeclampsia? Clin.
Immunol.129, 401412.
128. Toldi, G., Svec, P., Vasarhelyi, B., Meszaros, G., Rigo,
J., Tulassay, T.,Treszl, A. (2008) Decreased number of FoxP3
regulatory T cells inpreeclampsia.Acta Obstet. Gynecol. Scand. 87,
1229 1233.
129. Darmochwal-Kolarz, D., Kludka-Sternik, M., Tabarkiewicz,
J., Kolarz, B.,Rolinski, J., Leszczynska-Gorzelak, B., Oleszczuk,
J. (2012) The predom-inance of Th17 lymphocytes and decreased
number and function ofTreg cells in preeclampsia. J. Reprod.
Immunol. 93, 7581.
130. Saito, S., Nakashima, A., Ito, M., Shima, T. (2011)
Clinical implicationof recent advances in our understanding of
IL-17 and reproductive im-munology. Exp. Rev. Clin. Immunol.7,
649657.
131. Santner-Nanan, B., Peek, M. J., Khanam, R., Richarts, L.,
Zhu, E., Faze-kas de St Groth, B., Nanan, R. (2009) Systemic
increase in the ratiobetween Foxp3 and IL-17-producing CD4 T cells
in healthy preg-nancy but not in preeclampsia. J. Immunol. 183,
70237030.
132. Jianjun, Z., Yali, H., Zhiqun, W., Mingming, Z., Xia, Z.
(2010) Imbal-ance of T-cell transcription factors contributes to
the Th1 type immu-nity predominant in pre-eclampsia. Am. J. Reprod.
Immunol.63, 3845.
133. Saito, S. (2010) Th17 cells and regulatory T cells: new
light on patho-physiology of preeclampsia. Immunol. Cell Biol. 88,
615617.
134. Toldi, G., Rigo Jr., J., Stenczer, B., Vasarhelyi, B.,
Molvarec, A. (2011)Increased prevalence of IL-17-producing
peripheral blood lymphocytesin pre-eclampsia. Am. J. Reprod.
Immunol.66, 223229.
10 Journal of Leukocyte Biology Volume 94, July 2013
www.jleukbio.org
-
8/10/2019 Inmunologia de Preeclampsia
11/11
135. Jensen, F., Wallukat, G., Herse, F., Budner, O.,
El-Mousleh, T., Costa,S-D., Dechend, R., Zenclussen, A. C. (2012)
CD19CD5 cells as indi-cators of preeclampsia. Hypertension59,
861868.
136. Berland, R., Wortis, H. H. (2002) Origins and functions of
B-1 cellswith notes on the role of CD5. Annu. Rev. Immunol. 2 0,
253300.
137. Sato, S., Ono, N., Steeber, D., Pisetsky, D., Tedder, T.
(1996) CD19regulates B lymphocyte signaling thresholds critical for
the develop-ment of B-1 lineage cells and autoimmunity. J. Immunol.
157, 43714378.
138. Vinuesa, C. G., Sanz, I., Cook, M. C. (2009) Dysregulation
ofgerminal centres in autoimmune disease. Nat. Rev. Immunol.
9,845857.
139. Ebeling, S. B., Schutte, M. E., Logtenberg, T. (1993) The
majority ofhuman tonsillar CD5 B cells express somatically mutated
V 4genes. Eur. J. Immunol. 23, 14051408.
140. Casali, P., Burastero, S., Nakamura, M., Inghirami, G.,
Notkins, A.(1987) Human lymphocytes making rheumatoid factor and
antibody tossDNA belong to Leu-1 B-cell subset. Science236,
7781.
141. Wallukat, G., Homuth, V., Fischer, T., Lindschau, C.,
Horstkamp, B.,Jpner, A., Baur, E., Nissen, E., Vetter, K., Neichel,
D., Dudenhausen,J. W., Haller, H., Luft, F. C. (1999) Patients with
preeclampsia developagonistic autoantibodies against the
angiotensin AT1 receptor. J. Clin.Invest.103, 945952.
142. Siddiqui, A. H., Irani, R. A., Blackwell, S. C., Ramin, S.
M., Kellems,R. E., Xia, Y. (2010) Angiotensin receptor agonistic
autoantibody ishighly prevalent in preeclampsia: correlation with
disease severity. Hy-
pertension55, 386393.143. Dechend, R., Homuth, V., Wallukat, G.,
Muller, D. N., Krause, M.,
Dudenhausen, J., Haller, H., Luft, F. C. (2006) Agonistic
antibodiesdirected at the angiotensin II, AT1 receptor in
preeclampsia. J. Soc.Gynecol. Investig.13, 7986.
144. Zhou, C. C., Irani, R. A., Dai, Y., Blackwell, S. C.,
Hicks, M. J., Ramin,S. M., Kellems, R. E., Xia, Y. (2011)
Autoantibody-mediated IL-6-depen-dent endothelin-1 elevation
underlies pathogenesis in a mouse modelof preeclampsia. J. Immunol.
186, 6024 6034.
145. Yang, X., Wang, F., Chang, H., Zhang, S., Yang, L., Wang,
X.,Cheng, X., Zhang, M., Ma, X. L., Liu, H. (2008)
Autoantibodyagainst AT1 receptor from preeclamptic patients induces
vasocon-striction through angiotensin receptor activation. J.
Hypertens. 26 ,16291635.
146. LaMarca, B., Wallace, K., Herse, F., Wallukat, G., Martin,
J. N.,Weimer, A., Dechend, R. (2011) Hypertension in response to
placentalischemia during pregnancy. Hypertension57, 865871.
147. Irani, R. A., Zhang, Y., Blackwell, S. C., Zhou, C. C.,
Ramin, S. M., Kel-lems, R. E., Xia, Y. (2009) The detrimental role
of angiotensin recep-tor agonistic autoantibodies in intrauterine
growth restriction seen inpreeclampsia. J. Exp. Med. 206, 2809
2822.
148. Hubel, C. A., Wallukat, G., Wolf, M., Herse, F., Rajakumar,
A., Rob-erts, J. M., Markovic, N., Thadhani, R., Luft, F. C.,
Dechend, R.(2007) Agonistic angiotensin II type 1 receptor
autoantibodies inpostpartum women with a history of preeclampsia.
Hypertension4 9,612617.
149. Ma, G., Li, Y., Zhang, J., Liu, H., Hou, D., Zhu, L.,
Zhang, Z., Zhang,L. (2013) Association between the presence of
autoantibodies againstadrenoreceptors and severe pre-eclampsia: a
pilot study. PLoS ONE8,e57983.
KEY WORDS:
preeclampsia STBM neutrophil dendritic cell lymphocyte mono-cyte
TLR B cell
Laresgoiti-Servitje The immune system in the pathophysiology of
preeclampsia
www.jleukbio.org Volume 94, July 2013 Journal of Leukocyte
Biology 11