Embed Size (px)
Citation preview

Institute for Studies on Diabetes Foundation, Inc.
Diabetic Neuropathy

Diabetic Neuropathy
63
UERMMMC-Institute for Studies on Diabetes Foundation, Inc.
Lot 4 Blk. 52 Apitong St., Marikina Heights, Marikina CityTelephone No: 941-9856, Telefax 713-3307
Email: [email protected]
Executive Officers
Chairman & PresidentVice President
Corporate SecretaryTreasurer
Executive Director
Ricardo E. Fernando, MD, FPCP, FPSEMLeorino M. Sobrepeña, MD, FPCP, MSRodolfo C. Rabanal, MD, FPCP, MSRima T. Tan, MD, FPCP, MSAraceli A. Panelo, MD, FPCP, MS
Ricardo E. Fernando, MD, FPCP, FPSEMLeorino M. Sobrepeña, MD, FPCP, MSRodolfo C. Rabanal, MD, FPCP, MSRima T. Tan, MD, FPCP, MSAtty. Crispino ReyesMr. Jose Cavada (Servier)Edwin Liwanag, MD, FPCP, MSMr. Peter Sy GaisanoEvelyn Fernando, MDMs. Marlowe Ngo (Therapharma)Ms. Violy Remo (Pfizer)Mr. Panfilo O. DomingoRomeo Divinagracia, MD, FPCP, FPCCCarmelita Divinagracia, RN, PhDEditha A. Dalisay, MD, FPCP, MS
Ricardo E. Fernando, M.D., FPSEMAraceli A. Panelo, M.D., MSEditha Arceo-Dalisay, M.D., MSElizabeth Ann F. Catindig, M.D., MSAgnes T. Cruz, M.D., MSGrace K. delos Santos, M.D., MSRichard Elwyn V. Fernando, M.D., MSMarcelo A. Lim, M.D., MSEdwin E. Liwanag, M.D., MSRodolfo C. Rabanal, M.D., MSLeorino M. Sobrepeña, M.D., MSRima T. Tan, M.D., MSErnesto L. Ang, M.D., MSNines P. Bautista, M.D.Luinio S. Tongson, M.D., FPSGSEleanor J. Galvez, M.D.Mary Queen Florencio, M.D.Tomas P. Lazatin, M.D.Maria Luisa H. Licaros. M.D.Olive de Guzman Quizon, M.D.
Faculty Members
The Board of Trustees

Diabetic Neuropathy
64
HISTORICAL BACKGROUND
In the early 70s, Dr. Ricardo E. Fernando, fired up by the zeal of a church minister that he did not become, embarked on another ministry; to spread the gospel of diabetes. He believed then as he still does today, that educating the medical practitioner would improve the lot of the ultimate benefactor, the Filipino diabetics whose lives will not only be prolonged but be made as compli-cation-free as possible.
He started giving out one-time lectures/seminars on a regular basis. Changes in the course content and teach-ing strategies were meticulously adopted, making each course an improvement of the previous ones. All sessions were always well-attended.
1980 saw the birth of the very popular Diabetes Mellitus Postgraduate Course (also known as Fernando lectures). Unlike the previous ones, participants were limited to senior residents or graduates of Internal Medicine. Each course lasted for three months with the students meeting every Saturday. A Certificate of Proficiency was granted the attendee at the end of the course depending on his performance.
Graduate of these courses formed the Diabetes Forum, a quarterly update on selected topics in Diabetes.
The overwhelming response to these programs inspired Dr. Fernando to dream more and more. In 1987, he thought of putting up an institute for diabetes. While there were several offers for the venue, he chose to link-up with UERMMMC, the school where he taught diabetes for twenty years. The then UE President Isidro Cariño gave the project full support. It was not difficult to get the cooperation of Dean Joven Cuanang, who worked for the immediate approval of the project with the Department of Education, Culture & Sports (DECS) sometime August 1988. Hence, the birth of the UE Institute for Studies on Diabetes, the first for the Philippines and the only one of its kind in Asia in 1989.
THRUST OF THE INSTITUTE
• A two-year masteral program in diabetes approved by the DECS and duly recognized by CHED conferring a Master of Science Degree on qualified internists.
• A two-year course entitled Diploma in Diabetes for non internals.
• Scholarships and hospital fellowships to deserving doctors and diabetes teaching nurses.
• Courses in diabetes for nurses and nutritionists in coop-eration with Association of Diabetes Nurse Educators of the Phils. (ADNEP) and Nutritionists and Dieticians Association of the Phils. (NDAP).
• Courses in diabetes for general practitioners, para-medical organizations and laymen in cooperation with other institutions.
• Resource speakers in diabetes for other medical center, societies, organizations, commercial firms, and the lay
• Technical support to the DOH in the formulation of programs for Diabetes Prevention and Control
Our Mission
Enable healthcare professionals to deliver excellent and
humane diabetes care.
Our Vision
Everyone receives excellent and humane diabetes care.
Our Values
A. Family
We are one in our aspiration to make a dent on diabetes. Our members and healthcare partners are family whom we value and respect. We care deeply for their well-being and growth. We deal in candor and openness. Our patients and their loved ones are family as well. They are our work's meaning.
B. Service
Service to Life is our ministry and driving force• for furthering the knowledge and skills that help make
life much better.• for diabetes sufferers and protect high-risk individuals
from the disease.We are committed to render service anytime, anywhere, and in any condition, so that no one shall be deprived of excellent and humane diabetes care.
C. Integrity
Ministering to life is an honorable mission for which our probity, zeal, and fairness, besides our expertise, keep us trustworthy. We practice Medicine in faithful ad-herence to the Hippocratic Oath, the physician's highest and noblest standard of ethics for centuries. D. Excellence
Life being our work's meaning, we strive to give our best at our best. We search continuously, trying to quench our insatiable thirst for knowledge. Our excellent and generous mentors, whom we owe much gratitude, challenge us ceaselessly with "What else?" and inspire us to renew constantly.
E. Love of Work
We love seeing happiness in the eyes of the diabetes patients we treat. We find fulfilment in enabling people to help us seek solutions to diabetes. We love working together in an atmosphere of trust, loyal friendship and fun. In all humility we celebrate with quiet and dedicated work our privileged role of enhancing, extending and saving God's greatest gift: Human life.
A Call to Arms
There has been an increasing global prevalence of diabetes in the past two decades, especially in develop-ing countries like the Philippines. Much of the efforts to date are focused on management of overt diabetes and prevention of its complications. Hardly is prevention of diabetes properly emphasized when this has more far-reaching implications than treatment.
Past studies have shown that the type 2 diabetes can be prevented - the Malmo study, the Da Qing study, the

Diabetic Neuropathy
65
Finnish study, the Diabetes Prevention Program, the TRIPOD, the STOP-NIDDM study. All have shown the positive effects of drugs and lifestyle changes with the latter proving definitely superior. Maybe a mixture of the two will prove more beneficial?
We live in a perverse society which eats all it can, drinks all it can, has become more sedentary and obese smokes and drinks wantonly, is subject to more and varying stresses in life. These studies are telling us that reversing our current lifestyle trends can save us from the burden of diabetes. Unfortunately lifestyle changes are perhaps the most difficult for all. For how do you change the lifestyle of people who have gradually moved into this compromised condition over the past hundred years?
The studies were aimed at high-risk subjects. That is Primary Prevention. The call of the hour is for primordial prevention on the entirety of our society. And if a reason-able Choice is to be made; it should be children 0-10 years old. In making decisions, one cannot demand for evidence base. The proof of the value of today's efforts will be seen in the next two generations when hopefully the prevalence of diabetes (and all other diseases of lifestyle) will subside to an acceptable low.
The one way doctors in the Philippines can help save the country is by beginning with themselves, their children and their families. Save your family, your clan, and your community. Children are most amenable to change. They are the potential diabetics of tomorrow. But children can not save themselves unless the parents - the elders - become role models. Each patient seen in a doctor's clinic is representative of a family. If you have 30 diabetic patients, that means 30 families - 200 people. Treat the patient but consider diabetes a family affair. Parents, brothers, sisters, children and grandchildren should not escape the warning that when there is diabetes in the fam-ily, everyone should be seriously involved in persistent preventive measures. Relatives have been seen falling prey to the disease one after the other with no one lifting a finger, as if any effort will prove futile. It is time for the community to wake up to the massive dangers diabetes threatens to throw into our future.
Communities should avail of parent-teachers' asso-ciations. Include the yayas. Involve social, civic, religious groups. The campaign that is more likely to succeed is the one that will take on the urgency and dedication of a truly missionary project. For it is the future not only of your families but the country as a whole that is at stake!
Ricardo E. Fernando, MD, FPCP, FPSEMInstitute for Studies on Diabetes Foundation, Inc.UERMMMC

Diabetic Neuropathy
66
those which cannot efficiently reduce this glucose transport.
Thus diabetes damages cells whose glucose transport does not decline rapidly as a result of hyperglycemia. This is important because it tells us that explanation for what causes complications must involve mechanisms going on inside these cells rather than outside.
Major Pathways of Hyperglycemic Damage
1. Polyol Pathway 2. AGE Precursors 3. PKC Pathway4. Hexosamine Pathway
The first such mechanism that was discovered was the polyol pathway and increased polyol pathway flux, described in peripheral nerve in the 1966 Sci-ence paper. Then 10 years later, in the late 1970s a second mechanism emerged: increased formation of advanced glycation end products. In the late 1980’s and early 1990’s a third mechanism was discovered, that is hyperglycemia induced activation of protein kinase C isoforms. And in the late 1990’s a fourth mechanism was discovered: increased hexosamine pathway flux and consequent overmodification of proteins by N acetyl glucosamine.
Diabetic Neuropathy: A Major Health Problem
Ø Occurs in >1/3 of diabeticsØ Highly affects quality of life due to its complicationsØ Its severity poses high morbidity and 5-fold mortality
in the presence of cardiac autonomic neuropathy and other vasculopathies
Three Categories of Diabetic Complications:
• Metabolic Complications Ketoacidosis Hyperosmolar nonketotic syndrome Hypoglycemia
• Macrovascular Complications Cardiovascular disease Cerebrovascular disease Peripheral vascular disease
• Microvascular Complications Diabetic neuropathy Diabetic retinopathy Diabetic nephropathy
Figure 1. General features of hyperglycemia-induced tissue damage
Cells vulnerable to tissue damaging effects of hyperglycemia
• Capillary endothelial cells in the RETINA• Mesangial cells in the RENAL GLOMERULUS• NEURONS AND SCHWANN CELLS in peripheral
nerves
Why Damage Occur in Selective Cells
• Hyperglycemia downregulates glucose transport inside most cells so internal glucose concentration remains constant.
• In contrast, cells damaged by hyperglycemia are
Repeated acute changes in cellular metabolism
Cumulative long-term changes in stable macromolecules
Independent accelerating factors (eg. hypertension,
hyperlipidemia)
Hyper-glycemia
Diabetic tissue
damage
∨ ∨
∨ ∨
∨∨
∨
∨
Genetic determinants ofindividual susceptibility

Diabetic Neuropathy
67
Diabetic Peripheral Neuropathy Can Progress Over Time
• Symptoms may occur any time and intermittently
• The majority of signs of DPN are not evident at the onset of the disease
• Foot ulcers and amputations are more common among patients with diabetes for more than 10 years
American Diabetes Association. Diabetes Care. 2003;26(suppl 1):S33-S50.Abbott CA, et al. Diabetes Care. 1998;21:1071-1075.Armstrong DG, et al. Ostomy Wound Manage. 1998;44:70-76.Armstrong DG, et al. Arch Intern Med. 1998;158:289-292.Carrington AL, et al. Diabetes Care. 2002;25:2010-2015.Feldman EL, et al. Diabetes Care. 1994;17:1281-1289.Shearer A, et al. Diabetes Care. 2003;26:2305-2310.Veves A, et al. Diabet Med. 1991;8:917-921.
Diabetic Peripheral Neuropathy is Underdiagnosed
• 75% of DPN patients experience none of these positive symptoms at any given point in time
• All DPN patients display one or more of these signs
• Periodic evaluation is essential for all patients since many are not aware of DPN
This is an illustration of cell, with the cytoplasm and the nucleus. Inside the nucleus we can see the DNA repair enzyme called PARP which is found exclusively in the nucleus. Normally PARP resides in the nucleus in an inactive form, waiting for DNA damage to activate it. When increased intercellular glucose generates increased ROS these free radicals induce DNA strand breaks thereby activating PARP. Once activated PARP splits the NAD+ molecule into its 2 component parts: nicotinic acid and ADP ribose. PARP then proceeds to make polymers of ADP-ribose which accumulate on GADPH and other nuclear protein. What is GADPH doing in the nucleus? Although commonly thought to reside exclusively in the cytosol, in fact it normally shuttles in and out of the nucleus where it plays a critical role in DNA repair.
BANTING LECTURE 2004 (Unifying mechanism of hyperglycemia – oxidative stress)
Hyperglycemia increases flux thru polyol pathway NADPH/Glutathione
Increased production of AGE→AGE receptor→ROSHyperglycemia activates PKC via increase in DAG (Enos, ET-1, VEGF, TGF-b, PAI-1, NFkB, NADPH)
Hyperglycemia increases flux thru hexosamine path→UDPGlcNAc
Hyperglycemia induces superoxide production thru the mitochondrial transport chain
Mitochondrial SO activates four major pathways by inhibiting GAPDH
activates PARP modifies GAPDH (decrease) → increase polyol, AGEs, PKC/NFkB, hexosamine
The Pathobiology of Diabetic Complications, Michael Brownlee 2004 Diabetes 54:1615-25

Diabetic Neuropathy
68
Abbott CA, et al. Diabetes Care. 1998;21:1071-1075.Apfel SC, et al. J Neurol Sci. 2001;189:3-5.Armstrong DG, et al. Ostomy Wound Manage. 1998;44:70-76.Armstrong DG, et al. Arch Intern Med. 1998;158:289-292.Carrington AL, et al. Diabetes Care. 2002;25:2010-2015.Feldman EL, et al. Diabetes Care. 1994;17:1281-1289.Shearer A, et al. Diabetes Care. 2003;26:2305-2310.Veves A, et al. Diabet Med. 1991;8:917-921.Vinik AI. Am J Med. 1999;107:17S-26S.
TREATMENT FOR DIABETIC NEUROPATHy
Glucose control does provide benefits for patients with DMC, but currently there are no other treatments with indications for all three DMC.
The treatment categories that have been labelled include antihyperlipidemics, antihypertensives, and antihypergly-cemics. Reduction in urinary albumin and progression of kidney disease can be provided by the antihypertensive agents ACE inhibitors and ARBs for patients with Type 1 or Type 2 diabetes, respectively.
Several agents that are under investigation have not yet been categorized but do have the potential to provide beneficial effects on the progression of DMC.
Among the investigational agents that are still non-catego-rized is a new class - protein kinase C (PKC) ß-inhibitors - that may address the microvascular damage associated with DMC.
Abbreviations:
ACEI–angiotensin-converting enzyme inhibitor AGE – advanced glycation endproducts ARB–angiotensin receptor blockerGLP-1–glucagon-like peptide-1 PARP–poly(ADP ribose) polymerase PKC ß–protein kinase C ß SOD–superoxide dismutase TZD–thiazolidinediones
Screening and Diagnosis for Diabetic Peripheral Neuropathy
History/Physical exam • Eliminate causes other than DPN
Neurological exam • Vibration detection threshold (VDT) - Tuning fork • Proprioception - Position sensitivity by flexion/extension of great and small toe • Deep tendon reflexes - Reflex hammer • Pressure sensation - Monofilament • Pain sensation - Pin prick • Light touch sensation - Cotton-wool swab
Diagnosis • Can be supported by: - Electrophysiology - Quantitative sensory testing
Among patients with diabetes, 37.9% have one or more symptoms of sensory DPN, although the percentage of patients with symptoms becomes greater as the duration of the disease increases.1 Several large studies have revealed that over a 25-year period, 50% of patients with DPN develop symptoms.2,3
A number of routine screening and diagnostic tests are available to enable physicians to assess the presence and severity of DPN.4 ADA advises patients to “Inspect your feet every day, and seek care early if you do get a foot injury. Make sure your healthcare provider checks your feet at least once a year–more often if you have foot problems.”5
References:1. Harris M, et al. Diabetes Care. 1993;16:1446-1452.2. Dyck PJ, et al. Neurology. 1993;43:817-824.3. Pirart J. Diabetes Care. 1978;1:168-188.
Tuning Fork Monofilament screening test

Diabetic Neuropathy
69
4. European Association for the Study of Diabetes. Available at: http://www.neurodiab.org/index05.htm.Accessed November 12, 2003.
5. American Diabetes Association. Available at:http://www.diabetes.org/health/body_care/foot/foot_care.jsp.Accessed November 10, 2003.
Additional references: 1. Simmons Z, Feldman EL. Curr Opin Neurol. 2002;15:595-603.2. Perkins BA, et al. Diabetes Care. 2001;24:250-256.3. Apelqvist J, et al. Diabetes Metab Res Rev. 2000;16(suppl 1):S84-S92.4. Rith-Najarian SJ, et al. Diabetes Care. 1992;15:1386-1389.5. Lee S, et al. J Korean Med Sci. 2003;18:103-107. 6. Rosenberg NR, et al. J Neurol Neurosurg Psychiatry. 2001;71:205-
209.7. Suzuki C, et al. Neurology. 2000;54:1932-1937.
Early Involvement of Spinal Cord in Diabetic Peripheral Neuropathy Significant reduction in spinal cord cross-sectional area at the stage of clinically detectable diabetic neuropathy using MRI imaging of the cervical spine and cord area measurements at disc level C2/C3 SCAI mean corrected spinal cord area index corrected for age, height and weight SCAI was significantly related to sural sensory conduc-tion velocities and the Neuropathic Composite and Symptom Score Selvarajah et. al. 2006 CARE 29;2664-2669
Treatment of Diabetic NeuropathyPreventive• Intensive blood glucose control• Lowers risk of microvascular complications and neu-
ropathy (DM1, DM2)• Proven in DCCT* Research Group and UKPDS• Insufficient data / population. Needs more controlled
studies on neuropathy*Diabetes control and complications trial D. Ziegler et al, Exp Clin Endocrinol Diabetes 1999
• Aldose Reductase Inhibitors Reduce polyol pathway hyperactivity• g-linolenic acid Prevent impairment of essential fatty acid & prostanoid
metabolism• Vasodilators (ACE inhibitors, prostacyclin ana-
logues) Improve nerve blood flow and prevent hypoxia• Nerve growth factor (NGF) Prevent deficits in neurotrophism & axonal transport • Aminoguanidine ↓ Accumulation of advanced glycosylation end prod-
ucts (AGEs) • Antioxidants Free radical scavenger
Ø Majority of trials were inconclusive. Some have seri-ous side effects.
Ø For antioxidants - Benefits proven in clinical trials (Alpha lipoic acid)
D. Ziegler et al, Exp Clin Endocrinol Diabetes 1999
Symptomatic• Neuropathic pain affects quality of life• Antidepressants, anticonvulsants, mexiletine, tramadol,
topical capsaicin• Partial effects
• Neurotoxic side effects in chronic use• No influence on underlying neuropathy
D. Ziegler et al, Exp Clin Endocrinol Diabetes 1999
CurativeA variety of experimental studies give new insights into the putative mechanisms in the pathogenesis of diabetic neuropathy
Cameron & Cotter 1997Tomlinson et al 1997
Diabetic neuropathy(numbness, cold sensation)
Vascular Theory
Combined Theory
↓Occlusion of
Neurotropic vessel↓
Neuropathy
Antiplatelet agentVasodilator(Cilostazol)
Therapeutic drug
↓Polyol
dysbolism↓
Neuropathy
Aldose Reductase Inhibitor
Therapeutic drug
↓↓
↓ ↓
Combined use
Metabolism Theory

Diabetic Neuropathy
70
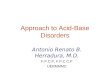
5 Standard Tests of Cardiovascular Autonomic Function (Ewing & Clarke)
Test Normal Borderline Abnormal Parasympathetic function HR response to > 1.21 1.11-1.20 < 1.10 Valsalva maneuver (Valsalva ratio) HR variation > 15 bpm 11-14 bpm < 10 bpm (R-R interval) Deep breathing > 1.04 1.01-1.03 < 1.00 (max-min) immediate HR response to standing (30:15 ratio) Sympathetic function BP response to < 10 mmHg 11-29 mmHg > 30 mmHg standing (SBP fall) BP response to > 16 mmHg 11-15 mmHg < 10 mmHg sustained handgrip (DBP increase)
*At least 2 are diagnostic Kempler, The British J of Diab & Vascular Disease, Mar 2003
Summary: Possible factors for high mortality & sudden death in CAN• Silent ischemia / MI• Cardiorespiratory arrest• High perioperative risk• Resting tachycardia• Ventricular arrhythmia• Prolonged QT • Orthostatic hypotension• Hypertension• “Non-dipper” phenomenon• Exaggerated BP response• Abnormal LV S/D function• Poor exercise tolerance• Impaired CV responsiveness• Heat intolerance • ↑risk for foot ulcers/amputation• Hypoglycemia unawareness• ↑risk of severe hypoglycemia• Obstructive sleep apnea
Kempler, The British J of Diab & Vascular Disease, Mar 2003
Treatment of Cardiac Autonomic Neuropathy
Intensive glycemic controlDCCT* and UKPDS• Primary & secondary prevention of neuropathy
EURODIAB IDDM Complications Study• Showed close relationship between CAN & long-term
glycemic control (HbA1c = 7%)• Prevents onset & slows progression of CAN (DM1,
DM2)
*Diabetes control and complications trial
Kempler, The British J of Diab & Vascular Disease, Mar 2003
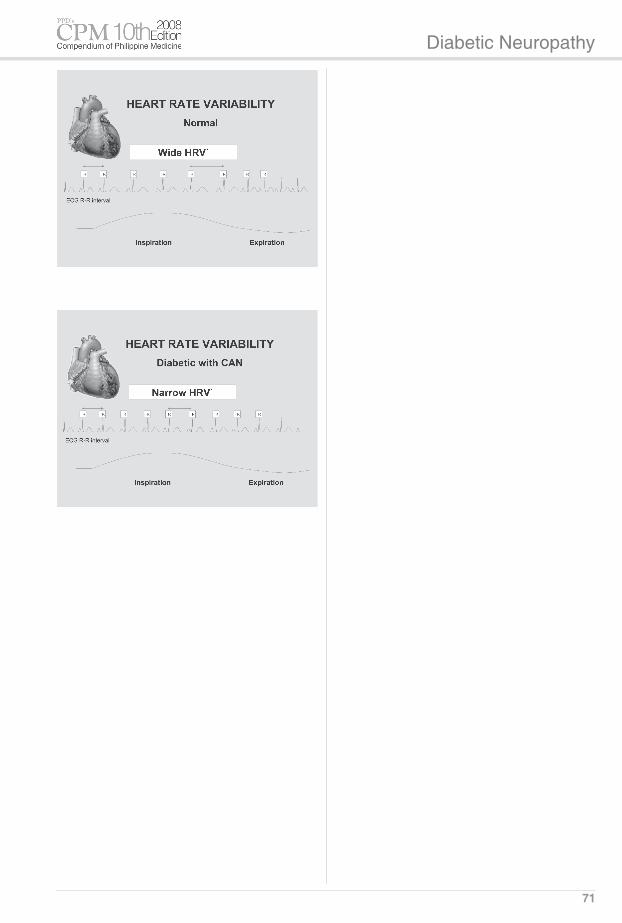
Cardiac Autonomic Neuropathy: A Serious Complication of Diabetes
Cardiovascular Autonomic Neuropathy (CAN) Among Filipinos with Type 2 Diabetes Mellitus
Conclusion:• Prevalence of CAN is 81.48%• Based on ASP questionnaires (symptoms), 63.89%
have CAN
Corvera et al. Phil J Int Med Nov-Dec 2005
Cardiac Autonomic Neuropathy (CAN)• Carries 5-fold risk of mortality in diabetes• Silent MI, fatal arrhythmias, cardiovascular & respira-
tory instability, sudden death• Cardiorespiratory arrest from anesthesia• Hypertension• “Non-dipper” phenomenon• Blunted or absent day-night BP variability
Kempler, The British J of Diab & Vascular Disease, Mar 2003
Diabetic Neuropathy
71

Diabetic Neuropathy
73
Recommended Therapeutics(Drugs Mentioned in the Treatment Guideline)The following index lists therapeutic classifications as recommended by the treatment guideline. For the prescriber's reference, available drugs are listed under each therapeutic class.
CNS DRUGS
AnticonvulsantsCarbamazepine
Epikor Tegretol ZynapsGabapentin
Calmpent Neurontin Reinin
AntidepressantsDuloxetine
Cymbalta
ANALGESICS
OpiatesTramadol
Dolcet Dolotral Milador/Inj/Retard Siverol TDL Tramal
ANTIDIABETIC DRUGS
InsulinsShort-acting Insulins Actrapid HM
Humalog Humulin R (Regular) Scilin RIntermediate-acting Insulins Humalog Mix 25 Humulin 70/30 Humulin N (NPH) Insulatard HM Mixtard 30 HM NovoMix 30 FlexPen Scilin M30 Scilin NLong-acting Insulins Lantus
Oral Hypoglycemics
Alpha Glucosidase InhibitorsAcarbose Glucobay 50/Glucobay 100 GluconaseVoglibose Basen
Biguanides Metformin HCl Avandamet* Denkaform Diafat Diazen Euglo Plus* Fornidd Glucophage 1 Gram Glucophage/Glucophage Forte Glucovance* Glumet Glumet-XR
Horsulin Humamet I-Max Neoform 500 Norsulin* Pharex Metformin RiteMED Metformin HCl Vimetrol
Dipeptidyl Peptidase 4 (DPP4) Inhibitor
Sitagliptin phosphate Januvia
MeglitinidesNateglinide StarlixRepaglinide Novonorm
SulfonylureasFirst GenerationChlorpropamide Diabinese
Second GenerationGlibenclamide Adsulin Amecladin Daonil Drugmaker's Biotech Glibenclamide Euglo Plus* Euglucon/Semi-Euglucon Eundin Glucovance* Glymod Melix Orabetic Sucron Gliclazide Clibite Clizid Diamicron/Diamicron MR Dianorm Drugmaker's Biotech Gliclazide Glubitor/Glubitor-OD Gluconil RiteMED Gliclazide Glimepiride Arya Euglim Glimed Imerid
Norizec Solosa Sulfast 1/2/3/4Glipizide Drugmaker's Biotech Glipizide Minidiab/Minidiab OD Norsulin*
ThiazolidinedionesPioglitazone Actos Glucozone Piozone ZypiRosiglitazone Avandia Avandamet*
CARDIOVASCULAR DRUGS
ACE InhibitorsBenazepril CibacenCaptopril Capoten Captace Drugmaker’s Biotech Captopril Hartylox Primace Septuagen Tensoril VasostadEnalapril Co-Renitec Hypace Naprilate Pharex Enalapril RenitecFosinopril BPNormLisinopril Lipril Zestoretic ZestrilMoexipril HCl Uniretic UnivascQuinapril HCl Accupril AccuzideRamipril Ramipro Triapin TritaceTrandolapril Tarka
Angiotensin II AntagonistsCandesartan Blopress Blopress Plus*Eprosartan Teveten Teveten Plus*Irbesartan Aprovel CoAprovel*Losartan Bepsar Combizar* Cozaar Hyzaar/Hyzaar DS* Lifezar LosargardOlmesartan OlmetecTelmisartan Micardis Micardis Plus* Pritor Pritorplus*Valsartan Co-Diovan* Diovan

Diabetic Neuropathy
74
Calcium Channel BlockersAmlodipine Amlodine Amvasc Envacar Norvasc VasalatDiltiazem Cordazem Dilatam Diltime Dilzem/Dilzem SA/Dilzem SR Drugmaker’s Biotech
Diltiazem Ritemed Diltiazem Tildiem Vasmulax ZandilFelodipine Dilahex Dilofen ER Felim Felop ER Tab Logimax Plendil ER Triapin Versant XRNicardipine CardepineNifedipine Adalat Calcheck Calcibloc Calcibloc OD Calcigard-5 Denkifed Drugmaker’s Biotech Nifedipine Heblopin Nifestad NormadilVerapamil HCl Isoptin/Isoptin SR Tarka
DiureticsHydrochlorothiazide Accuzide* Betazide* Blopress Plus* Co-Diovan* Co-Renitec* CoAprovel* Combizar* Diuzid* Diuzide Hytaz Hyzaar/Hyzaar Ds Micardis Plus Norplus Pritorplus Teveten Plus Uniretic Vascace Plus Vascoride Zestoretic Ziac
LipidRegulating Drugs
Fibric acid DerivativesBezafibrate
Bezastad
Ciprofibrate Modalim
Fenofibrate Fibrafen 200M Lipanthyl 67M/ Lipanthyl NT 145/ Lipanthyl Supra
Lipilfen Lipway SR Nubrex Trolip
Gemfibrozil Drugmaker's Biotech Gemfibrozil Lopid/Lopid OD Reducel
Nicotinic Acid and DerivativesNicotinic acid
Niaspan
Selective CholesterolAbsorption Inhibitors
Ezetimibe Ezetrol
Vytorin
StatinsAtorvastatin Envacar LipitorFluvastatin Lescol/Lescol XLPravastatin LipostatRosuvastatin
CrestorSimvastatin Afordel Drugmaker’s Biotech Simvastatin Eurocor Ivast Koleste Lipivas Normastin Orovas Pharex Simvastatin Ritemed Simvastatin Simtin Simvahex Uni-Per Vamstat Vastilan Vidastat Vytorin Wilsim Zocor/Zocor HP