Embed Size (px)
Citation preview
Intestinal parasites:
clinical significance and diagnosis
Tom van Gool, MD, PhD
Department of Clinical Parasitology
Academic Medical Center, Amsterdam, Netherlands
Persistent gastrointestinal illness after travel to
(sub) tropics: frequently observed.
intestinal parasites !
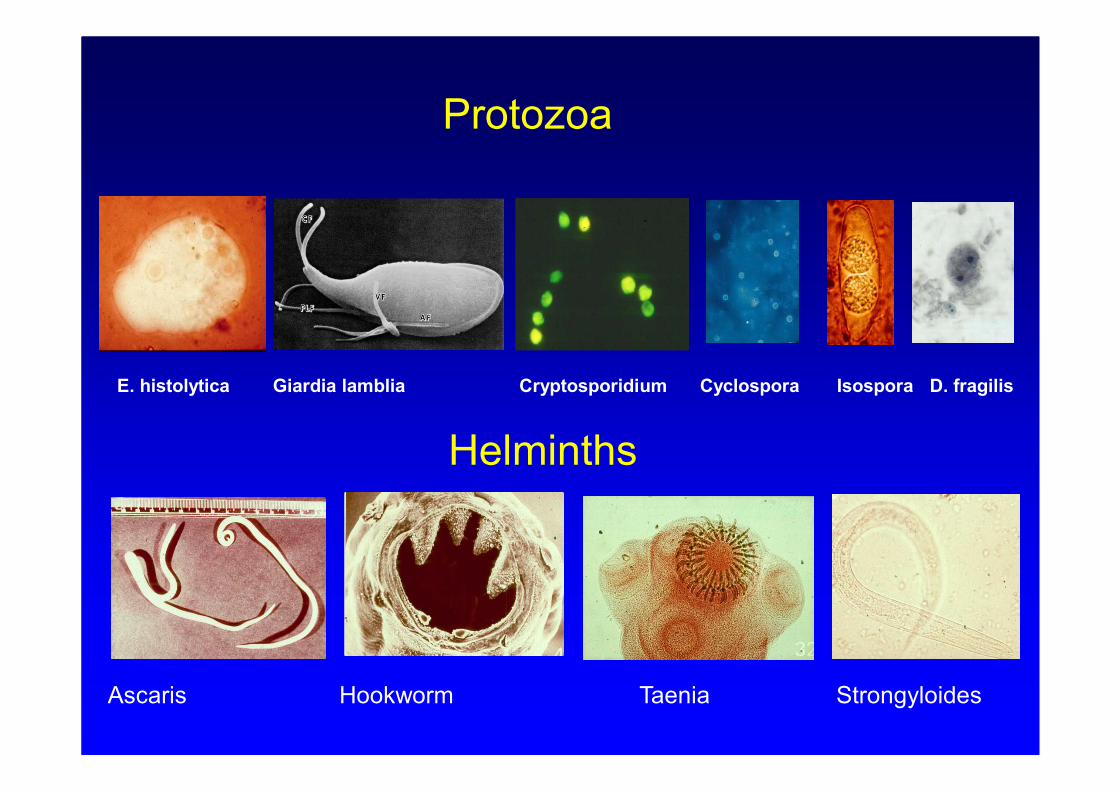
Protozoa
Helminths
E. histolytica Giardia lamblia Cryptosporidium Cyclospora Isospora D. fragilis
Ascaris Hookworm Taenia Strongyloides
Symptomatology due to intestinal parasites
most often non specific:
good laboratory diagnosis important !
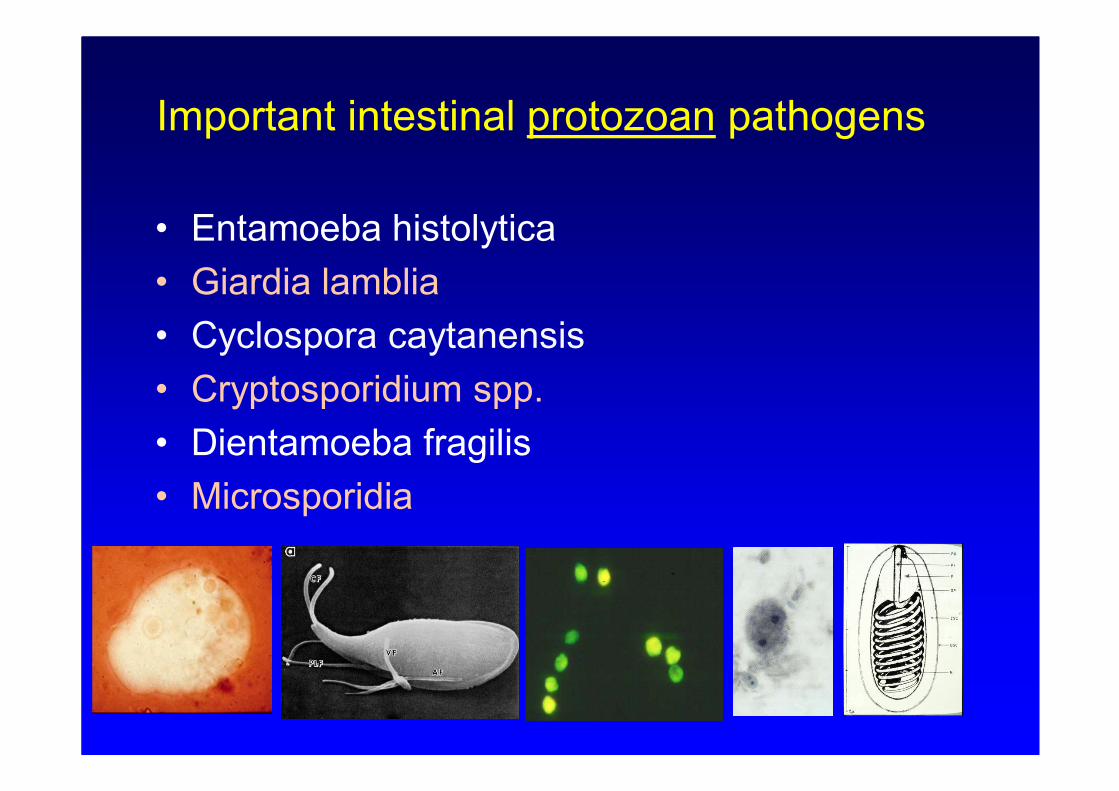
Important intestinal protozoan pathogens
• Entamoeba histolytica
• Giardia lamblia
• Cyclospora caytanensis
• Cryptosporidium spp.
• Dientamoeba fragilis
• Microsporidia

Important human helminths….
● Schistosoma haematobium
● Schistosoma mansoni
● Schistosoma intercalatum
● Schistosoma japonicum
● Fasciola hepatica
● Clonorchis sinensis
● Opisthorchis spp.
● Ascaris lumbricoides
● Capillaria philippinensis
● Enterobius vermicularis ● Hookworms
● Strongyloides srecoralis
● Trichuris trichiura
● Diphyllobothrium latum
● Hymenolepis diminuta
● Hymenolepis nana
● Taenia spp.
Diagnostic stages of all intestinal parasites are
relative large and have a distinctive morphology.
Easy to recognize under a light microscope
for a well trained laboratory technician!
The “old way” of diagnosis
for intestinal parasites:
microscopy
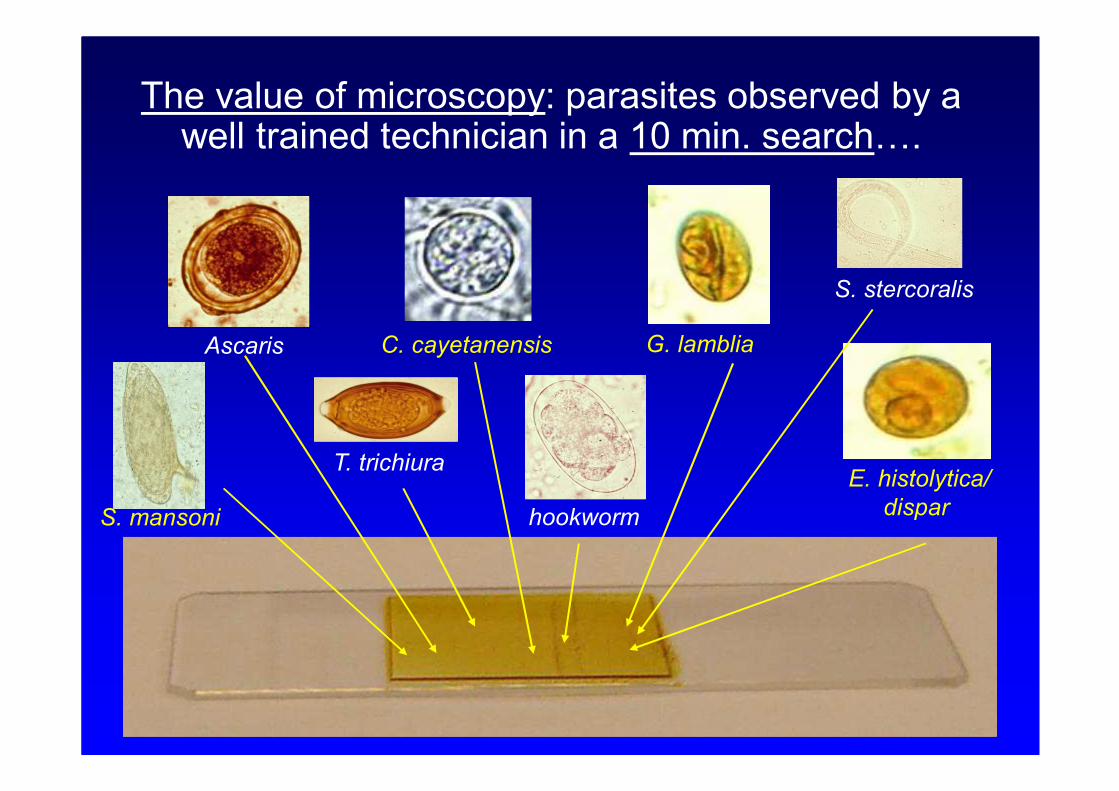
S. mansoni
Ascaris
T. trichiura
C. cayetanensis
E. histolytica/
disparhookworm
G. lamblia
S. stercoralis
The value of microscopy: parasites observed by a well trained technician in a 10 min. search….
Three day collection kit, two
tubes filled with SAF- fixative
For high sensitivity of microscopy, especially
for protozoa, multiple stool samples should be
examined.
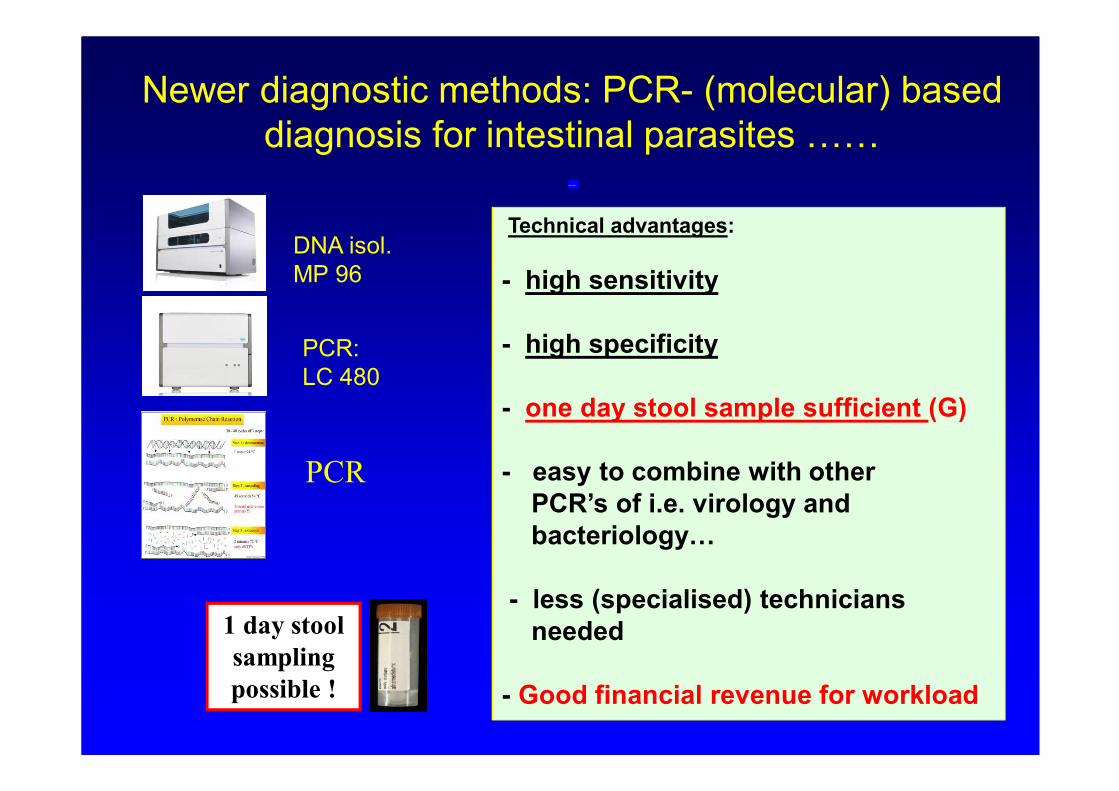
Newer diagnostic methods: PCR- (molecular) based
diagnosis for intestinal parasites ……
I
Technical advantages:
- high sensitivity
- high specificity
- one day stool sample sufficient (G)
- easy to combine with other
PCR’s of i.e. virology and
bacteriology…
- less (specialised) technicians
needed
- Good financial revenue for workload
DNA isol.
MP 96
PCR:
LC 480
PCR
1 day stool
sampling
possible !
Use of PCR - diagnosis in Dutch laboratories:
in routine clinical practice only a few intestinal
protozoans (3- 4) are examined
• Giardia lamblia
• Cryptosporidium spp.
• Entamoeba histolytica
(Dientamoeba fragilis)
No other protozoa and helminths !
Cost test in NL ~ 80 euro
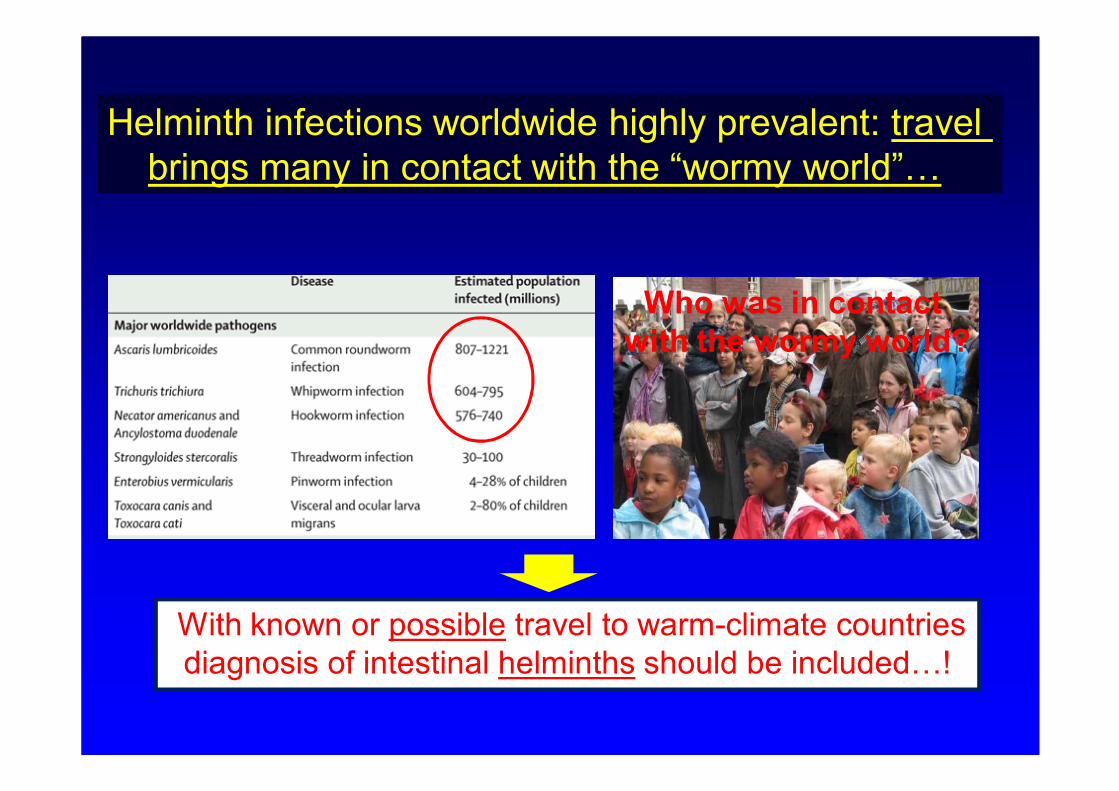
Who was in contact
with the wormy world?
Helminth infections worldwide highly prevalent: travel
brings many in contact with the “wormy world”…
With known or possible travel to warm-climate countries
diagnosis of intestinal helminths should be included…!
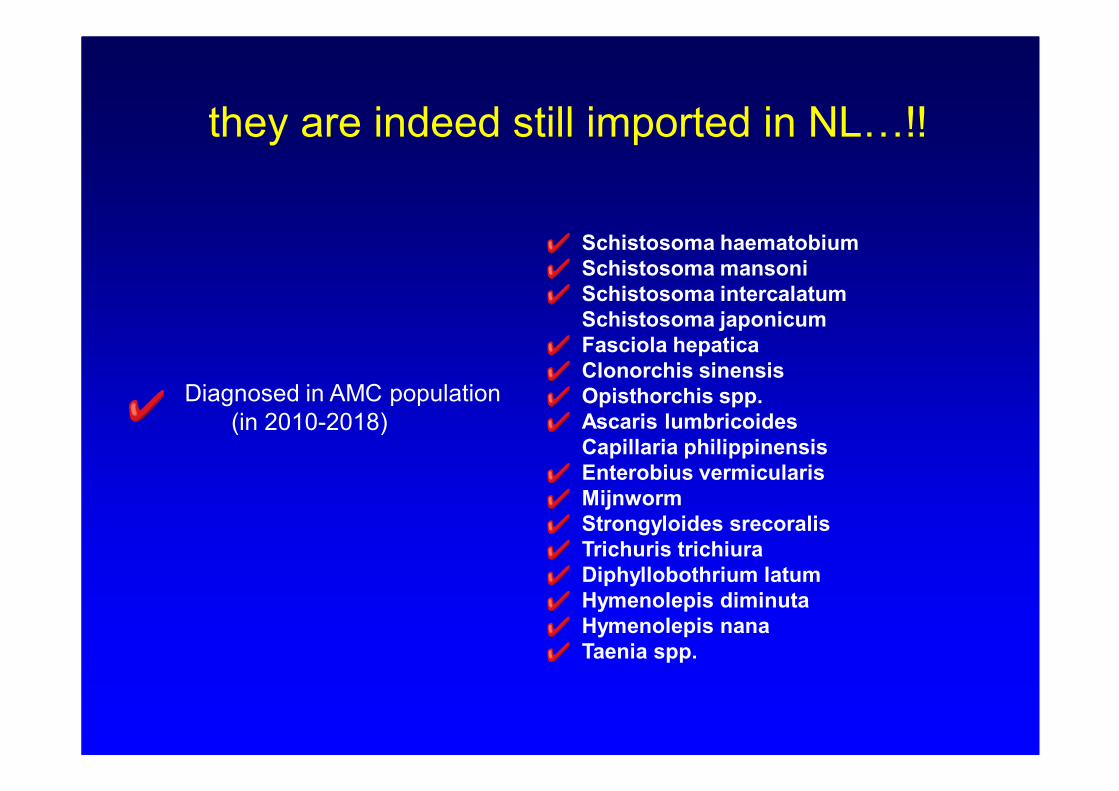
they are indeed still imported in NL…!!
Schistosoma haematobium
Schistosoma mansoni
Schistosoma intercalatum
Schistosoma japonicum
Fasciola hepatica
Clonorchis sinensis
Opisthorchis spp.
Ascaris lumbricoides
Capillaria philippinensis
Enterobius vermicularis
Mijnworm
Strongyloides srecoralis
Trichuris trichiura
Diphyllobothrium latum
Hymenolepis diminuta
Hymenolepis nana
Taenia spp.
Diagnosed in AMC population
(in 2010-2018)
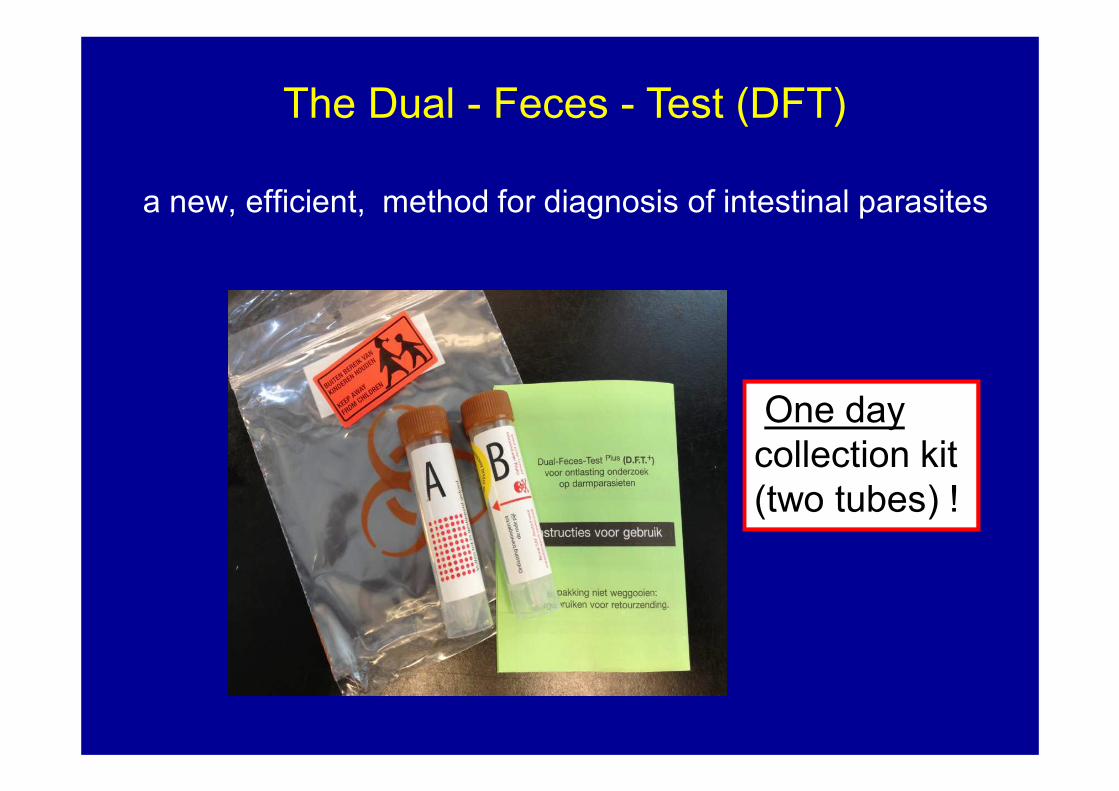
a new, efficient, method for diagnosis of intestinal parasites
The Dual - Feces - Test (DFT)
One day
collection kit
(two tubes) !
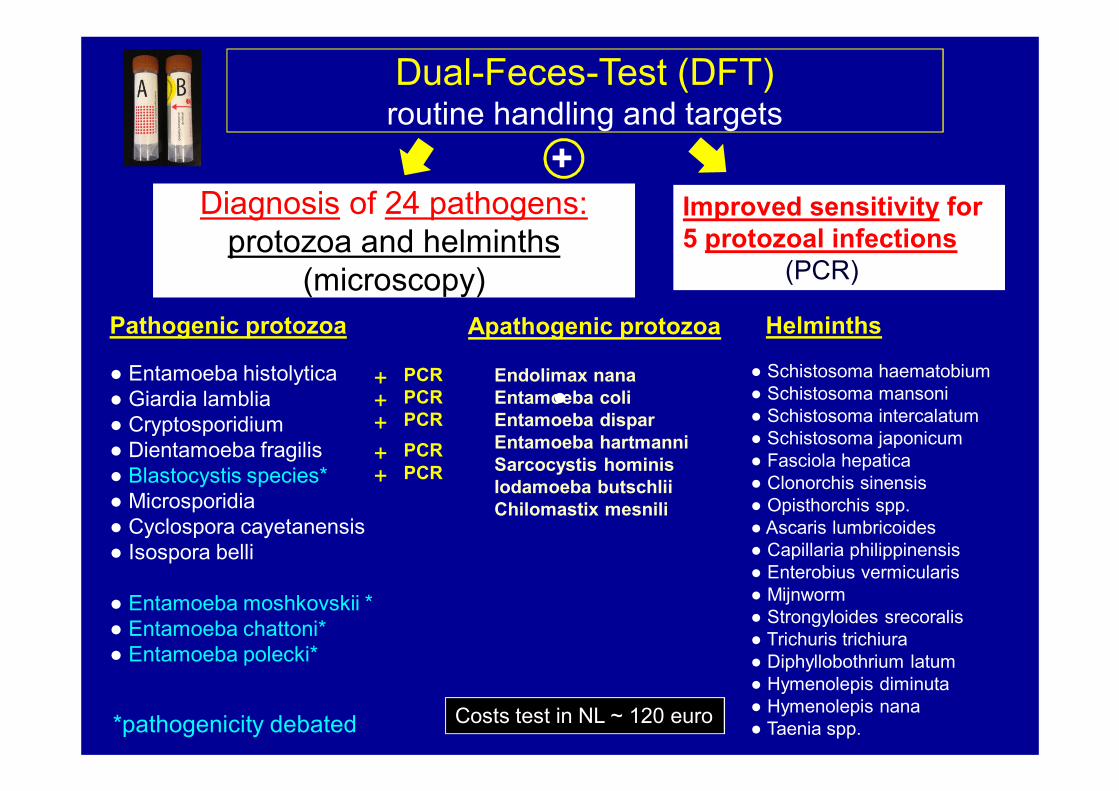
● Entamoeba histolytica
● Giardia lamblia
● Cryptosporidium
● Dientamoeba fragilis
● Blastocystis species*
● Microsporidia
● Cyclospora cayetanensis
● Isospora belli
● Entamoeba moshkovskii *
● Entamoeba chattoni*
● Entamoeba polecki*
Pathogenic protozoa Apathogenic protozoa
Endolimax nana
Entamoeba coli
Entamoeba dispar
Entamoeba hartmanni
Sarcocystis hominis
Iodamoeba butschlii
Chilomastix mesnili
Helminths
● Schistosoma haematobium
● Schistosoma mansoni
● Schistosoma intercalatum
● Schistosoma japonicum
● Fasciola hepatica
● Clonorchis sinensis
● Opisthorchis spp.
● Ascaris lumbricoides
● Capillaria philippinensis
● Enterobius vermicularis
● Mijnworm
● Strongyloides srecoralis
● Trichuris trichiura
● Diphyllobothrium latum
● Hymenolepis diminuta
● Hymenolepis nana
● Taenia spp.
Dual-Feces-Test (DFT)routine handling and targets
Diagnosis of 24 pathogens:
protozoa and helminths
(microscopy)
Improved sensitivity for
5 protozoal infections
(PCR)
PCR
PCR
PCR
++
++
Costs test in NL ~ 120 euro
+PCR
PCR
+
●
*pathogenicity debated
1,0
rare2,0
few
3,0
some
4,0
many
0,0
negative
microscopic load
20
25
30
35
40
45C
p P
CR
valu
e
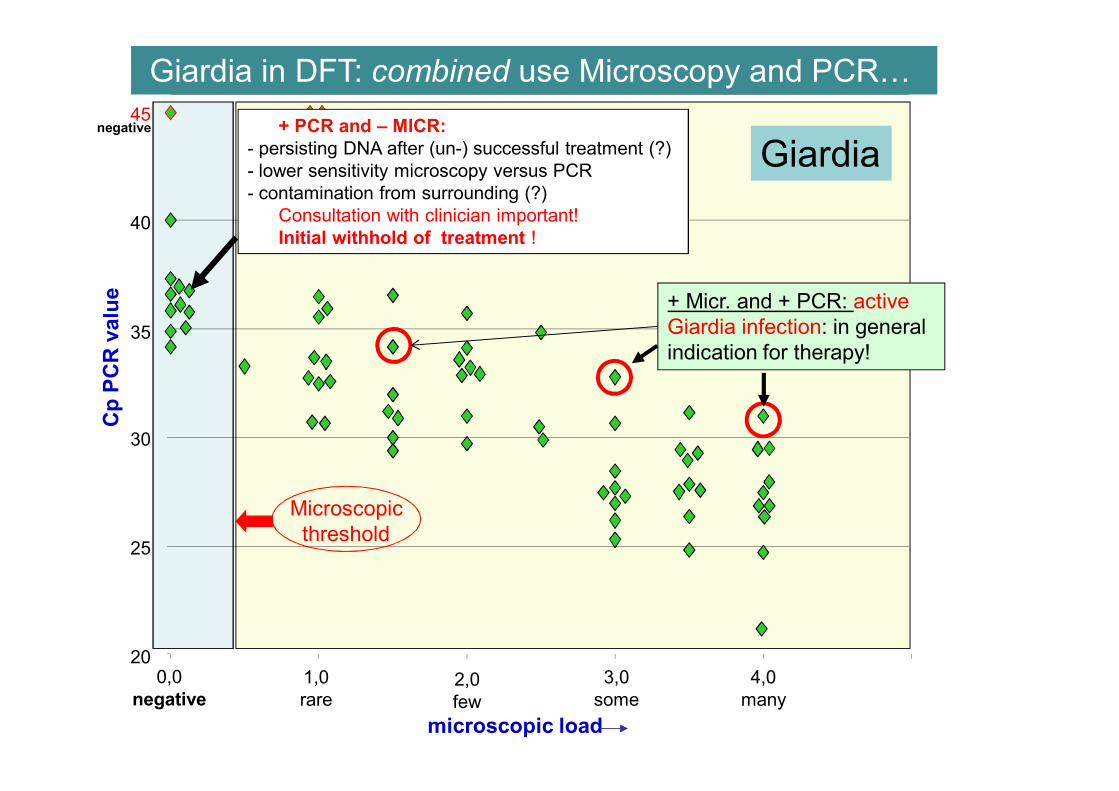
Giardia+ PCR and – MICR:
- persisting DNA after (un-) successful treatment (?)
- lower sensitivity microscopy versus PCR
- contamination from surrounding (?)
Consultation with clinician important!
Initial withhold of treatment !
+ Micr. and + PCR: active
Giardia infection: in general
indication for therapy!
negative
Microscopic
threshold
Giardia in DFT: combined use Microscopy and PCR…
Amoebiasis
due to Entamoeba histolytica
an “old” but still most important - dangerous- cause
of intestinal and liver disease……
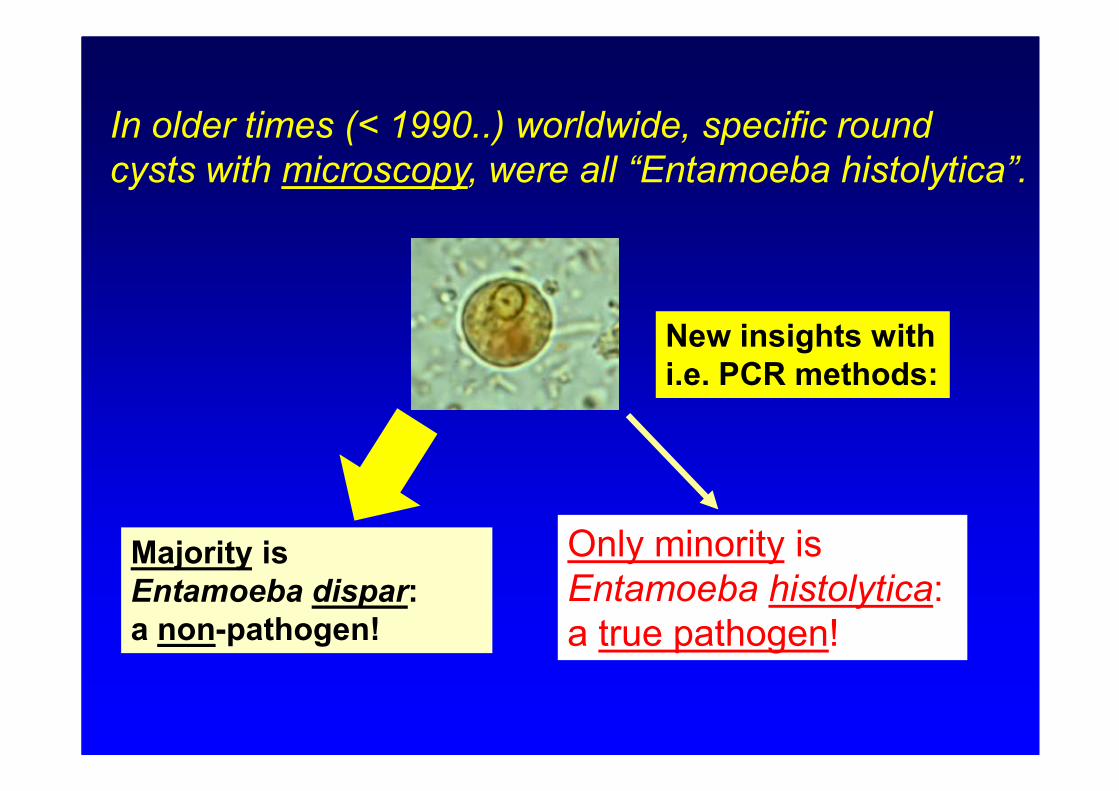
In older times (< 1990..) worldwide, specific round
cysts with microscopy, were all “Entamoeba histolytica”.
Majority is
Entamoeba dispar:
a non-pathogen!
Only minority is
Entamoeba histolytica:
a true pathogen!
New insights with
i.e. PCR methods:
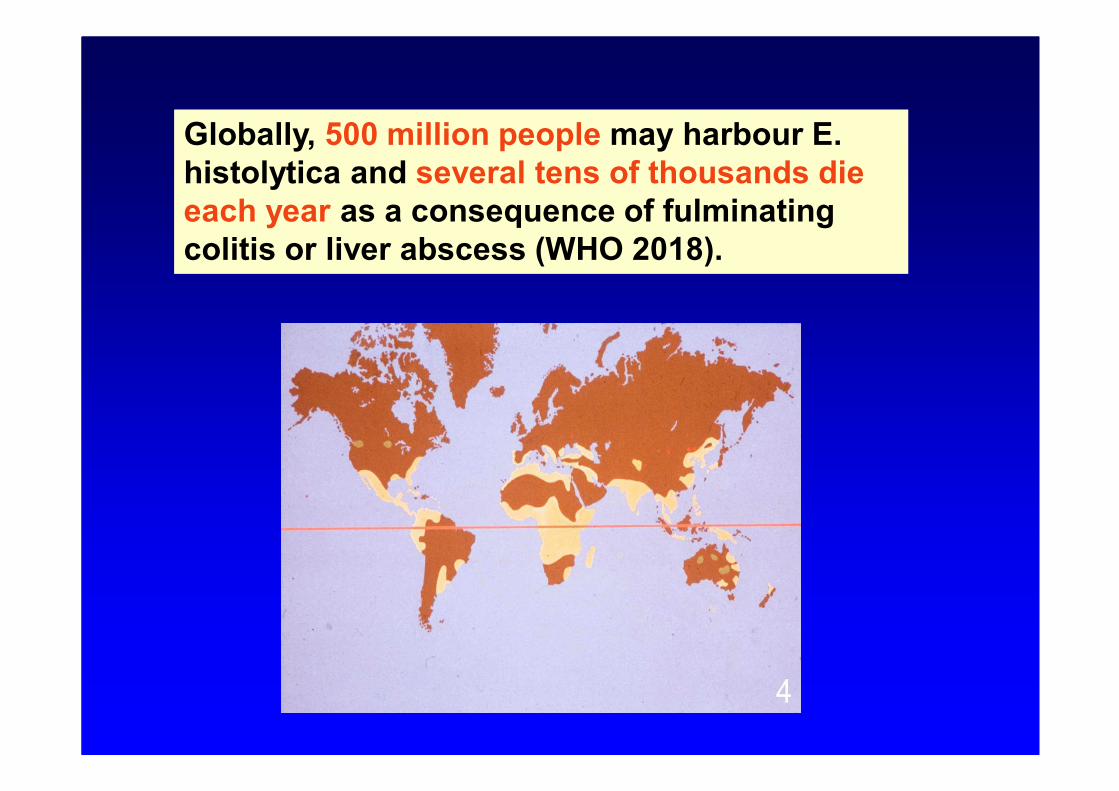
Globally, 500 million people may harbour E.
histolytica and several tens of thousands die
each year as a consequence of fulminating
colitis or liver abscess (WHO 2018).
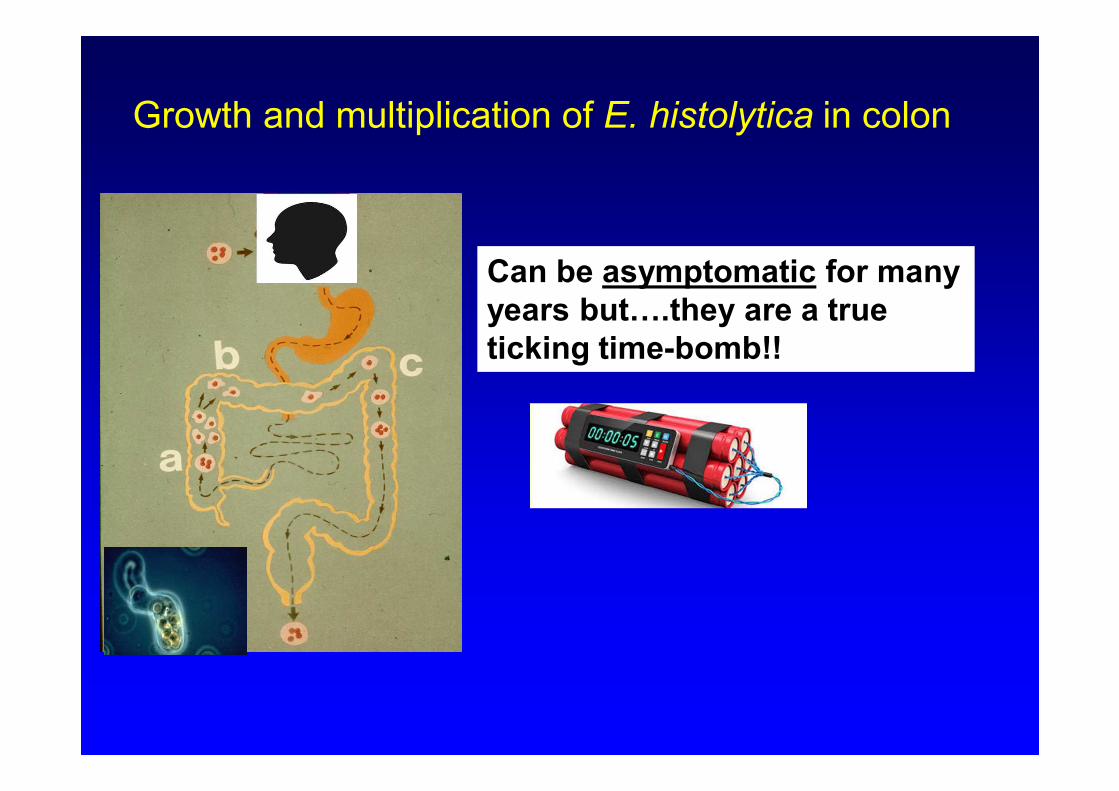
Growth and multiplication of E. histolytica in colon
Can be asymptomatic for many
years but….they are a true
ticking time-bomb!!
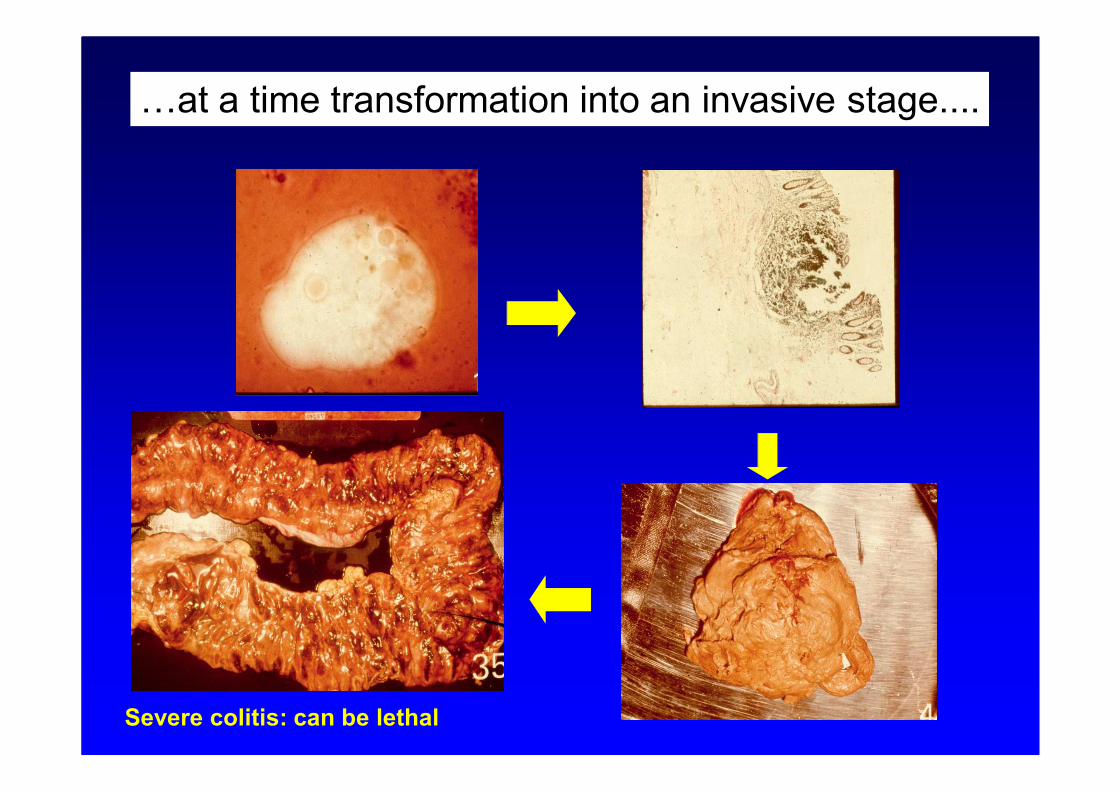
…at a time transformation into an invasive stage....
Severe colitis: can be lethal
Beware: in non- endemic countries….
DD E. histolytica infection and Crohn’s disease!
Numerous cases in world literature with presumed
“Crohn’s disease” while afterwards... amoebiasis
Before diagnosis of “Crohn’s disease”
always exclude E. histolytica infection!!
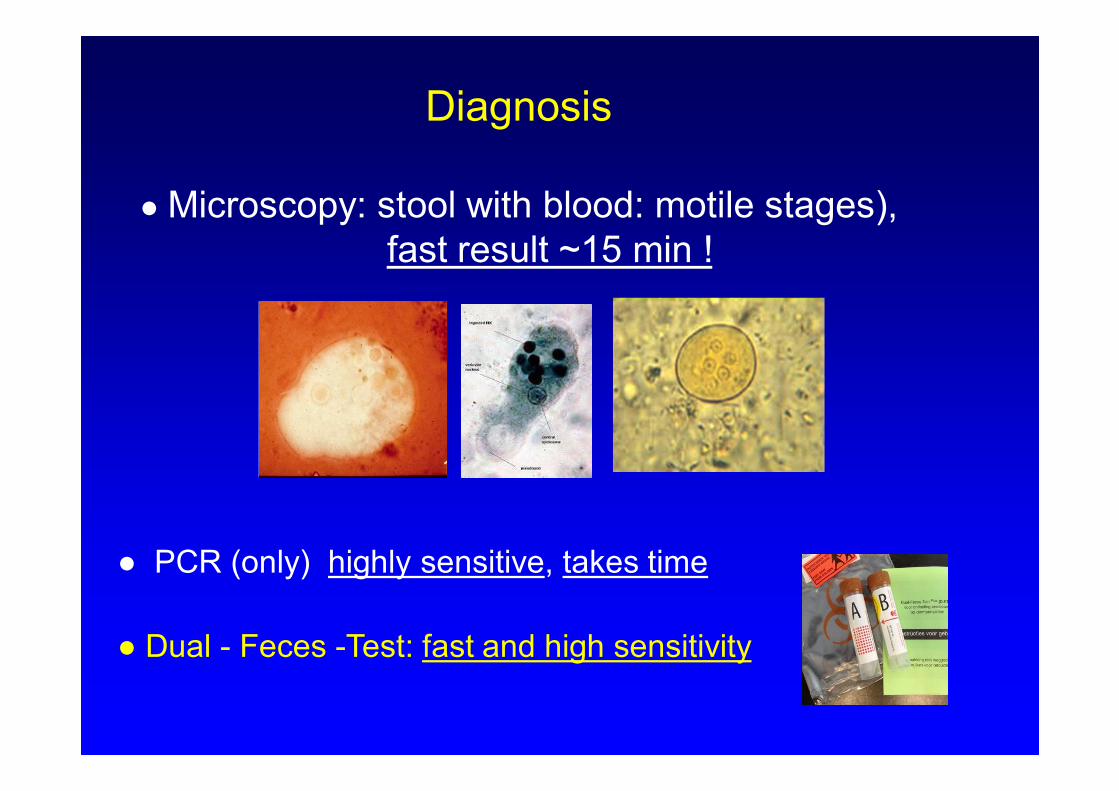
Diagnosis
● Microscopy: stool with blood: motile stages),
fast result ~15 min !
● PCR (only) highly sensitive, takes time
● Dual - Feces -Test: fast and high sensitivity
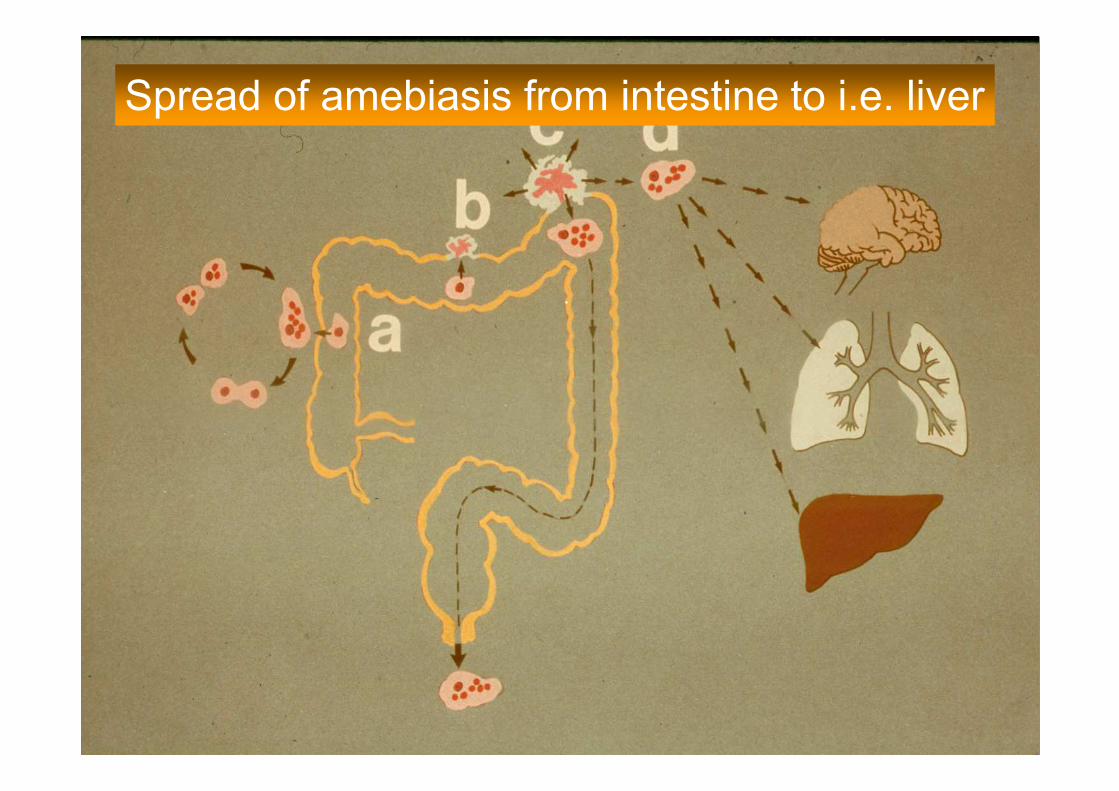
Spread of amebiasis from intestine to i.e. liver
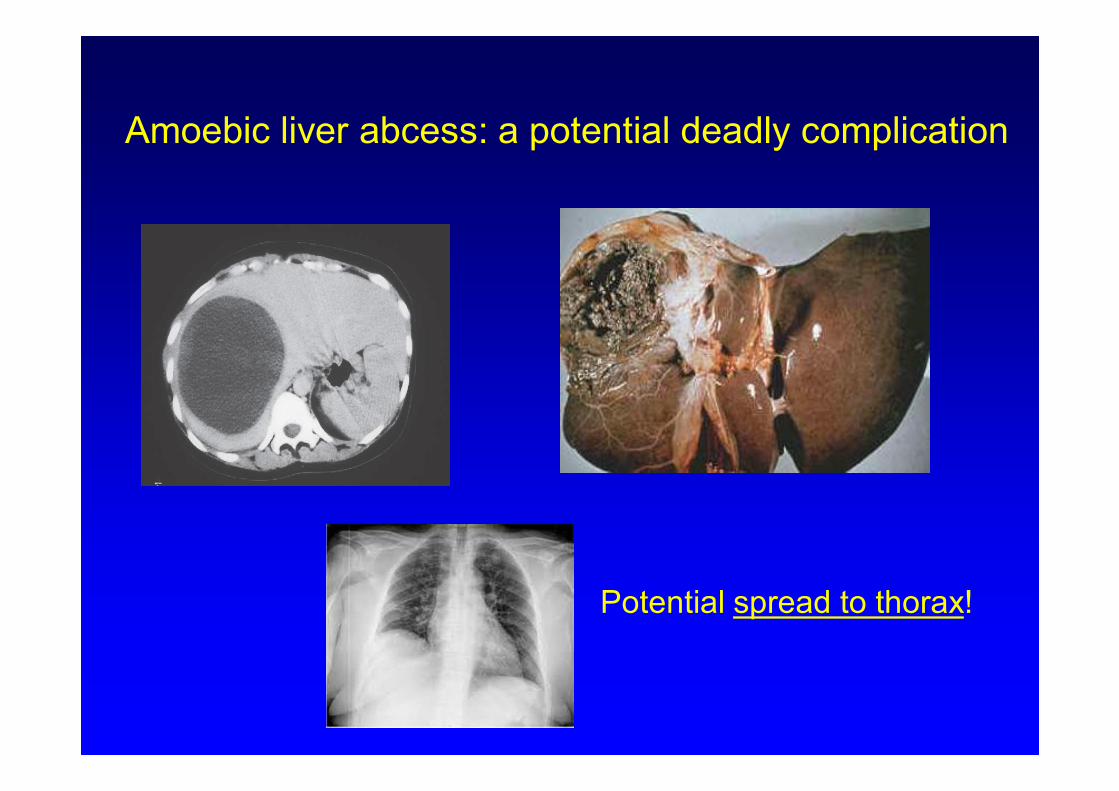
Amoebic liver abcess: a potential deadly complication
Potential spread to thorax!
For diagnosis of amoebic abscess in the liver
serology is important !
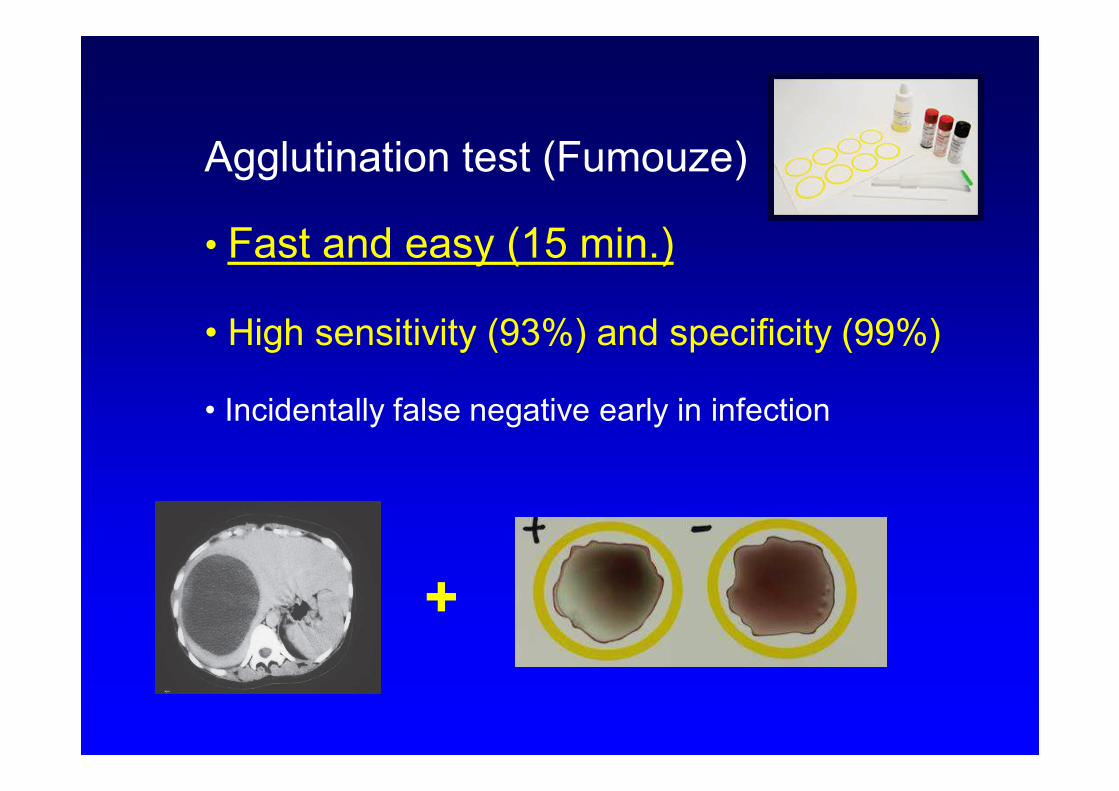
Agglutination test (Fumouze)
• Fast and easy (15 min.)
• High sensitivity (93%) and specificity (99%)
• Incidentally false negative early in infection
+
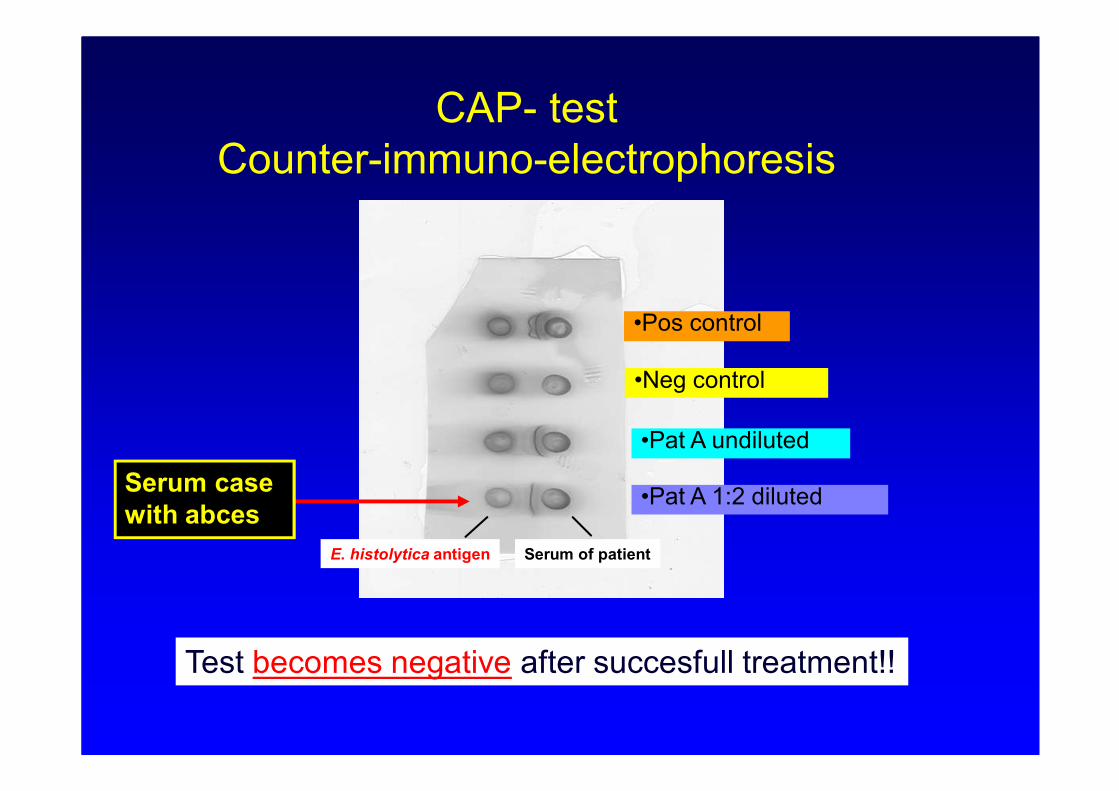
CAP- test
Counter-immuno-electrophoresis
•Pos control
•Neg control
•Pat A undiluted
•Pat A 1:2 diluted
Serum of patientE. histolytica antigen
Test becomes negative after succesfull treatment!!
Serum case
with abces
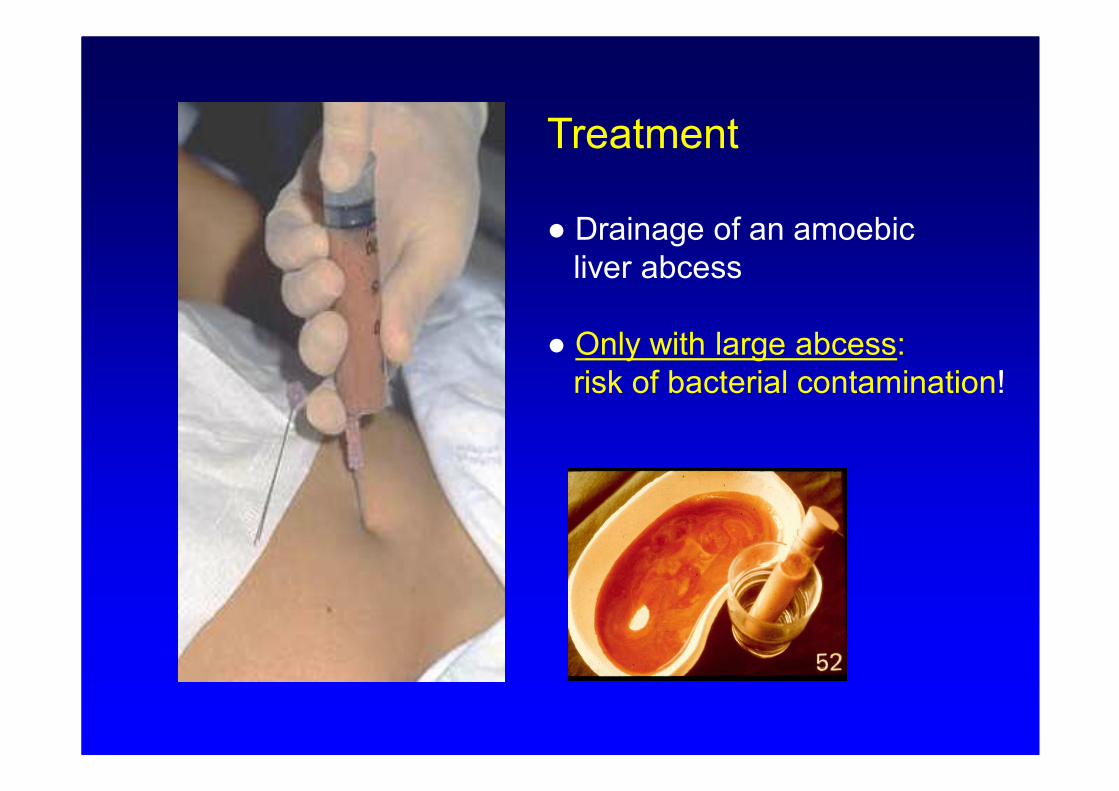
Treatment
● Drainage of an amoebic
liver abcess
● Only with large abcess:
risk of bacterial contamination!
Treatment
● tissue phase: metronidazol (750 mg tid x 7-10d)
● luminal agents : clioquinol (3dd 250mgx 10d)
diloxanide furoate (3dd 500 mg 10d)
paromomycin (30 mg/kg x 7d)
Always treat with a luminal agent after
treatment of the tissue phase!
II Giardia lamblia
an important cause of prolonged diarrhoea in
both tropical and western countries
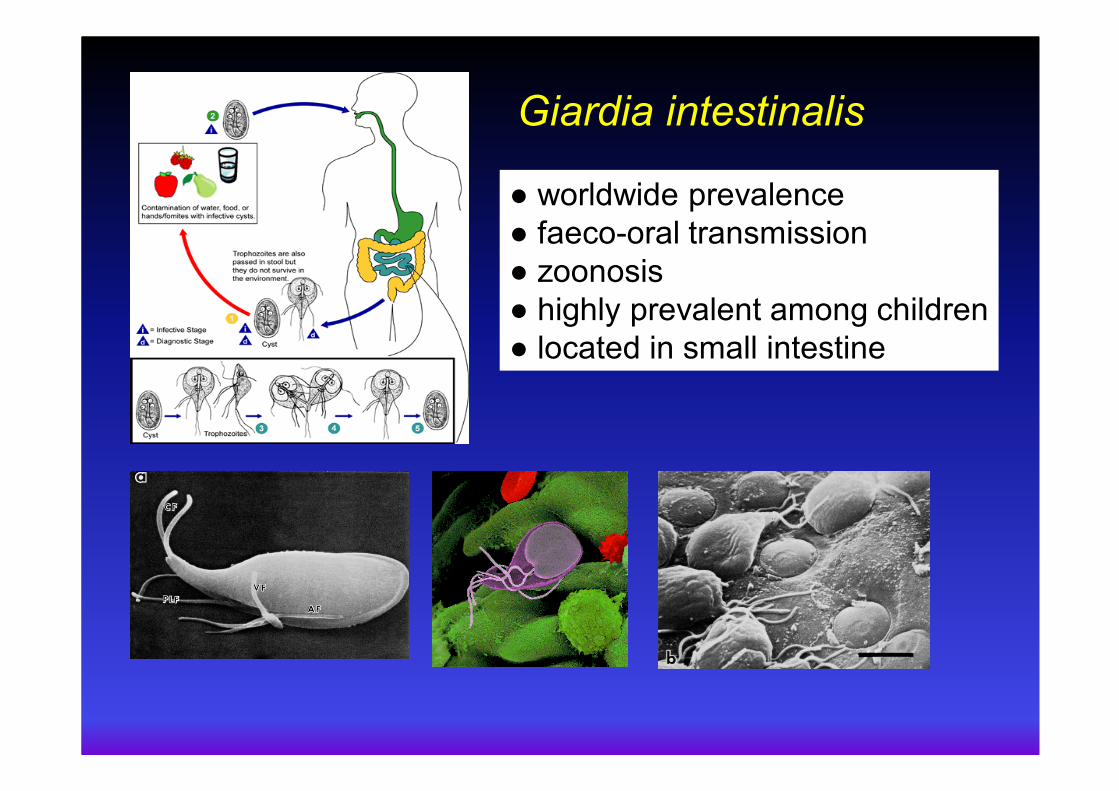
Giardia intestinalis
● worldwide prevalence
● faeco-oral transmission
● zoonosis
● highly prevalent among children
● located in small intestine
Symtomatology Giardia infection
• Asymptomatic carrier state: commonly occuring (80% infected)
important source of infection
• Acute diarrhoea: often self limiting (2- 4 weeks), weight loss,
abdominal cramps, nausea, flatulence,
steatorrhoea (in 50% of cases).
Chronic diarhoea: persistence of diarrhoea, weight
loss, impairment of growth and developement
especially in children in developing countries
Post infectious IBSPost infectious IBSPost infectious IBSPost infectious IBS
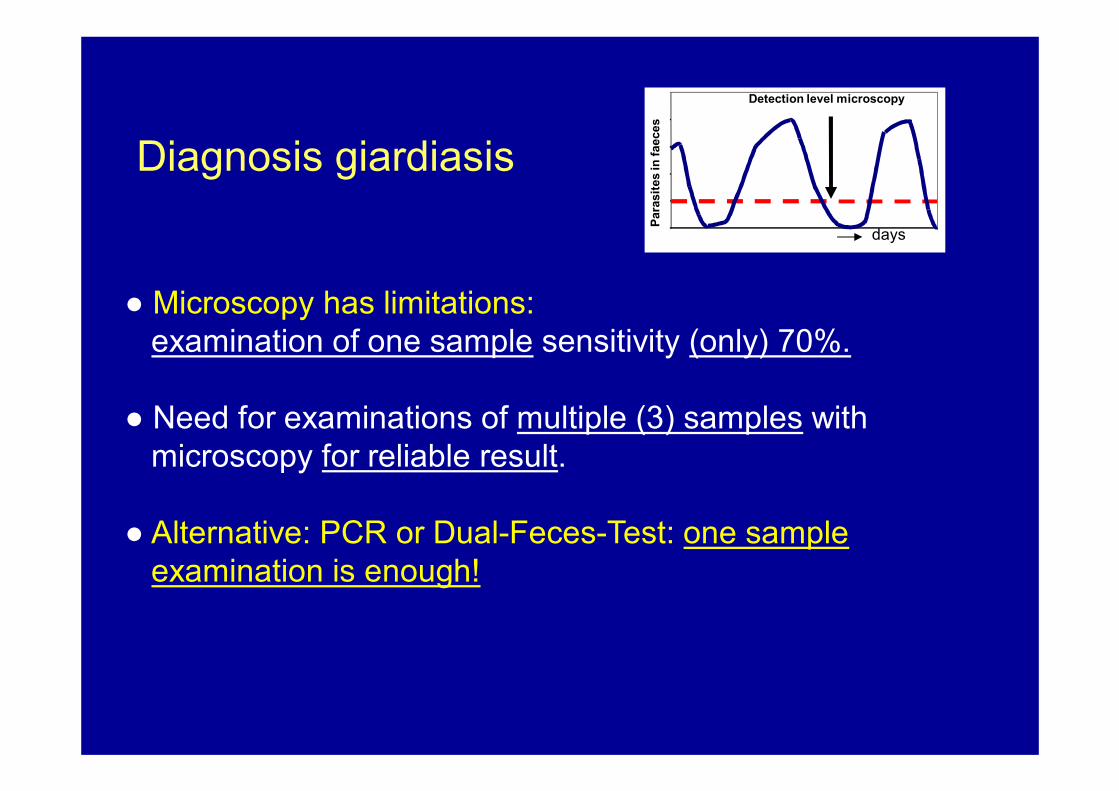
Diagnosis giardiasis
● Microscopy has limitations:
examination of one sample sensitivity (only) 70%.
● Need for examinations of multiple (3) samples with
microscopy for reliable result.
● Alternative: PCR or Dual-Feces-Test: one sample
examination is enough!
Para
sit
es in
faeces
Detection level microscopy
days
Current therapy
metronidazole: 500mg 3dd, 7 days
main alternatives:
tinidazol: 2 gram / day once (USA no.1) !!
albendazol: > 1 year: 400 mg. 1dd, 5 dgn
A frequent, under recognised, problem:
Regular treatment not effective to eradicate Giardia infection: nitroimidazole - resistant Giardiasis (Refractory Giardiasis , RG).
E.R. Carter, *, L.E. Nabarro 1, L. Hedley 2, P.L. Chiodini
The Hospital for Tropical Diseases, UK, Pharmacy, University College London
Hospitals NHS Foundation Trust, London, UK
How to deal with a patient with persistent Giardia
infection after standard treatment?
• Councelling for possible re-infections from environment :
partners (MSM), children, pets, and water sources.
• Examination for IgA deficiency, HIV, coeliac disease
When negative: possible true therapy resistance of Giardia
isolates. Difficult to examine in routine clinical practice !
start “pragmatic approach guided by experience” for
other treatment regimen (i.e. Carter 2017)
When negative: possible true nitroimidazle resistant Giardia
isolates. Not possible to examine in clinical practice
Suggested treatment regimens in RG:
1: tinidazol (1d, 2 gr) , albendazol (400 mg 2dd, 5d), tinidazol (1d, 2gr)“
2: mepacrine (100mg 3dd, 3-7d)
3: aldendazol (2dd 400mg, 14 d….(?))
Carter et al 2017++
also with microscopy!!
III Cyclospora cayetanensis
the “overlooked” parasite….
1986 Soave. Patients in Haiti and Mexico with
diarrhea. Structures 8 -10 µm, defined
wall, granular material inside: coccidian
body/fungal spore. “Big Crypto”.
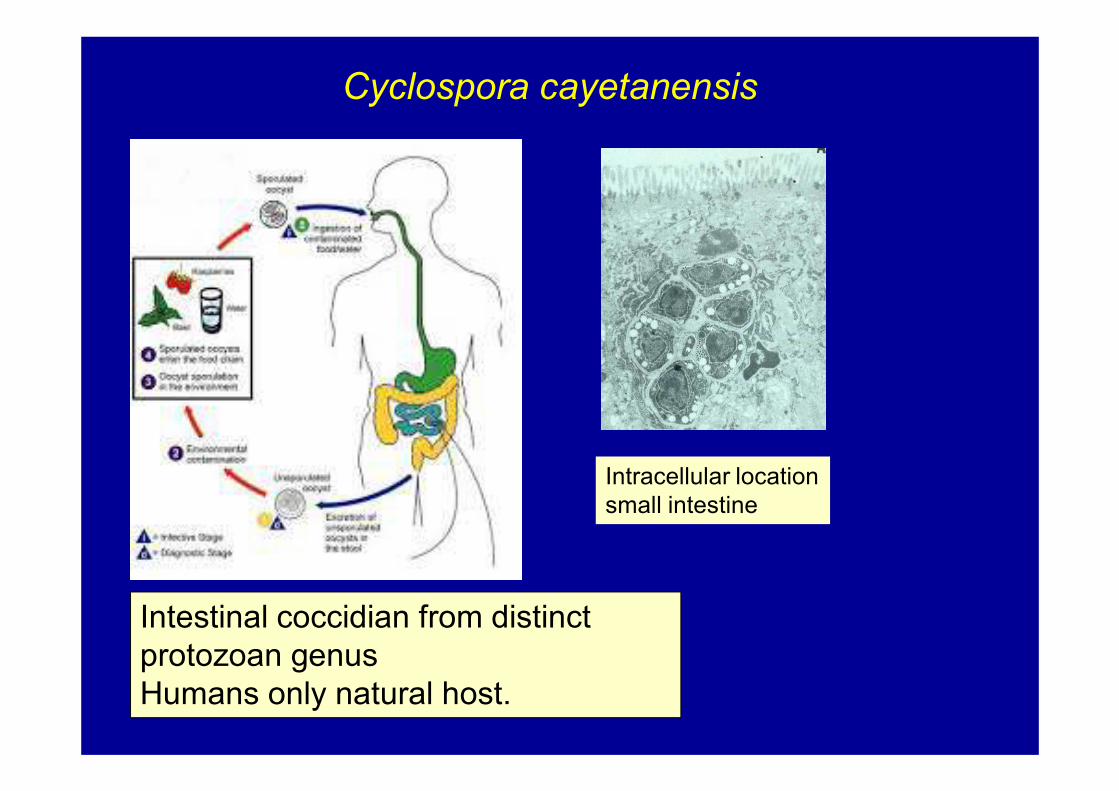
Intestinal coccidian from distinct
protozoan genus
Humans only natural host.
Cyclospora cayetanensis
Intracellular location
small intestine

Diagnosis: relative easy with microscopy!
● 8-10 um with several globlets inside.
● when properly trained technicians “cannot miss it”!!
The importance of microscopy… also in NL!
Additional routine microscopy (10 min search) :
result: many cysts of Cyclospora
A group of persons with severe symptomatology i.e. severe
abdominal pain and loss of weight (8 kg in two weeks)
Standard: PCR for E. histolytica, Giardia and Cryptosporidium:
Result (2x): “No parasites” found.
All patients persisted, for two weeks, to be most ill !!!
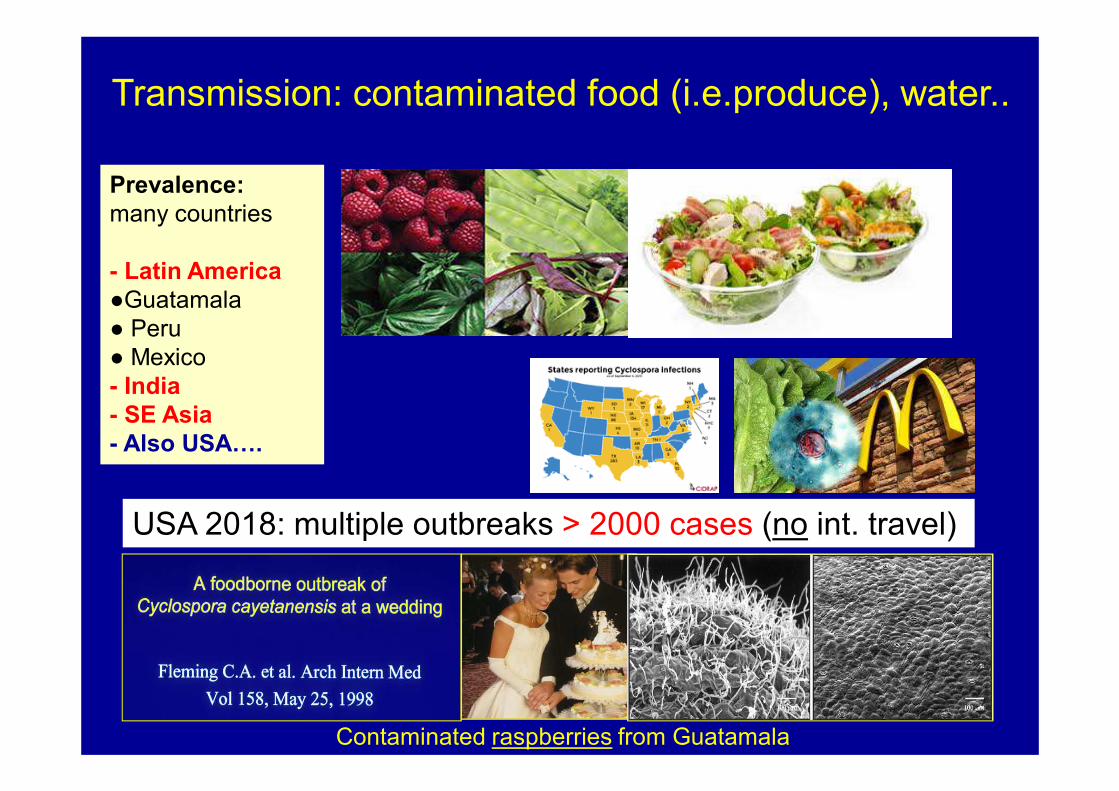
Transmission: contaminated food (i.e.produce), water..
Prevalence:
many countries
- Latin America
●Guatamala
● Peru
● Mexico
- India
- SE Asia
- Also USA….
USA 2018: multiple outbreaks > 2000 cases (no int. travel)
Contaminated raspberries from Guatamala
Symptomatology associated with
Cyclospora infection
• patients often feel very ill!
• predominant symptom: watery diarrhea often in relapsing, cyclical pattern
• important associated symptoms:• heartburn-like symptoms, abdominal cramps
• fatigue
• anorexia, weight loss (up to 10 kg!) and vomiting
• infection may last for weeks (but is self-limiting)
Effective treatment available!!
In case of severe complaints:
Co-trimoxazole (trimethoprim - sulfamethoxazole
(160/800 mg) 2x dd for 7-10 days
Fast effect after start of treatment!
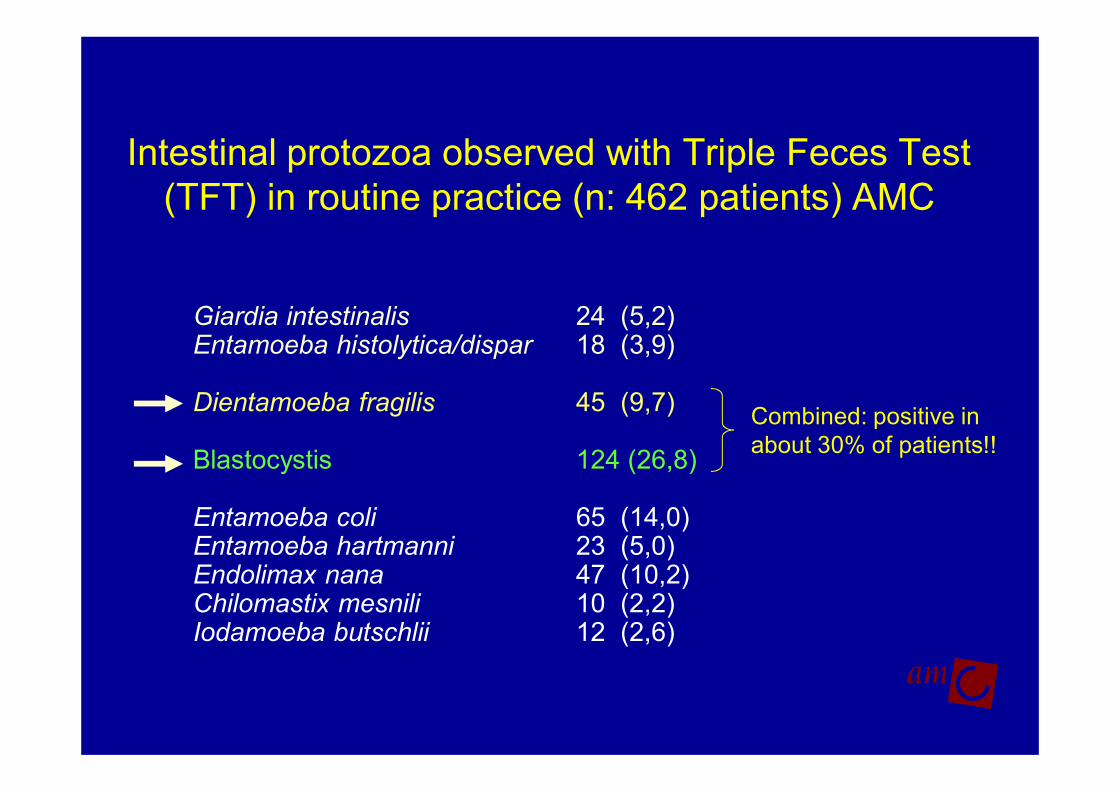
Intestinal protozoa observed with Triple Feces Test
(TFT) in routine practice (n: 462 patients) AMC
Giardia intestinalis 24 (5,2) Entamoeba histolytica/dispar 18 (3,9)
Dientamoeba fragilis 45 (9,7)
Blastocystis 124 (26,8)
Entamoeba coli 65 (14,0)Entamoeba hartmanni 23 (5,0)Endolimax nana 47 (10,2)Chilomastix mesnili 10 (2,2)Iodamoeba butschlii 12 (2,6)
Combined: positive in
about 30% of patients!!
Dientamoeba fragilis
a parasite of importance for childrenand (some) adults!
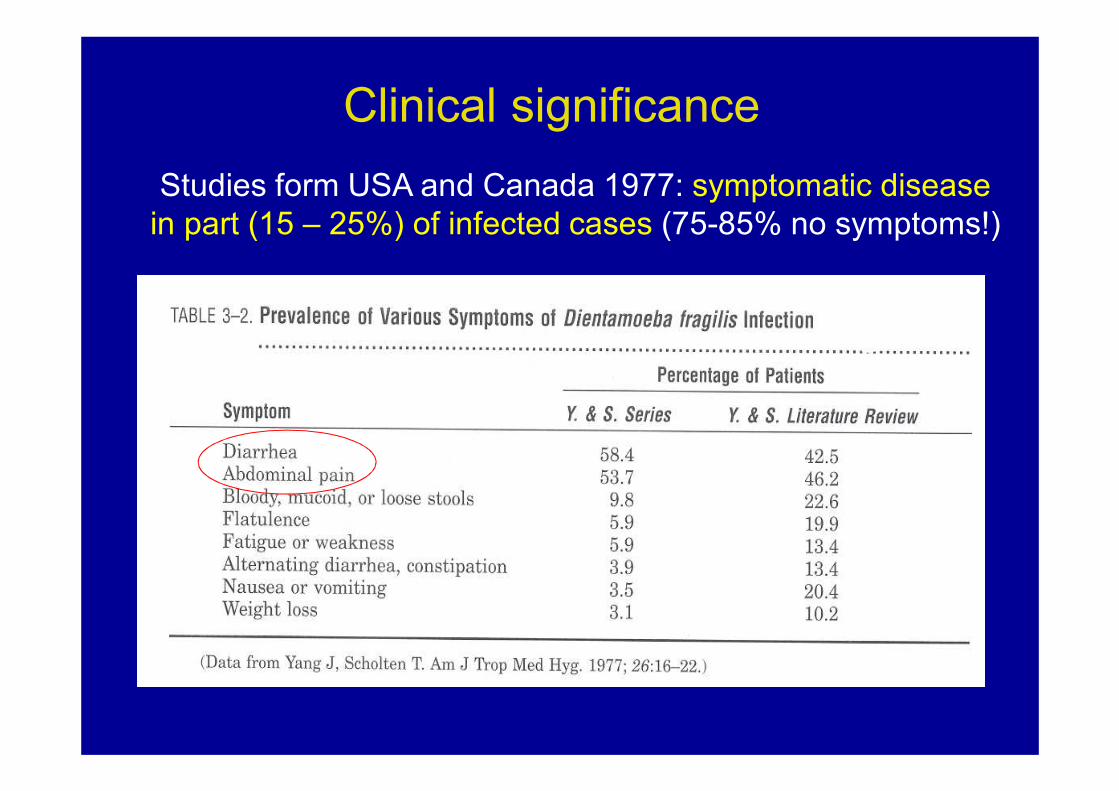
Clinical significance
Studies form USA and Canada 1977: symptomatic disease
in part (15 – 25%) of infected cases (75-85% no symptoms!)
Dientamoeba fragilis
Important to consider in children with persistent
intestinal complaints !
NTVG 2004
▪ 43 children with abdominal complaints and no other cause▪ treatment clioquinol or metronidazol (27C , 6 M/T)
▪ In 33 / 43 children after therapy eradication of parasites.In 27 out of 33 (82%) symptoms were considerably less or were completely disappeared.
▪ From 10 children without clearance of parasites after treatment, in 2 (20%) complaints were less or disappeared
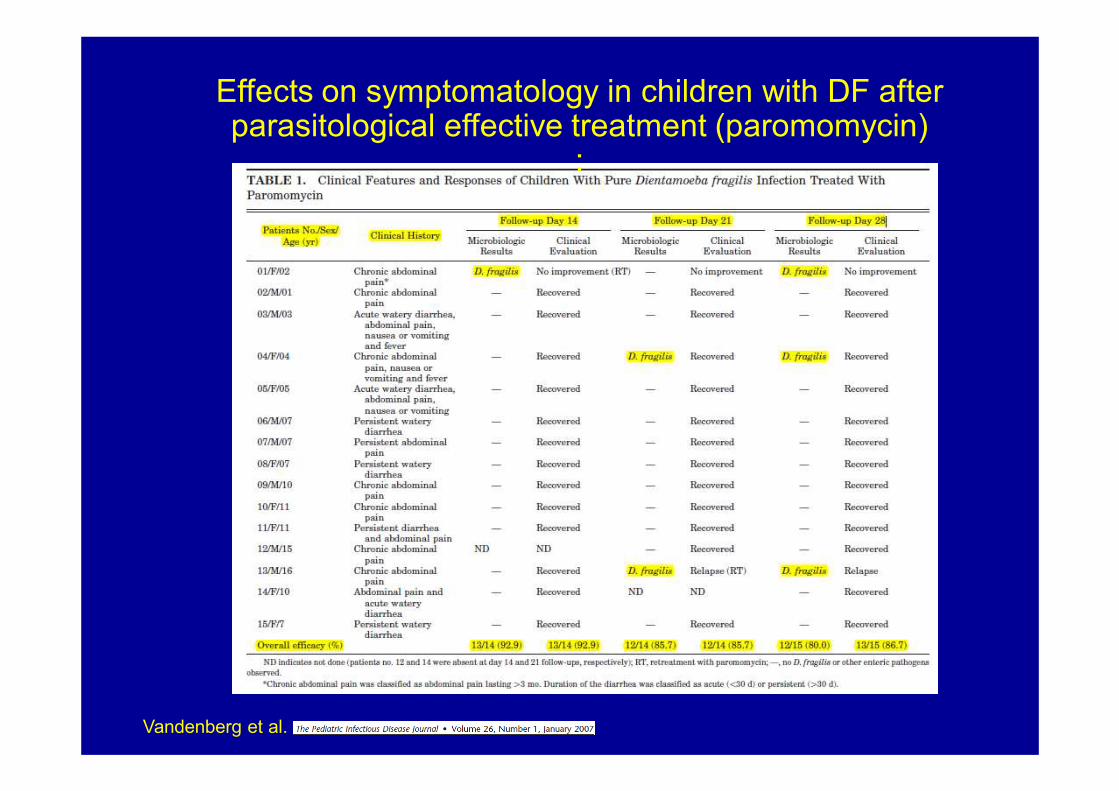
Effects on symptomatology in children with DF after parasitological effective treatment (paromomycin)
:
Vandenberg et al.
Many other reports, worldwide, which suggest pathogenicity of D. fragilis…..
Simon et al. (1967)Spencer et al. (1979) Keystone et al. (1983)Dardick (1983)Millet et al. (1983)Oxner et al. (1987)Preiss et al. (1991) Butler (1996)Cuffari et al. (1998) Girginkardesler et al. (2003)Bosman et al. (2004) Vandenberg et al. (2006, 2007).Kurt et al. (2008)Stark et al. (2010)van Hellemond et al. (2012)
Longstanding worldwide evidence /observations that D. fragilis infections can elicit symptomatology in humans.
Pathogenesis is unknown
As with Giardia, there are also many asymptomatic carriers with DF !!
In The Netherlands….
After introduction of PCR for diagnosis of D. fragilis
no difference in prevalence in between symptomatic and asymptomatic individulas…
“D. fragilis is not (never) a cause of disease”
Diagnosis is also no longer indicated
End
But only in this country (NL), after
introduction of PCR for diagnosis,
D. fragilis is declared to be an
apathogen…!!
Fifty years English literature:
“ D. fragilis can, in a selected group of persons,
be a cause of symptomatology…”
?
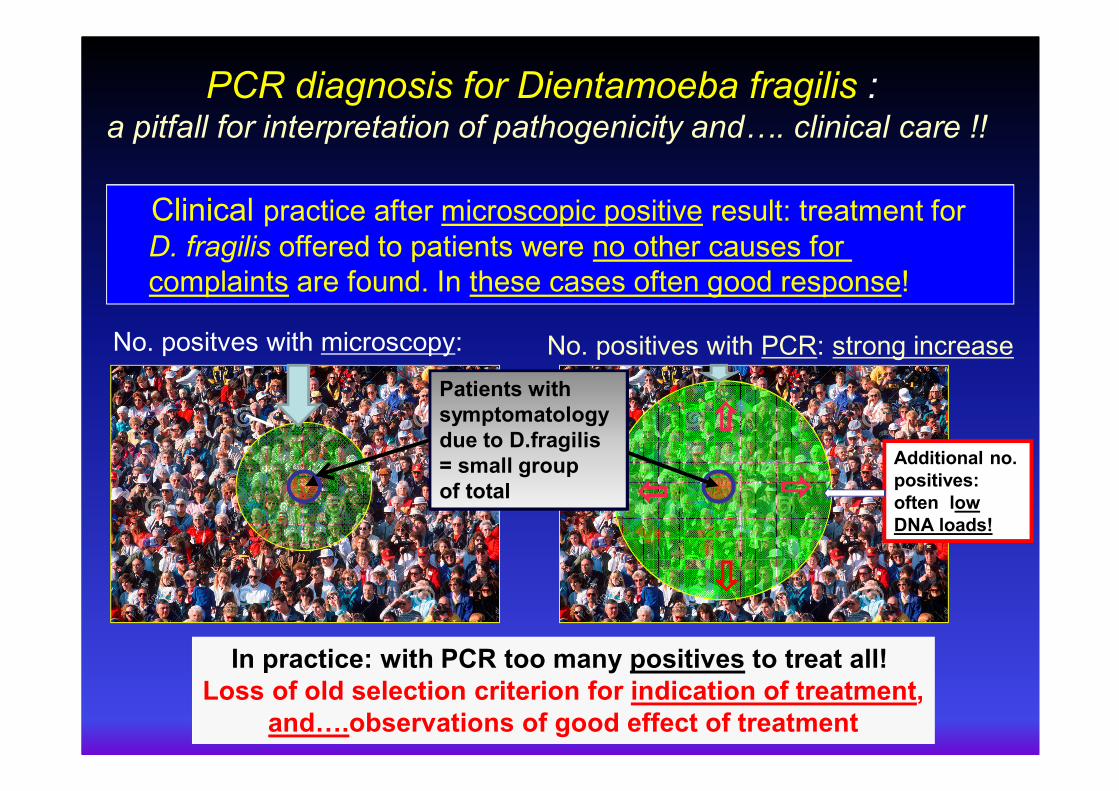
Clinical practice after microscopic positive result: treatment for
D. fragilis offered to patients were no other causes for
complaints are found. In these cases often good response!
In practice: with PCR too many positives to treat all!
Loss of old selection criterion for indication of treatment,
and….observations of good effect of treatment
PCR diagnosis for Dientamoeba fragilis : a pitfall for interpretation of pathogenicity and4. clinical care !!
Additional no.
positives:
often low
DNA loads!
Patients with
symptomatology
due to D.fragilis
= small group
of total
No. positves with microscopy: No. positives with PCR: strong increase
@amc.uva.nl
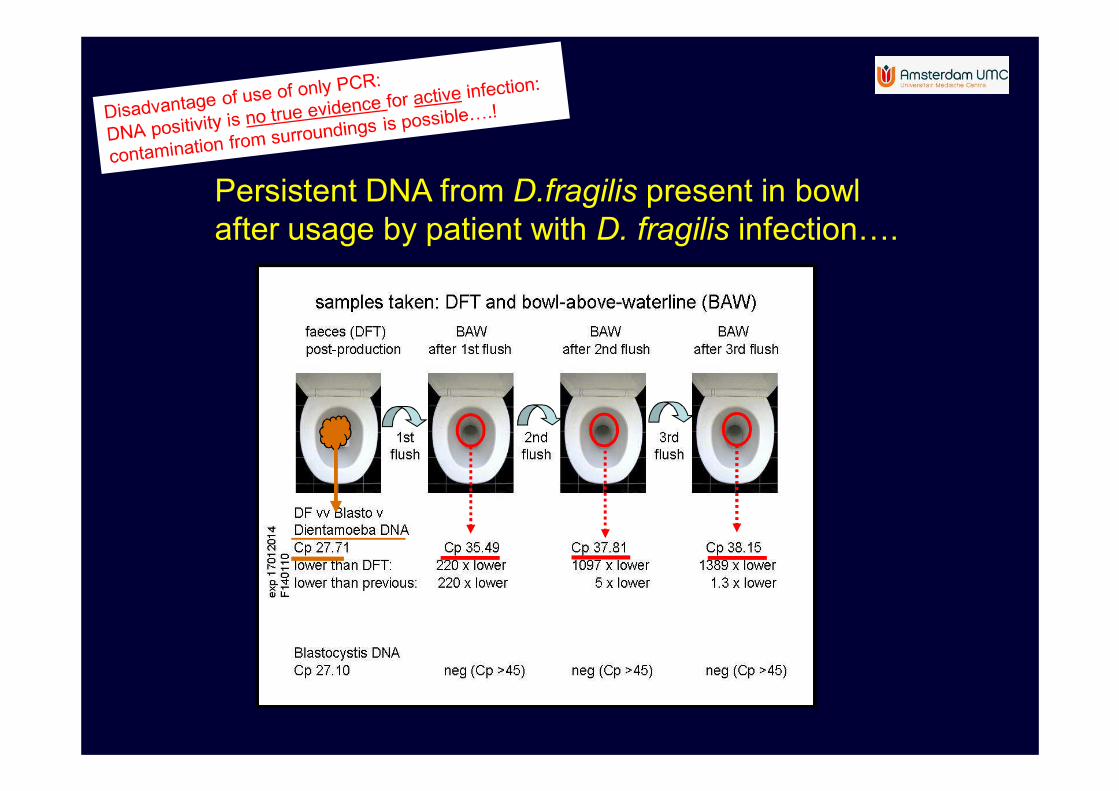
Persistent DNA from D.fragilis present in bowl
after usage by patient with D. fragilis infection….
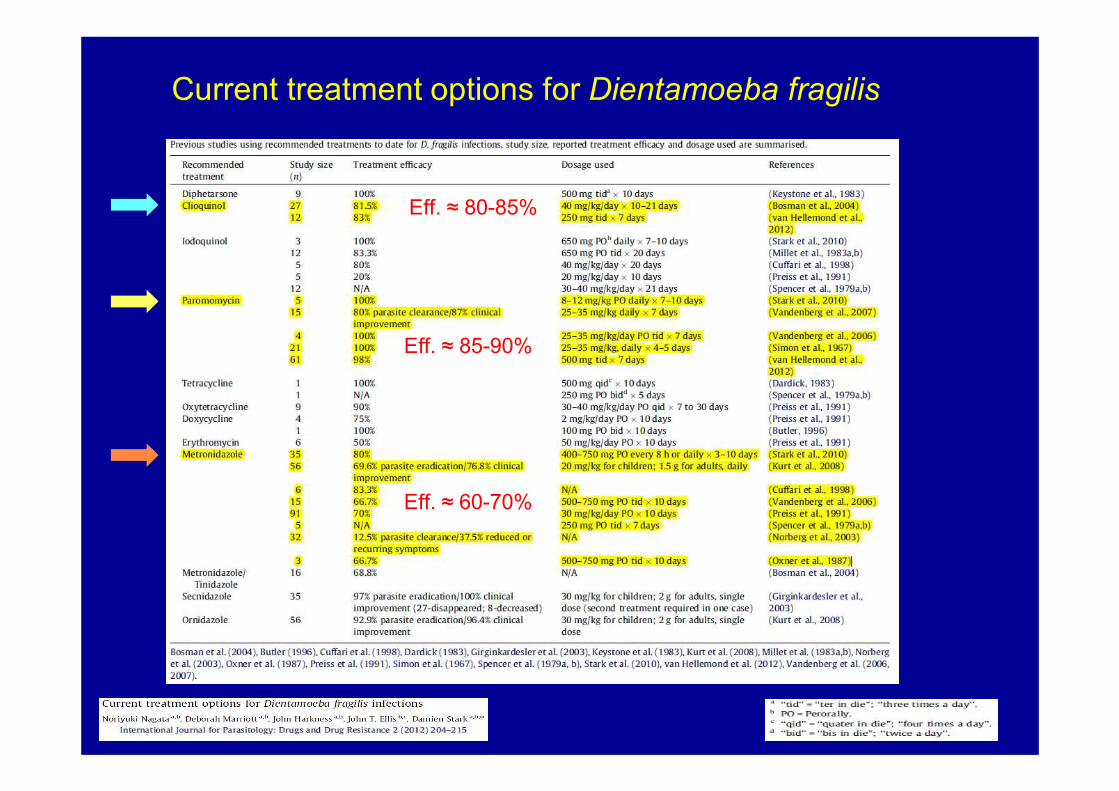
Current treatment options for Dientamoeba fragilis
Eff. ≈ 80-85%
Eff. ≈ 85-90%
Eff. ≈ 60-70%
▪ Use of clioquinol is safe in dosage of 3 dd 250 mg (adults) and 10-15 mg/kg/day divided in three doses (children), for 7-10 days.
▪ Neurotoxicity (SMON) described in Japan, especially after usage of high dosages in short period of time, or prolonged usage (months-years) . Side effects possible related to deficiency of Vit B12 in post war Japan.
▪ Outside Japan complications only seldom observed: only some cases described in over 500 million doses provided (!) , before side effects inJapan were noticed.
▪ No evidence of accumulation in the body after treatment in recent studies*:
▪ Clioquinol not detectable in plasma 3 days after 7-14 days of treatment with a dosage of 750 mg/day.
▪ Intracellular concentrations of clioquinol in Peripheral Blood Mononuclear cells very low after treatment with 800 mg/day for 8 days. Clinical no side effects < 2400 mg /day for 8 days.
*(potential use as anticancer agent: studies in 2003, 2007, 2012)
Clioquinol usage in The Netherlands:
with restricted use, it is safe.
(also in common use in Amsterdam UMC)
Practical aspects use of clioquinol
• Can be obtained from every pharmacy in NL
• Suspension 100 mg/ml according to FNA
• Preferable produced by “ De Magistrale Bereider” (preparation of a proper suspension is difficult)
• Do shake bottle thoroughly in advance: most important, otherwise “only water” will be used
• Important to calculate appropriate volume and instruct mother with handling of syringe
• Costs: relative cheap: 43 euro per bottle (= 100 ml of 100 mg/ml, )
• Dosage: 15 mg/kg/day (max 750 mg), divided over 3 doses, for 10 days.

Blastocystis spp. infection
an intriguing “new” field of interest !
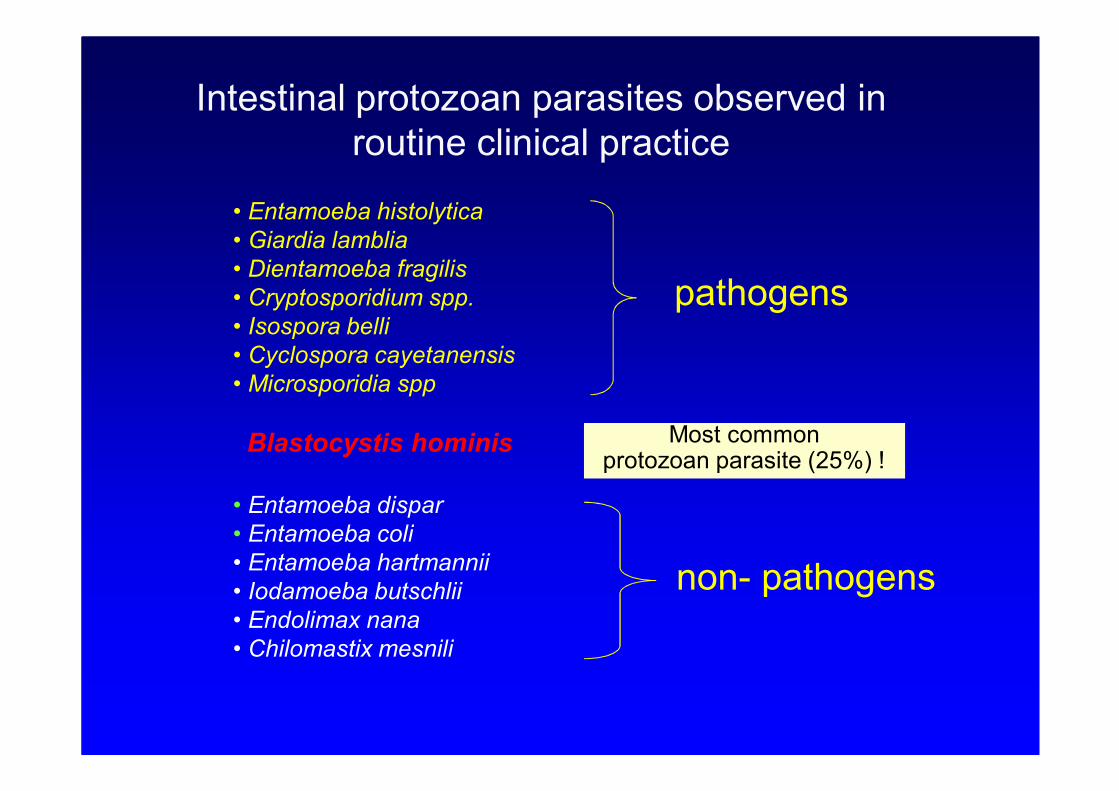
Intestinal protozoan parasites observed in
routine clinical practice
• Entamoeba histolytica
• Giardia lamblia
• Dientamoeba fragilis
• Cryptosporidium spp.
• Isospora belli
• Cyclospora cayetanensis
• Microsporidia spp
Blastocystis hominis
• Entamoeba dispar
• Entamoeba coli
• Entamoeba hartmannii
• Iodamoeba butschlii
• Endolimax nana
• Chilomastix mesnili
pathogens
non- pathogens
Most common protozoan parasite (25%) !
Blastocystis spp:
many answers to be answered…!
• Taxonomic status …
• Mode of transmission….
• Clinical significance….
• Best diagnostic procedure….
• Effective therapy…..
But…..
• there were many more “subgroups” of Blastocystis!
• also common in animals!
• terminology was confusing: clusters, clades…
• now at least 14 species identified of which 4 species commonly are observed in humans
Formerly assumed in humans onlyone species: “Blastocystis hominis”
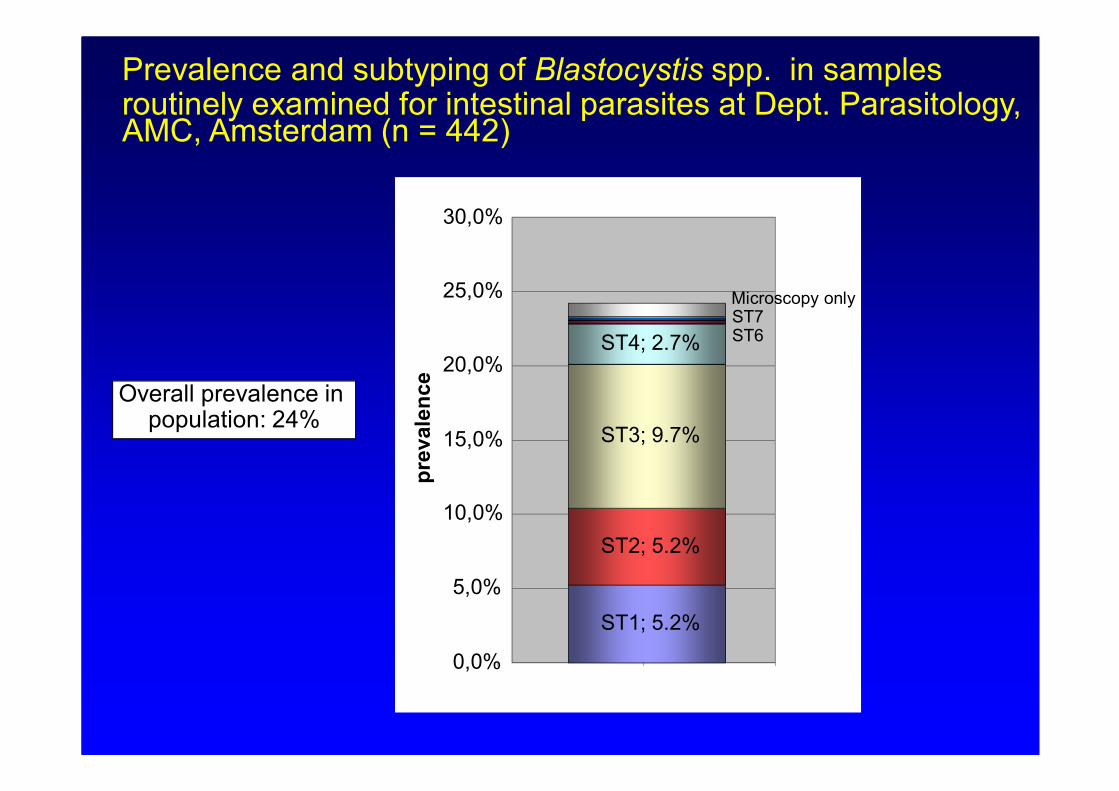
Prevalence and subtyping of Blastocystis spp. in samples routinely examined for intestinal parasites at Dept. Parasitology, AMC, Amsterdam (n = 442)
ST1; 5.2%
ST2; 5.2%
ST3; 9.7%
ST4; 2.7%
0,0%
5,0%
10,0%
15,0%
20,0%
25,0%
30,0%
pre
vale
nce
ST6ST7
Overall prevalence in population: 24%
Microscopy only
country
No Blasto infections
prevalence (%)
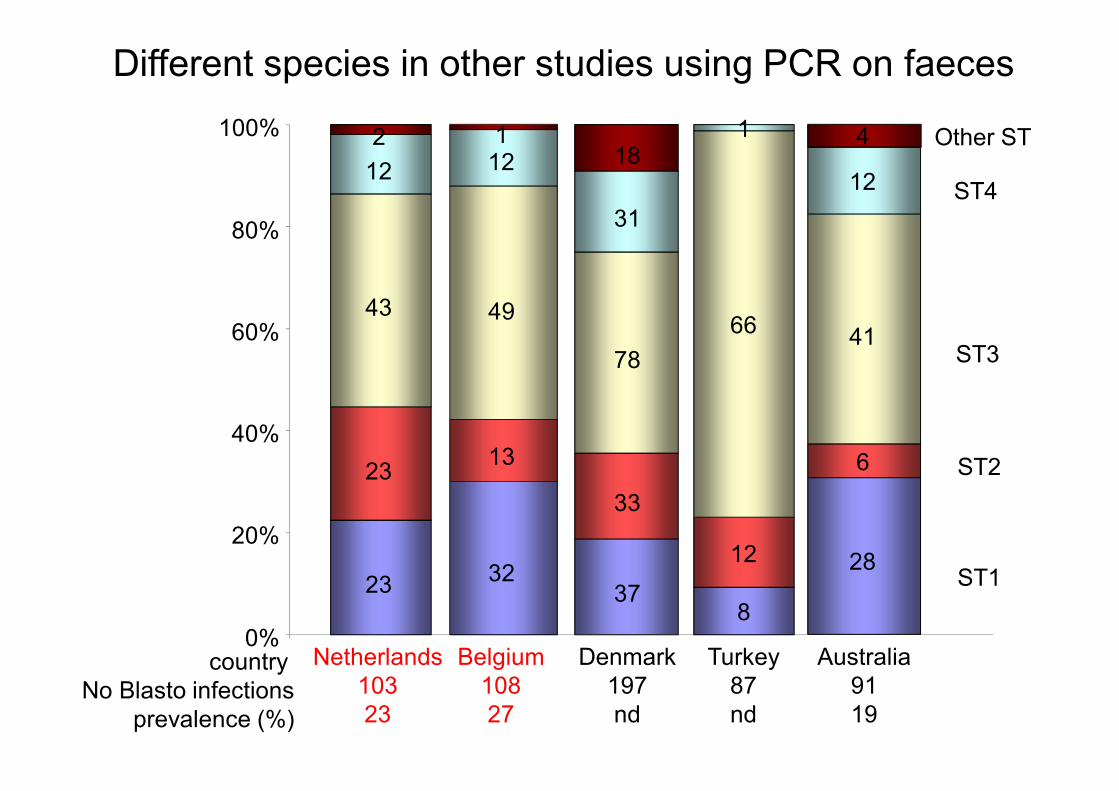
Netherlands
103
23
23
23
43
12
2
Denmark
197
nd
37
33
78
31
18
Turkey
87
nd
8
12
66
1
0%
20%
40%
60%
80%
100% Other ST
ST4
ST3
ST2
ST1
Different species in other studies using PCR on faeces
Belgium
108
27
12
49
13
32
1 4
12
41
6
28
Australia
91
19
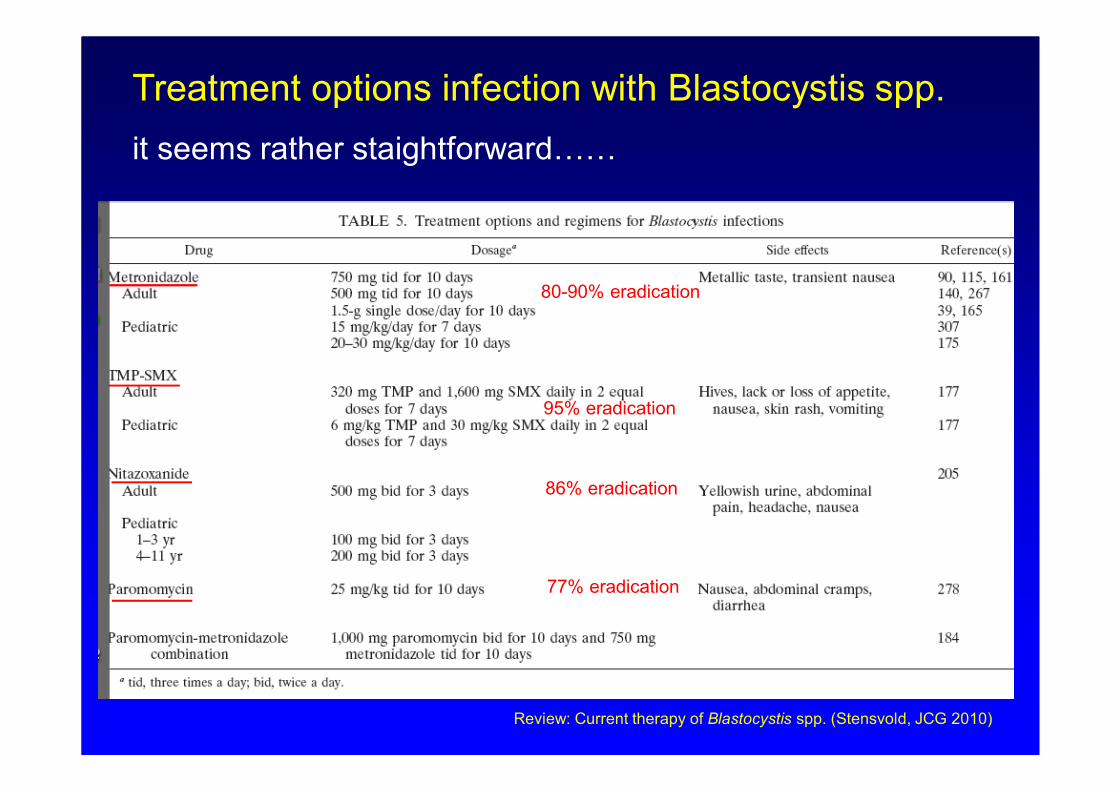
Treatment options infection with Blastocystis spp.
it seems rather staightforward……
Review: Current therapy of Blastocystis spp. (Stensvold, JCG 2010)
80-90% eradication
95% eradication
86% eradication
77% eradication
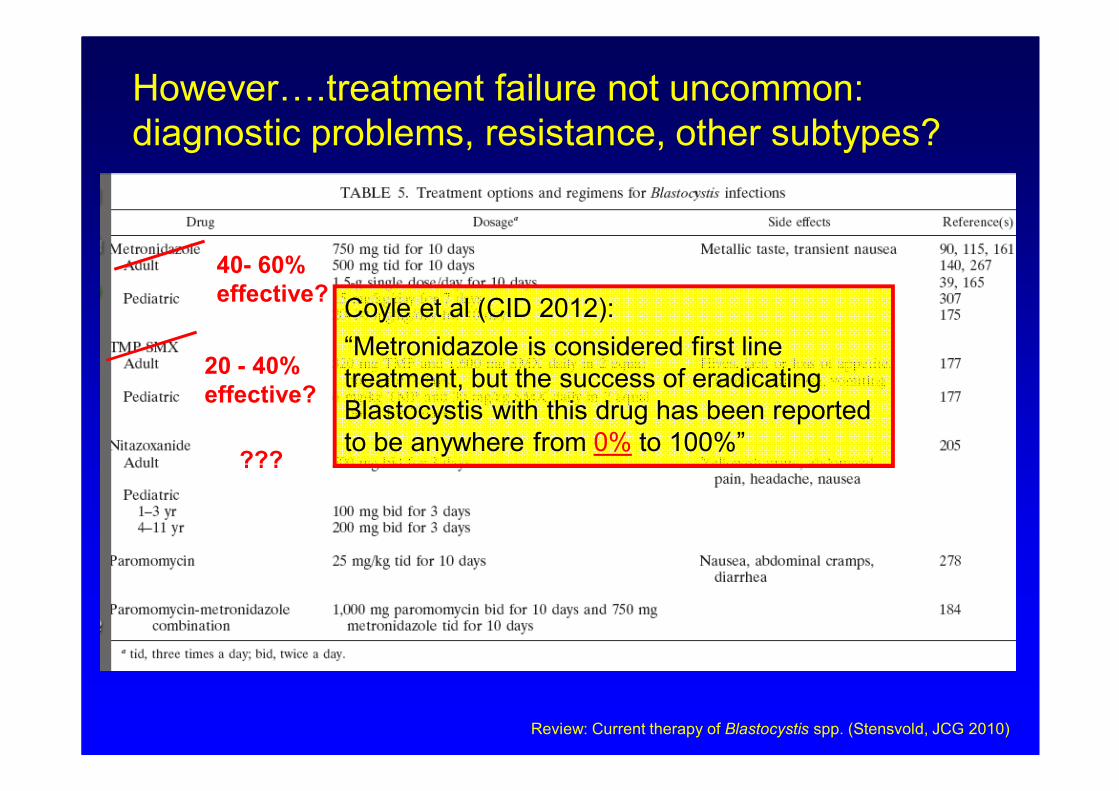
However….treatment failure not uncommon:
diagnostic problems, resistance, other subtypes?
20 - 40%
effective?
40- 60%
effective?
???
Review: Current therapy of Blastocystis spp. (Stensvold, JCG 2010)
Coyle et al (CID 2012):
“Metronidazole is considered first line
treatment, but the success of eradicating
Blastocystis with this drug has been reported
to be anywhere from 0% to 100%”
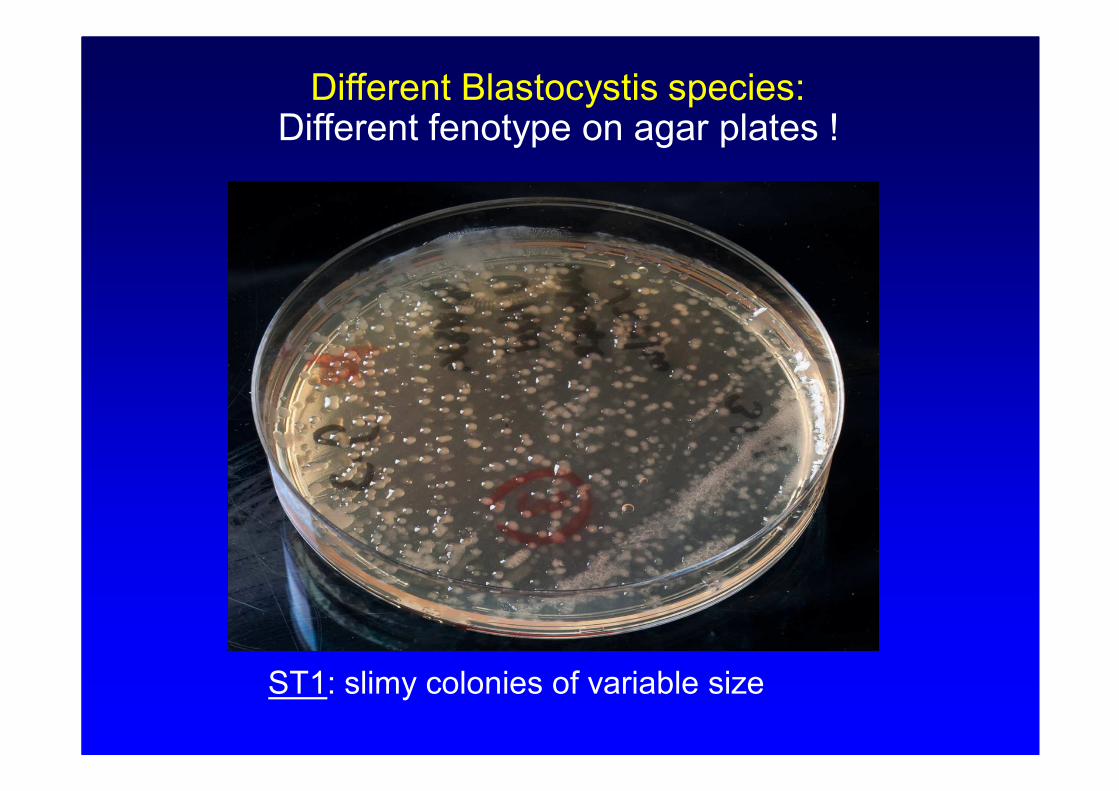
Different Blastocystis species:Different fenotype on agar plates !
ST1: slimy colonies of variable size
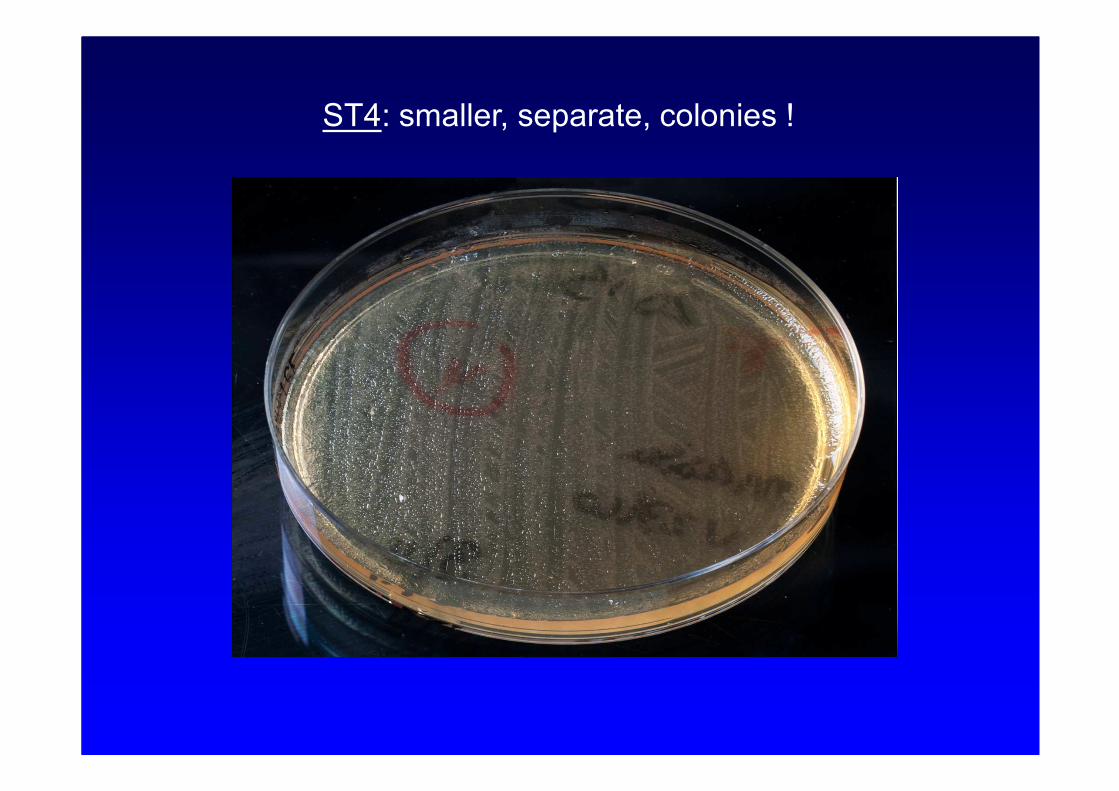
ST4: smaller, separate, colonies !
End
Microsporidia
from an incidental to highly prevalent human pathogens….
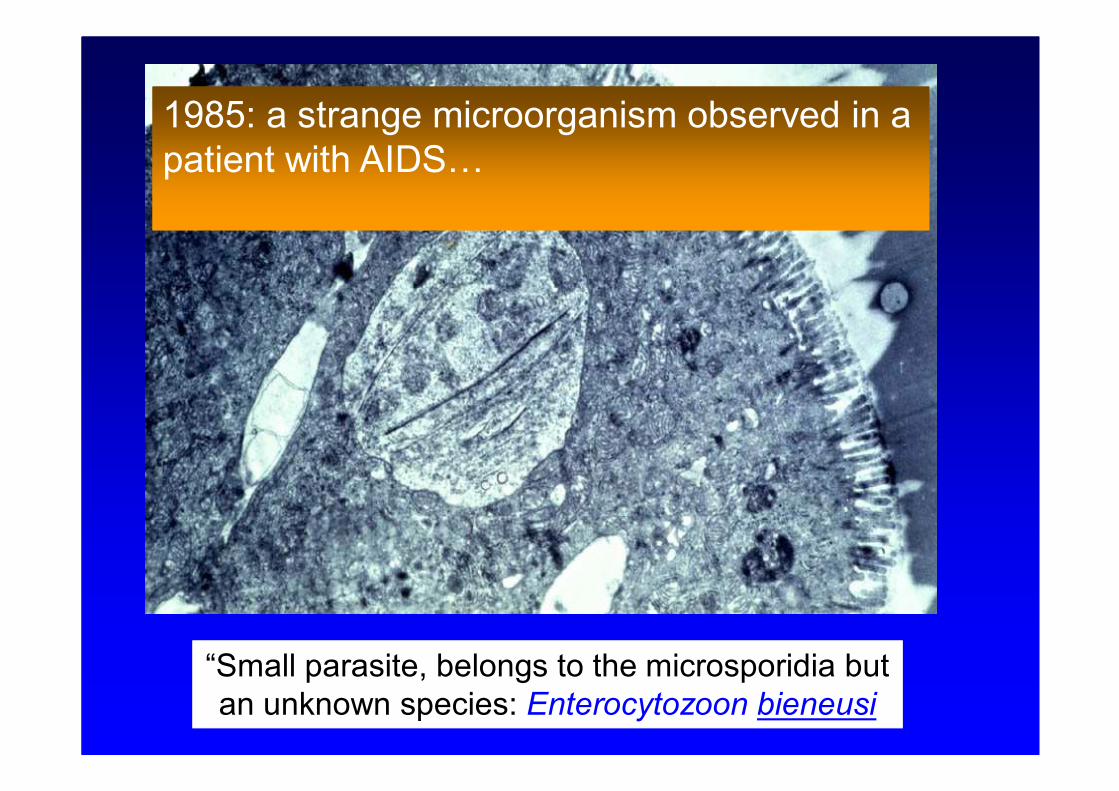
“Small parasite, belongs to the microsporidia but
an unknown species: Enterocytozoon bieneusi
1985: a strange microorganism observed in a
patient with AIDS…
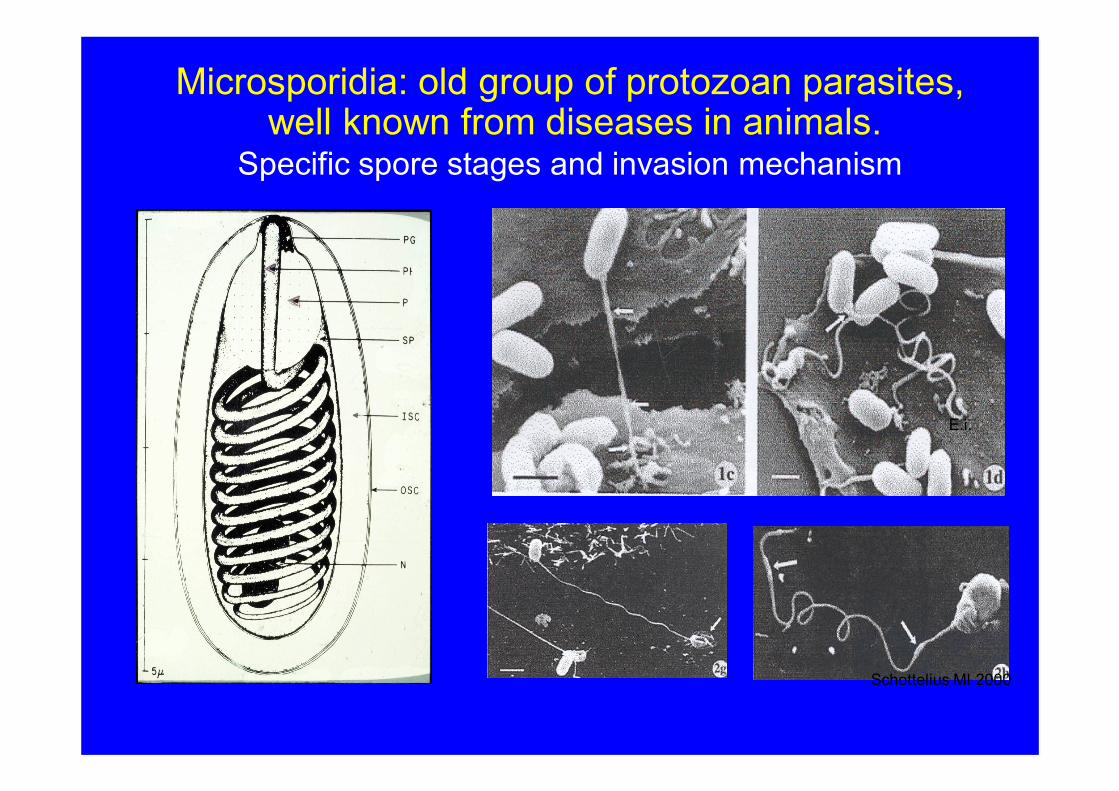
Microsporidia: old group of protozoan parasites, well known from diseases in animals.
Specific spore stages and invasion mechanism
Schottelius MI 2000
E.i.
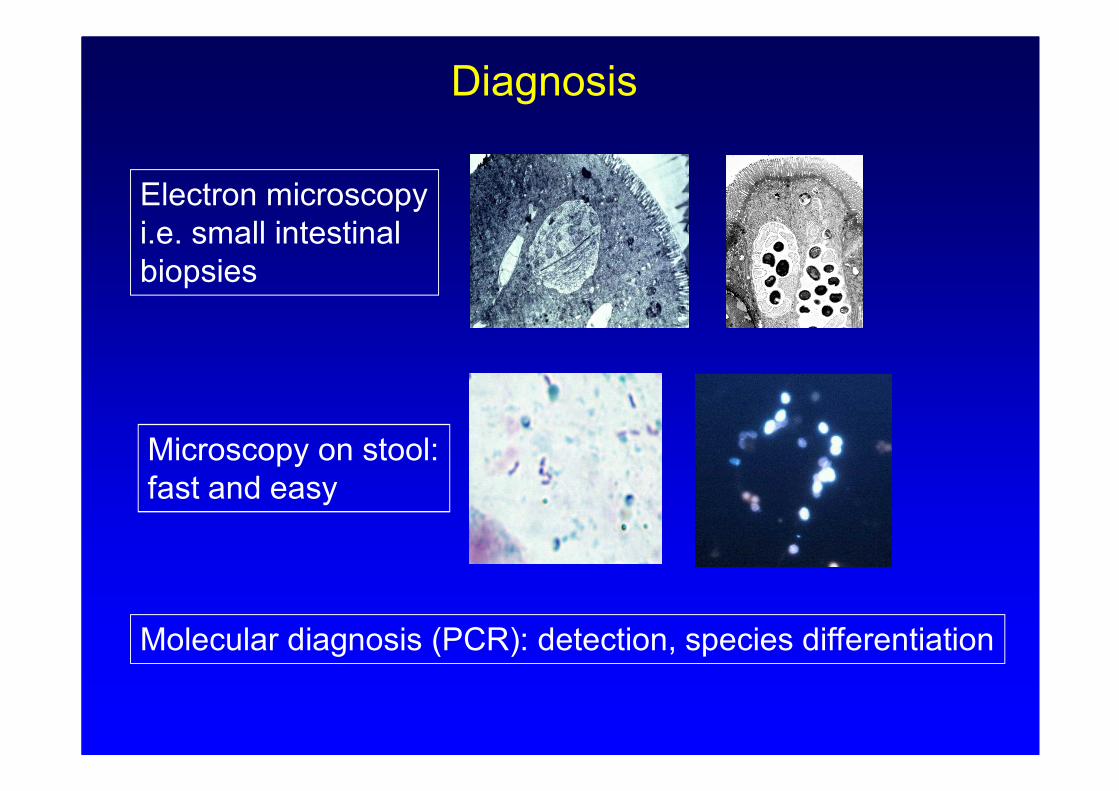
Diagnosis
Microscopy on stool:
fast and easy
Molecular diagnosis (PCR): detection, species differentiation
Electron microscopy
i.e. small intestinal
biopsies
• chronic diarrhea
• cholangiopathy
• rhinosinusitis
Treatment difficult: fumagilin
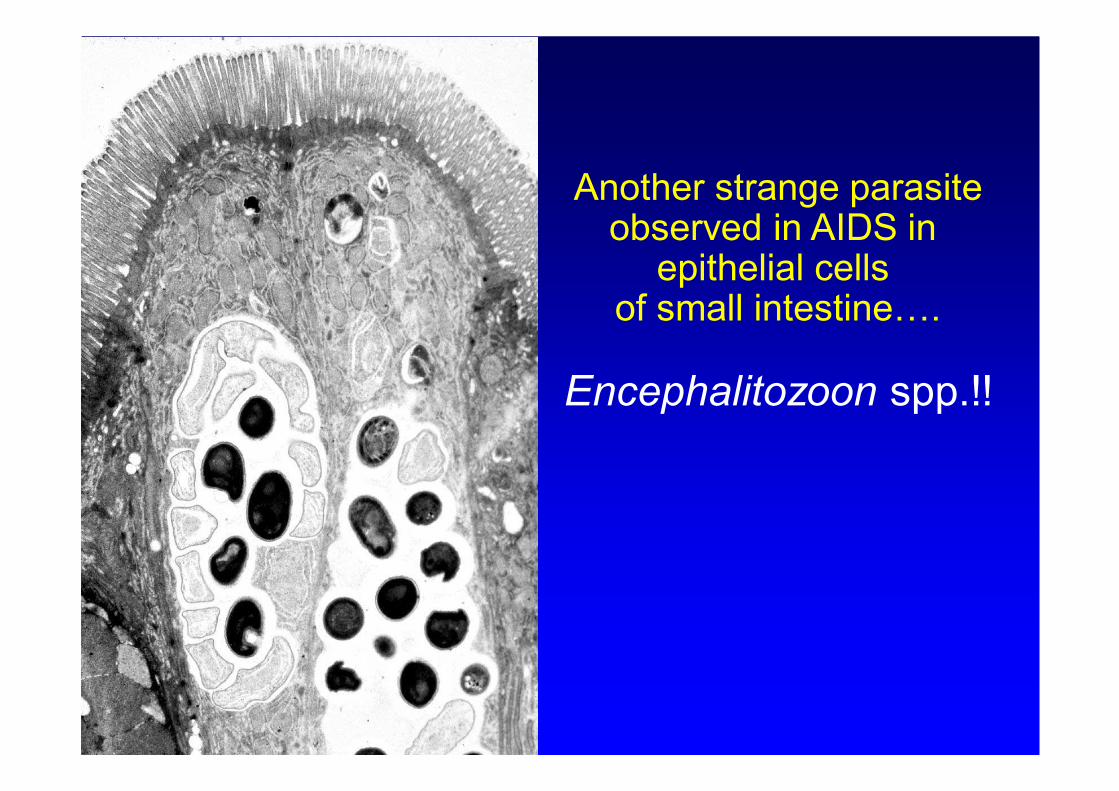
Another strange parasite observed in AIDS in
epithelial cells of small intestine….
Encephalitozoon spp.!!
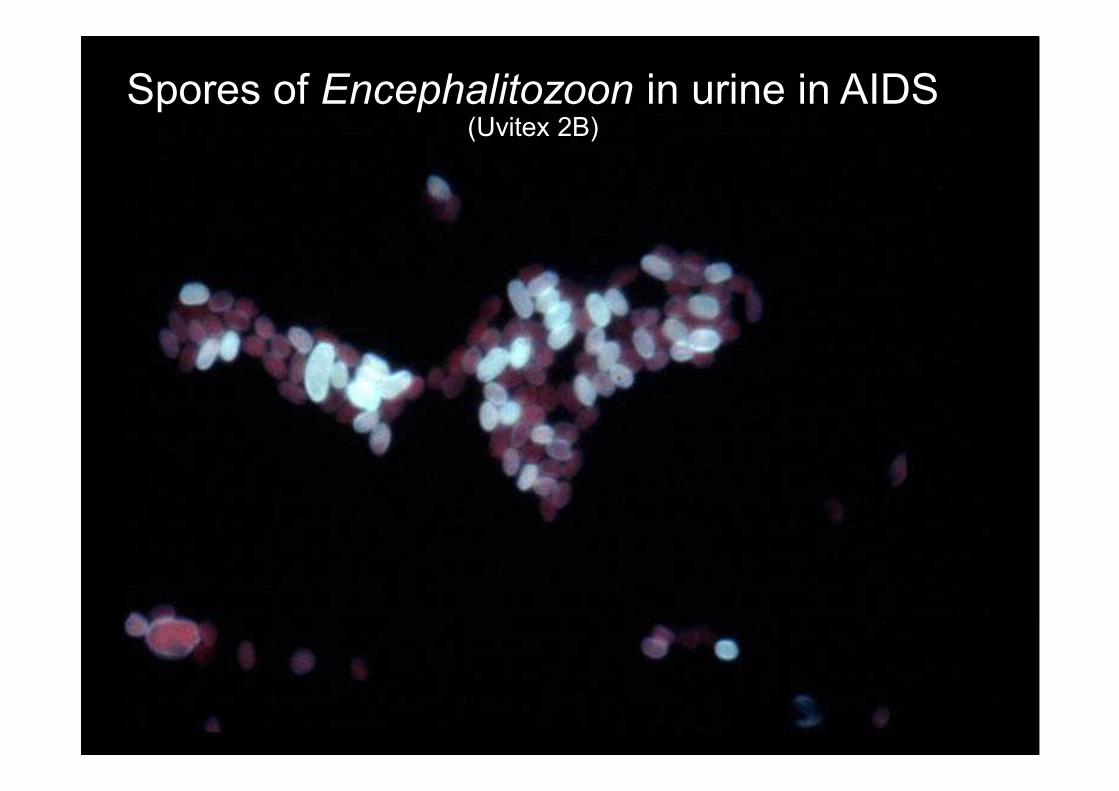
Spores of Encephalitozoon in urine in AIDS(Uvitex 2B)
Pathology due to Encephalitozoon infections in
AIDS: involvement of multiple organs
● encephalitis
● diarrhea
● hepatitis
● nephritis
● keratoconjunctivitis
Treatment of Encephalitozoon species
• Albendazole 400 mg twice a day for 4 weeks
– Rapid disappearance of spores from body fluids
– Prolonged treatment necessary to prevent
relapses
Microsporidiosis in immunosuppression other than AIDS
● Solid organ tranplantation (kidney, heart- long and liver)
● Bone marrow transplant recipiënts.
E. bienusi: prolonged diarrhea
Encephalitozoon spp.: multipe organ involvement
Antibodies to microsporidia frequently present in general Dutch and French population (7%)!
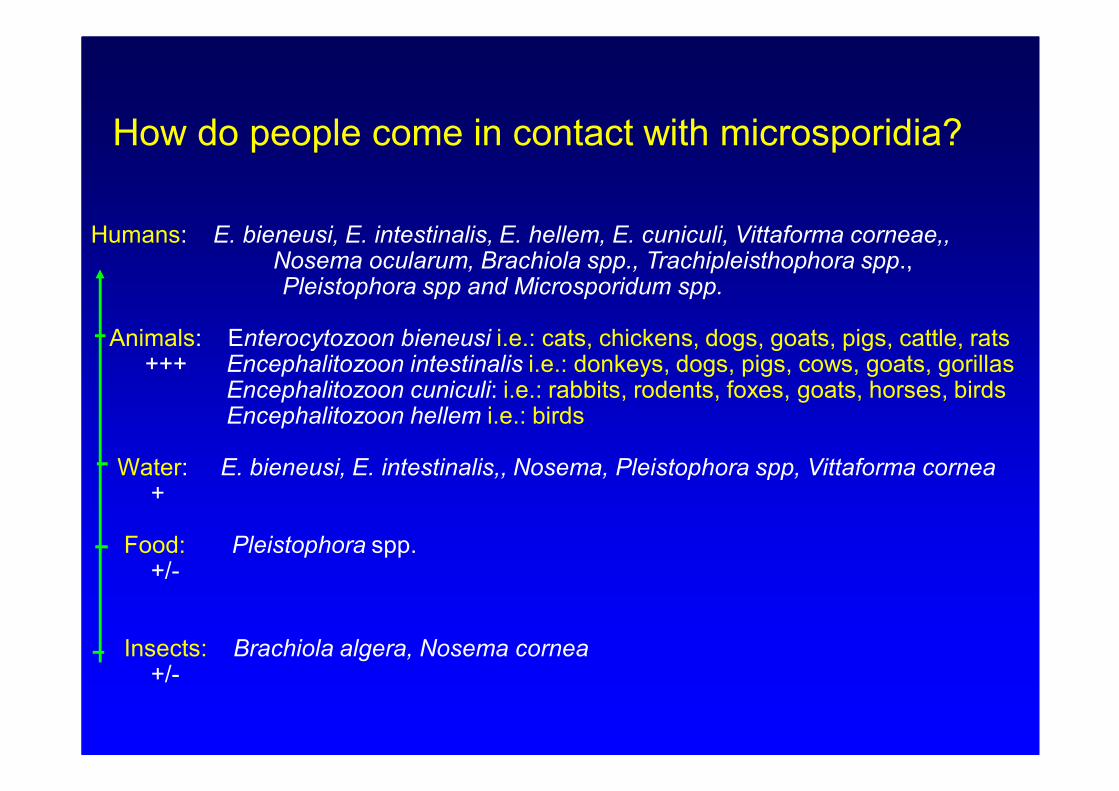
How do people come in contact with microsporidia?
Humans: E. bieneusi, E. intestinalis, E. hellem, E. cuniculi, Vittaforma corneae,, Nosema ocularum, Brachiola spp., Trachipleisthophora spp., Pleistophora spp and Microsporidum spp.
Animals: Enterocytozoon bieneusi i.e.: cats, chickens, dogs, goats, pigs, cattle, rats+++ Encephalitozoon intestinalis i.e.: donkeys, dogs, pigs, cows, goats, gorillas
Encephalitozoon cuniculi: i.e.: rabbits, rodents, foxes, goats, horses, birdsEncephalitozoon hellem i.e.: birds
Water: E. bieneusi, E. intestinalis,, Nosema, Pleistophora spp, Vittaforma cornea+
Food: Pleistophora spp.+/-
Insects: Brachiola algera, Nosema cornea+/-
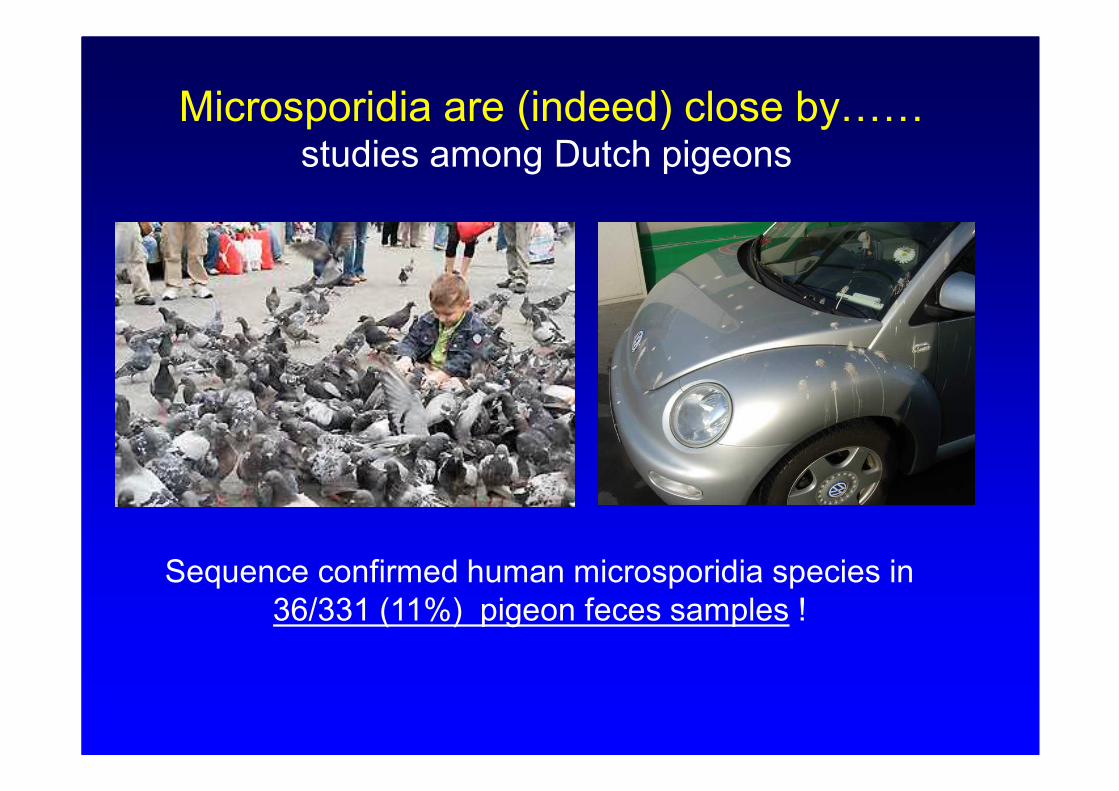
Microsporidia are (indeed) close by……studies among Dutch pigeons
Sequence confirmed human microsporidia species in
36/331 (11%) pigeon feces samples !
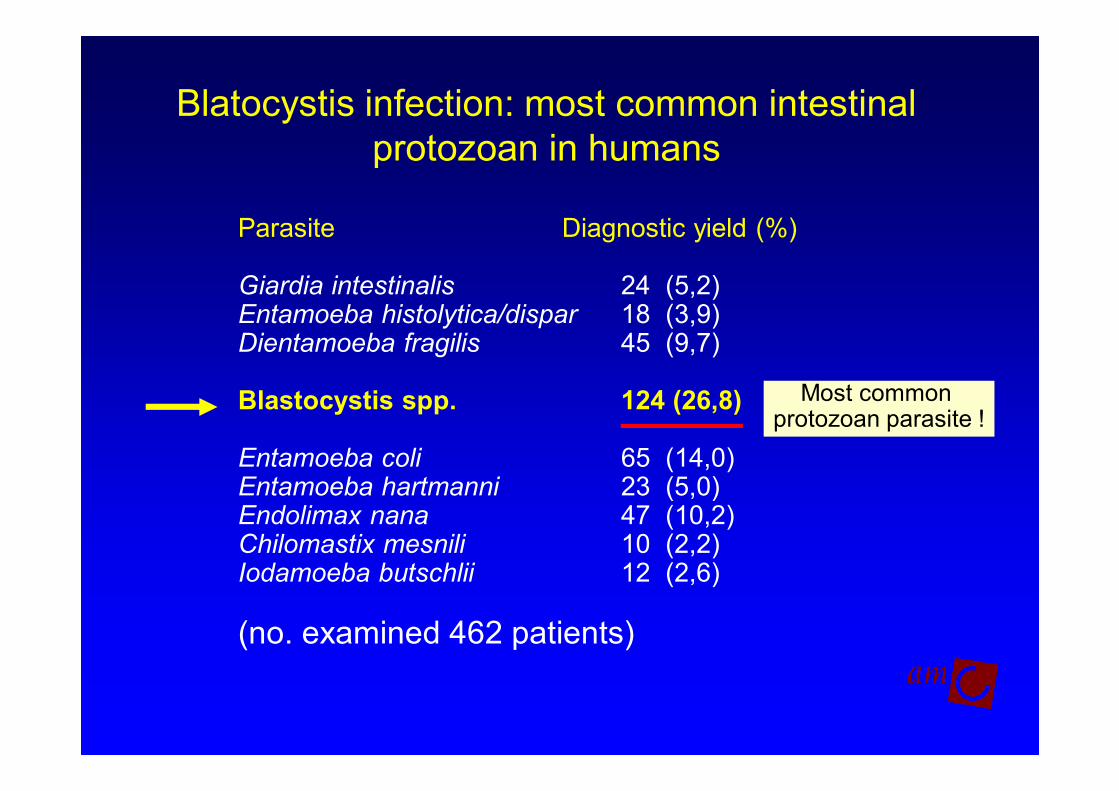
Blatocystis infection: most common intestinal
protozoan in humans
Parasite Diagnostic yield (%)
Giardia intestinalis 24 (5,2) Entamoeba histolytica/dispar 18 (3,9)Dientamoeba fragilis 45 (9,7)
Blastocystis spp. 124 (26,8)
Entamoeba coli 65 (14,0)Entamoeba hartmanni 23 (5,0)Endolimax nana 47 (10,2)Chilomastix mesnili 10 (2,2)Iodamoeba butschlii 12 (2,6)
(no. examined 462 patients)
Most common protozoan parasite !
Culture of Blastocystis spp. in liquid media
Growth with intestinal bacteria:
difficult to estimate effectiveness of antibiotics!
. . . .. . . .
… . . . .
. . …
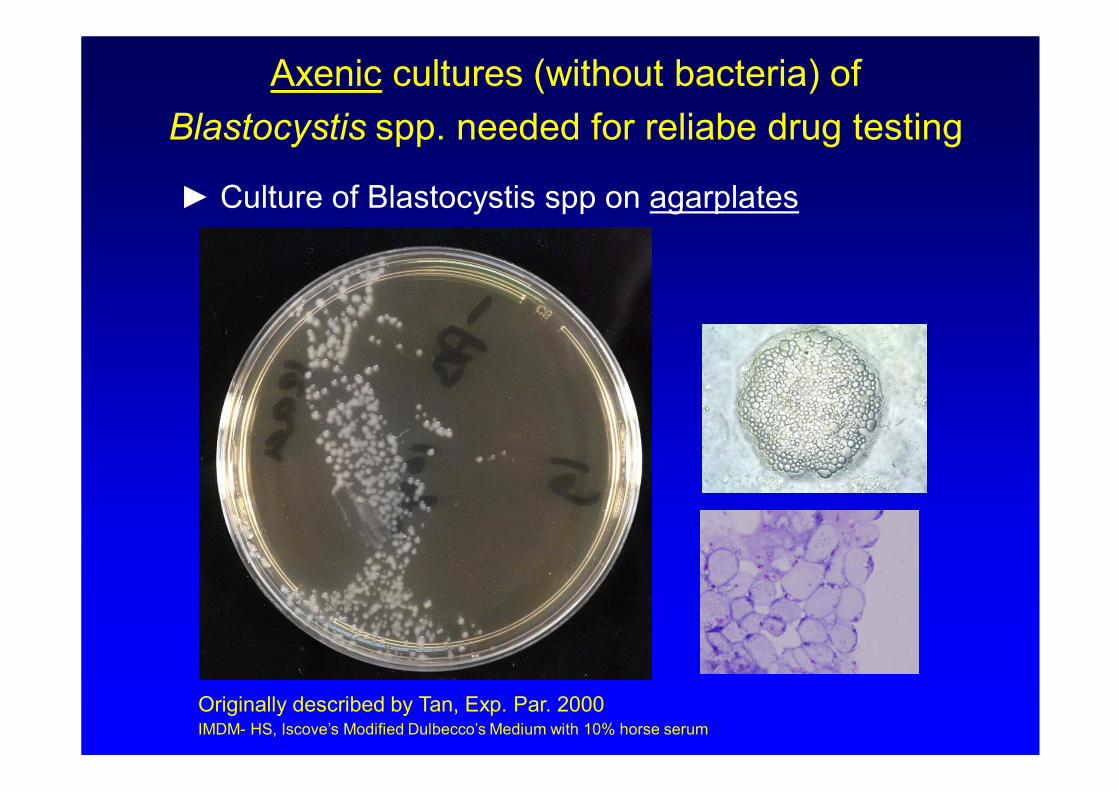
Axenic cultures (without bacteria) of
Blastocystis spp. needed for reliabe drug testing
Originally described by Tan, Exp. Par. 2000IMDM- HS, Iscove’s Modified Dulbecco’s Medium with 10% horse serum
► Culture of Blastocystis spp on agarplates
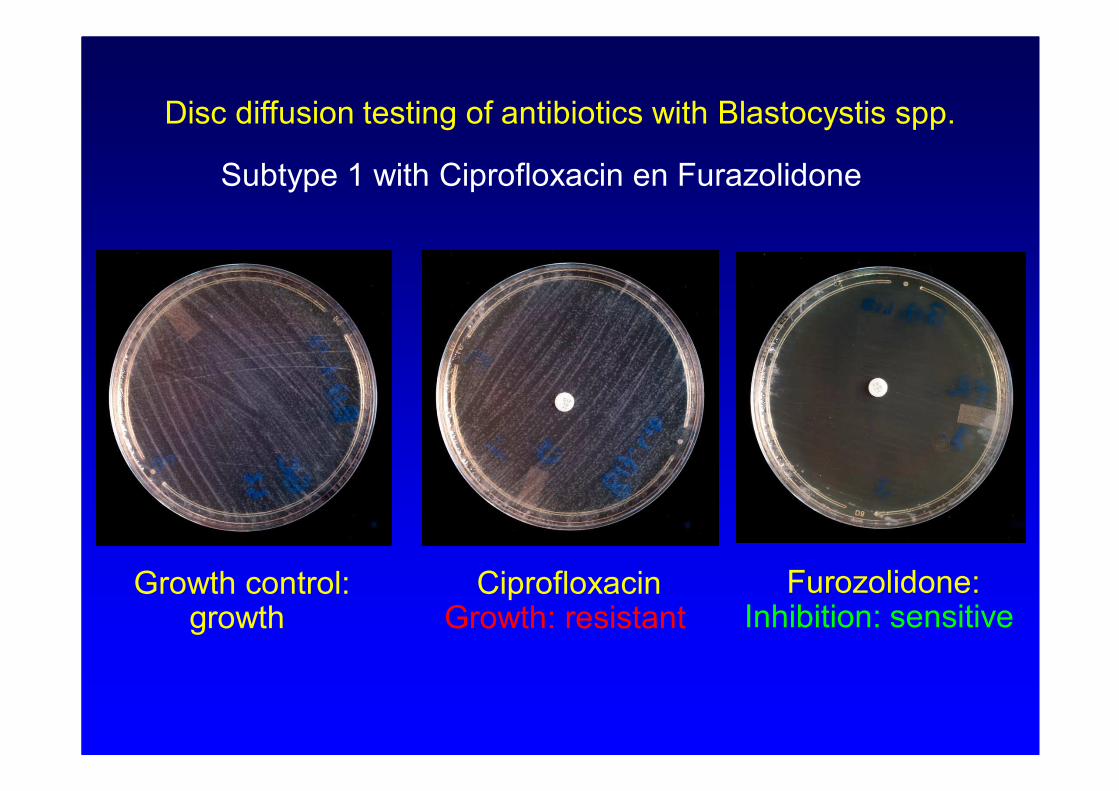
Disc diffusion testing of antibiotics with Blastocystis spp.
Subtype 1 with Ciprofloxacin en Furazolidone
Growth control:growth
CiprofloxacinGrowth: resistant
Furozolidone:Inhibition: sensitive
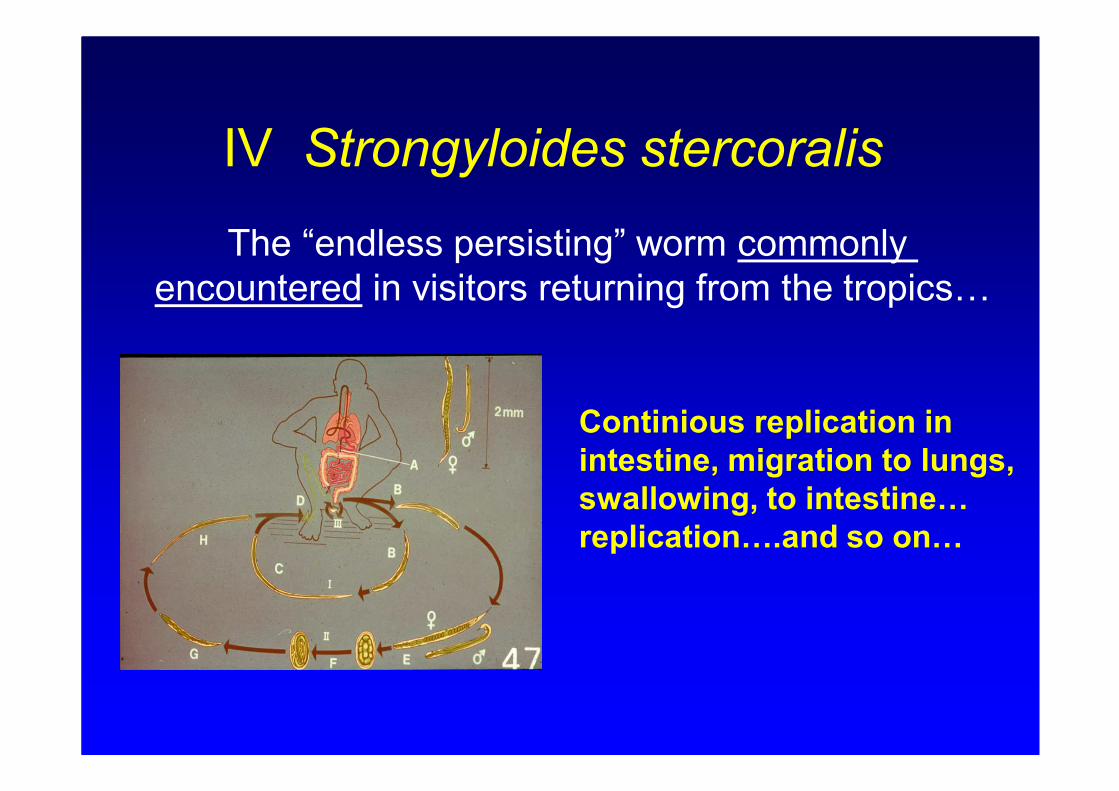
IV Strongyloides stercoralis
The “endless persisting” worm commonly
encountered in visitors returning from the tropics…
Continious replication in
intestine, migration to lungs,
swallowing, to intestine…
replication….and so on…
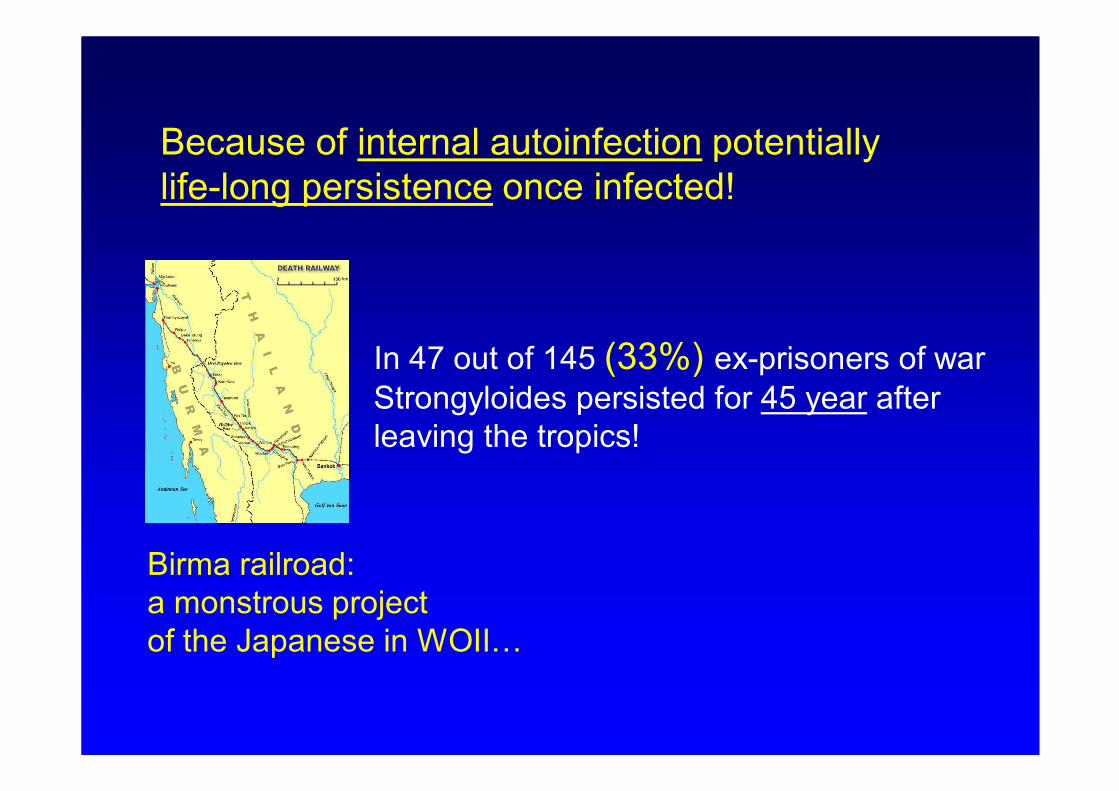
Birma railroad:
a monstrous project
of the Japanese in WOII…
In 47 out of 145 (33%) ex-prisoners of war
Strongyloides persisted for 45 year after
leaving the tropics!
Because of internal autoinfection potentially
life-long persistence once infected!
Prevalence
● Present in most tropical and subtropical countries
● Especially also South America (Surinam!) and
South East Asia (Indonesia).
● Also in rural areas Spain, Italia, Poland, Romania
Occasionally in Turkey
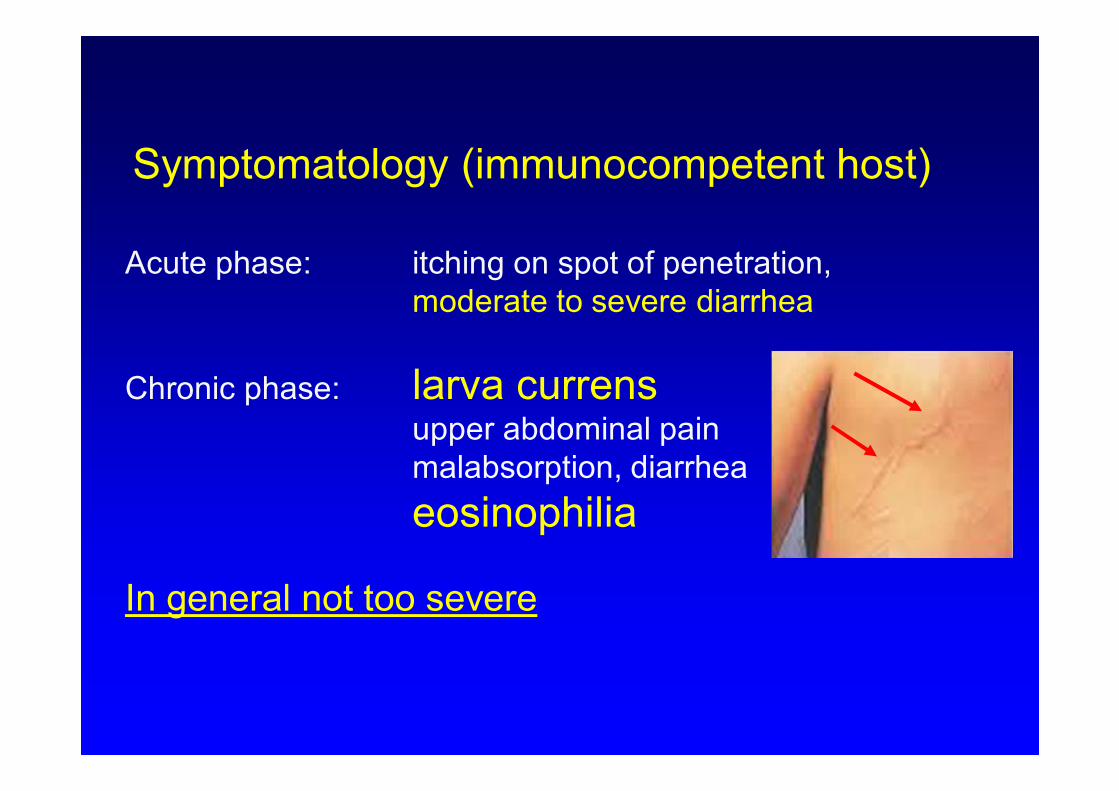
Symptomatology (immunocompetent host)
Acute phase: itching on spot of penetration,
moderate to severe diarrhea
Chronic phase: larva currensupper abdominal pain
malabsorption, diarrhea
eosinophilia
In general not too severe
The major complication of infection with
Strongyloides stercoralis infection
hyperinfection syndrome
Immunosuppression results in massive
proliferation of Strongyloides stercoralis!
Without prompt treatment: lethal condition!
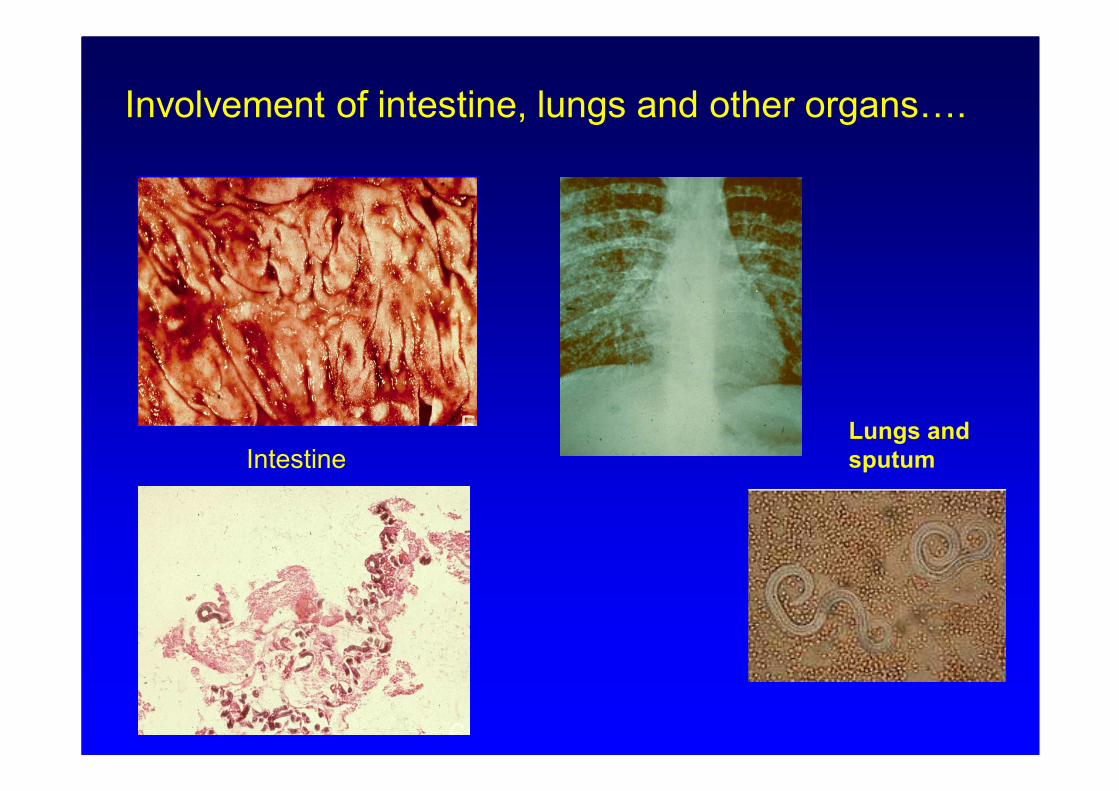
Involvement of intestine, lungs and other organs….
IntestineLungs and
sputum
Patients at risk for hyperinfection syndrome:
- administration of corticosteroids (even 6-17 days courses)
- hematopoietic stem cell transplantation
- organ transplantation
- cytotoxic drugs
- Human T-lymphotropic virus type I (HTLV-I) infection
Prevention of hyperinfection syndrome
Anyone at risk: serodiagnosis with specific IgG
In case of a positive serological result: treatment with
ivermetine 0,2 mg/kg body weight daily, 2 days
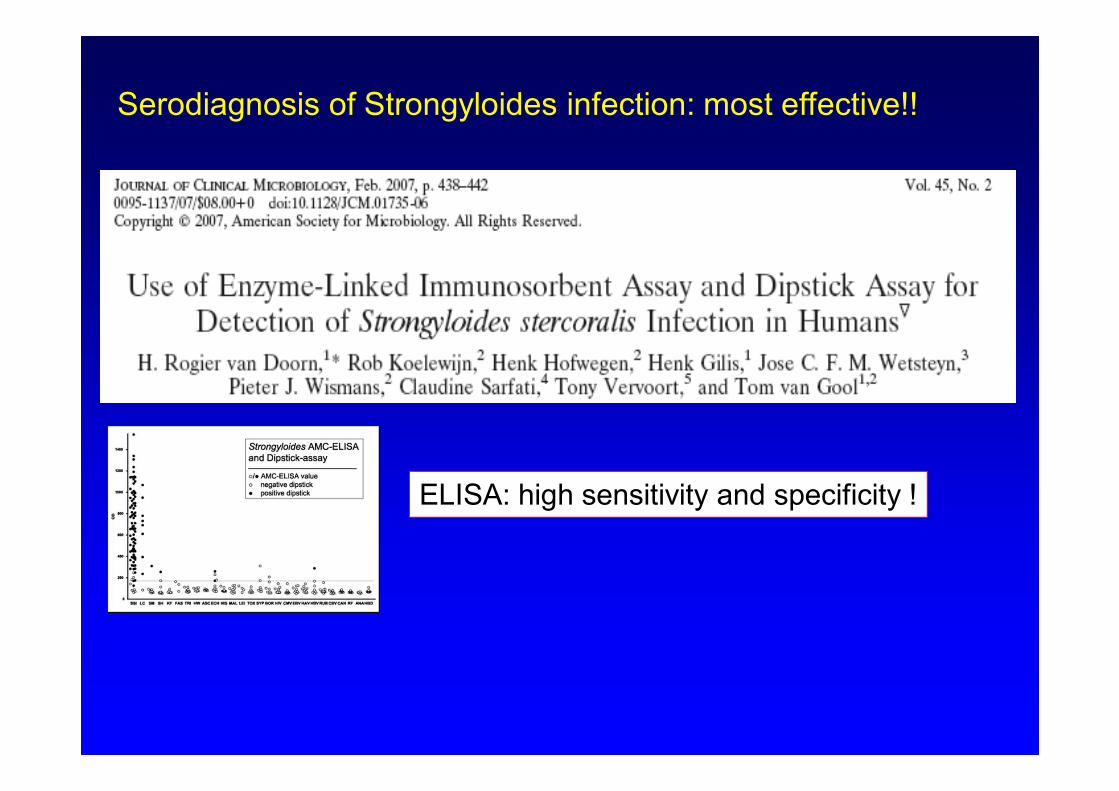
Serodiagnosis of Strongyloides infection: most effective!!
ELISA: high sensitivity and specificity !
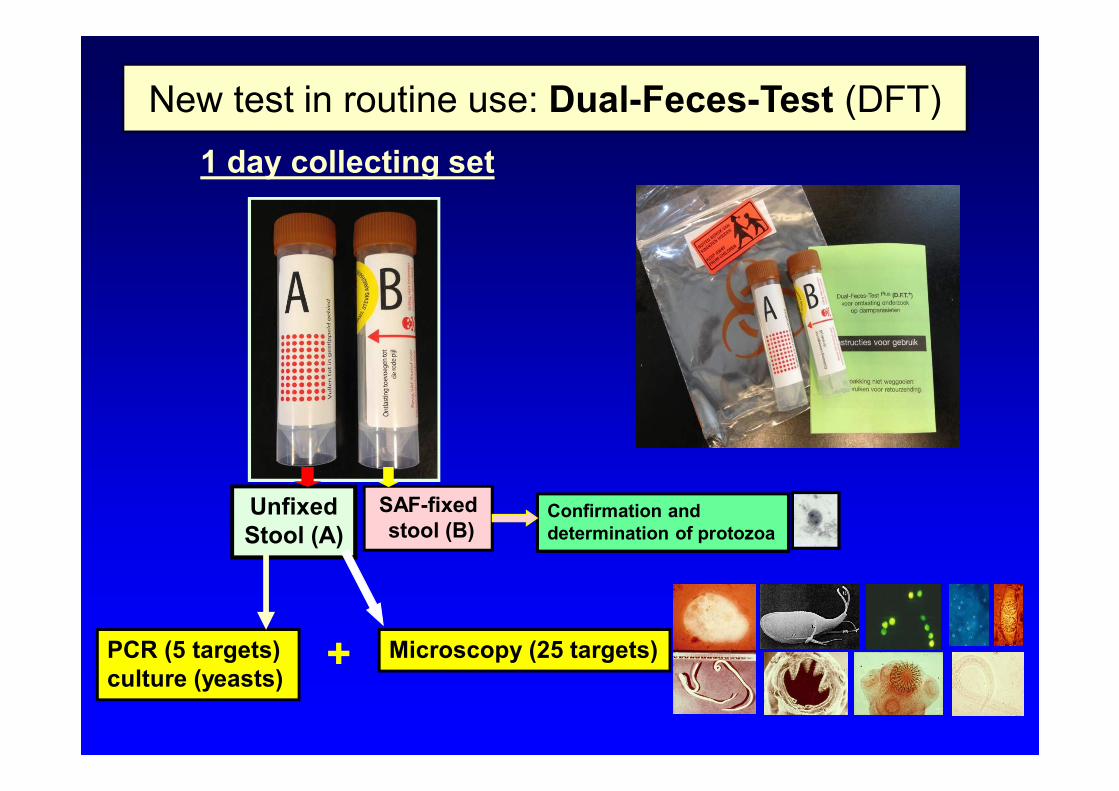
New test in routine use: Dual-Feces-Test (DFT)
1 day collecting set
Unfixed
Stool (A)
SAF-fixed
stool (B)
PCR (5 targets)
culture (yeasts)
Microscopy (25 targets)
Confirmation and
determination of protozoa
+
Op empirisch gronden werken met geneesmiddelen en
combinaties daarvan die in vivo bewezen effectiviteit hebben
tegen Giardia.
Meest gebruikt:
•Metronidazol
•Tinidazol
•Albendazol
•Paromomycine
•Nitazoxanide
•Meparicine
Combinaties: oa tinidazol met albendazol
Beleid behandeling
refractaire giardiasis
1: 1d tinidazol , 5d albendazol, 1d tinidazol“ We have chosen this regimen on the basis of the small trial performed by Cacopardo et al. which demonstrated the
superior efficacy of nitroimidazole–albendazole combination therapy over albendazole alone. Furthermore, in our
own experience, 60% of patients with refractory disease are cured with this combination”.
2: 3dd 100mg 3-5 (7) d Mepacrine
3: Aldendazol 2dd 400mg 14 d….(?)
-> Controle diagnostiek direct (tot 1 week) na einde
behandeling!
Carter et al 2017