Embed Size (px)
Citation preview

Intra-Aortic Balloon Pumps: A Review for Cardiologists
Quinn Capers, IV, MD, FACC, FSCAIDivision of Cardiovascular MedicineThe Ohio State University Medical
Center

IABP: Definition
40 cc volume, cylindrical balloon
Advanced from femoral artery into aorta
Usually percutaneously (Seldinger technique), with a sheath (6.5-10.5)

IABP: Definition
Attached via gas and arterial pressure tubing to portable control module
Inflated with inert gas immediately at aortic valve closure
Actively deflated immediately prior to systole

4
IABP inflates with aortic valve closure:Provides pressurized pulse of blood against closed aortic valve, increasing coronary perfusion
IABP deflates immediately prior to aortic valve opening:Reduces LV afterload

IABP: Physiology
Inflation at aortic valve closure: Increases aortic diastolic blood pressure Increases diastolic coronary perfusion Net neutral effect on cerebral perfusion Increases C.O./“runoff” to subdiaphragmatic organs
Deflation prior to systole: Reduces impedance to LV ejection (afterload) Reduces myocardial oxygen consumption

IABP: Physiology
2 main beneficial effects:
1) Augmented coronary perfusion
2) Reduced LV afterload/Increased CO

IABP: Physiology
2 main beneficial effects:
1) Augmented coronary perfusion Only in normal coronary arteries No augmentation beyond severe stenoses pre PCI Augmentation beyond severe stenoses post PCI
2) Reduced LV afterload/Increased CO

IABP: Physiology
2 main beneficial effects:
1) Augmented coronary perfusion
2) Reduced LV afterload/Increased CO Most important of 2 main effects when severe coronary
stenoses present

9
Cardiogenic shock Unstable AMI pt Prior to hi risk PCI Prior to hi risk CABG Refractory CHF Refractory VT/VF Severe MR Refractory angina
“Rescue” after failed PCI going to CABG
Bridge to heart txp
IABP: Indications

10
Absolute
Known severe aortic pathology (dissxn, ulcer, mobile plaques)
Significant AI Patient refusal
Relative
Severe PVD AAA Mild AI
IABP: Contraindications

IABP: Current Practice
Ferguson. JACC 2001. Registry, 6/96-8/00: 16, 909 pts in 203 ctrs Indications:
20.6% high risk cath/PCI 18.8% cardiogenic shock 16.1% weaning from CPB 13% preop CABG, high risk or
unstable pt 12.3% refractory USA

IABP: Complications
Ferguson. JACC 2001. Benchmark Registry. 16, 909 pts, 203 ctrs Complications:
2.9% Limb ischemia 2.4% Access site bleeding 1% Balloon leak 0.05% Death attributable to IABP

IABP: ComplicationsRisk Factors Odds Ratios for Major complications with IABP
therapy:
PVD: 2.0 Female Gender: 1.7 Small BSA: 1.5 Advanced age: 1.3
(Little Old Ladies!!!)

IABP Insertion: Methods
Choose groin with strongest pulse
Consider iliac angiogram
Document pedal pulses before IABP inserted

IABP Insertion: Methods
Note that sheath is not mandatory
Advantage: IABP passage may be less traumatic
Disadvantage: Bigger hole, ? more limb ischemia

IABP Insertion: Methods
Advance IABP over wire under fluoro
Distal (cephalad) marker placed at carina(Caudad to L SC artery)
Aspirate blood from lumen of IABP
Hook up “bubble free” to fluid filled pressure tubing

IABP Insertion: Methods
Connect gas line and fill IABP
Begin pumping 1:2 under fluoro
Ensure full expansion, no kinking, IABP not in iliac artery
Examine pressure wave forms

18

19

20

21

22

23

24

25

26

IABP: Essential Questions
Anecdotally, we think it is a beneficial in cardiogenic shock and high risk coronary revascularization.
1. Do we have randomized data that it is beneficial in high risk PCI?
2. If IABP is beneficial in high risk PCI, does the timing of IABP placement matter? (i.e., prior to PCI, during PCI after complications arise, after PCI?)
3. Is anticoagulation necessary when IABPs are in place?

IABP: To Anticoagulate or Not?
J Zheijiang Univ Sci 2003 Sep-Oct; 4 (5): 607-611 153 pts with IABP x 48 hrs randomized to IV heparin
or placebo No difference in limb ischemia, clot on balloon surface
upon removal Increased major and minor bleeding in heparin group

Acute Card Care. 2008The role of heparin anticoagulation during intra-aortic balloon counterpulsation in the coronary care unit.
Cooper HA1, Thompson E, Panza JA.
Universal Heparin (n=102) vs Strategic Heparin (n=150) in IABP pts
100% of UH pts and 47% of SH pts received Heparin
Major bleeding 10.8% vs 3.2% (p<0.05) in Universal vs Strategic group
Bleeding was non-access site related

J Card Surg. 2012 Heparin-free management of intra-aortic balloon pump after cardiac surgery.Kogan A1, Preisman S, Sternik L, Orlov B, Spiegelstein D, Hod H, Malachy A, Levin S, Raanani E.
203 pts requiring IABP post-CABG
None treated with Heparin
IABP duration: < 24 hr in 81 pts, > 24 hrs in 122 pts
No major bleeding complications in any pts

IABP: To Anticoagulate or Not?
No recommendations by manufacturers
Generally not thought to be necessary if pumping 1:1
Reasonable if during a long wean while pumping 1:2 or 1:3

IABP in High-Risk PCIIs it Useful? IABP placed for PCI
Brodie AJC 1999 Cardiac arrest decreased by 52%
O’Murchu JACC 1995 Decrease MI in rotational atherectomy
Ohman Circ 1994 Decreased reocclusion of IRA in MI pts Decreased MACE

IABP in High-Risk PCI
IABP placed after PCI
Van’t Hof Eur Heart J 1999 No benefit
PAMI II JACC 1997 No benefit

IABP in High-Risk PCI
What if it’s placed before the high risk PCI?

IABP in High-Risk PCI
Mishra AJC 2006 300 high risk pts, 69 had IABP inserted
prophylactically
Remaining pts had sheath inserted, leads on chest, IABP in the room, “on standby”
46 pts needed “rescue” IABP

IABP in High-Risk PCI
Prophylactic (69) “Rescue” (46)
In hosp death: 0% 22%
MI: 20% 62%
30 day death: 4% 27%
Mishra AJC 2006

IABP in High-Risk PCI
Briguori AHJ 2003 133 pts with LVEF < or = 30%
Prophylactic “Rescue” Shock: 0% 15% MACE: 0% 17%
(MI, CABG, Death)
*Prophylactic pts had more high risk characteristics

IABP in High-Risk PCI
Prophylactic strategy proven superior to “standby” strategy in several studies:
SHOCK trial (Death rate 57% vs 72%)1
GUSTO (MACE rate 47% vs 60%)2
NRMI (MACE rate 49% vs 67%)3
1Hochman Circ 1995
2Topol JACC 1995
3Circ 2003

IABP in High-Risk PCI?
Briguori AHJ 2006 219 pts with unprotected LM lesions
Prophylactic (69) “Rescue” (150) Shock: 0% 8% MACE: 1.5% 9.5%
*Prophylactic pts had more high risk characteristics

IABP in High-Risk PCI
A strategy of prophylactic placement of IABP before high risk PCI appears to be superior to a “rescue” strategy
If you think you need it, you probably do!

41Date of download: 7/18/2013
Copyright © 2012 American Medical Association. All rights reserved.
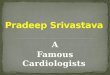
From: Elective Intra-aortic Balloon Counterpulsation During High-Risk Percutaneous Coronary Intervention: A Randomized Controlled Trial
JAMA. 2010;304(8):867-874. doi:10.1001/jama.2010.1190
Mortality at 6 months was numerically lower in the elective intra-aortic balloon pump (IABP) group than in the no planned IABP group, although this was not statistically significant (4.6% vs 7.4%, P = .32 by the χ2 test).
Figure Legend:

N Engl J Med. 2012 Oct 4;367(14):1287-96. doi: 10.1056/NEJMoa1208410. Epub 2012 Aug 26.Intraaortic balloon support for myocardial infarction with cardiogenic shock.Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Böhm M, Ebelt H, Schneider S, Schuler G, Werdan K; IABP-SHOCK II Trial Investigators.
600 pts with STEMI complicating cardiogenic shock
Randomized to IABP vs no IABP
Primary endpoint: Mortality

43
“there was no significant difference in mortality between the 37 patients (13.4%) in whom the balloon pump was inserted before revascularization and the240 patients (86.6%) in whom the balloon pump was inserted after revascularization”
N Engl J Med. 2012 Oct 4;367(14):1287-96. doi: 10.1056/NEJMoa1208410. Epub 2012 Aug 26.Intraaortic balloon support for myocardial infarction with cardiogenic shock.Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Böhm M, Ebelt H, Schneider S, Schuler G, Werdan K; IABP-SHOCK II Trial Investigators.
“In this large, randomized trial involving patients with cardiogenic shock complicating acute myocardial infarction, for whom early revascularization was planned, intraaortic balloon pump support did not reduce 30-day mortality.”

44
“In the group assigned to elective IABP treatment, the balloon catheter is inserted at the start of the procedure, before coronary intervention.”—BCIS trial investigators
BCIS-1 long term follow up vs IABP-Shock II(What’s the difference?)
“there was no significant difference in mortality between the 37 patients (13.4%) in whom the balloon pump was inserted before revascularization and the 240 patients (86.6%) in whom the balloon pump was inserted after revascularization”---IABP Shock II investigators

IABP: Important Questions:
1) Do we have randomized data?
2) Does it matter if they are placed prior to or after PCI?
3) Is anticoagulation necessary?
Yes, but mostly anecdotal and registry
?
No, if </= 48hrs

Impella
Percutaneous LVAD
14 Fr sheath
Increases cardiac output (2.5 L/min) & unloads LV
Pressure Lumen
Motor
Blood outlet
Blood Inlet

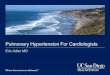
PROTECT II MACCE**PROTECT II MACCE**
47
Per Protocol Population, N=426Per Protocol Population, N=426
Log rank test, p=0.04Log rank test, p=0.04
Death, Stroke, MI,Death, Stroke, MI,Repeat revasc.Repeat revasc. IABPIABP
IMPELLAIMPELLA

48
IABP: Post-Test
• Iliac artery atherosclerosis is an absolute contraindication for placing an IABP. True or False?
• There is no evidence that systemic anticoagulation is indicated in patients with an indwelling IABP. True or False?
• The most common complication of IABPs is related to balloon rupture/leak. True or False?

49
IABP: Post-Test
• In patients with multiple, critical coronary stenoses and refractory angina, IABPs are useful to decrease angina. In such situations the main mechanism of benefit is:
• LV afterload reduction• Increased coronary perfusion• Increased peripheral arterial blood pressure• Increased peripheral arterial “runoff”

50
IABP: Post-Test
• You are about to perform a complex PCI in a patient with severe LMCA disease and severe LV dysfunction? You think you may need a balloon pump. How will you proceed?
• Placing the IABP prior to PCI • Placing the IABP after PCI• Having the IABP “ready to go” (in the room, sheath
in groin, IABP EKG leads on pt) in case the patient “crashes”

51
IABP: Post-Test
• Based on currently available evidence, which of the following pts would you predict to have the highest risk for a complication of IABP placement?:
• A morbidly obese (350#) man with diabetes• A 65 year old man with femoral bruits• A 90 year old woman that weighs 90 # and suffers
from severe claudication• A 70 year old man with a small (3.5 cm) AAA

52
IABP: Post-Test
Analyze this aortic pressure waveform in a pt with an IABP in place. What is the problem? How do you fix it?

Conclusions
IABPs are extremely useful in stabilizing pts with complicated cardiac disease
Risk factors for complications with IABPs are: female sex, PVD, small BSA, age
Troubleshooting with waveform analysis is critical, and is just as important as knowing how to insert an IABP

Conclusions
Prophylactic insertion of an IABP for hemodynamic support in high risk PCI pts may be superior to a “rescue” strategy
Controversy has arisen as to the utility of IABPs, but registry data, randomized data, and anecdotal data can be quoted to support their benefit.
More studies needed, especially re: impact of timing of placement