Embed Size (px)
Citation preview

“WHAT IS REAL AND WHAT IS NOT”
A THERAPEUTIC APPROACH TO PSYCHOSIS THAT TAKES EXPERIENCE
SERIOUSLY AND UNDERMINES STIGMA
Isabel ClarkeConsultant Clinical Psychologist

Moving on from the Illness Model
The illness model has the virtues of certainty and protectiveness
BUT Inadequate reflection of what is happening
Leaves out the universality of the other way of knowing
Leaves out or marginalizes the effects of life events, trauma and adversity
It does not encourage psychotherapeutic approaches – only marginally relevant.
It is damaging to mental health recovery.

The Blight of Stigma
Biological v. Social constructions of psychosis: Read, Mosher & Bentall 2004
Role of Trauma and adversity – e.g. Varese et al meta-analysis 2012
The self = work in progress Social Rank Theory (Gilbert 1992, Gilbert & Allan
1998). ‘Sealing over’ – effect on Recovery Brett, Heriot-Maitland, Peters et al - effect of how
experiences are construed. Social messages – epidemiological research. Meaning – The Hearing Voices approach

A Clinical Model based on ICS
When Emotion Mind/Implicational does not mesh properly with Reasonable Mind/Propositional
A different quality of experience results Anomalous experiences are accessible The everyday world becomes less
important, less graspable Might be frightening and disorienting;
might be fine in the short term A problem when the person becomes
stuck This is a universal potential given the
‘right’ conditions

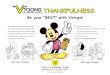
States of Mind Diagram. Applied to Psychosis
REASONABLEMIND – SHAREDREALITY
EMOTIONMIND – UNSHAREDREALITY
IN THE PRESENTIN CONTROL
WISEMINDIn touch with both
Reasonable Mind Memory
Emotion Mind Memory

A therapeutic approach using this model
Validate the experience as their experience Validate the emotion (as opposed to ‘the
story’) Sit lightly to explanations – all explanations,
including medical and CBT ones! Model sitting with uncertainty, recognizing
mystery ‘Shared’ and ‘Unshared’ reality – a way of
talking about this Helping the person to take control of their
‘unshared reality’ is key – how to close off openness to invasion – from within or without

The “What is Real” Approach
Introduces and normalizes “Unshared Reality”
Balance between vulnerability and potential – positive side of high schizotypy
Practical ways to manage the threshold between the two 2 “realities”
Motivation to use coping to do this - counter giving up and opting out
Individual formulation based on coping strategy model – for some

Group Programme:
Openness to Unusual Experiencing
Acknowledging that psychosis feels different
Normalising the difference in quality of experience as well as the continuity
Reference Romme & Escher research Identifying and exploring pros and cons of
‘shared’ and ‘unshared’ reality Sensitivity and openness to anomalous
experience – continuum with normality: Gordon Claridge’s Schizotypy research.
Positive side as well as vulnerability – creativity, spirituality – effect on self esteem

Shared Reality Unshared Reality
Ordinary Clear limits Access to full
memory and learning Precise meanings
available Separation between
people Clear sense of self Emotions moderated
and grounded A logic of ‘Either/Or
Supernatural Unbounded Access to
propositional knowledge/memory is patchy
Suffused with meaning or meaningless
Self: lost in the whole or supremely important
Emotions: swing between extremes or absent
A logic of ‘Both/And’

Understanding and taking charge of the Threshold
Brainstorm the factors leading to vulnerability Lack of sleep, food, stress, isolation Pressure of events – life transitions Effect of past trauma and adversity Drugs, alcohol Spiritual practice – with vulnerability/to excess
Choice – you can take charge – you do not have to shut it down completely
Motivation to use coping strategies in order to take charge

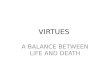
Session 2. The role of Arousal shaded area = anomalous experience/symptoms are more
accessible.
Level of Arousal
Ordinary, alert, concentrated, state of arousal.
Low arousal: hypnagogic; attention drifting etc.
High Arousal - stress

Session 2 cont. DIALECTICAL BEHAVIOUR THERAPY: Linehan’s STATES OF MIND applied
to PSYCHOSIS
reasonable mind
Ordinary thinking
Shared reality.
wiseMind –in touch With both
in the presentin control
emotion mind
or open to other ways
of experiencing
Non-shared reality
Shared and Non-shared Reality
Ways of coping suggested by this approach – management of arousal and distraction.

Ways of taking charge and making sense
Motivation to take charge – David Bowie e.g. Arousal Management – up and down Grounding Mindfulness - Haddock research
on Focusing and Distraction. How do people make sense of their
experiences? Discussion of different ways of making sense of them.
Clue: what was happening when they first started?
Mike Jackson’s Problem Solving idea Positive potential sketched in

Grounding Mindfulness
Aim: To bring yourself 100% into the present, where you are in control.
Exercise: Take your attention away from your thoughts, away from your head and into your body.
Awareness of body Notice what it feels like to be a body sitting in a
chair Notice your weight on the chair Notice how your back feels against the chair Notice all the things you can feel Things that normally our mind does not notice
because they are not ‘interesting’

Individual work Therapeutic Alliance
As this approach represents a new normalisation, it can greatly aid the therapeutic alliance
Prepared to start from wherever the individual is Their experience is taken seriously and valued Encouragement to join the shared world, while
respecting their wish to retain access to the unshared (if wanted).
Risk and detention. Appreciation of the team’s perspective – people concerned about them
Their responsibility to manage those concerns.

Formulation Template
Try to escape from the emotion by avoidance, self harm, unshared reality etc.
Feel better short term
Bad longer term consequences.Aversive emotion worse.
Past: abuse, trauma etc.
Recent triggering event
Another maintaining cycle
feeding the emotion
HorribleFeeling

Using EFF with Psychosis
Approach with caution – based on an understanding of the States of Mind diagram
Exploring the emotion Might be accessible (fear in paranoia) Might be masked (psychosis as escape from
intolerable emotion) – caution needed The past – might need to be vague –
normalize its effect on the present Their coping strategies normalized – what
gets the person by but keeps them stuck

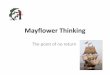
Psychosis formulation
FEARTHREAT!
THE PAST
Being in crowds, busy places:Body reacts to threat
Body reacts to threat: Intrusive thoughts
Withdraw, hide awayOr Fight, become aggressive
Escapes from thoughts By slipping into unshared world
Hears voices
More tension, sweaty, heart races
Unrealistic, worse, fears
RECENT TRIGGER

Breaking the Vicious Circles
Arousal management Grounding mindfulness Mindfulness of unusual
experiences/unshared beliefs – takes courage Fear and avoidance Facing that it is unshared – e.g. when grandiose
Facing emotion - DBT skills Self Compassion Relationship management

Spiritual Crisis Network Approach
There to offer a more hopeful, alternative, perspective – while stressing the role of NHS to manage risk
Small, unfunded, UK charity Website with email contact Supportive, validating responses Team of rota responders given training Awareness raising events and conferences A few local groups Ambitions to do more (e.g. Phone response)

SCN Email Responding Empathise with what they are going through
(might be a relative, friend or other supporter) Normalize – others have experienced the same
(majority of SCN responders have own crisis) Hopeful – in retrospect a transformative
experience for many, if difficult while in the midst of it.
Practical suggestions (next slide) Any suggestion of risk – strongly encourage
contacting NHS, taking medication as advised etc, while acknowledging they might be reluctant.
No outright advice or therapy recommendations

Grounding Advice Grounding when the experience is
overwhelming. Grounding activity. Grounding food.
Sleep Mindfulness activity in the now Importance of support Maintain ordinary relationships – even when this
feels irrelevant Managing arousal – breathing control to reduce
arousal and manage fear Mindful activity in the present to prevent it
slipping. Moderate spiritual practice Avoid substances

Contact details, References and Web addresses
Clarke, I. (Ed.) (2010) Psychosis and Spirituality: consolidating the new paradigm. Chichester: Wiley
Clarke, I. ( 2008) Madness, Mystery and the Survival of God. Winchester:'O'Books.
Clarke, I. & Wilson, H.Eds. (2008) Cognitive Behaviour Therapy for Acute Inpatient Mental Health Units; working with clients, staff and the milieu. London: Routledge.
Wilson, H, Clarke, I & Phillips,R., (2009) Evaluation of an Inpatient Group CBT for Psychosis Program Designed to Increase Effective Coping and Address the Stigma of Diagnosis Psychosis. http://www.isabelclarke.org/clinical/icspsychosis.shtml
Clarke, I. (2013) Spirituality: a new way into understanding psychosis. In E.M.J. Morris, L.C.Johns and J.E. Oliver eds. Acceptance and Commitment Therapy and Mindfulness for Psychosis. Chichester: Wiley-Blackwell, p. 160-168.
www.isabelclarke.org www.SpiritualCrisisNetwork.org.uk