Embed Size (px)
Citation preview

A Fernando, mi maestro, mentor y amigo.
“Y ou can´t transplant islets unless you know how to isolate them”
Paul E. Lacy (1924-2005)

List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Caballero-Corbalán, J., Eich, T., Lundgren T., Foss A.,
Felldin M., Källen R., Salmela K., Tibell A., Tufveson G., Korsgren O., Brandhorst D. (2007) No beneficial effect of two-layer storage compared with UW-storage on human islet isola-tion and transplantation. Transplantation; 84(7): 864–869
II Caballero-Corbalán, J., Brandhorst H., Malm H., Felldin M.,
Foss A., Salmela K., Tibell A., Tufveson G., Korsgren O., Brandhorst D. (2011). Using HTK for prolonged pancreas preservation prior to human islet isolation. J Surg Res; Mar 31. [Article in press]
III Caballero-Corbalán, J., Friberg, A. S., Brandhorst H., Nilsson
B., Andersson H.H., Felldin M., Foss A., Salmela K., Tibell A., Tufveson G., Korsgren O., Brandhorst D. (2009) Vitacyte col-lagenase HA: A novel enzyme blend for efficient human islet isolation. Transplantation; 88(12): 1400-1402. Erratum in: Transplantation; 89(7): 907.
IV Caballero-Corbalán, J., Brandhorst H., Asif S., Korsgren O.,
Engelse M., de Koning E., Pattou F., Kerr-Conte J., Brandhorst D. (2010) Mammalian tissue-free liberase: a new GMP-graded enzyme blend for human islet isolation. Transplantation; 90(3): 332-333
V Caballero-Corbalán, J., Brandhorst H., Brandhorst D.,
Korsgren O. (2011). Predicting the outcome of human islet iso-lation. Manuscript.
Reprints were made with permission from the respective publishers.

Additional Publications
Christoffersson G., Henriksnäs J., Johansson L., Rolny C., Ahlström H., Caballero-Corbalán, J., Segersvärd R., Permert J., Korsgren O., Carlsson PO., Phillipson M. (2010) Clinical and experimental pancre-atic islet transplantation to striated muscle: establishment of a vascular system similar to that in native islets. Diabetes; 59(10): 2569-2578
Contents
Introduction ................................................................................................... 11
Aims .............................................................................................................. 12 General Aim ............................................................................................. 12 Specific Aims ........................................................................................... 12
Background ................................................................................................... 15 Diabetes Mellitus in 2011 ........................................................................ 15
Blood glucose regulation ..................................................................... 16 Insulin treatment in diabetes: hyperglycemia and hypoglycemia ....... 16 Brittle diabetes and hypoglycemia unawareness ................................. 17
Beta-cell replacement therapy: pancreas vs. islet transplantation ............ 18 Transplanting the endocrine pancreatic islet mass .............................. 19
Organ procurement for human islet isolation and transplantation ........... 19 Ischemia and organ preservation in islet transplantation .................... 19
Islet isolation: a technical challenge ........................................................ 23 Pancreas dissociation: a physical-chemical process ............................ 23
Pancreas histology: WYSIWYG? (What you see is what you get?) ....... 27
Material and Methods ................................................................................... 28 The two-layer method (UW/Perfluorodecalin) (Paper I) .................... 28 Characterization of islet morphology by insulin immunostaining (Paper V) ............................................................................................. 29 Statistics ............................................................................................... 29
Results and Discussions ................................................................................ 30 The ischemic tolerance of pancreatic tissue with the Two-Layer Method (Paper I) ................................................................................. 30 Lower islet yields using HTK during prolonged pancreas preservation (Paper II) .............................................................................................. 31 Vitacyte HA decreases digestion time without damaging islets (Paper III) ........................................................................................................ 33 Mammalian Tissue-Free Liberase in successful human islet isolation (Paper IV) ............................................................................................ 34 Prediction of isolation outcome in the human pancreas (Paper V) ..... 36

Conclusions ................................................................................................... 38 Paper I .................................................................................................. 38 Paper II ................................................................................................ 38 Paper III ............................................................................................... 38 Paper IV ............................................................................................... 38 Paper V ................................................................................................ 39
Future Perspectives ....................................................................................... 40
Summary in Spanish ..................................................................................... 41
Acknowledgements ....................................................................................... 43
References ..................................................................................................... 46

Abbreviations
AEC 3-amino-9-ethylcarbazole CC1 Collagenase class I CC2 Collagenase class II CIT Cold ischemia time CP/G C-peptide to glucose ratio DCCT Diabetes Control and Complication Trial ECM Extracellular matrix EDIC Epidemiology of Diabetes Interventions and
Complications ESRD End-stage renal disease GMP Good manufacturing practice HAAF Hypoglycemia associated autonomic failure HbA1c Glycated hemoglobin HES Hydroxyethyl starch HTK Histidine-tryptophan-ketoglutarate IDF International Diabetes Federation IE Islet equivalent IN Islet number MODY Maturity-onset diabetes of the young NP Neutral protease NS Not significant PAK Pancreas after kidney PBS Phosphate buffered saline PFD Perfluorodecalin PTA Pancreas transplant alone SEM Standard error of the mean SI Stimulation index SIK Simultaneous islet kidney SPK Simultaneous pancreas kidney TLM Two-layer method UNOS United Network for Organ Sharing UW University of Wisconsin WHO World Health Organization (PZ)-U 4-phenylazobenzyloxycarbonyl-L-prolyl-L-
leucylglycyl-L-prolyl-D-arginine

11
Introduction
The treatment of type-1 diabetes has been revolutionized by the introduction of innovative ways of insulin delivery and formulations. However, insulin is able to delay hyperglycemia-related complications but cannot prevent them. Hypoglycemia is a dangerous complication following insulin treatment, leading to physical and psychological morbidity in the diabetic patient. The ultimate goal is to achieve blood glucose homeostasis in a physiological manner. Islet transplantation has contributed to a better quality of life and better glycemic control of diabetics suffering from severe hypoglycemia, hypoglycemia unawareness and/or advanced complications that are not eli-gible for whole pancreas transplantation. Several travails hinder the widespread clinical application of the procedure. Among others, the low efficacy of the islet isolation procedure is determi-nant in the fact the islets from multiple organs are needed to achieve insulin independence. The work within this doctoral thesis aims to improve different steps in the isolation procedure: pancreas preservation, enzymatic pancreas dissociation and prediction of the isolation outcome. Several preservation solutions have been compared to optimize the protection of the human pan-creas against ischemia. We have also studied the outcome of isolations pro-cedures with different enzyme blends for clinical islet isolation aiming at minimizing the time that islets are exposed to the harmful environment dur-ing the dissociation process. We further investigated whether isolation out-come could be predicted from a biopsy taken from the head of the pancreas, showing that islet morphology does not correlate to the isolated islet yield. The improvement of the quality of the pancreas and the islets throughout the isolation and transplantation procedures is a prerequisite for successful islet engraftment and functioning over time in the transplanted diabetic patient.
12
Aims
General Aim The work within this thesis aims to increase the success of human islet isola-tion, in particular by improving human pancreas preservation, optimizing enzymatic pancreas dissociation and predicting isolation outcome.
Specific Aims Paper I
• To investigate the effect of the perfluorodecalin-based two-layer method in human pancreas preservation compared to the standard organ preservation method using the University of Wisconsin solution.
• To investigate the effect of pancreas preservation on islet isolation outcome of pancreata from elderly donors (>60 years).
• To study the effect of pancreas preservation with the two-layer method on post-transplant islet function by means of the C-peptide to glucose ratio.
Paper II
• To study whether histidine-tryptophan-ketoglutarate is effec-tive as a static preservation solution for prolonged human pancreas cold storage before islet isolation.
• To compare histidine-tryptophan-ketoglutarate with the Uni-versity of Wisconsin preservation solution.
• To study whether tissue edema is induced in the human pan-creas during preservation with histidine-tryptophan-ketoglutarate and whether this influences islet isolation out-come.
Paper III • To compare the efficacy of a new clinical-grade collagenase
blend called Vitacyte CIzyme HA with the commonly used Serva NB1 for human islet isolation.
13
Paper IV • To evaluate the efficacy of a new GMP-graded, mammalian
tissue-free collagenase blend called Liberase MTF-S for human islet isolation.
Paper V • To study whether human islet isolation outcome can be pre-
dicted from morphological parameters in a biopsy taken from the pancreatic head.

14
15
Background
Diabetes Mellitus in 2011 Diabetes Mellitus is a chronic disease characterized by an endocrine pancre-atic dysfunction, which results in a deficient blood sugar counterregulation. Traditionally, diabetes has been classified into two main groups: type 1 (T1DM), previously named as insulin-dependent or juvenile-onset, and type 2 (T2DM), previously referred as non insulin-dependent or adult-onset (1). T1DM is characterized by an absolute insulin deficiency as a result of the beta-cells destruction, most often autoimmune mediated. T2DM, the most common, results from a progressive insulin secretory defect on the back-ground of peripheral and hepatic insulin resistance (2). Other less common types of diabetes include gestational diabetes, pancreatogenic (when a pa-tient is subjected to a sub-total or total pancreas resection), inherited mono-genic forms such as maturity-onset diabetes of the young (MODY), etc. (3).
90 years after its discovery, insulin is still not available on a regular basis in developing countries, leading to a poor outcome in life expectancy of children with newly diagnosed T1DM (4). It is the major cause of blindness and kidney failure, being responsible for a million lower limb amputations every year (5) In 2008, diabetes mellitus led to 1.26 million deaths, being the 9th more common cause of death in the world (6). Despite major efforts for raising the awareness about the importance of the disease (7, 8), diabetes is one of the most common non-communicable diseases, accounting for one of the main global burden of disease.
The World Health Organization estimated the prevalence of diabetes to rise from 2.8% in year 2000 to 4.4% in 2030 (9), but recent data from the International Diabetes Federation (IDF) increases this figures to a global prevalence of 7.8 % or 438 million adults by 2030 (10). New emerging economies such us China present a rapid increase in the prevalence of the disease. The diabetes epidemic in this country has reached 92.4 million adults by 2010 (11), and it is estimated to be close to half a billion by 2030 (12). Scandinavia has the highest incidence of T1DM among children (10). Furthermore, diabetes nephropathy is the primary cause of end-stage renal disease (ESRD) among new patients receiving dialysis in Sweden (13).
16
Blood glucose regulation Glucose is the main source of energy in mammalian cells. Its narrow regula-tion results from the balance of glucose intake (carbohydrates) in the intes-tine and glucose utilization (basal metabolism, exercise). After eating, glu-cose is stored directly as glycogen in the liver and in the muscles (glyconeo-genesis). In the fasting state, the liver plays a key role in endogenous glucose production by releasing the glucose into the blood from the previously stored glycogen (glycogenolysis). Glucose is also produced from other nu-trients such as proteins or fatty acids (neoglucogenesis) (14).
Two hormones mainly regulate the fine-tuning of glucose homeostasis: insulin and glucagon. Insulin is an anabolic hormone that enhances glucose utilization by facilitating glucose metabolism by fat and muscle cells (14), which results in a decreased blood glucose concentration. On the contrary, glucagon is a catabolic hormone that increases blood glucose mainly by stimulating glycogenolysis in the liver. Both hormones are produced in the pancreatic islets of Langerhans, small endocrine organs within the pancreas. The total islet mass accounts for 1-2 % of the volume of the pancreas and is spread throughout the whole organ. They are controlled by central stimuli as well as paracrine mechanisms.
Insulin treatment in diabetes: hyperglycemia and hypoglycemia Diabetes is characterized by a relative or absolute lack of internal insulin secretion. As a result, glucose cannot be metabolized by muscle and fat cells and accumulates in the blood (hyperglycemia). Thus, cells starve in the ab-sence of insulin and the patient enters a catabolic state leading to death if left untreated.
The high amount of circulating glucose affects the blood vessels of dif-ferent organs (15). Intracellular hyperglycemia occurs in tissues not able to downregulate their glucose uptake, affecting the smaller blood vessels (mi-croangiopathy) in the eyes (retinopathy), nerves (neuropathy) and kidneys (nephropathy). Other blood vessels may as well be damaged due to athero-sclerosis (macroangiopathy), leading to a higher risk of cardiovascular dis-ease.
Exogenous insulin replacement has been the standard of care since the discovery of insulin in 1921. Intensive insulin treatment and its capacity to delay the onset and slow down the progression of diabetes-related complica-tions were extensively studied in T1DM patients in the early 1990’s in the Diabetes Control and Complication Trial (DCCT) (15). In this trial, conven-tional therapy (1-2 daily insulin injections) was compared to intensive thera-py (3 or more insulin injections or insulin pump). It was found that HbA1c correlates directly with the appearance of macro and microvascular compli-cations. Furthermore, the Epidemiology of Diabetes Interventions and Com-

17
plications trial (EDIC), with 90% of the patients from the DCCT trial, showed a further reduction in diabetes complications and, moreover, a 42% reduction in overall cardiovascular risk (16). On the other hand, these trials did not study patients with severe complications and/or frequent hypoglyce-mia.
The DCCT trial showed that intensive insulin therapy leads to a 3-fold in-crease in iatrogenic severe hypoglycemia(17). Severe hypoglycemia is often described as a “hypoglycemic episode requiring intervention from another person”. It has been estimated to account for 1.3 episodes per patient per year, affecting one third of all patients with type 1 diabetes (18).
Brittle diabetes and hypoglycemia unawareness As the body of a diabetic patient is unable to control the glycemia, blood sugar levels can vary extremely, leading to both hypo- and hyperglycemia. In insulin-treated patients, iatrogenic hypoglycaemia (low blood sugar lev-els) is the result of insulin excess (due to differences in the pharmacokinetics between exogenous and endogenous insulin and in relation to the carbohy-drate intake and the level of physical exercise) and the malfunction of the hypoglycaemia counterregulation mechanisms. The fear for hypoglycemia hinders the patient from the maintenance of euglycemia (19), thereby in-creasing the risk for diabetes complications. It implies both physical and psychological morbidity for the patient, being often identified as the limiting factor in the management of diabetes (20).
In healthy individuals, the falling blood glucose concentration stimulates adrenalin secretion and inhibits insulin release thereby increasing insulin concentration in the beta cells of the pancreas (21). As a result, alpha-cells will be enhanced via a paracrine signal to secrete glucagon, which in turn activates glycogenolysis in the liver and the release of glucose into the bloodstream (22).
All type 1 diabetes patients will loose their ability to counteract hypogly-cemia in a physiological manner at a certain point after diagnosis, which directly correlates with the remaining pancreatic beta-cell function (23). Being unable to activate a normal response, diabetics are rendered dependent on an adrenaline-mediated response to rise their blood sugar and recover from hypoglycemia (24). Furthermore, frequent hypoglycemia lowers the glycemic thresholds for sympatho-adrenal responses (25) and for the activa-tion of neuroglycopenic symptoms (hypoglycemia unawareness). These two features are described in a clinical syndrome called Hypoglycemia-associated autonomic failure (HAAF).

18
Beta-cell replacement therapy: pancreas vs. islet transplantation The avoidance of hypoglycemic episodes restores the ability to sense hypo-glycemia (26). Today a number of technical applications are available for more physiological insulin delivery, providing better metabolic control and fewer hypoglycemic episodes (27), e.g. insulin pumps (subcutaneous, intra-peritoneal), sensor-augmented pumps and close-loop devices (28, 29). Even though these devices are a step closer to an “artificial pancreas”, the restora-tion of the blood glucose homeostasis has been only achieved by replacing the insulin-producing beta cells (30).
Pancreas transplantation as a mean of treating brittle or unstable diabetes has been explored since the end of the 19th century, even before insulin was discovered and linked to the beta cells within the pancreatic islets (31). The first clinical report comes from 1966, with rather poor results due to the complications related to the pancreatic surgery (32). Over the years, the technique has improved and, thanks to modern immunosuppressive drugs and effective infection control, this therapy offers today long-term graft sur-vival comparable to other transplanted organs, especially in combined pan-creas-kidney transplantation (SPK) (33). The number of patients receiving a pancreas after kidney (PAK) or only a pancreas (PTA) has also increased (34) thanks to the possibility of achieving long-term metabolic control and reduction of diabetes complications (35). However, the stringent donor re-quirements and the high co-morbidity limit this therapy to relatively young patients with advance kidney disease and/or severe hypoglycemia but no history of cardiovascular disease (34).
If the patient suffers from brittle diabetes and/or hypoglycemia unaware-ness and has already a transplanted kidney or preserved kidney function, islet transplantation may be a better option (36). For islets to be transplanted, they need to be separated from the surrounding exocrine tissue, a procedure known as islet isolation. (37).
After organ procurement, isolation of human pancreatic islets takes place in a GMP-certified laboratory. Islet viability and functionality is controlled before purified islet fractions are transplanted into the liver by infusion via a catheter into the portal vein system. Although not free from potential com-plications, modern islet transplantation technique offers a low risk for side effects and is associated with short hospital stay as compared to vascularized pancreas transplantation (38).
It has long been discussed how to allocate organs for pancreas vs. islet transplantation, as both treatment modalities compete for organs of good quality (39). In fact, pancreata from old and obese donors are considered to be not suitable for vascularized organ transplantation (40, 41) while they frequently provide high yields in islet isolation (42, 43). At present, pancre-

19
ata from young and slim donors are usually prioritized for whole-organ transplantation while pancreata for islet isolation are mostly retrieved from old and obese donors. The reason that long-term graft survival is inferior for islet transplantation compared to whole-pancreas is still under debate. Islets from older “extended criteria” donors have been shown to have a decreased functional capacity compared to younger donors (44). Whether this influ-ences current clinical human islet isolation results remains to be elucidated (45).
As both therapies require lifelong immunosuppression, the decision whether the patient is a candidate for either pancreas or islet transplantation or both relies on a careful evaluation of the risk-to-benefit ratio.
Transplanting the endocrine pancreatic islet mass Beta-cell replacement therapy by means of islet transplantation is a para-digm of cell transplantation and a promising option for the treatment of pa-tients suffering from brittle diabetes and life-threatening hypoglycemia una-wareness. With the introduction of new immunosuppressive protocols and the improvement of the isolation technique (46), the success rate of the pro-cedure is today comparable of whole pancreas transplantation (47, 48). Re-cent analysis of the Edmonton Trial has shown that even if insulin independ-ence is not sustainable after transplantation, persistent islet function provides both protection from severe hypoglycemia and improvement of glycated hemoglobin (49).
Despite this promising appraisal, the low efficacy of the isolation proce-dure in relation to the shortage of suitable donors is up to now one of the biggest disadvantages. Islets from multiple donors are needed to treat one single recipient and there is a loss of graft function over time. These facts provide evidence of the destruction and/or low engraftment of the majority of the implanted cells and the subsequent malfunction of the remaining ones over time (50).
Organ procurement for human islet isolation and transplantation
Ischemia and organ preservation in islet transplantation Regionalization of islet-processing facilities is being explored as a solution to maximize utilization of donor pancreata. It has shown to improve isola-tion efficiency and reduce costs, leading to the realization of clinical trials in islet transplantation (49, 51, 52). To date, several multicenter networks have

20
been established in Europe and the United States, among them the Nordic Network for Clinical Islet Transplantation in Scandinavia (53).
Due to logistical reasons, organs are usually transported between hospi-tals and sometimes between countries to optimize pancreas allocation. Transportation of a vascularized organ unequivocally implies ischemia due to the lack of oxygenated blood and the accumulation of metabolic end products within the ischemic tissue. As a time-dependent mechanism, is-chemia progressively damages the endothelial cells in the transplantable organ, making it unable to recover its function after transplantation and reperfusion.
Cold static organ preservation is the current standard for organ transplan-tation (54). During organ retrieval, blood vessels are perfused with a cold preservation solution to remove the blood and prevent intravascular throm-bosis, accelerate the cooling of the organ and counteract the ischemic and hypothermic damage to cells. Hypothermic preservation solutions are there-fore used to make the organ tolerant to ischemia and hypothermia.
During hypothermia (usually 4°C), cell metabolism decreases leading to a reduced oxygen and nutrient consumption. Since 10–12% of the normal metabolic activity is still operative in the ischemic tissue at 4°C, hypother-mic organ perfusion and subsequent immersion in various preservation solu-tions such as University of Wisconsin solution (UW) or Histidine-Tryptophan-Ketoglutarate (HTK) do not completely prevent irreversible pancreas injury once a critical period of cold ischemia is exceeded (55). The temperature-related reduction in the activity of Na/K ATPase pump leads to an intracellular accumulation of sodium and the resulting osmotic influx of water (56). To prevent this, colloids are added to the preservation solution. Other common components in preservation solutions are antioxidants, en-zyme inhibitors and vasoactive substrates. The overall aim of all these com-pounds is to prevent the deterioration of the organ during hypothermic stor-age and the so-called ischemia-reperfusion injury once the circulation to the organ is restored in the recipient.
Efficient preservation of the pancreas prior to islet isolation has been re-ported to be of high importance for achieving a high islet yield (57, 58). In the present thesis, papers I and II explore two different solutions to preserve the pancreas prior to the isolation procedure.
University of Wisconsin solution The UW solution has been the most frequently used preservation solution for static cold storage in abdominal organ preservation for the past 20 years. It has been successfully applied for preservation of kidney, liver, pancreas, heart and small bowel as well as pancreatic islets and hepatocytes (59).
It was originally designed for pancreas preservation with a similar elec-trolyte composition as the intracellular microenvironment (high K+ and low
21
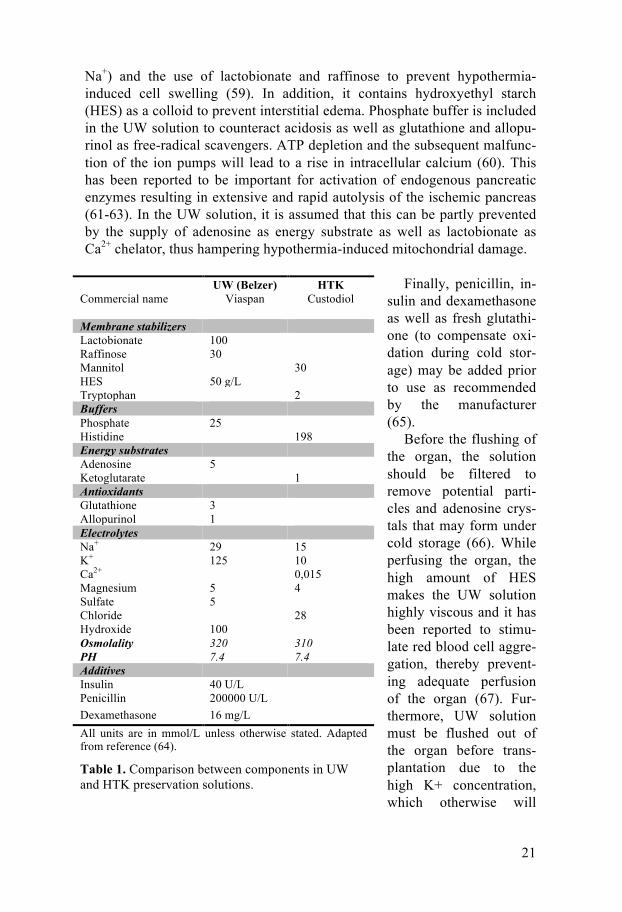
Na+) and the use of lactobionate and raffinose to prevent hypothermia-induced cell swelling (59). In addition, it contains hydroxyethyl starch (HES) as a colloid to prevent interstitial edema. Phosphate buffer is included in the UW solution to counteract acidosis as well as glutathione and allopu-rinol as free-radical scavengers. ATP depletion and the subsequent malfunc-tion of the ion pumps will lead to a rise in intracellular calcium (60). This has been reported to be important for activation of endogenous pancreatic enzymes resulting in extensive and rapid autolysis of the ischemic pancreas (61-63). In the UW solution, it is assumed that this can be partly prevented by the supply of adenosine as energy substrate as well as lactobionate as Ca2+ chelator, thus hampering hypothermia-induced mitochondrial damage.
Finally, penicillin, in-
sulin and dexamethasone as well as fresh glutathi-one (to compensate oxi-dation during cold stor-age) may be added prior to use as recommended by the manufacturer (65).
Before the flushing of the organ, the solution should be filtered to remove potential parti-cles and adenosine crys-tals that may form under cold storage (66). While perfusing the organ, the high amount of HES makes the UW solution highly viscous and it has been reported to stimu-late red blood cell aggre-gation, thereby prevent-ing adequate perfusion of the organ (67). Fur-thermore, UW solution must be flushed out of the organ before trans-plantation due to the high K+ concentration, which otherwise will
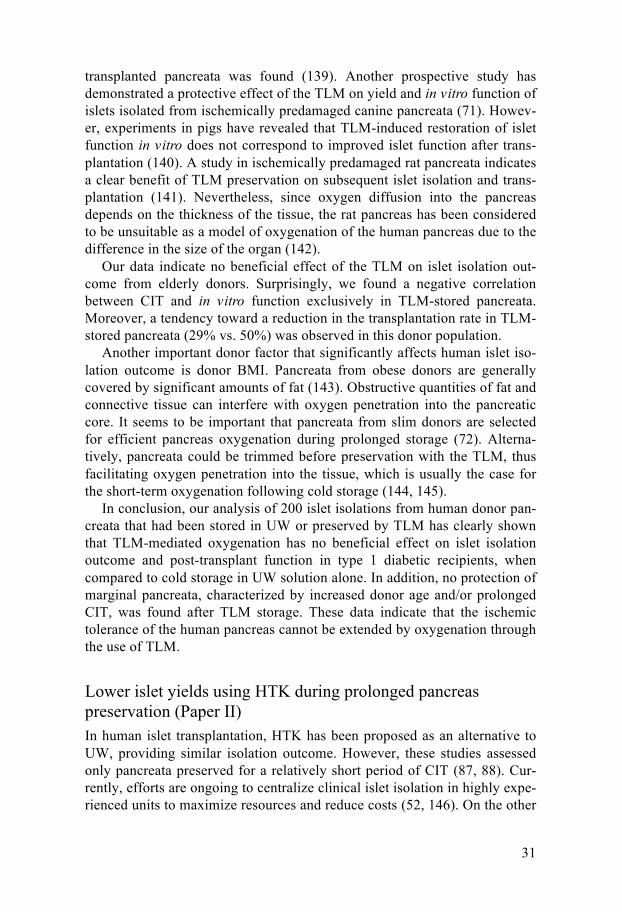
UW (Belzer) HTK Commercial name Viaspan Custodiol Membrane stabilizers Lactobionate 100 Raffinose 30 Mannitol 30 HES 50 g/L Tryptophan 2 Buffers Phosphate 25 Histidine 198 Energy substrates Adenosine 5 Ketoglutarate 1 Antioxidants Glutathione 3 Allopurinol 1 Electrolytes Na+ 29 15 K+ 125 10 Ca2+ 0,015 Magnesium 5 4 Sulfate 5 Chloride 28 Hydroxide 100 Osmolality 320 310 PH 7.4 7.4 Additives Insulin 40 U/L Penicillin 200000 U/L Dexamethasone 16 mg/L All units are in mmol/L unless otherwise stated. Adapted from reference (64).
Table 1. Comparison between components in UW and HTK preservation solutions.
22
lead to vasoconstriction (68) and cardiac arrest. The UW solution has been used for pancreas preservation prior to whole
organ transplantation but, when used before human islet isolation, it seems to be suitable only for a limited period of time (55).
Two-Layer Method The inability to isolate a critical mass of viable islets from UW-preserved pancreata with prolonged CIT encouraged the concept of supplying ischemic pancreatic tissue with oxygen utilizing the hyperoxygen carrier perfluorode-calin (PFD) (69). By storing the organ in the interface between an oxygen-saturated oxygen carrier and UW, it was hypothesized that both oxygen and nutrients are provided to maintain ATP production (70).
Evidence in the canine model (69, 71) led to several pilot studies indicat-ing the benefit of preserving the human pancreata with the TLM during cold storage (72, 73). In addition, it was suggested that pancreata from marginal donors could be recovered for clinical islet transplantation (74) after addi-tional preservation with the TLM (75).
Despite initial enthusiasm, several studies from others (76) and us (paper I) could not show a significant positive effect on isolation outcome or post-transplant islet function in a large cohort of pancreata. These disappointing results could be explained by experiments in pig pancreata demonstrating that the TLM can oxygenate only a small fraction of the surface of the pan-creas, but is not able to reach the hypoxic core (77).
Histidine-Tryptophan-Ketoglutarate Originally designed as a cardioplegic solution in the 1970´s (78), HTK solu-tion has been increasingly used as an alternative to the UW solution for ab-dominal organ preservation. Compared to UW (Table 1), HTK uses histidine instead of phosphate as a buffer, tryptophan as a membrane stabilizer, ke-toglutarate instead of adenosine as energy substrate and mannitol as imper-meant instead of raffinose and lactobionate. The low Na+ levels resemble an intracellular fluid while the low K+ makes HTK safe for release into the circulation of the recipient.
Due to the lower viscosity, it was suggested that HTK accomplish a better perfusion and faster cooling during organ procurement (79). Even though a greater volume of solution was used, HTK perfusion remained less costly than UW solution (80). To date, there is no general consensus over its suita-bility for organ preservation, with a series of late conflicting reports rising concerns about the efficiency of the solution for different indications (81-84).
In vascularized pancreas transplantation, several studies have shown no difference between HTK and UW in terms of early graft function and patient survival (83, 85, 86). However, pancreata flushed with HTK have been asso-

23
ciated with a higher incidence of postoperative complications including pan-creatitis and decreased rate of insulin-independence at hospital discharge (81). In a recent study on the UNOS (United Network for Organ Sharing) database including over 4000 patients, HTK preservation was associated with increased early graft loss (84).
In islet transplantation, HTK solution has been reported to be similar to UW in terms of islet yield, viability and in vitro insulin secretion (87). Fur-thermore, the percentage of preparations suitable for clinical transplantation increased by two fold in HTK-preserved pancreata (88). However, the high flushing volume may induce tissue edema, affecting pancreas viability and subsequent islet isolation in a negative way (paper II).
Islet isolation: a technical challenge The islet isolation procedure essentially consists of two main consecutive steps: first, the dissociation of the pancreatic tissue by a combination of en-zymatic digestion and mechanical disruption and second, the separation of the islets from the exocrine tissue by means of density gradient centrifuga-tion. Islet isolation has been attempted since the beginning of the 20th centu-ry, but the combined mechanical and enzymatic approach was first described by Moskalewski in 1965 (89). Subsequent discoveries in terms of enzymatic digestion (90, 91) and tissue purification (81, 92) paved the way for success-ful large-scale human islet isolation (93, 94) (for review see ref. (37, 95)).
As stated by Dr. Paul E. Lacy, a pioneer of islet transplantation, in his last public speech in December 2004 (96), the discovery made by the young Camillo Ricordi was to set a new reference for enzymatic pancreas dissocia-tion that still today is the standard in most laboratories (93). This, however, means that neither the main steps in human islet isolation nor the results have substantially developed since the 1980´s, which reflects nothing but the complexity of the technique and the need for further research.
Pancreas dissociation: a physical-chemical process Islet isolation starts with the trimming of the peripancreatic fat and connec-tive tissue under aseptic conditions. The pancreas is distended with the en-zyme solution via the pancreatic duct in order to distribute the enzyme in the acinar tissue. The distended organ is then cut into several pieces and trans-ferred to the digestion chamber. To enhance the pancreas dissociation, the chamber is agitated so that the perfused tissue progressively disintegrates while incubating at 37°C. Complete removal of exocrine tissue from the surface of the islet is crucial for the subsequent density-based separation procedure.
24
Islets of Langerhans are highly vascularized mini-organs spread through-out the pancreas. The separation and release of the islets from the acinar tissue is performed by enzymatic degradation of the extracellular matrix (ECM) in the endo-exocrine interface. The pancreatic ECM is rich in colla-gen (97), an essential structural component of the connective tissue. Because of its structural function, collagen fibers are only degraded by a few proteas-es. The current protocols for human islet isolation use collagenase from the bacterium Clostridium histolyticum.
Clostridial enzyme blends for human pancreas dissociation The crude bacterial collagenase product obtained from fermentation of Clos-tridium histolyticum contains different active components, such as colla-genase, the most essential one, phospholipase, clostripain, elastase, ami-nopeptidase, galactosidase and other proteases (98). Crude collagenase is therefore a mixture of enzymes working together to disaggregate the pancre-atic tissue. Collagenase is characterized into six different isoforms (α, β, γ, δ, ε, ζ), which are further divided into two subclasses1: Class I and Class II (99).
In the past, islet isolation was performed utilizing crude collagenase (100). However, the introduction of purified enzyme blends during the 1990’s improved isolation outcome in the clinical setting. As a result, crude collagenase was abandoned for human islet isolation (101, 102). On the oth-er hand, the purification of crude collagenase did not eliminate batch-to-batch variability, contributing to unpredictable isolation results (103).
Collagenases are highly specific enzymes that hydrolyze the native colla-gen molecules. Collagenase class I (CC1) and II (CC2) are the main compo-nents of purified enzyme blends for islet isolation. We know that they have different roles in collagenase digestion: CC1 (α, β and γ) is more stable and has a greater activity toward native collagen, whereas CC2 (δ, ε and ζ) has a moderate collagen activity, being characterized by the ability to digest a broader range of peptide substrates as compared to CC1 (104, 105). The ratio between collagenase classes has been reported to be of importance for optimal islet cleavage as proven in the rat and human pancreas (106, 107). Furthermore, both CC1 and CC2 act synergistically on collagen degradation (108).
Purified collagenase blends are unable to fully dissociate the pancreatic ECM due to the lack of non-collagenolytic enzymes and other macromole-cules as compared to the crude collagenase (104, 109). As a result, addition-al collagenolytic proteases are needed to achieve adequate tissue digestion (109). Neutral protease (NP) from Clostridium histolyticum has been exten-sively used in clinical islet isolation (110). Thermolysin, a thermostable neutral protease produced by the gram-positive bacteria Bacillus thermopro- 1 Based on their activities toward native collagen and the synthetic peptide FALGPA.

25
teolyticus, has been previously used to replace clostridial neutral protease (101)and today is present in several efficient collagenase blends (Paper III and IV). Based on our experience (110) and that of others (111), neutral proteases should be carefully titrated as to avoid islet damage (112). This exemplifies the complexity of islet isolation by means of enzymatic pancreas dissociation (113, 114).
Commercial enzymes for islet isolation: what do we get? The current policy of collagenase manufacturers is to purify enzyme blends to the highest possible extent and to obtain a product that consists solely of collagenase and a neutral protease. The first available purified enzyme blend called Liberase HI was introduced in 1994 and became the gold standard for human islet isolation (115, 116). This product contained collagenase class I and II as well as the neutral protease thermolysin, with a low endotoxin level (101). Several years after its release, it became obvious that a strong intra- and inter-lot variability was present in Liberase HI (123).
Although recombinant collagenase was developed in parallel, the final product did not reach the market, even though it provided similar isolation results as Liberase (117) Nevertheless, the variable enzymatic activity of different batches is a persisting problem that exists among product from other enzyme manufacturers (89, 118), being a major obstacle in achieving reproducibility in islet isolation. As a result, a most recent study has shown the efficiency of crude collagenase for human islet isolation, concerning also the commercial background of islet isolation research (119).
Collagenase degradation during storage (114) or during isolation (120) due to the auto-digestion of the different components is suggested to be re-sponsible for the large inter- and intrabatch variability in efficiency of en-zymes blends. However, contamination from non-collagenolytic enzymes has recently been reported in protocols for islet isolation without the addition of NP (121). On the other hand, production of highly purified enzyme blends may remove toxic components (122) but also enzymatic activities such us clostripain, which may be crucial for isolation success (118). Another detri-mental byproduct of C histolyticum fermentation is endotoxin. It has been shown that this toxin is present in crude collagenase blends and can easily contaminate other reagents (123), resulting in deleterious effects on islet viability and transplantation outcome (124-126).
Currently, most manufacturers offer both collagenase and protease as separate vials, allowing for a customization of the digestion step (127). It also prevents collagenase degradation and increases stability of the enzyme products. However, this customization requires vast isolation experience as well as the utilization of human donor pancreata for enzyme testing, which can be a technical and financial handicap for those centers with limited re-sources or organ supply.
26
Enzymes for clinical islet isolation In 2007, Liberase HI was withdrawn from the market because of the risk
of potential transmission of bovine spongiform encephalopathy due to the use of bovine neural tissue in its manufacture procedure (128). As a result, the islet transplant activity worldwide decreased (129) while all active cen-ters performing clinical islet isolation had to switch to alternative enzymes such us Serva collagenase NB1 (120) or Vitacyte collagenase HA (130) (Paper III).
The discontinuation of Liberase HI from the market remains a plausible although not absolute explanation for the decline of islet transplant activity in the second half of the last decade (131). Nevertheless, this was a clear signal for the worldwide islet community that clinical islet transplantation programs depend on an oligopoly of enzyme manufacturers.
Shortly after Liberase HI was precluded from clinical islet isolation, most of the active transplantations centers switched to collagenase blends provid-ed by Serva. Stimulated by the growing demand for effective enzymes for islet isolation in clinical trials, Vitacyte collagenase HA was introduced in the market in 2007 as an alternative to Serva NB1 (131). Similar to Serva, Vitacyte offered the possibility of tailoring pancreas digestion by commer-cializing collagenase and thermolysin in different vials.
Further development within the Roche enzyme production led to the commercialization of a new enzyme blend free from exposure to mammalian tissue (Liberase MTF-S). Initial experience with this new combined enzyme blend has proved its efficacy in human islet isolation (Paper IV). Moreover, chromatographic analysis of this new GMP-grade (Good Manufacturing Practice) Liberase confirms the stability of the different collagenase frac-tions as compared to the NB1 enzymes by Serva (132).
The introduction of GMP standards in enzymatic islet isolation has im-proved the documentation and traceability of the islet production process as well as patient safety. This, however, has not resulted in an improved or more homogenous islet isolation results. To date it is still unclear how the different components in the collagenase blend accomplish the dissociation of the ECM or which of them are essentially needed for islet release. Novel insights into the crude collagenase product suggests that the native enzyme composition is equally effective as the combination of purified enzyme frac-tions, once the toxic components are removed, but for a fraction of the price of the GMP-compliant enzymes (119).
During decades, the development of enzyme products for islet isolation has been limited by the commercial application of these biological products. New clinical trials in islet transplantation and the availability of new enzyme blends for human islet isolation stimulates both islet researchers and enzyme manufacturers to improve standardization of enzymatic pancreas dissocia-tion and to increase human islet isolation outcome.
27
Pancreas histology: WYSIWYG? (What you see is what you get?) Human islet isolation outcome is characterized by a high variability, making the procedure unpredictable and difficult to standardize. As a result, only 50% of the isolated islet preparations fulfilled the criteria required for clini-cal transplantation: ≥ 5000 IE per kg body weigh of the recipient or 300,000 IE, islet purity >30%, packed tissue volume ≤5 mL and a biphasic insulin response to dynamic glucose perifusion corresponding to a SI of ≥ 2.0.
Several studies suggest that donor body mass index (BMI), age and CIT are critical for successful islet isolation (43, 57). Additional efforts have been made to predict isolation outcome through metabolic testing of the beta-cell mass in the donor (133).
It has been discussed whether islet number and morphology in the native pancreas determines isolation success (134). Characterization of the pancre-atic ECM has provided evidence for correlation of islet yield with the islet morphology in the human pancreas (135). In the pig model, pre-digestion screening of pancreatic biopsies has proven to increase isolation success by selecting the most suitable organs for processing (136). A biopsy taken dur-ing pancreas procurement may help us to decide whether to process a pan-creas for islet isolation or not based on the islet morphological features and the weight of the organ.
28
Material and Methods
Please refer to the appropriate section in the respective papers for descrip-tions of materials and methods. Methods of particular interest are described in this chapter.
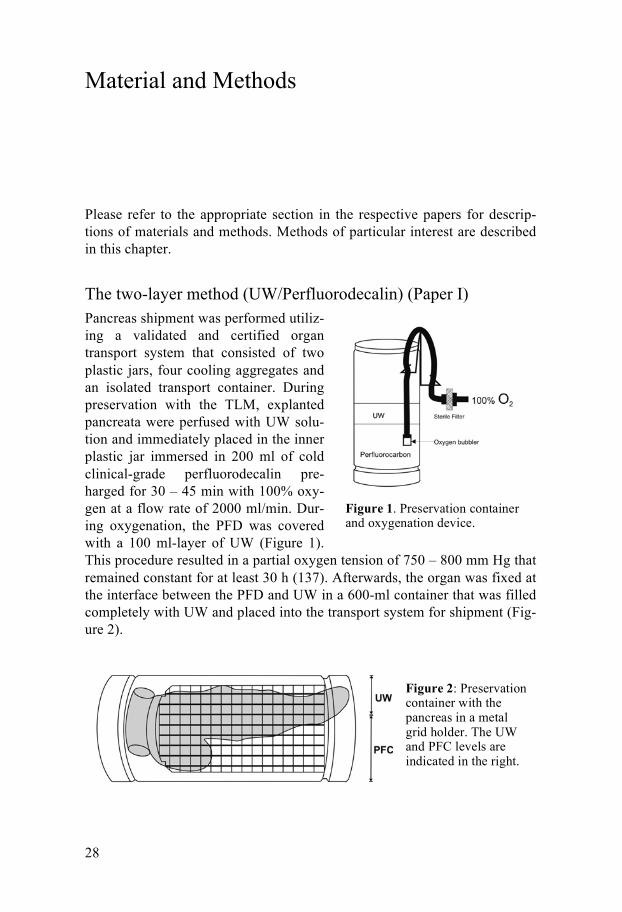
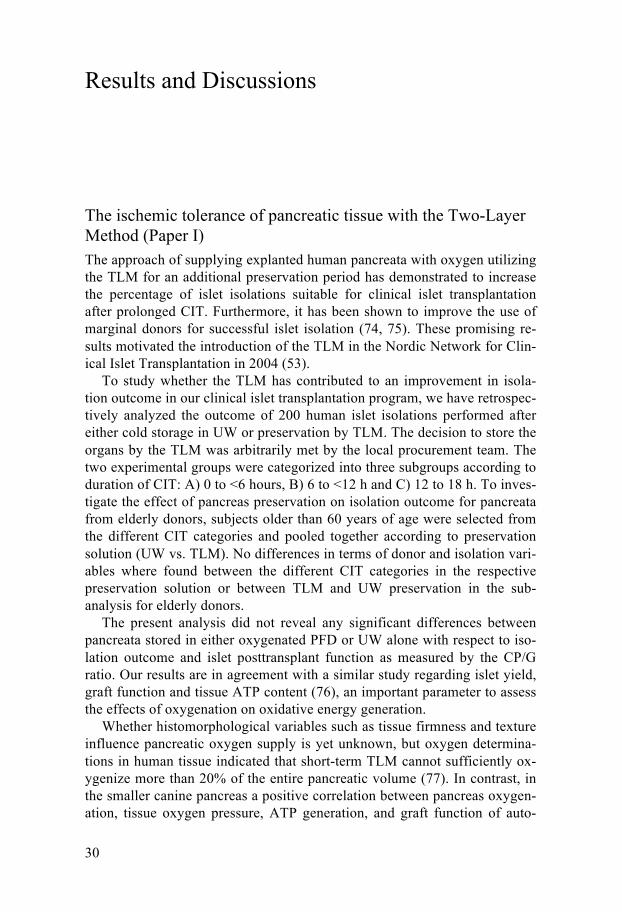
The two-layer method (UW/Perfluorodecalin) (Paper I) Pancreas shipment was performed utiliz-ing a validated and certified organ transport system that consisted of two plastic jars, four cooling aggregates and an isolated transport container. During preservation with the TLM, explanted pancreata were perfused with UW solu-tion and immediately placed in the inner plastic jar immersed in 200 ml of cold clinical-grade perfluorodecalin pre-harged for 30 – 45 min with 100% oxy-gen at a flow rate of 2000 ml/min. Dur-ing oxygenation, the PFD was covered with a 100 ml-layer of UW (Figure 1). This procedure resulted in a partial oxygen tension of 750 – 800 mm Hg that remained constant for at least 30 h (137). Afterwards, the organ was fixed at the interface between the PFD and UW in a 600-ml container that was filled completely with UW and placed into the transport system for shipment (Fig-ure 2).
Figure 1. Preservation container and oxygenation device.
Figure 2: Preservation container with the pancreas in a metal grid holder. The UW and PFC levels are indicated in the right.

29
Characterization of islet morphology by insulin immunostaining (Paper V) The human biopsies used in this study were taken from the head of the pan-creas in a routine fashion after removal of the duodenum, peripancreatic fat and connective tissue and before intraductal enzyme injection. The biopsies were immediately fixed in 4% paraformaldehyde and subsequently dehy-drated in increasing alcohol concentrations (70%, 80%, 95%, absolute alco-hol and xylene) and finally embedded in paraffin. Afterwards they were sectioned on a microtome at 4 µm and air-dried at 37°C overnight. The sec-tions were kept at room temperature until further processing. Prior to stain-ing, the tissue slides were deparaffinized to remove the embedding media and they were rehydrated with decreasing concentrations of alcohol. The sections were stained for insulin using the Envision system, which compris-es the following steps: blocking of endogenous peroxidases with 0.3% H2O2 in PBS (Phosphate buffered saline) for 15 min; incubation with a primary guinea pig anti-human insulin antibody at 37°C over night, followed by goat anti-rabbit Envision antibody, detection in AEC (3-amino-9-ethylcarbazole) substrate-chromogen, counterstaining with hematoxylin and finally embed-ding in glycerol gelatin.
The pancreas slides where digitalized using the digital scanner Aperio SCAN scope XT. The digitalized slides where further analyzed with soft-ware provided by the same company. Islet basic morphological features such as perimeter, area, and diameter were measured directly on the slides. Islet volume was calculated assuming the islets to be perfect spheres. Insulin staining was analyzed utilizing a built-in macro in the Aperio software. Islets were evaluated by determining islet particle number (IN/mm2), islet equiva-lent calculated according to a standard islet diameter of 150 µm, (IE/IN) and percentage of islet (insulin positive) area in the biopsy. Islets were divided into 50 µm diameter ranges as previously described (138).
Statistics All results are presented as mean ± standard error of the mean (SEM)
(Papers I, III, IV and V) or mean ± standard deviation (SD) (Paper II). Com-parisons of continuous variables were carried out by Mann-Whitney test. Categorical variables were analyzed using Fisher’s exact test. In paper I, the comparison of post-transplant CP/G values after each islet infusion between UW and TLM preserved organs was carried out by Wilcoxon test. In the same paper, correlation between CIT and islet yield was calculated by Spearman’s rank test considering a confidence interval of 95%. In Paper V, correlation between morphology parameters and isolation variables is ex-pressed as Pearson correlation coefficient. Differences were considered sig-nificant at P<0.05. P> 0,05 was termed as not significant (NS).
30
Results and Discussions
The ischemic tolerance of pancreatic tissue with the Two-Layer Method (Paper I) The approach of supplying explanted human pancreata with oxygen utilizing the TLM for an additional preservation period has demonstrated to increase the percentage of islet isolations suitable for clinical islet transplantation after prolonged CIT. Furthermore, it has been shown to improve the use of marginal donors for successful islet isolation (74, 75). These promising re-sults motivated the introduction of the TLM in the Nordic Network for Clin-ical Islet Transplantation in 2004 (53).
To study whether the TLM has contributed to an improvement in isola-tion outcome in our clinical islet transplantation program, we have retrospec-tively analyzed the outcome of 200 human islet isolations performed after either cold storage in UW or preservation by TLM. The decision to store the organs by the TLM was arbitrarily met by the local procurement team. The two experimental groups were categorized into three subgroups according to duration of CIT: A) 0 to <6 hours, B) 6 to <12 h and C) 12 to 18 h. To inves-tigate the effect of pancreas preservation on isolation outcome for pancreata from elderly donors, subjects older than 60 years of age were selected from the different CIT categories and pooled together according to preservation solution (UW vs. TLM). No differences in terms of donor and isolation vari-ables where found between the different CIT categories in the respective preservation solution or between TLM and UW preservation in the sub-analysis for elderly donors.
The present analysis did not reveal any significant differences between pancreata stored in either oxygenated PFD or UW alone with respect to iso-lation outcome and islet posttransplant function as measured by the CP/G ratio. Our results are in agreement with a similar study regarding islet yield, graft function and tissue ATP content (76), an important parameter to assess the effects of oxygenation on oxidative energy generation.
Whether histomorphological variables such as tissue firmness and texture influence pancreatic oxygen supply is yet unknown, but oxygen determina-tions in human tissue indicated that short-term TLM cannot sufficiently ox-ygenize more than 20% of the entire pancreatic volume (77). In contrast, in the smaller canine pancreas a positive correlation between pancreas oxygen-ation, tissue oxygen pressure, ATP generation, and graft function of auto-
31
transplanted pancreata was found (139). Another prospective study has demonstrated a protective effect of the TLM on yield and in vitro function of islets isolated from ischemically predamaged canine pancreata (71). Howev-er, experiments in pigs have revealed that TLM-induced restoration of islet function in vitro does not correspond to improved islet function after trans-plantation (140). A study in ischemically predamaged rat pancreata indicates a clear benefit of TLM preservation on subsequent islet isolation and trans-plantation (141). Nevertheless, since oxygen diffusion into the pancreas depends on the thickness of the tissue, the rat pancreas has been considered to be unsuitable as a model of oxygenation of the human pancreas due to the difference in the size of the organ (142).
Our data indicate no beneficial effect of the TLM on islet isolation out-come from elderly donors. Surprisingly, we found a negative correlation between CIT and in vitro function exclusively in TLM-stored pancreata. Moreover, a tendency toward a reduction in the transplantation rate in TLM-stored pancreata (29% vs. 50%) was observed in this donor population.
Another important donor factor that significantly affects human islet iso-lation outcome is donor BMI. Pancreata from obese donors are generally covered by significant amounts of fat (143). Obstructive quantities of fat and connective tissue can interfere with oxygen penetration into the pancreatic core. It seems to be important that pancreata from slim donors are selected for efficient pancreas oxygenation during prolonged storage (72). Alterna-tively, pancreata could be trimmed before preservation with the TLM, thus facilitating oxygen penetration into the tissue, which is usually the case for the short-term oxygenation following cold storage (144, 145).
In conclusion, our analysis of 200 islet isolations from human donor pan-creata that had been stored in UW or preserved by TLM has clearly shown that TLM-mediated oxygenation has no beneficial effect on islet isolation outcome and post-transplant function in type 1 diabetic recipients, when compared to cold storage in UW solution alone. In addition, no protection of marginal pancreata, characterized by increased donor age and/or prolonged CIT, was found after TLM storage. These data indicate that the ischemic tolerance of the human pancreas cannot be extended by oxygenation through the use of TLM.
Lower islet yields using HTK during prolonged pancreas preservation (Paper II) In human islet transplantation, HTK has been proposed as an alternative to UW, providing similar isolation outcome. However, these studies assessed only pancreata preserved for a relatively short period of CIT (87, 88). Cur-rently, efforts are ongoing to centralize clinical islet isolation in highly expe-rienced units to maximize resources and reduce costs (52, 146). On the other
32
hand, this may result in prolonged transportation, thus increasing CIT. The purpose of this study was to investigate whether islets can successfully be isolated from HTK-preserved pancreata after prolonged CIT within the Nor-dic Network for Clinical Islet Transplantation.
In a retrospective analysis including 64 human islet isolations, HTK-perfused pancreata with a CIT of more than 10 hours were matched to or-gans with a CIT of less than 10 hours according to age, BMI, gender, and pancreas weight. Finally, a similar number of UW-perfused organs were selected according to the variables mentioned above.
None of the isolation- and culture-related parameters differed significant-ly among HTK- or UW-perfused pancreata when the effect of CIT (<10 vs. >10 h) was compared. When pancreata were pooled in preservation groups independent of CIT, the trimmed pancreas weight was significantly higher in HTK organs as compared to UW (P=0.039). This finding corresponded to a dry-to-wet weight ratio that was approximately 16% lower after HTK perfu-sion (P=0.007). Regardless of duration of CIT, the volume of HTK utilized for flushing was approximately twice as much compared to UW perfusion volume (P<0.001).
The reduction in islet yield caused by prolonged CIT appeared to be quite marked when HTK was used for preservation. On the other hand, quality assessment did not reveal any significant differences between HTK or UW-perfused organs or between CIT categories within the same preservation group.
The reasons for replacement of UW by HTK can be partially related to economic considerations (80) and the improvement of organ cooling thanks to the high perfusion volume and relatively low pressure (79). Moreover, the specific composition and high viscosity of UW can result in harmful for-mation of adenosine crystals during cold storage (66). The presence of HES can also lead to stimulation of red blood cell aggregation, thereby preventing adequate perfusion of the organ (67). Crystal formation and deposits has not been found in HTK (66, 147). As reviewed in the introduction of this thesis, UW solution must be removed before implantation of the organ because of the high K+ content bearing the risk of undesirable cardiovascular events (68).
The low viscosity of HTK may benefit the clearance of the perfused or-gans compared with UW (148). In this context, it has been speculated whether the adverse effect of HTK on graft survival is related to pancreas edema caused by using high perfusion volumes as recommended by the pro-ducer (86, 148, 149). Although obvious edema was not seen during inspec-tion of the HTK-preserved organs, the dry-to-wet weight ratio clearly indi-cated a higher fluid content in the tissue, probably caused by the higher per-fusion volume of preservation solution. This may explain why islet yield

33
was significantly reduced after HTK perfusion when calculated per gram pancreas but not per whole pancreas as compared to UW storage.
Several islet studies so far did not find any difference between HTK and UW with regard to isolation and post-transplant outcome (87, 88, 150). This is in agreement with numerous studies evaluating the effect of HTK on pan-creas (82, 83, 86), kidney (151), and liver transplantation (152). In contrast, a reduced efficacy of HTK compared with UW was particularly noticed in pancreas (84) and liver transplantation (153) after prolonged cold storage.
The present study suggests that HTK has certain limitations for pancreas preservation prior to human islet isolation in comparison to the UW solution. Although the functional integrity of islets isolated after CIT of >10 h was not affected by HTK preservation, prolonged cold storage resulted in a re-duced islet yield. Nevertheless, no significant difference was found with respect to isolation outcome when CIT was <10 h. Our findings indicate that UW preservation should be preferred when clinical islet transplantation is intended after prolonged CIT.
Vitacyte HA decreases digestion time without damaging islets (Paper III) Islet isolation outcome depends significantly on the efficiency of the enzyme blend utilized for pancreas dissociation. With the withdrawal of Liberase HI, Serva collagenase became the standard enzyme blend utilized for clinical purposes in most centers. Since 2008 a new enzyme named Vitacyte CIzyme collagenase HA (Vitacyte HA) has been available for clinical human islet isolation. This study investigates whether Vitacyte HA can be considered as a significant alternative to Serva collagenase NB1 (Serva NB1) regarding isolation outcome and islet quality.
For that purpose, the outcome of 18 human islet isolations performed with Vitacyte HA was compared to 18 donor-matched pancreata processed with Serva NB1 using identical procedures for isolation and quality assess-ment. In the study, Serva NB1 was complemented with Serva neutral prote-ase NB, whereas Vitacyte HA was complemented with Vitacyte CIzyme thermolysin.
Vitacyte HA and Serva NB1 provided similar islet yield and purity (P=0.076). Although the amount of collagenase activity infused per gram pancreatic tissue (PZ)-U/g was significantly lower for Vitacyte HA com-pared with Serva NB1 (P<0.01), the average digestion time required for sufficient islet release was significantly shorter (P<0.01). Furthermore, the average packed tissue volume per gram pancreas tended to be slightly larger using Vitacyte HA (P=0.058) whereas enzyme selection did not affect the percentage of undigested tissue.
34
The percentage of islets belonging to the different size categories was nearly identical in both experimental groups, indicating that islet integrity was not affected by the choice of enzyme blend. Islet recovery and post-culture purity were also similar. Although the intracellular insulin content was significantly lower in islet isolated with Vitacyte HA (P<0.05), the stimulation index and the profile of dynamic glucose-stimulated insulin re-lease indicated a similar insulin secretory capacity in both groups. The ADP/ATP ratio was significantly lower when islets were isolated using Vitacyte HA (P<0.01).
Among other donor and isolation variables analyzed, only digestion time correlated significantly with the ADP/ATP ratio (P<0.01). No significant differences were found between Vitacyte HA and Serva NB1 regarding the cytokine and tissue factor expression.
The rapid liberation of islets during pancreas digestion is important to minimize the tissue damage induced by the harmful environment character-ized by anoxia and hyperosmolarity (154). This is supported by the finding that islet ADP/ATP ratio correlates with digestion time. Most importantly, the higher efficiency of Vitacyte HA did not deteriorate islet integrity com-pared with Serva NB1 as expressed by similar islet size distribution, survival after culture, insulin secretory capacity, and cytokine expression. Whether the potency of Vitacyte HA is related to a preserved integrity of collagenase class I, as indicated by a slightly increased islet purity (99, 130), or to the application of a complementary protease different from that of Serva NB1 remains to be clarified.
From this study, we conclude that the combination of Vitacyte colla-genase and thermolysin is an efficient enzyme blend for human islet isola-tion, providing isolation results similar to those obtained with Serva NB1. Furthermore, it reduces the digestion time and facilitates a more cost-effective isolation with the use of a lesser amount of enzyme.
Mammalian Tissue-Free Liberase in successful human islet isolation (Paper IV)
After the withdrawal of Liberase HI from the market due to safety rea-sons, the manufacturing company developed a new enzyme blend with simi-lar components, where no mammalian tissue was used in the manufacture process, hence giving the name of the new product: Liberase MTF-S (mam-malian tissue-free)
Together with the islet transplant centers of the University of Leiden (The Netherlands) and Lille (France), we described our first experience with the new GMP-grade enzyme blend Liberase MTF-S. In this multicenter study, 14 human pancreata were processed according to similar isolation protocols (37, 155).
35
Liberase MTF-S was provided by the manufacturer as a premixed blend containing 1570 (PZ)-U of collagenase and 79,328 caseinase units of ther-molysin per vial. In 10 of 14 cases, one vial was used for processing of one pancreas whereas 1.5 vials were administered in four cases. The amount of collagenase and thermolysin was adapted to the pancreas weight due to the large variability in organ weight. The average recirculation time required for islet release was 18.1±1.8 min.
After digestion, the percentage of undigested tissue remaining in the di-gestion chamber was 14.5%±2.1%. Packed tissue volume per gram pancreas was 0.46±0.04 ml/g. Islet yield pre-purification was 416,570±61,840 IE, equivalent to 3660±510 IE/g. Purification failed in 2 of 14 preparations be-cause of technical problems. These preparations were excluded from the study. Of the remaining 12 pancreata, three were considered unsuccessful as they yielded less than 100,000 IE. Islet recovery post-Ficoll reached 65.9%±6.2% with a purity of 59.0%±3.8% and 13.8%±3.2% of embedded islets. After culture, islet survival was 73.9%±4.9%, with similar purity to freshly isolated islets. Islet fragmentation index (islet count/IE) was deter-mined pre-Ficoll (1.0±0.1), post-Ficoll (1.2±0.2), and after culture (1.4±0.2, P=0.05 vs. post-Ficoll).
Quality assessment showed a viability of 86.7%±2.8%, an SI of 2.8±0.7 and intracellular insulin content of 376±91 U/ng DNA. Two of the processed preparations did not respond adequately to glucose stimulation. However, 5 of 12 preparations fulfilled all criteria for clinical islet transplantation.
This data demonstrates that Liberase MTF-S reduces digestion time re-quired for complete human pancreas dissociation and for efficient islet re-lease. The increase of the fragmentation index reflects a certain extent of islet disintegration during islet separation and culture, indicating the aggres-sive character of the MTF-S enzyme. This is additionally stressed by an islet recovery of 74±5%, which is inferior as compared to results obtained with the use of Liberase HI or Serva NB1 (120).
Liberase MTF-S is characterized by a low percentage of degraded colla-genase class I, the collagenase isoform that seems to be responsible for the lot-to-lot variability observed in Liberase HI (130, 156-158). The variability observed in our study reflects most likely a learning curve with this new product, which was characterized by a higher thermolysin to collagenase ratio compared with Liberase HI (158, 159). Indeed, most of the isolations that did not meet the criteria for clinical transplantation were performed during the initial phase of the study.
High doses of non-collagenolytic activities seem to be beneficial for rapid islet release but can deteriorate islet viability, the reason why they should be administered carefully (110). Notably, these results were obtained using a premixed enzyme blend. The efficiency of Liberase MTF-S could be further
36
optimized if it is applied as a two-component product facilitating the indi-vidual adjustment of thermolysin.
Prediction of isolation outcome in the human pancreas (Paper V) The ability to predict isolation outcome could dramatically improve the suc-cess rate of the isolation procedure, save the costs spent for failed islet isola-tions and increase the chance for an islet preparation to be transplanted into a type 1 diabetes recipient.
A previous study observed a positive correlation between the islet mor-phology and isolation outcome, suggesting a possible role of the native islet mass as a determinant factor for isolation success (135).
The current retrospective study was performed to correlate the outcome of strictly standardized isolation procedures with morphometric evaluation of pancreatic biopsies. After insulin staining and digitalization of the pancre-atic slides, islet morphology from 29 human pancreatic routine biopsies was correlated to the outcome of islet isolations performed with validated batch-es of Serva collagenase NB1. Isolations were further categorized as success-ful or unsuccessful if they yielded more or less than 2000 IE/g, respectively.
Donor and isolation variables were similar in successful and unsuccessful isolations except for the digest pellet volume (P=0.0083) and purity (P=0.019) that were higher in the successful group. The mean biopsy area measured 27.61±2.55 mm2 and contained 91.7±8.2 islets or 9.94±0.43 is-lets/mm2. Beta cells (positive insulin staining) covered 1.53±0.2% of the biopsy surface. In average, sectioned islets had a perimeter of 188±8.13 µm, a diameter of 63.55±2.63 µm and an area of 3303±835 µm2. The mean vol-ume of an individual sectioned islet was 429,677±74901 µm3.
On average, almost 50% of the islets were smaller than 50 µm in diameter whereas 15 % were larger than 100 µm and only 4.5% larger than 150 µm. The different size categories were equally distributed in both experimental groups except for the percentage of islets with a diameter between 100 and 150 µm, being higher in biopsies from successful isolations (P=0.051). In our hands, none of the morphological parameters included in this study cor-related with isolated islet yield.
One possible explanation for this finding is that our biopsies were taken from the head of the pancreas, which may not be representative for the whole gland. Previous studies in the native human pancreas demonstrated that the insulin content in the tail is higher as compared to the head (160). This is, however, in contrast to early histology studies suggesting that the human pancreas has a relatively constant islet size distribution throughout the gland with a slightly higher frequency of small islets in the head (134, 161)

37
A previous biopsy study found that islet size and number of islets per de-fined area correlates positively but not significantly with total isolated islet yield in the human pancreas. Nevertheless, in this study samples were taken both from the head and tail of the pancreas (135). Furthermore, the study focused on a semi-quantitative evaluation of the peri-islet tissue rather than on morphological analysis, showing that edema and low interstitial fat con-tent affects negatively the isolated islet yield, which may have implications for enzymatic pancreas digestion (Paper II).
As reported in the pig model, isolations were successfully performed after identifying the presence of large islets in a biopsy as a predictive factor for successful isolation (136). Likewise, in a study by Anazawa et al. (162), the number of native islets in the splenic lobe of the pig pancreas significantly correlated with islet yield.
Since none of the morphological parameters assessed in the present study were predictive for the isolated islet yield, other factors might determine the suitability of a donor pancreas for human islet isolation. Several studies in-dicate that the composition of the collagen fiber matrix (163, 164) and its distribution within the pancreas (165) may be important for the dissociation process. The fact that the extent of islet encapsulation by the collagen matrix is extremely variable has implications for islet integrity and viability during isolation (166). Since CC1, CC2 and neutral protease have no specificity toward the peri-insular extracellular matrix and the intra-islet connective tissue, islets that are not fully covered by the collagen capsule can be dam-aged by the enzymatic digestion (105). Furthermore, total collagen, pancre-atic edema and intraparenchymal fat show a remarkable heterogeneity be-tween individuals, suggesting that along with donor-related factors, varia-tions in the native pancreatic tissue determine isolation outcome (166).
Previous observations that in vitro collagen degradation differs from “re-al” enzymatic pancreas digestion indicate that there is no correlation be-tween the collagen degradation capacity of an enzyme and its capacity to dissociate pancreatic tissue (105). Furthermore, detachment of other struc-tures in the islet-exocrine interface such as cell-to-cell and cell-to-matrix contacts may be an additional requirement for dissociation of pancreatic tissue (167). Taken all together, this indicates that a morphological analysis alone is not a reliable method to predict effective pancreas dissociation and isolation success.
38
Conclusions
Paper I • The two-layer method (PFD/UW) cannot extend the ischem-
ic tolerance of the human pancreas as compared to the UW solution alone.
• The TLM is unable to improve preservation from pancreas from elderly donors.
• Preservation with the TLM does not benefit islet graft func-tion as compared to UW storage.
Paper II • HTK is effective for short-term pancreas preservation as
compared to UW solution. • Tissue edema under HTK preservation may lead to lower
isolation yields from human pancreata with prolonged cold ischemia as compared to storage in UW solution.
Paper III • Vitacyte HA is an efficient enzyme blend for isolation of
human pancreata. • Vitacyte HA provides similar isolation outcome as compared
to Serva NB1, but with shorter digestion time and lesser amount of enzyme.
Paper IV • MTF-Liberase is able to provide successful isolation results
from human pancreata. • The high neutral protease (thermolysin) content present in
MTF-Liberase may damage islet morphological integrity, as seen by the higher islet fragmentation.

39
Paper V • Human islet isolation outcome does not entirely depend on
the native islet mass within the pancreas as evaluated in bi-opsies taken from the head of the pancreas.
40
Future Perspectives
Towards one-to-one equation in clinical islet transplanta-tion The outcome of human islet transplantation has been limited by several trav-ails: pancreas donor shortage, unpredictable isolation outcome, impossibility to diagnose islet rejection, low islet engraftment and reduced long-term graft function. This thesis aimed to improve two of them: pancreas preservation and enzymatic pancreas dissociation. The implementation of the research findings described above will hopefully improve isolation outcome, bringing us closer to the achievement of normoglycemia and insulin independence by transplanting one single islet preparation.
Organ preservation Improvement in the field of organ preservation has been achieved by the use of machine perfusion (168). Preliminary studies in islet isolation from the pig pancreas have shown promising results of machine perfusion as com-pared to cold storage (169). Due to the high cost of this technique, the use of lipophilic and biocompatible carriers for static cold preservation seems to be a reasonable alternative (170).
Enzymatic islet isolation and prediction of isolation outcome Standardization of enzymatic pancreas dissociation is required to improve islet isolation outcome (103). However, it should be complemented with the characterization of the pancreatic tissue due to the inner variability of colla-gen composition in the ECM of the human pancreas (166). Prediction of isolation outcome will most likely depend on our ability to tailor the enzy-matic and separation strategies to the current organ.
41
Summary in Spanish
El trasplante de islotes de Langerhans consiste en restituir las células pro-ductoras de insulina que la diabetes ha destruido. Se prefiere al trasplante de páncreas por su carácter mínimamente invasivo y por el menor riesgo qui-rúrgico, aunque a día de hoy sus resultados a largo plazo son más limitados. Está indicado en pacientes con diabetes tipo 1 que sufren de un control ines-table con hipoglucemias severas inadvertidas, así como en pacientes diabéti-cos trasplantados de riñón y/o con otras complicaciones graves.
El principal problema para su aplicación clínica es la dificultad para ex-traer los islotes del páncreas durante el proceso conocido como “aislamiento de islotes”. Además, la imposibilidad de diagnosticar el rechazo temprano y la inmunosupresión ineficiente condicionan la baja supervivencia del tras-plante a largo plazo.
El trabajo recogido en esta tesis doctoral tiene como objetivos: 1. Optimi-zar la preservación del páncreas durante el transporte desde el quirófano hasta el laboratorio de aislamiento; 2. Mejorar la digestión enzimática del páncreas para liberar los islotes de forma rápida y efectiva, sin dañar su fun-ción; 3. Analizar la anatomía del páncreas como factor determinante en el resultado del aislamiento de islotes humanos.
El estudio sobre la tolerancia isquémica del páncreas previo al aislamien-to de islotes muestran que el método de las dos capas (solución de la Univer-sidad de Wisconsin (UW)/perfluorocarbono) no puede aumentar el tiempo de isquemia fría del páncreas humano. La preservación del páncreas en la solución de histidina-triptófano-ketoglutarato (HTK) previa al aislamiento de islotes es equiparable a la solución de referencia UW a corto plazo, aun-que es limitada a largo plazo, posiblemente debido al edema producido du-rante la perfusión del páncreas del donante. Dos nuevas enzimas, Vitacyte HA y MTF-Liberase, han sido utilizadas para la digestión del páncreas hu-mano con objeto de obtener islotes libres de tejido acinar exocrino. La enzi-ma Vitacyte HA es una colagenasa rápida y eficiente, con unos resultados similares pero con tiempos de digestión más cortos y menor cantidad de enzima que la colagenasa Serva NB1. Además, los primeros aislamientos con la nueva enzima Liberase libre de tejido mamífero (MTF-S) han dado resultados prometedores en cuanto al número de islotes aislados y su viabili-dad así como el porcentaje de trasplantes clínicos. Finalmente hemos demos-trado que el estudio de la histología del páncreas y la morfología de los islo-

42
tes es incapaz de predecir la cantidad de islotes que se van a poder aislar del páncreas humano.
El avance de la técnica de aislamiento contribuirá a la obtención de un número suficiente de islotes para conseguir la independencia insulínica con un solo páncreas. Este es el paso previo para la aplicación clínica del tras-plante de islotes como tratamiento de la diabetes inestable con complicacio-nes graves.
43
Acknowledgements
The work in this thesis was carried out at the Department of Immunology, Genetics and Pathology, former Clinical Immunology division of the De-partment of Oncology, Radiology and Clinical Immunology at Uppsala Uni-versity. I wish to express my sincerest gratitude to everyone who has en-courage me and contributed to this thesis, especially to the following:
First of all I would like to thank my supervisor Olle Korsgren for the possi-bility to work in the field of islet transplantation and for being inspiring and patient. For your unconditional support through the entire PhD studies. With you I have discovered the true meaning of “Oceans of time”.
My co-supervisor Daniel Brandhorst for teaching me how to survive islet isolation, for sharing your huge experience and knowledge in the field. Thanks to Heide Brandhorst for co-supervising my statistics and scientific writing.
My co-supervisor at Karolinska Huddinge Ralf Segersvärd for sharing your enthusiasm and continuous support in the intramuscular islet transplantation project, and for your valuable comments to this thesis.
To my collaborators Andrew Friberg, Torsten Eich, Sana Asif and Torbjörn Lundgren as well as the islet isolation laboratories in Lille and Leiden for supporting my projects with your research expertise and data.
Special thanks to Magnus, Andrew, DongSoo, Ulrika and Mavi, for turning my chaotic scientific English into this doctoral thesis.
To Mona Persson, for taking care of me that rainy October night six years ago, and thereafter. Thanks to Ann-Sofie Lindberg, obrigado amiga!, Anette Lindberg, Elin Ekberg, Anna-Maria Andersson and the rest of the admin-istration at IGP. Thanks to Anna Karin Lidehäll for your coordinating pa-tience and valuable advice.
Past and present members of Clinical Immunology at C11 and C5, the islet isolation facility and quality assessment laboratories, especially to Ulrika Johansson., for taking care of me when I first came to Uppsala, and ever since. “Porque tu lo vales”. I want to listen to you one more time..., Naomi “syrra” Forslund for sharing the frustration and satisfaction of everyday science, Minna Honkanen-Scott, who would have told you that you were going to meet a crazy sauna Spanish guy?, Andrés del Monte Libre for
44
working out the PhD shoulder to shoulder, for helping me with this book and bringing me cereals from the US, Anna Svensson for sharing your true swe-dishness with us, and Angelika Danielsson for putting Ludvika and Prästhyt-tan with its wood-heated sauna on the map.
Graciela Elgue, for enlightening every dark day in the long Swedish winter, and for nice swims and asados argentinos in the short summer nights. There will always be an eternal fight in “el clásico”. To Javier Sánchez, it might be true that if it wasn´t for you I would not be here. In that case I would never have had the pleasure of meeting you and your lovely family.
Valeria Giandomenico and Magnus Essand, for sharing your passion in food and science, bringing together the best of southern and northern Europe.
My colleagues at the department of Endocrine Oncology, especially Barbro Eriksson, Kjell Öberg and Staffan W elin, for showing me a very different side of islet research and for supporting me in the last months of my PhD studies.
Friends and family outside the lab that has contributed to the peaceful work at the lab:
To Lauri and Balázs: “thank you for coming”. For holding our friendship together across time and distance. Punkt, Ende, Tchüss, kein Thema!
To Chepe and Frida, for all the memorable dinners and laughs trying to sur-vive Sweden.
To Becke and Per, thanks to you I found my way back to the two wheels. Vätternrundan is waiting!
To DongSoo for encouraging me in my science carrier over the Atlantic.
Ann-Marie och Martin Egnér, vår svenska mormor och morfar, för att ni mottagit oss in i er familj som om vi alltid hade funnits där. Ni har öppnat, förutom dörren till ert hus även till era hjärtan. Tack vare er kommer Sverige och Uppsala alltid att finnas i våra liv.
Karin Dovelius, för allt vi har lärt varandra om livet och annat när vi bodde hos dig i den idylliska timmerstugan i Norby.
Lena och Peter W allensteen, för att ni alltid tittat till Ana och mig. För att ni visat oss det underbara universitetslivet och delat med er utav er passion för fredsforskning.
A mi familia, mis raíces. Porque sois lo más importante para mi, porque desde España me habéis apoyado en cado paso de mi carrera. A mis padres, porque espero que con esta tesis veáis el fruto de lo que un día sembrasteis y que tanto os ha costado criar.
A Ana, la luz de mi vida. For making every single day an unforgettable day. Come what may…

45
This thesis is dedicated to the memory of the late Professor Fernando Sánchez Gascón. His work as a doctor, lecturer in medicine and as a re-searcher was the source of inspiration for me to start a research career.

46
References
1. Kuzuya T, Matsuda A. Classification of diabetes on the basis of etiologies versus degree of insulin deficiency. Diabetes Care 1997; 20 (2): 219.
2. American Diabetes Association. Standards of Medical Care in Diabetes 2009. Diabetes Care 2009; 32 (Supplement 1): S13.
3. World Health Organization (WHO). Report of a WHO Consultation. Definition, diagnosis and classification of diabetes mellitus and its complications. 1. Diagnosis and classification of diabetes mellitus . WHO/NCD/NCS/99.2. Geneva: WHO., 1999.
4. Makame M. The Diabetes Epidemiology Research International Study Group. Childhood Diabetes, Insulin and Africa., 1992.
5. International Diabetes Federation (IDF). The Diabetes Atlas. Third edition. Brussels: International Diabetes Federation with support of the World Diabetes Foundation, 2008.
6. World Health Organization (WHO). The top 10 causes of death, vol 2011: World Health Organization (WHO), 2008.
7. World Health Organization (WHO). WHO Diabetes Programme: WHO, 2009.
8. Diabetes Care and Research in Europe: The St Vincent Declaration 1989. Istambul: The St Vicent Declaration Diabetes Action Programme, 1999.
9. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004; 27 (5): 1047.
10. International Diabetes Federation (IDF). The Diabetes Atlas. Fourth edition.: International Diabetes Federation, 2009.
11. Yang W, Lu J, Weng J, et al. Prevalence of diabetes among men and women in China. The New England journal of medicine 2010; 362 (12): 1090.
12. Mbanya JCobotIDF. New diabetes figures in China: IDF press statement. Brussels, 2010.
13. Svenskt Njurregister (SNR). Aktiv uremivård i Sverige 1991-2010. 2010.
14. Zierler K. Whole body glucose metabolism. The American journal of physiology 1999; 276 (3 Pt 1): E409.
15. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus. N Engl J Med 1993; 329 (14): 977.
47
16. Nathan DM, Cleary PA, Backlund JY, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. The New England journal of medicine 2005; 353 (25): 2643.
17. Hypoglycemia in the Diabetes Control and Complications Trial. The Diabetes Control and Complications Trial Research Group. Diabetes 1997; 46 (2): 271.
18. Ulrik Pedersen-Bjergaard SP, Simon R Heller, Tara M Wallace, Åse K Rasmussen, Hanne V Jørgensen, David R Matthews, Philip Hougaard, Birger Thorsteinsson,. Severe hypoglycaemia in 1076 adult patients with type 1 diabetes: influence of risk markers and selection. Diabetes/Metabolism Research and Reviews 2004; 20 (6): 479.
19. Cryer PE. Hypoglycaemia: the limiting factor in the glycaemic management of Type I and Type II diabetes. Diabetologia 2002; 45 (7): 937.
20. Cryer PE. The barrier of hypoglycemia in diabetes. Diabetes 2008; 57 (12): 3169.
21. Raju B, Cryer PE. Loss of the decrement in intraislet insulin plausibly explains loss of the glucagon response to hypoglycemia in insulin-deficient diabetes: documentation of the intraislet insulin hypothesis in humans. Diabetes 2005; 54 (3): 757.
22. Cryer PE. Hypoglycemia in type 1 diabetes mellitus. Endocrinology and metabolism clinics of North America 2010; 39 (3): 641.
23. Bolli G, de Feo P, Compagnucci P, et al. Abnormal glucose counterregulation in insulin-dependent diabetes mellitus. Interaction of anti-insulin antibodies and impaired glucagon and epinephrine secretion. Diabetes 1983; 32 (2): 134.
24. Popp DA, Shah SD, Cryer PE. Role of epinephrine-mediated beta-adrenergic mechanisms in hypoglycemic glucose counterregulation and posthypoglycemic hyperglycemia in insulin-dependent diabetes mellitus. J Clin Invest 1982; 69 (2): 315.
25. Amiel SA, Sherwin RS, Simonson DC, Tamborlane WV. Effect of intensive insulin therapy on glycemic thresholds for counterregulatory hormone release. Diabetes 1988; 37 (7): 901.
26. Dagogo-Jack S, Rattarasarn C, Cryer PE. Reversal of hypoglycemia unawareness, but not defective glucose counterregulation, in IDDM. Diabetes 1994; 43 (12): 1426.
27. Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control in Type 1 diabetes: meta-analysis of multiple daily insulin injections compared with continuous subcutaneous insulin infusion. Diabetic medicine : a journal of the British Diabetic Association 2008; 25 (7): 765.
28. Tamborlane WV, Beck RW, Bode BW, et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes. The New England journal of medicine 2008; 359 (14): 1464.
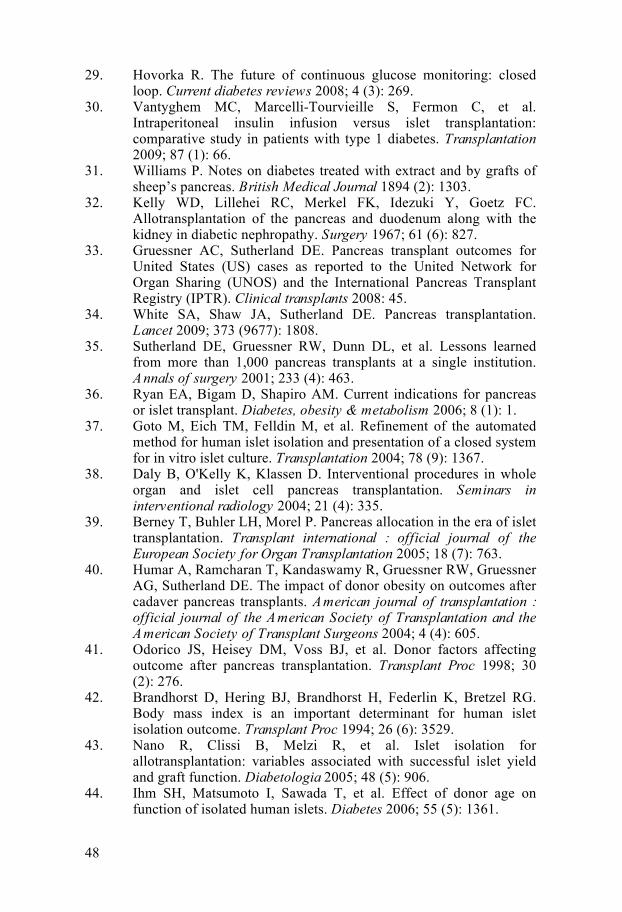
48
29. Hovorka R. The future of continuous glucose monitoring: closed loop. Current diabetes reviews 2008; 4 (3): 269.
30. Vantyghem MC, Marcelli-Tourvieille S, Fermon C, et al. Intraperitoneal insulin infusion versus islet transplantation: comparative study in patients with type 1 diabetes. Transplantation 2009; 87 (1): 66.
31. Williams P. Notes on diabetes treated with extract and by grafts of sheep’s pancreas. British Medical Journal 1894 (2): 1303.
32. Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery 1967; 61 (6): 827.
33. Gruessner AC, Sutherland DE. Pancreas transplant outcomes for United States (US) cases as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR). Clinical transplants 2008: 45.
34. White SA, Shaw JA, Sutherland DE. Pancreas transplantation. Lancet 2009; 373 (9677): 1808.
35. Sutherland DE, Gruessner RW, Dunn DL, et al. Lessons learned from more than 1,000 pancreas transplants at a single institution. Annals of surgery 2001; 233 (4): 463.
36. Ryan EA, Bigam D, Shapiro AM. Current indications for pancreas or islet transplant. Diabetes, obesity & metabolism 2006; 8 (1): 1.
37. Goto M, Eich TM, Felldin M, et al. Refinement of the automated method for human islet isolation and presentation of a closed system for in vitro islet culture. Transplantation 2004; 78 (9): 1367.
38. Daly B, O'Kelly K, Klassen D. Interventional procedures in whole organ and islet cell pancreas transplantation. Seminars in interventional radiology 2004; 21 (4): 335.
39. Berney T, Buhler LH, Morel P. Pancreas allocation in the era of islet transplantation. Transplant international : official journal of the European Society for Organ Transplantation 2005; 18 (7): 763.
40. Humar A, Ramcharan T, Kandaswamy R, Gruessner RW, Gruessner AG, Sutherland DE. The impact of donor obesity on outcomes after cadaver pancreas transplants. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons 2004; 4 (4): 605.
41. Odorico JS, Heisey DM, Voss BJ, et al. Donor factors affecting outcome after pancreas transplantation. Transplant Proc 1998; 30 (2): 276.
42. Brandhorst D, Hering BJ, Brandhorst H, Federlin K, Bretzel RG. Body mass index is an important determinant for human islet isolation outcome. Transplant Proc 1994; 26 (6): 3529.
43. Nano R, Clissi B, Melzi R, et al. Islet isolation for allotransplantation: variables associated with successful islet yield and graft function. Diabetologia 2005; 48 (5): 906.
44. Ihm SH, Matsumoto I, Sawada T, et al. Effect of donor age on function of isolated human islets. Diabetes 2006; 55 (5): 1361.
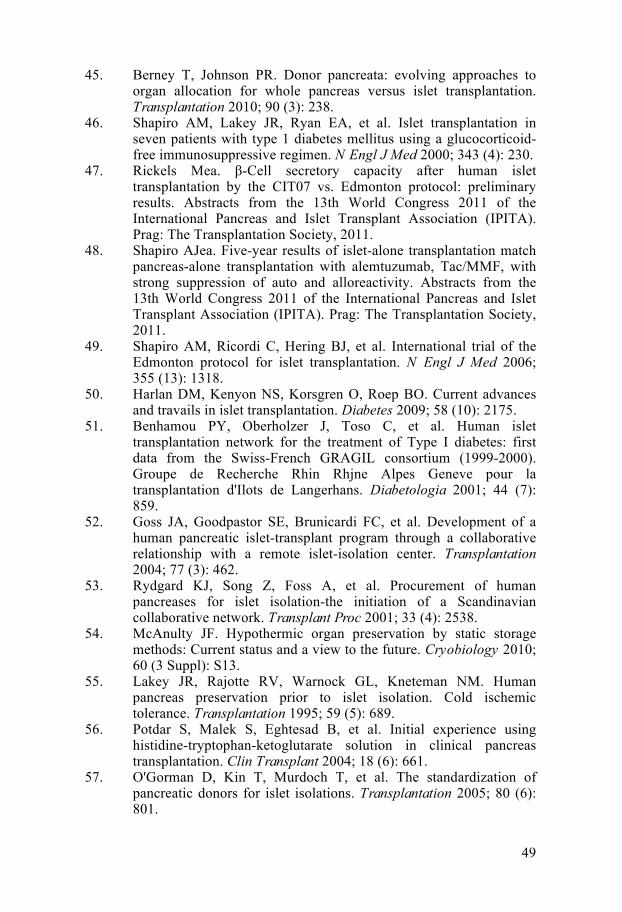
49
45. Berney T, Johnson PR. Donor pancreata: evolving approaches to organ allocation for whole pancreas versus islet transplantation. Transplantation 2010; 90 (3): 238.
46. Shapiro AM, Lakey JR, Ryan EA, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000; 343 (4): 230.
47. Rickels Mea. β-Cell secretory capacity after human islet transplantation by the CIT07 vs. Edmonton protocol: preliminary results. Abstracts from the 13th World Congress 2011 of the International Pancreas and Islet Transplant Association (IPITA). Prag: The Transplantation Society, 2011.
48. Shapiro AJea. Five-year results of islet-alone transplantation match pancreas-alone transplantation with alemtuzumab, Tac/MMF, with strong suppression of auto and alloreactivity. Abstracts from the 13th World Congress 2011 of the International Pancreas and Islet Transplant Association (IPITA). Prag: The Transplantation Society, 2011.
49. Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006; 355 (13): 1318.
50. Harlan DM, Kenyon NS, Korsgren O, Roep BO. Current advances and travails in islet transplantation. Diabetes 2009; 58 (10): 2175.
51. Benhamou PY, Oberholzer J, Toso C, et al. Human islet transplantation network for the treatment of Type I diabetes: first data from the Swiss-French GRAGIL consortium (1999-2000). Groupe de Recherche Rhin Rhjne Alpes Geneve pour la transplantation d'Ilots de Langerhans. Diabetologia 2001; 44 (7): 859.
52. Goss JA, Goodpastor SE, Brunicardi FC, et al. Development of a human pancreatic islet-transplant program through a collaborative relationship with a remote islet-isolation center. Transplantation 2004; 77 (3): 462.
53. Rydgard KJ, Song Z, Foss A, et al. Procurement of human pancreases for islet isolation-the initiation of a Scandinavian collaborative network. Transplant Proc 2001; 33 (4): 2538.
54. McAnulty JF. Hypothermic organ preservation by static storage methods: Current status and a view to the future. Cryobiology 2010; 60 (3 Suppl): S13.
55. Lakey JR, Rajotte RV, Warnock GL, Kneteman NM. Human pancreas preservation prior to islet isolation. Cold ischemic tolerance. Transplantation 1995; 59 (5): 689.
56. Potdar S, Malek S, Eghtesad B, et al. Initial experience using histidine-tryptophan-ketoglutarate solution in clinical pancreas transplantation. Clin Transplant 2004; 18 (6): 661.
57. O'Gorman D, Kin T, Murdoch T, et al. The standardization of pancreatic donors for islet isolations. Transplantation 2005; 80 (6): 801.
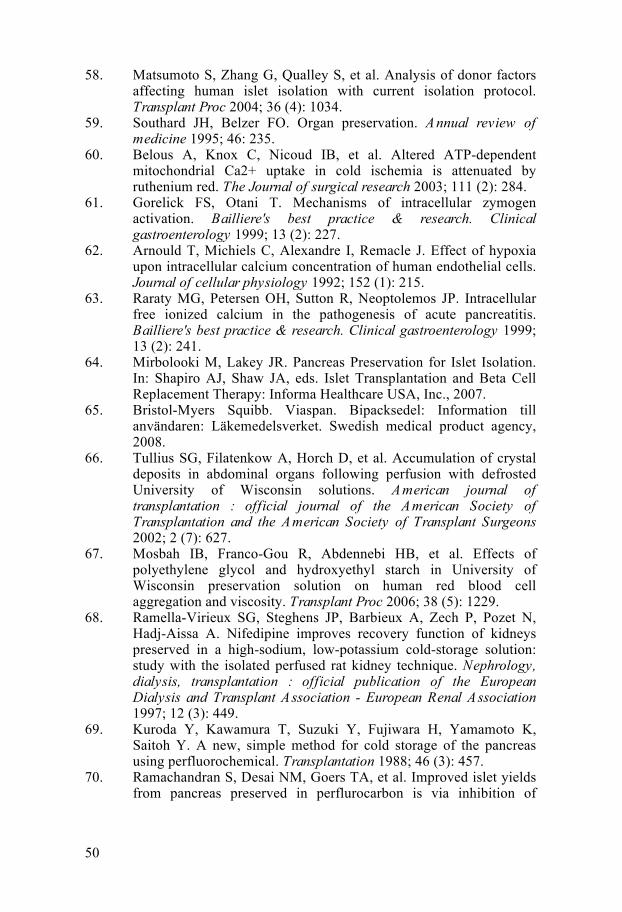
50
58. Matsumoto S, Zhang G, Qualley S, et al. Analysis of donor factors affecting human islet isolation with current isolation protocol. Transplant Proc 2004; 36 (4): 1034.
59. Southard JH, Belzer FO. Organ preservation. Annual review of medicine 1995; 46: 235.
60. Belous A, Knox C, Nicoud IB, et al. Altered ATP-dependent mitochondrial Ca2+ uptake in cold ischemia is attenuated by ruthenium red. The Journal of surgical research 2003; 111 (2): 284.
61. Gorelick FS, Otani T. Mechanisms of intracellular zymogen activation. Bailliere's best practice & research. Clinical gastroenterology 1999; 13 (2): 227.
62. Arnould T, Michiels C, Alexandre I, Remacle J. Effect of hypoxia upon intracellular calcium concentration of human endothelial cells. Journal of cellular physiology 1992; 152 (1): 215.
63. Raraty MG, Petersen OH, Sutton R, Neoptolemos JP. Intracellular free ionized calcium in the pathogenesis of acute pancreatitis. Bailliere's best practice & research. Clinical gastroenterology 1999; 13 (2): 241.
64. Mirbolooki M, Lakey JR. Pancreas Preservation for Islet Isolation. In: Shapiro AJ, Shaw JA, eds. Islet Transplantation and Beta Cell Replacement Therapy: Informa Healthcare USA, Inc., 2007.
65. Bristol-Myers Squibb. Viaspan. Bipacksedel: Information till användaren: Läkemedelsverket. Swedish medical product agency, 2008.
66. Tullius SG, Filatenkow A, Horch D, et al. Accumulation of crystal deposits in abdominal organs following perfusion with defrosted University of Wisconsin solutions. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons 2002; 2 (7): 627.
67. Mosbah IB, Franco-Gou R, Abdennebi HB, et al. Effects of polyethylene glycol and hydroxyethyl starch in University of Wisconsin preservation solution on human red blood cell aggregation and viscosity. Transplant Proc 2006; 38 (5): 1229.
68. Ramella-Virieux SG, Steghens JP, Barbieux A, Zech P, Pozet N, Hadj-Aissa A. Nifedipine improves recovery function of kidneys preserved in a high-sodium, low-potassium cold-storage solution: study with the isolated perfused rat kidney technique. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association 1997; 12 (3): 449.
69. Kuroda Y, Kawamura T, Suzuki Y, Fujiwara H, Yamamoto K, Saitoh Y. A new, simple method for cold storage of the pancreas using perfluorochemical. Transplantation 1988; 46 (3): 457.
70. Ramachandran S, Desai NM, Goers TA, et al. Improved islet yields from pancreas preserved in perflurocarbon is via inhibition of
51
apoptosis mediated by mitochondrial pathway. Am J Transplant 2006; 6 (7): 1696.
71. Deai T, Tanioka Y, Suzuki Y, Kuroda Y. The effect of the two-layer cold storage method on islet isolation from ischemically damaged pancreas. The Kobe journal of medical sciences 1999; 45 (3-4): 191.
72. Salehi P, Mirbolooki M, Kin T, et al. Ameliorating injury during preservation and isolation of human islets using the two-layer method with perfluorocarbon and UW solution. Cell Transplant 2006; 15 (2): 187.
73. Tsujimura T, Kuroda Y, Churchill TA, et al. Short-term storage of the ischemically damaged human pancreas by the two-layer method prior to islet isolation. Cell Transplant 2004; 13 (1): 67.
74. Ricordi C, Fraker C, Szust J, et al. Improved human islet isolation outcome from marginal donors following addition of oxygenated perfluorocarbon to the cold-storage solution. Transplantation 2003; 75 (9): 1524.
75. Tsujimura T, Kuroda Y, Kin T, et al. Human islet transplantation from pancreases with prolonged cold ischemia using additional preservation by the two-layer (UW solution/perfluorochemical) cold-storage method. Transplantation 2002; 74 (12): 1687.
76. Kin T, Mirbolooki M, Salehi P, et al. Islet isolation and transplantation outcomes of pancreas preserved with University of Wisconsin solution versus two-layer method using preoxygenated perfluorocarbon. Transplantation 2006; 82 (10): 1286.
77. Papas KK, Hering BJ, Guenther L, Rappel MJ, Colton CK, Avgoustiniatos ES. Pancreas oxygenation is limited during preservation with the two-layer method. Transplant Proc 2005; 37 (8): 3501.
78. Bretschneider HJ. Myocardial protection. Thorac Cardiovasc Surg 1980; 28 (5): 295.
79. Troisi R, Meester D, Regaert B, et al. Physiologic and metabolic results of pancreatic cold storage with Histidine-Tryptophan-Ketoglutarate-HTK solution (Custodiol) in the porcine autotransplantation model. Transplant international : official journal of the European Society for Organ Transplantation 2000; 13 (2): 98.
80. Fridell JA, Mangus RS, Tector AJ. Clinical experience with histidine-tryptophan-ketoglutarate solution in abdominal organ preservation: a review of recent literature. Clinical transplantation 2009; 23 (3): 305.
81. Alonso D, Dunn TB, Rigley T, et al. Increased pancreatitis in allografts flushed with histidine-tryptophan-ketoglutarate solution: a cautionary tale. Am J Transplant 2008; 8 (9): 1942.
82. Englesbe MJ, Moyer A, Kim DY, et al. Early pancreas transplant outcomes with histidine-tryptophan-ketoglutarate preservation: a multicenter study. Transplantation 2006; 82 (1): 136.
83. Schneeberger S, Biebl M, Steurer W, et al. A prospective randomized multicenter trial comparing histidine-tryptophane-
52
ketoglutarate versus University of Wisconsin perfusion solution in clinical pancreas transplantation. Transpl Int 2009; 22 (2): 217.
84. Stewart ZA, Cameron AM, Singer AL, Dagher NN, Montgomery RA, Segev DL. Histidine-tryptophan-ketoglutarate (HTK) is associated with reduced graft survival in pancreas transplantation. Am J Transplant 2009; 9 (1): 217.
85. Becker T, Ringe B, Nyibata M, et al. Pancreas transplantation with histidine-tryptophan-ketoglutarate (HTK) solution and University of Wisconsin (UW) solution: is there a difference? JOP 2007; 8 (3): 304.
86. Fridell JA, Mangus RS, Powelson JA. Histidine-tryptophan-ketoglutarate for pancreas allograft preservation: the Indiana University experience. Am J Transplant 2010; 10 (5): 1284.
87. Brandhorst H, Hering BJ, Brandhorst D, et al. Comparison of histidine-tryptophane-ketoglutarate (HTK) and University of Wisconsin (UW) solution for pancreas perfusion prior to islet isolation, culture and transplantation. Transplant Proc 1995; 27 (6): 3175.
88. Salehi P, Hansen MA, Avila JG, et al. Human islet isolation outcomes from pancreata preserved with Histidine-Tryptophan Ketoglutarate versus University of Wisconsin solution. Transplantation 2006; 82 (7): 983.
89. Moskalewski S. Isolation and Culture of the Islets of Langerhans of the Guinea Pig. Gen Comp Endocrinol 1965; 44: 342.
90. Lacy PE, Kostianovsky M. Method for the isolation of intact islets of Langerhans from the rat pancreas. Diabetes 1967; 16 (1): 35.
91. Horaguchi A, Merrell RC. Preparation of viable islet cells from dogs by a new method. Diabetes 1981; 30 (5): 455.
92. Scharp DW, Kemp CB, Knight MJ, Ballinger WF, Lacy PE. The use of ficoll in the preparation of viable islets of langerhans from the rat pancreas. Transplantation 1973; 16 (6): 686.
93. Ricordi C, Lacy PE, Finke EH, Olack BJ, Scharp DW. Automated method for isolation of human pancreatic islets. Diabetes 1988; 37 (4): 413.
94. Gray DW, McShane P, Grant A, Morris PJ. A method for isolation of islets of Langerhans from the human pancreas. Diabetes 1984; 33 (11): 1055.
95. Lakey JR, Burridge PW, Shapiro AM. Technical aspects of islet preparation and transplantation. Transpl Int 2003; 16 (9): 613.
96. Islet transplantation and beta cell replacement therapy: Informa Healthcare USA, Inc, 2007: 16.
97. Van Deijnen JH, Van Suylichem PT, Wolters GH, Van Schilfgaarde R. Distribution of collagens type I, type III and type V in the pancreas of rat, dog, pig and man. Cell and tissue research 1994; 277 (1): 115.
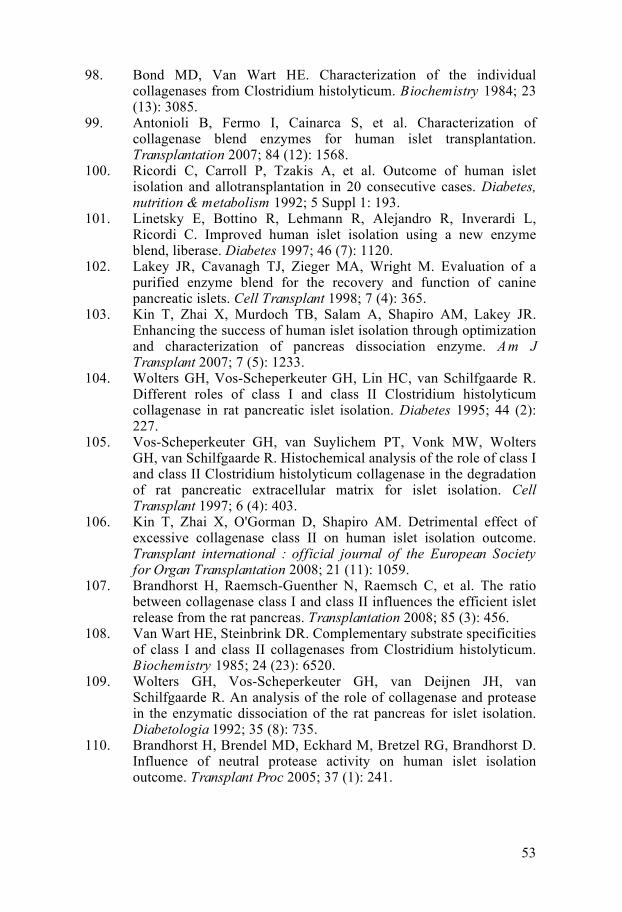
53
98. Bond MD, Van Wart HE. Characterization of the individual collagenases from Clostridium histolyticum. Biochemistry 1984; 23 (13): 3085.
99. Antonioli B, Fermo I, Cainarca S, et al. Characterization of collagenase blend enzymes for human islet transplantation. Transplantation 2007; 84 (12): 1568.
100. Ricordi C, Carroll P, Tzakis A, et al. Outcome of human islet isolation and allotransplantation in 20 consecutive cases. Diabetes, nutrition & metabolism 1992; 5 Suppl 1: 193.
101. Linetsky E, Bottino R, Lehmann R, Alejandro R, Inverardi L, Ricordi C. Improved human islet isolation using a new enzyme blend, liberase. Diabetes 1997; 46 (7): 1120.
102. Lakey JR, Cavanagh TJ, Zieger MA, Wright M. Evaluation of a purified enzyme blend for the recovery and function of canine pancreatic islets. Cell Transplant 1998; 7 (4): 365.
103. Kin T, Zhai X, Murdoch TB, Salam A, Shapiro AM, Lakey JR. Enhancing the success of human islet isolation through optimization and characterization of pancreas dissociation enzyme. Am J Transplant 2007; 7 (5): 1233.
104. Wolters GH, Vos-Scheperkeuter GH, Lin HC, van Schilfgaarde R. Different roles of class I and class II Clostridium histolyticum collagenase in rat pancreatic islet isolation. Diabetes 1995; 44 (2): 227.
105. Vos-Scheperkeuter GH, van Suylichem PT, Vonk MW, Wolters GH, van Schilfgaarde R. Histochemical analysis of the role of class I and class II Clostridium histolyticum collagenase in the degradation of rat pancreatic extracellular matrix for islet isolation. Cell Transplant 1997; 6 (4): 403.
106. Kin T, Zhai X, O'Gorman D, Shapiro AM. Detrimental effect of excessive collagenase class II on human islet isolation outcome. Transplant international : official journal of the European Society for Organ Transplantation 2008; 21 (11): 1059.
107. Brandhorst H, Raemsch-Guenther N, Raemsch C, et al. The ratio between collagenase class I and class II influences the efficient islet release from the rat pancreas. Transplantation 2008; 85 (3): 456.
108. Van Wart HE, Steinbrink DR. Complementary substrate specificities of class I and class II collagenases from Clostridium histolyticum. Biochemistry 1985; 24 (23): 6520.
109. Wolters GH, Vos-Scheperkeuter GH, van Deijnen JH, van Schilfgaarde R. An analysis of the role of collagenase and protease in the enzymatic dissociation of the rat pancreas for islet isolation. Diabetologia 1992; 35 (8): 735.
110. Brandhorst H, Brendel MD, Eckhard M, Bretzel RG, Brandhorst D. Influence of neutral protease activity on human islet isolation outcome. Transplant Proc 2005; 37 (1): 241.
54
111. Bucher P, Bosco D, Mathe Z, et al. Optimization of neutral protease to collagenase activity ratio for islet of Langerhans isolation. Transplant Proc 2004; 36 (4): 1145.
112. Brandhorst H, Alt A, Huettler S, et al. The ratio between class II and class I collagenase determines the amount of neutral protease activity required for efficient islet release from the rat pancreas. Transplant Proc 2005; 37 (1): 215.
113. Johnson PRV, White SA, London NJM. Collagenase and human islet isolation. Cell Transplant 1996; 5 (4): 437.
114. Kin T, Johnson PR, Shapiro AM, Lakey JR. Factors influencing the collagenase digestion phase of human islet isolation. Transplantation 2007; 83 (1): 7.
115. Fetterhoff TJ, Cavanagh TJ, Wile KJ, et al. Human pancreatic dissociation using a purified enzyme blend. Transplant Proc 1995; 27 (6): 3282.
116. Gill JF, Chambers LL, Baurley JL, et al. Safety testing of Liberase, a purified enzyme blend for human islet isolation. Transplant Proc 1995; 27 (6): 3276.
117. Brandhorst H, Brandhorst D, Hesse F, et al. Successful human islet isolation utilizing recombinant collagenase. Diabetes 2003; 52 (5): 1143.
118. Brandhorst H, Friberg A, Andersson HH, et al. The importance of tryptic-like activity in purified enzyme blends for efficient islet isolation. Transplantation 2009; 87 (3): 370.
119. Wang Y, Paushter D, Wang S, et al. Highly Purified versus Filtered Crude Collagenase: Comparable Human Islet Isolation Outcomes. Cell Transplant 2011.
120. Brandhorst H, Friberg A, Nilsson B, et al. Large-scale comparison of Liberase HI and collagenase NB1 utilized for human islet isolation. Cell Transplant 2010; 19 (1): 3.
121. Kin T, O'Gorman D, Senior P, Shapiro AM. Experience of islet isolation without neutral protease supplementation. Islets 2010; 2 (5): 278.
122. Brandhorst H, Raemsch-Guenther N, Raemsch C, et al. Degraded collagenase deteriorates islet viability. Transplant Proc 2008; 40 (2): 370.
123. Linetsky E, Inverardi L, Kenyon NS, Alejandro R, Ricordi C. Endotoxin contamination of reagents used during isolation and purification of human pancreatic islets. Transplant Proc 1998; 30 (2): 345.
124. Berney T, Molano RD, Cattan P, et al. Endotoxin-mediated delayed islet graft function is associated with increased intra-islet cytokine production and islet cell apoptosis. Transplantation 2001; 71 (1): 125.
125. Eckhardt T, Jahr H, Federlin K, Bretzel RG. Endotoxin impairs the engraftment of rat islets transplanted beneath the kidney capsule of C57BL/6-mice. Journal of molecular medicine 1999; 77 (1): 123.
55
126. Vargas F, Vives-Pi M, Somoza N, et al. Endotoxin contamination may be responsible for the unexplained failure of human pancreatic islet transplantation. Transplantation 1998; 65 (5): 722.
127. Kin T, O'Gorman D, Zhai X, et al. Nonsimultaneous administration of pancreas dissociation enzymes during islet isolation. Transplantation 2009; 87 (11): 1700.
128. International Society for Cellular Therapy. Risk of bovine spongiform
encephalopathy (BSE) in collagenase enzymes, 2007. 129. Alejandro R, Barton FB, Hering BJ, Wease S. 2008 Update from the
Collaborative Islet Transplant Registry. Transplantation 2008; 86 (12): 1783.
130. Balamurugan AN, Breite AG, Anazawa T, et al. Successful human islet isolation and transplantation indicating the importance of class 1 collagenase and collagen degradation activity assay. Transplantation 2010; 89 (8): 954.
131. CITR. Collaborative Islet Transplant Registry: Sixth Annual Report. Rockville, MD: The EMMES Corporation, 2009.
132. O'Gorman D, Kin T, Imes S, Pawlick R, Senior P, Shapiro AM. Comparison of human islet isolation outcomes using a new mammalian tissue-free enzyme versus collagenase NB-1. Transplantation 2010; 90 (3): 255.
133. Hubert T, Strecker G, Gmyr V, et al. Acute insulin response to arginine in deceased donors predicts the outcome of human islet isolation. Am J Transplant 2008; 8 (4): 872.
134. Saito K, Iwama N, Takahashi T. Morphometrical analysis on topographical difference in size distribution, number and volume of islets in the human pancreas. The Tohoku journal of experimental medicine 1978; 124 (2): 177.
135. Mahler R, Franke FE, Hering BJ, et al. Evidence for a significant correlation of donor pancreas morphology and the yield of isolated purified human islets. Journal of molecular medicine 1999; 77 (1): 87.
136. Krickhahn M, Buhler C, Meyer T, Thiede A, Ulrichs K. The morphology of islets within the porcine donor pancreas determines the isolation result: successful isolation of pancreatic islets can now be achieved from young market pigs. Cell Transplant 2002; 11 (8): 827.
137. Brandhorst D, Bretzel RG, Brandhorst H. Oxygen and pancreas preservation: reply. Transplantation 2006; 81 (3): 492; author reply 492.
138. Ricordi C, Gray DW, Hering BJ, et al. Islet isolation assessment in man and large animals. Acta diabetologica latina 1990; 27 (3): 185.
139. Matsumoto S, Kuroda Y, Hamano M, et al. Direct evidence of pancreatic tissue oxygenation during preservation by the two-layer method. Transplantation 1996; 62 (11): 1667.
56
140. Brandhorst D, Iken M, Bretzel RG, Brandhorst H. Pancreas storage in oxygenated perfluorodecalin does not restore post-transplant function of isolated pig islets pre-damaged by warm ischemia. Xenotransplantation 2006; 13 (5): 465.
141. Tanaka T, Suzuki Y, Tanioka Y, et al. Possibility of islet transplantation from a nonheartbeating donor pancreas resuscitated by the two-layer method. Transplantation 2005; 80 (6): 738.
142. Avgoustiniatos ES, Hering BJ, Papas KK. The rat pancreas is not an appropriate model for testing the preservation of the human pancreas with the two-layer method. Transplantation 2006; 81 (10): 1471.
143. Brandhorst H, Brandhorst D, Hering BJ, Federlin K, Bretzel RG. Body mass index of pancreatic donors: a decisive factor for human islet isolation. Experimental and clinical endocrinology & diabetes : official journal, German Society of Endocrinology [and] German Diabetes Association 1995; 103 Suppl 2: 23.
144. Matsumoto S, Rigley TH, Qualley SA, Kuroda Y, Reems JA, Stevens RB. Efficacy of the oxygen-charged static two-layer method for short-term pancreas preservation and islet isolation from nonhuman primate and human pancreata. Cell Transplant 2002; 11 (8): 769.
145. Matsumoto S, Qualley SA, Goel S, et al. Effect of the two-layer (University of Wisconsin solution-perfluorochemical plus O2) method of pancreas preservation on human islet isolation, as assessed by the Edmonton Isolation Protocol. Transplantation 2002; 74 (10): 1414.
146. Guignard AP, Oberholzer J, Benhamou PY, et al. Cost analysis of human islet transplantation for the treatment of type 1 diabetes in the Swiss-French Consortium GRAGIL. Diabetes Care 2004; 27 (4): 895.
147. Fischer JH, Jeschkeit S. Effectivity of freshly prepared or refreshed solutions for heart preservation versus commercial EuroCollins, Bretschneider's HTK or University of Wisconsin solution. Transplantation 1995; 59 (9): 1259.
148. Mangus RS, Tector AJ, Fridell JA, Kazimi M, Hollinger E, Vianna RM. Comparison of histidine-tryptophan-ketoglutarate solution and University of Wisconsin solution in intestinal and multivisceral transplantation. Transplantation 2008; 86 (2): 298.
149. Agarwal A, Powelson JA, Goggins WC, Milgrom ML, Fridell JA. Organ preservation with histidine-tryptophan ketogluatarate solution in clinical pancreas transplantation: an update of the indiana university experience. Transplant Proc 2008; 40 (2): 498.
150. Brendel MD, Eckhard M, Brandhorst D, Brandhorst H, Bretzel RG. HTK storage for pancreatic grafts prior to human islet isolation and clinical transplantation. In: Hesse, U. J.; de Hemptinne, B., eds. Contributions to transplantation. Lengerich-Berlin-Düsseldorf-Leipzig: Pabst Science Publishers; 1999:180-189, 1999.
57
151. de Boer J, De Meester J, Smits JM, et al. Eurotransplant randomized multicenter kidney graft preservation study comparing HTK with UW and Euro-Collins. Transplant international : official journal of the European Society for Organ Transplantation 1999; 12 (6): 447.
152. Mangus RS, Tector AJ, Agarwal A, Vianna R, Murdock P, Fridell JA. Comparison of histidine-tryptophan-ketoglutarate solution (HTK) and University of Wisconsin solution (UW) in adult liver transplantation. Liver Transpl 2006; 12 (2): 226.
153. Stewart ZA, Cameron AM, Singer AL, Montgomery RA, Segev DL. Histidine-Tryptophan-Ketoglutarate (HTK) is associated with reduced graft survival in deceased donor livers, especially those donated after cardiac death. Am J Transplant 2009; 9 (2): 286.
154. Bottino R, Balamurugan AN, Tse H, et al. Response of human islets to isolation stress and the effect of antioxidant treatment. Diabetes 2004; 53 (10): 2559.
155. Hubert T, Gmyr V, Arnalsteen L, et al. Influence of preservation solution on human islet isolation outcome. Transplantation 2007; 83 (3): 270.
156. Barnett MJ, Zhai X, LeGatt DF, Cheng SB, Shapiro AM, Lakey JR. Quantitative assessment of collagenase blends for human islet isolation. Transplantation 2005; 80 (6): 723.
157. Yamamoto T, Ricordi C, Messinger S, et al. Deterioration and variability of highly purified collagenase blends used in clinical islet isolation. Transplantation 2007; 84 (8): 997.
158. Roche Diagnostics GmbH. Report of analytical results of Liberase MTF-S (lot 10829200). Indianapolis, IN, Quality Control Biotechnology Operations, Roche Diagnostics GmbH. 2009.
159. Shapiro AM, Ricordi C, Hering BJ, et al. International trial of the Edmonton protocol for islet transplantation. The New England journal of medicine 2006; 355 (13): 1318.
160. Brandhorst H, Brandhorst D, Brendel MD, Hering BJ, Bretzel RG. Assessment of intracellular insulin content during all steps of human islet isolation procedure. Cell Transplant 1998; 7 (5): 489.
161. Hellman B. Actual distribution of the number and volume of the islets of Langerhans in different size classes in non-diabetic humans of varying ages. Nature 1959; 184(Suppl 19): 1498.
162. Anazawa T, Balamurugan AN, Matsumoto S, et al. Rapid quantitative assessment of the pig pancreas biopsy predicts islet yield. Transplant Proc 2010; 42 (6): 2036.
163. White SA, Hughes DP, Contractor HH, London NJ. An investigation into the distribution of different collagen types within adult and juvenile porcine pancreata. Journal of molecular medicine 1999; 77 (1): 79.
164. Hughes SJ, Clark A, McShane P, Contractor HH, Gray DW, Johnson PR. Characterisation of collagen VI within the islet-exocrine interface of the human pancreas: implications for clinical islet isolation? Transplantation 2006; 81 (3): 423.
58
165. van Suylichem PT, van Deijnen JE, Wolters GH, van Schilfgaarde R. Amount and distribution of collagen in pancreatic tissue of different species in the perspective of islet isolation procedures. Cell Transplant 1995; 4 (6): 609.
166. Tons HA, Terpstra OT, Bouwman E. Heterogeneity of human pancreata in perspective of the isolation of the islets of langerhans. Transplant Proc 2008; 40 (2): 367.
167. van Deijnen JH, Hulstaert CE, Wolters GH, van Schilfgaarde R. Significance of the peri-insular extracellular matrix for islet isolation from the pancreas of rat, dog, pig, and man. Cell and tissue research 1992; 267 (1): 139.
168. Vaziri N, Thuillier R, Favreau FD, et al. Analysis of machine perfusion benefits in kidney grafts: a preclinical study. Journal of translational medicine 2011; 9: 15.
169. Taylor MJ, Baicu S, Greene E, Vazquez A, Brassil J. Islet isolation from juvenile porcine pancreas after 24-h hypothermic machine perfusion preservation. Cell Transplant 2010; 19 (5): 613.
170. Brandhorst H, Asif S, Andersson K, et al. A new oxygen carrier for improved long-term storage of human pancreata before islet isolation. Transplantation 2010; 89 (2): 155.