Embed Size (px)
Citation preview

www.krspine.org
Acute Sciatic Nerve Palsy after Sleeping in a Sitting Position -Case Report-
Dae Ho Ha, M.D., Sung Kyun Oh, M.D., You Mi Kim, M.D.
J Korean Soc Spine Surg 2011 Dec;18(4):259-262.
Originally published online December 31, 2011;
http://dx.doi.org/10.4184/jkss.2011.18.4.259
Korean Society of Spine SurgeryDepartment of Orthopedic Surgery, Inha University School of Medicine
#7-206, 3rd ST. Sinheung-Dong, Jung-Gu, Incheon, 400-711, Korea Tel: 82-32-890-3044 Fax: 82-32-890-3467
©Copyright 2011 Korean Society of Spine Surgery
pISSN 2093-4378 eISSN 2093-4386
The online version of this article, along with updated information and services, islocated on the World Wide Web at:
http://www.krspine.org/DOIx.php?id=10.4184/jkss.2011.18.4.259
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Korean Society of
Spine Surgery

259© Copyright 2011 Korean Society of Spine Surgery www.krspine.org
J Korean Soc Spine Surg. 2011 Dec;18(4):259-262. http://dx.doi.org/10.4184/jkss.2011.18.4.259Case Report pISSN 2093-4378
eISSN 2093-4386
Received: February 11, 2011Revised: May 6, 2011Accepted: June 10, 2011Published Online: December 31, 2011Corresponding author: Sung Kyun Oh, M.D.Department of Orthopaedic Surgery, Wonkwang University SanbonHospital ,Sanbondong,Gunpo city,Gyeongido,KoreaTEL: 82-31-390-2224, FAX: 82-31-390-2244E-mail: [email protected]
“This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.”
This paper was supported by Wonkwang university in 2011.
Acute Sciatic Nerve Palsy after Sleeping in a Sitting Position -Case Report-Dae Ho Ha, M.D., Sung Kyun Oh, M.D., You Mi Kim, M.D.Department of Orthopedic Surgery, Wonkwang University Sanbon Hospital,Gunpo, KoreaInstitue of Wonkwang Mecal Science, Iksan, Korea.
Study Design: A case report. Objective: We wanted to present the clinical manifestation and imaging findings of a rare case of acute sciatic nerve palsy with a foot drop similar to lumbar disc herniation developed after sleeping for 8 hours in a sitting position in inebriated condition. Summary of Literature Review: Sciatic nerve palsy as a complication from being operated in a sitting position have been reported, but here have not been any reported cases of after-sleep sciatic nerve palsy. Study Subject and Methods: Sixty eight year old male admitted to hospital due to acute onset of right foot drop, subsequent walking difficulty, and numbness of the right calf and foot. Symptoms began after 8 hours of sleeping in a sitting position. Pelvic MRI exam revealed sciatic neuropathy, and also electrophysiological exam revealed sciatic nerve palsy.Results: The subject patient’s conditions started improving after 6 weeks and he was able to walk again on his own.Conclusion: Sciatic nerve injury by prolonged pressure around the buttocks or posterior thighs, albeit rare, can develop and may cause foot drop, parethesia and sciatica.
Key Words: Sciatic neuropathy, Foot drop, Sitting position, Acute sciatic nerve palsy
INTRODUCTION
The sciatic nerve is the thickest peripheral nerve of the human
body that runs from within the pelvis through the greater sciatic
notch and it runs along the gluteus maximus, femoral region and
biceps; it can cause complications due to constraints from the
surrounding structures. A common cause is piriformis syndrome
that stems from spasms of the piriformis, and others are nerve
lesions such as ganglion and external pressures.1-3) In the case of
unilateral sciatic neuropathy, because the symptoms are similar
to those of disc herniation, in order to accurately diagnose
the condition, in-depth medical history and neurological
examination, electromyography and nerve conduction tests are
necessary. The authors of this study wanted to report, along with
literature discussions, about one case involving rhabdomyolysis
that occurred after sleeping in a sitting position.
CASE REPORT
A 68-year-old male patient visited the emergency room for
radiating pain in both sides of his buttocks and right lower leg,
which occurred suddenly on the day of his hospital visit. He
appealed of the weakness in the lower right leg and severe pain
below his ankle; he stated that the symptoms were similar to
what he experienced before his back surgery 2 years prior and
he stated that he couldn’t walk due to paralysis. The patient
was a regular drinker of alcohol, and he drank 2-3 bottles of
Soju (a Korean distilled spirit) 2-3 times a week. Day before
the visit he had drunk alcohol and slept in a sitting position

Sung Kyun Oh et al Volume 18 • Number 4 • December 2011
www.krspine.org260
in crapulent state as well, and he and his family denied any
previous similar incidences. Regarding his past medical history,
about 2 years prior he was diagnosed with a lumbar spinal
stenosis and had his lumbar number 3-4 and 4-5 undergo
posterior decompression and lumbar 3-4 posterolateral fusion
procedure. On physical examination he appealed of bilateral hip
tenderness, and no signs of injury due to trauma were observed.
Neurological examination revealed his right knee flexion had
been reduced to a grade 3, and his ankle dorsiflexion and ankle
plantar flexion to grade 0, and a foot drop was observed on the
right side. His ability to sense pain in his right sciatic nerve region
and vibrations had also decreased. A general blood test yielded
higher level of neutrophils which indicated increased white blood
cell count, and in biochemistry test it showed his CK (creatine
kinase) was 19,573 (normal range; 30-200IU/L), CK-MB 151
(normal range; 0-7.8ng/mL), and AST increased to 138 (normal
range; 5-34IU/L). Under the diagnosis of rhabdomyolysis, he
was administered a 3-liters per day fluid therapy; the magnetic
resonance imaging scans taken on the day of hospital visit, other
than posterior decompression observation, although no other
observations were made (Fig.1A, 1B), pelvic magnetic resonance
imaging observed damages and near-necrosis accompanied by
dermatomyositis in the muscles proximal to the sciatic nerve
such as gluteus maximus, gluteus medius, gluteus minimus, and
piriformis, culminating in observations suspecting prevalent
rhabdomyolysis (Fig.2A, B). In addition, the pressure from soft
tissue swelling around the sciatic nerve was causing compression
of the sciatic nerve, the suspected pattern of which was also
observed (Fig.2C, 2D). The nerve conduction test conducted
2 weeks after the discovery of symptoms showed that the
amplitudes of compound muscle action potential (CMAP) was
reduced, and the follow-up nerve conduction test conducted 4
months later did not show any sensory nerve action potential
(SNAP) for the peroneal nerve and sural nerve.
The EMG tests showed abnormal spontaneous activities in the
semitendinosus muscles, femoral biceps, calf cramp muscle, and
peroneal (Table 1). The neurological examination and imaging
findings, and electrophysiological test and observations were
used to diagnose neuropathy in the sciatic nerve on the right.
Two weeks after the initial visit to the hospital, the patient’
s plantar flexion improved to grade 2, and 6 weeks later the
patient’s dorsi flexion improved to grade 3 and knee flexion
to grade 4; the patient was able to walk by himself using a
walking cane. Because the pain persisted in the lower right
body, neurological epidural injections were administered, and
the patient showed improvement trend by going from a VAS
(visual analogue scale) 9 to VAS 4. One year after discharge, the
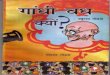
Fig. 1. Preoperative (A) and postoperative (B) image of T2 sagittal MR show decompression state of lumbar spinal canal.
Table 1. Findings of Electromyography
Muscle Spontaneous Voluntary MaximalRectus femoris,right Normal Normal RIP
Semitendinosus,right PSW 3+,fibrillation Normal RIP
Biceps femoris-short head,right PSW 3+,fibrillation Normal RIP
Gastrocnemius-medial,right PSW 2+,fibrillation Normal RIP
Gluteus medius,right Normal Normal FIP
Peroneous longus,right PSW 3+,fibrillation Normal RIP
Tibialis anterior,right PSW 3+,fibrillation Normal RIP
Vastus lateralis,right Normal Normal FIP
PSW ; positive sharp wave, RIP ; reduced interference pattern, FIP; full interference pattern

Acute Sciatic Nerve Palsy after Sleeping in a Sitting PositionJournal of Korean Society of Spine Surgery
www.krspine.org 261
outpatient follow-up showed all sensations were restored to
normal and both the dorsum and bottom of the foot showed
recovery to grade 4; the patient was able to walk by himself
without the use of a waking cane, and the pain was being kept
under VAS 1 level through the use of tricyclic antidepressants
(amytryptyline) and painkillers (oxycodone).
DISCUSSION
In the case of the sciatic nerve, because it is fixed in the sciatic
notch and fibular head, when the hip joint is bent with the
knee extended, the nerve is extended and in this position it is
vulnerable to external damages. In particular, a few cases of nerve
damage after long operations in a sitting position with the hip
joint in bent position are being reported.3,4) Besides these cases,
sciatic nerve damage can occur due to staying in an unnatural
position for prolonged periods, the compartment syndrome,
bleeding or tumors in the pelvic cavity, or the piriformis
syndrome.1,5) In particular, related to alcohol or drugs, there were
cases being reported as a form of Saturday night paralysis.6,7)
In our patient’s case, he had underwent surgery for spinal
stenosis and he complained of radiating pain in his lower body
accompanied by pain in his buttocks, which could have been
confused as a spinal lesion at the beginning, and positive findings
were observed in straight-leg raising test as well; it was difficult
to distinguish from spinal column pains such as a herniated disc.
In biochemical tests, the sharp increase in CK, which suggested
rhabdomyolysis, and pelvic MRI to address the tenderness in the
femoral incisura were performed and it was possible to diagnose
the patient with a sciatic neuropathy caused by pressure. In the
initial physical examination of patient, there were no symptoms
to suspect compartment syndrome such as severe swelling or
edema in the buttocks, which seemed to be due to the thick
subcutaneous layer of the buttocks; in the case of the inner fascia
including the sciatic nerve, swelling in the surrounding structures
was observed through MRI. In our patient’s case, it seemed that,
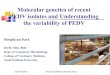
Fig. 2. (A) Pelvis T2 weighted coronal MR image showing sciatic nerve (arrow), bilateral gluteus muscle, obturator muscle and right pyriformis muscle swelling and marked enhancement (B). Axial image of T2 weighted (C) and T1 weighted enhance MR (D) show sciatic nerve and adjacent soft tissue edema.

Sung Kyun Oh et al Volume 18 • Number 4 • December 2011
www.krspine.org262
as a first level cause, the patient’s sleeping in the same sitting
position for 8 hours after drinking was culpable; based on the
past cases where the patients developed sciatic nerve palsy due
to sitting in unnatural positions, since this condition can occur
after undergoing lengthy operations in a sitting position or after
alcohol intake or drug use, it is necessary to distinguish between
radiating spinal pain and sciatic neuropathy.
Although one could first suspect spinal origins like disc
herniation in the cases of acute unilateral radiating pain in the
lower leg or a foot drop, sleeping in an unnatural position
or sciatic neuropathy needs to be, albeit rare, considered as a
possible cause, as illustrated in this case study.
REFERENCES
1. Baima J, Krivickas L. Evaluation and treatment of peroneal
neuropathy. Curr Rev Musculoskelet Med. 2008;1:147-
53.
2. Benson ER, Schutzer SF. Posttraumatic piriformis
syndrome: diagnosis and results of operative treatment. J
Bone Joint Surg Am.1999;81:941-9.
3. El-Rubaidi OA, Horcajadas-Almansa A, Rodriguez-
Rubio D, Galicia-Bulnes JM. Sciatic nerve compression
as a complication of the sitting position. Neurocirugia.
2003;14:426-30.
4. Gozal Y, Pomeranz S. Sciatic nerve palsy as a complication
after acoustic neurinoma resection in the sitting position. J
Neurosurg Anesthesiol. 1994;6:40-2.
5. Henson JT, Roberts CS , Giannoudis PV. Gluteal
compartment syndrome. Acta Orthop Belg. 2009;75:147-
52.
6. Manigoda M, Dujmovic-Basuroski I, Trikic R , Drulovic
J. Acute sciatic neuropathy “post-Saturday palsy”. Srp Arh
Celok Lek. 2005;133:58-61.
7. Tacconi P, Manca D, Tamburini G, Cannas A , Giagheddu
M. Bed footboard peroneal and tibial neuropathy. A
furtherunusual type of Saturday night palsy. J Peripher Nerv
Syst. 2004;9:54-6.
좌식 수면 후 발생한 좌골신경마비 - 증례 보고 -하대호 • 오성균 • 김유미원광대학교 산본병원 정형외과
연구 계획: 증례 보고
목적: 요추 추간판 탈출증과 유사한 족하수를 동반한 좌골신경병증의 임상양상 및 영상의학소견에 대해 보고하고자 한다.
선행문헌의 요약: 수술 자세에 따른 합병증으로서 좌골신경마비를 보이는 경우가 보고된 예가 있으나 좌식 수면 후 발생한 좌골신경마비의 경우 보고
된 바 없다.
대상 및 방법: 좌식수면 후 발생한 급성 일측 하지 방사통과 족하수를 주소로 응급실로 내원한 68세 남자환자로 횡문근 융해증과 함께 좌골신경을압박
하는 소견이 MRI상 관찰되고 있었고 전기신경생리검사로도 좌골신경마비로 진단할 수 있었다.
결과: 환자의 족하수는 수상 6주후 부터 호전되어 자력보행이 가능하였다.
결론: 급성 족하수 및 좌골신경통을 보이는경우 부적절한 자세의 수면이나 압박에 의한 좌골신경병증도 드문 원인이 될 수 있음을 고려해야 한다.
색인 단어: 좌골신경, 좌식수면, 족하수
약칭 제목: 급성 좌골신경 마비







![Hum Sunni Kyun Hain [Mehr Muhammad Mianwalvi]](https://img.pdfslide.net/doc/110x75/553344a5550346b2038b474d/hum-sunni-kyun-hain-mehr-muhammad-mianwalvi.jpg)