Embed Size (px)
Citation preview

Volume 5 Issue 1 October to December 2013
Journal of the Venu Eye Institute & Research Centre
Facts about vision testing chart
Orthokeratology
Pediatric Refraction & Prescription
Duane’s Retraction Syndrome
Convergence Insufficiency
Contact Lens Options for Presbyopia
Contrast Sensitivity
Differential Diagnosis of Diplopia
Jackson’s cross-cylinder technique
Pg. 2
Pg. 4
Pg. 6
Pg. 9
Pg. 12
Pg. 14
Pg. 15
Pg. 17
Pg. 21

2 Verge Journal of the Venu Eye Institute & Research Centre
Distance Vision Charts are generally used at 6 meter.
6 meter = 19.685 feet, but generally we consider it as 20 feet, which is 5 inch more than 6 metre.
Same thing happens when we use it at 3 meter with mirror.
Note:Always measure chart distance from the front surface of the chart to the mirror and from mirror to front plane of the face (when patient is seated in a comfortable posture on the refraction chair)20 feet or 6 m is the most widely used test distance, 4 m has been recommended by Hofstetter" which is generally used in ETDRS chart. A 4-m test distance facilitates making a dioptric allowance of 0.25 D (P=1/f, P=1/4, P=0.25D) to the refractive correction to allow for the chart being closer than optical infinity. Also, using 4 m as the standard for testing distance vision facilitates comparison with near-vision measurements, in which 40 cm is commonly used as a standard test distance.
IlluminationFor standardized illumination of the distance vision chart range from 85 to 300 cd/m2 (two bulbs of 50 watt can be used). Widely used standard luminance is 160 cd/m2, in this luminance range, doubling the luminance changes the visual acuity score by about 0.02 log units (1 VAR unit), which corresponds to one-
fifth of a line or a 5% change in MAR. In video display chart it depends upon the screen resolution, pixels and brightness of the screen. At least 20 pixels are required per letter height so that the spatial structure or shapes of individual, optotypes do not show significant variation from
one size to the next.
In testing room 380 cd/m2 illumination is required. In low light, patient's pupil become relatively dilated so any refractive error or optical irregularities are more likely to affect visual acuity.
Contrast and Glare Cont r a s t i s ano the r variable that affects visual acuity .Generally 100% contrast is used in charts (black letters on white background) so, it can't be copied as it reduces the contrast. Measurement of visual acuity with low contrast (grey) optotypes is becoming more widely used, mainly for patients with corneal or lenticular disorders or for those who have had re f rac t ive
surgery. Low-contrast visual acuity and its difference from high-contrast visual acuity are often regarded as measures of contrast sensitivity.
When illuminating charts, one should take care to avoid glare sources within the patient's field of view.
Facts about vision testing chartMr. Bhaskar Ghosh, Sr. Optometrist Venu Eye Institute & Research Centre

July - September 2012 Journal of the Venu Eye Institute & Research Centre Perfect Vision 3
Dear friends
A very happy & prosperous new year from the Venu family
With immense pleasure we are proud to present this issue of our in-house journal “ VERGE” in remembrance of our founder Dr. R. K. Seth. This issue includes articles on various aspects of eye care prepared by the optometry faculty of Venu Eye Institute & research centre.
Among various achievements of optometry services at Venu in this quarter are-FIACLE examination for contact lens educator, optometry fellowship examination, collaboration with Amity University for internship of Bsc. Students, contact l e n s w o r k s h o p , i n a u g u r a t i o n o f teleophthalmology centres; which is first of its kind in the country with support from government of India, Co hosting of annual conference of community ophthalmological society of India at Mandvi, Surat (Gujrat)
In this issue we are presenting various topics from basics of optometry to newer treatment modality.
Basics of vision testing & evaluation of astigmatism through Jackson cross cylinder forms the base of refraction and all of us should be well versed with it. Contrast sensitivity is a common problem in refractive errors & elderly patients and should be optimally corrected to give
a proper vision. Convergence insufficiency is a major cause of headache among young population & its diagnosis & treatment is sometimes very tricky. Diplopia can be very troublesome both to the patient and the doctor, so, we should be well acquainted with the diagnostics investigation in patient presenting with diplopia.
The present issue deals with the problem of paediatric refraction and glass prescription among paediatric patients which is the most difficult part of optometry training and the most interesting one.
Duane retraction syndrome- its diagnosis & treatment, a rare entity has been discussed in detail.
Presbyopia is an ageing process and all the patients should be made cognizant of the recent treatment with contact lenses. Orthokeratology / reverse geometry CL is a temporary measure to correct moderate degree of refractive error.
Keeping in touch with technology this issue can be accessed online on Venu's website.
We hope you enjoy this issue of verge as much as we have put our efforts in bringing these articles together.
Wishing you & your family a great year ahead
Editorial team
From the editors desk
Managing Editor : Ms. Tanuja Joshi
Editor : Dr. Suryakant Jha
Editorial board : Dr. S.C. Gupta: Mr. Bhaskar Ghosh: Ms. Sheeba Qumar
Editorial Support : Mr. Jitender Saroya

4 Verge Journal of the Venu Eye Institute & Research Centre
Orthokeratology Ms. Sheeba Qumar, Sr. Optometrist Venu Eye Institute & Research Centre
Orthokeratology, also known as Ortho-K, Overnight vision correction or corneal refractive therapy (CRT) is the non-surgical temporary reduction of myopia achieved by the programmed application of special contact lenses (called ortho-k lenses) to reshape the cornea. Such lenses are worn overnight and the patient gets clear vision in the morning without contact lenses or glasses.
George Jessen first explained the concept 'ortho-focus' in 1962.
In 1989, Richard Wlodyga and Nick Stoyan first designed Orthokeratology lens with 'reverse geometry curve'.
The goal of ortho-k is to flatten the front surface of the eye and thereby correct mild to moderate amount of nearsightedness and astigmatism.
Principle: It works on the principle of corneal shape change caused by compression and redistribution of epithelial cells and fluid from centre to periphery.
Mechanism of action:Many theories exist to explain the mechanism of orthokeratology with the most widely acceptable being that of corneal “sphericaization”. The normal cornea is aspheric with central portion being steepest and becomes progressively flatter towards periphery. GP contact lens wear is postulated to cause central corneal flattening accompanied by paracentral steepening, which
results in a corneal shape factor that approaches zero (i.e., spherical). This process is accelerated by the use of r e v e r s e geometry lens designs which h a v e a s e c o n d a r y curve that is steeper than the base curve t o a l l o w a p p r o p r i a t e changes in the m i d -p e r i p h e r a l cornea In other words, when a rigid contact lens applies pressure to the cornea in one area, the cornea yields to that force and pushes out in another area where there is less force. Therefore, flattening of the apex of the central cornea is accompanied by mid-peripheral steepening, essentially resulting in a redistribution of corneal tissue.
Lens Design: Ortho-K lenses are reverse geometry curve lenses with 5 curves with one base curve, one reverse curve, two alignment curves and one peripheral curve.
?Base curve: It is 6.00mm wide and is flatter than the central corneal radius creating positive pressure and thus creates the central

October - December 2013 Journal of the Venu Eye Institute & Research Centre Verge 5
corneal compression providing treatment zone of 5.00mm or more.
?Reverse curve: It is 3-5D steeper than the base curve which allows migration of epithelial cells and intracellular fluid. This curve creates an annulus tear reservoir inducing negative pressure
?Alignment curve: As the name suggests, two alignment curves keep the lens in alignment. They align with the peripheral cornea providing the bearing zone. 1st alignment Curve is generally equal to the flat K of the cornea being fit and 2nd Alignment Curve is steeper than the base curve but flatter than first alignment and Reverse Curve.
?Peripheral curve: It is flatter than alignment curve providing edge lift and allows lens movement, tear and debris exchange
Advantages: ? It is reversible process? Not painful? Non-surgical procedure? Less expensive than LASIKDisadvantages:? Frequent follow-ups are required? Patient's compliance level needs to be good.
? It is essential to wear the retainer lenses as it is reversible process.
Patient's selection: Orthokeratology corrects till -6.00D of myopia and -1.75D astigmatism. The eligibility criteria should fulfill the following factors too.? Motivation? Patient's expectation? Time frame
Ideal fitting of ortho-K lens:Dynamic and static fit should be assessed including an ideal 1-2 m m o f l e n s movement post-bl ink. In s tat ic fitting, fluorescein p a t t e r n s h o u l d exhibit central 4-6mm touch, Green colored ring with equal width in Reverse Curve Zone and Black part with equal width in Alignment Zone.
Follow up visits:Periodical Follow-up check Schedule:? 1 day after wearing lens? 1 week after wearing lens? 3 weeks after wearing lens? 3 month after - periodically
Examination criteria:? Interview: wearing time, time to maintain
visual acuity, feeling.? Slit lamp examination : for cornea and
conjunctiva ? Visual acuity test: unaided vision, stability of
visual acuity.? Lens wearing examination: lens movement
and centration etc.? Lens appearance examination : scar, breakage,
deposits (protein, etc)? Re-education of lens care : cleaning,
wearing/removing, soaking

6 Verge Journal of the Venu Eye Institute & Research Centre
Who can ever think that the child's behavior can reveal the mysteries of his/her refractive status?
Have you ever thought the same? If not, then think. A Child holding toys too close to his eyes or squeezing too much can be a myope. A Baby tilting his head while viewing the vision chart can be an astigmat or a little princess complaining of too much headache but still having 6/6 vision can be a hyperope
But still, these all assumptions cannot lead to the final prescription. Remember that examining kids is a difficult prospect as they universally hate strangers messing with their eyes.
Moreover, in children there are lots of confusing variables like the following-
1. Unreliable visual acuity2. Subjective refraction may not always be
possible.3. Variable accommodation4. Association of strabismus
We have limited time for refraction before the child further decompensate.
Traditional objective procedures for assessment of refractive error do not work well with children because of poor fixation. In particular, the child's age, their cooperation and dynamic refractive status are the key factors which influence the accuracy of refraction. For this reason, it is often necessary to choose procedures which inhibit or minimize accommodative activity.
As a result alternative methods have been developed which includes the following-
Bruckner's testOne quick method to estimate refractive error is by examining the red-reflex. Hold a direct
ophthalmoscope from 100cm distance in a dark room and shine it so that the circle of light, lights up both pupils at the same time. Examine the red-reflex from each eye. Assuming that the child is looking right at us, the placement of the red-reflex gives some clues. Inferior crescents indicate myopia (near-sightedness) while superior crescents indicate hyperopia.
Most children have some degree of hyperopia, as their eyes are small and still growing. This makes the Bruckner test more useful for picking up myopic (near-sighted) errors, but overall the test isn't very accurate in undilated children as they have the ability to accommodate. Also, if the eyes are not well aligned, such as strabismus, the results are inaccurate.
Cycloplegic refractionIt is an integral part of examination of each pediatric patient.
Indications for Cycloplegic refraction-
There are several instances when a Cycloplegic refraction is indicated, including:
? Hypermetropia over +5.00D? Anisometropia more than 1.50D? Suspect and/or manifest strabismus
(especially esotropia)
Pediatric Refraction & Prescription (Handling the small child) Ms. Nikita Gupta, Bsc. Optometry Intern.
Venu Eye Institute & Research Centre

Journal of the Venu Eye Institute & Research Centre Verge 7
? Family history of strabismus, high hypermetropia and amblyopia
? In the presence of unstable esophoria, pseudomyopia and asthenopia
? Poor cooperation/fixation of the child? When the retinal reflex during retinoscopy
changes motion or brightness due to dynamic accommodative status.
There are also some instances where cycloplegic refraction is contraindicated, including:? Cases where administration of cycloplegic
agents will cause undue stress for the child, resulting in a complete lack of co-operation
? Risk of ocular and/or systemic side effects (which are more likely with atropine than cyclopentolate and tropicamide)
? Risk of developing acute angle closure glaucoma in those with a shallow anterior chamber
Control of accommodation in children of pre-school age is more commonly achieved by pharmacological means, using cycloplegic agents such as cyclopentolate and tropicamide; atropine can only be used by certified practitioners. All of these drugs are muscarinic receptor blockers, thus they work by blocking the muscarinic receptors in the ciliary body, which in turn prevents accommodation. The selection of the cycloplegic drug depends upon the age of the patient and as well as on the pigmentation of the iris. Those with light coloured irides may exhibit an increased response to drugs as compared with darkly pigmented irides, and therefore a lower concentration/dose ought to be selected.List of commonly used cycloplegic agents includes-
Cyclopentolate? Esotropic patients with hyperopia < 2.00D)? 3-6 years old children? Where atropine is contraindicated (Seizures,
cardiac problem)
Esotropia A manifest inward deviation often alters the way final power is prescribed. An esotropia with refractive component demand for full c y c l o p l e g i c irrespective of age of child. Our general r u l e s , f o r undercorrection of hyperopia on the grounds of functionally large range of accommodation doesn't hold validity in these situations. In contrary to this full correction is prescribed to relax accommodation. If such condition coexist with an abnormal AC/A ratio, near addition is prescribed in order to prevent any exertion of accommodative effort. Full correction and near addition in an executive bifocals are prescribed in such children.
AmblyopiaAmblyopia cases require special treatment regimen since the visual acuity improvement
achieved in the period of plasticity (<16 years) will freeze and remain same for the rest of the life. Refraction plays a key role in a m b l y o p i a t r e a t m e n t . R e f r a c t i o n i n amblyopic patients
differ from normal subject in sense that even the small amount of hyperopia cannot be neglected on the grounds of active accommodation because of the fact that accommodation is impaired in such subjects. Hence full correction (hyperopia or myopia) is prescribed to ensure clear retinal
October - December 2013

8 Verge Journal of the Venu Eye Institute & Research Centre
image for proper development. On every follow up, refraction should be repeated and even the minor changes are implemented.
HeterophoriaThe rule for maximum plus or minimum minus is not the only thing that we will mould to our objective findings. We also need to consider the state of the ocular balance in order to get the perfectly tailored prescriptions. Exophoria are usually handled with full negative correction or slightly under-corrected positive powers so as to stimulate accommodation which will in turn stimulate convergence and balance the exophoria. On the other hand esophoria demands for full plus correction in order to prevent any further increase in the amount of esophoria.
AstigmatismAs we know that adults w h o a r e d iagnosed with high cylindrical power are prescribed with partial correct ion on first visit just to make
them adapt to these powers. On the other hand children being more plastic, the initial chunks of partial cylinder can be bigger and full cylindrical correction can be swiftly achieved.
Post surgical
Binocular aphakia A binocular aphakia patient demands for a full hyperopic correction in order to ensure proper visual development. The age of child also effect the prescription.
For an infant up to 6 months of age having the world of interest can find only to the n e a r l i m i t s , t h e distance correction is clubbed with + 3D near addition. As the child starts crawling his area of interest grows from near to intermediate ranges and distance refraction is now clubbed with +2D lens instead of a + 3D lens. As the child starts walking and enters the preschool, only the distance correction along with a separate addition for reading is prescribed in the executive bifocals.
Uniocular aphakia For a uniocular aphakia, best tolerated distance correction for the aphakia is prescribed and routine examination is performed in order to rule out the development of amblyopia. Aniseikonia encountered by the patient is quite large with spectacles so contact lenses are much more superior since it helps in the development of binocular single vision by reducing the difference between image sizes in two eyes.
PseudophakiaIn uniocular pseudophakia nothing much is done except the distance correction for operated eye. The near vision is balanced by the non operated eye. For bilateral pseudophakia, full distance connection with + 3D near addition in executive glasses are prescribed.
So next time, whenever you have a doubt regarding “what to prescribe”, always reconsider your decisions, because THE SMILE AND VISION OF A SMALL CHILD LIES IN YOUR HAND.

Verge Journal of the Venu Eye Institute & Research Centre 9
Alexander Duanes, in 1905, emphasized that the retraction of the globe is an essential clinical feature of this syndrome. Because of this feature which is so diagnostic the term “Duane's Retraction Syndrome” is deeply entrenched.
Classification Huber's classification uses the clinical descr ip t ions together with electromyograp h i c information to simplify this c o m p l e x syndrome.
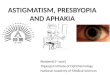
Type I : It is t h e m o s t common type ( 7 8 % ) characterized b y m a r k e d limitation of abduction with minimally defective or normal adduction, retraction of globe and narrowing of the palpebral fissure in adduction, widening of the fissure on abduction. Electromyography shows absence of electrical activity in the lateral rectus muscle on abduction but paradoxical electrical activity on adduction.
Type II: It is the least common type (<10%) characterized by marked limitation of adduction with exotropia of the affected eye, abduction normal or slightly limited, retraction of the globe and narrowing of the fissure on attempted adduction . On electromyography the lateral rectus showed peak impulses on abduction and a second paradoxical peak on attempted adduction. Type III: It is present in 15% cases and is characterized by a combined limitation or
absence of both abduction and adduction, retraction of the globe and narrowing of the palpebral fissure on attempted adduction. The electromyogram demonstrates co -contraction of the horizontal rectus muscles on both adduction and abduction.
T h e m o s t characteristic clinical p r e s e n t a t i o n o f Duane's syndrome is a n a b s e n c e o f abduction of an eye with some degree of restricted adduction and retraction when an attempt is made to adduct. Additionally, either an upshooting or downshooting or both, of the adducted e y e f r e q u e n t l y occurs, particularly as the adducting eye
begins to move in the oblique position of up and in or down and in.
Pathogenesis There is abnormal firing pattern of the lateral rectus muscle varying from paradoxical innervation to innervation with incomplete inhibition in adduction and recruitment in abduction. The co-contraction of the horizontal rectus muscles on adduction causes the retraction of the globe and also may cause slippage of the globe causing upshoot /downshoot depending on the relative position of the globe in reference to the muscles.
FeaturesA. Incidence - The frequency of Duane's syndrome in the general population of strabismus patients has been estimated to be 1-4%
Type 1 DRS showing retraction of the globe of the left eye and narrowing of the palpebral fissure on adduction
Widening of palpebral fissure on abduction
October - December 2013
Duane’s Retraction SyndromeMs. Shagufta Parveen, Optometrist Venu Eye Institute & Research Centre

10 Verge Journal of the Venu Eye Institute & Research Centre
B. Sexual Distribution - The gene responsible, besides being autosomal dominant with incomplete penetrance, was also partly sex-limited, making females more susceptible to the effects of the gene.
C. Laterality - There is a predilection for left eye involvement.
D. Types of Presentation - The most common form of the syndrome is Type I of the Huber classification system.
E. Ocular Deviation in Primary Position -Esotropia was the most common presenting deviation in primary gaze in the majority or reviewed studies.
F. Refractive Errors -Reviews of DRS patients have shown hypermetropia of greater than +1.50 in 71% of the patients
G. Amblyopia - Most amblyopia in studies was found to be due to strabismus and not due to anisometropia.
Assoc iated Congenital Anomalies & Syndromes
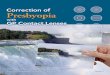
1. Associated O c u l a r Findings - T h e m o s t f r e q u e n t l y encountered ocular abnormality are nystagmus, epibulbar dermoid, anisocoria and ptosis .
2. Associated Nonocular Findings - Goldenhar's syndrome (oculo-auriculo-vertebral dysplasia, Klippel-Fiel anomaly, Wildervanck syndrome (cervico-oculo-acoustic syndrome).
Clinical Features & Diagnosis
1. Defects in Abduction and Adduction - The most characteristic findings is an absence of abduction of an eye with some degree of restricted adduction.
2. Esotropia and Exotropia- Although many patients with DRS are orthophoric in primary position, exotropia in straight ahead position also occurs. Esotropia, however, is the most commonly diagnosed type of strabismus.
3. Upshoots and Downshoots- The characteristic vertical deviations include the over elevation and depression seen in the adducted position. T h i s a b n o r m a l movement had been postulated to be related to a slipping of the lateral rectus muscle over the globe as 'bridle effect’
4. A and V Patterns - Various types of A and V patterns may be found in DRS. V- pattern is more common than A- pattern.
5. Eyelid Changes and Globe Retraction - The eyelid changes found in DRS in adduction are related to a drooping of the upper lid and elevation of the lower lid.
6. Torticollis - Face turn is a major characteristic of DRS. The face is turned in the direction of the horizontal muscle with the greatest deficit.
Differential Diagnosis ? Abducens Nerve Palsy (6th Nerve)? Moebius Syndrome? Congenital or Infantile Esotropia
Epibulbar dermoid
Upshoot of left eye on adduction

Verge Journal of the Venu Eye Institute & Research Centre 11
Therapeutic Modalities
Goals of Treatment The most common indication for surgical treatment is an unacceptable face turn. O c c a s i o n a l l y s t rabismus i t se l f r a t h e r t h a n t h e s e c o n d a r y h e a d posture can be the main indication for surgical correction. A n u p s h o o t , d o w n s h o o t , o r retraction can be s u f f i c i e n t l y disturbing to the patient or the parents to warrant surgical treatment.
The goal in Duane syndrome should be to avoid disrupting normal binocular development. Thus, young age is a relative contraindication for surgery.
Surgical Procedures Horizontal Muscle Surgery
Face turn towards Left
? Medial Rectus Muscle Recession for esodeviation in primary position.
? Lateral Rectus Muscle Recession for exodeviation in primary position
SummaryThe literature on Duane's retraction syndrome suggests that the syndrome involves a complex set of clinical ocular findings which are caused by a spectrum of mechanical, innervational and central nervous system anomalies that occur together or separately. It is most frequently sporadic, but approximately 10% of cases are familial. The frequent association of DRS with nonocular anomalies, such as Wildervanck's syndrome, point to a teratogenic event occurring between the fourth and eighth week of gestation. In unilateral cases of the syndrome the frequency of left side involvement averages 72%. No reasonable explanation for this phenomenon has been hypothesized. Female preponderance has been postulated as being due to inheritance in an autosomal dominant fashion with the pleiotropic gene responsible also being partially sex-limited. Recently MRI scanning has been utilized to determine if there is any vertical displacement of the horizontal recti muscles.
October - December 2013

12 Verge Journal of the Venu Eye Institute & Research Centre
Convergence insufficiency is a common condition that is characterized by a person's inability to maintain proper binocular eye alignment on objects as they approach from distance to near.
When looking at distance, our eyes are almost parallel. However, when looking at a near object, they come close to each other to maintain binocular fixation. Such simultaneous turning of the two eyes towards the nose is called convergence.
Efficient convergence is necessary for trouble free near-point work. Convergence insufficiency gives rise to eye-strain, headaches, watering and intermittent double vision (jumbling together of letters) following a certain period of near-point work like reading or writing.
Pathophysiology:The underlying etiology for convergence insufficiency is probably innervational. The dramatic reduction of symptoms demonstrated by patients after undergoing appropriate therapy, which is accompanied by objective clinical findings of improved near point of convergence and fusional convergence amplitudes, strongly supports this hypothesis.
Some cases of convergence insufficiency also appear to have an etiologic connection to accommodative dysfunction.
Convergence insufficiency is associated most commonly with an exophoria at near, but patients with this disorder may demonstrate orthophoria or even mild esophoria at the time of their examination. The reasons for this variability are described within this article.
In the past, many ophthalmologists considered convergence insufficiency and its associated
symptoms to be a neurological manifestation of non-related psychological problems best dealt with by a psychiatrist. However, it is now clear that convergence insufficiency is a legitimate, problematic binocular dysfunction. The clinician must consider that the behavioral manifestations displayed by patients result from the frustration caused by their inability to perform desired near visual tasks.
Symptoms:A person who has convergence insufficiency may show and/or complain of the following while doing close work (i.e., reading, computer work, deskwork, playing hand held video games, doing crafts, etc.)?eyestrain (especially with or after reading) ?headaches ?blurred vision ?double vision ?inability to concentrate ?short attention span ?frequent loss of place ?squinting, rubbing, closing or covering an eye ?sleepiness during the activity ?trouble remembering what was read ?words appear to move, jump, swim or float ?problems with motion sickness and/or vertigo
Test - Do you have convergence insufficiency?
For this test, prepare a small rectangular card with a dark yet fine vertical line along its breadth (see picture below).
Convergence Insufficiency Ms. Meenakshi, Optometrist
Venu Eye Institute & Research Centre

Verge Journal of the Venu Eye Institute & Research Centre 13
The Test Procedures:- ? Hold the card in your hand, with the arm
extended. ? Keep looking at the vertical line with both the
eyes. ? Slowly bring the card towards your eyes; stop
when the card is six inches from your eyes. ? Does the line appear single or double?
Evaluation of Your Test Result:A person with good convergence power sees a single line even when the card is held as close as six inches from the eyes.
If the line appears double as the card approaches the inner limit of six inches, your convergence is insufficient. This means that both your eyes are not pointing towards the line.
The greater the insufficiency of convergence, the greater will be the distance of the card from the eyes when the line starts appearing double.
Guidelines for Eye Exercises:Before we go on to the eye exercises for farsightedness, there are a few points to take note of:
? First, we have to understand the steps of each eye exercise carefully.
? Exercise should be done with glasses or contact lenses in case of refractive error.
? Should do the eye exercises in non-glaring light. Vision chart or targets should be well lit at all times..
? Should not strain our eyes while doing the eye exercise. The result would be better if we do not strain your eyes.
? Should rest our eyes after each eye exercise, and also at the end of the whole eye exercise.
? As our eyes are tired after a whole-day work, early morning is the best time for eye exercises.
? If we do not have enough time to complete all the eye exercises for farsightedness, we can do some in the morning and finish the rest in the later part of the day.
? Should learn about the different stages that we will experience when you begin to build your visual habits during the exercise.
Treatment:Orthoptic therapy to increase fusional convergence amplitudes and enhance voluntary convergence is the primary treatment of convergence insufficiency
While the majority of eye care professionals treat children diagnosed with CI using some form of home-based therapy, a new study concludes that clinic-based treatment by a trained therapist along with at-home reinforcement is more effective.
Suggested Eye Exercises for Convergence Insufficiency:-
? Pen push up exercise ? String exercise: This exercise aims to achieve
correct fixation and simultaneous perception (with two eyes) and to overcome suppression
? The 'x' card exercise? This is an effective method to exercise the
convergence and compel us to view with both the eyes together.
? Fusion exercise
October - December 2013

Once we reach our mid-40s, presbyopia makes it difficult to focus on near objects. Reading glasses used to be the only option available to contact lens wearers who wanted to read a menu or do other everyday tasks that require good near vision but now a days there are several ways of fitting contacts for patients who require presbyopic correction which includes combination of distant vision contacts and reading glasses, a monovision contact lens fit, modified monovision and multifocal contact lenses.
Multifocal contact lenses offer the best of both worlds: no glasses, along with good near and distance vision.
Some multifocal contact lenses have a bifocal design with two distinct lens powers — one for your distance vision and one for near. Others have a multifocal design somewhat like progressive glasses, with a gradual change in lens power for a natural visual transition from distance to close up.
Monovision contact lenses:The monovision contact lens concept involves fitting one eye for distance vision and the other eye for near. Normally, the presbyopia patient wears a contact lens for distance correction in the dominant eye, and a contact lens for near vision correction in the non-dominant eye.
It works on the principle that the visual system can suppress the central focus image and thus, enable the object of interest to be seen clearly. Monovision remains an effective means of correcting presbyopia with contact lenses, especially in lower addition. The limitation of monovision is compromised stereopsis.
Modified monovision: In this variation, a single vision contact lens for
distance is worn in the dominating eye and a bifocal contact lens is worn on the non-dominating eye. Modified monovision can provide sharper distance vision than standard monovision, while still providing acceptable near vision without reading glasses for many close-up tasks.
The distance power of the bifocal lens also can be adjusted to provide sharper vision at arm's length for tasks such as computer work.
Multifocal Designs:Alternating lens designs (also called translating designs) have distinct zones in the lens for distance vision and near vision. Like bifocal glasses, the top part of an alternating multifocal lens is for distance vision and the bottom part is for near. The two zones are separated by a nearly invisible line that helps your eye care professional determine if the lens is fitting properly.
The primary disadvantage of the translating bifocal contact lens is that, as with spectacles, the patient must move his/her eyes downward to use the near portion of the lens. Therefore, this design is not a good option for those individuals who need to view close objects at the straight ahead position.
Simultaneous vision contact lens: Rely on an optical system that places two images on the retina simultaneously and then relies on the visual system to select the clearer picture.
Contact Lens Options for PresbyopiaMs. Mamta Bhadula, Optometry Intern
Venu Eye Institute & Research Centre
Cont. on Page No. 16
14 Verge Journal of the Venu Eye Institute & Research Centre

Definition and its importanceContrast sensitivity refers to the ability of the visual system to distinguish between an object and its background. This differs from common visual acuity testing in a routine eye exam, which measures the ability to recognize smaller and smaller letter on a standard eye chart with high contrast.
Contrast sensitivity is a very important measure of visual function especially in situations of low light, fog or glare, when the contrast between the object and their background often is reduced because the visibility of objects in our environment is limited. For example driving at night requires good contrast sensitivity for the safety. On many surveys, contrast sensitivity is the visual parameter that is most commonly related to the problems experience in activities of daily living.
Even if we have 20 /20 visual acuity, we can have eyes or health conditions that may diminish contrast sensitivity and make us feel that we are not seeing well.
Symptoms of reduced contrast sensitivityIf we have low contrast sensitivity we may have problems with night driving including difficulty seeing pedestrians walking along side poorly lit street. Or we might notice that our eyes tired more easily while reading or watching television.
Low contrast sensitivity can be a symptom of a certain eye conditions or diseases such as cataracts glaucoma or diabetic retinopathy. Changes in contrast sensitivity also can occur after LASIK, PRK and other types of refractive surgery. e.g sometimes a person who has undergone LASIK may be able to see 20 / 20 after the procedure but might complain of poor night vision. This could be caused by a loss of contrast sensitivity from the surgery and vice versa also
occur.
In most cases, people with cataract notice a significant improvement in both visual acuity and contrast sensitivity after the surgery!
Contrast sensitivity testingContrast sensitivity testing often isn't included in a routine eye e x a m . I t i s performed if there is a specific visual c o m p l a i n t o f patient suspects a condition that is affecting their ability to discern contrast.
Probably the most widely used chart to test contrast sensitivity is Pelli Robson contrast sensitivity chart. Like a standard snellen's visual acuity chart, the Pelli Robson chart consists of horizontal lines of capital letters, but ins tead of the l e t t e r s g e t t i n g smaller on each successive line, it is the contrast of the letter (relative t o t h e c h a r t background) that decreases with each line.
Other most sophisticated devices used for contrast which uses target call sine wave greetings that consist of a number of fuzzy, parallel bars of light and dark. These bars can vary in width as well as contrast from target to target.
Some sine wave gratings tests include a bright light source to stimulate glare situation.
Contrast SensitivityMs. Nazish Wasi Ansari, OptometristVenu Eye Institute & Research Centre
Verge Journal of the Venu Eye Institute & Research Centre 15 October - December 2013

16 Verge Journal of the Venu Eye Institute & Research Centre
The contrast sensitivity test is done after full correction of refractive error and before dilation.
Contrast sensitivity function: Detailed contrast sensitivity measurements that include both size (spatial frequency) and contrast sensitivity function.
It is essentially plotting of the curve that defines the lowest contrast level that detect for each spatial frequency tested. Eye conditions need to check for Contrast SensitivityAll conditions which include field loss of vision.
Central field loss macular degeneration, bert's disease, stargadt's disease, achromatopsia, cone dystrophies.
Peripheral feel lossR e t i n i t i s p i g m e n t o s a , h e m i a n o p i a , chorioretinitis, glaucoma, aniridia, marfan's syndrome, retinal detachment, leber's amaurosis.
Combined lossColoboma, optic nerve disorders, optic dysplasia, hypoplasia, strokes.
In additionAlbinism, high myopia and amblyopia.
Cont. from Page No. 14
Simultaneous vision contact lenses may further subdivided according to the power distribution across the surface of the lens.
Concentric Bifocals lenses are simultaneous vision lenses with two or more distinct regions of power. The pupil is covered simultaneously by both distance and near portion of the contact lens.The brain selects the clear image at the required distance.
Aspheric multifocal lenses are simultaneous vision lenses with a gradual change in power from near to distance. These lenses can be designed in one of the two ways-
Centre Distance: A lens usually has a back surface aspheric curve resulting in the central

Differential Diagnosis of DiplopiaMs. Farheen Qamar, Optometrist
Venu Eye Institute & Research Centre
Verge Journal of the Venu Eye Institute & Research Centre 17 October - December 2013
Every practitioner should be aware of the importance of an appropriate response to the symptom of diplopia as the aetiology can vary from uncorrected astigmatism to life threatening intracranial anomalies.
Patient presenting at a hospital may have: monocular diplopia, binocular diplopia, infranuclear palsies, mechanical anomalies (muscular or traumatic), concomitant deviations, or convergence/accommodation deficits, supranuclear palsies, due to spectacle intolerance.
This article emphasises the importance of not jumping to the conclusion that every patient complaining of diplopia has an underlying sinister pathology. In addition, as less than half the incomitancies are due to single muscle infranuclear palsy, caution should be exercised when trying to describe an ocular motility pattern in terms of a single muscle defect.
Extraocular muscle actions
The major tools used in the differential diagnosis of diplopia are:
Neurological disease affecting the ocular motor system most commonly results in an incomitancy, but can present as a concomitant deviation. Suggested below is a diagnostic routine and methodology that can be used in the event of a patient presenting with diplopia.
Diagnostic techniques are:1. History and symptomsThe value of a good history should never be underestimated in the differential diagnosis of diplopia. Careful description of the diplopic images can help differentiate monocular or refractive diplopia from a problem of the ocular motor system, the former often being describe as a 'ghosting' rather than a true diplopia. The frequency with which diplopia is recognized can provide useful information. A patient who has suddenly recognized physiological diplopia will generally report it as being present only when they are tired. Questioning about the diplopia can indicate the acuteness of the onset, as can clues from the previous ocular and medical history.
a) Previous ocular historyAn abnormal head posture present since childhood indicates a congenital incomitancy. History of occlusion therapy or childhood surgery may indicate a recent decompensation of a long-standing deviation or a breakdown in suppression. History of eye exercises or use of p r i smat ic l enses po in t s to p rev ious decompensation or intermittent binocular control of a long-standing deviation.
b) General healthThe general health may show signs associated with a systemic condition such as the weakness and fatigue associated with Myasthenia gravis, or previous episodes of poor vision that could be associated with Multiple sclerosis. Vertigo and tinnitus are symptoms of a middle or inner ear defect, which can occasionally be associated with a VIth nerve lesion. Equally, headaches can be associated with diplopia, either in relation to asthenopic symptoms, ophthalmic migraine or intra-cranial anomalies.
c) Family historyFamily medical and ocular history can also be of
Muscle Primary action Secondary
action
Tetiary action
MR Adduction - -
LR Abduction - -
SR Elevation Intorsion Adduction
IR Depression Extorsion Adduction
SO Intorsion Depression Abduction
IO Extorsion Elevation Abduction

18 Verge Journal of the Venu Eye Institute & Research Centre
diagnostic value, especially where there is family history of hypermetropia or an ocular motor disorder.
2. Observationsa) Abnormal head posture (AHP) developed to compensate for an incomitancy is usually adopted to move the eyes into a position of comfortable binocular vision, in which case it can be a useful diagnostic tool. The presence of an AHP normally indicates that the patient has the capacity for good binocular functions. Using an AHP to move the eyes out of the direction of action of the defective muscle effectively makes the chin 'point' in the direction of action of the defective muscle. Normally, the right superior oblique (SO) moves the right eye down and to the left, so the AHP would be chin down and to the left, with a head tilt generally away from the affected side .
The Abnormal head posture for each single muscle palsy is shown in Table given below but this can be misleading, as moving the eyes out of the direction of action of a single muscle palsy is not the only reason for developing an Abnormal head posture.
b) Lid positionUnilateral partial ptosis will often accompany a SR paresis, as the SR and levator palpebrae superioris are innervated by the same branch of the IIIrd nerve. A total IIIrd nerve palsy is usually accompanied by complete ptosis, but in these cases the presenting symptom is unlikely to be diplopia. Bilateral partial ptosis, especially in the
evening, can be due to fatigue associated with myasthenia gravis. Alternatively, lid retraction, along with proptosis can be indicative of dysthyroid eye disease. Unusual patterns of lid movement can also occur in relation to Duane's syndrome.
C) PrescriptionHypermetropia may indicate a long-standing accommodative squint, whereas prismatic correction is a sure sign of previous therapy for a binocular vision problem. REFRACTIVE:? Edge effects of high prescription spectacles or
bifocals? Prismatic effect in ill-fitted spectacles? Contact lens edge effects
Diagnostic featuresConsistent image separation in different direction of gaze disappears on removal of refractive correction.
3. Monocular Testsa) Monocular occlusionMonocular diplopia may be present in each eye (eg. cortical diplopia) or in one eye only.
b) VA with and without pin-holeRefractive monocular diplopia will normally disappear through a pinhole.c) Amsler chartMetamorphosis could indicate an association with macula pathology.
d) Binocular Diplopia Diagnostic FeatureDiplopia resolved by occlusion of either eye.Physiological: Patient suddenly becomes aware of physiological diplopia of objects in front of or behind fixation.
Diagnostic FeatureDiplopia normally noticed fleetingly and only when tired.
Defective muscle Affecting right eye Affecting left eye
Chin Turn Tilt Chin Turn Tilt
Lateral Rectus x right x x left x
Medial Rectus x left x x right x
Superior Rectus up right right up left left
Inferior Rectus down right left down left right
Superior Oblique down left left down right right
Inferior Oblique up left right up right left

Verge Journal of the Venu Eye Institute & Research Centre 19 October - December 2013
4. Cover testThe cover test should be performed, at least initially, using an accommodative target for fixation. Any variation in the horizontal angle of deviation with accommodative effort needs to be taken into consideration when Performing ocular motility. Binocular diplopia is normally due to misalignment of the visual axis, so a movement of the deviating eye to take up fixation will be seen on occlusion of the fixating eye. Long-standing deviations can have intermittent suppression, so the cover test could reveal a misalignment of the visual axis even when there is no subjective report of diplopia. When the patient's symptoms suggest that the presenting diplopia is related to close work, the near cover test should be performed. This will differentiate between a defect of the convergence/ accommodation system and one in which the symptoms are evoked by down gaze. 'A's and 'V's and SO palsies may fall into this latter group. Where there is an incomitancy, the angle of deviation normally differs depending on the fixating eye, with the secondary deviation being larger than the primary. The cover test should be repeated with and without any abnormal head posture. Normally, the angle of deviation will reduce with the head posture and a previously manifest deviation will become latent. It is necessary to determine whether the diplopia and manifest deviation are constant or intermittent, and whether the angle of deviation varies with fixation distance
5. Ocular motilityTo assess binocular versional eye movements, but where there appear to be restrictions it can also be used to examine monocular duction. Ocular motility is generally undertaken without spectacles while the patient fixates a spot light.
6. Near point of convergence Assessment of convergence can also provide useful information in differentiating a supranuclear from an infranuclear defect. The
anatomical centres for generation of horizontal eye movements and for convergence are located in different areas of the brain stem.
7. Fixation disparityAssessment of fixation disparity aids in the diagnosis of a decompensating heterophoria. Where a patient complains of intermittent diplopia, but on examination there is no manifest deviation, the presence of an uncompensated element may suggest a tendency for decompensation under conditions of visual stress.
8. Measurement of angle of deviationMeasurement of the deviation in different directions of gaze may help to confirm the direction of maximum misalignment of the visual axis. It can be useful to use an accommodative target for fixation when assessing A's and V's. The horizontal angle of the deviation will vary with accommodative effort in the primary position, up and down-gaze. In true incomitancies, the angle of deviation differs depending on which eye is fixating. In order to use the prism cover test to measure the angle when fixating with the right eye, for example, the strength of prism should be adjusted until the movement of the left eye is nulled. When fixating with the right eye, the angle of the left eye is being measured, and when fixating with the left eye, the angle of the right eye is being measured. As the secondary angle of a deviation is the greater, measurement of the angle of deviation fixating each eye in turn can help determine the eye with the defect.
Maddox double rod testConventional methods of measuring the angle of deviation can be used to measure the vertical and horizontal elements of a deviation, but cannot measure the torsional element. Maddox rods at the same orientation in front of each eye (normally vertically orientated to produce a horizontal streak) can be used to assess the angle

20 Verge Journal of the Venu Eye Institute & Research Centre
of torsion. If the streaks seen by each eye are not parallel, then the rods can be rotated until the streaks become parallel and horizontal, thus giving a measure of the rotation required and hence the torsion. This test is maximally dissociating and can produce erroneous results. Bagolini lenses can be used in the same way, but this method tends to underestimate the angle of torsion, due to fusion. In IVth nerve palsy, torsion greater than 10° is often thought to indicate a bilateral rather than unilateral condition.
9. Bielschowsky TestDue to the development of the muscle sequelae, the eye movement pattern in a longstanding SO palsy in one eye can be difficult to differentiate from a SR palsy of the other eye. If a patient has a SO palsy, as the head is tilted towards the affected side, the SR acts unopposed, so it not only intorts the eye but also elevates it.To perform the test, seat the patient upright, maintaining steady fixation straight ahead at a distance of 3m, so that fixation doesn't favour either the SO or SR. Tilt the head towards the eye with the suspected SO palsy (the hypertropic eye) and if the vertical angle of the deviation increases RSO the muscle is considered as SO.The Bielschowsky head tilt test can be used to differentiate a RSO and palsy from an LSR palsy. When the head is straight, the affected right eye is slightly hypertropic, esotropic and extorted. The angle of the right hypertropia increases on tilting the head towards the right shoulder (the affected side). This would not occur in a Left Superior Rectus Palsy. On tilting towards the left shoulder, there is little difference in the vertical angle of deviation.
10. Fusional ReservesMeasurement of fusional reserves can be of diagnostic value when differentiating long standing vertical muscle palsy from one of recent onset. Deviation will usually have a normal vertical fusion range (4D - 6D). Vertical fusion ranges can also increase over a long period of
gradual change in the direction of the visual axes.Measurement of the vertical fusion range can be done with the patient fixating either a near or a distant target. Patients with long-standing deviations may not appreciate diplopia after fusion breaks, so it may be useful to introduce visual controls to ensure neither eye is being suppressed. If a pen torch is used to illuminate a near fixation target, and obliquely orientated Bagolini lenses are positioned in front of each eye, the streaks produced by the Bagolini lenses can act as a control.
11. Diplopia ChartingThis can be a useful tool for differential diagnosis of incomitancy. A vertical bar of light is viewed through red and green goggles at a fixed distance from the eye. The bar light is moved into each direction of gaze, and the patient describes the image separation and appearance. The image separation can be measured. The red filter is always placed before the right eye. When interpreting a diplopia chart, it should always be remembered that the most distal image belongs to the under-acting eye. The position of the image is the reverse of the position of the eye. It is important to mark the patient's right and left on the chart. Ideally, the distance of fixation and image separation should also be recorded.
12. Field of binocular single vision (BSV)The field of BSV is a test used to describe the areas of BSV, and hence diplopia. It is very simple to do using a kinetic perimeter, or to approximate from ocular motility. The patient is seated at the perimeter, with the chin central to fixation. The target is moved outwards until the patient recognizes diplopia, and the point is marked. The target is then moved further until one image disappears, normally due to occlusion by facial contours, and this point is marked. The inner ring describes the area of BSV, the outer ring describes the limits of the binocular field of fixation.

Verge Journal of the Venu Eye Institute & Research Centre 21 October - December 2013
Jackson’s cross-cylinder technique Mr. Tarun Goyal, Optometrist Fellow
Venu Eye Institute & Research Centre
The cross cylinder is a combination of two cylinders of equal strength, but with opposite sign placed with their axis at right angle to each other and mounted on a handle. The commonly used cross cylinders are of +/- 0.25 and +/-0.50D. The Jackson cross cylinder, in Edward Jackson's words, is probably 'far more useful and, far more used' than any other lens in clinical refraction. E v e r y practitioner should be f a m i l i a r w i t h t h e principles involved in i t s u s e . A l t h o u g h the c ross cylinder is usually used to refine the cylinder axis and power of a refraction already obtained, it may also be used for the entire astigmatic refraction.
There are some steps followed in cross-cylinder refraction.
Adjust sphere to the most plus or least minus that gives best visual acuity. This is done by fogging the eye (adding plus sphere before the eye), while viewing a visual acuity chart, and then decreasing the fog until best visual acuity is obtained. The goal, if astigmatism is present, is to place the circle of least diffusion of the conoid of sturm on the retina, thus creating mixed astigmatism.
Discovering the astigmatism if no cylindrical correction is present initially, the cross cylinder may still be used, placed arbitrarily horizontally, vertically & obliquely to check for the astigmatism. If a preferred flip position is found, a cylinder is added with axis parallel to the respective plus or minus axis of the cross cylinder
Refinement of the axis: It is always done first. This is because the correct axis can be found in the presence of an incorrect power, but the full cylinder power will not be found in the presence of an incorrect axis. To refine the axis cross cylinder (+/-0.50D) is placed before the eye with its axis at 45 degree to the axis of cylinder in trial frame (first with -0.50D cylinder and then +0.50D cylinder or vice versa) and the patient is asked to tell about any change in the visual acuity. If the patient notices no difference between the two positions, the axis of the correction cylinder in the trial frame is correct. However, if the visual improvement is attained in one of the position, a 'plus' correcting cylinder should be rotated in direction of the plus cylindrical components of the cross cylinder (and vice versa). The test is then repeated several times until the neutral point is reached.
Refinement of cylinder power: To check the power of the cylinder, the cross cylinder of +/-0.25D is placed, with i t s a x i s parallel to the axis of the cylinder in the trial frame, f i r s t w i t h opposite sign. In the first position the cylinder correction is enhanced by 0.25D and in the second it is diminished by the same amount. When the visual acuity does not improve in either of the position, the power of cylinder in trial frame is correct. However, if the visual acuity improves in any of the position, a corresponding correction should be made and re verified till final correction is attained.

Volume 17 issue 1VERGEOctober-December 2013
Applied for Registered With Registrar of Newspapers of India
Regd. No. PendingVolume 5 Issue 1